")
Back to Journals » International Journal of Women's Health » Volume 13
Determinants of Stillbirth Among Deliveries Attended in Bale Zone Hospitals, Oromia Regional State, Southeast Ethiopia: A Case–Control Study
Authors Mekonnen Dagne H , Takele Melku A , Abdurkadir Abdi A
Received 12 August 2020
Accepted for publication 5 December 2020
Published 8 January 2021 Volume 2021:13 Pages 51—60
DOI https://doi.org/10.2147/IJWH.S276638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Henok Mekonnen Dagne,1 Abulie Takele Melku,1 Adem Abdurkadir Abdi2
1World Vision Ethiopia, Hawassa, Ethiopia; 2Department of Public Health, Madda Walabu University Goba Referral Hospital School of Health Science, Bale Goba, Ethiopia
Correspondence: Abulie Takele Melku
Department of Public Health, Madda Walabu University Goba Referral Hospital School of Health Science, PO Box 302, Bale Goba, Ethiopia
Tel +251911060837
Email [email protected]
Background: Stillbirth is one of the adverse outcomes of pregnancy, and it is among the major public health problems in developing countries including Ethiopia. Stillbirth has wide-reaching consequences for parents, care providers, community and society at large.
Purpose: To assess the determinant of stillbirth among deliveries attended in Bale zone hospitals Southeast Ethiopia.
Methods: An institution-based unmatched case–control study was conducted. Cases were deliveries whose birth outcome was stillbirth and controls were deliveries with live birth. A pretested and structured checklist was used to collect data from a sample of 402 (134 cases and 268 controls). Systematic random sampling was used to recruit samples from a list of charts in the delivery registration book. Data were entered into EpiData version 4.2 and exported to SPSS version 20 for analysis. Crude and adjusted odds ratio with 95%CI was calculated and P-value < 0.05 was used to declare statistical significance.
Results: A total of 402 charts of mothers (134 cases and 268 controls) were included in the analysis. Preceding birth interval < 24 months (AOR: 2.991; 95%CI: 1.351– 6.621), antenatal visit started at third trimester (AOR: 2.739; 95%CI: 1.048– 7.158), referred from other health facility (AOR: 3.215; 95%CI: 1.430– 7.229), labor length ≥ 24 h (AOR: 3.169; 95%CI: 1.241– 8.091), presence of meconium stained amniotic fluid (AOR: 2.670; 95%CI: 1.082– 6.592) and giving birth to a baby < 2500 g (AOR: 3.155; 95%CI: 1.235– 8.07) were determinants of stillbirth.
Conclusion: Preceding birth interval of < 24 months, antenatal visit started at third trimester, referred from other health facility, presence of meconium stained amniotic fluid, labor length ≤ 24 h and giving birth to a baby < 2500 g were found the determinants of stillbirth. Intrapartum care, early identification of labor complications and referral system are required.
Keywords: stillbirth, determinant, cases, controls
Introduction
Stillbirth is one of the prevalent adverse outcomes of pregnancy and has been defined by the WHO as “a baby born without any signs of life at or after 28 weeks of gestation or at least 1000 gram by weight.” This criterion is recommended by WHO for international comparability and is being used by 193 countries including Ethiopia.1 There is no uniformity among states regarding the criteria for reporting stillbirth based on their standards of neonatal intensive care. In the US, stillbirth is pregnancy loss at or after 20 weeks of gestation or at least 350 g by weight.2
Global estimate of 2015 indicates that, every year more than 7300 stillbirths occur, ie 18.4 per 1000 total births. Ninety-eight percent of all stillbirths occur in low and middle-income countries, where 77% of them are from south Asia and sub-Saharan Africa.3 In Africa, approximately one million babies are stillborn each year, of which at least 300,000 die during labor.4 This significant loss of life is frequently unrecognized and hidden due to the stigma associated with stillbirth in many countries.5
Stillbirth rate varies sharply by country, from the lowest rates of two per 1000 births in Finland and Singapore, to the highest 47 in Pakistan and 42 in Nigeria.6 It is estimated that 1.8 million stillbirths occur in ten countries: India, Pakistan, Nigeria, China, Bangladesh, Democratic Republic of Congo, Ethiopia, Indonesia, Afghanistan, and the United Republic of Tanzania. Almost half of stillbirths (1.2 million) happen when the woman is in labor and these deaths are directly related to the lack of skilled care at this critical time.6
The stillbirth rate is an important indicator of quality of care in pregnancy and childbirth, as well as a sensitive marker of health-care system. Post-2015 initiatives show that stillbirths are a hidden agenda worldwide and are continued in the sustainable development goal.7 A target to end preventable stillbirths was included in the Every Newborn Action Plan and endorsed for 194 countries including Ethiopia on the world health assembly in 2014. The plan was set with a goal of reducing national stillbirth rate to 12 or fewer per 1000 births by 2030.8
Stillbirth remains hidden from society, and has wide-reaching consequences for parents, care providers, community, and society that are frequently overlooked and undermined. The estimated direct financial cost of stillbirth is 10–70% greater than the cost of a live birth.5 An estimated 4.2 million women are living with depression associated with stillbirth. Care providers are also deeply affected both personally and professionally, experiencing guilt, anger, anxiety, and sadness.7
The main causes of stillbirth have been identified as childbirth complications, maternal infections in pregnancy, maternal disorders (especially preeclampsia and diabetes), fetal growth restriction and congenital abnormalities. An estimated 1.1 million stillbirths could be averted with universal coverage of comprehensive emergency obstetric care, syphilis detection and treatment, detection and management of fetal growth restriction and hypertension during pregnancy, malaria prevention and folic acid fortification.9
The World Health Statistics 2013 report has shown that Ethiopian stillbirth rate accounts 26 per 1000 deliveries which is third highest in East African countries next to Djibouti and Somalia; and seventh among the ten countries that account for two-thirds of all third trimester stillbirths in the world. In 2015, 3,200,000 babies were born in Ethiopia which is approximately 8700 every day; of which 258 (3%) stillbirths occur every day.10 The Ethiopian Demographic and Health Survey of 2016 also indicated that the national perinatal mortality rate is 33 per 1000 births and 30 per 1000 births in Oromia region, which is among the highest compared to other regions of the country.11
Factors determining the occurrence of stillbirth might be related to the maternal sociodemographic, maternal medical status, pregnancy, labor and delivery and fetal factors. Studies have shown that factors such as place of residence, maternal age greater than 35 years, lack of antenatal care, prematurity, prolonged labor, no parity, mode of delivery, congenital anomalies, multiple pregnancy, preeclampsia, antepartum hemorrhage and premature rupture of membrane were found to be among factors significantly associated with stillbirth.3,12,13
In order to prevent stillbirth, its main modifiable risk factors need to be understood. In addition, the interrelationship between maternal health and obstetric factors needs to be investigated. Research is critical to develop interventions aimed at averting such risk factors of stillbirth. Hence, this study was conducted to identify sociodemographic, maternal health-related and obstetric-related factors that possibly result in stillbirth in the study area that could be used to design sound interventions.
Methods and Materials
The study was conducted at the five public hospitals found in Bale zone. Bale zone is located in Oromia regional state in Southeast Ethiopia. Robe town, the capital of Bale zone is found 430 km away from Addis Ababa, the capital city of Ethiopia. Currently, the zone has 21 districts of which three are town administrations and of the rural districts nine are agrarian and nine are agro-pastoralist. The zone has a total population of 1,888,366 of which 951,736 are male, 936,630 are female and the expected deliveries in the study year accounts are 65,526. A total of five public hospitals are found in the zone; namely Goba Referral Hospital, Robe General Hospital, Ginnir General Hospital, Dalo Mena General Hospital and Madda Walabu Primary Hospital. There are also 87 functional health centers in the zone. Concerning comprehensive maternal service delivery, all the hospitals deliver comprehensive emergency, obstetric, and neonatal care service and 76 health centers deliver basic emergency, obstetric and neonatal care services.
Study Period and Design
The study was conducted from July 2018 to June 2019 and an institution-based unmatched case–control study design was employed.
Population
All charts of mothers who delivered from July 2018 to June 2019 in the five hospitals of Bale zone were the source population. All charts of mothers delivered from July 2018 to June 2019, which were selected by systematic random sampling as cases and controls in the five hospitals of Bale zone were the study population. Stillbirths whose charts are available and have full history recorded delivery summery and/or procedure notes during the study period were included in the study as cases. Live births, whose charts are available and have full history, delivery summery and or procedure notes during the study period were included in the study as controls. Twelve charts which were found incomplete on major variables under study (no information about antenatal period, labor status and/or delivery summary) and missed charts were excluded.
Sample Size Determination
Sample size is calculated using EpiInfo 7.0 StatCalc program by taking assumptions of 95% confidence level, two controls for each case, 80% power and the prevalence of exposure among control 7.1% with odds ratio 2.8 (1.78, 4.46) of variable low birth weight, were taken from an unmatched a case–control study done at Hawasa University Hospital, Ethiopia.12 A total sample size of 366 (122 cases and 244 controls) were calculated and adding 10% contingency for incomplete check list filled by data collectors and the final sample size was 402 (134 cases and 268 controls). A variable low birth weight was selected because it was the exposure variable that gave the highest sample size for cases and controls among the other variables in a study conducted in Hawasa University.
Sampling Techniques
The allocation of samples to each hospital was determined based on proportion of number of cases using report of the period (July 2018 – June 2019). Accordingly from Goba Referral Hospital 37 cases and 74 controls, Robe General Hospital 33 cases and 66 controls, Ginnir General Hospital 35 cases and 70 controls, Dalo Mena General Hospital 20 cases and 40 controls and Madda Walabu Primary Hospital nine cases and 18 controls were taken. Systematic random sampling with interval K=3 was used to recruit charts of cases after listing medical record numbers of all stillbirths in the study period from the delivery registration book of each hospital. Controls were also selected using systematic random sampling from the list of live births prepared from the delivery registration book and using the list as a sampling frame. Then, the selected charts, ie 134 for cases and 268 for controls were identified from the card room.
Study Variables
The dependent variable for the study was stillbirth. And the independent variables were sociodemographic factors (age, residence, marital status), maternal health and pregnancy related factors (gravidity, parity, preceding birth interval, history of stillbirth, maternal medical illness, antenatal follow up, tetanus toxoid vaccination, iron folic acid supplementation, antepartum hemorrhage, hypertensive disorder of pregnancy, premature rupture of membrane), labor and delivery related factors (mode of admission, partograph use, fetal presentation, cord accident, obstructed labor, color of amniotic fluid, labor augmentation, duration of labor, mode of delivery) and fetal related factors (gestational age at birth, birth weight, number of newborns, congenital structure).
Operational Definitions
Stillbirth: a baby born without any signs of life at or after 28 weeks of gestation or at least 1000 g in birth weight.1
Cases: were deliveries whose birth outcome was stillbirths, defined as babies born without any signs of life at or after 28 weeks of gestation or at least 1000 g in weight.
Controls: were deliveries whose birth outcome of live births, defined as babies showing evidence of life (such as beating of the heart, pulsation of umbilical cord) on delivery at or after 28 weeks of gestation or at least 1000 g in weight.
Partograph use: if the data on the three components of partograph (fetal condition, progress of labor, and maternal condition) were completed, it is considered that a partograph is utilized.
Data Collection Tool and Procedure
Data was collected by using pretested and structured checklist which was developed in English language adapted from literature related to stillbirth and modified according to the local context by the investigators. The checklist consists of information on sociodemographic data, maternal health and pregnancy data, labor and delivery data and birth outcome data.
Five data collectors who have midwifery profession were recruited for data collection and five senior midwives were also recruited for facilitation and supervision of daily data collection activities. During collection charts of cases and controls, the following steps were followed: first, all medical record numbers of stillbirths found in the study period were identified and listed from the delivery registration book of each hospital. Using a systematic random sampling method, cases were selected for each hospital proportionally to their annual stillbirth delivery load. Following selection of cases and controls, data collectors and card room workers have selected charts of mothers from card room using medial record numbers and reviewed the history, delivery summery, laboratory results, partograph, decision notes, progress notes, and operation notes and filled in the checklist. Incomplete charts on major variables under study (no information about antenatal period, labor status and/or delivery summary) were excluded. The selected charts were given study identification numbers to be used on the checklist for anonymity.
Data Quality Control and Assurance
Prior to data collection, the data collectors and supervisors were trained with a practical session for one day on techniques of sampling and data collection. Pretest was carried out on 5% of the samples before the actual data collection at Dodola General Hospital and modifications of the checklist were made on rephrasing and skipping patterns. In addition the average time required to complete one checklist was also estimated. Review of medical records was done carefully; charts with incomplete information on major variables under study such as information about antenatal period, labor status and/or delivery summary were excluded. Daily evaluation for completeness at the time of data collection was followed by the supervisor to assure collection of full information and appropriate documentation. The investigator has reviewed all checklists for omissions, clarity, and consistency of data to verify the completeness of the collected data.
Data Analysis
Data entering was performed using EpiData version 4.2 and coding, clearing and analysis was done using SPSS version 20 software statistical packages by the principal investigator. Frequency and proportions were used to describe the study population in relation to relevant variables. Those variables with a P<0.25 in the bivariate logistic regression analysis were entered to multivariate logistic regression analysis and declared significant at 95% confidence interval. Multiple logistic regression analysis was employed and significance was declared at P<0.05 and 95% confidence interval. Multicollinearity test was carried out to see the correlations between predictors of outcome variables. Finally the results were presented using tables and texts.
Ethical Consideration
Ethical clearance was secured and the official letter of permission was obtained from the Madda Walabu University, Goba Referral Hospital. Subsequently, a letter of permission was obtained from each hospital administrator and sent to each hospital maternal and child health units and medical record departments. The objective of the study was explained to the head of each unit and administrators of the hospitals. The permission of the patient to review their medical history was not required by the University of Madda Walabu and the hospitals. Personal identifiers such as name, phone number, etc have not been considered as a code and a care number has been used. At the end of the data collection process, strict attention was paid to the selected charts of study participants during the data collection phase, until the return was respected at the end of the data collection. All information taken from the client charts was kept confidential and only investigators had access to the information which was used only for the purpose of this study.
Results
A total of 402 sampled charts of mothers who gave birth in hospitals of Bale zone were included in the analysis with proportion of case to control ratio of one to two (134 cases and 268 controls) and the chart review response rate was 100%. From a total of 134 stillbirths reviewed, 54% were fresh stillbirths (fetal death during labor and delivery) and 46% of them were macerated stillbirths. Majority of the cases (59.7%) and controls (65.7%) were in mothers’ age 20–34 years and the mean age of the mothers was 28.8 with standard deviation of ±6.57 years. Around 61% of cases and 57.8% of controls were from rural residences and majority of cases (87%) and controls (85%) were married (Table 1).
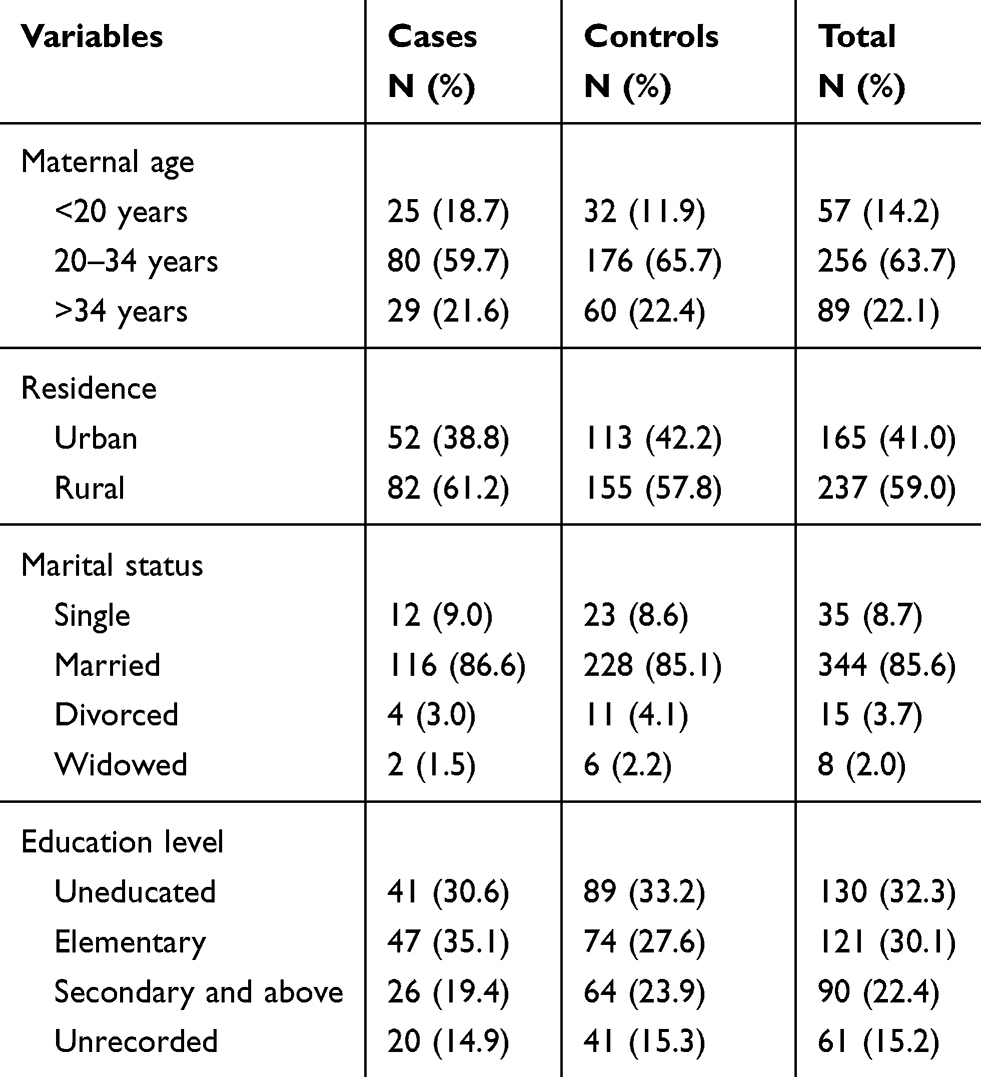 |
Table 1 Sociodemographic Characteristics of Mothers Who Gave Birth and Participated in the Study in Hospitals of Bale Zone, Oromia Regional State, Southeast Ethiopia, 2019 |
Maternal Health and Pregnancy Related Characteristics of Case and Controls
About 41% of cases and almost half of the controls (49%) were multigravida and 54% of cases and 33% of controls have preceding birth interval of less than 24 months. Concerning maternal medical illness about 22% of cases and 20% of controls have experienced different medical illnesses. Among the major medical illnesses, anemia accounts for 34% of cases and 24% of controls (Table 2).
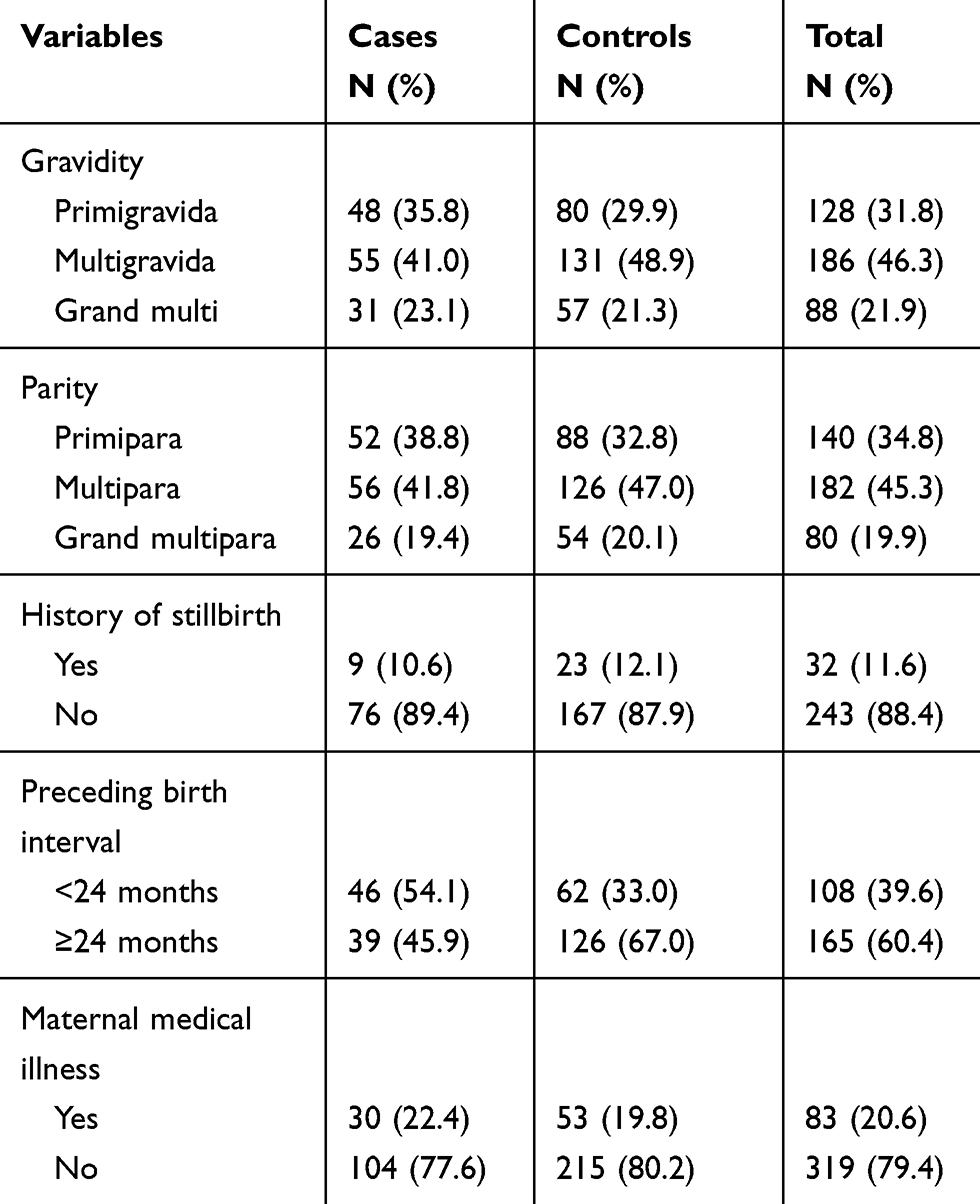 |
Table 2 Maternal Health Related Characteristics of Mothers Who Gave Birth and Participated in the Study in Hospitals of Bale Zone, Oromia Regional State, Southeast Ethiopia, 2019 |
Concerning pregnancy related characteristics, higher percent of mothers 65% of cases and 79% of controls had at least one antenatal follow-up visit. Of those who have history of antenatal visits 39% of cases and 33% of controls had started antenatal follow-up in their first trimester (Table 3).
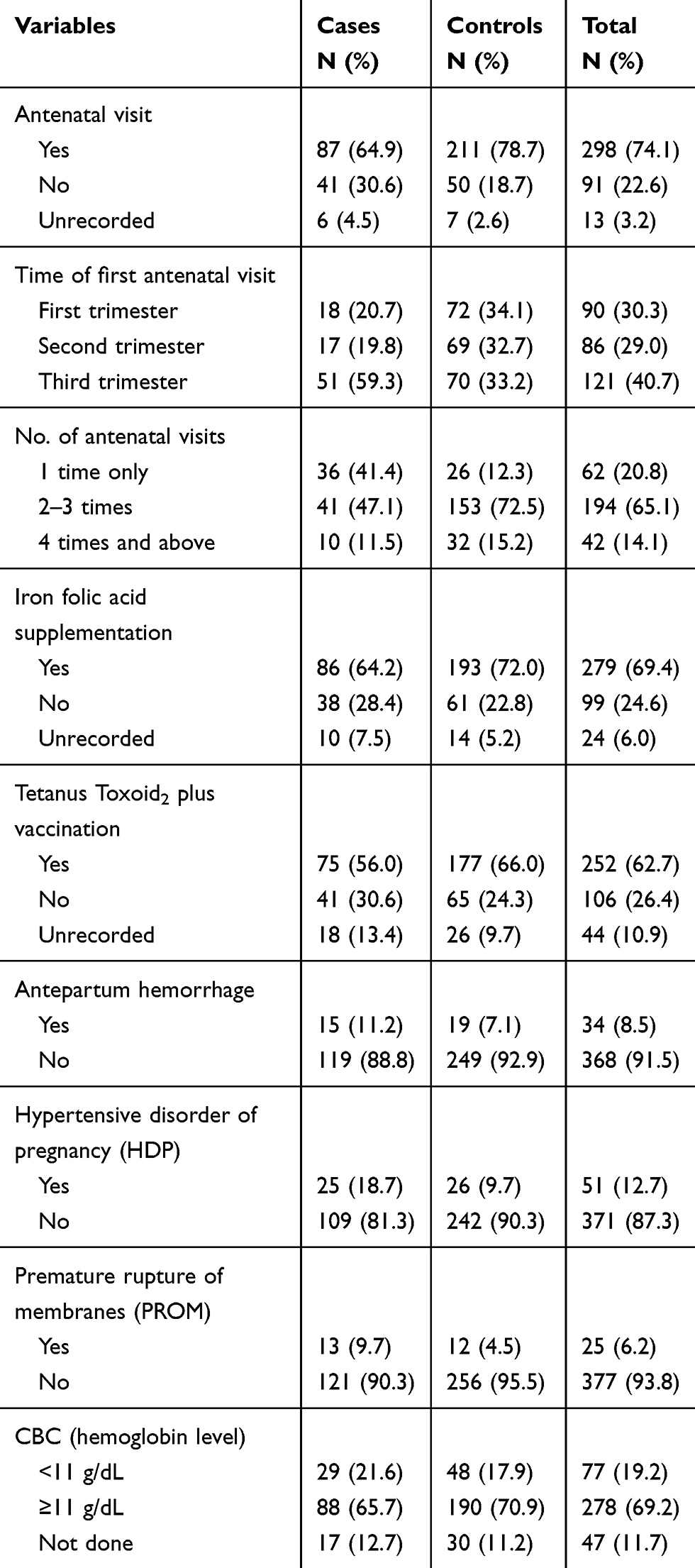 |
Table 3 Pregnancy Related Characteristics of Mothers Who Gave Birth in Hospitals of Bale Zone, Oromia Regional State, Southeast Ethiopia, 2019 |
Labor and Delivery Related Characteristics of Case and Controls
Of the total, 72% of cases and 40% controls were referred from other health institutions. For about 23% of cases and 34% of controls the three components of partograph (fetal condition, progress of labor, and maternal condition) were filled in. Augmentation of labor using two or more dose of augmentin was conducted for 21% of cases and 12% of controls (Table 4).
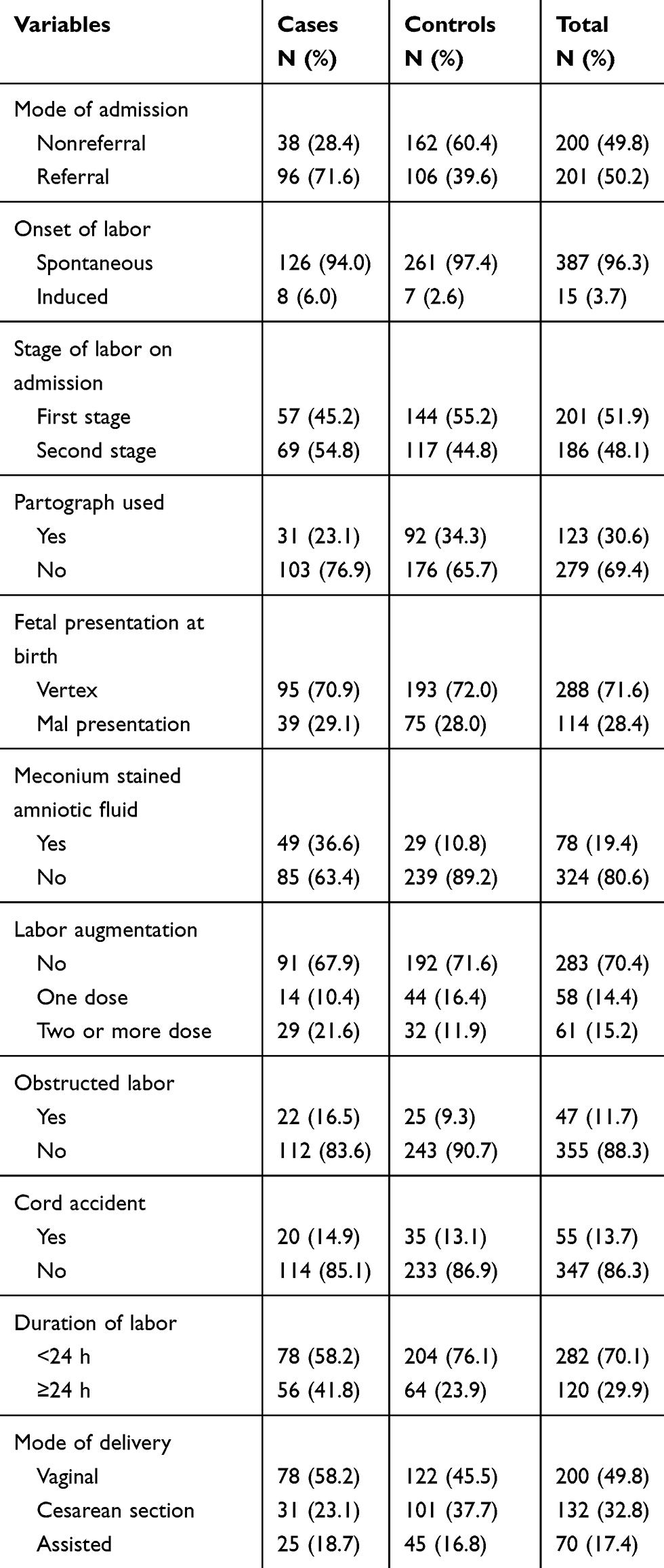 |
Table 4 Labor and Delivery Related Characteristics of Mothers Who Gave Birth in Hospitals of Bale Zone, Oromia Regional State, Southeast Ethiopia, 2019 |
Fetal Related Characteristics of Case and Controls
From a total of 134 cases reviewed, 53.7% were fresh stillbirth (fetal death during labor and delivery) and 46.3% of them were macerated stillbirth. A large proportions of cases (79%) and controls (83%) were delivered in their gestational age of between 37 and 41 weeks. Around 46% cases and 70% of controls have birth weight in the range of 2500–4000 g. Of the deliveries, nearly half of the mothers (48.5% of case and 47.8% of controls) delivered male newborns and only 6.7% of cases and 7% controls had multiple deliveries. Among deliveries 17.9% of cases and 0.7% of controls had congenital malformation.
Determinants of Stillbirth
The association of stillbirth with different independent variables was assessed in bivariate logistic regression and multivariate logistic regression analysis. The result revealed that variables like HDP, PROM, partograph utilization, obstructed labor, preceding birth interval, time first antenatal visit started, mode of admission, meconium stained amniotic fluid, mode of delivery, duration of labor and birth weight have shown statistical association with stillbirth in the bivariate logistic regression analysis (Table 5).
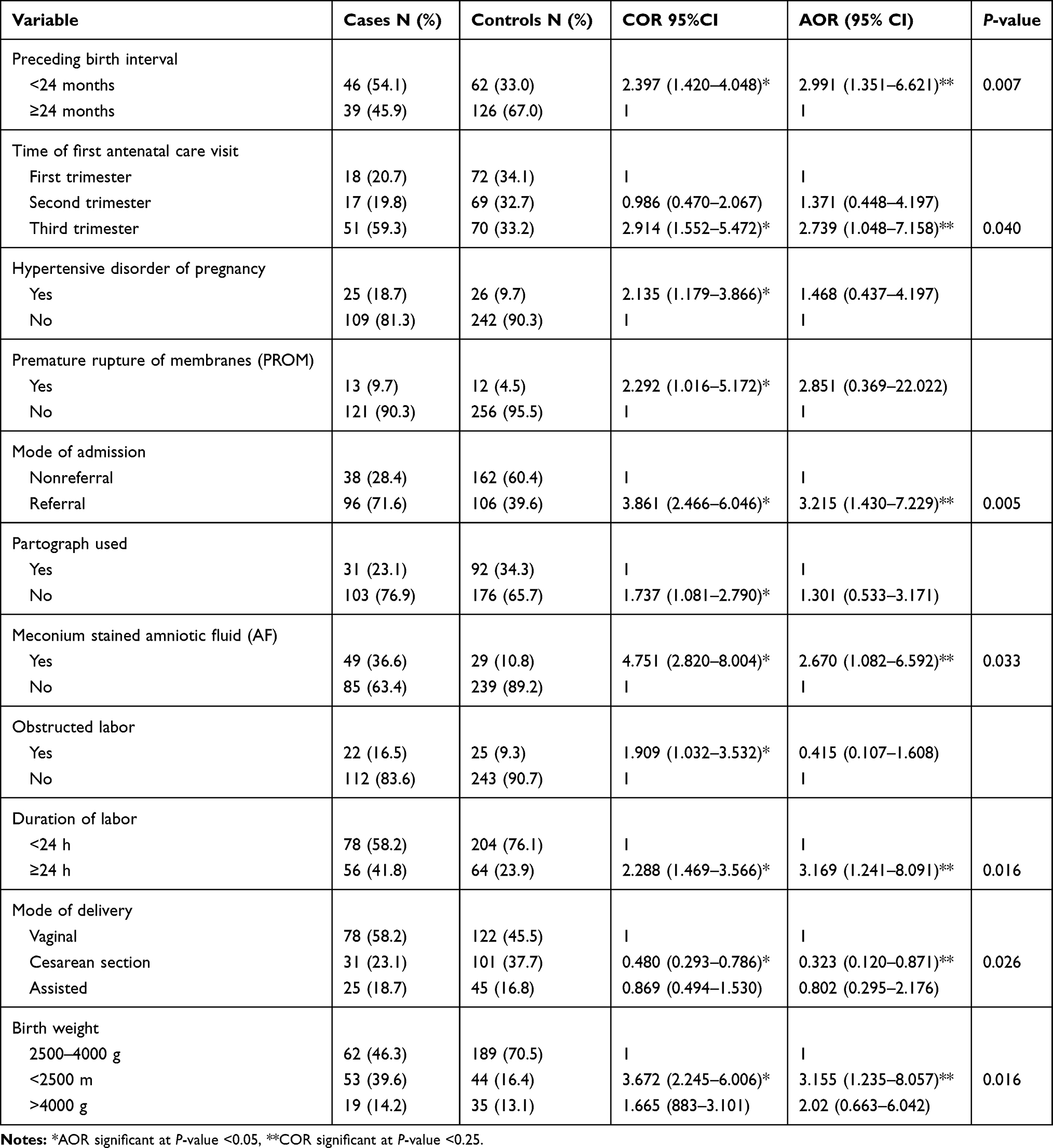 |
Table 5 Determinant Factors of Stillbirth Among Deliveries Attended in Hospitals of Bale Zone, Oromia Regional State, Southeast Ethiopia, 2019 |
Those variables with a P<0.25 in the bivariate logistic regression analysis were entered to multivariate logistic regression analysis and declared significant at 95% confidence interval. The results showed that, less than 24 months of preceding birth interval, being first antenatal visit start at third trimester, being referred from other health facility, having meconium stained amniotic fluid, delivery by cesarean section, labor duration 24 h and above, and birth weight less than 2500 g were found to have significant association with stillbirth (Table 5).
The odds of having stillbirth was three times greater (AOR: 2.991; 95%CI: 1.351–6.621) among mothers with short preceding birth interval than their counterparts. Similarly, stillbirths were 2.7 times higher (AOR: 2.739; 95%CI: 1.048–7.158) in those mothers who started antenatal visit late at the third trimester compared to those started in their first trimester. In the same manner, the odds of experiencing stillbirth was three times higher (AOR: 3.215; 95%CI: 1.430–7.229) in mothers referred from other health facility than those not referred. The risk of experiencing stillbirth was also three times (AOR: 3.169; 95%CI: 1.241–8.091) among mothers who had labored 24 h and above than their counterparts (Table 5).
Odds of stillbirth was 2.6 times greater (AOR: 2.670; 95%CI: 1.082–6.592) among mothers with meconium stained amniotic fluid than their counterparts. It also found that the odds of stillbirth was three times higher (AOR: 3.155; 95%CI: 1.235–8.07) among mothers who gave birth to babies weighing less than 2500 g compared to those who gave birth in the range of 2500–4000 g birth weight. In addition to the above findings, delivery through cesarean section was found to be a protective factor associated with stillbirth. The odds of experiencing stillbirth were 70% less likely (AOR: 0.323; 95%CI: 0.120–0.871) among mothers who had delivered through cesarean section compared to those delivered vaginally (Table 5).
Discussion
In this unmatched case–control study, the determinants of stillbirth among deliveries attended at Bale zone hospitals, Oromia regional state, Southeast Ethiopia were assessed and the result of the study revealed that, preceding birth interval of <24 months, starting antenatal visits at third trimester, being referred from another health facility, presence of meconium stained amniotic fluid, labor duration lasting ≥24 h and giving birth to less than 2500 g baby were the determinants of stillbirth that increased risk of fetal death. Whereas delivery by cesarean section was found to be a protective factor that decreased risk of fetal death.
The odds of experiencing stillbirth were found to be threefold higher among mothers who have preceding birth interval of <24 months in this study. This finding is in agreement with the studies conducted in Amhara region, Ethiopia14 and Addis Ababa public hospitals, Ethiopia.15 The finding is also in line with the Ethiopian Demographic and Health Survey report of 2016.11 This could be because with short birth interval the mother’s body cannot regain the important ingredients and result in inadequate replacement of maternal nutrient stores depleted in the previous pregnancy and lead to reduced fetal growth. This could predispose the fetus to prematurity and its complication which cause stillbirth. Similarly, a review of cause and risk factors of stillbirth in developing countries16 also suggests that short interpregnancy interval is a common threat factor for stillbirth in developing countries.
This study indicated that women who begin attending antenatal visit at the third trimester were around three times more likely to have a stillbirth than those who started attending in their first trimester. Although we did not see significant association between time of antenatal visit start and stillbirth in the literature we have used; the possible implication could be because in mothers who started antenatal visit late in the third trimester, it will be difficult to screen and detect certain risk factors to allow timely interventions and minimize the risk of stillbirth. In contrast, it is also noted that women who started antenatal visits at the third trimester did not have enough time to complete the four antenatal follow-up visits or may not have benefited from all the basic antenatal care packages which can possibly prevent stillbirth.17 Early antenatal care focusing on detection of complications has maximum benefits which can avert 21% of stillbirths.18
WHO also recommends pregnant women to start the first antenatal visit in their first trimester or in the first four months of pregnancy.8 However, according to the Ethiopian Demographic and Health Survey report of 2016, in Ethiopia only 20% of women had their first antenatal visit during the first trimester.11
The odds of having still birth was found to be three times greater among mothers referred from other health institutions compared to their counterparts in this study. This finding is consistent with the results of an intervention program conducted in south Ethiopia.19 This could be due to most of the referred cases coming from rural peripheral health facilities and might be after having serious complications. The distance to reach the hospitals to which they were referred contributes to delay in receiving care, which can obviously cost the life of their fetus. This finding is in contrast to the study done in Jima University Specialized Hospital, Ethiopia,20 which showed that a decrement in stillbirth among those pregnant women referred from another health facility compared to those not referred. The difference might be due to the differences in study area, study design and/or sample size.
This study found that women who had labor length ≥24 h were three times more at risk to have fresh stillbirth compared to those having labor length <24 h. This finding is in agreement with similar study findings at Mizan Tepi Teaching Hospital, Ethiopia,13 Bangladesh,21 and Yemen,17 which showed that labor length lasting ≥24 h was a significant factor for fresh stillbirth. The possible explanation and implications could be that as the length of labor is increasing the fetus could be exposed to stressful uterine contractions and fetal distress which finally leads to its death.
Odds of experiencing stillbirth were identified as 2.6 times higher among mothers with meconium stained amniotic fluid than their counterparts in this study. This finding is consistent with the finding of a study done in Yemen.17 This could be due to intrauterine passage of meconium into amniotic fluid which is thought to occur in response to fetal distress and the infant will inhale the meconium which in turn leads to airway obstruction, surfactant dysfunction and pneumonitis which results in loss of the fetus.
According to the findings of this study, delivery through cesarean section was found to be a protective factor associated with stillbirth. The odds of experiencing stillbirth were 70% less likely among mothers who had delivered through cesarean section compared to those delivered vaginally. This finding is in line with the studies done in Addis Ababa, Ethiopia,15 Hawassa Referral Hospital, Ethiopia,12 and Chandigarh, India.22 This could be due to this kind of delivery being commonly conducted when there was an obstetric complication to prevent further risks to the fetus. This also saves the life of the fetus by allowing it to be delivered before it dies due to fetal distress. This finding is in contrast to study done in Jimma University Specialized Hospital, Ethiopia,20 which showed that those mothers delivered vaginally were less likely to have a stillbirth than those delivered through cesarian section. The difference might be due to the differences in study design and/or sample size.
The other finding of this study was that, giving birth to a baby weighing less than 2500 g was three time more likely to cause stillbirth. This is in line with the studies done in Hawassa Referral Hospital, Ethiopia,12 Mizan Tepi Teaching Hospital, Ethiopia,13 and Nepal,23 which showed that very low and low birth weight babies were at higher risk for stillbirth. Low birth weight is a multifaceted public health problem that includes long-term maternal malnutrition, ill health, and poor health care during pregnancy, which all can result immature newborn and stillbirth.
Limitation of the Study
The study may limit generalizability to community level, since it is institutional based. There could be information bias or some degree of recall bias. The study is retrospective and from secondary data which may be prone to errors. The study does not consider the different types of stillbirth (fresh and macerated stillbirth) which may be caused by different risk factors.
Conclusion
The determinants of stillbirth identified in the current study were; less than 24 months of preceding birth interval, starting antenatal visits at the third trimester, being referred from another health facility, presence of meconium stained amniotic fluid, labor duration lasting 24 h and above, delivery by cesarean section, and giving birth to a baby weighing less than 2500 g.
The determinants of stillbirth identified are manageable and can be amenable to interventions. Therefore, appropriate prevention strategies during antepartum, intrapartum and newborn care and referral system should be focused to tackle these risk factors of stillbirth. Mothers are encouraged to make birth intervals wide. Likewise, pregnant women should be identified early and linked to the appropriate antenatal care and other maternal health-care services. Appropriate intrapartum care, early identification of labor complications and early referral systems should be prioritized.
Abbreviations
ANC, antenatal care; AOR, adjusted odds ratio; APH, antepartum hemorrhage; CBC, complete blood cell count; COR, crude odds ratio; CSA, central statistical agency; EDHS, Ethiopian Demographic and Health Survey; EmONC; emergency obstetric and neonatal care; GA, gestation age; HDP, hypertensive disorders of pregnancy; IFA, iron folic acid; IUFD, intrauterine fetal death; MCH, maternal and child health; PROM, prelabor rupture of membrane; STIs, sexually transmitted infections; TT, tetanus toxoid.
Data Sharing Statement
The data for this study is available with the authors and can be accessed based on the request from the concerned body.
Consent for Publication
All the information used for this study was collected with the consent of participants of the study. And all the authors have read the manuscript and have consented to publish it in this journal.
Acknowledgment
First of all we would also like to extend our thanks to Bale zone health office, Goba Referral Hospital, Robe General Hospital, Ginnir General Hospital, Dalomena General Hospital and Madda Walabu Primary Hospital for their cooperation and for providing relevant information. We would also like to thank all the staff and lecturers of the Madda Walabu University, Goba Referral Hospital, particularly, the Department of Public Health for their incredible support during the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding agencies do not have a role in the publication of the paper.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Stillbirths: Global Trends, Policies and Experience International Forum on Countdown to 2015. Geneva: World Health Organization; 2015.
2. ACOG. Obstetrics of Selected Publications, United States of America; 2010:20–21
3. Lawn JE, Blencowe H, Waiswa P, Amouzou A, Mathers C, Hogan D. Ending preventable stillbirths 2, Stillbirths: rates, risk factors, and acceleration towards 2030. Lancet. 2016;387:587–603. doi:10.1016/S0140-6736(15)00837-5
4. Lawn J, Mong P, Cousens S. Africa ’ s newborns – counting them and making them count; 2013:11–22.
5. Heazell AE, Siassakos D, Blencowe H, et al. Stillbirths: economic and psychosocial consequences. Lancet. 2016;387(10018):604–616. doi:10.1016/S0140-6736(15)00836-3
6. Blencowe H, Cousens S, Jassir FB, et al. National, regional, and worldwide estimates of stillbirth rates in 2015, with trends from 2000: a systematic analysis. Lancet Glob Health. 2016;4:41–58.
7. Susannah B, Leisher H, Lawn JE, Kinney MV, Kuo NT, de Bernis L. Stillbirths: investment in ending preventable stillbirths by 2030 will yield multiple returns and help achieve multiple sustainable development goals. Lancet. 2016;1–5.
8. WHO & UNICEF. Every Newborn: An Action Plan to End Preventable Deaths. Geneva: World Health Organization; 2014.
9. WHO. Stillbirths: The Invisible Public Health Problem. International Stillbirth Alliance. Geneva: World Health Organization; 2011:1–8.
10. Nesbitt U. Maternal and Newborn Health Disparities. Ethiopia;2016. Available from: https://data.unicef.org/resources/maternal-newborn-health-disparities-country-profiles/. Accessed December 31, 2020.
11. EDHS. Ethiopia demographic and health survey 2016 report. Central statistical Agency, Addis Ababa, Ethiopia; 2017.
12. Bayou G, Berhan Y. Perinatal mortality and associated risk factors: a case control study. Ethiop J Health Sci. 2012;22(3):153–162.
13. Weldegebriel TK, Dadi TL, Mihrete KM. Determinants of stillbirth in Bonga General and Mizan Tepi University Teaching Hospitals southwestern Ethiopia, a case - control study. BMC Res Notes. 2017;1–5.
14. Lakew D, Tesfaye D, Mekonnen H. Determinants of stillbirth among women deliveries at Amhara region, Ethiopia. BMC Pregnancy Childbirth. 2017;17(1):32–36.
15. Getiye Y, Fantahun M. Factors associated with perinatal mortality among public health deliveries in Addis Ababa, Ethiopia, an unmatched case control study. BMC Pregnancy Childbirth. 2017;1–7.
16. Mcclure EM, Saleem S, Pasha O, Goldenberg RL. Stillbirth in developing countries: a review of causes, risk factors and Stillbirth in developing countries: a review of causes, risk factors and prevention strategies. J Matern Fetal Neonatal Med. 2009;22:183–190. doi:10.1080/14767050802559129
17. Obad MA, Taher R, Qayad M, Khader YS. Risk factors of stillbirth in Yemen. J Neonatal Perinatal Med. 2018;11(2):131–136. doi:10.3233/NPM-181746
18. Bhutta ZA, Das JK, Bahl R, et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet. 2014;384(9940):347–370. doi:10.1016/S0140-6736(14)60792-3
19. Lindtjorn B, Mitikie D, Zidda Z, Yaya Y. Reducing stillbirths in Ethiopia: results of an intervention programme. PMC. 2018.
20. Tilahun D, Assefa T. Incidence and determinants of stillbirth among women who gave birth in Jimma University specialized hospital, Ethiopia. Pan Afri J. 2017;1–11.
21. Nahar S, Rahman A, Nasreen E. Factors influencing stillbirth in Bangladesh: a case - control study. Paediatr Perinat Epidemiol. 2013;27:158–164.
22. Newtonraj A, Kaur M, Gupta M, Kumar R. Level, causes, and risk factors of stillbirth: a population-based case control study from Chandigarh, India. PMC. 2017;1–9.
23. Kc A, Wrammert J, Ewald U, Clark RB, Gautam J, Baral G. Incidence of intrapartum stillbirth and associated risk factors in tertiary care setting of Nepal: a case-control study. BMC Pregnancy Childbirth. 2016;1–11.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.