")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Development and Evaluation of an Educational Program for Community Pharmacists on Cardiovascular Risk Assessment
Authors Zolezzi M , Abdallah O , Sankaralingam S
Received 15 September 2019
Accepted for publication 6 March 2020
Published 22 June 2020 Volume 2020:13 Pages 623—632
DOI https://doi.org/10.2147/RMHP.S231075
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Monica Zolezzi,1 Oraib Abdallah,2 Sowndramalingam Sankaralingam1
1Department of Clinical Pharmacy and Practice, College of Pharmacy, Qatar University, Doha, Qatar; 2Hamad Medical Corporation, Doha, Qatar
Correspondence: Sowndramalingam Sankaralingam
Department of Clinical Pharmacy and Practice, College of Pharmacy, Qatar University, Building I 06, 2nd Floor, Room S A2.06, Doha, Qatar
Tel +974 4403 5618
Fax +974 4403 5551
Email [email protected]
Purpose: Cardiovascular disease (CVD) risk assessment is an important strategy for the prevention of CVD. Pharmacists play an important role in CVD risk assessment and management (CVDRAM). Our previous study identified gaps in knowledge among community pharmacists for the provision of CVDRAM services as assessed through patient simulation. Therefore, our objectives were: a) to develop and evaluate an educational program on CVD risk assessment for community pharmacists, b) to assess the knowledge and skills of participating pharmacists in assessing and managing CVD risk before and after enrolling in the educational program and c) to explore pharmacists’ satisfaction and perceived effectiveness of the educational program.
Methods: Using a blended learning instructional approach, the educational program for a subset of 25 community pharmacists recruited from our previous study consisted of two face-to-face workshops, and an online 5-module course on CVD risk factors such as hyperlipidemia, hypertension, diabetes, obesity, and smoking cessation based on principles of adult learning. A repeated measures study design was utilized by measuring participants’ knowledge on pre- and post-questionnaires and an objective structured clinical examination (OSCE) at the conclusion of the educational program was also used to assess its impact on the knowledge and skills of community pharmacists in the provision of CVD risk assessment and management (CVDRAM) services. The knowledge questionnaire was completed by 23 pharmacists while the OSCE was completed by 8 pharmacists. In addition, a survey assessed the pharmacists’ level of satisfaction with the educational program.
Results: At the conclusion of the educational program, the participating pharmacists achieved knowledge and skills for the provision of CVDRAM services. Knowledge scores in relation to CVDRAM significantly improved after the educational program [out of a maximum of 20 points, the median (interquartile range) = 9 (7– 9) at pre- vs 12 (12– 13) at post-educational program], p< 0.001. On the OSCE, the median (interquartile range) scores for Stations 1 and 2 were 66 (63– 71) and 71 (67– 76), respectively. Out of the 21 pharmacists that completed the satisfaction survey, 71% were very satisfied and 29% were satisfied with the educational program.
Conclusion: The educational program improved pharmacists’ knowledge and skills for the provision of CVDRAM services.
Keywords: community pharmacists, cardiovascular disease risk assessment, educational program, pharmacists’ preparedness, evaluation
Introduction
Cardiovascular disease (CVD) is the most common cause of death globally.1 In Qatar, CVD was responsible for 24% of the total deaths reported in 2013.2,3 Furthermore, reports from the World Health Organization (WHO) have indicated high prevalence rates of CVD risk factors in Qatar, such as tobacco smoking, hypertension, obesity, dyslipidemia and diabetes.2,4,5 Despite considerable evidence-based knowledge about risk factor management, CVD remains the leading cause of disability and premature death throughout the world.4 Consequently, WHO recommends prevention2,3 of CVD through early detection and management of individuals who are at a high risk of developing CVDs.1 This necessitates the need for development and implementation of highly accessible screening programs to assess and manage cardiovascular risk. A precise estimate of the absolute risk for developing a first CVD event using tools such as the Framingham Risk Score is preferred when making prevention and treatment recommendations.4,5
Community pharmacists are one of the most accessible healthcare professionals that have been shown to play an effective role in screening and reducing the severity of established risk factors, as well as in the primary prevention and management of CVD.6–9 There is sufficient evidence for improved clinical outcomes when pharmacists are involved in the assessment of cardiovascular risk as outlined below. A recent large multi-centered controlled trial involving 56 community pharmacies in Canada that enrolled 723 patients has shown a 21% reduction in risk for CVD events after 3 months among patients that were under the care of pharmacists with competence in providing CVD risk assessment and management (CVDRAM) services compared to pharmacists providing usual care.10 A pilot study of 12 pharmacists in Australia that provided care for 67 participants showed a significant 25% proportional risk reduction in overall CVD risk.11 A meta-analysis of 30 randomized controlled trials of pharmacist-directed care or -collaborative care resulted in significant improvements in systolic and diastolic blood pressure, total cholesterol, low-density lipoprotein – cholesterol and reduction in smoking.12
Despite this evidence, pharmacists in Qatar appear to be largely under-utilized and poorly integrated into primary care teams. In a recent study in Qatar, community pharmacists perceived a lack of education as the top barrier in the provision of services which promote cardiovascular health.13 In another recent study in Qatar, researchers worked with standardized patients (SPs) to assess the knowledge and skills of community pharmacists in the provision of CVD risk assessment services.14 The results of the study indicated a gap in the pharmacists’ competence for the provision of CVDRAM services.
Currently, community pharmacists in the State of Qatar are primarily involved in dispensing medications and providing counseling. The State of Qatar has prioritized health promotion as part of its National Health Strategy. Consequently, there are plans to introduce enhanced and advanced pharmacy services managed by community pharmacists. It is therefore important to assess their baseline knowledge and skills to provide further education to successfully implement such services. No studies to date have reported the development and evaluation of educational programs for capacity building on CVD risk assessment among practicing pharmacists. The aim of the current study is to 1) develop and implement a CVD risk assessment educational program for community pharmacists; 2) to objectively evaluate the impact of the educational program on the knowledge and skills of participating pharmacists and 3) to assess the participant’s perception of the educational program. We believe that this is a novel approach in Qatar and the materials developed will be updated and used in the future to train a large cohort of community pharmacists to advance their skills and knowledge.
One of the long-term goals of this study is to implement the provision of CV risk assessment services by community pharmacists in Qatar to improve patients' outcomes. Pharmacist intervention through CV risk assessment has been shown to reduce absolute risk of developing CV events.10,11 Importantly, recent studies in the Middle East region have shown community pharmacist interventions to reduce overall Atherosclerotic Cardiovascular Disease or Framingham risk score15,16 suggesting feasibility of such models in Qatar. Our previous study has shown that community pharmacists in Qatar are willing to learn and provide CVDRAM services.14 Therefore, this educational program can prove to be useful for the implementation of such services in Qatar.
Methods
Study Participants
Fifty pharmacists working in various community pharmacies in urban areas in the State of Qatar, whose preparedness in the provision of CVDRAM had been assessed during an interaction with a trained SP in our previous study,14 were invited to participate in this CVDRAM educational program. Twenty-five pharmacists participated in our current educational program.
Educational Program Development
A team of two pharmacists and a physician from the College of Pharmacy designed this educational program. Several international guidelines were used to develop the content of this program,2,17-20 which was delivered in a blended format consisting of two face-to-face workshops that lasted 3 hrs each, complemented by an online course developed using Articulate 360® software (Articulate Storyline 360, 2018).21 Appendix 1 provides a detailed outline of the educational program.
In the first workshop, participants were introduced to the role of community pharmacists in CVD risk assessment. CVD risk factors such as hyperlipidemia, hypertension, diabetes, obesity, and smoking cessation and approaches to the provision of CVDRAM services in community pharmacies were briefly reviewed. Following the first workshop, participants were given access to the web-based course which consisted of 5 learning modules, one for each of the preventable CVD risk factors mentioned above. Recommendations for pharmacological and non-pharmacological management strategies, reference to guidelines and additional resources were also provided. The modules consisted of lectures that were recorded directly into PowerPoint and converted into a web-based course using the online platform provided by the course builder software Articulate 360®. This software provides a slide-based presentation with audio, guided quizzes, and active hyperlinks. Prior to launching, the content was peer-reviewed by experts in the field, and then circulated to two pharmacy students. Experts and students provided feedback (in the form of reflection notes) on content, format and overall impression of the course content. Their reflections were taken into considerations before launching the final version of the online course. The workshop, web-based learning modules and OSCE components were accredited by the Qatar Council for Healthcare Practitioners (QCHP) and participating pharmacists will receive continuous education (CE) credits.
Box 1 describes the content of the final version of the online course which continued to be available to participants beyond the study completion. Figure 1 shows a screenshot of the web-based course.
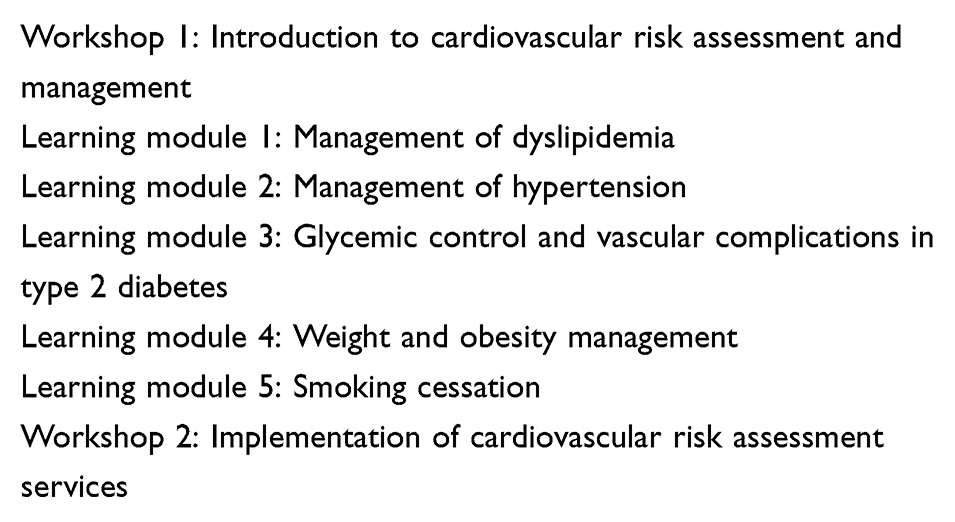 |
Box 1 Content of the Final Version of the Online Course on CVDRAM |
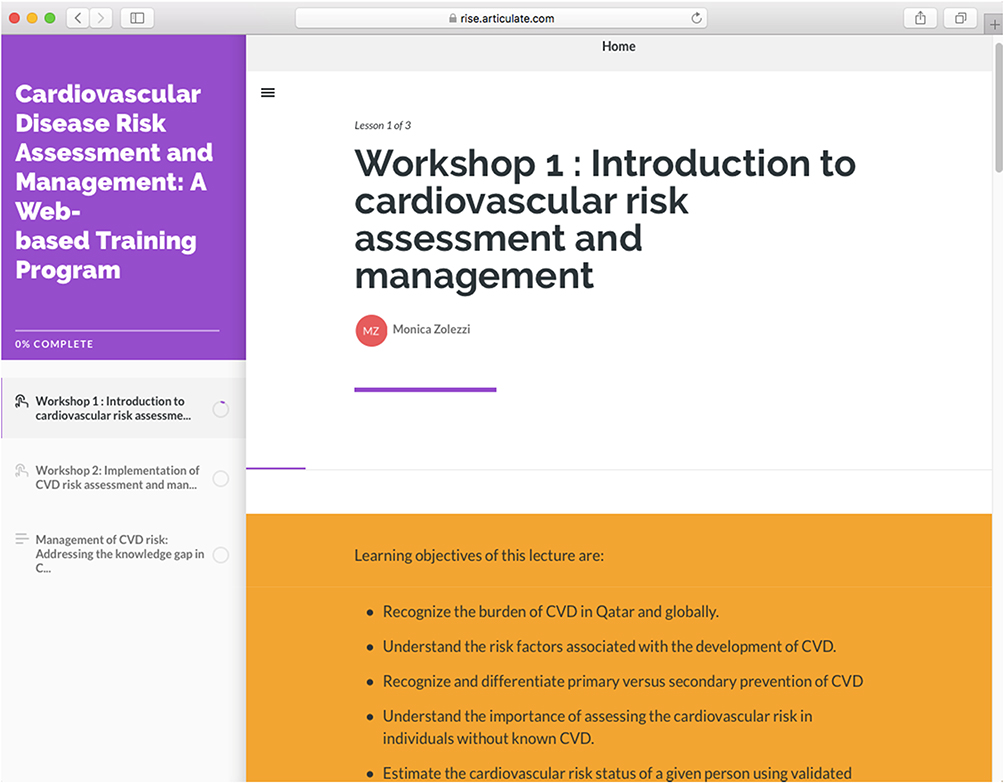 |
Figure 1 Screenshot of web-based course builder using Articulate 360® software. Representative screenshot of a course module developed using the Articulate 360® software is shown. |
The second face-to-face workshop was scheduled 1 month later, at which participants were introduced to the steps in the implementation of CVDRAM services, and provided them with the opportunity to have hands-on training on the use of screening tools and point-of-care (POC) devices appropriate for use in community pharmacies for assessing cardiovascular risk factors. In addition, participants were trained on physical examination skills necessary for CVD risk assessment such as measurement of blood pressure, height, and weight. As recommended in the guidelines on which this educational program was based on2,17-20 primary health care professionals need to convey information to patients in a way that allows them to understand their cardiovascular risk and the potential effects of lifestyle or pharmacological interventions, to actively engage patients in shared decision-making. As such, during the second workshop, participants also had the opportunity to interact with SPs in order to enhance their communication skills necessary for the provision of CVDRAM services. The case scenarios on which the SPs were trained and the SPs participating in this workshop were the same as those utilized in our previous study.14 Video recordings of both workshops were also incorporated into the final version of the web-based course.
Assessment
An attempt was made to follow the Kirkpatrick’s evaluation framework to assess the course outcomes. The Kirkpatrick’s framework is a widely used evaluation model to assess the effectiveness of CPD training and learning, a systematic approach consisting of four levels of evaluation involving examination of a course on multiple levels using different data sources.22 This model has been applied by several other researchers when developing courses in pharmacy practice education.23–27 As such, the course used pre-/post-questionnaires, interactive quizzes through the online module, SPs, OSCE and a satisfaction survey in an attempt to assess all 4 levels of Kirkpatrick’s evaluation framework.
Assessment of Participants’ Knowledge and Skills
Pre- and post-knowledge questionnaires were used to evaluate the impact of the educational program on pharmacists’ knowledge. A set of 13 multiple-choice questions and 7 true/false questions were developed based on the content covered in the workshops and in the 5 learning modules. The pre- and post-knowledge questionnaires used as part of the assessment process are provided as Appendix 2 and 3 respectively. The questions focused on knowledge related to risk factors necessary for estimating CVD risk, and on management guidelines including pharmacological and non-pharmacological approaches.
Upon completion of the educational program, competence in CVD risk assessment was assessed through an objective structured clinical examination (OSCE) that was offered to all participating pharmacists. The assessment consisted of two stations facilitated by the same trained SPs who participated in the second workshop. In Station 1, competence in performing physical examinations that are necessary for assessing CVD risk factors was evaluated. In Station 2, participants interacted with an SP and gathered relevant information for estimating the SP’s absolute CVD risk. At this station, participants also explained to the SP the meaning of the estimated CVD risk in lay language, and drafted an outline for lifestyle changes or pharmacological interventions necessary to address the SP’s CVD risk. The participant’s skills in this station were assessed using the same checklist that was used in our previous study14 which evaluated 3 competencies: CVD risk assessment, CVD risk management, and participant’s engagement with the SP. A passing mark for the OSCE was set at ≥65%. Thirty percent of the passing mark was derived from the participant’s performance in Station 1, and 70% from the participant’s performance in Station 2. The OSCE checklist for stations 1 and 2 are included as Appendix 4 and 5, respectively.
Satisfaction
A survey to assess the participants’ satisfaction and perceived effectiveness of the educational program was administered at the end of the educational program. Based on literature review, a 5-point Likert scale ranging from “Definitely yes”, “Some”, “Not sure”, “Not quite” to “Definitely not” was used to evaluate the level of satisfaction.28,29 For those who accepted to take part in the OSCE, a list of open-ended questions was given at the end asking them to reflect on various aspects of the educational program provided, about their OSCE experience, what they felt about doing things differently at their practice sites, and which steps they felt they were more prepared to take on the basis of what they had learnt through their participation in this educational program.
Data Analyses
Data were entered into SPSS® v.22 (IBM, New York, USA) to perform descriptive and inferential analyses. The One-Sample-Kolmogorov–Smirnov test determined that the data was “not normally” distributed. Therefore, descriptive statistics are expressed as median and interquartile range (IQR), and frequencies are expressed as number (n) and percentage (%) to present the results from pre- and post-questionnaires and from the satisfaction survey, as appropriate. Statistical significance of knowledge data before and after the educational program presented in Tables 1 and 2 were compared using the Wilcoxon signed-rank test and the McNemar Chi-square test, respectively.
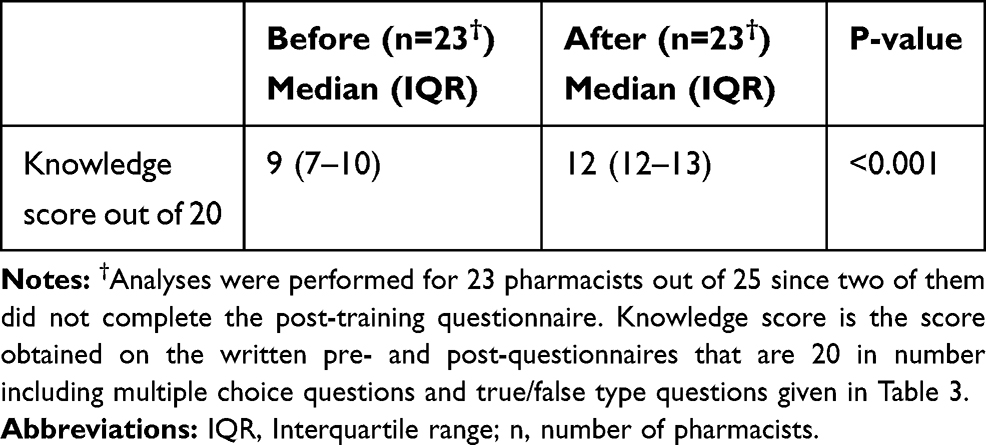 |
Table 1 Evaluation of Participants’ Knowledge in CVDRAM |
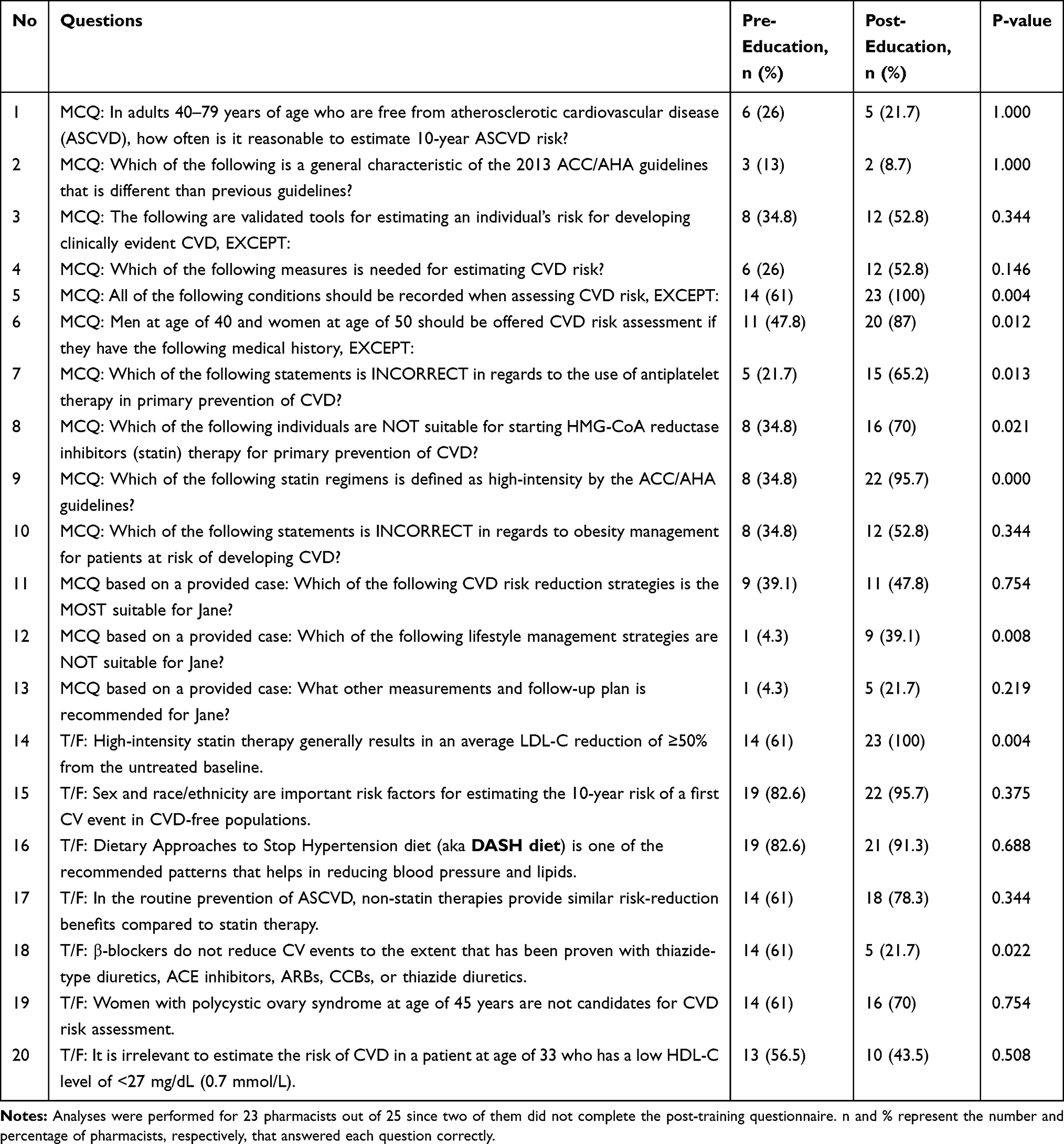 |
Table 2 Responses to Knowledge Questions in Pre- and Post-Education Questionnaire |
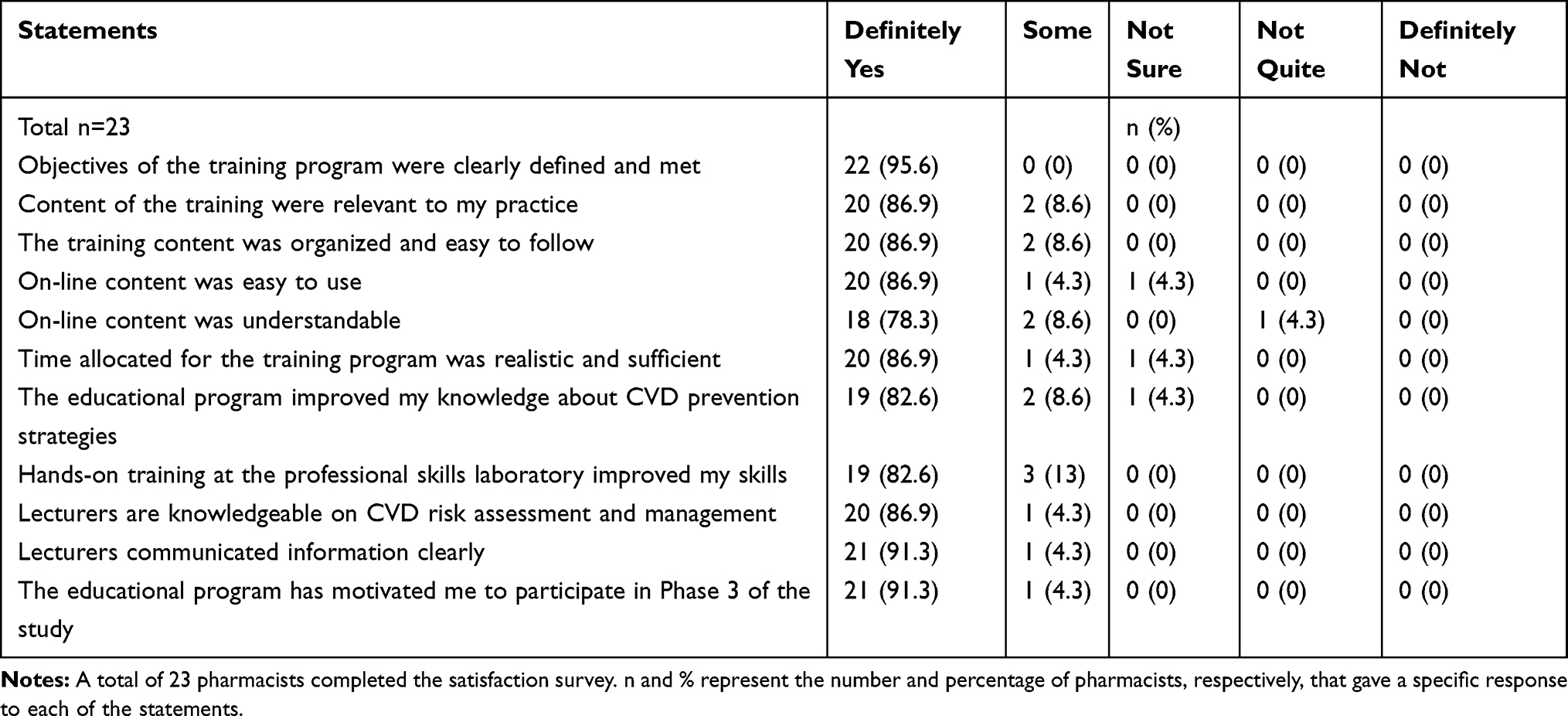 |
Table 3 Pharmacists’ Rating of the Individual Items on the Satisfaction Survey |
Ethical Compliance
Ethics approval for conducting this study was received from Qatar University Institutional Review Board (QU-IRB) in November 2016 (reference number: QU-IRB 672-EA/16). The study was carried out in accordance with the principles of the Declaration of Helsinki. The confidentiality of participating pharmacists is maintained. Consent to publish was obtained from the pharmacists as indicated in the participant sheet and consent form.
Results
Out of the fifty pharmacists who participated in our previous study,14 50% (n=25) successfully completed the educational program, of which 8 agreed to be evaluated through the OSCE (32 % of participants who enrolled in the educational program).
Impact of the Educational Program on Pharmacists’ Knowledge and Skills
The knowledge and skills of participating pharmacists on CVDRAM improved significantly after participation in the educational program (Table 1). Out of a maximum of 20, their knowledge scores improved from 9 (7–10) to 12 (12–13) [median (interquartile range)], p<0.001. Table 2 shows the number of pharmacists who had correct responses to knowledge-based questions on the pre- and post-questionnaires. As shown in this table, the number of participating pharmacists answering each of the questions correctly at post-educational program were significantly higher than that at pre-educational program, except for questions 1 (p<1.000), 2 (p<1.000) and 18 (p<0.022).
All pharmacists achieved a passing score in physical examination and clinical decision making skills by obtaining a passing mark in the OSCE (≥65%). The median (interquartile range) score for Station 1 was 66 (63–71) out of 100. The median score for Station 2 was 71 (67–76) out of 100. The highest scores were 74 and 80 for Stations 1 and 2, respectively. To determine whether a participating pharmacist passed the OSCE, 30% weightage was given to scores from Station 1 and 70% weightage to scores from Station 2 to arrive at an aggregate of 65% minimum passing score.
Participant’s Perception of the Educational Program
As illustrated in Figure 2, the majority of participants indicated to be either satisfied or very satisfied with the educational program. Percentage of pharmacists rating the individual items of the satisfaction survey are shown in Table 3. Participants who were evaluated through OSCE reflected positively on their experience. Some of the comments provided are outlined in Table 4.
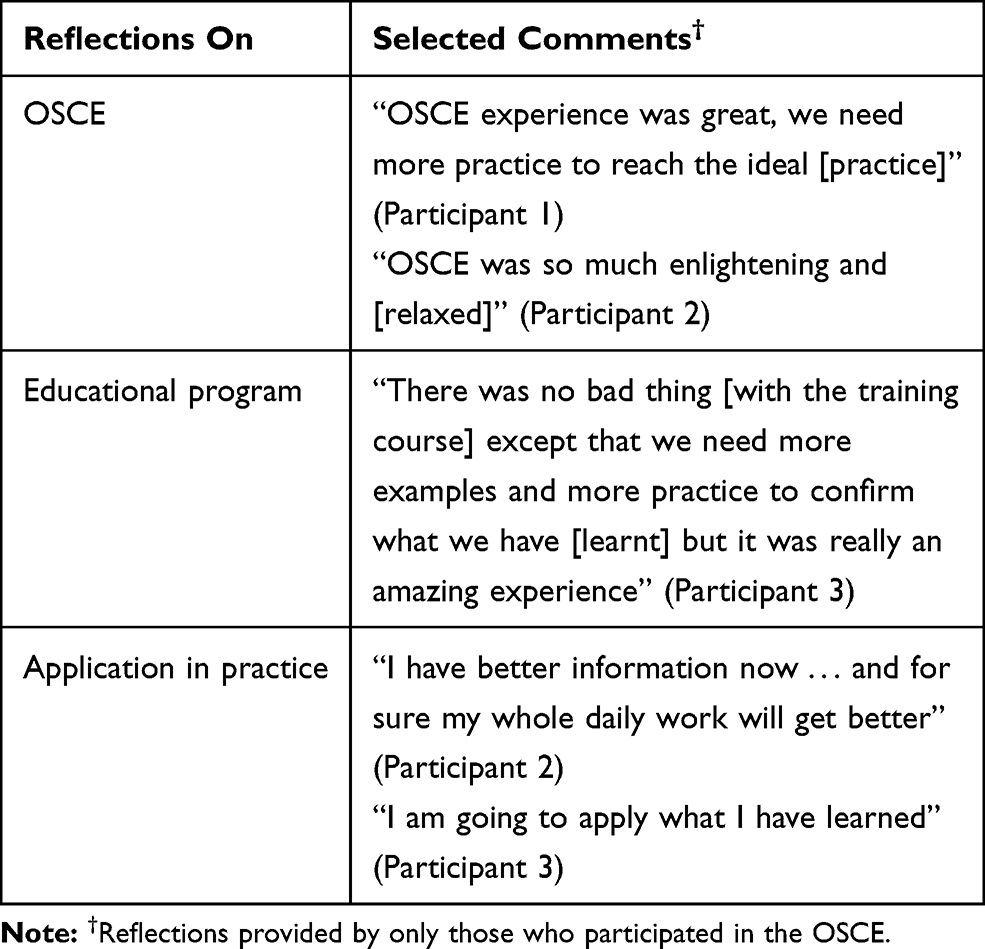 |
Table 4 Participants’ Selected Reflections on the Educational Program |
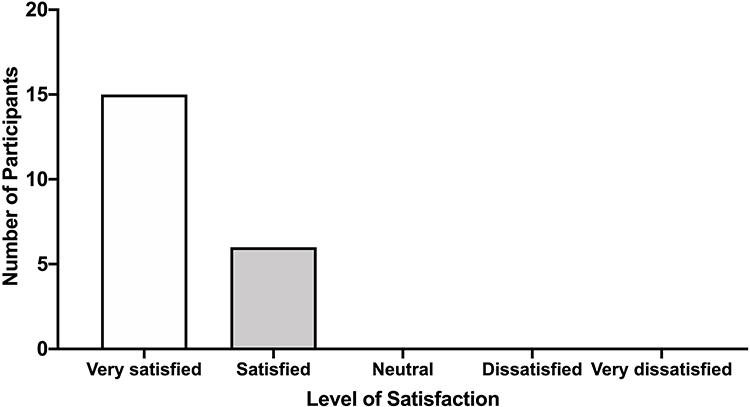 |
Figure 2 Participants’ satisfaction with the educational program. Participants were administered a satisfaction survey at the conclusion of the educational program that was graded on a 5-point scale (very satisfied, satisfied, neutral, dissatisfied and very dissatisfied). The height of the bars represents the number of respondents providing a given rating. |
Discussion
To the best of our knowledge, our study is novel in that this educational program in CVDRAM was designed systematically after obtaining pharmacists’ perceptions,14 baseline knowledge and skills and is the first of its kind to be delivered in Qatar. The study describes in detail the development of an educational program and its impact on the knowledge and skills of practicing community pharmacists to facilitate the provision of CVDRAM services. Moreover, the knowledge and clinical skills were evaluated using both written and OSCE formats.
Our CVDRAM course comprised a blended learning strategy that included direct instructions, self-study materials and multiple active learning components such as face-to-face interactive workshops that provided participants with the opportunity to familiarize with point of care (POC) devices and practice their physical assessment skills using SPs. To the best of our knowledge, this is the first study to include several learning strategies in a single educational program designed to train pharmacists on CVD risk assessment. Workshops,30,31 simulation-based training,32 direct instruction,33 use of SPs34,35 have been shown to improve knowledge and skills of pharmacists34,35 and students36 alike. The interaction with trained SPs during the workshops and the continuous availability of the workshop recordings incorporated into the online course provided participants with the opportunity to improve their communication skills and reduce their apprehension when delivering patient education on CVD risk and its management. Similar results were obtained in a study which assessed the learning outcomes when using a blended learning design to deliver a communication course to pharmacy students.37 Lastly, the study materials were made available throughout the educational program using Articulate 360® and supported the information delivered during the workshops. All of the components of the educational program were in line with advantages of blended learning courses previously described.38 Other authors have also reported on the successful use of earlier versions of this Articulate 360® web-based software in pharmacy education.39,40
The educational program was particularly effective in improving pharmacists’ knowledge on a number of concepts about CVDRAM, such as the management of dyslipidemia and blood pressure control. This improved knowledge may provide pharmacists with increased confidence to engage with patients for managing these important risk factors. A study on the provision of pharmaceutical care by community pharmacists reported improved adherence to statin therapy with positive clinical outcomes41 and on their counselling on lifestyle changes and DASH diet helped patients lower their blood pressure.42 Two of the three questions for which wrong responses prevailed in the post-questionnaire (specifically questions 1 and 2) were related to the CVDRAM guidelines. We speculate that the participants did not give much importance to this content. Studies have shown that healthcare providers are generally unaware of guidelines.43 Complexity of guidelines, lack of resources and time are other possible reasons why healthcare providers are not using guidelines.44 Our future educational programs will emphasize on guidelines and screening criteria for apparently healthy adults that would be translated into practice.
Despite the fact that all participants passed the OCSE, a low score was noted in the physical examination Station 1. This can be explained by two aspects. First, participants may be reluctant to learn and apply physical assessment skills in a community setting where the use of POC devices is not fully supported by Qatar Ministry of Public Health. Second, time to practice physical assessment skills during the workshops could have been insufficient. Thus, reassessing the course delivery for additional practice sessions or increased time for practice is needed to improve participant performance in the future. Compared to our previous study in which participating pharmacists averaged a score of 38%, participants performed well in the post-educational assessment. This could be due to lack of sufficient knowledge as well as unaware of being assessed during their community pharmacy practice work hours where they could have been busy with a series of customers and patients.
The educational program has also been positively evaluated by participating pharmacists, some of whom reported reflections indicative of them being likely to implement what was learnt into their practice settings. This is consistent with findings in similar studies which utilized courses with a blended-learning design to which participants reported positive learning experiences and high satisfaction ratings.39,45-47
Low sample size is a limitation of this study. However, the aim of this study was to describe the educational program and its potential application to pharmacy practice in Qatar and elsewhere. Results of the course assessments are informative and should be taken into consideration when deciding the type of educational strategies that are most suitable to deliver CPD programs to improve competencies of community pharmacists in Qatar. Future iterations of the course must more thoroughly evaluate all 4 levels of the Kirkpatrick’s evaluation framework, through administration of in-depth interviews with previous participants, their patients, and their managers.
Conclusions
Overall, the blended-learning educational program in CVDRAM was well received and successful in improving the knowledge and skills of the participating pharmacists. It represents an important resource and a first step in support of implementing access to CVDRAM services within primary care in Qatar.
Data Sharing Statement
Data supporting the results reported in the manuscript are currently securely stored in password-protected electronic format but can be obtained from the researchers. The content of the educational module described and evaluated herein is not publicly available and it is considered intellectual property of the researchers. Online access to the module is password protected. Access can be solicited to the researchers. No other data than the one presented herein remain unpublished.
Ethics and Consent Statement
Ethics approval for conducting this study was received from Qatar University Institutional Review Board (QU-IRB) in November 2016 (reference number: QU-IRB 672-EA/16). The study was carried out in accordance with the principles of the Declaration of Helsinki. The confidentiality of participating pharmacists is maintained. Consent to publish was obtained from the pharmacists as indicated in the participant sheet and consent form.
Acknowledgments
We thank all pharmacists who participated in the CVDRAM educational program and CPD-HP (QU Health) which is accredited by QCHP as a provider of CPD in Qatar for their assistance in accrediting the program.
Funding
This work was made possible by Qatar University (QU) grants QUUG-CPH-15/16-3 and QUST-CPH-SPR-15/16-15 awarded to Dr. Monica Zolezzi and Dr. Sowndramalingam Sankaralingam respectively. The publication of this article was funded by Qatar National Library.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Cardiovascular diseases. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
2. WHO. Prevention of cardiovascular disease: guidelines for assessment and management of cardiovascular risk. 2007. Available from: http://www.who.int/cardiovascular_diseases/guidelines/PocketGL.ENGLISH.AFR-D-E.rev1.pdf?ua=1.
3. Labarthe DR, Dunbar SB. Global cardiovascular health promotion and disease prevention: 2011 and beyond. Circulation. 2012;125(21):2667–2676. doi:10.1161/CIRCULATIONAHA.111.087726
4. Grundy SM, Pasternak R, Greenland P, Smith S
5. Cardiovascular disease risk assessment for primary prevention: our approach. 2019. Available from: https://www.uptodate.com/contents/cardiovascular-disease-risk-assessment-for-primary-prevention-our-approach.
6. Blenkinsopp A, Anderson C, Armstrong M. Systematic review of the effectiveness of community pharmacy-based interventions to reduce risk behaviours and risk factors for coronary heart disease. J Public Health Med. 2003;25(2):144–153. doi:10.1093/pubmed/fdg030
7. Ifeanyi Chiazor E, Evans M, van Woerden H, Oparah AC. A systematic review of community pharmacists’ interventions in reducing major risk factors for cardiovascular disease. Value Health Reg Issues. 2015;7:9–21. doi:10.1016/j.vhri.2015.03.002
8. Machado M, Bajcar J, Guzzo GC, Einarson TR. Sensitivity of patient outcomes to pharmacist interventions. Part II: systematic review and meta-analysis in hypertension management. Ann Pharmacother. 2007;41(11):1770–1781. doi:10.1345/aph.1K311
9. Sinclair HK, Bond CM, Stead LF. Community pharmacy personnel interventions for smoking cessation. Cochrane Database Syst Rev. 2004;(1):CD003698.
10. Tsuyuki RT, Al Hamarneh YN, Jones CA, Hemmelgarn BR. The effectiveness of pharmacist interventions on cardiovascular risk: the multicenter randomized controlled RxEACH trial. J Am Coll Cardiol. 2016;67(24):2846–2854. doi:10.1016/j.jacc.2016.03.528
11. McNamara KP, O’reilly SL, Dunbar JA, et al. A pilot study evaluating multiple risk factor interventions by community pharmacists to prevent cardiovascular disease: the PAART CVD pilot project. Ann Pharmacother. 2012;46(2):183–191. doi:10.1345/aph.1Q572
12. Santschi V, Chiolero A, Burnand B, Colosimo AL, Paradis G. Impact of pharmacist care in the management of cardiovascular disease risk factors: a systematic review and meta-analysis of randomized trials. Arch Intern Med. 2011;171(16):1441–1453. doi:10.1001/archinternmed.2011.399
13. El Hajj MS, Mahfoud ZR, Al Suwaidi J, Alkhiyami D, Alasmar AR. Role of pharmacist in cardiovascular disease-related health promotion and in hypertension and dyslipidemia management: a cross-sectional study in the State of Qatar. J Eval Clin Pract. 2016;22(3):329–340. doi:10.1111/jep.12477
14. Zolezzi M, Abdallah O, Kheir N, Abdelsalam AG. Evaluation of community pharmacists’ preparedness for the provision of cardiovascular disease risk assessment and management services: a study with simulated patients. Res Soc Admin Pharm. 2019;15(3):252–259.
15. Fahs IM, Hallit S, Rahal MK, Malaeb DN. The community pharmacist’s role in reducing cardiovascular risk factors in lebanon: a longitudinal study. Med Prin Pract. 2018;27(6):508–514. doi:10.1159/000490853
16. Jahangard-rafsanjani Z, Hakimzadeh N, Sarayani A, et al. A community pharmacy-based cardiovascular risk screening service implemented in Iran. Pharm Pract (Granada). 2017;15(2):919.
17. Anderson TJ, Gregoire J, Pearson GJ, et al. 2016 Canadian Cardiovascular Society guidelines for the management of dyslipidemia for the prevention of cardiovascular disease in the adult. Can J Cardiol. 2016;32(11):1263–1282. doi:10.1016/j.cjca.2016.07.510
18. Goff DC
19. Ministry of Public Health (MOPH), Doha Q. Clinical guidelines for the state of Qatar. Atherosclerotic cardiovascular disease risk assessment and management. 2016. Available from: https://www.moph.gov.qa/health-strategies/Documents/Guidelines/Guideline-ASCVD risk assessment and managementv1-1FINAL.pdfMOPH.
20. Zealand. MoHN. Cardiovascular Disease Risk Assessment and Management for Primary Care. Wellington: Ministry of Health; 2018.
21. ASC. 2018. Available from: https://articulate.com/360.
22. Kirkpatrick DL, Kirkpatrick JD. Evaluation of Training Programs: The Four Levels. San Francisco (CA): Berrett-Koehler Publishers; 1994.
23. Agness CF, Huynh D, Brandt N. An introductory pharmacy practice experience based on a medication therapy management service model. Am J Pharm Educ. 2011;75(5):82.
24. Bloom BS. Effects of continuing medical education on improving physician clinical care and patient health: a review of systematic reviews. Int j Technol Assess Health Care. 2005;21(3):380–385.
25. Ebn Ahmady A, Barker M, Fahim M, Dragonetti R, Selby P. Evaluation of web-based continuing professional development courses: aggregate mixed-methods model. JMIR Med Educ. 2017;3(2):e19. doi:10.2196/mededu.5993
26. Moore DE
27. Wilbur K, Shabana S, Maraghi F, ElMubark A, Kheir N. An evaluation of the translation of continuing education into diabetes public health care by pharmacists. Int J Clin Pharm. 2017;39(4):774–782. doi:10.1007/s11096-017-0477-8
28. Abdulghani HM, Shaik SA, Khamis N, et al. Research methodology workshops evaluation using the Kirkpatrick’s model: translating theory into practice. Med Teach. 2014;36(Suppl 1):S24–S29. doi:10.3109/0142159X.2014.886012
29. Gheewala PA, Peterson GM, Zaidi ST, Bereznicki L, Jose MD, Castelino RL. A web-based training program to support chronic kidney disease screening by community pharmacists. Int J Clin Pharm. 2016;38(5):1080–1086. doi:10.1007/s11096-016-0330-5
30. Keller DR, O’dell DV, Skochelak SE, Cochran GL, Shull SJ, Gjerde CJ. Teaching the basics of clinical pharmaceutical care: innovative pharmacy workshops at the University of Wisconsin and the University of Nebraska. Fam Med. 2004;36(Suppl):S89–S92.
31. Mehra IV, Wuller CA. Evaluation of a pilot clinical skills workshop series for community pharmacists. Am J Pharm Educ. 1998;62:136–141.
32. Crea KA. Practice skill development through the use of human patient simulation. Am J Pharm Educ. 2011;75(9):188. doi:10.5688/ajpe759188
33. Fakeye TO, Adisa R, Erhun WO. Developing a model for teaching and learning clinical pharmacy components of the pharmacy curriculum in Nigeria. Pharm Educ. 2017;17:60–66.
34. Garcia Corpas JP, Ocana Arenas A, Gonzalez Garcia L, et al. Changes in knowledge after attending a community pharmacists’ asthma workshop. Pharm Pract (Granada). 2006;4(3):139–142.
35. Nguyen TS, Nguyen TLH, Van Pham TT, Hua S, Ngo QC, Li SC. Pharmacists’ training to improve inhaler technique of patients with COPD in Vietnam. Int J Chron Obstruct Pulmon Dis. 2018;13:1863–1872. doi:10.2147/COPD.S163826
36. Bolesta S, Trombetta DP, Longyhore DS. Pharmacist instruction of physical assessment for pharmacy students. Am J Pharm Educ. 2011;75(2):29. doi:10.5688/ajpe75229
37. Hess R, Hagemeier NE, Blackwelder R, Rose D, Ansari N, Branham T. Teaching communication skills to medical and pharmacy students through a blended learning course. Am J Pharm Educ. 2016;80(4):64. doi:10.5688/ajpe80464
38. Garrison DR, Kanuka H. Blended learning: uncovering its transformative potential in higher education. Internet High Educ. 2004;7(2):95–105. doi:10.1016/j.iheduc.2004.02.001
39. Crouch MA. An advanced cardiovascular pharmacotherapy course blending online and face-to-face instruction. Am J Pharm Educ. 2009;73(3):51. doi:10.5688/aj730351
40. Tangiisuran B, Tye SC, Tan KW. Implementation and assessment of flipped classroom learning on medication distribution system to pharmacy undergraduates. Pharm Educ. 2017;17(1):109–114.
41. Vegter S, Oosterhof P, van Boven JF, Stuurman-bieze AG, Hiddink EG, Postma MJ. Improving adherence to lipid-lowering therapy in a community pharmacy intervention program: a cost-effectiveness analysis. J Manage Care Spec Pharm. 2014;20(7):722–732. doi:10.18553/jmcp.2014.20.7.722
42. Cheema E, Sutcliffe P, Singer DR. The impact of interventions by pharmacists in community pharmacies on control of hypertension: a systematic review and meta-analysis of randomized controlled trials. Br J Clin Pharmacol. 2014;78(6):1238–1247. doi:10.1111/bcp.12452
43. Zeng L, Li Y, Zhang L, et al. Guideline use behaviours and needs of primary care practitioners in China: a cross-sectional survey. BMJ Open. 2017;7(9):e015379. doi:10.1136/bmjopen-2016-015379
44. Rauh S, Arnold D, Braga S, et al. Challenge of implementing clinical practice guidelines. Getting ESMO’s guidelines even closer to the bedside: introducing the ESMO Practising Oncologists’ checklists and knowledge and practice questions. ESMO Open. 2018;3(5):e000385. doi:10.1136/esmoopen-2018-000385
45. Carbonaro M, King S, Taylor E, Satzinger F, Snart F, Drummond J. Integration of e-learning technologies in an interprofessional health science course. Med Teach. 2008;30(1):25–33. doi:10.1080/01421590701753450
46. Pahinis K, Stokes CW, Walsh TF, Cannavina G. Evaluating a blended-learning course taught to different groups of learners in a dental school. J Dent Educ. 2007;71(2):269–278.
47. Shaw T, Long A, Chopra S, Kerfoot BP. Impact on clinical behavior of face-to-face continuing medical education blended with online spaced education: a randomized controlled trial. J Contin Educ Health Prof. 2011;31(2):103–108. doi:10.1002/chp.20113
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.