")
Back to Journals » International Journal of Women's Health » Volume 14
Determinants of Premature Rupture of Membrane (PROM) Among Pregnant Women in Southern Ethiopia: A Case-Control Study
Authors Enjamo M, Deribew A , Semagn S, Mareg M
Received 17 December 2021
Accepted for publication 18 March 2022
Published 31 March 2022 Volume 2022:14 Pages 455—466
DOI https://doi.org/10.2147/IJWH.S352348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Melkamu Enjamo,1 Amare Deribew,2 Selamawit Semagn,1 Moges Mareg1
1Department of Reproductive Health, School of Public Health, College of Medicine and Health Science, Dilla University, Dilla, Ethiopia; 2Departent of Public Health, St. Paul Hospital Millennium Medical College, Nutrition International’s Country Director, Addis Ababa, Ethiopia
Correspondence: Moges Mareg, Tel +251923527030, Email [email protected]
Background: Premature rupture of membrane (PROM) varies from country to country and complicates 4 to 10% of pregnancies worldwide it has an overwhelming effect on maternal and newborn health. Even though many interventions implemented to tackle it, the problem is persisted.
Objective: To identify determinants of premature rupture of membrane among pregnant women who have visited labor wards in four hospitals found in Gedeo zone, Southern Ethiopia.
Methods: Hospital-based unmatched case-control study was conducted from February to May 2020. Data were collected among 75 cases and 223 controls using face-to-face interviews. Cases and controls were recruited consecutively from pregnant women who have visited the labor ward. Data were entered into Epi-data version 3.1 and analyzed by using SPSS version 20. Bivariable and Multivariable logistic regression was used to check the association between dependent and independent variables, statistically significant association was declared at p-value < 0.05.
Results: A total of 75 cases and 233 controls were enrolled in the study. Hypertension during index pregnancy [AOR = 2.81 (95% CI: 1.09 − 7.23)], history of abortion [AOR = 3.7 (95% CI: 1.41– 9.73)], history of caesarean section [AOR = 3.46 (95% CI: 1.34– 8.9)] and history of PROM [AOR = 4.77 (95% CI: 2.31– 9.89)] were associated with premature rupture of membranes.
Conclusion: Hypertension during the index pregnancy, history of abortion, history of PROM, and history of cesarean section has an association with premature rupture of membrane. The result of the study suggests early identification and treatment of abortion, hypertension, and cesarean section in pregnant women mitigates the risk of premature rupture of membrane.
Keywords: premature rupture of membrane, determinants, Southern Ethiopia, case-control study
Introduction
Premature rupture of membrane (PROM) is defined as the rupture of the chorioamnionitis membrane and passing a gush of fluid through the birth canal before the onset of true labor. Innumerable books classify PROM into two based on gestational age. PROM which occurs before the gestational age of 37 weeks is termed as preterm premature rupture of membrane (PPROM) whereas premature rupture of the membrane which occurs after the gestational age of 37 weeks is termed as term premature rupture of membrane (TPROM).1
The time between the rupture of membrane and the onset of true labor is referred to as the latent period and it may vary from minutes to days. If the duration between rupture of membrane and onset of true labor is greater than 12 hours termed as prolonged latent period.2
Even though the cause of PROM is not known scholars over the world come across both maternal and fetal risk factors that have been implicated as an etiology like sexually transmitted infections (STI), maternal cigarette smoking, previous history of preterm delivery, short cervical length, polyhydramnios, multiple gestations, history of threatened abortion, poor socioeconomic status, poor nutritional status, and connective tissue disorders.3
The infection of amniotic fluids by itself is the risk factor for the premature rupture of the membrane. Premature rupture of membrane easily diagnosed either by taking a history from mother if she has experienced a passing gush of fluid or nitrazine lab test.4
PROM is associated with serious maternal and fetal infections when it has occurred both at term and preterm. Among these chorioamnionitis is the most common one when it occurs at preterm age.5 PROM complicates the prenatal health of newborns; those born from mothers with the problem are may acquire the problem of birth asphyxia, neonatal sepsis, and finally neonatal death.6
Overall, PROM is a significant contributor to perinatal morbidities and mortalities. Even premature rupture of the membrane has serious morbidity and mortality it is possible to minimize the morbidity and mortality with good clinical skills. World Health Organization (WHO) and American College of Obstetrics and Gynecology PROM recommends two types of clinical management, expectant management for those mothers whose membrane has ruptured at a gestational age of below 37 weeks and inducing labor for those who encountered the problem after the gestational age of 37 weeks.7
Although the prevalence of PROM varies from country to country, it complicates 4 to 10% of pregnancies all over the world. It is one of the major causes of perinatal morbidities and mortalities. Worldwide 30% of preterm deliveries and its complication like birth asphyxia and respiratory distress have been contributed due to PROM. PROM is one of the major causes of neonatal sepsis, fetal distress, and birth asphyxia which results from the rapid reduction of amniotic fluid volume.8 According to two years, follow-up studies done at Jimma University the incidence of PROM was 14.5%.9
PROM is also associated with perinatal infection, increases the risk of placental abruption by 5% as compared with the general population, delayed motor and brain developmental, palsy have seen among babies born from women with premature rupture of the membrane.8,10
According to a study conducted in India, 33% of perinatal morbidity and 15% perinatal mortality have been occurred due to premature rupture membrane.11 Besides perinatal morbidities and mortalities, PROM is also contributing to the serious maternal infection of amniotic fluid which can progress into fatal sepsis and cord prolapse.11,12
The problem is found to be more common in blacks than whites due to their poor socio-demographic status.4 Relatively premature rupture of the membrane more commonly occurs at term than preterm.13 In Africa, the maternal mortality ratio increased by 5% from 2013 to 2015 against the millennium development goal recommendation.14 It was planned to reduce maternal mortality by 3/4th by the end of 2015.14,15
According to the 2016 Ethiopian Demographic Health Survey (EDHS) report, the maternal mortality ratio was estimated to be 412 per 100,000 live births. Maternal death accounts for around one-fourth of all death in reproductive-aged women related to childbearing directly or indirectly.16
Risk factors that are contributing to PROM include: educational status of the mother, poor nutritional status of the mothers, cervical insufficiency, cigarette smoking during pregnancy, urinary tract and sexually transmitted infections, having high volume of amniotic fluid (polyhydramnios), multiple gestations, history of threatened abortion, poor socioeconomic status, poor nutritional status, maternal age, and connective tissue disorders.1,10,17
Nations over the globe are working through their national health policy to promote maternal and child health. Besides the national health policies and programs, international agreements including millennium development goals, sustainable development goals are remarkable for their contribution in reducing neonatal and maternal mortalities and morbidities.18
Several strategies developed to alleviate maternal as well as neonatal morbidity and mortalities as planned were, ensuring that every birth should be undergone with the skilled health personnel, access to emergency obstetric and newborn care free of charge, training of health professionals on compassionate and respectful care (CRC) as well access to integrated management of newborn and childhood illnesses and effective referral system were the major.14
The Federal Ministry of Health of Ethiopia launched the national maternal death surveillance and response (MDSR) system in May 2013 as a tool to improve the quality of maternal health care, particularly during pregnancy, laboring, and the postpartum periods.19
Also, the problem has an adverse outcome on neonates, ministry of health trying to establish neonatal intensive care units (NICU) at different hospitals for those who born with complications due to different reasons like preterm delivery, low birth weight, birth asphyxia, and neonatal sepsis as a result of premature rupture of membrane.
Despite the efforts, maternal and child morbidities and mortalities remains the major challenge of the developing countries. And countries fail to achieve their plan of reducing maternal mortality child mortality and need to design another strategy called sustainable development goal (SDG).18
The current global agenda sustainable development goal (SDG) particularly goal 3 is intended to promote maternal and child health through reducing poverty, improving the nutritional status of mothers, universal access to quality primary health care.18
Now day countries over the world working with high motivation to accomplish the plan of this goal of reducing and neonatal mortality 12/1000 live birth whereas maternal mortality 70 per 100,000 live births.18 To speed up the reduction of maternal and neonatal mortality identifying factors that have an association with one cause of maternal mortality and morbidity, premature rupture of the membrane is very crucial. Therefore this study was important to provide additional information since the problem is not much studied in this locality so that intended to identify risk factors of premature rupture of membrane among pregnant women who had visited labor wards of hospitals found Gedeo zone.
Furthermore, since no similar study was done in this area, the result of this study may be used as an input for zonal health departments and hospitals health managers to implement determinant-focused surveillance initiatives to understand and combat the burden of premature rupture of the membrane by prioritizing specific potentially modifiable factors. It can also be used as input for another researcher in this zone.
Materials and Methods
Study Area
The study was conducted in four public hospitals found in Gedeo Zone namely, Dilla University referral hospital, Yirgachefe, Bule, and Gedeb primary hospital from February to May 2020 among women admitted in the labor ward. Gedeo Zone is one of the 15 Zonal administrations of Southern Nations, Nationalities, and Peoples (SNNP) regional states. The zone is located in the Southern part of the region and is 371 km far from Addis Ababa, the capital city of Ethiopia, and 96 km from Hawassa city, the administration center of the South Nation Nationality and People Region (SNNPR).
Currently, the zone has 1 referral hospital, 3 primary hospitals, 38 health centers, 146 health posts, and 12 private and 4 NGO clinics. According to the zonal health department, the potential health coverage is estimated to be 87% based on health center expansion. Concerning human resources, there are 53 physicians, 38 Health officers, 428 nurses (all types), and 325 health extension workers.
Study Design and Period
Hospital-based unmatched case-control was employed from February 25 to May 20.
Source Population
The source population for cases and controls group showed independently as follows:
For cases: Pregnant women who have visited the labor ward of four hospitals found in the Gedeo zone during the study period and who were diagnosed as having premature rupture of membrane.
For controls: Pregnant women who have visited the labor ward of four hospitals found in the Gedeo zone during the study period and had no premature rupture of membrane.
Study unit: The study unit for cases was selected pregnant women case of premature rupture of the membrane in the study hospitals.
The study unit for the controls was selected pregnant women who visited the labor ward, with other diagnoses confirmed to be free of premature rupture of membrane.
Eligibility Criteria
Inclusion Criteria
Pregnant women who had visited the hospitals for labor care, diagnosed with premature rupture of the membrane were enrolled as cases.
For controls, pregnant women who had visited the study hospitals for labor care and had no PROM were included.
Exclusion Criteria
Women, who were mentally incompetent, seriously ill in the course of data collection, were excluded from both cases and controls.
Sample Size Determination
The sample size was calculated using the statistical calculator of Epi-info version 7 used for sample size determination designed for an unmatched case-control study. The following assumptions were made during calculating sample size: 95% confidence level, 80% power, and case to control the ratio of 1:3 to increase the detection of differences in predictive factors between the cases and controls. History of cesarean section in a previous pregnancy was the main exposure variable for premature rupture of the membrane which yields the maximum sample size based on a study in Mekelle city.20 According to the study, 16.2% of cases and 4.4% of controls were delivered by cesarean section during their precedent pregnancy. This gave the maximum sample size of 286. By considering the 10% nonresponse rate of the total sample size was 314 (80 for cases and 234 for controls).
Sampling Technique
The convenient sampling method was used to enroll cases and controls. Before the study, an assessment was done in the study hospitals using records to determine the cases and controls. Based on the estimated number of cases and controls the sample size was allocated proportionally to the study hospitals as shown in the diagram below (Figure 1).
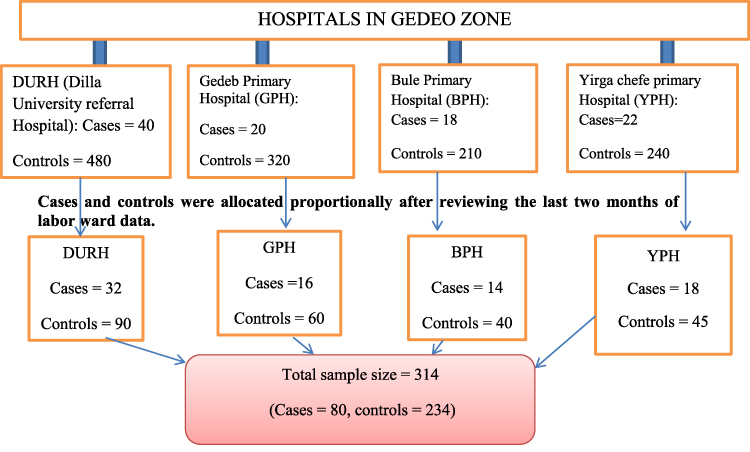 |
Figure 1 Schematic representation of the sampling procedure to select pregnant women who visited labor wards of public hospitals found in Gedeo zone, South Ethiopia, 2020. |
Data Collection Tools
The structured questionnaire adapted from published literatures8,9,20–23 were used after modification to the local situation. To identify the cases the standard definition of premature rupture of membrane (PROM) was used.
Data Collection Procedure
Cases and controls were interviewed face-to-face by trained data collectors using structured, pre-tested questionnaires, non-stretchable tape meter used to measure upper arm circumference and measurement was taken at nearest one millimeter, finally, medical records reviewed to complete questions needs medical confirmation; like diagnoses of PROM and diabetes mellitus. The interview was conducted where patients were in admission. A total of eight Diploma midwives, two midwives in each hospital who are fluent in speaking the local language and Amharic were recruited as data collectors, and four senior degree nurses; one for each hospital were recruited as supervisors. Intensive orientation was given for one day on data collection techniques, data collection tools, the confidentiality of the information, participant’s right, informed consent, and practical demonstration of the interview. The data was collected under close supervision and the facilitation of the principal investigator.
Study Variables
Dependent Variable
Presence or absence of Premature ruptures of the membrane (PROM).
Independent Variables
Socioeconomic and demographic factors: including place of residence, maternal age, marital status, maternal educational level, maternal occupation, wealth index.
Obstetric factors:- previous history of premature rupture of membrane, history of abortion, number of parity, birth interval, a cesarean section in a previous pregnancy, history of trauma to the abdomen in the index pregnancy.
Medical and other factors:- history of genitourinary tract infection, history of vaginal discharge in the current pregnancy, hypertension in the current pregnancy, body mass index of the mother, history smoking of smoking, the mid-upper circumference of the mother.
Data Quality Assurance
The questionnaire was prepared by the investigator in English language and translated into the Gedeoffa version and then back to the English version to check its consistency. Pretest was done on 5% of the total sample size in Kebado primary hospital to minimize ambiguity of words applicability to the local context and to make a necessary adjustment. There was a misunderstanding of some questions; based on their suggestion the comments were accommodated before actual data collection. The data collectors and supervisors were given one day of intensive training on tools and procedures. Through close supervision, the questionnaire was checked daily for consistency and completeness. Finally, the completeness of the questionnaire was checked before entering data into the computer software program and before analysis and interpretation. The data was stored in a secure place for confidentiality and in time when needed for a backup.
Term Definition
Premature rupture of membrane: Is defined as passing gush of fluid through the birth canal as a result of breakage of amniotic sac before the onset of true labor.1
Optimal birth interval: If the gap between two consecutive birth is equal to or greater than two years it is said to be optimal.21
Data Management and Analysis
The data were entered into Epidata version 3.1, then exported to and analyzed with SPSS version 20. In the analysis: proportions, frequencies, and mean were calculated to study the variables to compare cases and controls.
Data were analyzed by using logistic regression. First, the variables were fitted to the bivariate logistic regression. Then all variables having a p-value < 0.25 in the bivariable analysis were further entered into a multivariable logistic regression model.
The Hosmer and Lemeshow goodness of fit test was used to determine whether the model adequately describes the data and the model adequately fitted for the final model.
A total of 24 variables were considered for the bivariate analysis, the variables were; the age of the women, place of residency, educational status of the women, wealth index, body mass index, MUAC of the women, number of gravidity and parity, ANC utilization, hypertension during pregnancy, chronic cough, birth interval, history of abortion, vaginal bleeding, previous history of PROM, history of preterm delivery, history of abdominal surgery, vaginal bleeding, history of cesarean sectioning in last pregnancy, abdominal trauma, carrying a heavy object, sex in last two weeks, drinking alcohol and smoking during pregnancy. Among these Confounders were controlled with multivariable logistic regression. Adjusted odds ratio (AOR) with 95% CI, was estimated to assess the presence and strength of associations, and statistical significance was declared at p-value < 0.05. Finally, results were compiled and presented using tables and texts.
The wealth index was determined by computing Principal Component Analysis (PCA). Twenty-six items were considered for PCA. Initially, all items were dichotomized into one for asset presence and zero for the absence of asset. Then descriptive statistics were used to explore all variables that measure the wealth index. Those variables with empty categories and less than 5% and more than 95% of observation were excluded from PCA. Initially, requirements; adequacy of sample size, the ratio of cases to a variable, correlation matrix, measure of sampling adequacy, and Bartlett test of sphericity of PCA were checked. In the second phase, we also assessed deriving a factor model satisfaction (communality, complex structure or loading, and many components’ variable). Finally, seven components were produced explaining collectively 68.7% of the variance in the set of variables. Scores were then used to create breakpoints that define the wealth index from lowest quintile (poorest) to highest quintile (wealthiest).
Each household’s assets for which information was collected were assigned a weight or factor score generated through PCA. The PCA result showed that variables highly loaded on the first PCA component were having a private house, pipe water as a source of drinking water, cooking with electricity, corrugate roof, floor ceramic, wall block, and types of latrine were variables loaded on the third component.
Ethical Consideration
All the steps during the data collection were in accordance with the institutional review board (IRB) of Dilla University and Helsinki. Before data collection, appropriate ethical clearance (approval) and a supportive letter were obtained from Dilla University College of Health Science and Medicine IRB.24 Written permission was obtained from the hospital managers. Informed consent was directly obtained from study participants. For those who were less than 18 years old assent were obtained from their families and consent were obtained from the participants.
Participants of the study were recruited voluntarily and informed about the right not to participate or withdraw at any time without compromising their hospital care. Confidentiality information was also assured and the name of the participant was not written on the questionnaire rather codes were used.
Result
Socio-Demographic Factors
A total of 298 participants (223 controls and 75 cases) consented to participate in this study were interviewed, resulting 94.9% response rate. The mean age of cases and controls was 26.3 and 26.9 with a standard deviation of ±5.9 and ±5.5 years respectively. Of the total respondent, the majority of the controls 215 (96.4%), and cases 70 (93.3%) were currently in marital union. Regarding the place of residence more than half of the cases 3 8(50.7%) and controls 130 (58.3%) were rural residents. Fifty-eight (77.3%) cases and 153 (68.6%) of the controls attended primary education. About 31 (41.3%) cases and 105 (47.1%) controls were merchants. About 7 (8%) cases and 8.1% of controls had a very rich wealth index and 26 (34.7%) of cases and 58 (26%) controls had very poor (the lowest quintile) wealth index (Table 1).
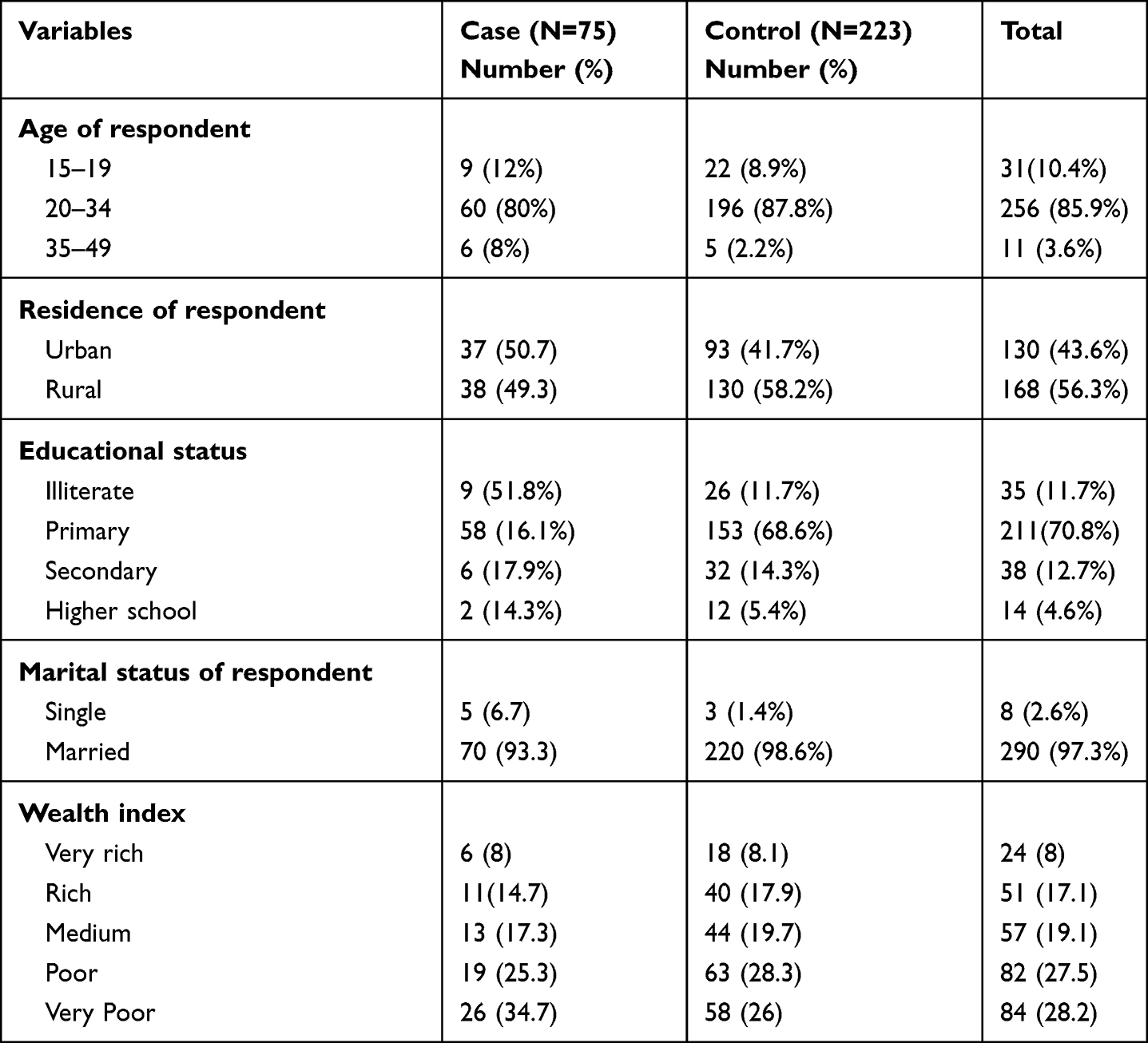 |
Table 1 Socio-Demographic Characteristics of Pregnant Women Who Visited Labor Wards of Public Hospitals Found in Gedeo Zone, South Ethiopia, 2020 |
Risky Physical Activities
Among the study participants more than half, 54 (72%) of cases had a history of carrying heavy objects during the index pregnancy. Regarding sleep patterns, 85.3% of cases and 91.9% of controls reported that they sleep more than 8 hours per day. It was answered that less than a quarter of both cases and controls had a history of abdominal trauma within the last two weeks of the current pregnancy. Few participants from both cases and the controls group reported that they have faced physical violence in the index pregnancy. From the total study participants, a total of 60 women, 24 cases, and 36 controls have been drinking alcohol during the index pregnancy. Of the total of 60 drinkers, 80% of cases drank alcohol twice and above per week till they were intoxicated with it. And 12% of both cases and controls smoke either a cigarette or local products of tobacco during the index pregnancy.
Obstetric and Medical History of the Participants
From the participants included in this study, a major proportion of 65 (86.7) cases and 209 (93.7) controls have utilized antenatal services in this pregnancy. Of whom, 166 participants 39 cases and 127 controls have visited antenatal clinics four times and above. Regarding the history of abortion, twenty-five (31.2%) of cases and 10.6% of controls had an abortion. Among the women who had a history of abortion, a major proportion of both 68% cases and 78.4% of controls had only one abortion. One hundred ninety-nine controls and 86.7% of cases have no history of preterm delivery. As far as concerning to history of premature rupture of membrane 36 (48%) cases and 27 (12.1%) controls have a history of PROM. From the study participants, 25 (33.3%) of cases and 11 (4.9%) of controls groups had a cesarean section in their last pregnancy. A few women in both case and control groups had abdominal surgery. Among the total participants, a major proportion of 61 (81.3) cases and 195 (87.4) controls have normal body mass index. From women who participated in study 58 (77.3%) of cases and 186 (83.4%) of controls, mid-upper arm circumference was greater than 23 centimeters. The low proportion of both cases and controls had low body mass index during the index pregnancy. The majority of the study participants has visited hospitals for labor care at term. Of the study participants, low proportion of cases 27 (36%) and 27 (12.1%) controls have chronic cough during the current pregnancy. Regarding the pregnancy outcome, a large proportion of cases and control have given birth to a single child and 64% of cases and 60.5% of controls have a non-optimal inter-pregnancy interval. 29 (38.7%) women of cases and 17 (7.6%) controls were hypertensive in the index pregnancy and a low proportion of cases and controls have abnormal vaginal discharge during the current pregnancy. Of the study participants, 20 (26.7%) cases and 31 (13.9%) controls had abnormal vaginal bleeding in this pregnancy (Table 2).
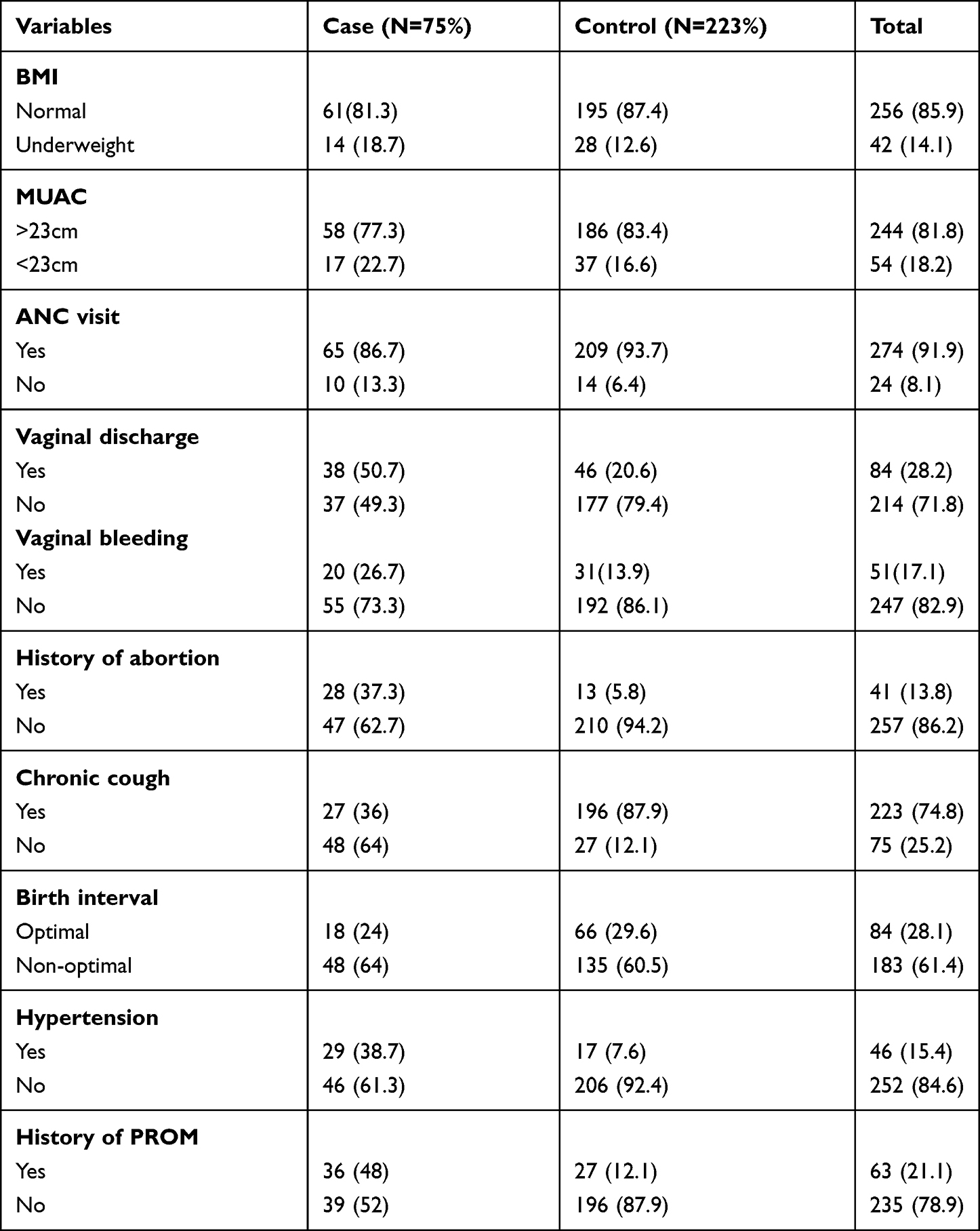 |
Table 2 Obstetric Characteristic of Pregnant Women Visited Labor Ward Public Hospitals Found in Gedeo Zone, Southern Ethiopia, 2020 |
Determinants of Premature Rupture of Membrane
The factor that remained significantly associated with premature rupture of the membrane in multiple logistic regression analyses by adjusting for other variables were hypertension during the index pregnancy, history of abortion, history of premature rupture of membrane, and history of cesarean section in last pregnancy.
Accordingly, women who were hypertensive during pregnancy were 2.8 times [AOR= 2.80, 95% CI (1.09–7.23)] more likely to have PROM than normotensive women. Similarly, women who had a history of abortion were 3.7 times [AOR=3.70, 95% CI (1. 41–9.73)] more likely to have premature rupture of membrane compared to women who did not experience abortion.
Women who had a history of premature rupture of the membrane in previous pregnancies were 4.7 times [AOR= 4.77, with 95% CI (2.31 −9.89)] more likely to develop premature rupture of membrane compared to women who did not have a history of premature rupture of the membrane in the previous pregnancies. Likewise, women who had a history of cesarean section in their last pregnancy were, 3.4 times [AOR =3.46, 95% CI (1.34–8.9)] more likely to have premature rupture of the membrane when compared to women who did not have a history of cesarean section in the preceding pregnancy (Table 3).
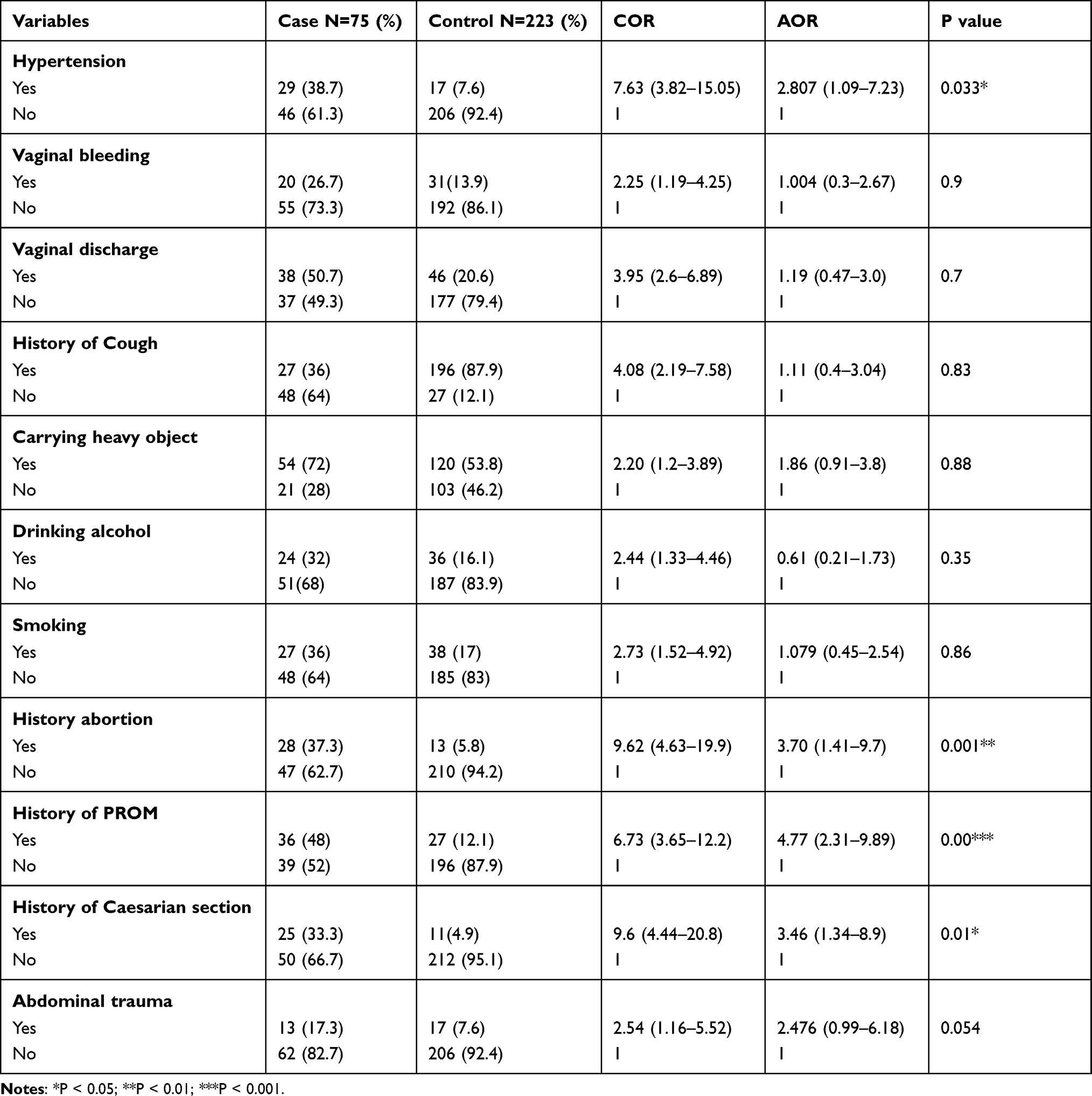 |
Table 3 Determinants of Premature Rupture of Membrane Among Pregnant Women Visited Labor Ward of Public Hospitals in Gedeo Zone, Southern Ethiopia, 2020 |
Discussion
Though the cause of premature rupture of the membrane is multifactorial, in this study hypertension during pregnancy, history of abortion, history of cesarean section in last pregnancy, and history of premature rupture of pregnancy in a previous pregnancy were found to be associated with the occurrence of premature rupture of membrane among women seeking labor care in public hospitals found in Gedeo zone.
In this study women who were hypertensive in current pregnancy were 2.8 times more likely to develop premature rupture of the membrane when compared with normotensive women. This result is similar to studies done in the United Kingdom, Iran, and Southern Ethiopia where, hypertension during pregnancy increases the odds of developing premature rupture of the membrane.5,12,21 This might be due to the diminished blood supply to the uterus in hypertensive women that resulted in abnormal cytotrophoblast invasion of spiral arterioles and endothelial dysfunction that in turn leads to placental ischemia and endothelial damage of the placenta which leads to premature rupture of membrane.
This study also identified the history of abortion as a risk factor for premature rupture of the membrane. A woman who experienced abortion was 3.7 times more likely to develop premature rupture of the membrane when compared with women who did not have abortion experience. This result is supported by researches conducted in India, Brazil, China, and Northern Ethiopia, hospitals found in Mekelle city.9,20,25,26 This might be because abortion procedure especially dilatation and curettage disrupt cervical and uterine elasticity which leads to uterine scarring as well as cervical insufficiency and end up with premature rupture of membrane.
In this is studied women who had a history of premature rupture of the membrane in previous pregnancies were 4.7 times more likely to develop premature rupture of the membrane as compared to their counterparts. This result is supported by studies done in America, Iran, the United Kingdom, Thailand, India, Nigeria as well as a study done in Tigray region hospitals found in Mekelle city.5,6,20,21,24,25,27 This might be due to abnormal anatomical formation of the uterus and cervix.
This study identified a history of cesarean section in the last pregnancy found to be a risk factor for premature rupture of membrane. Women who delivered their last baby with cesarean section were 3.4 times higher odds of having premature rupture of the membrane as compared with women who delivered through a normal birth canal. This result is parallel with a study conducted in Mekelle city public hospitals.20 This might be a cesarean section scar on the wall of the uterus increases the risk of rupturing prematurely.
Strength and Limitation of the Study
This study used both primary and document review which increase the reliability of information generated. Due to resources limitations and functionalities of the study hospitals some factors like measuring the amniotic fluid pool which needs detailed investigation were not assessed.
Conclusion and Recommendation
Conclusion
The study identified hypertension during pregnancy; history of abortion, history of cesarean section in last pregnancy, and history of premature rupture of pregnancy in a previous pregnancy were found to be associated with the occurrence of the premature rupture of membrane.
Recommendation
According to the findings of this study, the following recommendation was forwarded to the concerned bodies.
For health planners: Interventions aimed at improving better access to medical care to rural women to minimize the effect of hypertension on obstetrics outcome, increasing access to safe abortion services in health facilities especially in rural communities minimizes utilization of unsafe abortion, and reducing the risk of developing premature rupture of membrane.
For Health professionals: Early detection and treating any risky medical conditions which can compromise the quality of life in pregnant women is very crucial to minimize maternal and newborn death. Providing abortion care responsibly without damaging the wall is also reduces the risk of premature rupture of the membrane in a future pregnancy.
Additional Information
No additional information is available for this paper.
Data Sharing Statement
The datasets used in this study can be available from the corresponding author upon the reasonable request.
Acknowledgments
Our sincere gratitude goes to the Gedeo zone health department for their cooperation and for forgiving all the valuable information, data collectors, supervisors, and study participants for giving their valuable time. Lastly, my deepest thanks go to Dilla University referral hospital, Bule primary hospital, Yirga-cheffe, and Gedeb primary hospital managers and study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive a grant from any funding agencies.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. William NP, Beckmann MD. Obstetrics and Gynecology.
2. Thaddeus P, Brain M. Preterm PROM. Clin Obstetr Gynacol. 2011;54(2):307–312. doi:10.1097/GRF.0b013e318217d4d3
3. Joyce S. Demographic, Clinical, and Environmental Risk Factors for Prelabour Rupture of Membranes in Western Australia. University of Western Australia; 2008.
4. Caughey AB, Robinson JN, Norwitz ER. Contemporary diagnosis and management of preterm premature rupture of membranes. Rev Obstetr Gynacol. 2008;1(1):11.
5. Boskabadi H, Zakerihamidi M. Maternal risk factors, delivery, and neonatal outcomes of premature rupture of membrane. J Pediatr Rev. 2019;7(2):77–88.
6. Emechebe CI. Determinants and complications of Pre-Labour Rupture of Membranes (PROM) At the University of Calabar Teaching Hospital (UCTH), Calabar, Nigeria. J App Med Sci. 2015;3(5B):1912–1917.
7. Stringer M, Miesnik SR, Brown L, Martz AH, Macones G. Nursing care of the patient with preterm premature rupture of membranes. MCN: The American Journal of Maternal/Child Nursing. 2004 May 1;29(3):144-50.
8. Haiyan Y, Wang X, Gao H, et al. Perinatal outcomes of pregnancies complicated by preterm premature rupture of the membranes before 34 weeks of gestation in a tertiary center in China: a retrospective review. Biosci Trends. 2015;9(1):35–41. doi:10.5582/bst.2014.01058
9. Zhang LX, Sun Y, Zhao H, et al. A Bayesian stepwise discriminant model for predicting risk factors of preterm premature rupture of membranes: a case-control study. Chin Med J. 2017;130:2416–2422. doi:10.4103/0366-6999.216396
10. Frenette P, Dodds L, Armson BA, Jangaard K. Preterm prelabour rupture of membranes: effect of latency on neonatal and maternal outcomes. J Obstetr Gynaecol Can. 2013;35(8):710–717. doi:10.1016/S1701-2163(15)30861-6
11. Khade SA, Bava AK. Preterm premature rupture of membranes: maternal and perinatal outcome. Int J Reprod Contracept Obstetr Gynecol. 2018;7(11):4499. doi:10.18203/2320-1770.ijrcog20184496
12. Varner M, Aris IM, Logan S, et al. Preterm prelabour rupture of membranes: a retrospective cohort study of association with adverse outcome in subsequent pregnancy. BJOG. 2017;124:1698–1707. doi:10.1111/1471-0528.14462
13. Benli AR, Cetin benli N, Usta AT, et al. Preterm premature rupture of membranes: diagnosis and management. J Clin Med Res. 2015;7(2):97–102. doi:10.14740/jocmr1904w
14. Rao S, Swathi P, Unnikrishnan B, Hegde A. Study of complementary feeding practices among mothers of children aged six months to two years-A study from coastal south India. Australas Med J. 2011;4(5):252. doi:10.4066/AMJ.2011.607
15. African Union. Status report on maternal new born child and adolescent health: focusing on unfinished business in Africa. Addis Abeba. AU report 2017.pdf. 2017.
16. Bazezew K, Worku W, Abebe Z. Timely initiation of complementary feeding practices in Gondar Town Northwest Ethiopia: a cross-sectional study. Ecol Food Nutr. 2020;59(3):329–341. doi:10.1080/03670244.2020.1733994
17. Devika S. Management of preterm rupture of membrane SLCOG National guidelines. 2021.
18. Marmot M, Bell R. The sustainable development goals and health equity. Epidemiology. 2018 Jan 1;29(1):5-7.
19. Federal Ministry of Health. Maternal Death Surveillance and Response (MDSR) technical guideline (final draft). Edited by Federal Democratic Republic of Ethiopia Ministry of Health. Addis Ababa, Ethiopia. 2014.
20. Assefa NE, Berhe H, Girma F, et al. Risk factors of premature rupture of membranes in public hospitals at Mekele city, Tigray, a case control study. BMC Pregnancy Childbirth. 2018;18(1):386. doi:10.1186/s12884-018-2016-6
21. Workineh Y, Birhanu S, Kerie S, Ayalew E, Yihune M. Determinants of premature rupture of membrane in Southern Ethiopia, 2017: case control study design. BMC Res Notes. 2018;11(1):927. doi:10.1186/s13104-018-4035-9
22. Nakubulwa S, Kaye DK, Bwanga F, Tumwesigye NM, Mirembe FM. Genital infections and risk of premature rupture of membranes in Mulago Hospital, Uganda: a case control study. BMC Res Notes. 2015;8:573. doi:10.1186/s13104-015-1545-6
23. Federal Democratic Republic of Ethiopia. Ethiopia demographic and health survey. 2016.
24. Getahun D, Strickland D, Ananth CV, et al. Recurrence of preterm premature rupture of membranes in relation to interval between pregnancies. Am J Obstet Gynecol. 2010;202:
25. Choudhary M, Rathore S, Chowdhary J, et al. Pre and post conception risk factors in PROM. Int J Res Med Sci. 2015;3(10):2594–2598. doi:10.18203/2320-6012.ijrms20150797
26. Hackenhaar AA, Albernaz EP, da Fonseca TM, Hackenhaar AA, Albernaz EP, Fonseca TM. Preterm premature rupture of the fetal membranes: association with sociodemographic factors and maternal genitourinary infections. J Pediatr (Rio J). 2014;90(2):197–202. doi:10.1016/j.jped.2013.08.003
27. Kovavisarach E, Sermsak P. Risk factors related to premature rupture of membranes in term pregnant women: a case-control study. Aust NZ J Obstet Gynaecol Zoao. 2000;40(1):3032.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.