")
Back to Journals » Clinical Interventions in Aging » Volume 13
Development and assessment of a web-based intervention for educating older people on strategies promoting healthy cognition
Authors Vanoh D, Ishak IH, Shahar S, Manaf ZA, Ali NM, Noah SAM
Received 17 November 2017
Accepted for publication 12 March 2018
Published 17 September 2018 Volume 2018:13 Pages 1787—1798
DOI https://doi.org/10.2147/CIA.S157324
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Walker
Divya Vanoh,1,2 Intan Hafizah Ishak,1 Suzana Shahar,1 Zahara Abdul Manaf,1 Nazlena Mohamad Ali,3 Shahrul Azman Mohd Noah4
1Centre for Healthy Aging and Wellness, Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia; 2Dietetics Programme, School of Health Sciences, University Sains Malaysia, Kubang Kerian, Kelantan, Malaysia; 3Institute of Visual Informatics (IVI), Universiti Kebangsaan Malaysia, Bangi, Selangor, Malaysia; 4School of Information Technology, Faculty of Information Science and Technology, Universiti Kebangsaan Malaysia, Bangi, Selangor, Malaysia
Background: The increase in the population of aging people has increased the occurrence of cognitive decline leading to predemented stage of dementia, ie, mild cognitive impairment (MCI). The cognitive tools that are web-based have been proven to be useful in decreasing the risk of MCI. Thus, in the present study, an education tool that is web-based, called WESIHAT 2.0©, had been created to educate elderly people about precautionary strategies against MCI.
Methodology: WESIHAT 2.0 was devised in a senior-friendly style, which includes touch screen, greater font size, larger icons, and employed multimedia components of text, images, and videos. The components employed in WESIHAT 2.0 were a screening tool called TUA-WELLNESS, 10 guides for memory improvement, health diary, and guide for a healthy menu. This application assessed a group of 73 candidates consisting of elderly people, health professionals, caregivers, and information technology (IT) professionals for 1 month.
Results: All the elderly people, caregivers, and 75% of IT and health professionals were satisfied with the subject matter of WESIHAT 2.0. About more than half of the elderly people, caregivers, and IT and health professionals had given a consensus on the comprehensive ease of the terminologies, sentences, images, table, and advice related to diet included in the web application. Proposals for improvements of the web portal included suggestions such as using smaller sentences, using greater font size, adding more images, and avoiding the use of unfamiliar terminologies.
Conclusion: WESIHAT 2.0 is a suitable tool for educating older people about the lifestyle modification strategies to slower progression to cognitive impairment, with regard to the significance of expert advice.
Keywords: senior-friendly, computer, health, lifestyle, education tool
Introduction
The problem of aging has become a major public health matter. With declining rate of mortality, the population of elderly people has been increasing worldwide, which causes worries among health care professionals, caregivers, and ruling government because of increased health care liability and expenses to treat elderly people who are usually at a greater health risk.1,2 The number of older people burdened with dementia is expected to increase to >115 million by year 2050.3 Dementia is an irreversible neurodegenerative disease that affects the cognitive function and capability of elderly in performing activities of daily living. The global rise in the prevalence of dementia has a negative impact on the life quality of elderly people and their caregivers.4 On the other hand, the predementia stage of cognitive impairment is known as a mild cognitive impairment (MCI).5 Early detection of MCI, as mentioned by Petersen et al,6 as the reversible phase between normal aging and memory loss is desirable. MCI involves impairment in a cognitive test, minor forgetfulness, or trivial impairment in instrumental actions of daily life such as being incapable to take own medicines or to transport oneself outside.7
Using tools to fight MCI has been a vast area of research considering the increasing occurrence of MCI. Recently, Krell-Roesch et al8 proved that employment of computers has decreased the MCI risk after 4 years among 1929 cognitively normal elderly people who have taken part in the Mayo Clinic Ageing Study. This is synchronous with the growth of the e-health field, especially in the health care sector.9 Health-related tools based on the Internet for elderly people are cost-efficient and may support patient empowerment in managing their own health to decrease the increasing cost of health care.10 More frequently, the society had observed that elderly people may not be too aware about the Internet use. Nevertheless, a survey has demonstrated that there has been an increase in the number of elderly people surfing the web in America between 2000 and 2016.11 Several websites were accessible for management of recurrent diseases such as diabetes,12–15 cardiovascular ailments,16 and blood pressure problems.17 Anstey et al18 have created a web-based application for recognizing dementia. Identification of threat of cognitive impairment is yet in its early stages and requires further research. Therefore, this study sought to develop a comprehensive website for educating the elderly regarding the lifestyle modification strategies for slowing progression to MCI and to further analyze the website acceptance among healthy elderly people.
Methodology
Development of WESIHAT 2.0© web-based application
WESIHAT 2.0 is an acronym for “WargaEmasSihat”, which means healthy senior citizens. The creation of WESIHAT 2.0 involved a number of stages: 1) content study by thorough literature review; 2) designing the web application considering its target users; 3) assessment of acceptance; and 4) redesigning the web application based on users’ comments in the acceptance stage. The first phase was the formation of a team consisting of experts from multidisciplinary domains such as physiotherapists, dieticians, psychogeriatrician, optometrist, audiologist, and web designers. A systematic review of the literature was conducted considering risk factors causing cognitive decline such as eating habits, exercise, good health, smoking, alcohol, and mental activities. The data collected were reviewed thoroughly, and the contents were developed based on suitability of the local context. For instance, food choices selected for the web application were the usual food items consumed by the Malaysians. The website content was based on the data gathered from the study of literature and the outcome from the evaluation of the first phase of the research.19
Another step in the development of WESIHAT 2.0 was the website designing considering the target users who were chiefly elderly people. WESIHAT 2.0 was proposed and implemented with the inclusion of multimedia components such as text, images, and videos. Not much text was included in the design of interface, and more images were added to represent textual data. WESIHAT 2.0 was a website that was senior friendly, developed for elderly people with poor vision, concentration, and motor functioning. Therefore, several approaches were taken into account in the designs of the touch screen-based user interface (UI), greater font size, larger icons such as the backward and forward arrow, and the button of home page for better visibility for elderly people, easy page navigation, and using Sans Serif font type.20,21
WESIHAT 2.0 employed Malay language and comprised four modules called tool for the detection of memory impairment (TUA-WELLNESS), 10 guides for memory enhancement, health diary, and guide for healthy menu. The first component is the TUA-WELLNESS tool for screening, which comprised 10 items focusing on diet, health, quality of life, working status, and involvement in lifestyle activities (UI of TUA-WELLNESS is shown in Figure 1). After giving response to all questions, users can view and download their individual report with suggestions. Users with 11 points and above were considered to be at decreased risk of cognitive impairment.22
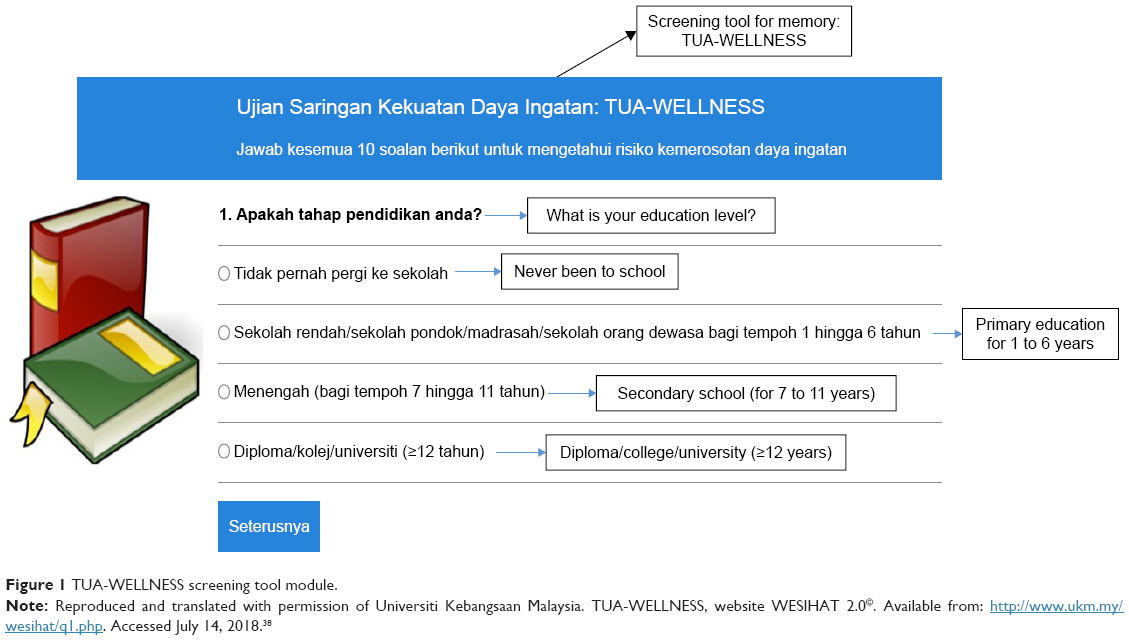 | Figure 1 TUA-WELLNESS screening tool module. |
The “Panduan Meningkatkan Daya Ingatan” (Guides for Memory Enhancement) contained 10 comprehensive suggestions for enhancement of cognition among elderly people such as consuming more fruits and vegetables, controlling blood cholesterol, controlling blood sugar, increasing fish intake, practicing calorie-restricted diet, engaging in mental stimulation activities, being active physically, avoiding smoking and reducing alcohol intake, practicing optimistic attitude, and holistic health care. These 10 suggestions were obtained from reviews of previous literature and a local demonstrative study performed among 1993 Malaysian older people for discovering risk factors regarding cognitive impairment (Figure 2 shows the UI of the 10 guides for memory enhancement).19
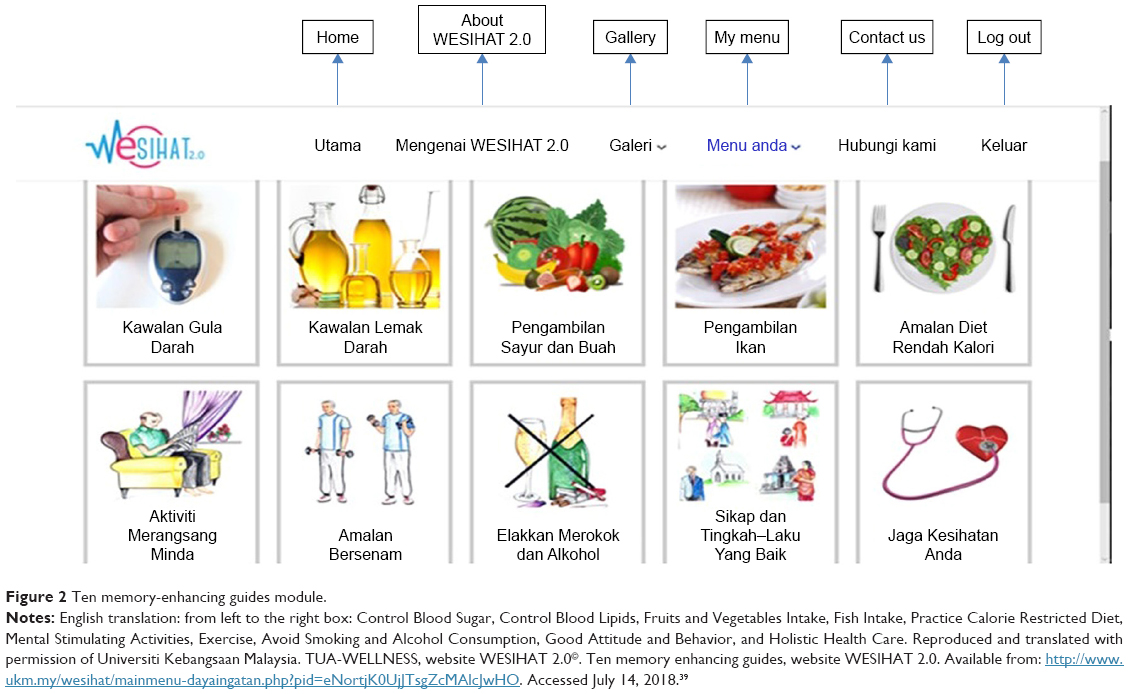 | Figure 2 Ten memory-enhancing guides module. |
Alternatively, health diary is a web-based biochemical recording system for the result of user’s blood test to replace traditional filing approach. Health diary was vital for both the users and the health practitioners to keep track of the results of the participant’s blood test over time (an instance of the UI is shown in Figure 3).
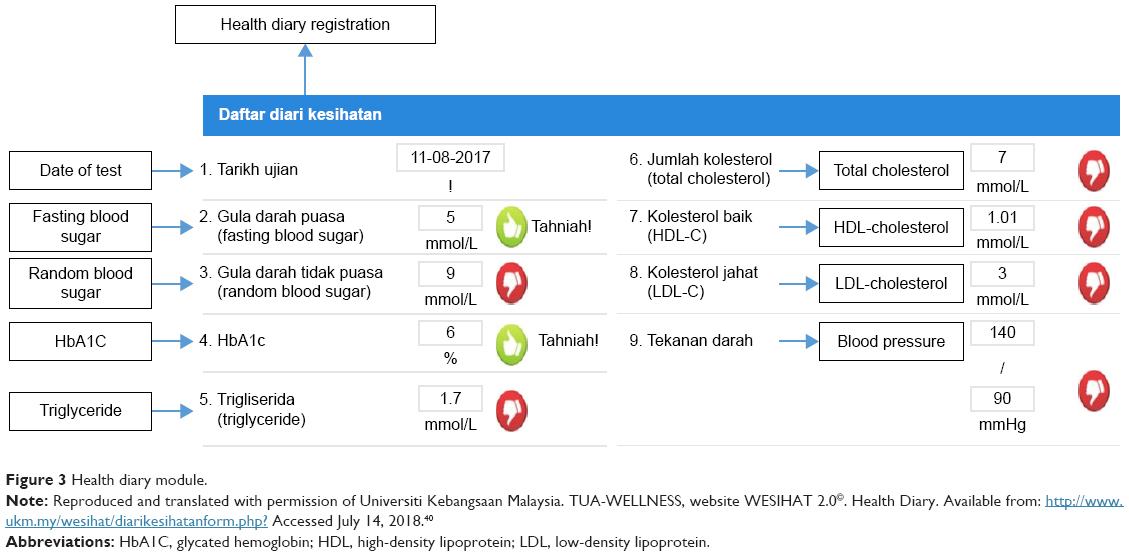 | Figure 3 Health diary module. |
Moreover, the Guide for Healthy Menu contained healthy recipes and videos for people belonging to different ethnicities showing methods to cook simple food by use of healthy cooking procedures. Additionally, this section had clever shopping tips as well as a quiz section for the assessment of user’s knowledge level related to healthy diet. The Guide for Healthy Menu was a very important component of WESIHAT 2.0 in order to educate elderly people about the healthy food choices. Figure 4 displays sample UIs of WESIHAT 2.0 that demonstrate this module.
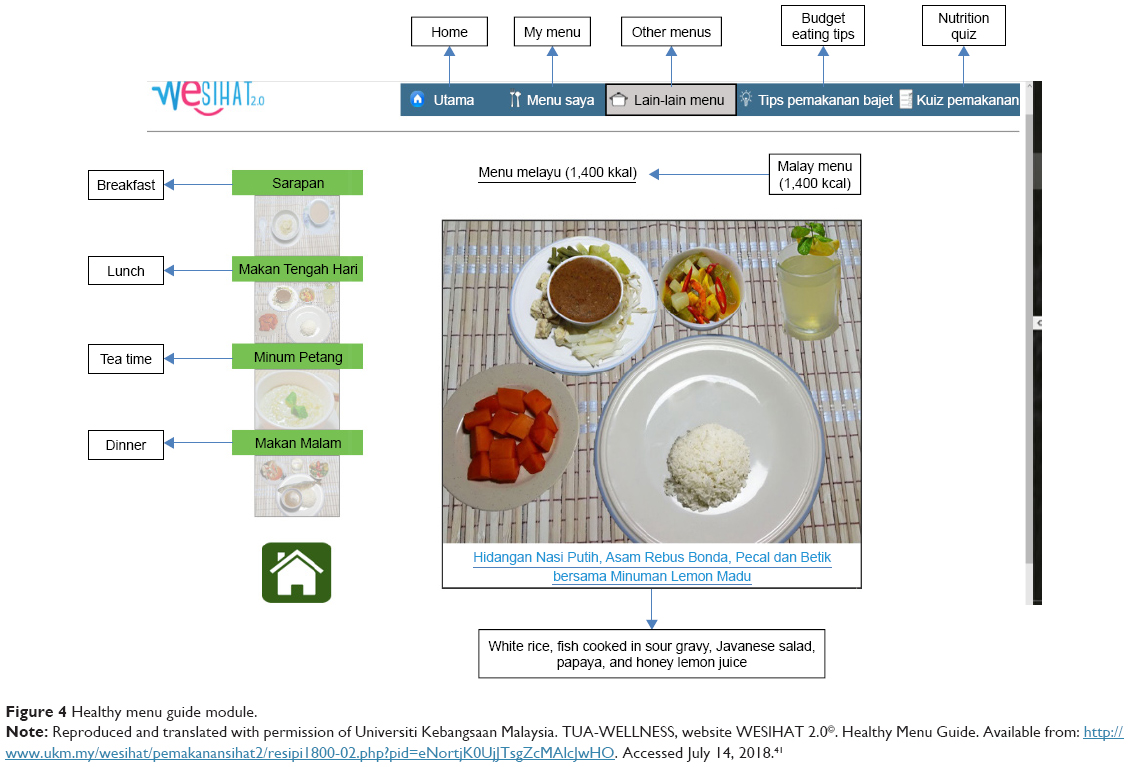 | Figure 4 Healthy menu guide module. |
An educational approach based on videos has been proven to be useful in promoting positive behavior regarding health especially when included in websites because of its accessibility to a broad range of viewers.23 Therefore, 12 videos were embedded in the web application, out of which five were on elderly-specific work out demonstration, six on healthy menu preparation, and one special video on encouraging life-long education through University of Third Age. Because of its importance, written information was also included in the pages containing videos for healthy food preparation. Furthermore, the font type used was Gotham and color of font was either white or black depending on the color of the background. Gotham had been selected as the preferred font because it belongs to the Sans Serif family, which is usually recommended as the most appropriate font for website for elderly people.24 The particulars of font type and size are given in Table 1. Figures 5 and 6 display examples of UI created for WESIHAT 2.0.
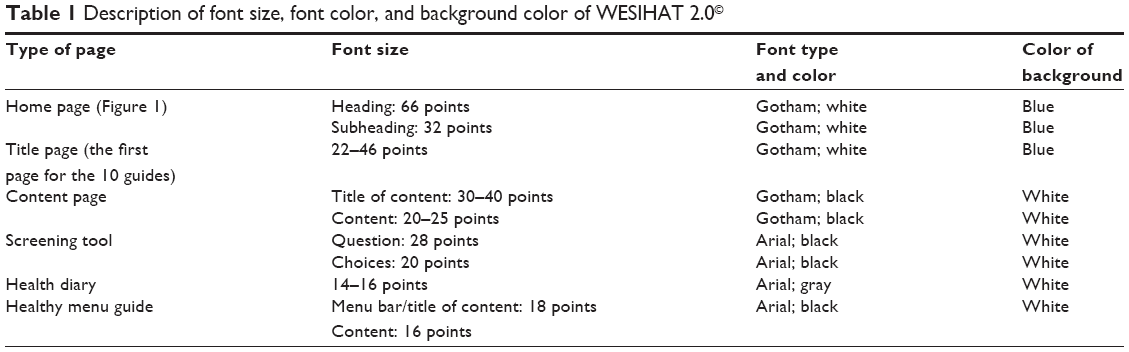 | Table 1 Description of font size, font color, and background color of WESIHAT 2.0© |
 | Figure 5 Front page of WESIHAT 2.0©. |
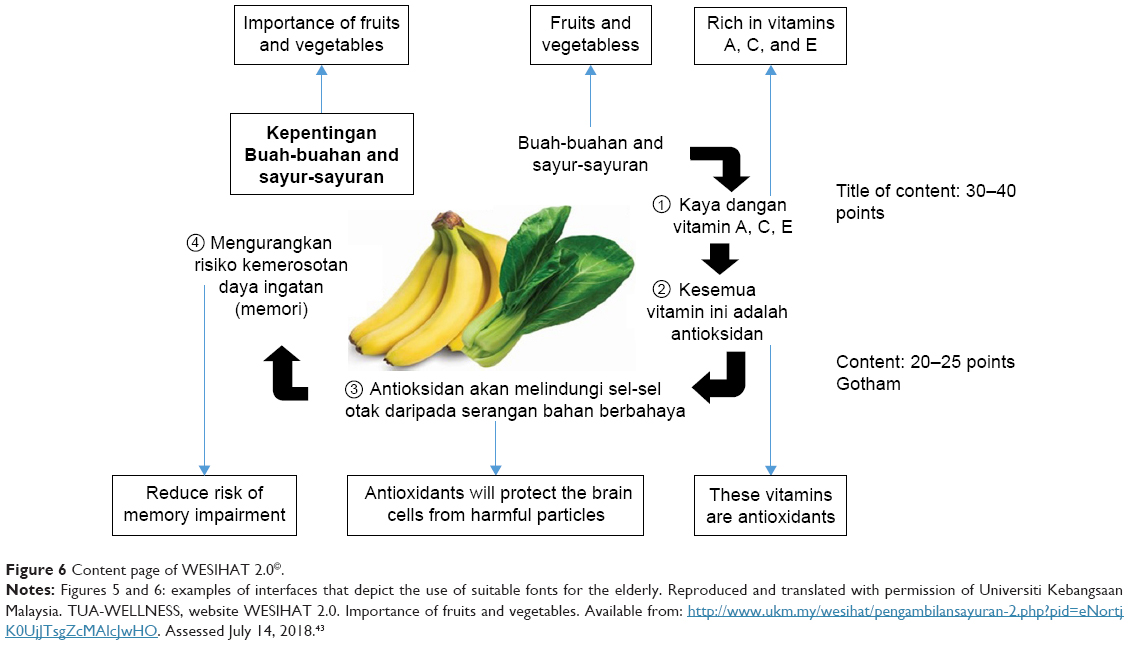 | Figure 6 Content page of WESIHAT 2.0©. |
Methodology for acceptance study
The third phase in the creation of WESIHAT 2.0 was the study of acceptance. The significance of the study of acceptance was to discover both the benefits and the drawbacks of the web application. This process was known as a participatory model, and it was used as a means of enhancing the new application for future users.25 The study of acceptance was carried out using sample design with stratified sampling technique in six states of Malaysia, namely Pahang, Penang, Kedah, Johor, Selangor, and Kelantan. The time period for this study was from September 22, 2016 to October 21, 2016, which was around a month. Ethical approval was obtained from the Malaysian Medical Research Ethics Committee in Universiti Kebangsaan Malaysia. All participants gave written informed consent before the commencement of the research.
The sample size calculation for this study is based on the Cochrane26 formula: n = (zα/2)2 p(1-p)/Δ2.
n = number of subjects included in the sample, Δ = estimate for accuracy or delta, zα/2 = 1.96 (two tailed at 95% CI), p = prevalence. Prevalence of all-type MCI among urban, multiethnic community-dwelling elderly in Malaysia was 21.1%.7 CI was set at 95%, and estimate of accuracy was 0.1 (10%); thus, a sample size of 71 was obtained.
On the whole, the 73 subjects who took part in the study of acceptance consisted of 30 elderly people, nine health care experts, 32 caregivers, and two information technology (IT) experts chiefly working in web design. For the older adult subjects, at first, the list of candidates was made available by the President of Member’s Association in the particular areas by means of random selection. After that, those who fulfilled the criteria were selected. Finally, each candidate on the list was called and those who consented to participate were chosen to join the research. A subsample of caregivers was recruited from the list.
In this study, the health care experts included were taken from multidisciplinary areas such as doctors, dieticians, physiotherapists, nurses, and web design experts. The health care experts were required to analyze the information concerned about nutrition, medical treatment, health, and physical activity. Additionally, the IT professionals examined the UI of the website to make sure that it was suitable for the elderly people.
The selection of the elderly people for the study was based on the following factors: they must have at least secondary level of education (7 years or more), no dementia or any form of cognitive impairment, should have the basic know-how of using computer, should have computer/i-pad/tablet at their place, and should have Internet connection for accessing the website. The selection criteria for caregivers included the following: should have at least secondary-level education, should have a computer with Internet accessibility at home, should have familiarity with a computer, and should have past or current experience of caring for elderly people. Caregivers include relatives, children, or grandchildren of the elderly people selected for the study. On one hand, the factors excluded for selection for the elderly people were having had memory loss or were not eager to use or learn how to use a computer. On the other hand, the selection criteria for health care professionals were that they should have had knowledge of managing geriatric cases and should have worked in the private or government hospitals or institutions such as wellness center. Alternatively, the IT professionals involved in this research were supposed to have knowledge and skill in the design and development of a web application.
The list of questions used for this research was inspired from Ali et al,27 which comprised the sociodemographic segment and items concerned with understanding website content, satisfaction with the content of the website as an educational module for promoting healthy cognitive function, font size, language, images, audio, color, and elements that needed enhancements. The sociodemographic segment involved personal details such as computer-related proficiency and health issues. Elderly people troubled with health issues were not in the group of successful aging, which is regarded as being free of the six diseases (heart ailments, diabetes, hypertension, stroke, lung problems, or chronic kidney diseases), no depression, no functional restrictions, normal global cognitive function, good life quality, and good self-perception regarding their health.28
The acceptance analysis was done separately and the participants browsed the initial website version for not less than 1 hour. The study was conducted in a computer room that was quiet. The participants were guided by the researcher, although, during the experiment, there was no interference of the researcher except any doubts raised by the participant. The researcher had provided the participants with a written manual for using WESIHAT 2.0 and it was done in order to ensure consistency in the process of browsing. The last step in the enhancement of WESIHAT 2.0 was the remodeling of the web application based on the responses given by the participants. Remodeling involved modification of the color, simplification of the sentences considered to be lengthy, and incorporation of more images.
Descriptive analysis was used to evaluate the acceptance level of the website by elderly people, caregivers, and health experts using SPSS version 22.0. Descriptive analysis had been stratified according to sex to identify differences between men and women. Also, the independent t-test was employed for investigating average differences between genders, with the presence of a single categorical and numerical variable. In addition, the association between two categorical variables was determined using cross-tabulation analysis. The significance level was set at p <0.05.
Results
The average ages of elderly people and caregivers were 65.07±3.83 and 29.9±10.1 years, respectively. Most of the elderly people (76.7%) and caregivers (93.8%) had obtained tertiary education. Overall, 76.7% of elderly people and 93.8% of caregivers had decent computer awareness. Approximately, 56.2% of the caregivers were currently getting an education. Elderly people (66.7%) reselected for this research were not in the group of successful aging as they suffered from chronic ailments such as diabetes mellitus, hypertension, hypercholesterolemia, arthritis, and heart problems (Tables 2 and 3). The criteria of successful aging have been described in the “Methodology” section.
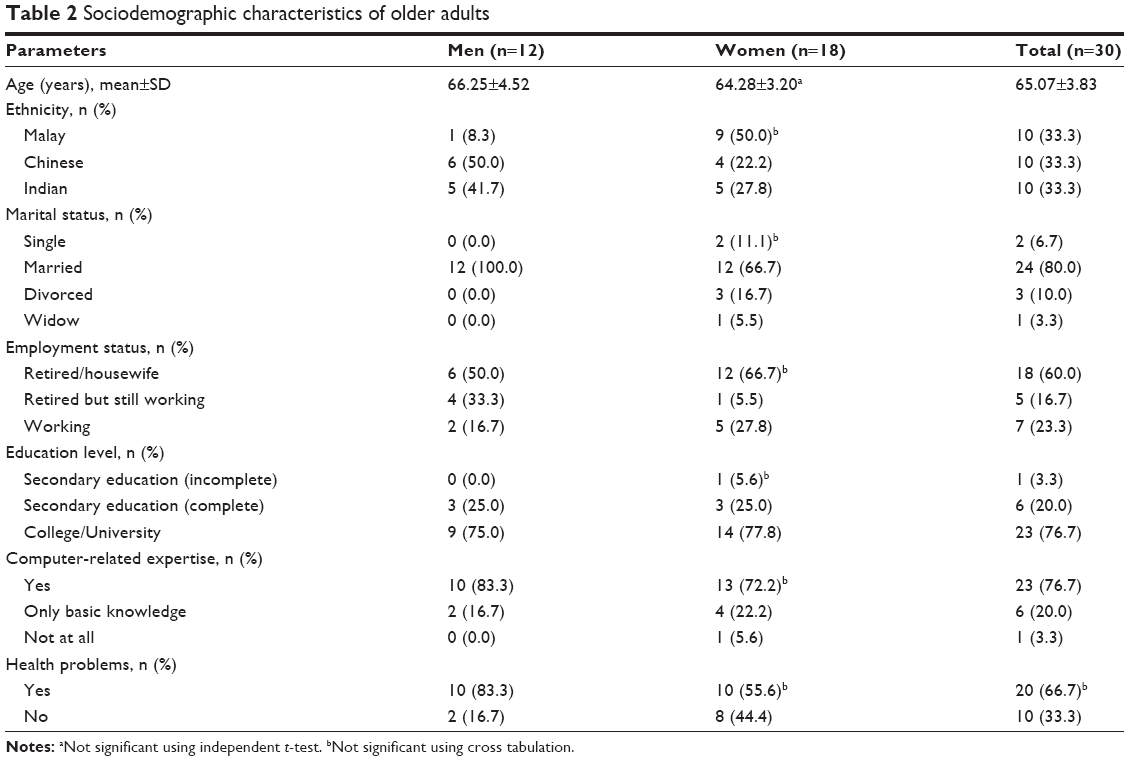 | Table 2 Sociodemographic characteristics of older adults |
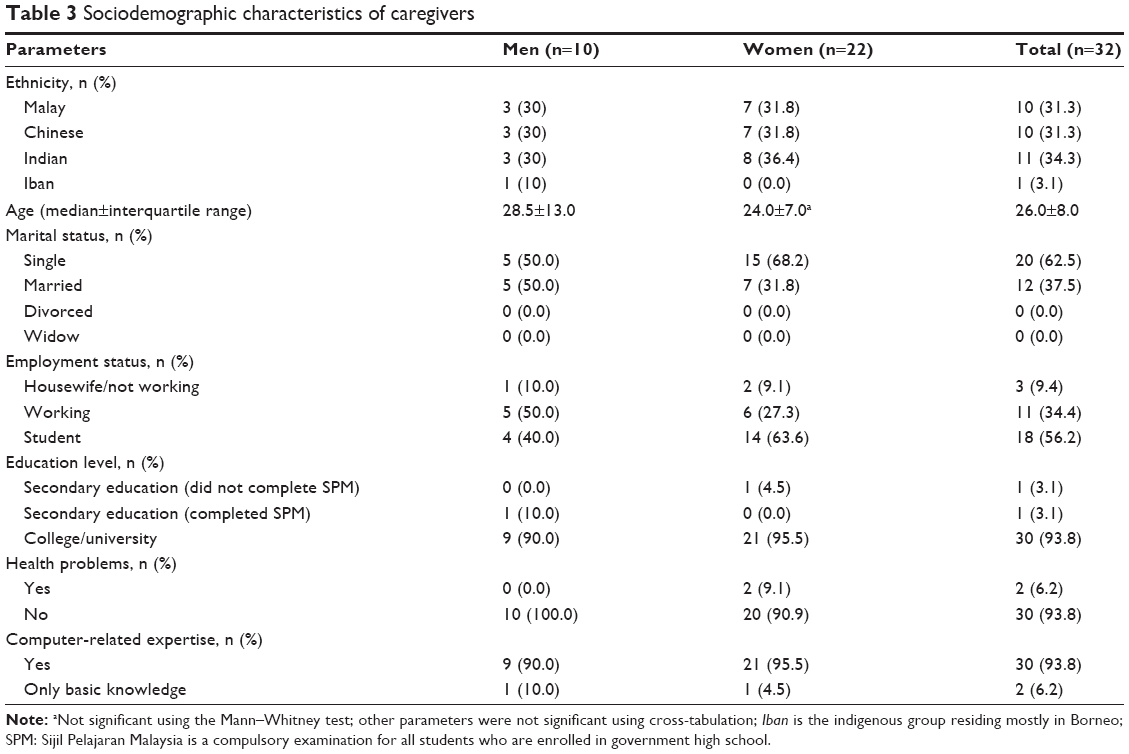 | Table 3 Sociodemographic characteristics of caregivers |
All the professionals chosen for this study had knowledge of managing geriatric cases and they had good experience with computer use. The average age of IT and health care expert was 32.8±10.4 years. The expert group included equal percentages (18.2%) of doctors, nurses, physiotherapists, and web application developers but more dieticians were selected (27.2%) on account of the extensive nutritional content in the website (Table 4).
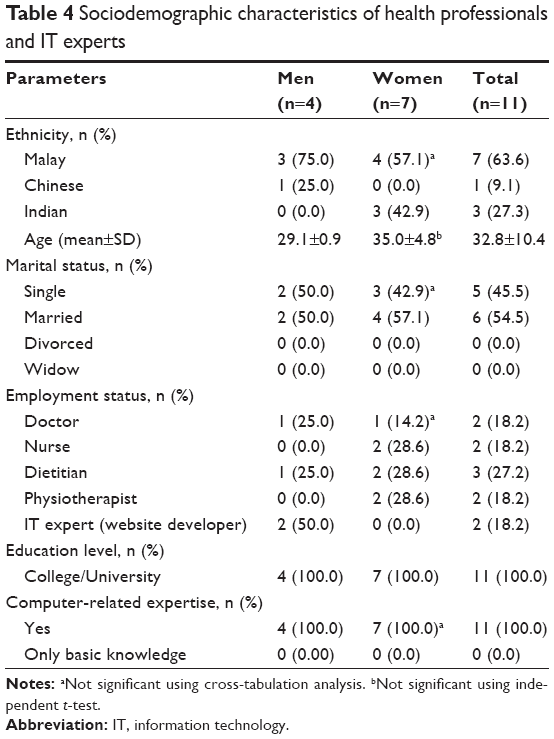 | Table 4 Sociodemographic characteristics of health professionals and IT experts |
The outcomes revealed that all the elderly people and caregivers included in this research were satisfied with the whole presentation of WESIHAT 2.0. Nevertheless, caregivers stated that they have a lower approval of the detailed elements of WESIHAT 2.0 in comparison to the elderly people. Just ~59.4% of caregivers approved the images or illustration incorporated in the website in comparison to 86.7% of the elderly people. Overall, 75% of the caregivers approved the length of sentences and the complexity of terminologies included in the web application. Around 10.0% elderly people and 15.6% caregivers expressed their disapproval of the font size in the website (Table 5).
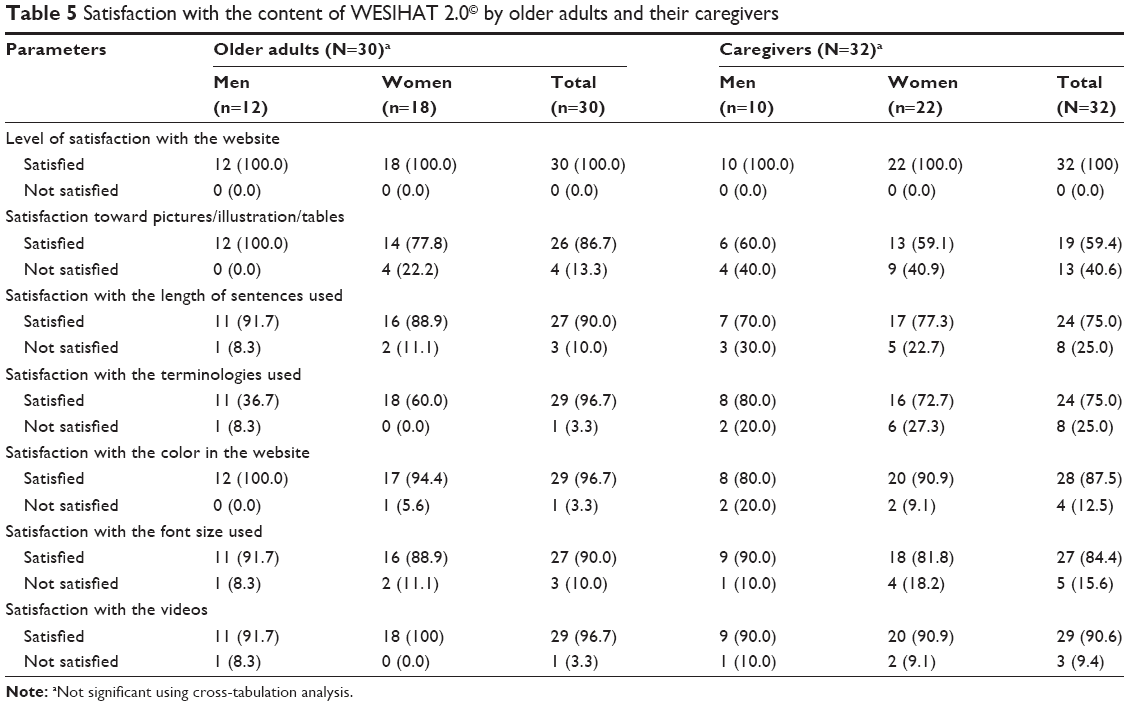 | Table 5 Satisfaction with the content of WESIHAT 2.0© by older adults and their caregivers |
Table 6 displays the satisfaction of the experts regarding WESIHAT 2.0. In total, 54.5% of the experts were not content with the images or illustration incorporated in the website. Furthermore, 45.5% of them reported that the videos embedded in the website were not easy to view as they could not be viewed on the full screen although 63.6% of the experts reported that they were satisfied with the terminologies, the language, and the dietary recommendations given in the web application.
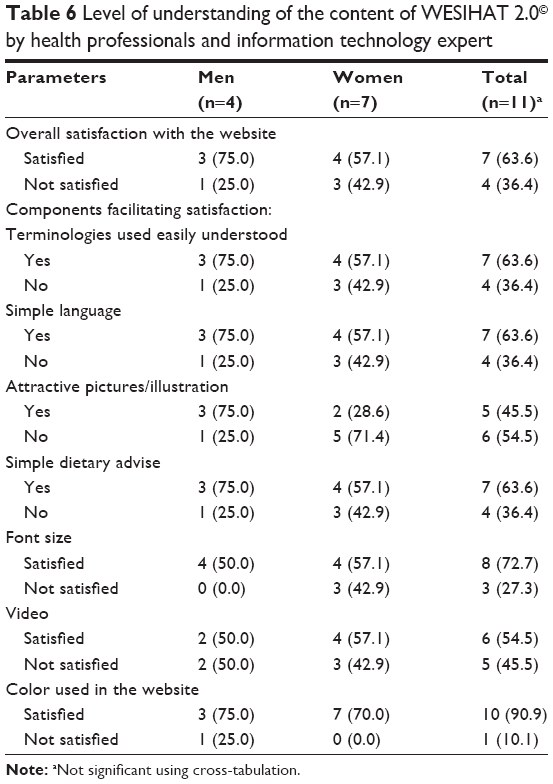 | Table 6 Level of understanding of the content of WESIHAT 2.0© by health professionals and information technology expert |
The WESIHAT 2.0 was modified based on the comments given in Table 7. The edited version of WESIHAT 2.0 was then used for exploring the usefulness of WESIHAT 2.0 in several areas including physical function, cognition, biochemical factors, oxidative stress indicators, food intake, and psychosocial parameters.
 | Table 7 Comments provided by subjects to improve WESIHAT 2.0© |
Directions for the updated version of WESIHAT 2.0
The results have shown that although subjects agreed that the content presented in WESIHAT 2.0 is helpful, it can still be improved by modifying various elements before the website is made online. The previous version presented at the time of the study of acceptance still contained scientific jargons, improper font size, more textual content than images, and poor color choice. Thus, we have modified WESIHAT 2.0 taking into account the feedback to create a new version more suitable for the elderly people. It agreed with Alpay et al29 who had developed a senior-friendly web application incorporating similar components to WESIHAT 2.0.
Discussion
The aim of WESIHAT 2.0 is to offer health-based recommendations and to inculcate positive approaches for everyday life for slowing the development of memory decline among elderly people. WESIHAT 2.0 is a friendly application for elderly people with a brief inspection tool for analyzing the risk of the cognitive disorder. In this research, the website has been considered as a platform to communicate information because already there is a locally available research conducted on enhancing the cognitive function of urban elderly people using a booklet.30 Even though booklets are portable, they have their disadvantage particularly for the elderly people who may lose it. A website is not prone to get lost as it is accessible through the Internet. In an investigation done by Department of Statistics (Malaysia), it shows that the number of people among Malaysians who use a computer have increased from 56.0% in 2013 to 68.7% in 2015. The rise in the socioeconomic level of the Malaysians boosted the household use of computers by 8.2% between 2013 and 2015.31 Besides that, older people who had computer skills from their prior job were more likely to participate in computer classes to improve their knowledge in information and communication technology.32 Moreover, education level was the determinant of computer use among older people in Malaysia and better-educated elderly were more engaged in cognitively stimulating activities such as reading or using a computer.33 Besides that, the prevalence of computer use in rural regions had shown rise because of the rural computer-buying scheme promoted by the government, which facilitates people to buy a computer using simple payment method. In addition, computer classes were organized in rural regions for making the villagers skillful in using the computer in order to make development of their villages.34
Moreover, 10.0% of older people remarked that the size of font was small. At first, we used 20 points, which was according to the senior-friendly web application development guidelines. Nevertheless, after the feedback, we increased the size of the font to 22 points. Bigger font size is desirable as aging causes limited sensitivity of visual contrast. Font type Microsoft Sans Serif was selected as it was the preferable type for the text displayed on the computer screen.35 Text readability is crucial as it motivates the elderly people to keep reading the text with more interest. With the undersized font, elderly people may quit reading the text and lose interest. Scrolling is closely linked with font size. Proper font size should be selected to reduce both horizontal and vertical scrolling, which may prove to be difficult for the elderly people.
WESIHAT 2.0 is also useful as a touch screen web application. Touch screen style has been employed considering decreased motor ability with age advancement. Elderly people might have problem selecting elements on an interface with a mouse, which may impact their use of the computer. Findlater et al36 evaluated the performance of elderly and younger people using four tasks with both touch screen and mouse approaches and discovered that touch screen has helped elderly people and reduction in error. Touch screen is less complicated and does not involve much training, has a lesser demand for space and limited hand coordination, which is better for the elderly people.37
The benefit of this research is that it effectively developed an application with an objective of screening early phase of cognitive disorder and further offered proven preventive approaches to solve the problem of cognitive decline. Furthermore, the acceptance study was carried out among elderly people in the six states of the Malaysian peninsula and thus was confirmed to be appropriate for elderly people who were able to read Malay. Although this outcome has to be confirmed by conducting a large-scale research involving more number of elderly people, this website can be employed in community centers, hospitals, or memory clinics for inspection and education of elderly people and the caregivers allotted to them. It is also helpful for stakeholders for development of policies especially to handle early stage of the cognitive disorder. Additionally, WESIHAT 2.0 can be employed by researchers for performing longitudinal studies investigating the effects of lifestyle-based methodology for healthy cognition. Therefore, WESIHAT 2.0 can be utilized in the entire Malaysia for educating elderly people about the dangers of cognitive impairment.
Conclusion
WESIHAT 2.0 was well recognized by elderly people and caregivers as a tool for inspection and education for the primitive stage of memory loss and usability. Nonetheless, the participants have recommended minor modifications with regard to font size, smaller sentences, restricted use of unfamiliar terminologies, and adding more images before the final product is appropriate to be fully used by the elderly people. Based on these feedback, WESIHAT 2.0 was modified before being utilized for future study. Wrapping up, WESIHAT 2.0 was a suitable measure to recognize early signs of cognitive impairment through the TUA-WELLNESS screening tool among elderly Malaysian people and the information offered may increase dietary and health knowledge among elderly people, but it will never substitute the consultation from professionals.
Acknowledgments
We would like to thank the Ministry of Higher Education for providing monetary assistance under the grants LRGS TUA (LRGS/BU/2012/UKM-UKM/K/01) and FRGS/1/2014/ICT02/UKM/01/1. We highly appreciate the participation of subjects, health care professionals, caregivers, and experts in information technology. We are also grateful to the local authorities who aided us in subject recruitment.
Disclosure
The authors report no conflicts of interest in this work.
References
Harper S. Economic and social implications of aging societies. Science. 2014;346(6209):587–591. | ||
Kim ES, Strecher VJ. Purpose in life and use of preventive health care services. Proc Natl Acad Sci USA. 2014;111(46):16331–16336. | ||
Arevalo-Rodriguez I, Smailagic N, Figuls MR, et al. Mini-Mental State Examination (MMSE) for the detection of Alzheimer’s disease and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst Rev. 2015;(3):CD010783. | ||
Joling KJ, van Hout HP, Schellevis FG, et al. Incidence of depression and anxiety in the spouses of patients with dementia: a naturalistic cohort study of recorded morbidity with a 6-year follow-up. Am J Geriatr Psychiatry. 2010;18(2):146–153. | ||
Li JQ, Tan L, Wang HF, et al. Risk factors for predicting progression from mild cognitive impairment to Alzheimer’s disease: a systematic review and meta-analysis of cohort studies. J Neurol Neurosurg Psychiatry. 2016;87(5):476–484. | ||
Petersen RC, Caracciolo B, Brayne C, Gauthier S, Jelic V, Fratiglioni L. Mild cognitive impairment: a concept in evolution. J Intern Med. 2014;275(3):214–228. | ||
Lee LK, Shahar S, Chin AV, Mohd Yusoff NA, Rajab N, Aziz SA. Prevalence of gender disparity and predictors affecting the occurrence of mild cognitive impairment (MCI). Arch Gerontol Geriatr. 2012;54(1):185–191. | ||
Krell-Roesch J, Vemuri P, Pink A, et al. Association between mentally stimulating activities in late life and the outcome of incident mild cognitive impairment, with an analysis of the APOE ε4 genotype. JAMA Neurology. 2017;74(3):332–338. | ||
Meier CA, Fitzgerald MC, Smith JM. e-Health: extending, enhancing, and evolving health care. Annu Rev Biomed Eng. 2013;15:359–382. | ||
Samoocha D, Bruinvels DJ, Elbers NA, Anema JR, van der Beek AJ. Effectiveness of web based interventions on patient empowerment: a systematic review and meta-analysis. J Med Internet Res. 2010;12(2):e23. | ||
Demographics of Internet Users [webpage on the Internet]. Washington, DC: Pew Internet & American Life Project (US). 2017 August [cited 2017-01-12]. Available from: http://www.pewinternet.org/fact-sheet/internet-broadband/. Accessed February 05 2018. | ||
Bond GE, Burr RL, Wolf FM, Feldt K. The effects of a web-based intervention on psychosocial well-being among adults aged 60 and older with diabetes: a randomized trial. Diabetes Educ. 2010;36(3):446–456. | ||
Glasgow RE, Boles SM, McKay HG, Feil EG, Barrera M. The D-Net diabetes self-management program: Long-term implementation, outcomes, and generalization results. Prev Med. 2003;36(4):410–419. | ||
McMahon GT, Gomes HE, Hickson-Hohne S, Hu TM, Levine BA, Conlin PR. Web-based care management in patients with poorly controlled diabetes. Diabetes Care. 2005;28(7):1624–1629. | ||
Cho JH, Lee HC, Lim DJ, Kwon HS, Yoon KH. Mobile communication using a mobile phone with a glucometer for glucose control in Type 2 patients with diabetes: as effective as an Internet-based glucose monitoring system. J Telemed Telecare. 2009;15:77–82. | ||
Keyserling TC, Sheridan SL, Draeger LB, et al. A comparison of live counselling with a web-based lifestyle and medication intervention to reduce coronary heart disease risk: a randomized clinical trial. JAMA Intern Med. 2014;174(7):1144–1157. | ||
Thiboutot J, Sciamanna CN, Falkner B, et al. Effects of web based patient activation intervention overcome clinical inertia on blood pressure control: cluster randomized controlled trial. J Med Internet Res. 2013;15(9):e158. | ||
Anstey KJ, Bahar-Fuchs A, Herath P, Rebok GW, Cherbuin N. A 12-week multidomain intervention versus active control to reduce risk of Alzheimer’s disease: study protocol for a randomized controlled trial. Trials. 2013;14:60. | ||
Vanoh D, Shahar S, Din NC, et al. Predictors of poor cognitive status among older Malaysian adults: baseline findings from the LRGS TUA cohort study. Aging Clin Exp Res. 2016;29(2):173–182. | ||
Kurniawan SH, Zaphiris P. Proceedings of the ACM SIGACCESS Conference on Computers and Accessibility. ASSESTS 2005; October 9–12, 2005; Baltimore, MD, USA. | ||
Mouton A, Cloes M. Web-based interventions to promote physical activity by older adults: promising perspectives for a public health challenge. Arch Public Health. 2013;71(1):16. | ||
Vanoh D, Shahar S, Rosdinom R, Din NC, Yahya HM, Omar A. Development of TUA-WELLNESS screening tool for screening risk of mild cognitive impairment among community dwelling older adults. Clin Interv Aging. 2016;11:579–587. | ||
Tuong W, Larsen ER, Armstrong AW. Videos to influence: a systematic review of effectiveness of video-based education in modifying health behaviors. J Behav Med. 2012;37(2):218–233. | ||
National Institute on Aging/National Library of Medicine (NIA/NLM): Making your website senior friendly: a check list [Internet]. Available from http://www.nlm.nih.gov/pubs/checklist.pdf. Accessed October 09, 2002. | ||
Archambault D, Penaz P, Zagler W. Computers Helping People with Special Needs. ICCHP 2014. Lecture Notes In Computer Science. Vol. 8547. Cham: Springer; 2014:332–339. | ||
Cochran WG. Sampling Techniques. 2nd ed. New York, NY, USA: John Wiley and Sons, Inc; 1963. | ||
Ali NM, Shahar S, Kee YL, Norizan AR, Mohd Noah SA. Design of an interactive digital nutritional education package for elderly people. Inform Health Soc Care. 2012;37(4):217–229. | ||
Hamid TA, Yadollah AM, Rahimah I. Predictors and prevalence of successful aging among older Malaysians. Gerontology. 2012;58(4):366–370. | ||
Alpay LL, Toussaint PJ, Ezendam NPM, Rovekamp AJM, Graafmans WC, Westendorp RGJ. Easing Internet access of health information for elderly users. Health Inform J. 2004;10(3):185–194. | ||
Johari SM, Shahar S, Rajikan R, Aziz SA. Development and acceptance of a nutrition and lifestyle education booklet to improve mild cognitive impairment among elderly. JSKM. 2011;9(2):45–50. | ||
DOSM. ICT Use and access by individuals and households survey report, Malaysia 2015. Department of Statistics, Putrajaya, Malaysia. 2016. | ||
Hisham S. Localising the user interface for elderly people in Malaysia’, HCI, the web and the older population, a full-day workshop at British HCI 2006 Queen Mary, University of London, London, UK 12 September 2006. | ||
Minhat HS, Amin RM. Sociodemographic determinants of leisure participation among elderly in Malaysia. J Community Health. 2012;37(4):840–847. | ||
Kamaruddin K. Adult computer literacy programme in rural areas in Peninsular Malaysia. Malay. 2008;137(166):246. | ||
Darroch I, Goodman J, Brewster S, Gray P. The effect of age and font size on reading text on handheld computers. In: Costabile MF, Paternò F, editors. Human-Computer Interaction – INTERACT 2005. Lecture Notes in Computer Science. Springer, Berlin, Heidelberg: Springer; Vol. 3585. | ||
Findlater L, Froehlich JE, Fattal K, Wobbrock JO, Dastyar T. Age-Related Differences in Performance With Touchscreens Compared to Traditional Mouse Input. Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Paris, France, Apr 27 – May 2. CHI; 2013;2013:343–346. | ||
Wood E, Willoughby T, Rushing A, Bechtel L, Gilbert J. Use of computer input devices by older adults. J Appl Gerontol. 2005;24(5):419–438. | ||
Universiti Kebangsaan Malaysia. TUA-WELLNESS, website WESIHAT 2.0. Available from: http://www.ukm.my/wesihat/q1.php. Accessed July 14, 2018. | ||
Universiti Kebangsaan Malaysia. TUA-WELLNESS, website WESIHAT 2.0. Ten memory enhancing guides, website WESIHAT 2.0. Available from: http://www.ukm.my/wesihat/mainmenu-dayaingatan.php?pid=eNortjK0UjJTsgZcMAlcJwHO. Accessed July 14, 2018. | ||
Universiti Kebangsaan Malaysia. TUA-WELLNESS, website WESIHAT 2.0. Health Diary. Available from:http://www.ukm.my/wesihat/diarikesihatanform.php?. Accessed July 14, 2018. | ||
Universiti Kebangsaan Malaysia. TUA-WELLNESS, website WESIHAT 2.0. Healthy Menu Guide. Available from:http://www.ukm.my/wesihat/pemakanansihat2/resipi1800-02.php?pid=eNortjK0UjJTsgZcMAlcJwHO. Accessed July 14, 2018. | ||
Universiti Kebangsaan Malaysia. TUA-WELLNESS, website WESIHAT 2.0. Homepage WESIHAT 2.0. Available at URL http://www.ukm.my/wesihat/index.html. Accessed July 14, 2018. | ||
Universiti Kebangsaan Malaysia. TUA-WELLNESS, website WESIHAT 2.0. Importance of fruits and vegetables. Available from: http://www.ukm.my/wesihat/pengambilansayuran-2.php?pid=eNortjK0UjJTsgZcMAlcJwHO. Assessed July 14, 2018. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.