")
Back to Journals » Patient Preference and Adherence » Volume 15
Determinants of Non-Adherence to the Medications for Dyslipidemia: A Systematic Review
Received 11 May 2021
Accepted for publication 6 July 2021
Published 24 August 2021 Volume 2021:15 Pages 1853—1871
DOI https://doi.org/10.2147/PPA.S319604
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
João Lopes,1 Paulo Santos1,2
1Department of Community Medicine, Information and Health Decision Sciences (MEDCIDS), Faculty of Medicine, University of Porto, Porto, Portugal; 2CINTESIS - Center for Health Technology and Services Research, University of Porto, Porto, Portugal
Correspondence: João Lopes
Department of Community Medicine, Information and Health Decision Sciences (MEDCIDS), Faculty of Medicine, University of Porto, Alameda Prof. Hernâni Monteiro, Porto, 4200-319, Portugal
Tel +351 220426600
Email [email protected]
Purpose: Dyslipidemia is a major cardiovascular risk factor, and its control leads to less cardiovascular events. Many patients will need some medications to achieve ideal targets. Non-adherence to medications is a complex problem with high impact on their effectiveness. This study aims to identify the determinants of non-adherence to medications in patients with dyslipidemia.
Patients and Methods: We conducted a systematic review. PubMed and Scopus databases were searched for original articles, published between 2000 and 2020, using the MeSH terms “Dyslipidemias” and “Medication Adherence”.
Results: From the initial 3502 identified articles, we selected 46 to include in the final qualitative synthesis. The determinants associated with non-adherence were lower age (≤ 50 years), female sex, African American ethnicity, smoking habits, being a new user of lipid-lowering medications, reporting or having concerns about lipid-lowering medication side effects and some comorbidities (chronic obstructive pulmonary disease, Alzheimer’s disease/dementia, depression and diabetes). On the contrary, adherence is higher in older patients, alcohol drinking habits, taking β-blockers, having a higher number of comorbidities, having a history of cardiovascular events, cardiac interventions or revascularization procedures, having health insurance and having more provider follow-up visits.
Conclusion: There are important identifiable determinants of non-adherence in patients with dyslipidemia. These patients benefit from a specific approach to minimize the problem and maximize the potential benefit of the prescription.
Keywords: medication adherence, dyslipidemias, causality, epidemiologic factors, heart disease risk factors
Introduction
Dyslipidemia is an important risk factor for developing cardiovascular diseases (CVD), the leading cause of death in the world, both for ischemic heart disease1 and stroke.1 In Europe, CVD account for more than 4 million deaths per year, about 45% of the total.2 In this study, we consider dyslipidemia as a broader term, covering a wide range of lipid abnormalities, and not merely having elevated total cholesterol and low-density lipoprotein.3 Therefore, patients were considered as having dyslipidemia if they had any lipid abnormalities that justified treatment, including secondary prevention of cardiovascular events and laboratory confirmation of hypercholesterolemia, hypertriglyceridemia or both. Medication non-adherence is a serious and complex problem. Adherence is defined as the extent to which the patients’ behavior correspond to the agreed recommendation of their doctors, both in taking the medications, following a diet or executing lifestyle changes.4 It depends on several variables related to the condition itself, the therapeutics, the factors related to the patient, including social and cultural features and the health system-related factors. It develops in an interactive triangle of patient, healthcare provider and healthcare system, where each one insert both barriers and facilitators, complementary and interdependently for the outcome.5
About half of patients do not take the medications accordingly to the doctor’s prescription,6 with a significant impact on treatment’s efficacy. Also, non-adherence presents an important economic impact, with annual costs varying from 3347$ to 19,472$ per patient.7
In the context of CVD, non-adherence to medications is associated with significant increase in CVD events8 and higher economic costs.9 It may justify about 9% of all CVD events.10
It is crucial to take action to improve adherence to medications, namely in patients with dyslipidemia. The risk of non-adherence varies with several factors including patients’ characteristics, the disease itself and constraints of health system organizations.5,11 The capacity to predict this risk is an important help to allow a better adjustment of the personalized approach in the decision-making of the clinical consultation. Patients with a predictably higher risk of non-adherence benefit from better attention and greater intervention to improve it, thus better controlling dyslipidemia and consequently the cardiovascular risk. Therefore, it is essential to perceive and better characterize this group of patients with higher risk of non-adherence.
The aim of our study is to identify the determinants of non-adherence to medications in patients with dyslipidemia.
Patients and Methods
In January 2021, we performed a literature search in the PubMed and Scopus databases for all the records published from January 2000 to December 2020 (including), in English, Portuguese and Spanish, using the MeSH terms “Dyslipidemias” and “Medication Adherence”. To organize this systematic review, we used the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).12 All the articles and references were managed using the citation manager software EndNote (version 20).
Study Selection and Data Extraction
The process for selecting studies involved two phases: screening by title and abstract; and assessing the eligibility in full text. Data collected from each study and selected for the final qualitative synthesis, were the study identification (author and citation), study design and setting, patient population size for each study, the type of measure of adherence and the determinants associated with non-adherence. Article screening and data collection were conducted by two independent authors. All differences were discussed and decided by mutual agreement.
Inclusion Criteria
We included studies on patients with dyslipidemia that evaluated the adherence to any dyslipidemia medication, including statins, or the predictors of adherence to medications. We did not include studies evaluating adherence to dyslipidemia guidelines, interventions to improve adherence or validation of such interventions, studies for evaluation or validation of methods to measure medication adherence, studies on adherence trends, and studies of cost or outcome analysis.
Exclusion Criteria
We excluded reviews and case reports, studies involving pediatric populations, studies that assessed concomitantly the adherence to medications to other cardiovascular risk factors beyond dyslipidemia (including antidiabetics and antihypertensives), and studies that limited the population to specific groups, like sex or diseases beyond CVD or cardiovascular risk factors beyond dyslipidemia.
Assessment of Study Quality
To assess the quality of the studies, we used an adapted version of the 2018 Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies from the National Heart Lung and Blood Institute.13 We choose 4 questions out of 14 that compose the tool, based on the adequacy for the proposal of this study: “1. Was the research question or objective in this paper clearly stated?”, “2. Was the study population clearly specified and defined?”, “11. Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants?” and “14. Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)?”. We classified each question in “Yes” (1) or “No” (0) for each study. The resulting score ranged from 0 to 4. Only studies with 2 or more points were considered with the sufficient quality and therefore accepted for inclusion in the final analysis.
Ethical Concerns
Previous ethical appraisal by the ethics committee was not mandatory due to the review nature of this research. Nevertheless, we assumed the commitment to the ethical principles of the Helsinki Declaration, in the conception, analysis and discussion of our results.
Results
We identified 1954 records from PubMed search database and 1548 from the Scopus search database, in a total sample of 2644 articles, after eliminating the duplicates. The screening by title and abstract excluded a total of 2507 records, and the remaining 137 records were selected for a full-text assessment. From this final assessment, 90 articles were excluded. In this phase, 47 studies remained for the inclusion on the qualitative synthesis. The process is summarized in Figure 1.
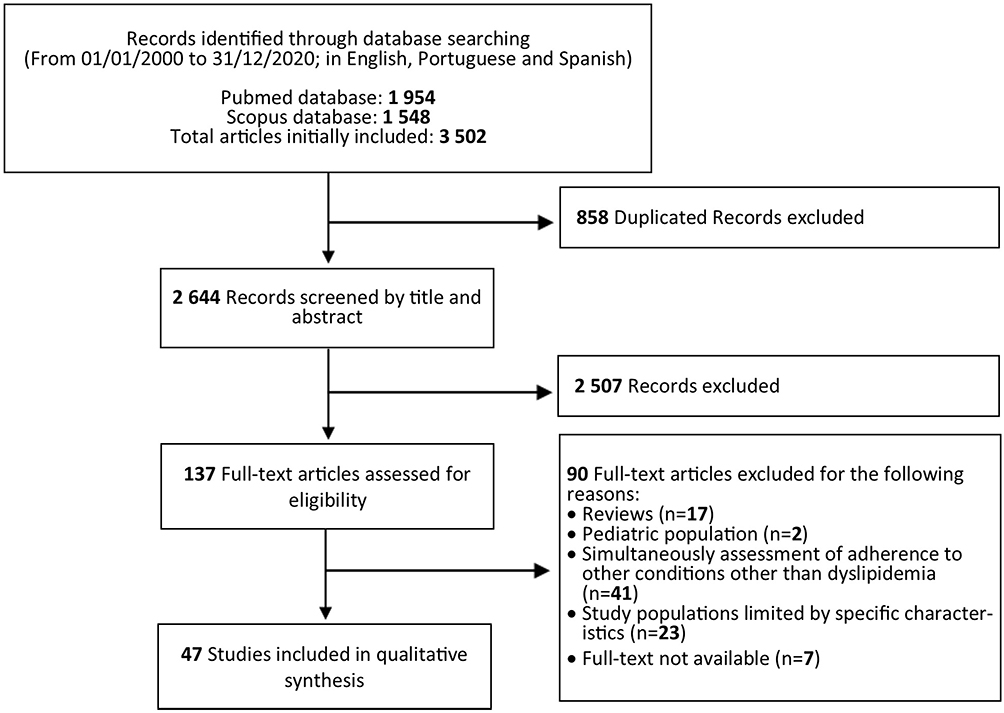 |
Figure 1 PRISMA flow diagram for the review. Notes: PRISMA figure adapted from Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of Clinical Epidemiology. 2009;62(10). Creative Commons.12. |
Quality Assessment
The results of the quality assessment of each article are described in Table 1. From the 47 studies analyzed: 29 had a score of 4, 16 had a score of 3, 1 had a score of 2 and 1 had a score of 1. Consequently, only one study was excluded, and the remaining 46 were included in the final qualitative synthesis.
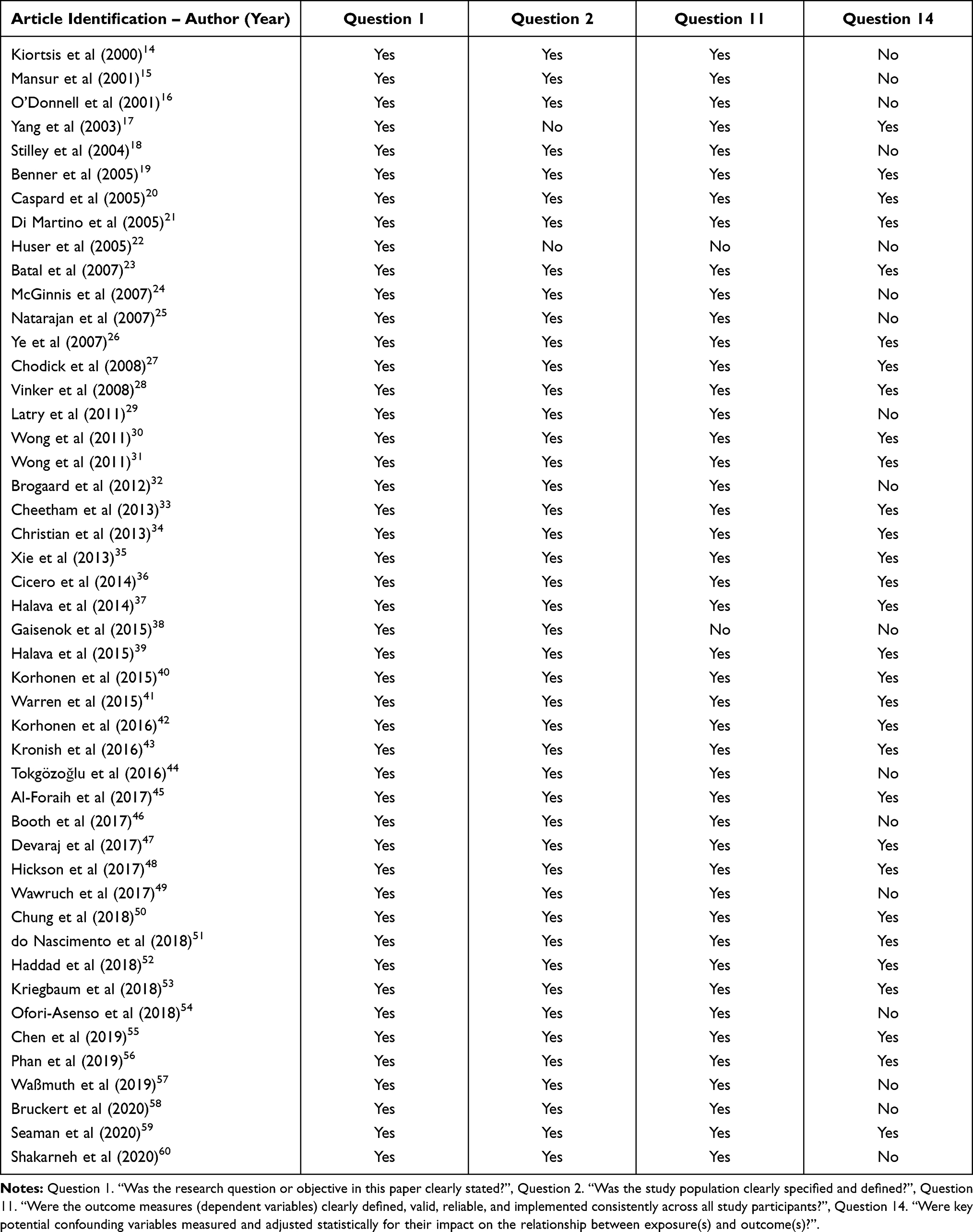 |
Table 1 Quality Assessment of the Articles |
Two authors read independently all 46 studies, searching for outcomes of non-adherence. The studies evaluated non-adherence, adherence, discontinuation, or persistence with medication. All articles were interpreted in a case-by-case approach and considered in terms of non-adherence. The outcomes of non-adherence searched preferentially were statistical measures: odds ratio, risk ratio and hazard ratio. Many studies only presented a qualitative assessment of the results that were also considered.
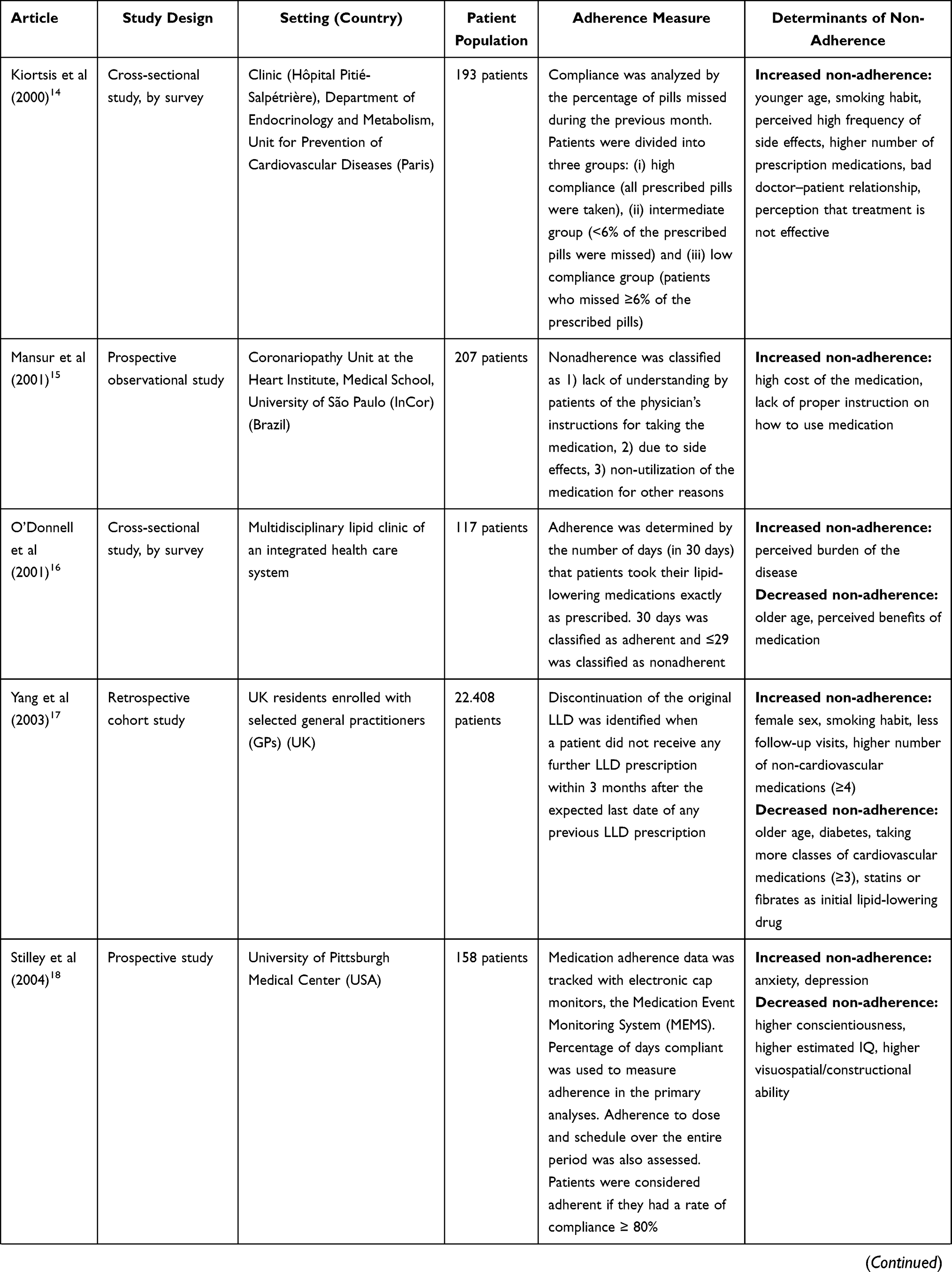
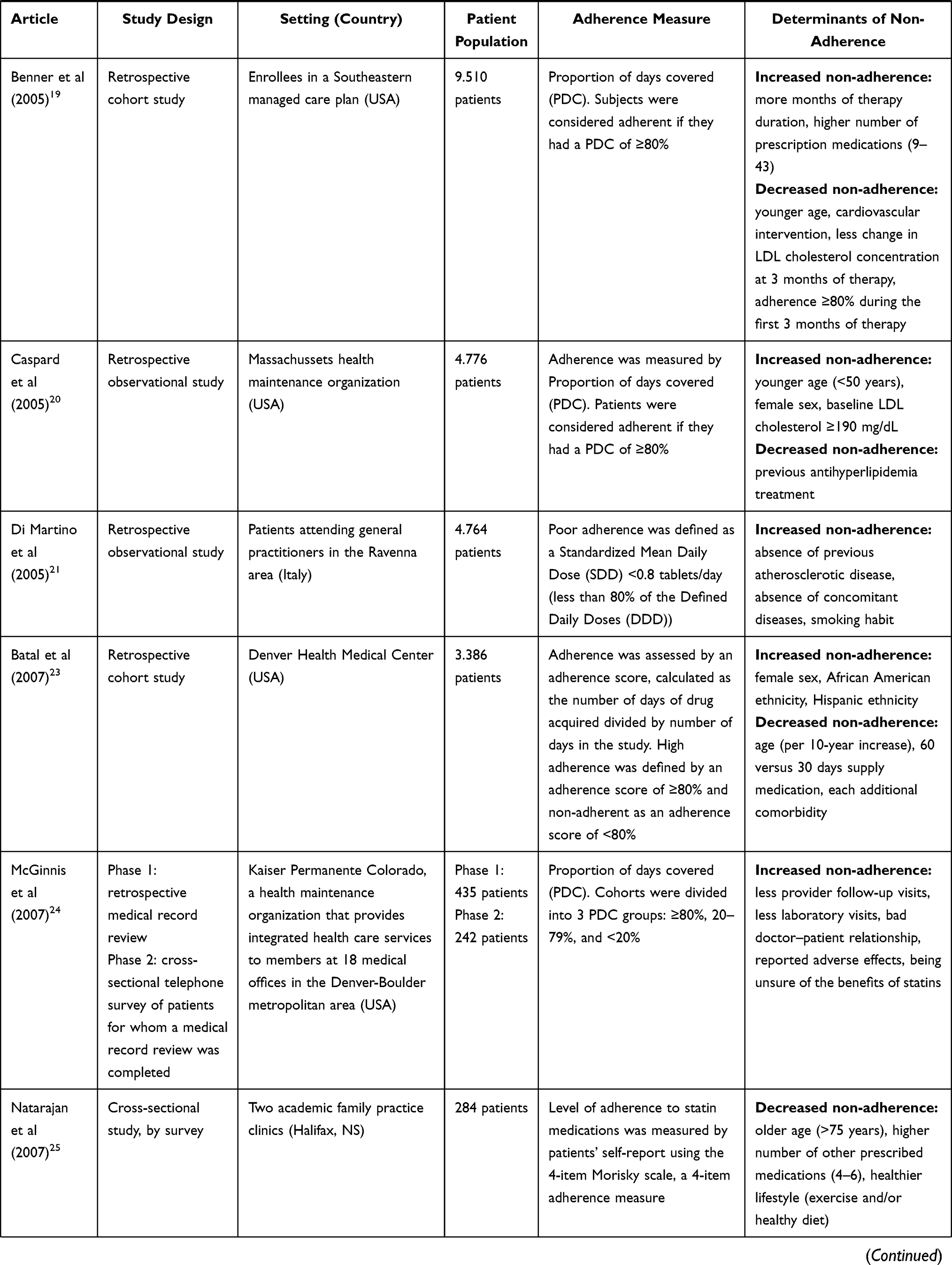
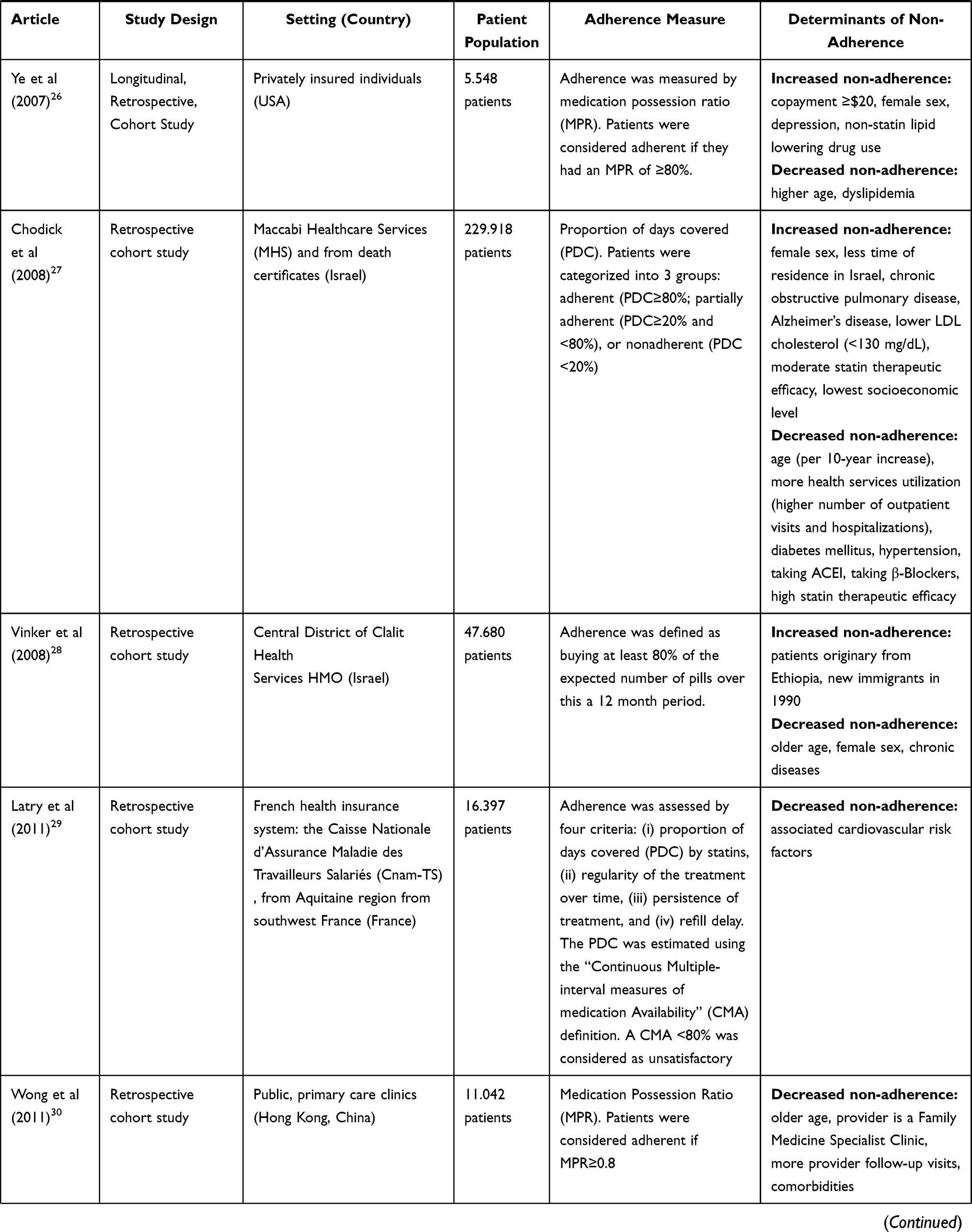
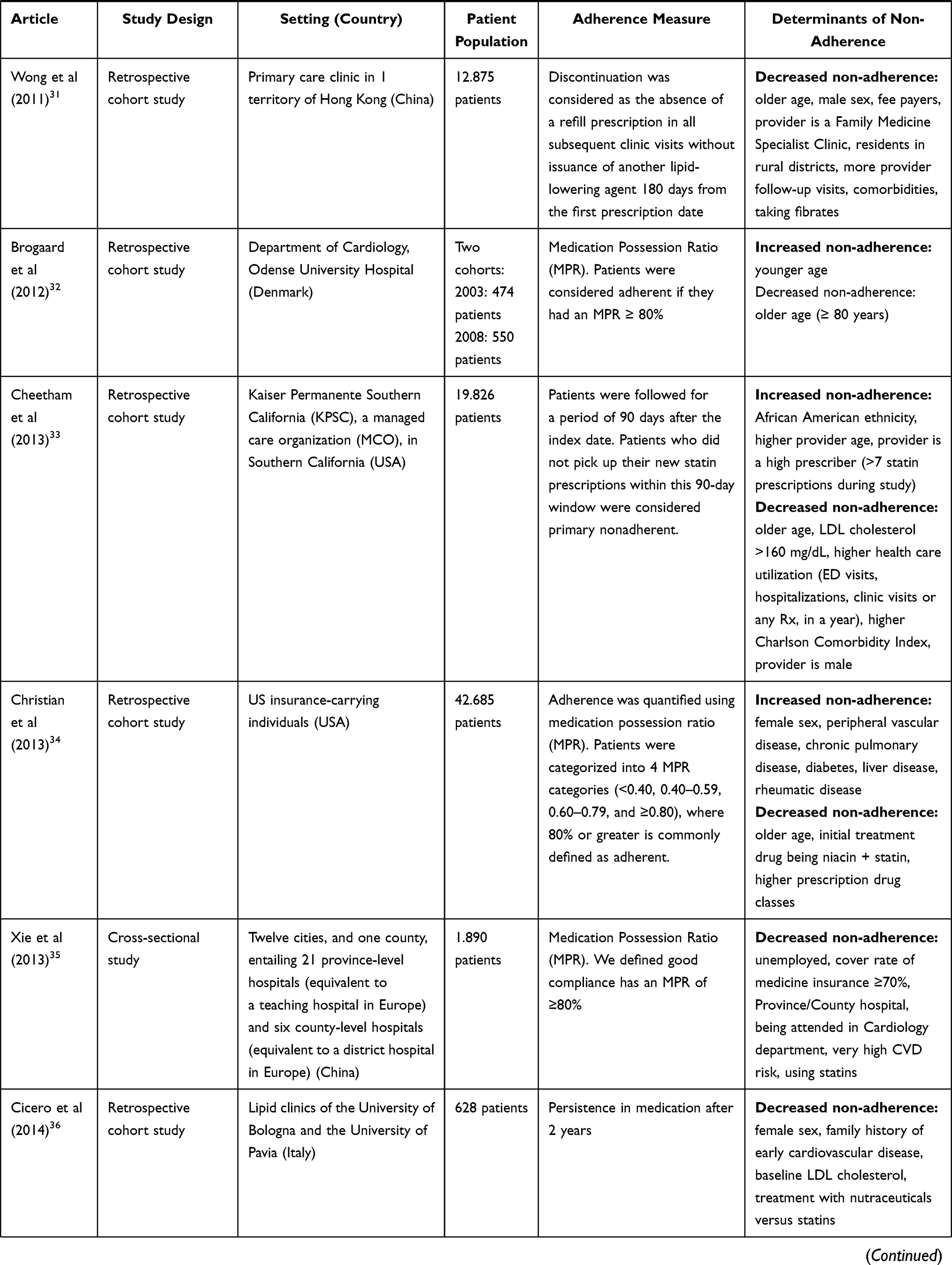
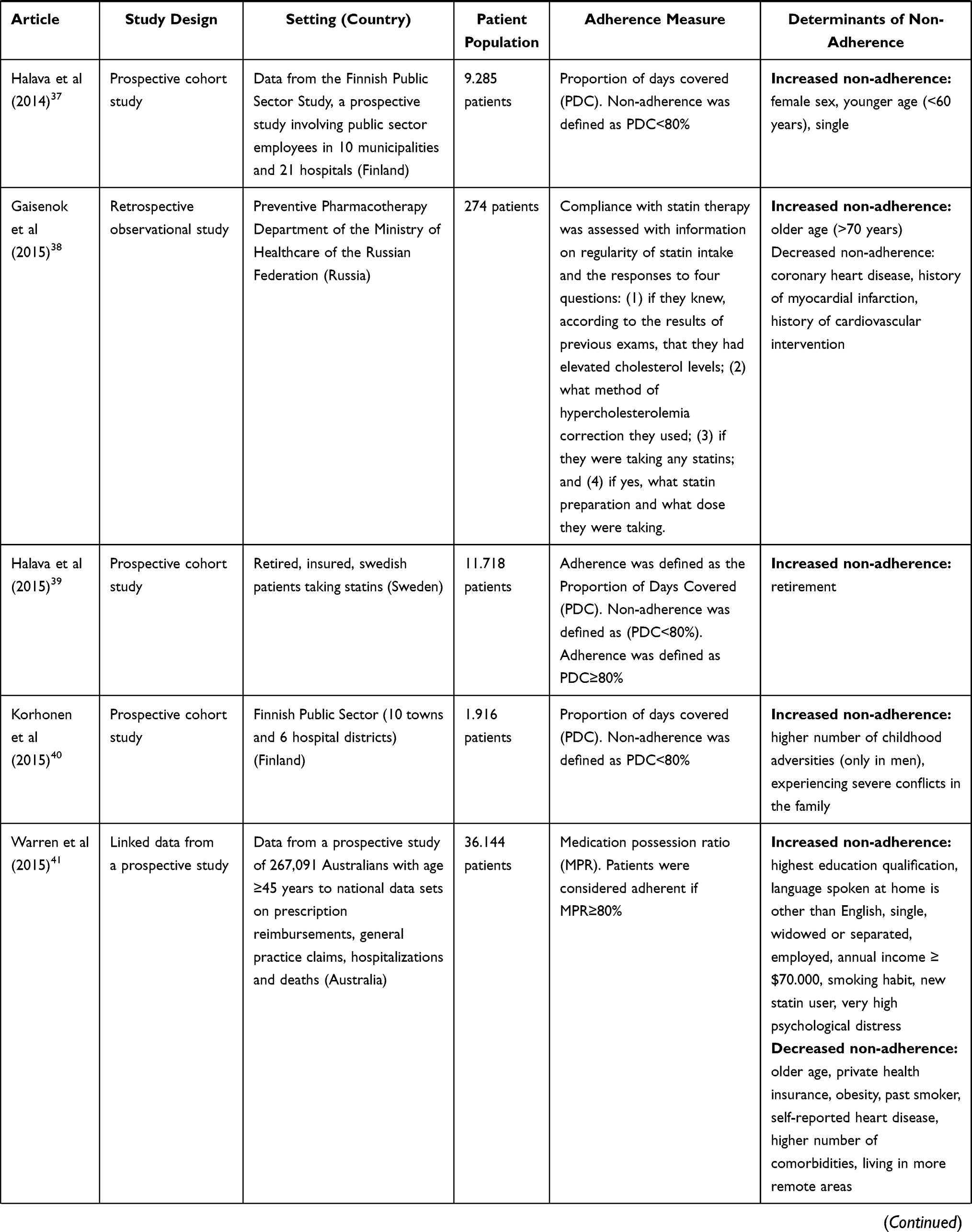
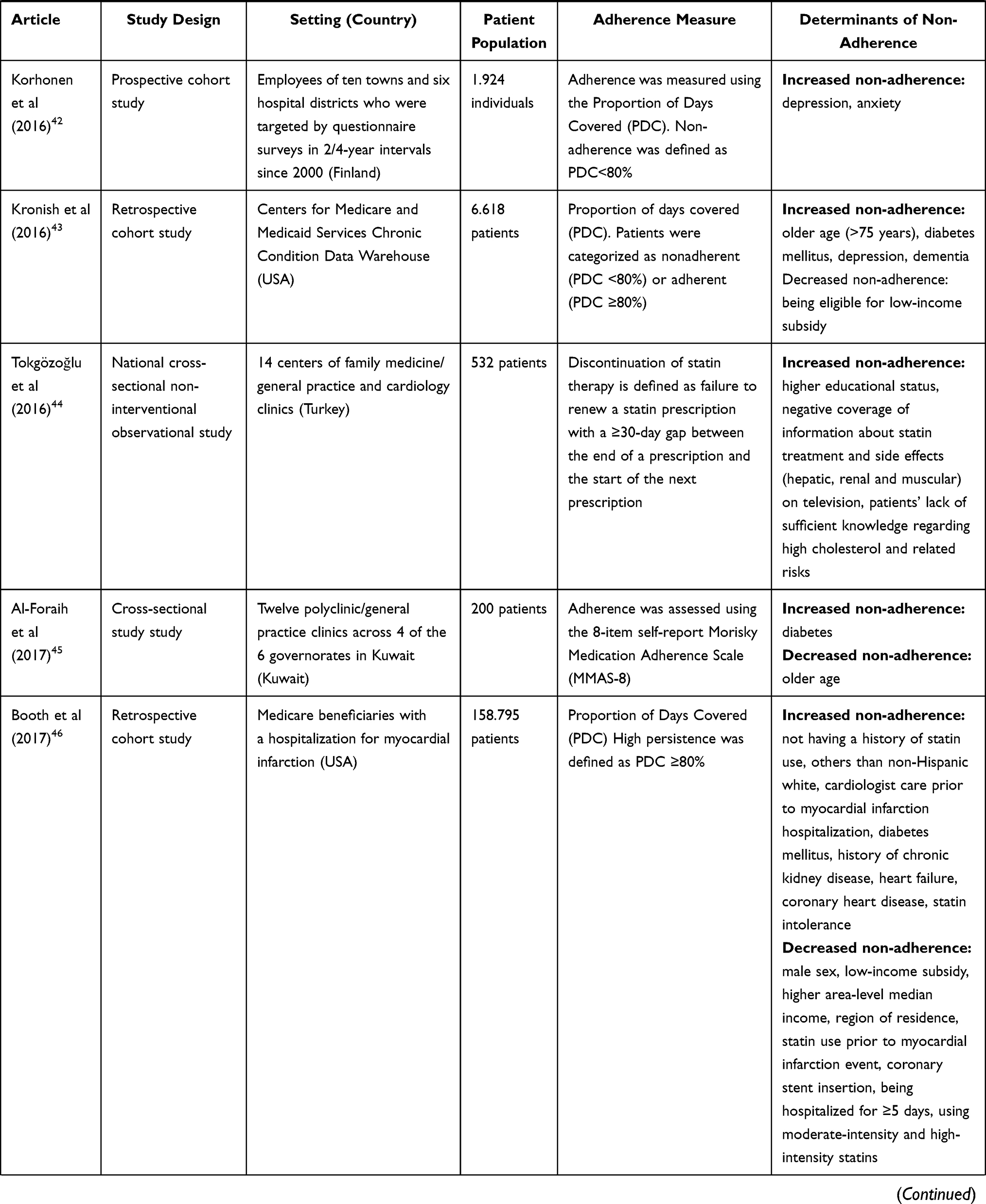
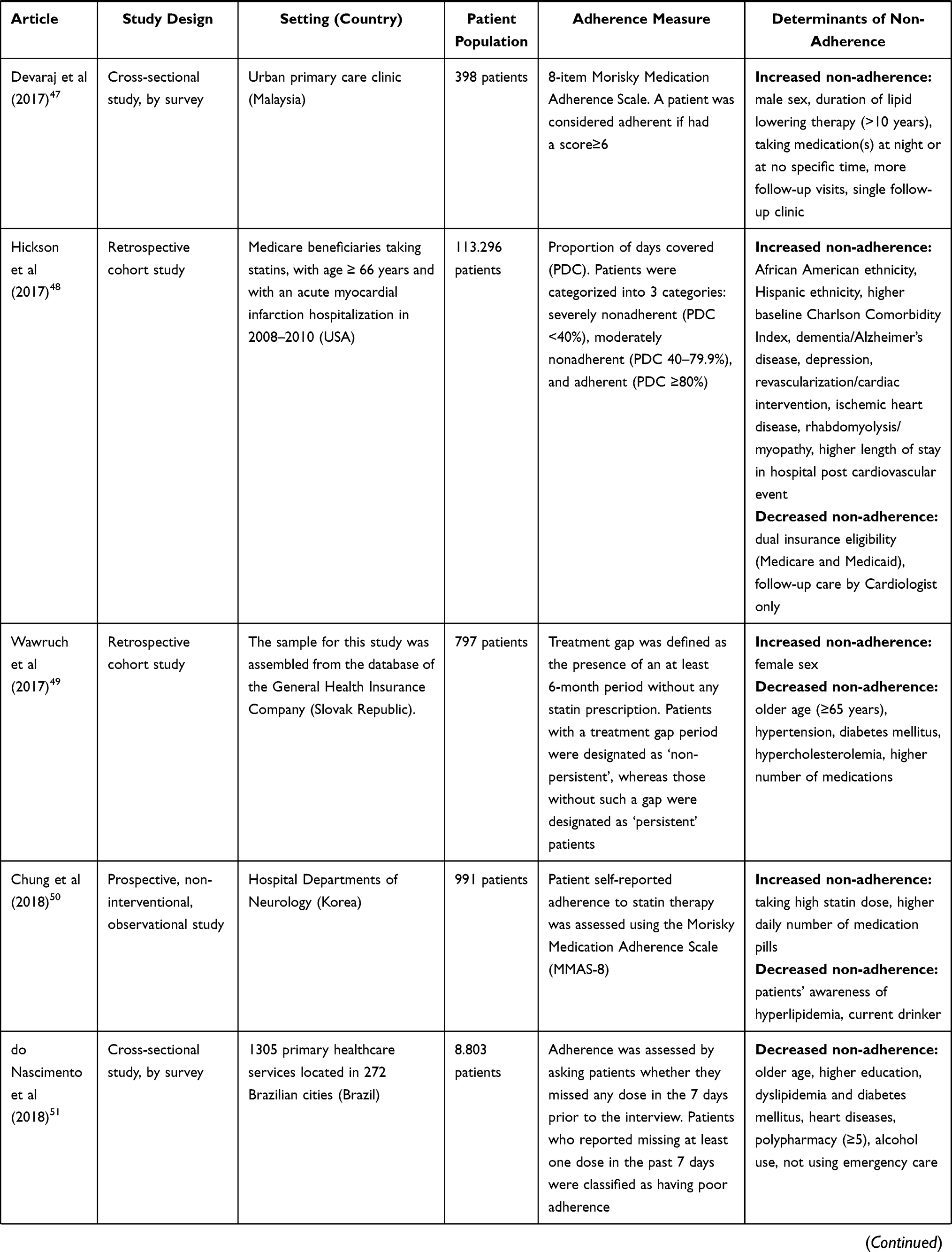
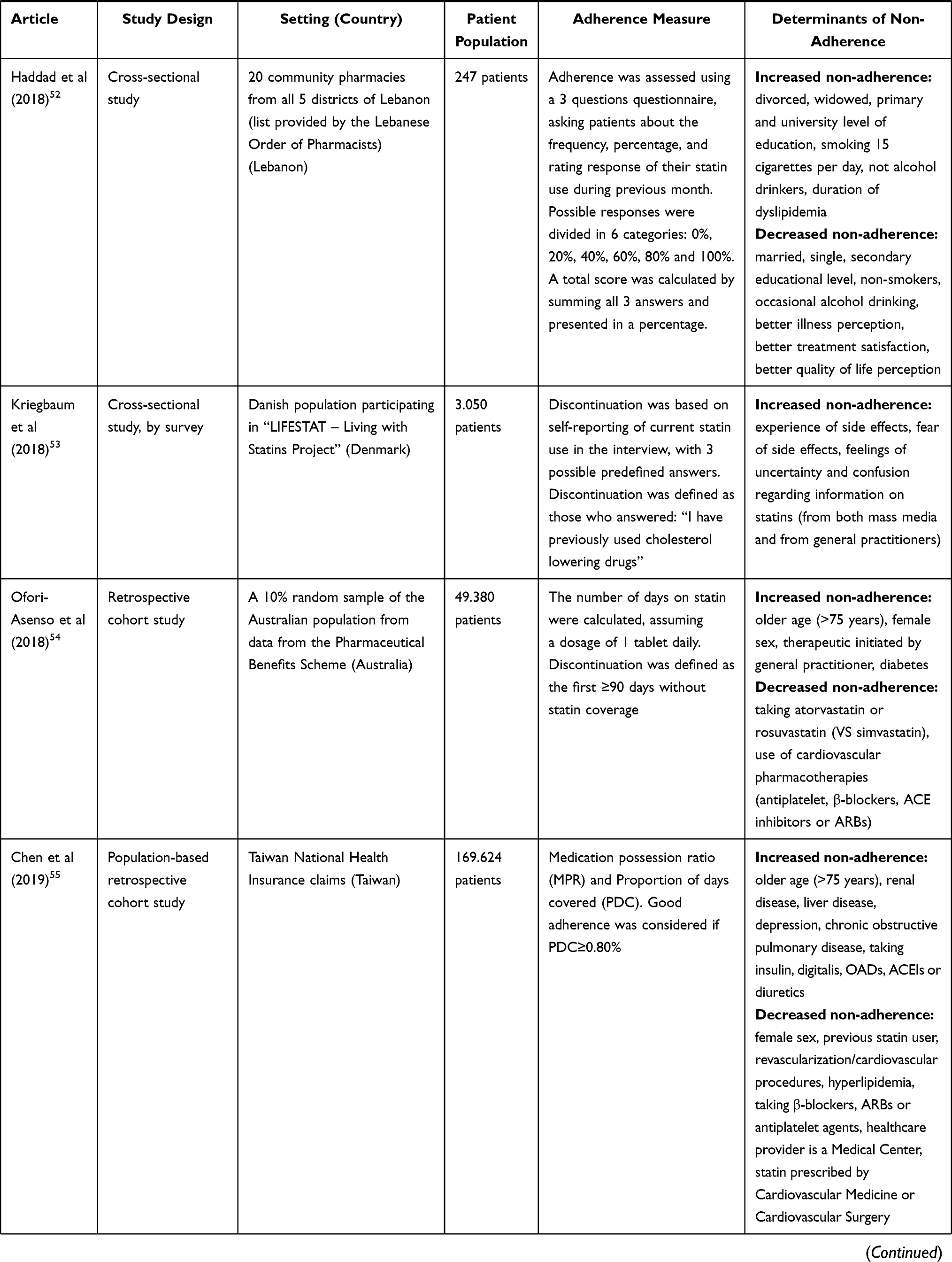
All the variables assessed for each of the 46 articles selected for the final qualitative synthesis are summarized in Table 2. From these 46 observational studies analyzed, 25 were retrospective, 12 cross-sectional studies and 9 prospective cohort studies. The patient’s population in the studies ranged from 117 to 229.918 patients. In terms of measures of adherence, 15 studies used the “Proportion of Days Covered (PDC)”, 7 used the “Medication Possession Ratio (MPR)”, 3 used the “8-item self-report Morisky Medication Adherence Scale (MMAS-8)” and 2 used the “4-item self-report Morisky Medication Adherence Scale (MMAS-4)”. The remaining 18 studies had a more specific measure of adherence, designed for each, individually.
 |
 |
 |
 |
 |
 |
 |  |
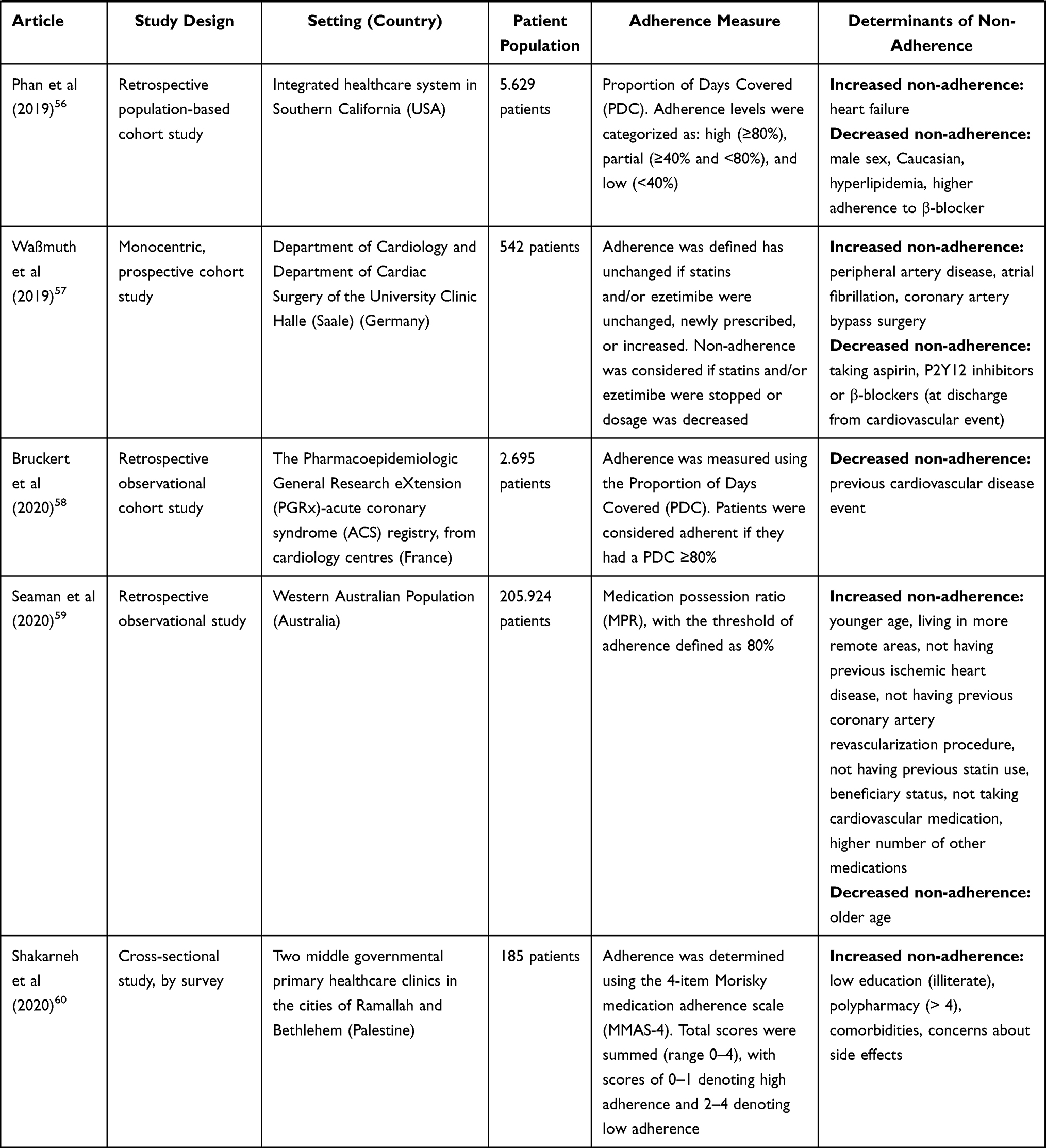 |
Table 2 Articles Assessed in Qualitative Synthesis |
Determinants for Non-Adherence to Medications
We found several relevant determinants associated with non-adherence, summarized in Table 3.
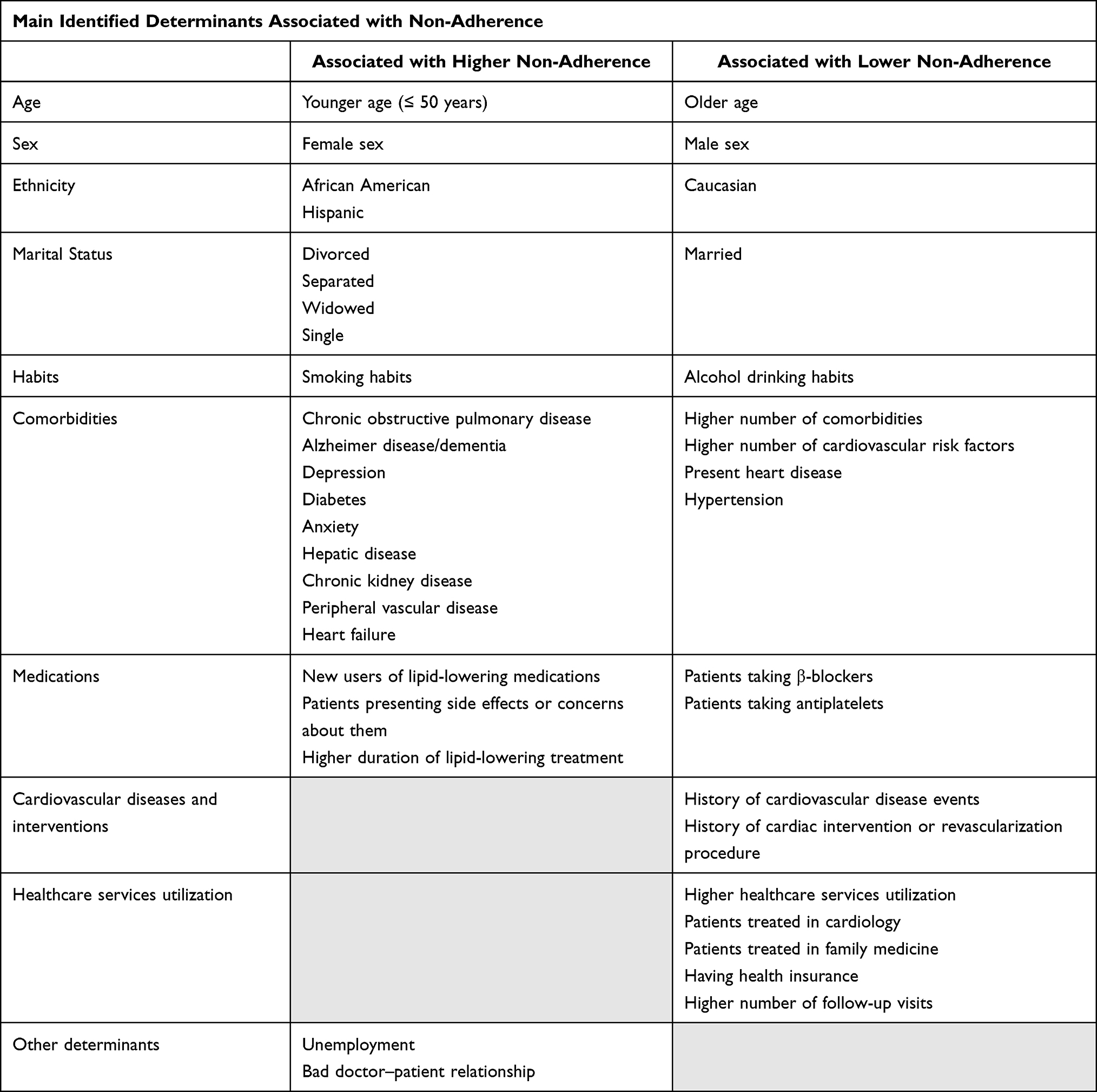 |
Table 3 Main Determinants Associated with Non-Adherence |
Sociodemographic Variables
Age
Non-adherence decreases with age.16,26,33,45 For each 10-year increase in age, the risk of non-adherence decreases about 5–11%.23,27 Analyzing particular age groups, we observed the same trend of decreasing non-adherence with higher age. Non-adherence is higher in younger patients (age ≤ 50 years),14,32,37,59 reaching values of 50%.20 It is lower between 50 and 70 years (8–34%),17,19,20,28,30,31,41 and in older patients (age ≥ 70 years),25,30,31,59 who present the risk of non-adherence of 11–65%.17,28,41,49
Sex
In general, females are more non-adherent than males,26,31,34,37,46,56 with an increased risk of 5–31%.17,20,23,27,49,54
Ethnicity
Several studies show an increase of non-adherence in African American patients,33,48 up to 30%.23 Hispanics23,48 are also associated with worst adherence to medications.
Marital Status
Non-adherence is lower in married patients,52 higher in single patients37,41 and increased in divorced, separated or widowed patients.41,52
Employment Status
Non-adherence is worst in unemployed.35,41
Lifestyle Variables
Smoking Status
Non-adherence is higher in current smokers,14,41,52 with an increase of 18–163%.17,21
Alcohol Drinking Status
Non-adherence is lower in active alcohol drinkers,52 showing values of odds ratio between 0.61 and 0.71.50,51
Medication Use
Several conditions regarding medications are associated with non-adherence. In general, non-adherence is higher in new users of lipid-lowering medications,20,46,55,59 justifying up to 47% more risk.41 Also, in patients presenting side effects or expressing concerns about them, non-adherence is higher,14,24,53 with an associated odds ratio of 2.89.60 Non-adherence is also worst in patients having a higher duration of lipid-lowering treatment.19,47 On the other hand, several studies have shown that non-adherence is lower in patients taking β-blockers,55–57 who have approximately less 12% risk of non-adherence27,54 as in patients taking other cardiovascular medications.17,24,59
Comorbidities/Disease Status
Number of Patients’ Comorbidities
Non-adherence decreases with a higher number of comorbidities. For each comorbidity present, the risk of non-adherence decreases by 4%.23 This is apparent since the first comorbidity,30,31,41 leading to 5% improvement.41 This is even more apparent in patients with two or more comorbidities,30,31,41 with a 7–8% improvement in adherence.41 Inversely, the absence of concomitant diseases is associated with a 59% increase in the risk of non-adherence.21
Type of Comorbidity
Several comorbidities are identified as especially associated with higher non-adherence: chronic obstructive pulmonary disease,34,55 with a 7–10% increased risk;27 Alzheimer’s disease or other dementias,48 with a 20% increased risk;27,43 depression,18,26,48,55 with a 9–15% increased risk;42,43 diabetes,34,45,46 with a 7–10% increased risk of non-adherence;43,54 anxiety;18,42 hepatic disease;34,55 chronic kidney disease;46,55 peripheral vascular disease;34,57 and heart failure.46,56
On the other hand, non-adherence is lower in patients with present heart diseases,41,51 in patients with a higher number of cardiovascular risk factors,29,35 in patients with hypertension27,49 and in patients taking antiplatelets.54,55
Cardiovascular Diseases and Interventions
The history of cardiovascular disease events is associated with lower non-adherence.38,58,59 Patients with a previous cardiac intervention or a revascularization procedure, present lower non-adherence,46,59 with odds ratio of 0.19–0.68.19,38,55 Patients without a previous atherosclerotic event present 135% more risk of non-adherence.21
Healthcare Related Variables
Healthcare Services Utilization
Non-adherence is decreased in patients with higher healthcare services utilization.27,33 It is also influenced by providers, with cardiology35,48 and family medicine30,31 contributing for lower levels of non-adherence.
Having Health Insurance
Non-adherence is lower in patients who had health insurance.35,48 These patients have 3–5% less risk of non-adherence.41
Follow-Up Visits
The follow-up visits are associated with lower non-adherence,24,30,31 with an impact on the risk of 60%.17
Physician–Patient Relationship
Having a bad doctor–patient relationship14,24 is associated with increased non-adherence.
Discussion
Adherence is a cornerstone of the effectiveness of the medications. The best therapeutic will never work if the patient does not take it. In this review, we identify a set of determinants related to non-adherence to medications in patients with dyslipidemia. Although the different weight, each characteristic is associated with a significant variation in non-adherence, allowing to adjust and to personalize the therapeutic decision in these patients. The more of these conditions the higher should be our concern about the risk of non-adherence in the patient.
Our review included studies related to dyslipidemia, in a broader approach, to find a wide range of factors related to adherence. Our results are in line with other studies. Ofori-Asenso et al published a systematic review with meta-analysis, focused on the non-adherence to statins in patients aged ≥65 years.61 It included 45 articles and identified the female sex, African American ethnicity, new lipid-lowering drug users, taking lower number of cardiovascular medications and having depression as factors associated with higher non-adherence. Contrary to our findings, this study identified kidney disease as a factor for decreased non-adherence. Mann et al also reviewed 22 cohort studies with meta-analysis, focusing on non-adherence to statins. He described a U-shaped association with age, higher in the younger and in the elderly and lower in middle ages, as in patients with diabetes.62 Unlike other reviews, we focused on patients with dyslipidemia, irrespective of the medication, and tried obtaining practical and objective information that could allow physicians to rapidly consult that information in a context of a consultation, namely on the visit where the first prescription occurs.
A difficulty in our review was the differences observed between the studies: the different study designs; different sample sizes of study population; different tools to measure adherence (“Proportion of Days Covered (PDC)”, “Medication Possession Ratio (MPR)”, the “8-item self-report Morisky Medication Adherence Scale (MMAS-8)”, the “4-item self-report Morisky Medication Adherence Scale (MMAS-4)”); different outcomes (many evaluated non-adherence, but others evaluated adherence, discontinuation, persistence); and the way to quantify them (odds ratio, risk ratio, hazard ratio, or a simple qualitative assessment). This heterogeneity does not seem to be enough to condition our results, as more than the quantification of non-adherence, it was more important to identify their causes. Some factors that our review does not account for are the impact of media and more precisely social media platforms. In fact, in today’s society, these platforms of social interaction are of the utmost relevance as, in our view, they can contribute to changes in patients’ perceptions and preconceptions regarding medications. We think that this reality possibly negatively influences patients’ medical literacy and could, in most cases, create misconceptions and negatively affect patients’ motivation to adhere to medications, undermining the importance of adherence.
This review allows to draw the profile of the non-adherent patient, to whom we should pay special attention and a hard intervention to lead them to take the lipid-lowering medications appropriately, in their own benefit. Several strategies help to enhance the adherence to medications.63 First of all, it is really important that healthcare providers can detect non-adherence. This should be a systematic practice in every visit, in every patient, to quantify the problem and to register it in the clinical file. There are many ways to do it, both directly (counting pills or renewal of the prescriptions) or indirectly (by questionnaire or by comparison with the expected effect). Then, we must think about the best simplification of the regimen (using longer acting drugs or pills combing several drugs, adapting drug regimen to patients’ daily activities and preferences, and thoroughly introducing the therapeutic regimen, gradually increasing complexity). Literacy plays a major role.64 Patients need to be aware of their disease and the associated risks. We must be sure that they, and most of times also their families, understand reasonably the instructions and have enough time to express their expectations, their fears and doubts:65 using a simple and clear language; writing the instructions and letting the patient to repeat them; giving the patient several options, if possible. Communication skills are crucial, as it is a good doctor–patient relationship and the continuity of care, creating a trustful environment and empathy. The strengthened therapeutic alliance facilitates the sharing of responsibility toward health, where physicians and patients play their own specific role. Time is also a major factor to consider, as it is increasingly scarce in nowadays medical practice. Indeed, all the above items require time: time investment in the visit, time to listen to the patients and time to establish a real and meaningful doctor–patient relationship.
This review provides a synthesis of the determinants for non-adherence in patients with dyslipidemia in a practical perspective. Our results allow the physicians to identify the factors in each patient and adjust their intervention to better deal with the risk of non-adherence in a preventive approach. With this information, the healthcare providers may better estimate the probability of non-adherence of the patient since the initial evaluation. Patients with higher probability of non-adherence would benefit from earlier and more robust approach to minimize the risk of not taking the medications. Logically, being a qualitative assessment, this probability is subjective and is highly dependent on the physician expertise and experience to evaluate the patient in each visit. Perhaps more work to further assess the determinants of non-adherence and the posterior development of a score based on that information could allow a more objective approach to these situations, further facilitating the systematization of this practice of evaluation of non-adherence profiles.
In the future, more research is necessary to further understand the weight of the different aspects and the way they interact with each other, including the patients’ preferences, expectations and perceptions. More than a disease, dyslipidemia is a cardiovascular risk factor. Its treatment is mainly a preventive approach, and the efficacy is the non-occurrence of the event. This is very different from myocardial infarction, stroke or heart failure, where every measure presents a quick effect, measurable by the patient’s own perception. In fact, patient’s perception of the importance of adherence in dyslipidemia, along with the associated potential benefit, is a fundamental part of the problem that we ought to collectively improve.
Conclusion
There are important identifiable determinants of non-adherence in patients with dyslipidemia. Healthcare providers should identify such characteristics to approach patients in a personalized way, investing more time in improving adherence. These patients benefit from a specific approach to minimize the problem of non-adherence and improve the therapeutic success, improve health and save lives.
Disclosure
The authors report no conflict of interests in this work.
References
1. Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937–952. doi:10.1016/S0140-6736(04)17018-9
2. Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M. Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J. 2016;37(42):3232–3245. doi:10.1093/eurheartj/ehw334
3. Catapano AL, Graham I, De Backer G, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: the Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;2999–3058. doi:10.1093/eurheartj/ehw272
4. Sabaté E; World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. Vol. xv. World Health Organization; 2003:198. Available from: http://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf;jsessionid=28AA4EDC4BD4B97052696A4F4990D5D0?sequence=1. Accessed Aug 17, 2021.
5. Osterberg L, Blaschke T. Adherence to medication. Review. N Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
6. Naderi SH, Bestwick JP, Wald DS. Adherence to drugs that prevent cardiovascular disease: meta-analysis on 376,162 patients. Am J Med. 2012;125(9):882–7.e1. doi:10.1016/j.amjmed.2011.12.013
7. Cutler RL, Fernandez-Llimos F, Frommer M, Benrimoj C, Garcia-Cardenas V. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open. 2018;8(1):e016982. doi:10.1136/bmjopen-2017-016982
8. De Vera MA, Bhole V, Burns LC, Lacaille D. Impact of statin adherence on cardiovascular disease and mortality outcomes: a systematic review. Br J Clin Pharmacol. 2014;78(4):684–698. doi:10.1111/bcp.12339
9. Bitton A, Choudhry NK, Matlin OS, Swanton K, Shrank WH. The impact of medication adherence on coronary artery disease costs and outcomes: a systematic review. Am J Med. 2013;126(4):
10. Chowdhury R, Khan H, Heydon E, et al. Adherence to cardiovascular therapy: a meta-analysis of prevalence and clinical consequences. Eur Heart J. 2013;34(38):2940–2948. doi:10.1093/eurheartj/eht295
11. Carvalho AS, Santos P. Medication adherence in patients with arterial hypertension: the relationship with healthcare systems’ organizational factors. Original. Patient Prefer Adherence. 2019;13:1761–1774. doi:10.2147/PPA.S216091
12. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
13. National Heart Lung and Blood Institute. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies [internet]. National Institutes of Health; 2021 [cited 2021 Mar 31] Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. Accessed August 23, 2021.
14. Kiortsis DN, Giral P, Bruckert E, Turpin G. Factors associated with low compliance with lipid-lowering drugs in hyperlipidemic patients. J Clin Pharm Ther. 2000;25(6):445–451. doi:10.1046/j.1365-2710.2000.00315.x
15. Mansur AP, Mattar APL, Tsubo CE, Simão DT, Yoshi FR, Daci K. Prescription and adherence to statins of patients with coronary artery disease and hypercholesterolemia. Article. Arq Bras Cardiol. 2001;76(2):111–118. doi:10.1590/S0066-782X2001000200002
16. O’Donnell DC, Brown CM, Piziak VK. Alternative therapy use and adherence to antihyperlipidemic drugs in a lipid clinic. Note. Ame J Health Syst Pharm. 2001;58(11):1017–1021. doi:10.1093/ajhp/58.11.1017
17. Yang CC, Jick SS, Testa MA. Discontinuation and switching of therapy after initiation of lipid-lowering drugs: the effects of comorbidities and patient characteristics. Br J Clin Pharmacol. 2003;56(1):84–91. doi:10.1046/j.1365-2125.2003.01818.x
18. Stilley CS, Sereika S, Muldoon MF, Ryan CM, Dunbar-Jacob J. Psychological and cognitive function: predictors of adherence with cholesterol lowering treatment. Ann Behav Med. 2004;27(2):117–124. doi:10.1207/s15324796abm2702_6
19. Benner JS, Pollack MF, Smith TW, Bullano MF, Willey VJ, Williams SA. Association between short-term effectiveness of statins and long-term adherence to lipid-lowering therapy. Am J Health Syst Pharm. 2005;62(14):1468–1475. doi:10.2146/ajhp040419
20. Caspard H, Chan AK, Walker AM. Compliance with a statin treatment in a usual-care setting: retrospective database analysis over 3 years after treatment initiation in health maintenance organization enrollees with dyslipidemia. Clin Ther. 2005;27(10):1639–1646. doi:10.1016/j.clinthera.2005.10.005
21. Di Martino M, Degli Esposti L, Ruffo P, et al. Underuse of lipid-lowering drugs and factors associated with poor adherence: a real practice analysis in Italy. Eur J Clin Pharmacol. 2005;61(3):225–230. doi:10.1007/s00228-005-0911-z
22. Huser MA, Evans TS, Berger V. Medication adherence trends with statins. Article. Adv Ther. 2005;22(2):163–171. doi:10.1007/BF02849887
23. Batal HA, Krantz MJ, Dale RA, Mehler PS, Steiner JF. Impact of prescription size on statin adherence and cholesterol levels. BMC Health Serv Res. 2007;7:175. doi:10.1186/1472-6963-7-175
24. McGinnis B, Olson KL, Magid D, et al. Factors related to adherence to statin therapy. Ann Pharmacother. 2007;41(11):1805–1811. doi:10.1345/aph.1K209
25. Natarajan N, Putnam RW, Yip AM, Frail D. Family practice patients’ adherence to statin medications. Can Fam Physician. 2007;53(12):2144–2145.
26. Ye X, Gross CR, Schommer J, Cline R, St. Peter WL. Association between copayment and adherence to statin treatment initiated after coronary heart disease hospitalization: a longitudinal, retrospective, cohort study. Article. Clin Ther. 2007;29(12):2748–2757. doi:10.1016/j.clinthera.2007.12.022
27. Chodick G, Shalev V, Gerber Y, et al. Long-term persistence with statin treatment in a not-for-profit health maintenance organization: a population-based retrospective cohort study in Israel. Article. Clin Ther. 2008;30(11):2167–2179. doi:10.1016/j.clinthera.2008.11.012
28. Vinker S, Shani M, Baevsky T, Elhayany A. Adherence with statins over 8 years in a usual care setting. Am J Manag Care. 2008;14(6):388–392.
29. Latry P, Molimard M, Dedieu B, Couffinhal T, Bégaud B, Martin-Latry K. Adherence with statins in a real-life setting is better when associated cardiovascular risk factors increase: a cohort study. BMC Cardiovasc Disord. 2011;11:46. doi:10.1186/1471-2261-11-46
30. Wong MC, Jiang JY, Griffiths SM. Adherence to lipid-lowering agents among 11,042 patients in clinical practice. Int J Clin Pract. 2011;65(7):741–748. doi:10.1111/j.1742-1241.2011.02706.x
31. Wong MCS, Jiang JY, Yan BP, Griffiths SM. Subjects at risk of discontinuation of lipid-lowering agents: a 6-month cohort study among 12,875 patients in a Chinese population. Article. Clin Ther. 2011;33(5):617–628. doi:10.1016/j.clinthera.2011.04.019
32. Brogaard HV, Køhn MG, Berget OS, et al. Significant improvement in statin adherence and cholesterol levels after acute myocardial infarction. Dan Med J. 2012;59(9):A4509.
33. Cheetham TC, Niu F, Green K, et al. Primary nonadherence to statin medications in a managed care organization. J Manag Care Pharm. 2013;19(5):367–373. doi:10.18553/jmcp.2013.19.5.367
34. Christian JB, Rabatin V, Lowe KA. Adherence, persistence, and predictors associated with early niacin termination. Article. J Pharm Technol. 2013;29(4):178–185. doi:10.1177/875512251302900406
35. Xie G, Zaman MJ, Myint PK, Liang L, Zhao L, Wu Y. Factors associated with compliance to lipid-lowering treatment in China. Eur J Prev Cardiol. 2013;20(2):229–237. doi:10.1177/2047487312438847
36. Cicero AF, Derosa G, Parini A, Baronio C, Borghi C. Factors associated with 2-year persistence in fully non reimbursed lipid-lowering treatments. Atherosclerosis. 2014;235(1):81–83. doi:10.1016/j.atherosclerosis.2014.04.016
37. Halava H, Korhonen MJ, Huupponen R, et al. Lifestyle factors as predictors of nonadherence to statin therapy among patients with and without cardiovascular comorbidities. Article. CMAJ. 2014;186(12):E449–E456. doi:10.1503/cmaj.131807
38. Gaisenok O, Martsevich S, Tripkosh S, Lukina Y. Analysis of lipid-lowering therapy and factors affecting regularity of statin intake in patients with cardiovascular disease enrolled in the PROFILE registry. Rev Port Cardiol. 2015;34(2):111–116. doi:10.1016/j.repc.2014.08.021
39. Halava H, Westerlund H, Korhonen MJ, et al. Influence of retirement on adherence to statins in the insurance medicine all-Sweden total population data base. PLoS One. 2015;10(6):e0130901. doi:10.1371/journal.pone.0130901
40. Korhonen MJ, Halonen JI, Brookhart MA, et al. Childhood adversity as a predictor of non-adherence to statin therapy in adulthood. PLoS One. 2015;10(5):e0127638. doi:10.1371/journal.pone.0127638
41. Warren JR, Falster MO, Tran B, Jorm L. Association of continuity of primary care and statin adherence. PLoS One. 2015;10(10):e0140008. doi:10.1371/journal.pone.0140008
42. Korhonen MJ, Pentti J, Hartikainen J, Kivimäki M, Vahtera J. Somatic symptoms of anxiety and nonadherence to statin therapy. Int J Cardiol. 2016;214:493–499. doi:10.1016/j.ijcard.2016.04.003
43. Kronish IM, Ross JS, Zhao H, Muntner P. Impact of hospitalization for acute myocardial infarction on adherence to statins among older adults. Circ Cardiovasc Qual Outcomes. 2016;9(4):364–371. doi:10.1161/circoutcomes.115.002418
44. Tokgözoğlu L, Özdemir R, Altındağ R, et al. Patient characteristics and statin discontinuation-related factors during treatment of hypercholesterolemia: an observational non-interventional study in patients with statin discontinuation (STAY study). Turk Kardiyol Dern Ars. 2016;44(1):53–64. doi:10.5543/tkda.2015.47041
45. Al-Foraih M, Somerset S. Factors affecting adherence to statins in hypercholesterolemic Kuwaiti patients: a Cross-Sectional Study. Med Princ Pract. 2017;26(1):35–40. doi:10.1159/000450644
46. Booth JN
47. Devaraj NK, Mohamed M, Hussein N. Prevalence, factors influencing and knowledge about adherence to lipid-lowering therapy among hyperlipidemia patients. Med J Malaysia. 2017;72(3):157–164.
48. Hickson RP, Robinson JG, Annis IE, et al. Changes in statin adherence following an acute myocardial infarction among older adults: patient predictors and the association with follow-up with primary care providers and/or cardiologists. J Am Heart Assoc. 2017;6(10):e007106. doi:10.1161/jaha.117.007106
49. Wawruch M, Zatko D, Wimmer G
50. Chung PW, Yoon BW, Lee YB, et al. Medication adherence of statin users after acute ischemic stroke. Eur Neurol. 2018;80(1–2):106–114. doi:10.1159/000493530
51. Do Nascimento R, Guerra AA
52. Haddad C, Hallit S, Salhab M, et al. Association between adherence to statins, illness perception, treatment satisfaction, and quality of life among Lebanese patients. Article. J Cardiovasc Pharmacol Ther. 2018;23(5):414–422. doi:10.1177/1074248418769635
53. Kriegbaum M, Lau SR. Medication non-adherence and uncertainty: information-seeking and processing in the Danish LIFESTAT survey. Res Social Adm Pharm. 2018;14(8):736–741. doi:10.1016/j.sapharm.2017.09.002
54. Ofori-Asenso R, Ilomaki J, Tacey M, et al. Switching, discontinuation, and reinitiation of statins among older adults. J Am Coll Cardiol. 2018;72(21):2675–2677. doi:10.1016/j.jacc.2018.08.2191
55. Chen ST, Huang ST, Shau WY, et al. Long-term statin adherence in patients after hospital discharge for new onset of atherosclerotic cardiovascular disease: a population-based study of real world prescriptions in Taiwan. BMC Cardiovasc Disord. 2019;19(1):62. doi:10.1186/s12872-019-1032-4
56. Phan DQ, Duan L, Lam B, et al. Statin adherence and mortality in patients aged 80 years and older after acute myocardial infarction. J Am Geriatr Soc. 2019;67(10):2045–2049. doi:10.1111/jgs.16037
57. Waßmuth S, Rohe K, Noack F, Noutsias M, Treede H, Schlitt A. Adherence to lipid-lowering therapy in patients with coronary heart disease from the state of saxony-anhalt, Germany. Article. Vasc Health Risk Manag. 2019;15:477–483. doi:10.2147/VHRM.S197089
58. Bruckert E, Desamericq G, Khachatryan A, Ngo P, Gusto G, Sorio-Vilela F. Patient characteristics, treatment patterns, and adherence to lipid-lowering therapies following an acute coronary syndrome. Rev Cardiovasc Med. 2020;21(4):643–650. doi:10.31083/j.rcm.2020.04.189
59. Seamon K, Sanfilippo F, Bulsara M, et al. Predictors of ceasing or reducing statin medication following a large increase in the consumer copayment for medications: a retrospective observational study. Public Health Res Pract. 2020;30(1):1–9. doi:10.17061/phrp29121905
60. Shakarneh JK, Hallak HO, Awadallah HB, Al-Hamed DH, Khdour MR. Necessity and concerns about lipid-lowering medical treatments and risk factors for non-adherence: a cross-sectional study in Palestine. Int J Clin Pract. 2020;74(7):e13511. doi:10.1111/ijcp.13511
61. Ofori-Asenso R, Jakhu A, Curtis AJ, et al. A systematic review and meta-analysis of the factors associated with nonadherence and discontinuation of statins among people aged ≥65 years. J Gerontol A Biol Sci Med Sci. 2018;73(6):798–805. doi:10.1093/gerona/glx256
62. Mann DM, Woodward M, Muntner P, Falzon L, Kronish I. Predictors of nonadherence to statins: a systematic review and meta-analysis. Ann Pharmacother. 2010;44(9):1410–1421. doi:10.1345/aph.1P150
63. Atreja A, Bellam N, Levy SR. Strategies to enhance patient adherence: making it simple. MedGenMed. 2005;7(1):4.
64. Santos P. Challenge of health literacy in cardiovascular disease prevention. Curr Res Cardiol. 2018;5(special issue 4):18.
65. Santos P, Nazare I, Martins C, Sa L, Couto L, Hespanhol A. As Normas de Orientacao Clinica em Portugal e os Valores dos Doentes. [The Portuguese Guidelines and Patients Values]. Acta Med Port. 2015;28(6):754–759. doi:10.20344/amp.6301
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.