")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Determinants of Mother-to-Child Transmission of HIV in Public Hospitals of West Shewa Zone, Central Ethiopia: Case-Control Study
Authors Hunduma F , Gebrehanna E, Adugna Debela F
Received 29 December 2020
Accepted for publication 26 March 2021
Published 16 April 2021 Volume 2021:13 Pages 435—443
DOI https://doi.org/10.2147/HIV.S299585
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Video abstract of "Determinants of Mother to Child Transmission of HIV In Public Hospitals" [ID 299585].
Views: 430
Fufa Hunduma, Ewenat Gebrehanna, Fanna Adugna Debela
Department of Public Health, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Fufa Hunduma
Department of Public Health, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Tel +251 922956730
Email [email protected]
Background: Mother-to-child transmission (MTCT) of human immune deficiency virus (HIV) is the infection of baby by HIV that originated from an HIV-positive mother during pregnancy and breast feeding. Without intervention, the transmission rate of HIV ranges from 15– 45%, which can be reduced to below 5% with effective intervention. In Ethiopia, the final mother-to-child transmission rate was 15% in 2016, which was much higher than the target of the country to reduce transmission to lower than 5% by 2020. The study aims to identify determinants of transmission of HIV from mother to child in the West Shewa Zone.
Methods: An unmatched case–control study, among children less than 5 years who tested HIV positive and negative, at the end of PMTC follow-up, N=96 (24 cases, 72 controls) was conducted during June to August 2019, focusing on PCR done during the last 2 years (June 2017 to July 2019), in public hospitals. Data were collected using a structured questionnaire and data abstraction forms from mothers of exposed infants, medical records of mothers and children.
Results: The majority of cases (17, 70.8%) were not included in the option B+ program, but only 11.1% of controls were not included. Home delivery (adjusted odds ratio (AOR)=6.047, confidence interval (CI)=1.549– 29.230), non-inclusion into option B+ (AOR=18.0, 95% CI=5.0– 68.1), and partner non-involvement to HIV care (AOR=7.3, 95% CI=1.14– 37.459) had higher odds of transmitting HIV, while a mother-to-mother support program decreases the chance of transmission by 86.5% (AOR=0.135, 95% CI=0.11– 0.396) when compared to their counterparts.
Conclusion: Mother-to-mother support programs have a protective effect, while non-inclusion to option B+, partner non-involvement in HIV care, home delivery, and poor antenatal care (ANC) practices were determinant factors of HIV transmission from mother to child.
Keywords: mother-to-child transmission of HIV, Ethiopia, West Shewa, HIV transmission, prevention of MTCT
Background
Mother-to-child transmission (MTCT) of Human Immunodeficiency Virus (HIV) is when a HIV-positive mother passes the virus to her baby. This can occur during pregnancy, labor and delivery (at birth), or breastfeeding.1 Without treatment, around 15–30% of babies born to HIV positive women will become infected with HIV-1 during pregnancy and at birth. A further 5–20% will be infected through breastfeeding up to 18–24 months. More than 90% of HIV infections in children under 15 years were acquired from the mother,2 and more than 50% of postnatal transmission through breastfeeding occurs during the first 6 months of life.3 In the absence of any intervention, the transmission rate ranges from 15–45%. This can be reduced to below 5% with effective intervention during the periods of pregnancy, labor, delivery, and breastfeeding.4–7
In Ethiopia, according to the Central Statistics Agency (CSA), the estimated prevalence of HIV among adults was 0.4% in rural areas and 2.9% in urban areas in 2018. In the capital, Addis Ababa, it was estimated to be 3.4% in 2018. In Oromiya region, which includes West Shewa Zone, the prevalence was estimated to be 0.7%.8 The Ethiopian Federal Ministry of Health (FMOH) rolled out the prevention of mother-to-child transmission (PMTCT) program for the first time in 20079 but the country implemented the advanced PMTCT program (option B+) in 2011 with the aim of eliminating mother-to-child transmission of HIV. Before the implementation of PMTCT program, the transmission of HIV from mother to child was estimated to be 15–45%. According to the systemic review and meta-analysis done in 2018, the prevalence of MTC transmission in Ethiopia and Oromia was 9.93% and 12.11%, respectively.10
Despite option B+ (test and treat) being implemented in Ethiopia in 2011, by 2014 only an estimated 50% of infants born to women living with HIV received a virological test within 2 months of birth.11 At a national level, 58% of HIV-positive pregnant mothers in Ethiopia receive ART.12 In 2017, the number of mothers needing prevention of mother-to-child transmission (PMTCT) in the urban area was estimated to be 16,959.13 Ethiopian Public Health Institute (EPHI) estimates the number of mothers needing PMTCT in Addis Ababa was 1,466 in 2017.14 According to Ethiopian Demographic Health Survey (EDHS) 2016, countrywide, HIV testing, and counseling for ANC clients in the country was 19%, reaching 56% in urban areas and 14% in rural areas. The 2016 EDHS shows that 62% of women received ANC from a skilled provider at least once for their last birth.15
Preventing MTCT comprises strategic activities like primary prevention of HIV, prevention of unintended pregnancies, effective access to HIV testing and counseling, initiation of lifelong antiretroviral therapy (ART), with support for adherence, retention, and viral suppression for mothers living with HIV, safe delivery practices, optimal infant feeding practices, and access to postnatal antiretroviral (ARV) prophylaxis for all infants.16 Suppression of HIV in pregnant women is the most important and achievable action to reduce MTCT. However, failure to initiate ART early in pregnant HIV-positive mothers, poor adherence to ART, lack of ANC and early diagnosis, and poor application of national policies like option B+ among care providers hinder prevention of MTCT.17
In May 2016, the World Health Assembly endorsed the new WHO global health strategy on HIV, which calls for the Member States and WHO to work together towards the goals of zero new HIV infections in infants by 2020.9 Ethiopia has implemented a four-pronged approach to reduce and control the transmission of HIV from mother to child. These are primary prevention of HIV infection, prevention of unintended pregnancies in HIV positive women, prevention of HIV transmission from mother to her infants, and care and support for HIV positive mothers and her exposed infants.11 The target in Ethiopia for MTCT was set at <5% by 2020;16 however, in 2016 the MTCT rate was still 15%.7
Even though studies have been conducted in different parts of the country,3 similar studies have not been done in West Shewa, so we tried to fill the gap. This study intends to identify particular determinants of HIV transmission from mother to child among patients of West Shewa Zone. This study, therefore, will contribute to the identification of factors independently associated with PMTCT and have an input for interventional planning for future control of the epidemic.
Methods
Study Settings
West Shewa Zone is located in the central part of Ethiopia, between 9.1515°N and 37.808°E covering 14,788.78 square kilometers. It has 18 woredas with six functional hospitals currently and 2.5 million population. We selected three hospitals that have been providing ART services for more than 4 years (Figure 1).
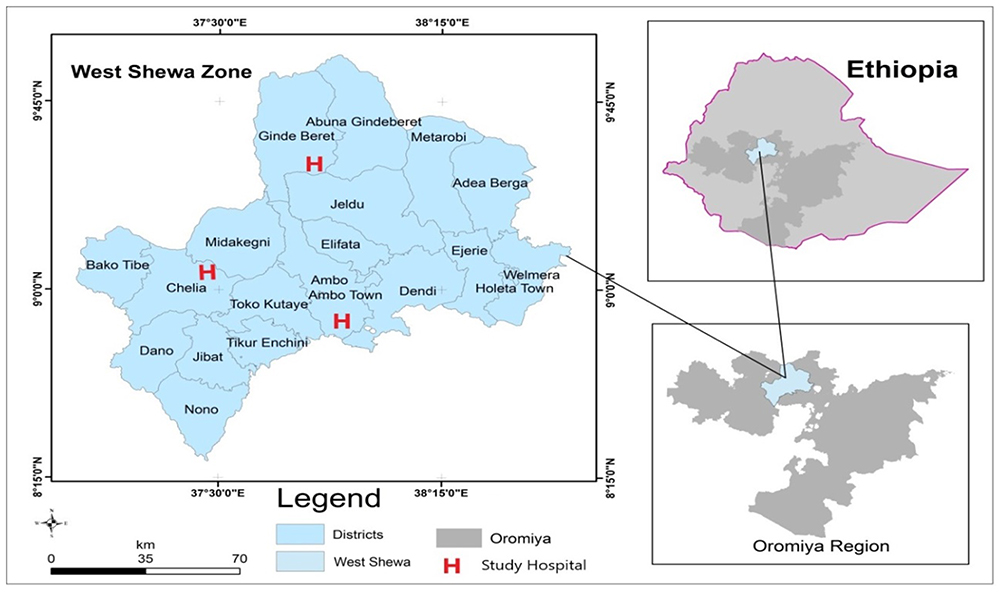 |
Figure 1 Geographical location of West Shewa zone in Ethiopia. West Shewa is located in the central part of Ethiopia and has a population of more than 2.5 million . It has six hospitals; however, we included the three hospitals shown on the image since they have been serving ART clinics for more than 4 years. The image was developed by corresponding author using QGIS. |
Study Design and Period
An unmatched case-control study was conducted employing exposed infants whose serostatus had been determined and was known to be positive and who were declared negative in the last 2 years (June 2017 to June 2019). The study took place from June 15 to August 10, 2019, focusing on a polymerase chain reaction (PCR) done during the last 2 years (June 2017 to July 2019).
Population
Target populations were Infants born to HIV positive mothers in West Shewa Zone. Study populations were Infants born to HIV positive mothers, whose serostatus was determined at Ambo, Gedo, and Gindabarat Hospitals, and their serostatus was determined to be negative or positive.
Cases and Controls
Children less than 5 years old who were born to HIV positive mothers and determined to be HIV positive were cases. Children less than 5 years old, who were born to HIV positive mothers and found to be seronegative according to national guidelines, and whose mothers came for regular follow-up were controls. We tried to check selection bias by sensitivity analysis considering possible biasing variables like the presence of additional complaints during the follow-up appointment, education level, place of residency, and income (represented by U), with each variables turned to be significantly associated to the outcome or variables of interest (represented by A) and S being selection indicator. Employing the formula ORtrue≥ORobs/(((RRUA1xRRs0A)/(RRUA1+RRS0A-1))x((RRUA0xRRS1U)/(RRUA0xRRS1U−1))), we have determined the lower and upper bound of estimate of true OR for respective variables. While RRUA1 describes increased probability of variable of interest among eligible controls without the suspected biasing variable, RRUA0 is increased probability of not having variables of interest but who have suspected biasing variable, RRS1U is increased probability of presence of biasing variable in controls who were selected compared with those who were not, and RRS0A represents increased probability of no biasing variables in controls who were not selected for the study compared with those who were selected. (In this case, variables of interest represent the variables that are turns to be significantly associated with the outcome.)
Inclusion and Exclusion Criterion
Singleton births with both maternal and child’s records available in the hospital were included. We excluded a child whose medical record was not available and not well-documented and orphaned/denied children with no maternal record.
Sample Size Determination
We determined sample size employing a two-population proportion formula. We assumed 80% power, 95% level confidence interval, 5% margin of error, and ratio of cases to controls being 1:3 and the percent of non-exposure to ANC follow-up among the infected group=67.5% and 34.4% among non-infected (from another similar study).3 A sample size of 24 cases and 72 controls was calculated.
Sampling Procedure
Three hospitals (Ambo Hospital, Gedo Hospital, and Gindabarat Hospitals) were purposively selected due to being the only hospitals that have been providing ART services for more than 4 years in the zone. Based on the total number of infants and children who were living with HIV at each hospital, we assigned cases proportionately. Cases were randomly captured at ART Out Patient Department (OPD) and three random controls were assigned to each case as they came for regular follow-up (Figure 2). To ensure the randomness of the selection, we included both cases and controls who came for regular follow-up at ART OPD.
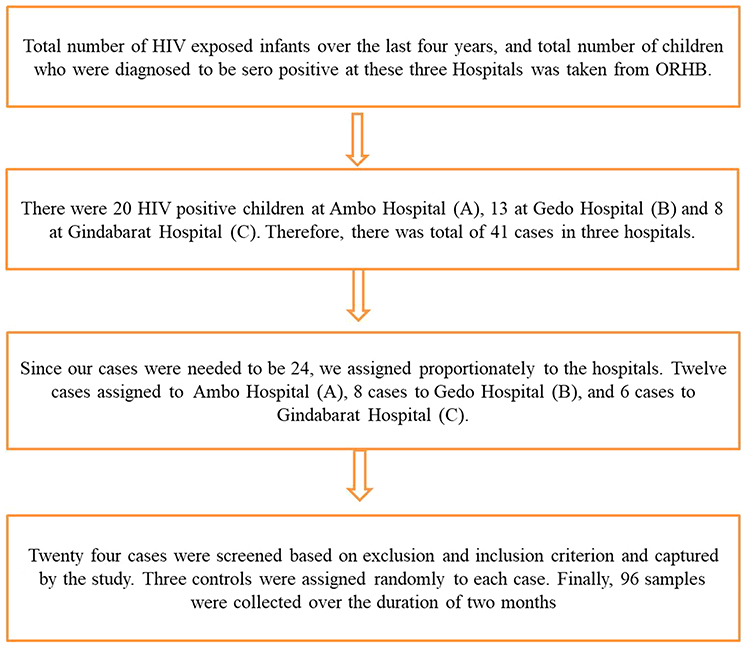 |
Figure 2 Approach used to select cases and controls from three hospitals. The flow chart of our steps to identify cases and controls. Initially we went to Oromia Regional Health Bureau to get the data of infected children, then we got a total number in the zone and stratified by hospitals and assigned cases and controls (source: developed by principal author based on study design of the project). |
Independent Variables
Age, sex, residence, socioeconomic status, clinical history, and obstetric history.
Dependent Variables
HIV positive.
The Operational Definition of Terms
Poor adherence: those who missed their ART dose more than 10% per month.
Fair adherence: those who missed 5–10% of their ART doses.
Good adherence: those who missed less than 5% of their ART doses.
Mother-to-mother (M2M) support program: a peer support program which employs HIV-positive mothers to provide support and advice to HIV-positive pregnant women and mothers of HIV-exposed babies.
Option B+: the program that utilizes initiating triple ARV drugs for all pregnant HIV positive mothers and continues throughout their life.
ARV prophylaxis: the administration of ARV drugs to a newborn without documented HIV infection to reduce the risk of HIV acquisition.
Data Collection Analysis and Interpretation
We prepared a structured questionnaire and data abstraction form to collect important variables of interest (it is provided in Supplementary materials). The structured questionnaire was used to collect information from mothers of study participants, while the data abstraction form was used to collect information from HIV/AIDS care records. To minimize information bias, the close-ended questionnaire was designed for mothers of exposed infants, and trained data clerks and ART care providing nurses, who could counter-check the information from Logbook and database, collected information from the medical record. We entered data into Microsoft Excel and checked for redundancy, incompleteness, and ambiguities and the data was analyzed by SPSS version 23. Descriptive statistics, including mean, and frequencies, were used to describe demographic and clinical characteristics of patients. We used Chi-square test and sensitivity analysis to evaluate the difference among cases and controls and to see the effect of selection bias, respectively. We employed bi-variate logistic regression to identify variables that are associated to the outcome with P-value≤0.20, and those variables fitted to the final model of multivariate logistic regression to determine variables significantly associated to the dependent variables. We declared the association was statistically significant at a P-value less than 0.05, and, considering the ranges of true OR derived from sensitivity analysis.
Result
General Description of the Study
There were 421 exposed infants delivered at those three study hospitals; among them 41 (9.7%) acquired HIV down from their mothers, that made the transmission rate of 9.7% in West Shewa hospitals. From 41 of those infected by HIV we included 24 (58.5%) as cases. Subsequently, there were 96 total participants included in the study from Ambo, Gindabarat, and Gedo Hospitals; among them 24 were cases and 72 were controls.
Among participants, slightly more than half of participants’ mothers were housewives (53.13%), the majority were married (89.5%), 29% were Orthodox and 25% were protestant by religion. During pregnancy and breast-feeding, the mothers of participants were classified according to WHO’s clinical staging and 12 (12.5%) were Stage I, 42 (43.75%) were Stage II, 19 (19.79%) were Stage III, and the remaining 22 (23.6%) were Stage IV.
Gedo Hospital has 135 exposed infants and among them 13 (9.6%) were HIV positive under-5 children over the last 4 years. This made a 9.6% transmission rate per 100 exposed infants. At Gindabarat Hospital, there were 94 exposed infants and, among them, eight were HIV positive, which made a 8.5% transmission rate from mother to children at Gindabarat hospital. There were 192 exposed infants registered at Ambo Hospital over the last 4 years and, among them, 20 (10.4%) were confirmed to be positive.
Among those who transmitted HIV to their children and were dwelling in rural areas, 75% said they did not start ART during the pregnancy and slightly over half of them (54.2%) had ANC visits at least once. However, 70.8% of them did not take ART during the follow-up. Half of all cases (50.5%) did not take ART during pregnancy and 37.5% of them did not start ART during breastfeeding either. All deliveries of cases were vaginal and 70.8% were delivered at home. The majority of controls’ partners were involved in HIV care (86.1%), but only 33.3% of partners of cases were involved in HIV care (Table 1). Among controls, however, all started ART during pregnancy and 97.2% of them adhered appropriately to the medication. We ran Chi-square tests to evaluate the sociodemographic differences of cases and controls, however, no significant difference was observed.
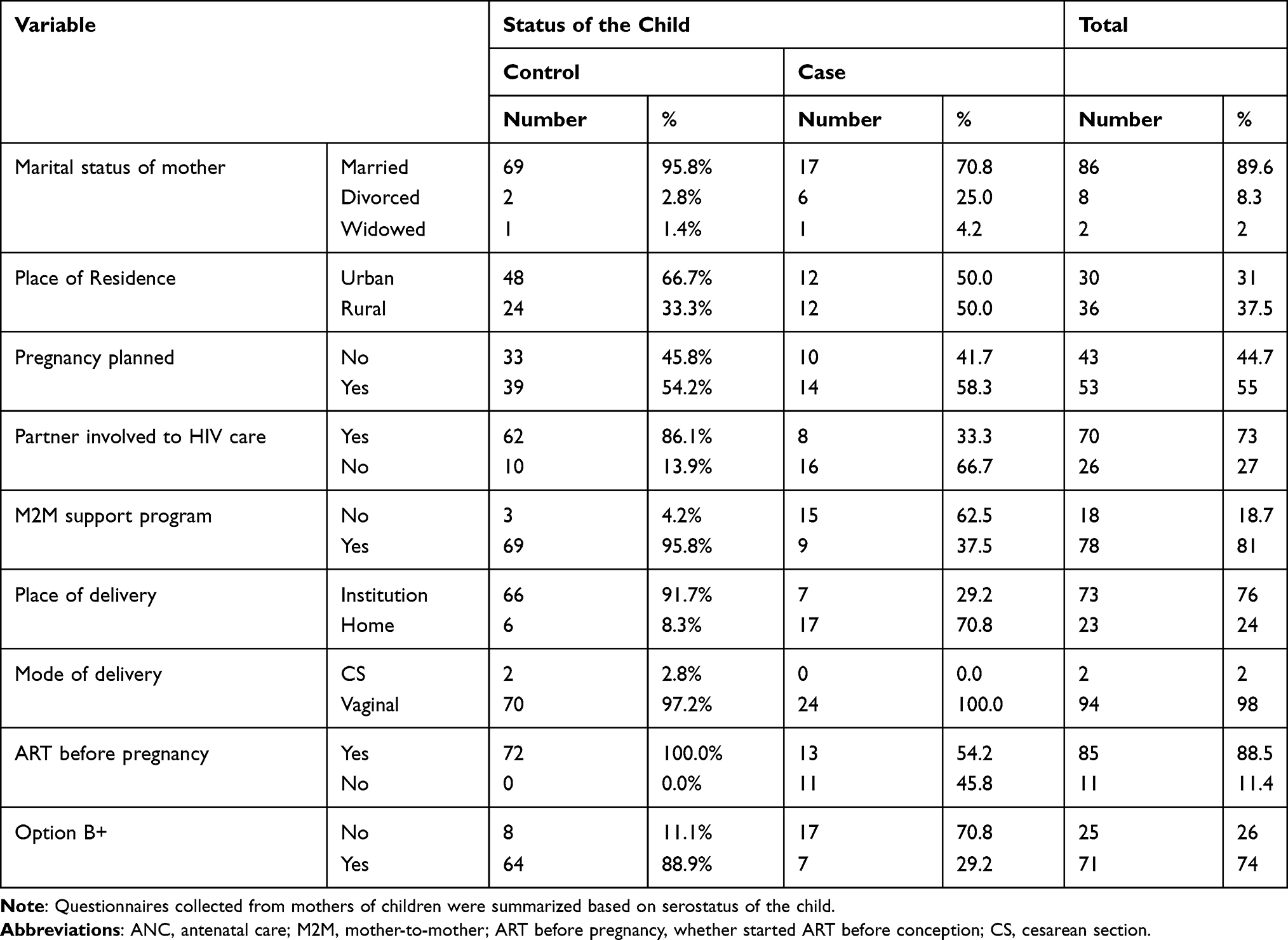 |
Table 1 Variables Related to Socioeconomic and Prevention Intervention Summary of Mother–Infant Pair of the Study |
Factors Associated with HIV MTCT
Based on multivariate analysis, the presence of a mother-to-mother support program has a protective effect, while the absence of partner involvement to HIV care, non-inclusion to option B+, and Home delivery have a significant association to the transmission of HIV from mother to child. Mothers who were included into a mother-to-mother (M2M) support program had a lower chance of transmitting HIV to their children. Thus, mothers who were not included in a mother-to-mother support program had 86.5% more chance of transmitting HIV to their children (AOR=0.135; 95% CI=0.111–0.396, P<0.05). Mothers whose partners were not involved in HIV care had higher odds of transmitting HIV to their children. Non-involvement of mother’s partner to HIV care increased the chance of transmitting HIV to her baby by 7.3-times when compared to those whose partners were involved (AOR=7.331; 95% CI=1.142–37.459, P<0.05). Mothers who were not included in the option B+ protocol has 18-times more chance of transmitting HIV down to her baby (AOR=18.0; 95% CI=5.0–68.1, P<0.05). Home delivery also increased the chance of transmitting HIV from mother to child by 6 times when compared to those who delivered at the institution; AOR = 6.047, with 95% CI (1.549–29.230), P < 0.05 (Table 2).
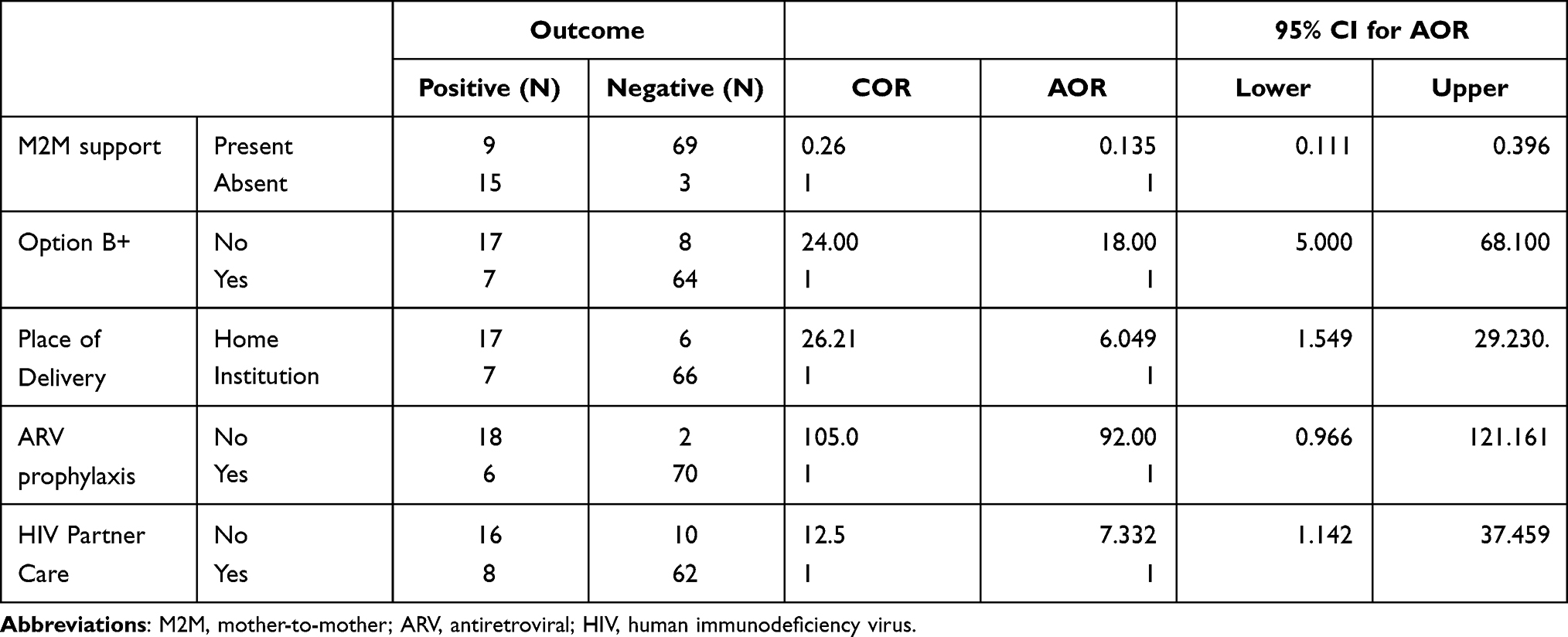 |
Table 2 Factors Associated with HIV Transmission from Mother to Child by Regressions Analysis (Source: Taken from the Main Document of the Project. Produced by SPSS from Raw Data of Participants by PI) |
Discussion
There were 421 exposed infants delivered at the study hospitals and, among them, 41 (9.7%) children acquired HIV down from their mothers. This made the transmission rate of 9.7% for exposed infants in West Shewa hospitals. This is slightly lower than the transmission rate of Ethiopia as a whole, which was reported to be 15% in 2016. This was significantly higher than the country’s target to reduce the transmission rate to lower than 5% by 2020.16
Vertical transmission of HIV in low- and middle-income countries has declined to less than 5% in the best-case scenarios after the introduction of PMTCT strategies, and in wealthy countries transmission rates are below 2%.4,5 Over the past two decades, improved interventions in developed countries have reduced MTCT rates to less than 2%.4 In resource-poor countries, applicable measures to reduce transmission of HIV from mother to child include safer delivery practices, infant feeding counseling and support, and use of antiretroviral (ARV) treatment or MTCT prophylaxis.5 In this study, the majority of MTCT happened among those who delivered at home, and among those who did not know their serostatus during pregnancy. This happened probably due to low activities to mobilize and create awareness among pregnant mothers to follow ANC and attend institutional delivery.
According to this study, the presence of a mother-to-mother support program has a protective effect, while the absence of partner involvement to HIV care, non-inclusion to option B+, and home delivery have significant associations to the transmission of HIV from mother to child. This was similar to studies done previously in Ethiopia and other African countries.3,18–21 According to Shroufi et al, Mother-to-Mother support programs offer great potential to empower communities affected by HIV to catalyze a positive behavior change and increase retention in PMTCT programs.22
Besides, this study revealed that the majority of cases (70.8%) were not included into option B+ and 76.5% did not go to an ANC visit even once. This low coverage of the service was probably due to bi-dimensional impediments: care receivers and caregivers. From the care receivers’ perspective, lack of sufficient awareness about the option B+ services or poor knowledge about the use of ANC could explain the problem. While lack of updated knowledge about the recent national policy guidelines and some kind of negligence could be caregivers cause of non-inclusion to option B+. However, provision of option B+ for HIV positive pregnant mothers is the core of HIV transmission prevention strategies in the country as well as worldwide. According to WHO the accelerated rollout of ART for pregnant women was an important factor in the success of the global plan towards the elimination of new HIV infection among children.6 Option B+ is a cost-effective treatment for comprehensive HIV prevention service and it can minimize the chances of MTCT of HIV infection if used optimally.23,24
Limitations
Since the study hospitals were purposively selected based on the duration of ART service, it might limit generalization for new hospitals, which started providing ART services in recent years.
Conclusion
According to this study, a mother-to-mother support program has a protective effect, while non-inclusion to option B+, absence of partner involvement to HIV care, and home delivery are significant factors associated with the transmission of HIV from mother to child. Among rural residents, there was a high probability of home delivery, lower inclusion to option B+, and lower ANC follow-up, that might result from lower awareness of use of health facility attendance. Future study needs to be conducted to assess the problems related to poor ART adherence and factors associated to home delivery, especially among rural residents. Besides, healthcare workers who are assigned to rural health facilities like health extension workers (HEW) should stick to national guidelines and actively be engaged in community awareness and identification of pregnant mothers to include them in prenatal care.
Declarations
We hereby declare that all source materials used for this research have been duly acknowledged.
Abbreviations
ANC, antenatal care; ART, anti-retroviral treatment; ARV, antiretroviral; EPHI, Ethiopian Public Health Institute; HEW, health extension worker; INH, isoniazid; MTCT, mother-to-child transmission; PCR, polymerase chain reaction; PMTCT, prevention of mother-to-child transmission (of HIV); SPHMMC, Saint Paul’s Hospital Millennium Medical College; STI, sexually transmitted infection; UNAIDS, United Nations Program on HIV/AIDS; UNICEF, United Nations Children’s Fund; VL, viral load.
Data Sharing Statement
Any data and materials related to this this study are available upon request from the Principal Investigator (Fufa Hunduma, email: [email protected]).
Ethical Approval and Consent to Participate
The ethical issue of the study was approved and ethical clearance was obtained from the Institutional Review Board of Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia. Consent to participate was obtained by written informed consent. Patients’ information used in this research will be kept confidential by not using the name of patients, address of patients and not sharing for third person. The participants were included after written informed consent was taken from the mother of participants after explaining the intention of the study, use of the study, and freedom of avoiding the study if they would intend to do so. There was no third party which needs one side shift of the result and no interest of sponsors, which could affect the result of this study, so that conflict of interest was minimal. Generally, we can confirm that the ethical issue of the study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We are grateful to Ambo Hospital, Gedo Hospital, and Gindeberet Hospitals’ staff for their active participation in helping us conduct this research. We also heartily thank Saint Paul’s Hospital Millennium Medical College for sponsoring and technically supporting this research.
Disclosure
The authors reported no conflicts of interest for this work.
References
1. Koye DN, Zeleke BM. Mother-to-child transmission of HIV and its predictors among HIV-exposed infants at a PMTCT clinic in northwest Ethiopia. BMC Public Health. 2013;13(1):398. doi:10.1186/1471-2458-13-398
2. Tindyebwa D. Handbook on Paediatric AIDS in Africa: african Network for the Care of Children Affected by AIDS (ANECCA); 2004. Available from: https://www.fhi360.org/sites/default/files/media/documents/Handbook%20on%20P%C3%A6diatric%20AIDS%20in%20Africa.pdf.
3. Burusie A, Deyessa N. Determinants of Mother to Child HIV Transmission (HIV MTCT); A Case Control Study in Assela, Adama and Bishoftu Hospitals, Oromia Regional State, Ethiopia. Cell Dev Biol. 2015;4:1000152. doi:10.4172/2168-9296.1000152
4. Woelk GB, Ndatimana D, Behan S, et al. Retention of mothers and infants in the prevention of mother-to-child transmission of HIV programme is associated with individual and facility-level factors in Rwanda. J Int AIDS Soc. 2016;19(5Suppl 4):20837. doi:10.7448/IAS.19.5.20837
5. Abtew S, Awoke W, Asrat A. Knowledge of pregnant women on mother-to-child transmission of HIV, its prevention, and associated factors in Assosa town, Northwest Ethiopia. HIV/AIDS Res Palliative Care. 2016;8:101. doi:10.2147/HIV.S100301
6. Global information and education on HIV and AIDS. Prevention of mother-to-child transmission (PMTCT) of HIV World Health Organization PMTCT guidelines; 2018. Available from: https://www.avert.org/professionals/hiv-programming/prevention/prevention-mother-child.
7. Federal democratic republic of ethiopia ministry of health. National Comprehensive And Integrated Prevention Of Mother-To-Child Transmission Of Hiv Guideline; 2018. Available from: https://www.afro.who.int/sites/default/files/201904/National%20Comprehensive%20HIV%20Care%20%20Guideline%202018.pdf.
8. Federal HIV/AIDS Prevention and Control Office, HIV Prevention in Ethiopia: national Road Map (2018–2021):pdf; 2018. Available from:: https://ethiopia.unfpa.org/en/publications/hiv-prevention-ethiopia-national-road-map-2018-2021.
9. Federal HIV/AIDS Prevention and Control Office; Federal Ministry of Health. Guidelines for Prevention of Mother-to-Child Transmission of HIV in Ethiopia; 2007. Available from: https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---ilo_aids/documents/legaldocument/wcms_125389.pdf.
10. Kassa GM. Mother-to-child transmission of HIV infection and its associated factors in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2018;18(1):216. doi:10.1186/s12879-018-3126-5
11. Tiruneh YM, Galárraga O, Genberg B, Wilson IB. Retention in Care among HIV-Infected Adults in Ethiopia, 2005–2011: a Mixed-Methods Study. PLoS One. 2016;11(6):e0156619. doi:10.1371/journal.pone.0156619
12. EPHI, feredal Menistry of Health. HIV related estimate and projections for Ethiopia, 2017. ECSA, Ethiopian Demographic and Health Survey, 2016. Available from: https://www.ephi.gov.et/images/pictures/download2009/HIV_estimation_and_projection_for_Ethiopia_2017.pdf.
13. Federal Democratic Republic of Ethiopia Ministry of Health. Annual Health Sector Performance Report Efy 2009 (2016/17); 2017. Available from: https://www.itacaddis.org/docs/2017_11_10_09_48_31_ARM%202017.compressed.pdf.
14. Federal Democratic Republic of Ethiopia Ethiopia, Central Statistical Agency. Demographic and Health Survey 2016. Maryland, USA, Survey, H. Ethiopia: The DHS Program ICF Rockville; 2017. Available from: https://dhsprogram.com/publications/publication-fr328-dhs-final-reports.cfm.
15. Hussein M, Jira C, Girma B. Assessment of Effective Coverage of HIV Prevention of Pregnant Mother to Child Transmission Services in Jimma Zone, South West Ethiopia. Ethiop J Health Sci. 2011;21(Suppl 1):1–7.
16. The gap report: children and pregnant women living with HIV. Geneva: UNAIDS; 2014. Available from: http://www.unaids.org/sites/default/files/media_asset/09_ChildrenandpregnantwomenlivingwithHIV.pdf.
17. UNICEF. Children, HIV and AIDS: the world today and in 2030; 2018. Available from: https://data.unicef.org/resouurces/children-hiv-and-aids-2030/.
18. WHO. Global HIV/AIDS response Epidemic update and health sector progress towards Universal Access, Progress Report 2011. Geneva: World Health Organization; 2011. Available from: http://www.who.int/hiv/pub/progress_report2011.
19. Audureau E, Kahn JG, Besson M, et al. Scaling up prevention of mother-to-child HIV transmission programs in sub-Saharan African countries: a multilevel assessment of site-, program- and country-level determinants of performance. BMC Public Health. 2013;13(286). doi:10.1186/1471-2458-13-286
20. Wudineh F, Damtew B. Mother-to-Child Transmission of HIV infection and its determinants among exposed infants on care and follow-up in dire Dawa City, Eastern Ethiopia. AIDS Research and Treatment. 2016;2016:1–6. doi:10.1155/2016/3262746
21. Abuhay Y, Abebe L, Fentahun N. Male involvement in prevention of mother to child transmission of HIV and associated factors among males in Addis Ababa, Ethiopia of Mother-to-Child Transmission of HIV. J Health Res. 2014;2:338–343. doi:10.11648/j.ajhr.20140206.13
22. Shroufi A, Mafara E, Saint-Sauveur JF, Taziwa F, Viñoles MC. Mother to Mother (M2M) peer support for women in Prevention of Mother to Child Transmission (PMTCT) programmes: a qualitative study. PLoS One. 2013;8(6):e64717. doi:10.1371/journal.pone.0064717
23. Wang X, Guo G, Zheng J, et al. Cost-effectiveness of option B+ in prevention of mother-to-child transmission of HIV in Yunnan Province, China. BMC Infect Dis. 2019;19(517). doi:10.1186/s12879-019-3976-5
24. Chaka TE, Abebe TW, Kassa RT. Option B+ prevention of mother-to-child transmission of HIV/AIDS service intervention outcomes in selected health facilities, Adama town, Ethiopia. HIV AIDS. 2019;11:77–82. doi:10.2147/HIV.S192556
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.