")
Back to Journals » International Journal of Women's Health » Volume 13
Determinants of Premature Rupture of Membranes Among Pregnant Women Admitted to Public Hospitals in Southern Ethiopia, 2020: A Hospital-Based Case–Control Study
Authors Habte A , Dessu S , Lukas K
Received 8 April 2021
Accepted for publication 13 June 2021
Published 22 June 2021 Volume 2021:13 Pages 613—626
DOI https://doi.org/10.2147/IJWH.S314780
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Aklilu Habte,1 Samuel Dessu,2 Kaleegziabher Lukas3
1Department of Reproductive Health, School of Public Health, College of Medicine and Health Sciences, Wachemo University, Hosanna, Southern Ethiopia; 2Department of Public Health, College of Medicine and Health Sciences, Wolkite University, Wolkite, Southern Ethiopia; 3Department of Epidemiology, School of Public Health, College of Medicine and Health Sciences, Wachemo University, Hosanna, Ethiopia
Correspondence: Aklilu Habte Tel +251912744786
Email [email protected]
Background: A gush of amniotic fluid any time before the onset of labor is known as premature rupture of the membranes (PROM). Its consequences vary from maternal and neonatal mortality and morbidity to country-wide economic loss. At the national level in general, and in the study area in particular, little is known about PROM and its determinants. Hence, this study aimed at identifying determinants of PROM among pregnant women admitted to public hospitals in Southern Ethiopia, 2020.
Methods and Materials: A hospital-based unmatched case–control study was conducted on 279 pregnant women (93 cases and 186 controls) admitted to public hospitals from October 1 to 30, 2020. Pregnant women admitted to maternity wards of selected hospitals with a painless gush of fluid spilling out from the vaginal canal were considered as cases. Interviewer-administered questionnaires and data abstraction tools were used to collect data. The data were coded and entered into Epi-Data version 3.1 and exported to SPSS version 23 for analysis. The determinants of PROM were identified by applying a multivariable logistic regression analysis at a p-value < 0.05.
Results: Term PROM accounted for the majority, 55 (59.2%) of cases. Previous history of abortion (AOR: 4.14, 95% CI: 2.21– 9.07), lack of ANC (AOR: 3.51; 95% CI: 1.33– 8.27), previous history of PROM (AOR: 4.91; 95% CI: 2.23– 9.82), caesarean delivery (AOR: 3.02, 95% CI: 1.24– 6,40), using of a maternal waiting room (MWR) (AOR: 0.33, 95% CI: 0.15– 0.74), and mid-upper arm Circumference (MAUC) < 23cm (AOR: 3.69, 95% CI: 1.58– 8.64) were identified as significant determinants of PROM.
Conclusion: Health-care providers should work on providing adequate ANC by tracing mothers who have not received it and advising pregnant women to use MWR in the final weeks of their pregnancy. Furthermore, maternal and child health care units must place a strong focus on screening and managing the nutritional status of pregnant women. Furthermore, women with a history of abortion, caesarean section, and PROM need due attention from health care providers to mitigate the occurrence of PROM.
Keywords: PROM, determinants, case-control, public hospitals, Ethiopia
Background
A fluid-filled sac called the bag of water or amniotic fluid covers the developing baby.1 Amniotic fluid is usually produced continuously, but after about 16 weeks of pregnancy, fetal urine production takes over. It defends against infection, fetal trauma, and compression of the umbilical cord. Compression of the umbilical cord and reduced placental blood flow may occur when amniotic fluid is low or absent.1,2
Deliveries before 37 weeks of gestation (or preterm deliveries) are a global health concern, as per the World Health Organization (WHO).1,3 Premature Rupture of Membrane (PROM) is a painless gush of amniotic fluid any time before the onset of labor from the vaginal canal with or without a decrease in the size of the uterus.4 It is supported by a basic pH test of vaginal fluid or ferning of dried vaginal fluid detected under microscopic evaluation and a decrease in amniotic fluid volume (AFV) of <5cm during an ultrasound examination.5 Preterm premature rupture of membranes (PPROM) refers to PROM that occurs before 37 weeks of pregnancy, while term premature rupture of membranes refers to PROM that occurs after 37 weeks of pregnancy.1,2,4 In Ethiopia, it is defined as a gush of amniotic fluid before the onset of labor in the period after 28 weeks of pregnancy (after fetal viability), since the rupture of the membrane before the 28th week of pregnancy is considered an automatic abortion.6
PROM affects about 5% to 10% of all births, while PPROM affects about 3%. Around 70% of PROM cases occur in full-term pregnancies, but in referral centers, more than 50% of cases may occur in preterm pregnancies.7–9 According to studies, PROM raises perinatal mortality by four times and neonatal morbidity by three times.10
Premature rupture of membranes is the common complication of pregnancy which is an important cause for perinatal and maternal morbidity and mortality. The consequences of PROM vary from maternal and neonatal mortality and morbidity to countrywide economic loss due to medication cost, hospital admission, absences from the job, and cost to the health professionals.11–13 PROM complicates 3–8% of births and leads to one-third of prematurity and 90% of deaths.13,14 Intraventricular hemorrhage, neonatal sepsis, and respiratory distress syndrome are neonatal complications due to prematurity that account for the majority of neonatal deaths.13–17 It also triggers significant maternal complications including puerperal infections, disseminated intravascular coagulopathy (DIC), placental abruption, surgical delivery, chorioamnionitis, and mental and breastfeeding issues.18,19 The longer the time between rupture and delivery, the higher the risk of maternal and fetal morbidity, as well as a higher risk of maternal, fetal, and fetal mortality.20
PROM was found to be 13.8% in rural Uganda21 and 1.94% in rural Nigeria,20 according to studies. According to hospital-based studies conducted in Northern and Western Ethiopia, the magnitude of PROM was found to be 13.7% and 13.4%, respectively.22,23
Since the purpose of PROM management is to prolong pregnancy, the most typical management scheme for pregnant women with a gestational age of fewer than 36 weeks is expectant, which involves admitting the patient to the hospital and monitoring for signs of sickness, fetal distress, or labor to allow the fetus enough time to grow and mature.24–26 The specific cause of PROM is unspecified. Different studies indicated that bad past pregnancy outcomes, uterine overdistention, smoking, low BMI, genitourinary tract infection, poor diet, and assisted fertility are the major contributing factors for PROM.27–29
It is hard to understate the significance of identifying and understanding the determinants of PROM for the pregnancy’s future outcome. A missed opportunity for effective intervention may result from a late diagnosis.10,30 To the best of the investigators’ knowledge and based on a review of the literature, very little is known about PROM and its determinants at the national level, with no study specifically undertaken in the current study area. Identifying and intervening on the determinants can help to prevent PROM from occurring in the future, reducing maternal and newborn complications. The findings could potentially be used as a roadmap for improving maternal and newborn health in the study area, resulting in a reduction in maternal and neonatal mortality across the country and the continent. Hence, this study aimed at identifying the determinants of PROM among pregnant women admitted to public hospitals in the Guraghe zone, southern Ethiopia.
Methods and Materials
Study Settings, Design, and Period
A hospital-based unmatched case-control study was conducted in public Hospitals of Guraghe Zone, Southern Ethiopia from October 1–30, 2020. The zone is situated 158 kilometers south of Addis Ababa, Ethiopia’s capital city, and 337 kilometers south of Hawassa (capital of southern Ethiopia region). The total population of the zone in the fiscal year 2020 was 1,835,110, with 19.84% of women in the reproductive age group (15–49 years old) and 63,495 expected live births. There are 527 health facilities, comprising 74 clinics, 9 hospitals, and 444 health posts.
The Population of the Study
The source population were all mothers with a gestational age of more than 28 weeks and admitted to labor, maternity, and high-risk wards of public hospitals in the zone. The study populations for cases were selected women who were admitted to labor, maternity, and high-risk wards of selected hospitals with a painless gush of fluid that spills out of the vagina and a shift in color or a decrease in the size of the uterus. The study population for controls were those selected pregnant mothers with a gestational age of more than 28 weeks and admitted to the same wards of the selected hospitals without any of the above signs during the study period. Those mothers who were initially assigned to the control group but later switched to the case group were excluded from the study. Participants with a gestational age of fewer than 28 weeks, as well as those who were seriously ill during the data collection period, were excluded.
Sample Size Determination
The sample size was determined using the StatCalc menu of Epi Info version 7 statistical software for an unmatched case-control study. The following assumptions were used: a 95% confidence level, an 80% power, a case-to-control ratio of 1:2, a percent of exposure among controls exposed (proportion of CS among women without PROM), and a percent of exposure among cases (proportion of CS among women with PROM). The percent of cases exposed for CS (16.2%) and percent of controls exposed for CS (4.4%) was taken from a study conducted in northern Ethiopia.28 Based on the above assumptions, the sample size was 252 (84 cases and 168 controls), and after adding for a 10% nonresponse rate, the final sample size for the study was 279 (93 cases and 186 controls).
Sampling Techniques
Of the nine, five public hospitals in the zone were selected by lottery method namely: Butajira Teaching and Referral Hospital, Wolkite Teaching and Referral Hospital, Buie General Hospital, Quante General Hospital, and Atat Saint Lurd Referral Hospital. Obstetric case management reports and registration books were observed over the last three months before the data collection period to assess the obstetric client/patient flow rate of the respective hospitals. The sample size was proportionally allocated amongst these selected hospitals based on their case-flow over the previous three months as follows: Butajira Teaching and Referral Hospital (23 cases and 46 controls), Atat Saint Lurd Referral Hospital (32 cases and 64 controls), Wolkite Teaching and Referral Hospital (25 cases and 50 controls), Buie General Hospital (7 cases and 14 controls), and Quante General Hospital (6 cases and 12 controls). Cases were recruited consecutively until the calculated sample size was achieved. A systematic sampling method was used to select and interview two controls for each case. The interval (K) was calculated by dividing the average number of controls who visited each hospital in the previous three months by the proportionally allocated control sample size.
Data Collection Tools, Methods, and Personnel
A standardized, structured, interviewer-administered questionnaire comprising socio-demographic variables, obstetric conditions, maternal health service-related characteristics, and medical condition was developed after reviewing literature in the area of interest.2,10,28,31 The data were collected by five trained BSc Midwives with experience in data collection, under the supervision of three public health officers, through face-to-face interviews. A tool adapted from the Ethiopian Demographic and Health Survey 2016 Report was used to assess the socioeconomic status of households.32 Medical and obstetric data that could not be accessed by interviews, such as gestational age, diagnosis of PROM, urinary tract infections, STIs, anemia, and hypertensive disorders of pregnancy, were collected from patient medical records and charts. The mothers’ middle upper arm circumference (MUAC) was measured using non-elastic, non-stretchable MUAC tapes placed at the midpoint between the tips of the left arm’s shoulder and elbow, and the measurement was taken to the nearest 0.1Centimeters.
Data Quality Management
Initially, the data collection questionnaire is prepared in English and then translated into the local language by an expert in that language. It was then back-translated into English to ensure consistency with the original meanings. About data collection methods and instruments, both data collectors and supervisors provided one-day training. A pre-test was conducted in Woliso Christian Hospital one week before the actual data collection for 5% of the sample size (5 cases and 10 controls). The reliability of the questionnaires was assessed and the reliability index for practical questions (Cronbach’s alpha), which was 0.79. Based on the pre-test result, all relevant corrections were made. Every day, after data collection, the supervisors and principal investigator checked and verified each questionnaire for completeness and supplemented it with feedback.
Data Analysis
The data entered and coded into EpiData Version 3.1 was exported to SPSS version 23 for analysis. Univariate analyses such as frequency, proportion, mean, and standard deviation were computed for both cases and controls. The Chi-square test was conducted to test the statistical significance between dependent and independent variables. The wealth status of each household was evaluated using principal component analysis (PCA). There were a total of 28 items used in the beginning. Kaiser-Meyer- Olkin’s (KMO) sampling adequacy measure (≥0.6), Bartlett’s Sphericity test (p-value<0.05), and anti-image correlations (>0.4) have all been used to ensure that PCA’s assumptions were met. At each step, variables with communalities less than 0.5 and complex structures (correlations greater than 0.4 in more than one component) were removed until the iterations met the requirements. Finally, three components were derived from the PCA that accounted for 68.9% of the overall variance and were used to divide study participants’ household wealth into quintiles.
The proportion of cases and controls between selected categorical variables was compared using the Chi-square test. Bivariable and multivariable logistic regression analyses have been used to identify the determinants of PROM. The strength of the association was measured using an odds ratio with a 95% confidence interval. A bivariable logistic regression model was used to determine the relationship between each independent variable and the dependent variable. To manage confounding factors and see the independent predictors of PROM, variables with a P-value of 0.25 in bivariate logistic regression were exported to a multivariable logistic regression model. The adjusted odds ratio with a 95% confidence interval was used to report the association between the outcome and explanatory variables, and the statistical significance was declared at a p-value of 0.05. Model fitness was measured using the Hosmer and Lemeshow goodness of fit measures, as well as the Nagelkerke R Square, which were 0.64 and 0.58, respectively. The variance inflation factor (VIF>10) was used to test for multicollinearity between the explanatory variables.
Measurement of Variables of the Study
Outcome Variable
Premature rupture of membrane (PROM): the dependent variable, was confirmed by sterile speculum examination and clinical features (painless gush of fluid that spills out of the vagina and a shift in color or a decrease in the size of the uterus).1,2,4,28 A basic pH test of vaginal fluid or ferning of dried vaginal fluid detected under microscopic evaluation and decrease in amniotic fluid volume (AFV) of <5cm during ultrasound examination also supported the diagnosis.5,22 Cases comprised mothers with gestational age 28 weeks and above who were admitted to the labor, Maternity, and high-risk ward and had PROM before the onset of labor, as diagnosed by general practitioners (GPs), gynecologists, or residents. Controls, on the other hand, were pregnant mothers of gestational age >28 weeks who were admitted to those wards and had no rupture of membranes before the onset of labor.
Explanatory Variables
Poor nutritional status: A mother with a Mid Upper Arm Circumference (MUAC) <23 cm.22
Anemia: A pregnant woman whose Haemoglobin level <11 gm/dl was considered as an anemic.
Heavy weight lifting during pregnancy: is considered when a woman lifts 26 lbs (12Kg) infrequently (less than once every 5 minutes), less than an hour of repetitive lifting of 22lbs (10Kg) a day, and more than 1 hour of repetitive lifting of 13 lbs (6kg) a day after 28 weeks of the current pregnancy.2
An adequate sleeping hour during pregnancy: when a woman can sleep more than 8 hours per day.28
Maternal waiting room (MWR): A home or residential facility near a hospital or a health center that offers emergency obstetric care (EmOC) with skilled birth attendants to women who are far from facilities and stayed there in their final weeks of pregnancy.33,34
MWR utilization: In this study, a woman was deemed an MWR user if she stayed in any of the maternal waiting rooms in hospitals before the onset of labor, whether she was near term or at term, and regardless of how long she stayed at home during the current pregnancy.33,35
Results
Socio-Demographic Characteristics of the Respondents
A total of 279 respondents were enrolled in the study (93 cases and 186 controls), with a 100% response rate. The cases and controls had mean (SD) ages of 29.81 (±5.48) and 29.56 (±4.75) years, respectively. The majority of cases (63.4%) and controls (83.3%) were between the age group 20–34 years. Over half of the cases (52.7%) were from rural communities, while the majority of the controls (63.4%) were from urban areas. In terms of educational status, almost half of the cases, 46 (49.5%), and 65 (34.9%) of controls have no formal education. The difference in educational level between cases and controls was statistically significant, according to the Chi-square test. In contrast to controls (15.0%), a relatively high proportion of cases (29.0%) were in the lowest wealth quintiles (Table 1).
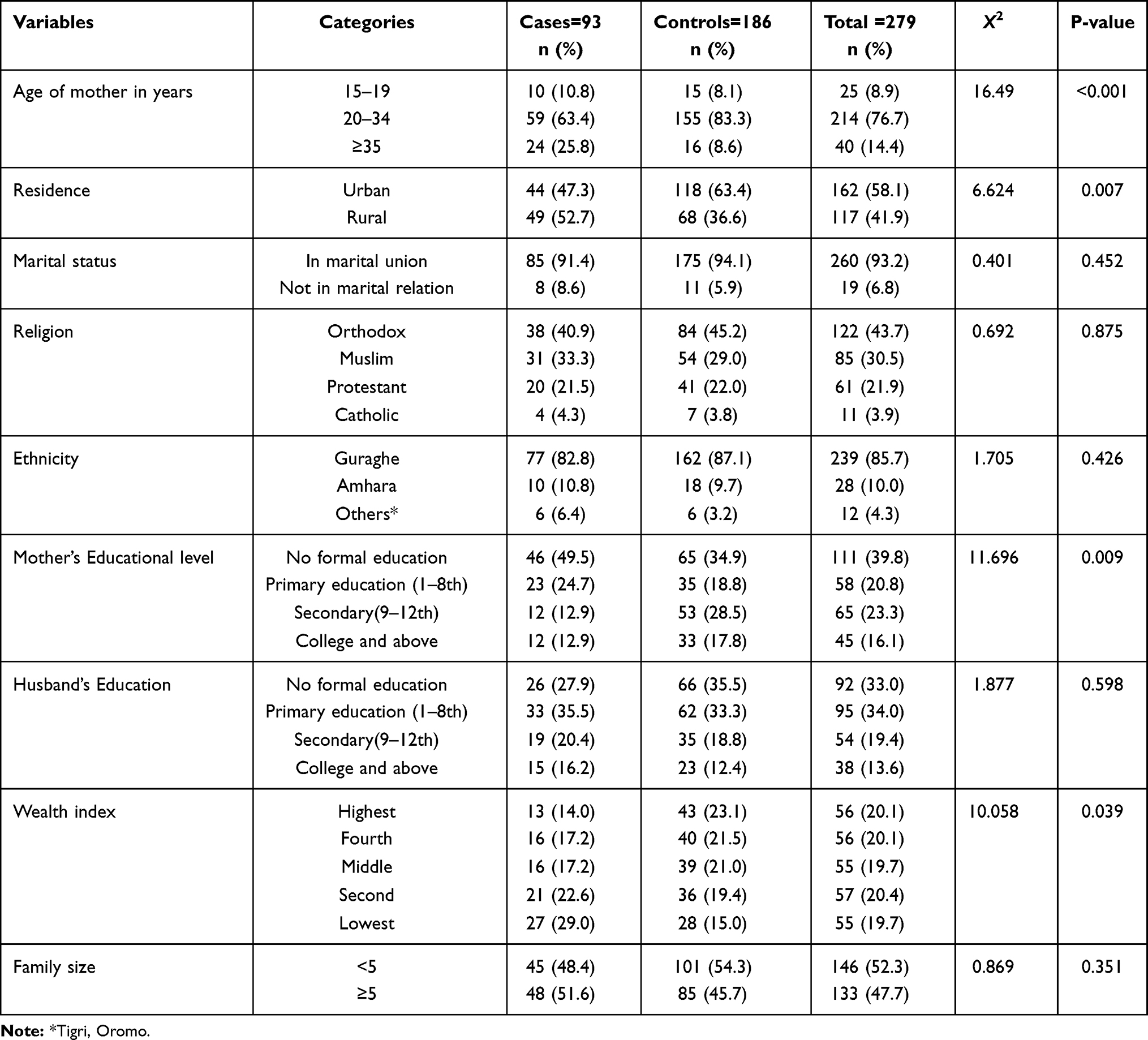 |
Table 1 Socio-Demographic and Economic Characteristics of Respondents Admitted to Public Hospitals in Guraghe Zone, Southern Ethiopia, 2020 |
Obstetric Characteristics of Respondents
Between cases and controls, there was no substantial difference in the proportions of Primigravida and Nulliparous respondents. The majority of cases, 43 (46.2%), and controls, 101 (54.4%), were multiparas, with 2–4 living children. Both cases and controls had experienced a comparable number of five or more pregnancies, 35.5%, and 32.3%, respectively. Twenty-seven (29.1%) cases and 21 (11.3%) controls had at least one previous history of abortion, with spontaneous abortion accounting for the most common type of abortion, in 21 (77.8%) of cases and 13 (61.9%) of controls. About a quarter of cases (25.6%) and one-tenth of controls (19.2%) have had at least one cesarean delivery. A prior history of PROM was reported in 35 (37.6%) of the cases and 20 (10.8%) of the controls (Table 2).
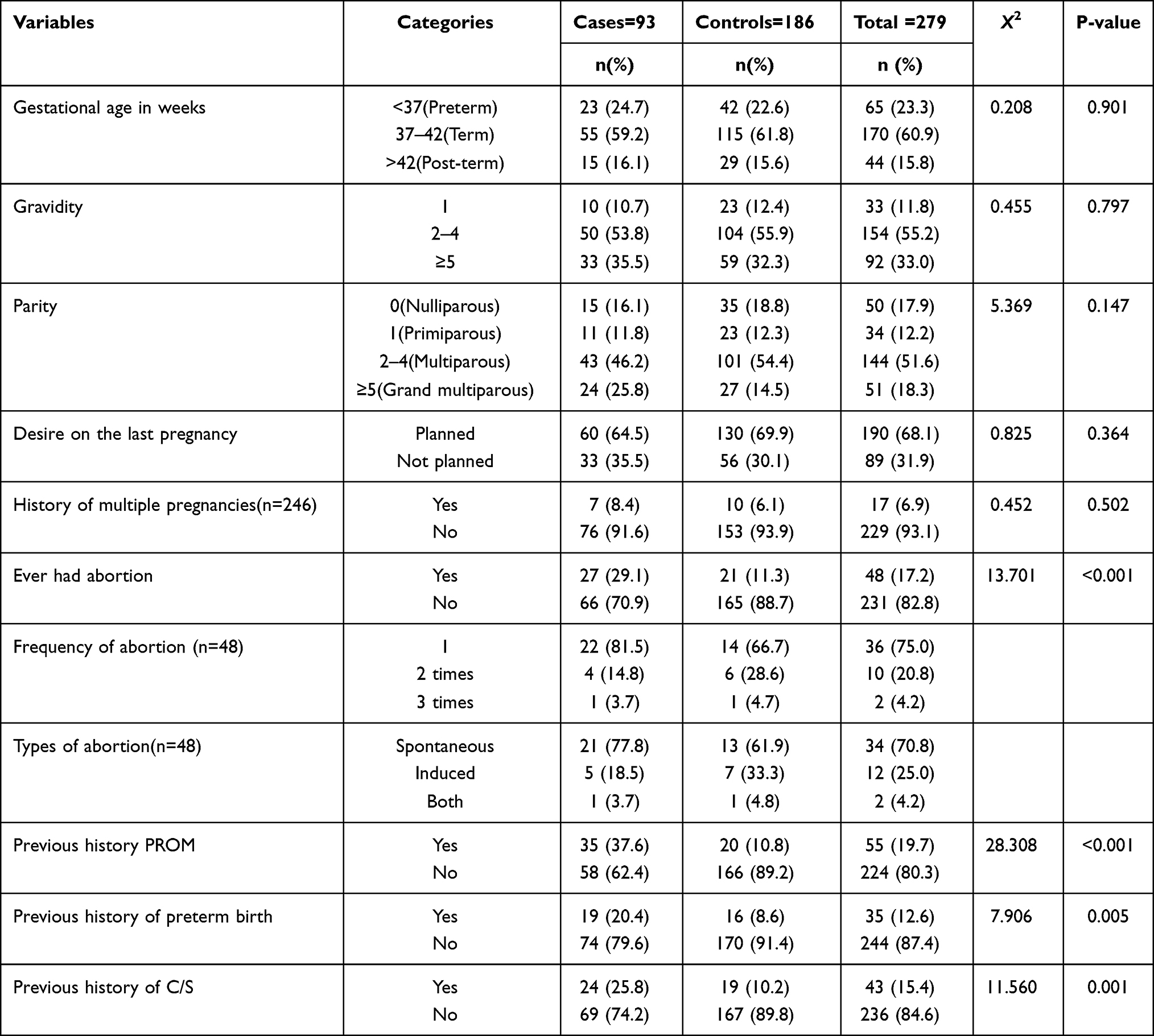 |
Table 2 Obstetric Characteristics of Respondents Admitted to Public Hospitals in Guraghe Zone, Southern Ethiopia, 2020 |
Maternal Health Service-Related Characteristics
The proportion of cases without ANC was double that of controls, at 26 (27.9%) and 26 (14.0%), respectively. A comparable proportion of cases, 56 (60.2%), and 119 (59.7%) of controls utilized modern contraceptives, in which injectables were the most common method-mix used by 19 (33.9%) and 49 (44.2%) of cases and controls, respectively. A few respondents in both cases (5.4%) and controls (5.7%) had previously undergone cervical cerclage. Fifty (53.8%) of cases and 102 (54.8%) of controls reached a health facility after traveling a distance that takes one hour and more (Table 3).
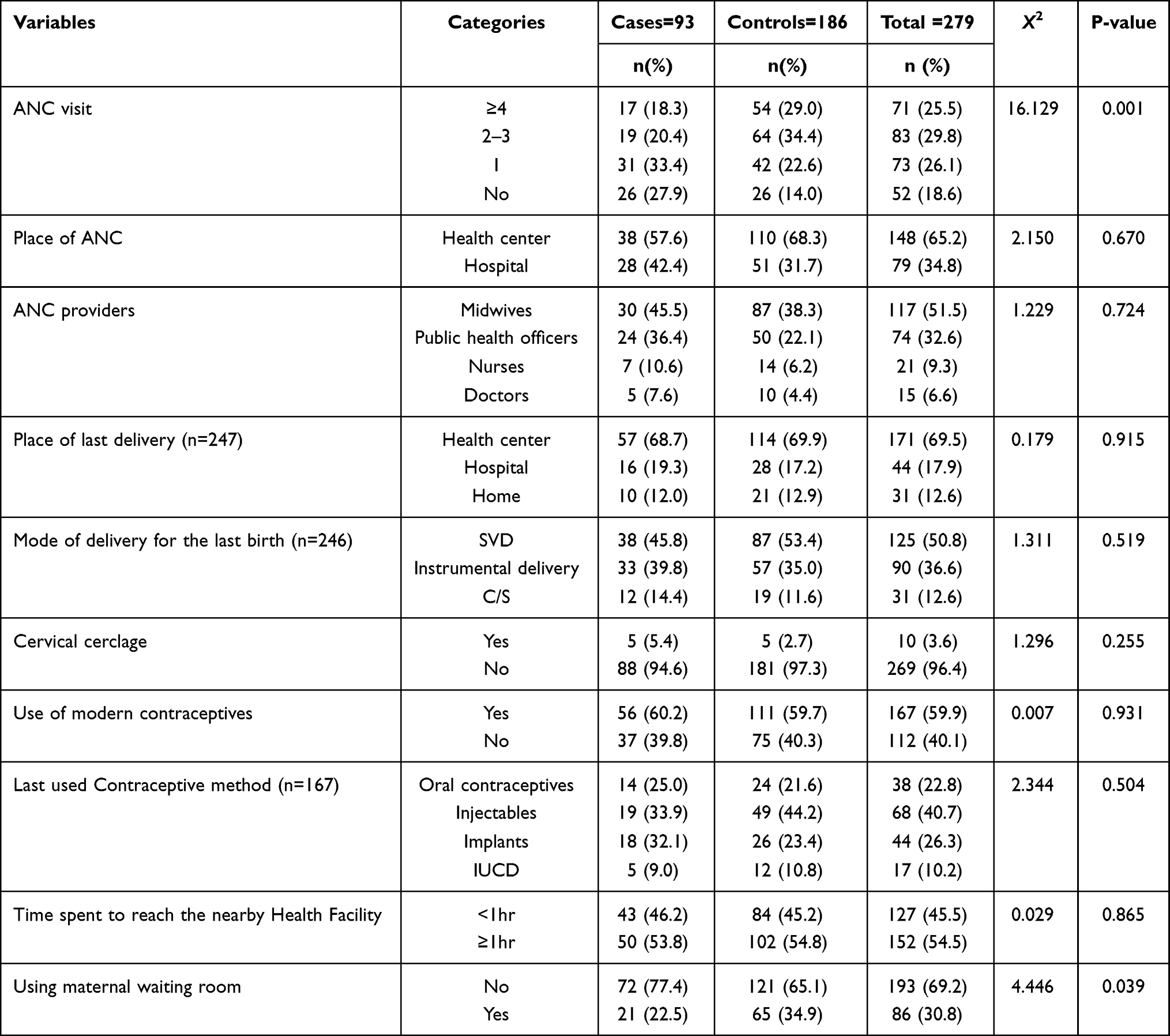 |
Table 3 Maternal Health Service-Related Characteristics of Respondents Admitted to Public Hospitals in Guraghe Zone, Southern Ethiopia, 2020 |
Clinical and Medical Conditions of the Respondents
A large difference was observed in the mid-upper arm circumference (MUAC) measurement, in which 29 (31.2%) of cases and 18 (9.7%) of controls measuring less than 23 cm. About a fifth (20.4%) of cases and 22 (11.8%) of controls reported abnormal vaginal discharge during the current pregnancy and a limited number of cases (5.4%) and controls (3.2%) were diagnosed with a genital ulcer (Table 4).
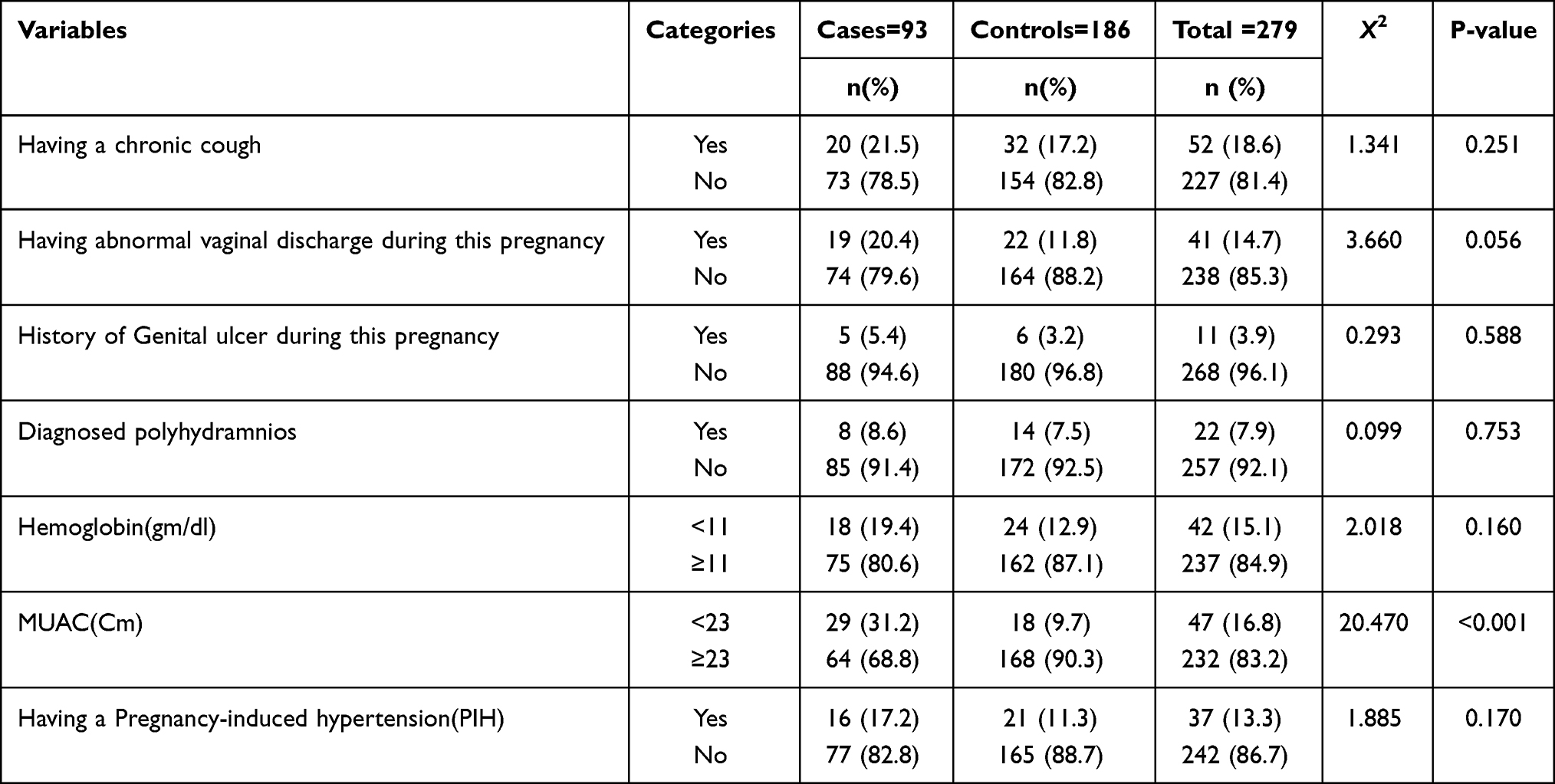 |
Table 4 Clinical and Medical Conditions of Respondents Admitted to Public Hospitals in Guraghe Zone, Southern Ethiopia, 2020 |
Risky Physical Activities and Habits Among Respondents
Twenty-one (22.6%) and twenty-one (11.3%) of the incidents and controls, respectively, had a history of falling down injuries. In both cases and controls, the number of smokers was low. Only 18.3% of cases and 15.0% of controls had intercourse during the third trimester. The majority of cases and controls have no history of chronic cough, lifting heavy objects, and alcohol consumption. A significant number of cases, 25 (26.9%) and controls, 54 (29.1%) of reported sleeping fewer than eight hours per day (Table 5).
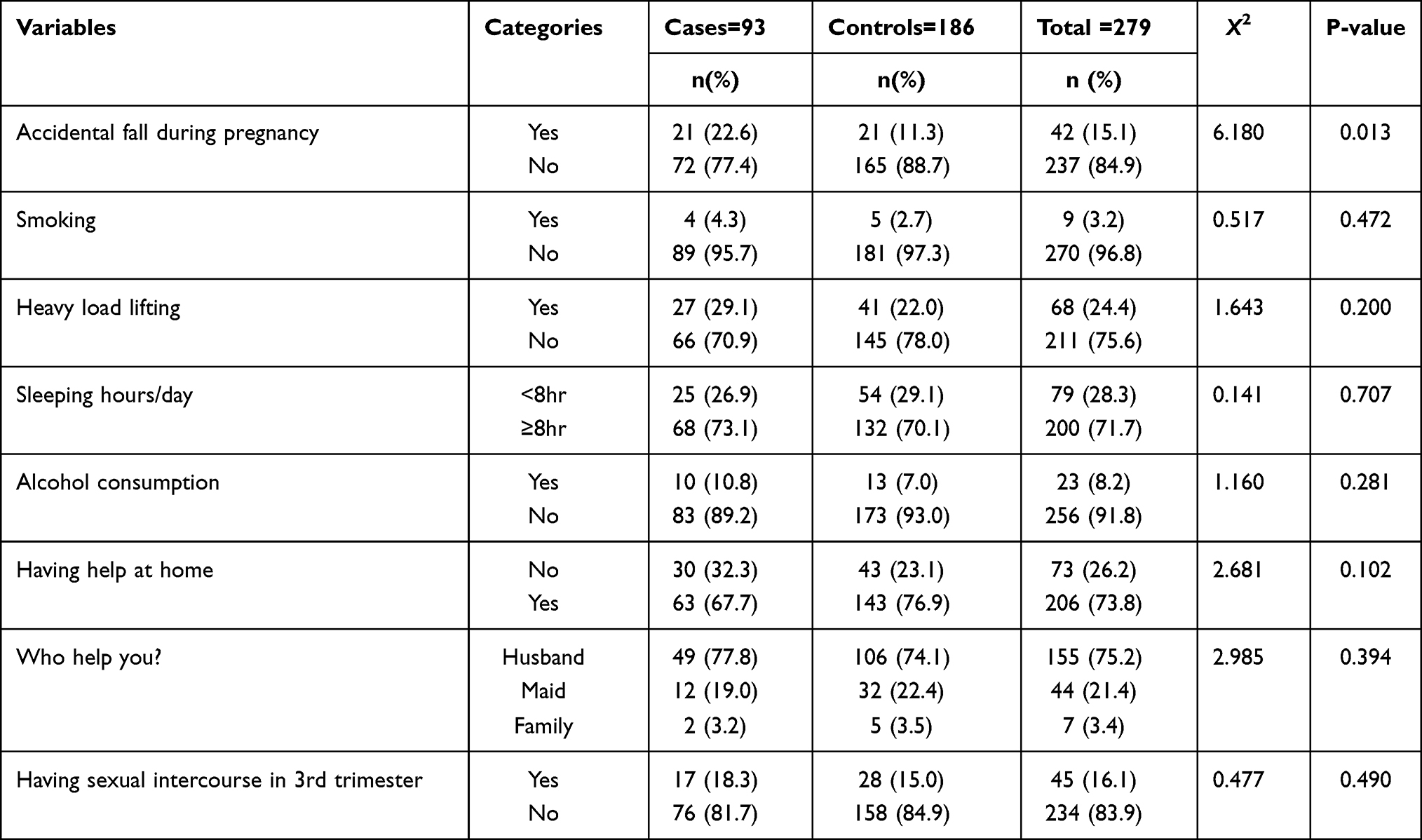 |
Table 5 Risky Physical Activities and Habits Among Respondents Admitted to Public Hospitals in Guraghe Zone, Southern Ethiopia, 2020 |
Premature Rupture of Membrane (PROM)
Of the 93 cases of PROM Term, pre-term, and post-term PROM accounted for 55 (59.2%), 23 (24.7%), and 15 (16.1%), respectively.
Determinants of Premature Rupture of Membranes (PROM)
Out of 13 variables that were eligible for multivariable logistic regression, six variables, namely lack of ANC, previous history of abortion, previous history of PROM, caesarean delivery, maternal waiting room (MWR) utilization, and MAUC<23cm, were identified as significant determinants of PROM.
As a result, abortion history was found to be a significant predictor of PROM. The likelihood of becoming a PROM case was 4.1 times higher among those respondents with a prior history of abortion than those who had not [AOR= 4.14; 95% CI: 1.7, 9.07]. Respondents who previously experienced a cesarean delivery had 3 times higher chance of becoming a PROM case than their counterparts [AOR= 3.02; 95% CI: 1.32, 6.40]. Lack of ANC was also identified as a risk factor for PROM in the current study. Those mothers with no ANC were 3.5 times more likely to develop a PROM than those respondents who got adequate ANC of 4 and more visits [AOR= 3.51; 95% CI: 1.39, 8.27]. Furthermore, women with a prior history of PROM had a 4.9-fold higher risk of developing PROM than their counterparts [AOR= 4.91; 95% CI: 2.23, 9.82]. When comparing respondents with MUAC ≥23cm, those with MUAC <23cm were almost 3.7 times more likely to sustain PROM [AOR= 3.69; 95% CI: 1.65, 8.64]. During pregnancy, the use of the maternal waiting room (MWR) was found to be a major predictor of PROM. Women who stayed in the maternal waiting room during their current pregnancy were 67% less likely than their counterparts to get a PROM case [AOR= 0.33; 95% CI: 0.15, 0.74] (Table 6).
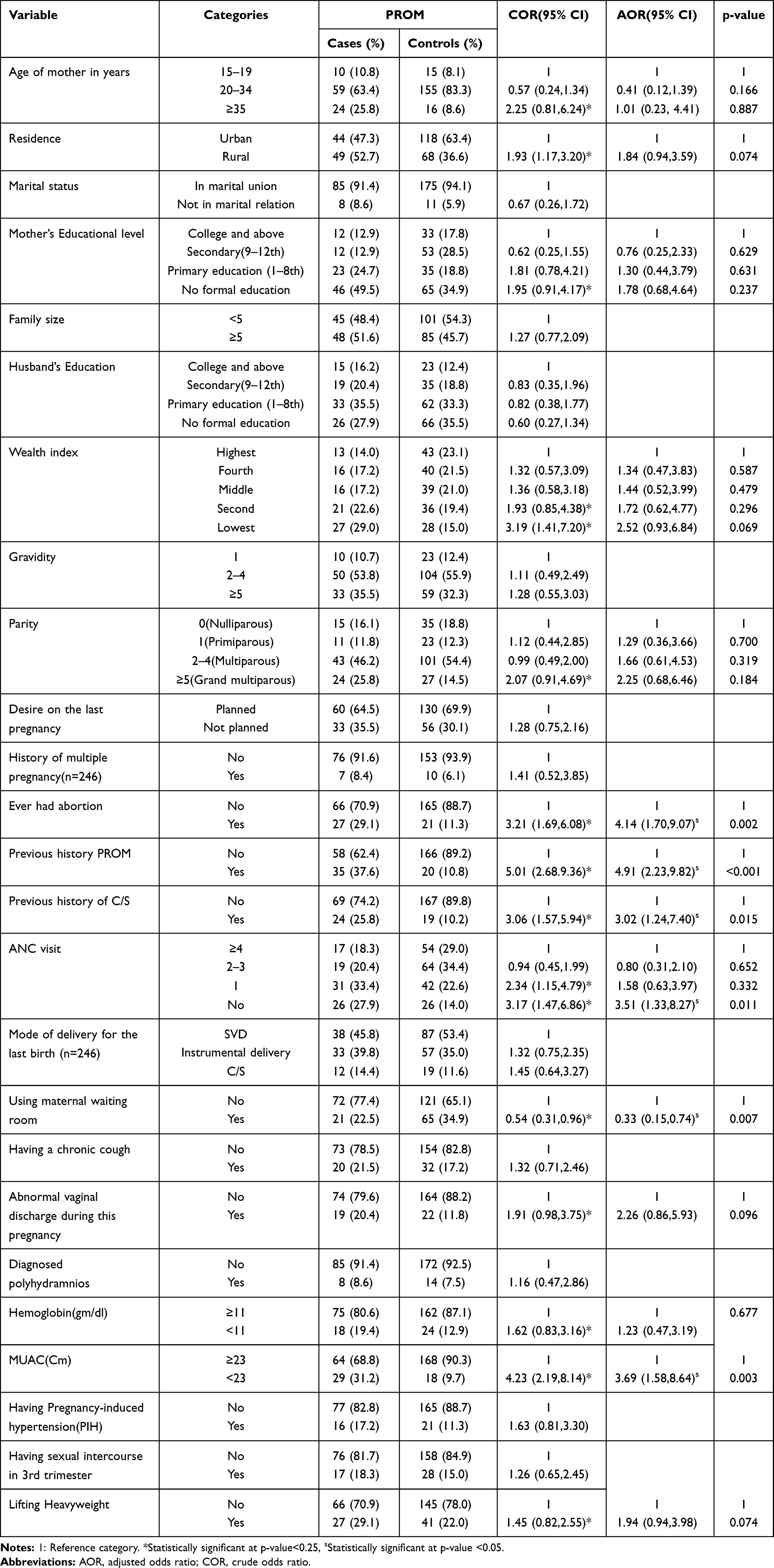 |
Table 6 Determinants of PROM Among Women Admitted to Public Hospitals in Guraghe Zone, Southern Ethiopia, 2020 |
Discussion
This study aimed at finding out determinants of premature membrane rupture (PROM). Accordingly, lack of ANC, previous history of abortion, previous history of PROM, cesarean delivery, maternal waiting room (MWR) utilization, and MAUC<23cm were all identified as significant determinants of PROM.
The probability of being a PROM case was 3.4 times higher among respondents with a previous history of abortion than their counterparts, according to the results of this study. This finding is supported by studies conducted in Hyderabad, India, Lithuania, China and Uganda.36–38 The result was also supported by two studies conducted in Northern and Western Ethiopia.23,28 This may be justified by the fact that women with a history of abortion, especially if it was an unsafe abortion, are more likely to develop intra-amniotic and intrapartum infections, which may lead to PROM.39 Furthermore, women who have had an abortion in the past, especially multiple abortions, are more likely to have a short cervix, which has been linked to an increased risk of PROM.2,40 As a result, health care providers must put a special emphasis on those mothers who have had prior abortions by providing health promotion during the ANC visit.
In line with previous studies conducted in Nigeria, India, Egypt, Bangladesh, and Sweden,20,41–44 this study also revealed that having a prior history of PROM is an important determinant for PROM. Women who had previously experienced PROM had 4.7 times higher chance of being a PROM case than women who have never even experienced PROM. This finding was also supported by studies conducted in Northern Ethiopia,22,28 Western Ethiopia.23 This could be due to the possibility of having similar obstetric causes between the previous PROM event and the present PROM occurrence, such as an untreated genitourinary infection and a short cervical length (Cervical incompetence). Furthermore, obstetric conditions are by their very nature recurrent. Therefore, health care providers at maternal health service delivery points must emphasize assessing past obstetric problems, and once those mothers are identified, diligent evaluation, health promotion, and follow-up measures must be provided.
Besides, the current study established a lack of ANC as a determinant of PROM. Mothers who did not receive ANC were 3.63 times more likely to develop a PROM than those who received four or more visits of ANC. This finding is supported by the current studies conducted in India and Western Ethiopia.23,41 This may be explained by the fact that ANC is a significant touchpoint for pregnant women’s overall wellbeing, as it facilitates the promotion and maintenance of the mother’s health throughout her pregnancy. On the other hand, mothers who do not receive ANC may be less aware of the potential risk factors for PROM, and they may be exposed to risky activities and habits that increase the likelihood of PROM. As a result, health care providers must work to track all mothers who do not receive ANC, which may be a strategy for minimizing the burden of PROM.
In our study, having had a Caesarean section was also found to be a major risk factor. PROM was 3.16 times more common in women with a history of C/S than in women without a history of C/S. This result was in line with studies conducted in Uganda, Northern Ethiopia, and Western Ethiopia, which found that C/S was linked to PROM.23,28,45 This may be due to a higher risk of C/S scar rupture in subsequent pregnancies.1 Despite the advantage of saving a woman’s and newborn’s lives, a cesarean section increases the risk of infection and uterine scarring, which might increase the likelihood of PROM.46,47 As a result, we recommend that health care providers consider the potential risk of a Caesarean section and therefore only perform it when there are compelling clinical indications. To say it another way, to reduce the health risks associated with C/S, non-medical indications for C/S delivery should be reduced to the WHO-recommended standard (5–15%).48
In the current study, those women with a Mid-Upper Arm Circumference (MUAC) of <23 cm had 3.79 times greater risk of developing PROM than those with a MUAC of ≥23 cm. A study conducted in Northern Ethiopia supplemented this finding.22 When the MUAC is less than 23 cm during pregnancy, it means that the mother is undernourished. Nutritional deficiencies, especially micronutrient deficiencies such as vitamin C or ascorbic acid, affect collagen formation and can impair the body’s ability to defend itself from degenerative processes caused by oxidative stress, which could lead to easy breakage of the membrane.49 Micronutrient deficiencies have been linked to an increased risk of PROM by disrupting collagen formation and structure.49,50 As a result, one of the most significant elements that health care providers should take is to strengthen nutritional counseling during prenatal care. Furthermore, maternal and child health care units must place a strong focus on screening and managing the nutritional status of pregnant women.
Another predictor that showed a significant relationship with PROM was the use of the maternal waiting room (MWR) during the current pregnancy. Women who stayed in the MWR during their current pregnancy had a 67% lower chance of becoming a PROM case than their counterparts. While there is little information on the relationship between this variable and PROM, some pieces of evidence showed that using MWR during pregnancy has a positive effect on maternal and child health by bridging the geographical accessibility gap.34,51 Furthermore, if a woman stays in an MWR during her final weeks of pregnancy, she may obtain sufficient rest and be less exposed to workload and heavy domestic activities, resulting in a lower risk of PROM and other maternal danger signs during pregnancy and childbirth. According to studies, MWR utilization decreased the likelihood of perinatal mortality and other social and economic effects for mothers by nearly half as compared to those who did not.52,53 As a result, government authorities in the study area should make an effort in favoring MWR for mothers who live a long distance away, as the majority of the study participants, 152 (54.5%), accessed health facilities after a one-hour or longer journey.
Although the reported cases were checked by senior doctors in the study hospitals, there may be misclassification bias. Another drawback of this study may be selection biases if some participants were unaware of when labor starts. The study included all women with PROM (preterm, term, and post-term) who were over 28 weeks of gestation, and there could be variations in determinants if the cases were separated for each category of PROM. Confounders were difficult to monitor because cases and controls were not matched with relevant variables since the study was unmatched case-control. The respondents might be prone to social desirability bias because some of the variables were based on self-reports. Finally, there might be a possibility of recall bias because women were asked about events that happened before the study.
Conclusion
In the current study, lack of ANC, previous history of abortion, previous history of PROM, caesarean delivery, maternal waiting room (MWR) utilization, and MAUC<23cm were identified as significant determinants of PROM. Hence, the stakeholders have to work on the provision of contraceptives to hamper the risks of abortion. Health-care providers should work on providing adequate ANC by tracing mothers who have not received it and advising pregnant women to use MWR in the final weeks of their pregnancy. Furthermore, maternal and child health care units must place a strong focus on screening and managing the nutritional status of pregnant women. Furthermore, women with a history of abortion, caesarean section, or PROM need extra attention from health care providers to mitigate the occurrence of PROM.
Abbreviations
ANC, antenatal care; AOR, adjusted odds ratio; CS, caesarean section; EDHS, Ethiopia demographic and health survey; MMR, maternal mortality ratio; MUAC, mid upper arm circumference; MWR, maternal waiting room; PROM, premature rupture of membranes.
Data Sharing Statement
The data used to strengthen the results of this study are to be had from the corresponding author based on reasonable request via the email address of [email protected].
Ethics Approval and Consent to Participate
This study was approved and conducted per the principles of the Helsinki Declaration. Ethical clearance was obtained from the Institutional review board of Wolkite University, college of medicine and health sciences. The Zonal Health Departments and participating hospitals gave their written permission. Written informed consent was obtained from study participants aged 18 and older after they were briefed on the study’s purpose and procedure. Furthermore, for those participants under the age of 18, consent was obtained from a parent or guardian via standard disclosure protocols. Participants’ privacy and confidentiality were ensured before data collection. Their right not to participate, not to answer any or all questions, and to withdraw from the interview at any time they want was respected.
Acknowledgments
We are grateful to Wolkite University’s College of Medicine and Health Science’s Department of Public Health for providing Ethical approval for this research. For their assistance and support during the study, we thank the managers and healthcare professionals who worked in the selected hospitals. Finally, we want to thank our supervisors, data collectors, and study participants for their contributions during the Authors’ contribution. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work”.
Disclosure
The authors report no conflicts of interest in this work.
References
1. DeCherney A. Current Diagnosis & Treatment: Obstetrics & Gynecology. Medical Late Pregnancy Complication, Section: Premature Rupture of Membranes. New York: McGraw-Hill; 2014.
2. Beckmann C. Obstetrics and gynecology. Williams’s Chapter. 2010;22:213–216.
3. Rajput U, Jain A. Impact of meconium stained amniotic fluid on early neonatal outcome. J Evol Med Dent Sci. 2013;2.
4. Gibbs R, Karlan B, Haney A, Nygaard I. Danforth’s Obstetrics and Gynecology.
5. American College of Obstetricians and Gynecologists. Prelabor rupture of membranes: ACOG practice bulletin, number 217. Obstet Gynecol. 2020;135(3):e80–e97. doi:10.1097/AOG.0000000000003700
6. FMOH. Management protocol on selected obstetrics. In: FMOH obstetrics management protocol; 2010. p. 160–165. Available from: https://www.slideshare.net/dawitdesta2/2010-management-protocol-on-selected-obstetric-topicsfederal-democr-ethipian.
7. Tc O, Jo E, Os O, Co A, Ec E, Pu A. The incidence and management outcome of preterm premature rupture of membranes (PPROM) in a tertiary hospital in Nigeria. Am J Clin Med Res. 2014;2(1):14–17. doi:10.12691/ajcmr-2-1-4
8. Asrat T, Lewis DF, Garite TJ, et al. Rate of recurrence of preterm premature rupture of membranes in consecutive pregnancies. Am J Obstet Gynecol. 1991;165(4):1111–1115. doi:10.1016/0002-9378(91)90481-6
9. Sae‐Lin P, Wanitpongpan P. Incidence and risk factors of preterm premature rupture of membranes in singleton pregnancies at Siriraj Hospital. J Obstetr Gynaecol Res. 2019;45(3):573–577.
10. Caughey AB, Robinson JN, Norwitz ER. Contemporary diagnosis and management of preterm premature rupture of membranes. Rev Obstet Gynecol. 2008;1(1):11.
11. Donders G, Desmyter J, De Wet DH, et al. The association of gonorrhoea and syphilis with premature birth and low birthweight. Genitourin Med. 1993;69:98–101. doi:10.1136/sti.69.2.98
12. Wanda NKF, Neil P. Economic burden of hospitalizations for preterm labor in the United States. Am Coll Obstetr Gynecol. 2000;96.
13. Merenstein GWL, Weisman LE. Premature rupture of the membranes: neonatal consequences. Semin Perinatol. 1996;20:375–380. doi:10.1016/S0146-0005(96)80004-8
14. Borna S, Borna H, Hantoushzadeh S. ‘Perinatal outcome in preterm premature rupture of membranes with Amniotic fluid index< 5 (AFI< 5). BMC Pregnancy Childbirth. 2014;4(1):1–4.
15. Racicot K, Cardenas I, Wünsche V, et al. Viral infection of the pregnant cervix predisposes to ascending bacterial infection. J Immunol. 2013;191:191. doi:10.4049/jimmunol.1300661
16. Rajan R, Menon V. Preterm premature rupture of membranes: correlates and pregnancy outcome in a tertiary care setting. Int J Res Med Sci. 2016;4(8):3310–3316. doi:10.18203/2320-6012.ijrms20162285
17. Boskabadi H, Zakerihamidi M. Evaluation of maternal risk factors, delivery, and neonatal outcomes of premature rupture of membrane: a systematic review study. J Pediatr Rev. 2019;7.
18. Vishwakarma K, Patel SK, Yadav K, et al. Impact of premature rupture of membranes on maternal & neonatal health in Central India. J Evid Based Med Healthc. 2015;2(49):8505–8508. doi:10.18410/jebmh/2015/1165
19. Idrisa A, Pius S, Bukar M. Maternal and neonatal outcomes in premature rupture of membranes at University of Maiduguri Teaching Hospital, Maiduguri, North-Eastern Nigeria. Trop J Obstet Gynaecol. 2019;36(1):15–20. doi:10.4103/TJOG.TJOG_89_18
20. Emechebe CI, Njoku COKA, Udofia U. Determinants and complications of pre-labour rupture of membranes (PROM) at the University of Calabar Teaching Hospital (UCTH), Calabar, Nigeria. Scholars J Applied Med Sci. 2015;3.
21. Byonanuwe S, Nzabandora E, Nyongozi B, et al. Predictors of premature rupture of membranes among pregnant women in rural Uganda: a cross-sectional study at a tertiary teaching hospital. Int J Reprod Med. 2020;2020:1–6. doi:10.1155/2020/1862786
22. Addisu D, Melkie A, Biru S. Prevalence of preterm premature rupture of membrane and its associated factors among pregnant women admitted in Debre Tabor General Hospital, North West Ethiopia: institutional-based cross-sectional study. Obstet Gynecol Int. 2020;2020:4034680. doi:10.1155/2020/4034680
23. Desta M, Amha H, Anteneh Bishaw K, et al. Premature rupture of membrane and its associated factors among pregnant women admitted to public hospitals in Nekemte town, western Ethiopia.International. Res J Obstetr Gynecol. 2020;3:27.
24. Fernandes G, Torloni MR, Hisaba WJ, et al. Premature rupture of membranes before 28 weeks managed expectantly: maternal and perinatal outcomes in a developing country. J Obstet Gynaecol. 2012;32:45–49. doi:10.3109/01443615.2011.609923
25. Goya M, Bernabeu A, García N, et al. Premature rupture of membranes before 34 weeks managed expectantly: maternal and perinatal outcomes in singletons. J Mater Fetal Neonatal Med. 2013;26:290–293. doi:10.3109/14767058.2012.733779
26. Kwizera A, Dünser M, Nakibuuka J. National intensive care unit bed capacity and ICU patient characteristics in a low income country. BMC Res Notes. 2012;5(1):475. doi:10.1186/1756-0500-5-475
27. Hackenhaar AA, Albernaz EP, Fonseca TM. Preterm premature rupture of the fetal membranes: association with sociodemographic factors and maternal genitourinary infections. J Pediatr Pediatr (Rio J). 2014;90.
28. Assefa NE, Park AL, Young J, et al. Risk factors of premature rupture of membranes in public hospitals at Mekele city, Tigray, a case control study. BMC Pregnancy Childbirth. 2018;18(1):1–7. doi:10.1186/s12884-017-1633-9
29. Chandra I, Sun L. Third trimester preterm and term premature rupture of membranes: is there any difference in maternal characteristics and pregnancy outcomes? J Chin Med Assoc. 2017;80(10):657–661. doi:10.1016/j.jcma.2016.12.006
30. Tchirikov M, Schlabritz-Loutsevitch N, Maher J, et al. Mid-trimester preterm premature rupture of membranes (PPROM): etiology, diagnosis, classification, international recommendations of treatment options and outcome. J Perinat Med. 2018;46(5):465–488. doi:10.1515/jpm-2017-0027
31. Workineh Y, Birhanu S, Kerie S, et al. Determinants of premature rupture of membrane in Southern Ethiopia, 2017: case control study design. BMC Res Notes. 2018;11(1):1–7. doi:10.1186/s13104-018-4035-9
32. Boeke A, Dekker JH, Peerbooms P. A comparison of yield from cervix versus vagina for culturing Candida albicans and Trichomonas vaginalis. Genitourin Med. 1993;69.
33. Tiruneh GT, Taye BW, Karim AM, et al. Maternity waiting homes in Rural Health Centers of Ethiop: the situation, women’s experiences and challenges. Ethiop J Health Dev. 2016;30(1):19–28.
34. Bayu BB, Aline U. Maternity waiting homes and skilled delivery in Ethiopia: review of strategy and implementation to drive sustainable development goals. Med Pract Rev. 2018;9(3):19–26. doi:10.5897/MPR2018.0137
35. Kurji J, Gebretsadik LA, Wordofa MA, et al. Factors associated with maternity waiting home use among women in Jimma Zone, Ethiopia: a multilevel cross-sectional analysis. BMJ Open. 2019;9(8):e028210. doi:10.1136/bmjopen-2018-028210
36. Padmaja J, Swarupa K. Maternal and perinatal outcome in premature rupture of membranes at term pregnancy. 2018.
37. Daiva V, Stafan B, Vidaa M. Antenatal risk factors associated with PPROM. Acta Medica Litutania. 2002;9(3).
38. Liu J, Feng ZC, Wu J. The incidence rate of premature rupture of membranes and its influence on fetal–neonatal health: a report from mainland China. J Trop Pediatr. 2009;56.
39. Gibson CS, Goldwater PN, MacLennan AH, Haan EA, Priest K, Dekker GA. Fetal exposure to herpesviruses may be associated with pregnancy-induced hypertensive disorders and preterm birth in a Caucasian population. BJOG. 2008;115(4):492–500. doi:10.1111/j.1471-0528.2007.01653.x
40. Gomez R, Romero R, Nien JK, et al. A short cervix in women with preterm labor and intact membranes: a risk factor for microbial invasion of the amniotic cavity. Am J Obstet Gynecol. 2005;192(3):678–689. doi:10.1016/j.ajog.2004.10.624
41. Choudhary M, Rathore SB, Chowdhary J, Garg S. Pre and post conception risk factors in PROM. Int J Res Med Sci. 2015;3(10).
42. Tarek KA, Sahar NM, Hamida AE, et al. Cervicovaginal infection during pregnancy and its relation to preterm pre-labour rupture of membranes. J Am Sci. 2012;8(12).
43. Lovereen S, Khanum MA, Nargis N, et al. Maternal and neonatal outcome in premature rupture of membranes. Bangla J Med Sci. 2018;17(3):479–483. doi:10.3329/bjms.v17i3.37004
44. Ladfors L, Mattsson L-Å, Eriksson M, et al. Prevalence and risk factors for prelabor rupture of the membranes (PROM) at or near term in an urban Swedish population. Journal of Perinatal Medicine. 2000;28. doi:10.1515/JPM.2000.066
45. Kaye D. Risk factors for preterm premature rupture of membranes at Mulago Kampala Uganda. East Afr Med J. 2001;78.
46. Chazotte C, Cohen WR. Catastrophic complications of previous cesarean section. Am J Obstet Gynecol. 1990;163(3):738–742. doi:10.1016/0002-9378(90)91059-L
47. Lotufo FA, Parpinelli MA, Haddad SM, et al. Applying the new concept of maternal near-miss in an intensive care unit. Clinics. 2012;67:225–230. doi:10.6061/clinics/2012(03)04
48. Fleming LC, Ansumana R, Bockarie AS, et al. Health-care availability, preference, and distance for women in urban Bo, Sierra Leone. Int J Public Health. 2016;61:1079–1088. doi:10.1007/s00038-016-0815-y
49. Oguntibeju OO. The biochemical, physiological and therapeutic roles of ascorbic acid. Afri J Biotechnol. 2008;7(25).
50. Hassanzadeh A, Paknahad Z, Khoigani MG. The relationship between macro-and micro-nutrients intake and risk of preterm premature rupture of membranes in pregnant women of Isfahan. Adv Biomed Res. 2016;5.
51. Van Lonkhuijzen L, Stekelenburg J, Van Roosmalen J. Maternity waiting facilities for improving maternal and neonatal outcome in low-resource countries. Cochrane Database Syst Rev. 2009;(3).
52. Sialubanje C, Massar K, Van Der Pijl MSG, Kirch EM, Hamer DH, Ruiter RAC. Improving access to skilled facility-based delivery services: women’s beliefs on facilitators and barriers to the utilisation of maternity waiting homes in rural Zambia. Reprod Health. 2015;12(1). doi:10.1186/s12978-015-0051-6
53. Buser JM, Lori JR. Newborn outcomes and maternity waiting homes in low and middle- income countries: a scoping review. Matern Child Health J. 2017;21(4):760–769. doi:10.1007/s10995-016-2162-2
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.