")
Back to Journals » Advances in Medical Education and Practice » Volume 11
Developing Medical Students’ Broad Clinical Diagnostic Reasoning Through GP-Facilitated Teaching in Hospital Placements
Authors Bansal A , Singh D, Thompson J, Kumra A , Jackson B
Received 24 December 2019
Accepted for publication 29 February 2020
Published 25 May 2020 Volume 2020:11 Pages 379—388
DOI https://doi.org/10.2147/AMEP.S243538
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Aarti Bansal, Davinder Singh, Joanne Thompson, Alexander Kumra, Benjamin Jackson
Academic Unit of Primary Care, The University of Sheffield, Sheffield, UK
Correspondence: Aarti Bansal
Academic Unit of Primary Care, The University of Sheffield, Herries Road, Sheffield S5 7AU, UK
Tel +44 114 222 2201
Email [email protected]
Purpose: Graduating medical students need broad clinical diagnostic reasoning skills that integrate learning across clinical specialties to deal with undifferentiated patient problems. The opportunity to acquire these skills may be limited during clinical placements on increasingly specialized hospital wards. We developed an intervention of regular general practitioner (GP) facilitated teaching in hospital placements to enable students to develop broad clinical diagnostic reasoning. The intervention was piloted, refined and delivered to a whole cohort of medical students at the start of their third year. This paper examines whether students perceived opportunities to improve their broad diagnostic clinical reasoning through our intervention.
Methods: GP-facilitated teaching sessions were delivered weekly in hospital placements to small groups of 6– 8 students for 90 mins over 6 weeks. Students practiced clinical reasoning with real patient cases that they encountered on their placements. Evaluation of learning outcomes was conducted through a student questionnaire using Likert scales with free-text boxes for additional explanation. Focus groups were conducted to gain a more in-depth understanding of student perspectives.
Results: As high as 87% of students agreed that their broad clinical diagnostic reasoning ability had improved. Thematic analysis of the qualitative data revealed four factors supporting this improvement: practicing the hypothetico-deductive method, using real patient cases, composing student groups from different speciality placements and the breadth of the facilitators’ knowledge. Students additionally reported enhanced person-centredness in terms of understanding the patient’s perspective and journey. Students perceived that the added value of general practitioner facilitators lay in their broad knowledge base and knowledge of patient needs in the community.
Conclusion: Our results suggest that medical students can develop broad clinical diagnostic reasoning skills in hospital settings through regular GP-facilitated teaching. Our approach has the advantage of working within the established curricular format of hospital placements and being deliverable at scale to whole student cohorts.
Keywords: education, medical, clinical reasoning, patient-centred care, longitudinal clerkships, curriculum, family practice
A Letter to the Editor has been published for this article.
A Response to Letter has been published for this article.
Introduction
The ability to diagnose a patient’s presenting problem safely and accurately is an essential skill for all doctors. Medical graduates need to be able to formulate diagnoses that start from the undifferentiated problems facing the patient, incorporate the patient perspective and integrate learning across medical specialties.1 Acquiring broad clinical diagnostic reasoning skills is therefore a fundamental objective of medical education.2
Variable and poor clinical diagnostic reasoning skills amongst senior medical students suggest that diagnostic reasoning is not passively acquired through observation.3 Teaching clinical reasoning skills has been shown to improve diagnostic accuracy and reduce diagnostic errors,4,5 and it is increasingly accepted that clinical reasoning should be explicitly taught in undergraduate medical curricula.6 The literature suggests that using a combination of both analytic (deliberate, cognitive) and non-analytic (intuitive, pattern recognition) strategies is likely to be most effective when teaching clinical reasoning.4,7 Key to these strategies is the importance of deliberate practice with feedback from a skilled clinical facilitator.8,9
It remains the case that the majority of clinical placement time in most medical school curricula is based in hospitals.10 As hospital wards become increasingly specialized, students are less likely to come across patients with undifferentiated problems. Although students have some opportunities to take histories from patients in accident and emergency settings or on acute medical wards, this opportunity is limited. Many hospitals no longer have general medical or surgical wards so that by the time students see patients on the wards, the initial diagnostic reasoning has already taken place. This presents a challenge as to how to support medical students to develop broad clinical diagnostic reasoning skills. One solution is to shift clinical placements into generalist settings such as the community. Another potential solution is to support students to develop their broad clinical reasoning skills during hospital placements. The clinical practice of general practitioners (GPs), which involves seeing many patients a day with undifferentiated illness, is synergistic to the acquisition of broad clinical diagnostic reasoning skills. It has been argued that primary care educators are ideally placed to deliver core competencies relevant to all clinicians.2,11
Our Context
Students at Sheffield Medical School have 2 years of pre-clinical learning on basic sciences delivered through lectures and small group learning. They also have early clinical experiences in the community. These involve 24 half-day small group problem-based learning sessions in general practice where students learn about chronic conditions (e.g., diabetes, inflammatory bowel disease) and then talk to patients with that particular condition to understand the impact on their life. They also have communication skills training prior to their first clinical placements. This involves a lecture introducing them to the Calgary-Cambridge model of consultation and two GP-facilitated 90 min small group simulation sessions, with an actor playing the patient, where students role-play the doctor and receive feedback. In their remaining three clinical years, they spend 15 weeks in general practice and the rest of their clinical placement time in hospitals.
In 2018, Sheffield Medical School replaced short hospital placements of 1 to 3 weeks duration in the 3rd and 5th year of the course with longer placements of approximately 12 weeks. The aim was to enable students to benefit from the improved learning outcomes associated with continuity and active participation seen in longitudinal integrated clerkships.12 In these longer hospital placements, students spend 50% of their times on a base ward, 40% doing integrated learning activities across the hospital (such as attending different speciality clinics, attending theatre, etc.) and 10% on planned educational activities. These longer placements are called longitudinal integrated clinical placements by our institution. This curricular change presented the opportunity to develop weekly planned educational activities to support students’ clinical diagnostic reasoning skills.
The literature gives examples of specific clinical reasoning teaching sessions that have been implemented on placements in certain specialties such as general practice13 and psychiatry.14 Our intervention was novel in its use of GP educators in hospital placements. We considered that GPs, whose daily clinical practice involves person-centred, broad clinical diagnostic reasoning (which integrates learning across clinical specialties), would be able to support students to develop these skills whilst on any type of hospital placement. We further considered that using educators from outside of the hospital placement would protect the teaching from being cancelled due to more pressing patient needs.15 We chose the pedagogical approach of regular small group sessions to provide continuity of peer group, facilitator and feedback. We wished to understand if students perceived improvement in their broad clinical diagnostic reasoning skills from this intervention and if this approach was beneficial when implemented at scale.
Methods
Design and Development of Teaching Intervention
Pilot Intervention
In 2017, hospitals piloted planned educational activities in preparation for the impending changes. Most hospitals delivered topic-based seminars and lectures. In collaboration with one hospital, we piloted a different arrangement of weekly small group GP-facilitated teaching sessions with continuity of group and GP facilitator over 6 weeks to 28 students (four groups of seven students). Three of the authors who are GPs created written scenarios which started from a hypothetical patient’s presentation in the community and followed them through their hospital admission and discharge. The scenarios were not presented to students in advance and information in the scenarios was split up with prompt questions for facilitators to encourage students to think. The sessions lasted 2 hrs and included time for students to reflect on their placement experiences. The focus group evaluation of this pilot found that firstly students felt that real patient cases were more suitable than the pre-written cases in supporting their clinical diagnostic reasoning; secondly, they felt that having general practitioners as facilitators helped them think across specialties and thirdly, that continuity of peer group and facilitator helped with feedback and reflective practice. Students also requested that the final session be scheduled a week earlier to give them two full weeks to focus on their end of placement OSCE.
Funding
In response to our pilot’s positive evaluation, hospitals agreed to replace topic-based seminars with GP-facilitated small group sessions for the second 6 weeks of the placement from their teaching tariff funds. Shorter sessions of 90 mins (instead of 2 hrs) enabled the cost to be kept to a reasonable level whilst maintaining small groups of 6–8 students.
Changes to Intervention
Pre-written cases were removed and instead students were asked to bring cases from patients they had spoken to during their clinical placements. Each session was given a broad theme such as “pain,” “fever,” “breathing difficulties” and “falls” to enable all students to be able to speak to a patient with a common presentation regardless of their ward base. Small groups were purposefully composed of students from different specialty wards to support students to integrate thinking across clinical specialties for any given patient presenting problem. The timing of the intervention was changed as per students’ request so that the focus on OSCE assessment did not interfere with their engagement with these sessions.
Training of GP Facilitators
GP facilitators were recruited from our experienced pool of small group tutors who deliver small group teaching to students during their community placements in year 4 and year 5. All facilitators attended a half-day training program in which educational strategies to support clinical diagnostic reasoning derived from the literature were demonstrated. These included both analytical strategies and non-analytic strategies.16–18 The analytic strategy focused on the hypothetico-deductive approach where students learn to develop hypothesis from clinical information (differential diagnosis) and then search for additional information through questioning to help them confirm, refine and refute these diagnoses. The non-analytic strategies involved encouraging students to recognize patterns of presentation, question assumptions and recognize any underlying biases in their thinking (Appendix 1). Facilitators were asked to devote roughly 1 hr to supporting clinical diagnostic reasoning through the real patient cases brought by the students and half an hour to facilitate reflection on placement experiences more generally. It was expected that all students would present a patient over the 6 weeks and that during each session one or two students would present a patient. Students were instructed to take a person-centred history as they had been trained during their consultation skills training sessions.
Design of Evaluation
Questionnaire
All 213 students who undertook the clinical placement received a request to complete an online end-of placement survey one week after the end of their clinical placement. We included six specific questions related to the GP-facilitated teaching sessions in this evaluation survey. The first four questions were derived directly from the pilot study evaluation findings and two other questions were included to check that learning was appropriate to stage and to understand if students found any added value in GPs facilitating the sessions. The students were asked how well they agreed with the statements on an ordinal Likert scale moving from “strongly disagree” to “strongly agree.” A different scale from “poor” to “excellent” was used for a final question about overall rating. To understand the reasons for their ratings students were also asked to explain their ratings in a free-text box below each question.
Our University ethics department confirmed that ethics approval was not required for the collection or publication of robustly anonymized routinely collected data.
Focus Groups
We conducted focus groups using the same questions as the questionnaire in four of the six hospital sites to ensure that we had sufficient depth of data to help explain the students’ ratings for the different learning objectives. Thirty-one students (11 males, 20 females), attended four 1-hr long focus groups, facilitated by faculty staff not involved in delivering the teaching, to enable the students to speak freely about their thoughts. Field notes were taken, and all four groups were audiotaped and later transcribed. Ethics approval to conduct these focus groups was obtained from the University of Sheffield Medical School Ethics department (reference 015963).
Analysis of Qualitative Data
Thematic analysis was first undertaken on the qualitative data from the students’ free-text comments in the questionnaire. All authors familiarised themselves with the data and the lead author (AB), conducted the initial coding. In two subsequent meetings, all authors met to agree the coding framework and the key themes present. Subsequently, the focus group data were analysed by the lead author to look for different, additional or contrasting themes as a form of data triangulation to enhance the rigour of our findings. All authors then met to consider whether the themes from the focus groups sufficiently mirrored the questionnaire free-text data for all the data to be reported as one dataset. It was agreed this was the case.
Results
Quantitative Data
A total of 210 out of 213 students responded to the questionnaire giving an overall response rate of 98.6%. The quantitative data from the questionnaire are illustrated in tabular and graphical form in Table 1 and Figure 1. Overall students agreed that learning objectives were achieved and rated the sessions highly. As high as 87% of students agreed that the sessions had improved their broad diagnostic clinical reasoning skills. Seventy six percent of students agreed that their understanding of how diagnosis and management is influenced by the individual patient had improved but only 54% agreed that the sessions had enabled them to better understand patient needs in the community. Seventy five percent of students agreed that they had been enabled to reflect on placement experiences, 83% agreed that the sessions were learner-centred and 90% agreed that it was useful to have a General Practitioner as facilitator. As high as 91% of students rated the sessions as good or excellent overall.
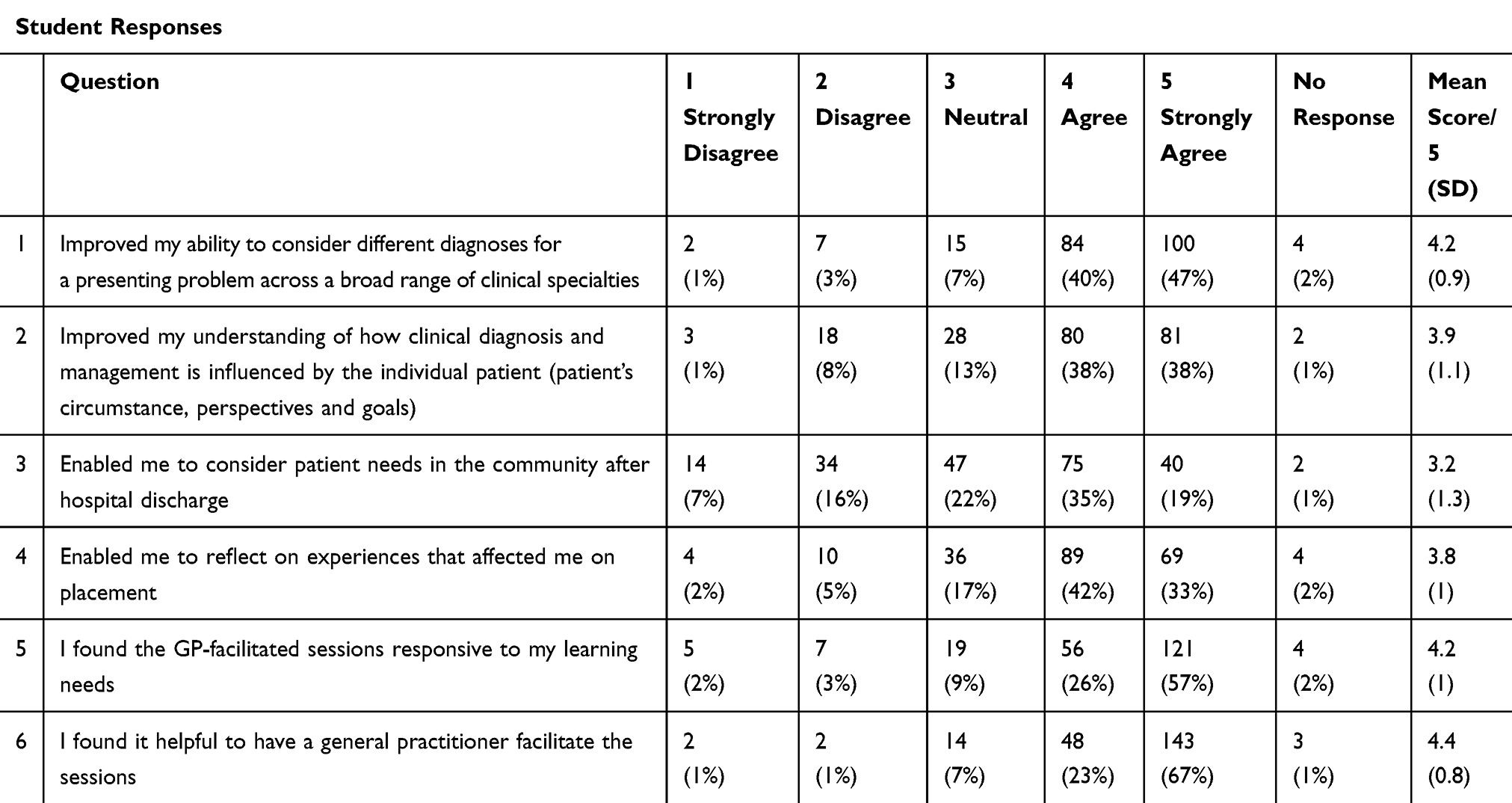 |
Table 1 Student Responses to Questionnaire Evaluation |
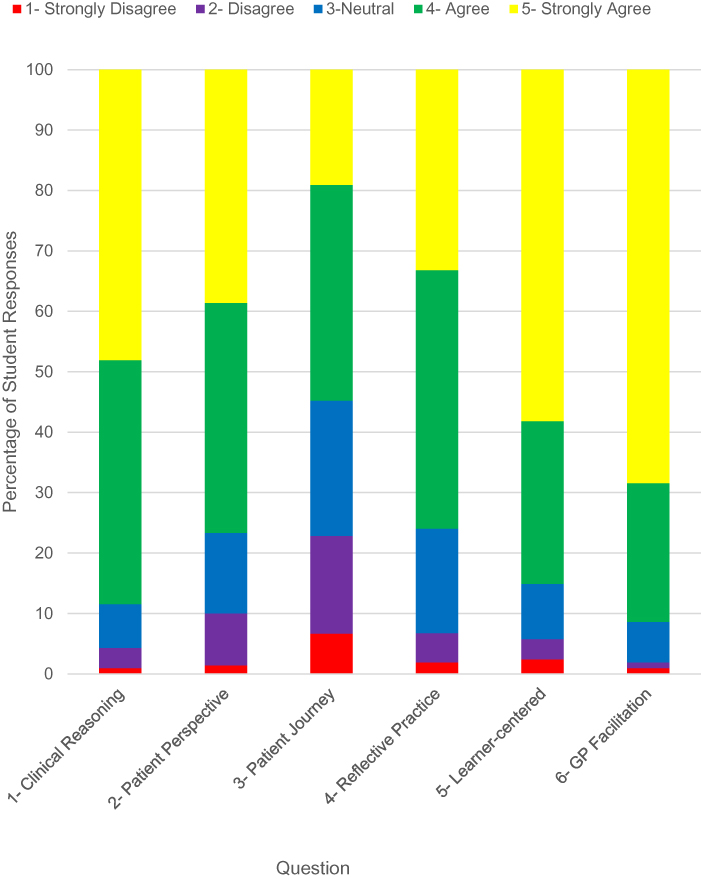 |
Figure 1 Graphical illustration of quantitative data from student questionnaire. |
Qualitative Data
In both the questionnaire free-text comments and the focus group data, students mostly discussed how the sessions had improved their broad diagnostic clinical reasoning skills and enhanced their person-centredness. Figure 2 illustrates the factors which facilitated these learning outcomes. Students additionally commented that the 30 mins of the session for reflection had promoted their personal emotional wellbeing through the opportunity to consider experiences that had affected them on practice and facilitated professional development through discussion of professional and ethical dilemmas. As these findings are not the focus of this paper, we have not elaborated on them further. Many students commented that they would like more sessions, ideally weekly throughout the twelve-week placement.
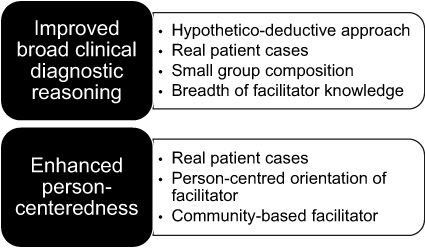 |
Figure 2 Thematic analysis of factors supporting student-perceived learning outcomes. |
Improved Broad Clinical Diagnostic Reasoning
The strongest theme in terms of the number, variety and depth of comments in both the questionnaire and the focus groups data was the students’ perception that their broad clinical diagnostic reasoning had improved with many mentioning phrases such as “vast improvement.” Our thematic analysis revealed that this outcome was enabled by four factors which are discussed below.
Students described moving away from a formulaic approach to history taking towards a hypothetico-deductive approach to clinical reasoning where they constructed hypothesis based on the symptoms the patient presented with and then asked questions which allowed them to confirm or refute these.
The sessions helped me to convert my history-taking from a list of questions to: what are the differential diagnoses here and what questions can I ask to confirm or rule out? (Evaluation Questionnaire)
I think it was really helpful because … when you’re taking a history rather than just in effect ticking all the boxes to get the information, you actually process the information at the same time. (Focus Group 2, F7)
They described learning the importance of considering a wide range of diagnostic possibilities for a presenting problem across a broad range of specialties and not just the most obvious ones or limited to a single organ system.
[It helped with] … thinking outside the box and not obviously just thinking of the system that is obvious to that presenting complaint, thinking about all the other systems. (Focus Group 1, F1)
Their comments suggested they learned the importance of avoiding “premature closure”, when important alternative diagnosis may be missed, and started to recognize that illnesses do not always present in a typical, “textbook” manner. They also described learning how to prioritize which diagnoses were most likely in a particular case. Many students described how they were able to track their own progress during the sessions as they applied this new reasoning approach to history taking on whilst on placement.
I think it’s a structured way of thinking that’s really improved and not necessarily ruling things out just because it’s not a theoretical textbook presentation and realizing that actually yes you can rule certain diagnoses out once you’ve considered a cluster of things, … so it’s being a bit more open minded in terms of your thinking. (Focus Group 1, M4)
As our sessions went on, we were quicker at reaching the differentials and you could see how, like, we’d progressed in our history taking and decision making. (Focus Group 2, F7)
They described finding this learning supported the development of skills that they recognized they would need to employ in real clinical practice as future doctors.
The GP sessions have added the actual, like, realistic aspect to it and it’s less like being a student and more like being a trainee doctor … you’re actually thinking of clinical aspects and patients as opposed to just ticking off what you need to tick off to get through the year. (Focus Group 1, M6)
Most student comments suggested that bringing real patient cases enabled an authentic exploration of clinical reasoning. With only one student in the group aware of the eventual diagnosis, other students could participate in an actual clinical reasoning process.
We were able to discuss patients that we had taken histories from and acted as the patient so that others could practice taking histories from us. It allowed us to form diagnoses from real life patients and discuss management as a group. (Evaluation Questionnaire)
Several students commented that composing the small groups with students assigned to different clinical specialty wards facilitated the breadth of their clinical diagnostic reasoning practice. This mitigated the problem of narrowing their clinical experience during these longer placements.
It was highly useful to sit and discuss with students who had been on different wards and experienced a different part of medicine to myself. This helped me develop awareness of important points in a history in areas other than Gastro where I had been placed. (Evaluation Questionnaire)
Many students commented that GPs are ideally suited to developing broad clinical diagnostic reasoning skills due to their generalist knowledge which enabled students to think across specialties. Within these comments, there was also an appreciation that as doctors in the community who regularly see patients with undifferentiated conditions, GPs practise the broad clinical diagnostic reasoning skills they needed.
Our GP was able to offer us the mind-set of a generalist; seeing the broader picture and the common conditions/pitfalls, rather than just focusing on a specific symptom of a specific disease. (Evaluation Questionnaire)
Enhanced Person-Centredness
Most students felt the sessions had enhanced their person-centredness both in terms of connecting the patient context and perspective to the diagnostic process and in terms of considering the patient journey from home to hospital and back. Thematic analysis suggested that this was supported by real patient cases and a facilitator with person-centred orientation, based in the community.
The use of real patient cases allowed the student presenting to discuss the individual patient’s circumstances, perspectives and goals and students commented that this helped them connect this information with the diagnostic process.
These sessions made me appreciate the patient’s viewpoint of their treatment more and how their aspirations can guide appropriate management. (Evaluation Questionnaire)
Many patients were from lower socioeconomic backgrounds and this brought to my attention a number of factors such as mobility, accommodation and income in the lives of patients’ post-discharge. (Evaluation Questionnaire)
Some students also commented that prior to these sessions they had not understood the importance and relevance of a person-centred approach. This suggests that for these students this was their first opportunity of understanding the real-world relevance of this principle.
Would not have considered asking the patients about their concerns and what they wanted to achieve prior to these sessions. (Evaluation Questionnaire)
Students felt that the person-centred orientation of their facilitators helped them to broaden the discussion from a disease-orientated approach, which they saw as the norm in hospital specialist practice, to understanding how different patient contexts, needs, perspectives and goals need to be taken into account in clinical decision-making.
GPs are so much more holistic I think in their approach and more in tune with long-term impacts for patients. (Evaluation Questionnaire)
GP tutor was very good about discussing how their circumstances can affect the treatment, likely diagnosis etc. (Evaluation Questionnaire)
Community-Based Facilitator
Students’ spoke of how having a GP facilitator enabled them to consider the journey of the patient from their home to the hospital and back. Some of these comments suggested that they learned as much from stories GPs told them of their practice as the patient cases they were discussing.
The GP gave an interesting view on how he would see these patients in the community before and after their hospital admission. He made us think more about the patient’s home situations and life outside of the hospital. (Evaluation Questionnaire)
For almost half the students who did not feel that they learned about patient needs in the community after discharge this was put down to it not being brought up by the facilitator, a lack of time or the students’ preference to engage with the diagnostic reasoning process.
Discussion
The key aim of this educational innovation was a useful opportunity for our novice undergraduate medical students to develop broad clinical diagnostic reasoning skills, which incorporated patient context and perspective. Both the Likert scores and the qualitative data suggest that students’ perceived that this outcome was achieved at scale.
Many of the students’ comments describe the difficulty they found in connecting their pre-existing knowledge and the process of taking a history with the ability to clinical reason from the starting point of the patient’s problems. This finding reinforces existing literature that the knowledge of medical sciences does not automatically lead to development of clinical reasoning and that students need support to learn how to use their knowledge to reason through real patient problems.8,17,19 A recent qualitative study suggested that students’ find the acquisition of clinical reasoning skills troublesome and that they require repeated practice under supervision.20 Continuity of feedback supports this repeated practice and is increasingly recognized as an important mechanism through which positive student learning outcomes can be achieved on clinical placements.21,22 Feedback has been suggested as the most critical factor to the development of clinical diagnostic reasoning in novices.23 Our intervention provided students with an opportunity to experience the benefits of deliberate practice and continuity of feedback which has been shown to be valuable even in comparatively short placements of between 3 and 12 weeks.24,25
Furthermore, some student comments suggest that their theoretical knowledge base led to a propensity to think in terms of “typical” presentations and to consider only a limited number of possibilities, often within a single organ system. The fact that they were based on specialized wards made broad thinking more problematic as they started to assume that certain symptoms (e.g., nausea) belonged to certain specialties (e.g., gastroenterology). Their comments underline how their knowledge organization reflects both teaching and clinical exposure.17 Composing the small groups from different speciality wards and having doctors with broad generalist expertise proved to be effective strategies for promoting students to think broadly across different clinical specialties when considering possible diagnoses. These GP-facilitated sessions may have helped to mitigate potential narrowing of diagnostic thinking as a result of placement on the same hospital ward for 12 weeks. Narrowing of thinking and premature closure are causes of diagnostic error and any educational intervention that promotes breadth of diagnostic thinking is therefore highly pertinent to the objective of improving the safety of medical practice.26
In terms of using non-analytic clinical reasoning processes such as pattern recognition, student comments only refer to “textbook” patterns they had come across in pre-clinical learning and assumptions around symptoms being related to one organ system or speciality. The use of pattern recognition from illness scripts is more often used by experts and a lack of clinical experience may have reduced the use of this strategy in these more novice clinical learners.27 It is also possible that our tutors focused more on the analytical approaches to clinical reasoning and less on asking students to challenge their possible underlying assumptions and biases. Future tutor training on the theory of clinical reasoning might encourage them to focus more on these non-analytical processes.
The use of real patient cases brought in by students proved to be an effective strategy for enabling clinical reasoning. As the facilitator was also unaware of the case or the diagnosis, the focus of the teaching could remain on the process of developing effective reasoning strategies rather than the “correct” answer.9 By questioning the reasons behind the students’ proposed diagnosis or requested information, the facilitator was able to give instant feedback on the students’ reasoning. Engagement with real patients has the additional important benefit of exposing students to the reality of complex atypical patient stories rather than “textbook” symptoms.9 Finally, student comments showed that they found these real patient cases engaging and recognized how they connected with their future clinical practice. This is consistent with the medical education literature which reports several benefits of using real patients for teaching including increasing student motivation through promoting relevance to clinical practice and developing appreciation of complexity.28–30
GP facilitation seemed to be a key factor in students’ perception of how the sessions enhanced their person-centredness, with students appreciating their facilitators' holistic orientation. An increased understanding of patient needs in the community was variably achieved. This was possibly due to a number of related factors mentioned by the students: a lack of time in a short 90-min session, a focus on diagnosis rather than management and facilitators not leading the discussion in that direction. However, where it was achieved, this was almost exclusively put down to the facilitator being ag eneral practitioner. Encouraging students to consider the patient journey across the primary and secondary care divide is a key objective of UK medical education.10 Many of the proposed solutions have involved following patients between primary and secondary care, often within the model of a longitudinal integrated clerkship (LICs). In the UK, the large majority of LICs are only available to small numbers of students.31 Our model offers a pragmatic opportunity for all students to consider the patient journey of hospital patients through education facilitated by a community-based clinician.
Finally, we also reflect that utilizing GPs to facilitate clinical reasoning in hospital placements increases students’ exposure to GP role models and highlights the intellectual work of consultations in general practice. Both of these are stated as possible factors in encouraging students to choose ag eneral practice career in a recent UK report.10 Increasing the number of medical students who choose general practice as a career to address population healthcare needs is a stated aim across many countries.32 Although this was not one of our primary aims and was not evaluated, our innovation has been included in a recent Scottish governmental report as an example of how to increase primary care input into undergraduate medical education.33
Future Developments
On the strength of this evaluation, our medical school has agreed to integrate GP-facilitated small group teaching into the two final year longitudinal integrated hospital placements planned for 2021 and which will constitute another 21 weeks of placement time. This will mean that students will be taught in GP-facilitated small groups in every year of our five-year curriculum. We plan to focus more on management, patient journey and discharge planning in these final year sessions.
Strengths and Limitations
There are several limitations to our study. Our evaluation is at a single institution and our context may be different to other institutions. We have only elicited student views on learning outcomes and our evaluation does not include objective measures to assess if these learning outcomes were indeed acquired. The themes from the written comments and focus groups were not checked with the student participants for agreement. There is also no comparator group of students who received a different educational intervention to see if there would be differential learning outcomes. It may have also been helpful to ascertain GP facilitator’s view of the teaching sessions in order to understand if some areas of learning were less well covered by them. There are however several strengths. Our intervention is delivered to large number of students across a whole year cohort and therefore does not suffer the problems of pilot evaluations where it is not clear if outcomes will be realized at scale. Also, the large amount of quantitative data and the agreement of the themes triangulated across from the written comments and focus groups gives us confidence in our results on student-perceived outcomes.
Conclusions
Our evaluation suggests that broad clinical diagnostic reasoning skills can be facilitated for medical students in specialised hospital settings through regular general practitioner facilitated sessions integrated into the placement. These sessions also have the potential to support the development of a person-centred perspective to information gathering and consider patient needs in the community. The design of our innovation combines known benefits of deliberate practice, feedback and supervisor continuity in a small group format with the resource of GP educators to deliver core curricular competencies. Importantly, our innovation presents a pragmatic opportunity to enhance student learning during longer hospital placements and being deliverable at scale to whole student cohorts.
Acknowledgments
The authors would like to thank Professor James Crossley for his strategic support in delivering the pilot intervention, Dr Michael Nelson for facilitating communication of the pilot evaluation findings with the education leads in hospitals and to Professor Maggie Bartlett for her advice on this manuscript. We would also like to thank GP educators Dr Rob Corker, Dr Lizz Lidbury, Dr Liz Martinez and Dr Paul Johnstone for their support in the pilot intervention and all the GP educators who took part in the first year of the rollout intervention.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Council GM. Outcomes for Graduates 2018; 2018.
2. Inui TS, Williams WT, Goode L, et al. Sustaining the development of primary care in academic medicine. Working Group on Sustaining the development of academic primary care. Association of American Medical Colleges. Acad Med. 1998;73(3):245–257. doi:10.1097/00001888-199803000-00012
3. Williams RG, Klamen DL, Markwell SJ, Cianciolo AT, Colliver JA, Verhulst SJ. Variations in senior medical student diagnostic justification ability. Acad Med. 2014;89(5):790–798. doi:10.1097/ACM.0000000000000215
4. Ark TK, Brooks LR, Eva KW. The benefits of flexibility: the pedagogical value of instructions to adopt multifaceted diagnostic reasoning strategies. Med Educ. 2007;41(3):281–287. doi:10.1111/j.1365-2929.2007.02688.x
5. Mamede S, Van Gog T, Sampaio AM, De Faria RMD, Maria JP, Schmidt HG. How can students’ diagnostic competence benefit most from practice with clinical cases? The effects of structured reflection on future diagnosis of the same and novel diseases. Acad Med. 2014;89(1):121–127. doi:10.1097/ACM.0000000000000076
6. Eva KW. What every teacher needs to know about clinical reasoning. Med Educ. 2005;39(1):98–106. doi:10.1111/j.1365-2929.2004.01972.x
7. Eva KW, Hatala Rm, LeBlanc VR, Brooks LR. Teaching for the clinical reasoning literature: combined reasoning strategies help novice diagnosticians overcome misleading information. Med Educ. 2007;41(12):1152–1158.
8. Ericsson KA. Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Acad Med. 2004;79(10SUPPL.):70–81. doi:10.1097/00001888-200410001-00022
9. Kassirer JP. Teaching clinical reasoning: case-based and coached. Acad Med. 2010;85(7):1118–1124. doi:10.1097/ACM.0b013e3181d5dd0d
10. Wass V, Gregory S, Petty-Saphon K, et al. By Choice — Not by Chance: Supporting Medical Students Towards Future Careers in General Practice. London; Health Education England and the Medical Schools Council, 2016. doi:10.1186/s12909-016-0589-1
11. Fazio SB, Demasi M, Farren E, et al. Blueprint for an undergraduate primary care curriculum. Acad Med. 2016;91(12):1628–1637. doi:10.1097/ACM.0000000000001302
12. Walters L, Greenhill J, Richards J, et al. Outcomes of longitudinal integrated clinical placements for students, clinicians and society. Med Educ. 2012;46(11):1028–1041. doi:10.1111/j.1365-2923.2012.04331.x
13. Gay S, Bartlett M, McKindley R. Teaching clinical reasoning to medical students. Clin Teach. 2013;10(5):308–312. doi:10.12968/hmed.2017.78.7.399
14. Harris A, Boyce P, Ajjawi R. Clinical reasoning sessions: back to the patient. Clin Teach. 2011;8(1):13–16. doi:10.1111/j.1743-498X.2010.00407.x
15. Bridgens J. Medical education in the real world. Med Educ. 2003;37(5):470. doi:10.1046/j.1365-2923.2003.01451.x
16. Linn A, Khaw C, Kildea H, Tonkin A. Clinical reasoning: a guide to improving teaching and practice. Aust Fam Physician. 2012;41(1–2):18–20.
17. Bowen JL, Cox M, Irby DM. Educational strategies to promote clinical diagnostic reasoning. N Engl J Med. 2006;355(21):2217–2225. doi:10.1056/NEJMra054782
18. Young ME, Dory V, Lubarsky S, Thomas A. How different theories of clinical reasoning influence teaching and assessment. Acad Med. 2018;93(9):1415. doi:10.1097/ACM.0000000000002303
19. Prince KJAH, Boshuizen HPA, Van Der Vleuten CPM, Scherpbier AJJA. Students’ opinions about their preparation for clinical practice. Med Educ. 2005;39(7):704–712. doi:10.1111/j.1365-2929.2005.02207.x
20. Pinnock R, Anakin M, Jouart M. Clinical reasoning as a threshold skill. Med Teach. 2019;41(6):683–689. doi:10.1080/0142159X.2019.1569754
21. Hirsh DA, Ogur B, Thibault GE, Cox M. “Continuity” as an organizing principle for clinical education reform. N Engl J Med. 2007;356(8):858–866. doi:10.1056/NEJMsb061660
22. Thistlethwaite JE, Bartle E, Chong AAL, et al. A review of longitudinal community and hospital placements in medical education: BEME Guide No. 26. Med Teach. 2013;35(8):e1340–e1364. doi:10.3109/0142159X.2013.806981
23. Norman G. Research in clinical reasoning: past history and current trends. Med Educ. 2005;39(4):418–427. doi:10.1111/j.1365-2929.2005.02127.x
24. Diuguid-Gerber J, Porter S, Quiah SC, et al. The Columbia-Bronx VA amalgamative clerkship: an effective, 12-week, integrated, longitudinal clinical experience. Med Educ Online. 2017;22(1):1301630. doi:10.1080/10872981.2017.1301630
25. Biggs JL, Sutherell JS, Remus R, Armbrecht ES, King MA. Positive outcomes of optimizing student–preceptor continuity in a traditional block clerkship. Teach Learn Med. 2018;30(2):202–212. doi:10.1080/10401334.2017.1412832
26. Croskerry P. Clinical cognition and diagnostic error: applications of a dual process model of reasoning. Adv Heal Sci Educ. 2009;14(S1):27–35. doi:10.1007/s10459-009-9182-2
27. Croskerry P. A universal model of diagnostic reasoning. Acad Med. 2009;84(8):1022–1028. doi:10.1097/ACM.0b013e3181ace703
28. Bell K, Boshuizen HPA, Scherpbier A, Dornan T. When only the real thing will do: junior medical students’ learning from real patients. Med Educ. 2009;43(11):1036–1043. doi:10.1111/j.1365-2923.2009.03508.x
29. Spencer J, Blackmore D, Heard S, et al. Patient-oriented learning: a review of the role of the patient in the education of medical students. Med Educ. 2000;34(10):851–857. doi:10.1046/j.1365-2923.2000.00779.x
30. Dammers J, Spencer J, Thomas M. Using real patients in problem-based learning: students’ comments on the value of using real, as opposed to paper cases, in a problem-based learning module in general practice. Med Educ. 2001;35(1):27–34. doi:10.1046/j.1365-2923.2001.00841.x
31. Brown MEL, Anderson K, Finn GM. A narrative literature review considering the development and implementation of longitudinal integrated clerkships, including a practical guide for application. J Med Educ Curric Dev. 2019;6:238212051984940. doi:10.1177/2382120519849409
32. Pfarrwaller E, Sommer J, Chung C, et al. Impact of interventions to increase the proportion of medical students choosing a primary care career: a systematic review. J Gen Intern Med. 2015;30(9):1349–1358. doi:10.1007/s11606-015-3372-9
33. Undergraduate education in Scotland: enabling more general practice based teaching. Scottish Government. 2019. Available from: https://www.gov.scot/publications/undergraduate-medical-education-scotland-enabling-more-general-practice-based-teaching/.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.