")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Determinants of Statin Initiation Among Adult Diabetic Patients in Bonga, Ethiopia
Authors Kebede zelalem B , Feyisa D
Received 27 September 2020
Accepted for publication 18 November 2020
Published 8 December 2020 Volume 2020:13 Pages 4839—4847
DOI https://doi.org/10.2147/DMSO.S283993
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Bezie Kebede zelalem, Desalegn Feyisa
School of Pharmacy, College of Health Science, Mizan-Tepi University, Mizan-Teferi, Ethiopia
Correspondence: Bezie Kebede zelalem Tel +251 921279910
Email [email protected]
Background: Diabetes mellitus (DM) is a chronic degenerative disease associated with a high risk of chronic complications and comorbidities. According t the World Health Organization, 16.7 million people worldwide die of cardiovascular diseases each year.
Aim of the Study: The aim of this study is to evaluate determinants of statin initiation among diabetic patients.
Methods: A hospital-based cross-sectional study was conducted to evaluate statin initiation and determinants in Gebre Tsadik Shewa General Hospital, Bonga, Ethiopia. This hospital covers a catchment population of about 1.4 million and offers diagnosis and treatment in outpatient and inpatient settings in different departments. Epi data 4.0.2.49 and STATA 14.2 were used for data entry and analysis. Before analysis, presence of co-linearity and model fitness were checked. Chi-square statistics were used to check adequacy of cells for binary logistic regression. Bivariate analysis was done and p < 0.25 was included in a multivariate model. Finally p-value less than 0.05 was considered a significant predictor.
Results: A total of 120 patients were included in this study, of which 77 (64.17%) were males. The mean age and standard deviation was 47.04 ± 12.13 years with 75% of patients ≥ 40 years. The mean duration of illness was 10.26 ± 0.6 years. Ninety-eight (81.67%) patients had varying comorbidities. Sixty-four (53.33%) patients developed complications. The majority of patients were evaluated by a general practitioner (GP). Fifty-one (42.5%) patients started statins. Of them, 31 (60.78%) started for secondary prevention. The majority of patients had atorvastatin with moderate dosage. Government insurance (p=0.029), polypharmacy (0.008), physician level of training (0.023) and previous counseling of patients about the importance of statins (p< 001) were significantly associated with initiation of statins.
Conclusion: Only near to 40% of patients started statins. Physician reluctance and unavailability of drugs were the most common reasons not to initiate statins. The hospital tries to provide medication. Physicians should evaluate patients in need of cardio-protective drugs.
Keywords: diabetes, statin initiation, determinants, primary prevention, secondary prevention, general hospital
Plain Language Summary
What is Known: The importance of statins as primary and secondary prevention of CVDs patients with DM.
What is Added: What the statin utilization pattern looks like and what factors negatively affect statin initiation.
Introduction
Diabetes mellitus (DM) is a chronic degenerative disease associated with a high risk of chronic complications (especially cardiac complications like atherosclerosis) and comorbidities.1 According to World Health Organization estimates, 16.7 million people worldwide die of cardiovascular diseases each year.2 Guideline recommended preventive measures can reduce cardiovascular disease (CVD) risk in adults with diabetes and CVD, yet the degree to which these high-risk adults are achieving guideline indicated secondary prevention interventions has been under-studied globally.3 The prevalence of cardiovascular (CV) risk factors continues to rise and globalization seems to have contributed to a higher prevalence in developing countries.4
The economic burden with hospitalizations and consultations were 22%, and costs related to the loss of productivity related to the disease were 15%. Health expenditures in Brazil are estimated at 9.5% of gross domestic product and the average cost of CVD was estimated at 0.7% of gross domestic product.5
CV risk reduction is critically important for the care of patients with diabetes, with or without known CVD and CV risk factors. Use of statins, aspirin, glucose-lowering therapies, and intensive lifestyle management are important to prevent CVD.6 Statins reduce the risk of CVD-associated morbidity and mortality through their lipid lowering, anti-inflammatory, plaque-stabilization and anti-thrombosis effects. Although statin therapy for patients with prior CV events is widely supported, use in patients without prior CV events is controversial.7 A case control study showed that statins use is also associated with reduced risk of hepato-cellular carcinoma development compared with non-users. The reduction in risk was significant in the presence and absence of DM.8
Although there are no nationwide data on CV burden in Ethiopia, DM and associated CV burden is high as evidenced by clinical practice. Studies show that statins prevent the occurrence and complications of CVD.9 However, in Ethiopia, statins use in diabetes patients is suboptimal.10 Therefore, there is an urgent need for evaluation of statin initiation and its determinants to prevent CVD. The aim of this study is to evaluate statin utilization patterns and determinant factors.
Method
Study Setting and Period
This study was done at Gebre Tsadik Shewa General Hospital, Bonga, Ethiopia. It is one of the governmentally established hospitals in Ethiopia. It covers a catchment population of about 1.4 million and offers diagnosis and treatment for nearby populations. In this hospital a total of 145 DM patients were on follow up. The hospital serves outpatient and inpatient settings in different departments. The study was conducted specifically at an outpatient department service which is a DM clinic, from November 1, 2019–December 22, 2019.
Study Design
Hospital-based cross-sectional study was used to evaluate statin initiation and contributing factors for statin initiation in general hospital of diabetic clinic.
Population and Sample Size Determination
All diabetes patients who have follow-up at this hospital were taken as the source population. Patients who had follow-up during the data collection period were treated as the sample population. Since the numbers of DM patients on follow-up were small (145), all subjects who fulfilled inclusion criteria were the subject of this study.
Inclusion and Exclusion Criteria
Inclusion criteria were confirmed cases of DM aged between 18 and 75 years, patients aged less than 40 years with suboptimal lipid profile (including TG>150 mg/dl, TC>200 mg/dl, and LDL >100 mg/dl) and patients with age greater than 40 years irrespective of lipid profile and who attended a follow-up DM clinic. Patients who had known heart failure class II–IV, patients unwilling to participate or on dialysis were excluded.
Study Variables
Statin initiation is the dependent variable, and sociodemographic, comorbidity, complication, duration of illness, number of comorbidities, number of complications, laboratory indices (lipid profile), type of statin, physician level of training and experience are independent variables.
Data Collection Tool and Procedures
Relevant patient data were collected via face to face interview and medical cards using a data abstracting form. The questionnaire included socio-demographic data, responsible physician for statin initiation (obtained from patient medical records) and clinical details (diabetes complications, comorbidities, duration of diabetes, laboratory values and statin medication profiles). The questionnaire was translated to the local language and retranslated to English for consistency. Data were collected by two pharmacists (B. Pharm) after one day of training. Supplementary information and clarifications on some patients’ medical information was obtained through discussion with respective nurses, physicians and care-givers. Statin initiation was dichotomized; patients who had statins and those who are not initiated based on the current guideline recommendations.11
Analysis
Data were entered using Epi data 4.0.2.49 and analyzed using STATA 14.2. Before data analysis, presence of colinearity between independent factors (having less than 2.5 variance inflation factor or all variables have tolerance greater than 0.77) and model fitness (with Hosmer–Lemeshow test p-value greater than 0.54 for binary logistic models) were checked.
Continuous variables/data were checked for the presence of deviation from normal distribution. All the data were normally distributed as evidenced with Shapiro–Wilk test, p >0.07. In all of the analyses, significance testing was conducted using two-sided p-values and 95% confidence intervals. Chi-square statistics were used to check adequacy of cells for binary logistic regression.
The association of independent predictors and statin initiation was evaluated using a multivariate binary logistic regression model. Finally, categorical variables are presented as percentages and continuous variables as means (standard deviations) or their 95% confidence intervals as appropriate. A p value < 0.05 was considered significant.
Results
Background Characteristics of Participants
One hundred and twenty patients fulfilled inclusion criteria and were included in this study, of which 77 (64.17%) were males. The mean age was 47.04 ± 12.13 years with 75% of patients ≥40 years. Eighty-six (71.67%) patients had type 2 DM and slightly more than half of the patients lived in an urban area. The mean duration of physician experience was 8.78 ± 2.67 years. Regarding educational status, 40 (33.33%) patients had attained secondary school and 37 patients were illiterate (30.83%). The majority of patients attended their appointment every two months and only 7 (5.83%) were currently smokers. Fifty-three (44.17%) patients consumed alcohol sometimes, especially during holidays. The majority of patients had no insurance coverage (Table 1). The mean total cholesterol and low density lipoprotein levels were 198 and 173.35 respectively (Table 2).
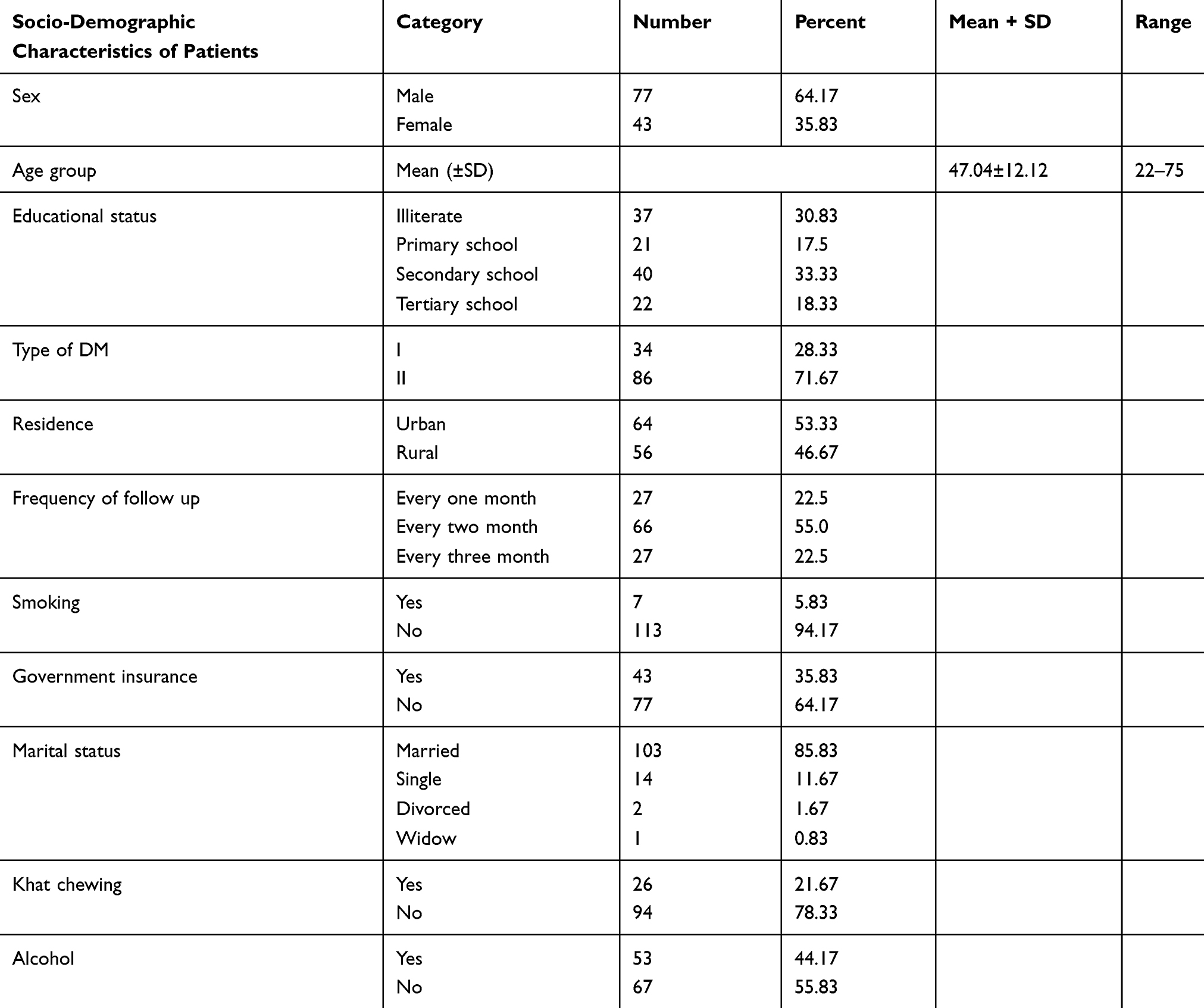 |
Table 1 Socio-Demographic Characteristics of Patients, in General Hospital, Ethiopia, 2020 |
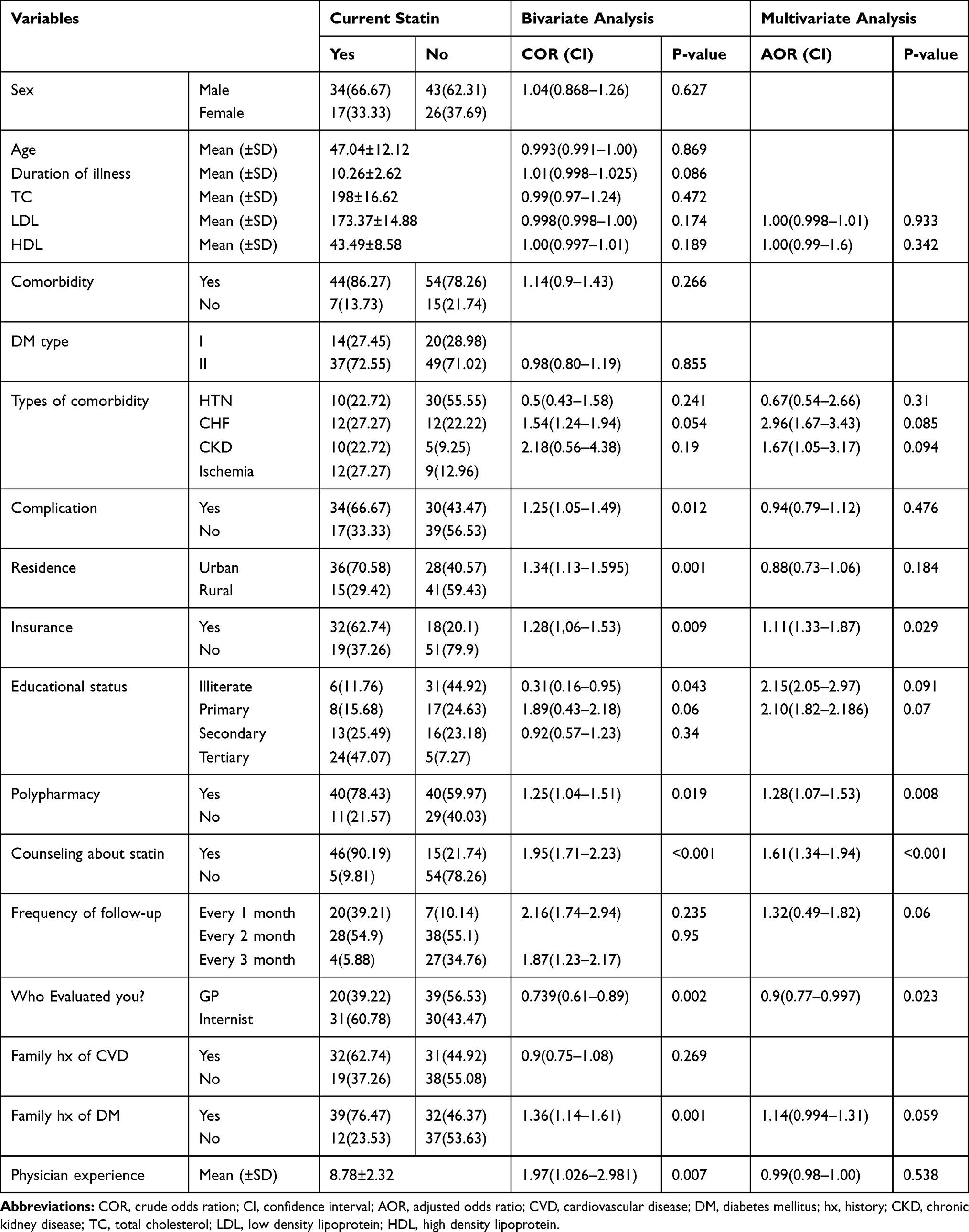 |
Table 2 Bivariate and Multivariate Binary Logistic Regression Analysis for Predictors of Statin Initiation, General Hospital, Ethiopia, 2020 |
Disease and Medication Related Characteristics
Patient mean duration of illness was 10.26 ± 0.6 years. Ninety-eight (81.67%) patients had comorbidities. Sixty-four (53.33%) patients developed complications and the majority of patients were evaluated by a general practitioner (GP). Fifty-one (42.5%) patients started on statins and 31 (60.78%) started for secondary prevention (treatment for complications). The majority of patients were put on atorvastatin with moderate dosage. Sixty-five patients developed medication side effects (obtained from patient medical record) in their life time (Table 3).
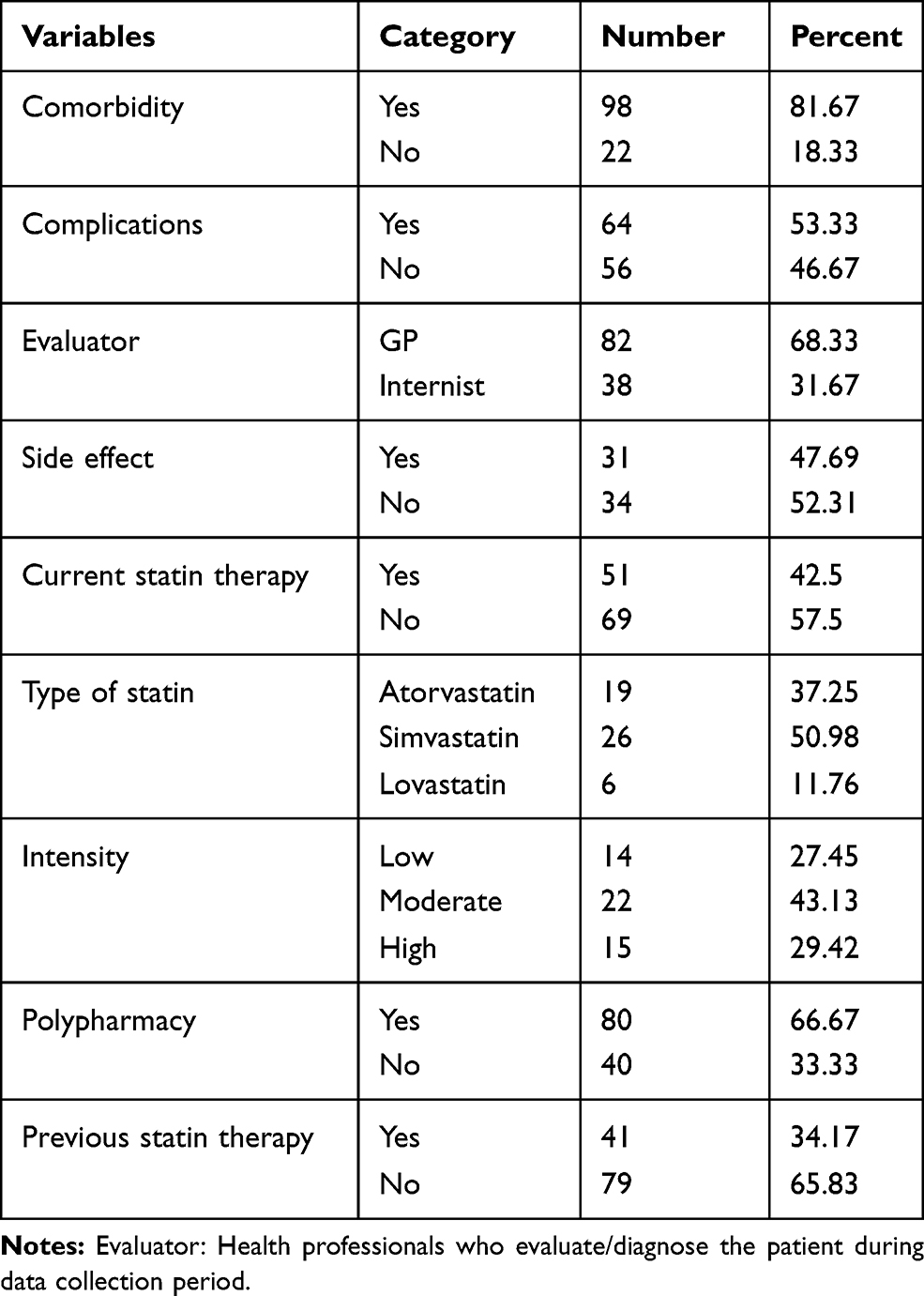 |
Table 3 Disease and Medication Related Characteristics of Patients, General Hospital, Ethiopia, 2020 |
As shown in Figure 1, 21 (30.43%) patients had not started statins because their physicians had not prescribed them, despite the patients being candidates for primary or secondary prevention, followed by 20 (28.99%) patients who had stopped taking statins due to unavailability of the drugs in the hospital.
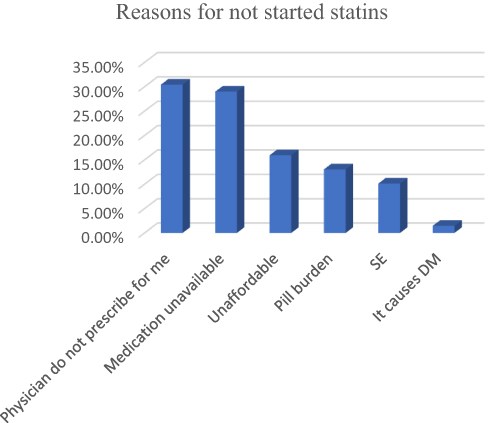 |
Figure 1 Reasons that the patient did not start statins, General hospital, Ethiopia, 2020. |
From the total of patients who were exposed to statins in previous or current therapy regimes, 13 (41.94%) reported right upper quadrant pain followed by muscular pains (12; 38.71%). The proportions of patients reporting nausea and vomiting (NV) and fatigue were similar and 55.0% patients were taking simvastatin (Figure 2). Ninety-eight patients had comorbidity in addition to DM, 40 (40.82%) had hypertension and 24 (24.49%) had congestive heart failure (Figure 3).
 |
Figure 2 Types of suspected SE the patient developed, General Hospital, Ethiopia, 2020. Abbreviations: RUQP, right upper quadrant pain, NV, nausea and vomiting. |
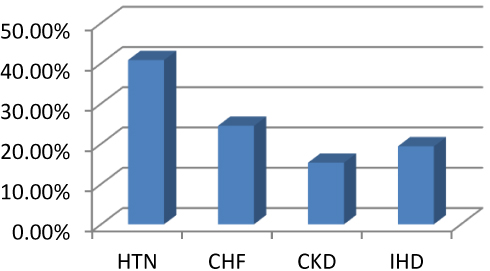 |
Figure 3 Types of comorbidity of participants in general hospital, Ethiopia, 2020. Abbreviations: HTN, hypertension; CHF, congestive heart failure; CKD, chronic kidney disease; IHD, ischemic heart disease. |
Statin Initiation
Only 51 (42.5%, 95% CI: 28.35–45.8) of the patients had started statins for primary or secondary prevention. Thirty-one (60.78%) patients had initiated statins for secondary prevention (treatment of CV complications) whereas 20 (39.22%) patients were treated for primary prevention of CV complication. Among patients who were on statins, 31 (60.78%) were evaluated by a medical internist. Thirty-two (62.74%) patients on statins had government insurance for their health service. Patient frequency of follow-up varied from every month to every three months. From the total of patients who were on statins, more than half (54.9%) patients visited their physician every two months. However, only 5.88% of participants followed their appointment every three months. Of the patients who were on statins, 34 (62.74%) and 39 (76.47%) had a family history of CVD and DM respectively and only 15 (29.41%) live in a rural area.
Bivariate analysis showed that statins were prescribed significantly more in patients who have a family history of DM compared with those who do not (COR=1.36, 95% CI: 1.14–1.61, p=0.001). Patients evaluated by a GP were less likely to be initiated with statins as compared with those evaluated by medical internists (COR=0.739, 95% CI: 0.61–0.89, p=0.002). Patients who had received counseling previously about the importance of statins were more likely to initiate statins as compared with those who had no previous counseling (COR=1.95, 95% CI: 1.71–2.23, p<0.001). In addition, government insurance was correlated with initiation of statins; patients under government insurance were more likely to be started on statins compared with those who had no government insurance (COR=1.28, 95CI: 1.06–1.53, p=0.009). Moreover, polypharmacy (COR=1.25, 95% CI: 1.04–1.51, p=0.019), presence of complications (COR=1.25, 95% CI: 1.05–1.49, p=0.012) and type of residence of the patient (COR=1.34, 95% CI: 1.13–1.59, p=0.001) were highly correlated with statin initiation (Table 2).
After adjusting confounding factors using multivariate binary logistic regression analysis, only four variables were significantly associated with statin initiation. Patients with government insurance were significantly associated with statin initiation as compared with those who had no insurance (AOR=1.11, 95% CI: 1.33–1.87, p=0.029). Statin initiation was significantly associated with patients having polypharmacy compared with those who had no multiple medications (≥3 medications) (AOR=1.28, 95% CI: 1.07–1.53, p=0.008). Previous counseling was significantly associated with statin initiation; patients who had received counseling about cardioprotective effects of statins were more likely to be associated with station initiation (AOR=1.61, 95% CI: 1.34–1.94, p<0.001). Moreover, patients who were evaluated by a GP were less likely to start statins compared with who were evaluated by a medical internist (AOR=0.9, 95% CI: 0.77–0.997, p=0.023) (Table 2).
Discussion
To our knowledge, no sufficient previous published research has explored initiation of statins and determinants for patients with DM in Ethiopia. This study describes the overall rate of statin initiation and associated factors among DM patients. The current study suggested that less than half of the patients (42.5%) were treated with statins. This is less than found previously in Ethiopia by Demoz et al.10 and from the USA12 in which 68.3% and 58.4% received moderate- to high-intensity statin therapy, respectively. This difference could be due to the availability of statins and the presence of a sufficient number of specialists in the previous study set up.
The majority of patients initiated statins for secondary prevention (i.e. for treatment of complication). Similar results were reported in Italy13 where statin use was higher for acute coronary syndrome than for patients having DM alone. This is also similar with the previous finding14 that less than 5% of the primary prevention and less than 30% of the secondary prevention population had received statins from healthcare providers.
More than half of the patients were evaluated by a GP. Patients evaluated with specialists were more likely to use statins as compared with those who were evaluated by a GP. Similar evidence has shown previously13 that patients evaluated with cardiologists were more likely to initiate statins as compared with others. As medical staff specialize, they become familiar with guidelines to optimize patient health and prevent unnecessary cost, complications associated with medications and promote the health status of patients.
The majority of patients had comorbidity with most of these patients suffering with hypertension. This result is the same as a previous study14 showing that the most common condition coexisting with type 2 diabetes is hypertension. The most commonly prescribed statins were simvastatin, atorvastatin and lovastatin. Moderate, high and low intensity doses of statins were prescribed more frequently respectively.
Different reasons were reported by patients as to why they did not start statins for prevention of cardiovascular complications. The first reason was physicians had not prescribed statins, followed by the unavailability of appropriate medication at the healthcare institution. Drug acquisition cost was another reason. Patients who had insurance coverage were more likely to be on statins as compared to with those who have no government insurance. Moreover, side-effects of medication was a reason that discouraged patients from starting statins, with the most common side-effects reported being right upper quadrant pain and rhabdomyolysis (a form of muscle toxicity involving muscle breakdown).
Regarding lipid profiles, levels of total cholesterol were ≥200 mg/dL in more than 50%, LDL ≥100 mg/dL in about 60.0%, triglycerides ≥150 mg/dL in 55.0%, and low HDL ≤ 40 for females in 36.67% and for males in 52.5%. However, in the current study, lipid profile was not significantly associated with the initiation of statins. This is not similar with a previous study done in India.17
Most of the patients’ TC, TG, LDL and HDL levels were beyond the standard. In our study, less than 40% of patients received high dosage statins. However, the American College of Cardiology/American Heart Association task force on practice guidelines recommended high dose statins in all patients with diabetes with age 40–75 or with suboptimal lipid profile.14 Anther review showed that diabetic patients between the age of 40–75 years and LDL-C > 70 mg/dL should be treated with a moderate-intensity statin.9,15–17 Although some patients were on moderate intensity statins, overall prescriptions of statins as well as high intensity statins were suboptimal and much lower than the guidelines. Evidence shows that patients who do not start or have low adherence with statin therapy were more likely at risk for CVD.21
Although, polypharmacy was one of the reasons for not initiating statins, patients on multiple medications were more likely to start statins compared with those on less than three drugs. This could be becausepatients taking multiple drugs were suffering with complications which should be treated with statins. A second reason could be that patients with polypharmacy received more attention from their physicians, who can counsel them about the drugs and evaluate their conditions thoroughly.
Patients having family history of DM, physician duration of experience, patient residence and presence of complications, were correlated with statin initiation. However, after controlling confounding factors using multivariate binary logistic regression, these variables were not statistically associated with initiation of statins. Patients having family history of CVD, duration of illness, comorbidity and type of comorbidity were not correlated with statin initiation.
In this study the majority of patients were males. However, sex difference had no significant impact on the initiation of statins. The current finding is not in line with previous reports11,12 that men with DM were prescribed statins more than women. The discrepancy could be explained if women the previous study had lower coronary artery disease incidence than men.
Limitation of the Study
This study was conducted in a single health institution and with a small sample size, so it is difficult to give inferences for the general population.
Conclusion
In conclusion, only near to 40% of patients started statins. The most common reasons not to initiate statins were physician reluctance to prescribe and unavailability of drugs in the health institution. Insurance, polypharmacy, counseling patients about importance of statins for cardiac disease prevention and physicians’ level of training were statically significant predictors for initiation of statins. The hospital tries to provide medication. Physicians should evaluate their patients’ need for cardioprotective drugs and counsel them on the importance of statins.
Data Sharing Statement
All data analyzed during this study are available for publication.
Ethics and Consent
The study was done in accordance with Helsinki declaration (October 2000). Ethical approval was obtained from institutional review board of college of health science, Mizan-Tepi University and sent to Bonga Hospital. Written letter was obtained from drug and therapeutics committee of Bonga Hospital to collect data from the patients. Verbal informed consent from respective physicians and nurses (working in the outpatient department) was secured to extract data from medical charts if necessary. Written informed consent has been given for every patient to participate. Privacy and confidentiality were ensured during patient interview and review of patient charts.
Acknowledgment
We are very grateful to the nursing staff for their cooperation in giving sufficient patient information. We would like to specially thank my study participants for their cooperation in participating in this study and all individuals who helped us formally or informally.
Author Contributions
Both authors played a significant role on the work submitted including in conception, methodology, data acquisition, data analysis, drafting and revising of articles. Finally, both authors agreed for submission as the current format to the journal has been submitted. In addition, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Marcellusi A, Viti R, Sciattella P, et al. Economic aspects in the management of diabetes in Italy. BMJ Open Diabeties Res Care. 2016;1–11.
2. American Heart Organization. Statistical fact sheet-populations international cardiovascular disease statistics. Am Hear Organ. 2004.
3. Pagidipati NJ, Navar AM, Pieper KS, et al. with type 2 diabetes: international insights from the TECOS trial. HHS Public Access. 2018;136(13):1193–1203.
4. Nowbar AN, Gitto M, Howard JP, Francis DP, Al-Lamee R. Mortality from ischemic heart disease. BMJ Open Diabetes Res Care. 2019;12(6):6. doi:10.1161/CIRCOUTCOMES.118.005375
5. de SE SA, De Siqueira-filho AG, Land MGP. Análise do impacto econômico das doenças cardiovasculares nos últimos cinco anos no brasil. Arq Bras Cardiol. 2017;109(1):39–46.
6. Shumer E, Norman P, Spack NJN. HHS Public Access. 2017;176(12):139–148.
7. Sources D, Selection S, Extraction D, Outcomes M. Statins for prevention of cardiovascular disease in adults. JAMA. 2016;(19):2008–2024.
8. Kim G, Jang SY, Nam CM, Kang ES. Statin use and the risk of hepatocellular carcinoma in patients at high risk: a nationwide nested case-control study. J Hepatol. 2018;68(3):476–484. doi:10.1016/j.jhep.2017.10.018.
9. Li M, Wang X, Li X, et al. Statins for the primary prevention of coronary heart disease. Biomed Res Int. 2019;2019.
10. Demoz GT, Wahdey S, Kasahun GG, et al. Prescribing pattern of statins for primary prevention of cardiovascular diseases in patients with type 2 diabetes: insights from Ethiopia. BMC Res Notes. 2019;12:1–7. doi:10.1186/s13104-019-4423-9;.
11. Arnett DK, Blumenthal RS, Albert MA, et al. ACC/AHA guideline on the primary prevention of cardiovascular disease 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease. Am Coll Cardiol. 2019;2019.
12. Yashashwi Pokharel JM, Akeroyd DJ, Ramsey RS, et al. Statin use and its facility-level variation in patients with diabetes: insight from the veterans affairs national database. Clin Cardiol. 2016;39(4):185–191. doi:10.1002/clc.22503
13. Arca M, Ansell D, Averna M, et al. Statin utilization and lipid goal attainment in high or very-high cardiovascular risk patients: insights from Italian general practice. Atherosclerosis. 2018;271:120–127. doi:10.1016/j.atherosclerosis.2018.02.024
14. Brown F, Singer A, Katz A, Brown F, Singer A. Statin-prescribing trends for primary and secondary prevention of cardiovascular disease recherche tendances actuelles dans la prescription des statines en prévention primaire et secondaire des maladies cardiovasculaires. Can Fam Physician. 2017;63:495–503.
15. Zhang H, Plutzky J, Shubina M, Turchin A. Risk factors for lack of statin therapy in patients with diabetes and coronary artery disease. J Clin Lipidol. 2016;10(6):1406–1413. doi:10.1016/j.jacl.2016.09.010.
16. Stone NJ, Robinson JG, Lichtenstein AH, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiolo. Circulationation. 2014;129(25 suppl 2):S1–45. doi:10.1161/01.cir.0000437738.63853.7a
17. Gupta R, Lodha S, Sharma KK, et al. Evaluation of statin prescriptions in type 2 diabetes: India heart watch-2. BMJ Open Diabetes Res Care. 2016;4(1):1–7. doi:10.1136/bmjdrc-2016-000275
18. Khalil S, Khayyat S, Al-khadra Y, et al. Expert review of cardiovascular therapy should all diabetic patients take statin therapy regardless of serum cholesterol level ? Should all diabetic patients take statin therapy regardless of serum cholesterol. Expert Rev Cardiovasc Ther. 2019;17(4):237–239. doi:10.1080/14779072.2019.1590198
19. Subedi BH, Michael G, Minder CM, et al. The role of statins in diabetes treatment. Diabetes Spectr. 2013;26(3):3. doi:10.2337/diaspect.26.3.156
20. Dixon BDL, Pharm D, Cardiology B, et al. Primary prevention of cardiovascular disease. Prim Prev Cardiovasc Dis. 2018.
21. Mph AP, Eli J, Mha A, Fund N, Ma AC, Fesc MM. Statin therapy: diabetes mellitus risk and cardiovascular benefit in primary prevention. IMAJ. 2018;20:480–485.
22. Khan NNS, Kelly-blake K, Luo Z, Olomu A. Sex differences in statin prescribing in diabetic and heart disease patients in FQHCs: a comparison of the ATPIII and 2013 ACC/AHA cholesterol guidelines. Heal Serv Res Manag Epidemiol. 2019;6:1–8.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.