")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Determinants of Hypertension Among Patients with Diabetes mellitus in Public Hospitals of Kembata Tambaro Zone, South Nations Nationalities and Peoples Region, Ethiopia, 2021; A Case Control Study
Authors Kenore Y, Abrha S, Yosef A , Gelgelu TB
Received 20 June 2022
Accepted for publication 16 September 2022
Published 26 September 2022 Volume 2022:15 Pages 2141—2152
DOI https://doi.org/10.2147/JMDH.S379293
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Yeshialem Kenore,1 Solomon Abrha,2 Amanuel Yosef,2 Temesgen Bati Gelgelu2
1Hawassa University Comprehensive Specialaized Hospital, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia; 2School of Public Health, College of Health Sciences and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Correspondence: Amanuel Yosef, Tel +251 918451138, Email [email protected]
Introduction: Hypertension is commonly defined as a persistently raised blood pressure in which systolic blood pressure reading (SBP) is greater than or equal to 140 mmHg and diastolic blood pressure (DBP) is greater than or equal to 90 mmHg. The comorbidity of hypertension and diabetes mellitus is complex and is associated with a high risk of complications. However, there are limited studies on determinants of hypertension among patients with diabetes in Ethiopia. Therefore this study aimed to identify the determinants of hypertension among patients with diabetes mellitus in public hospitals of the Kambata Tambaro Zone, Ethiopia.
Methods and Materials: A hospital-based unmatched case-control study was conducted among a total sample of 326 patients with diabetes from June 17, 2021 to August 17, 2021. This study was conducted in five public hospitals. The data were entered into EpiData version 3.1 software and exported to and analyzed using SPSS software version 25.0. Bivariable and multivariable binary logistic regression analyses were used to determine the association between the dependent and independent variables.
Results: Of the 336 study participants, 326 diabetic patients (163 cases and 163 controls) were interviewed resulting in a response rate of 97%. Age group ≥ 50 years (Adjusted Odds Ratio = 7.00, 95% CI = 1.69– 28.9), inactivity in physical exercise (AOR = 5.84, 95% CI = 2.47– 13.81), patients who have a history of drinking alcohol (AOR = 2.61, 95% CI = 1.35– 5.03) and patients who had poor knowledge on diabetes (AOR = 3.04, 95% CI = 1.69– 5.47) were more likely to develop hypertension among diabetic patients.
Conclusion: This study concluded that age, inactivity in physical exercise, history of alcohol intake and poor knowledge were determinants of hypertension among diabetic patients.
Keywords: determinants of hypertension, diabetes, patients, Ethiopia
Background
Hypertension is commonly defined as a persistently raised blood pressure in which systolic blood pressure (SBP) is greater than or equal to 140 mmHg and diastolic blood pressure (DBP) is greater than or equal to 90 mmHg.1 Hypertension, usually known as “the silent killer” is a major public health problem both in developed and developing countries.1,2 Hypertension is mainly categorized as primary or secondary based on its cause. Primary or essential hypertension is defined as absence of an identified cause. The majority (95%) of hypertensive patients fall into this classification.3
Hypertension affects approximately 1.13 billion people globally and two-thirds of these live in low- and middle-income countries.4 Hypertension, is a global public health challenge among diabetic patients.5 In low- and middle-income countries, there has been an increase in the prevalence of hypertension and non-communicable diseases due to urbanization.6 Diabetes and hypertension are diseases that are usually chronic, with slow onset and lengthy progression, for which there are no known specific causative agents, and are generally non-communicable.7,8 Evidence has shown that 98% of diabetes treatment depends on having good self-care behaviors and patients with diabetes adhering to self-care can prevent complications associated with diabetes mellitus.9 Data from several studies show that the prevalence of hypertension in patients with diabetes mellitus is approximately 1.5–2.0 times greater than that in an appropriately matched non-diabetic population.8 Poor and inadequate diabetes control is a major cause of macro-vascular and micro-vascular complications and death. The comorbidity of hypertension and diabetes increases the risk of mortality by 7.2-fold with a greater risk of death in developing nations.10
The new epidemic comorbidity of hypertension and diabetes is not only an important public health problem, but it will also have great economic influence as a significant proportion of the productive population becomes chronically ill or dies, exposing their families to poverty.11 Up to 80% of people with diabetes die of cardiovascular disease, especially hypertension (HTN) and stroke, since most patients with diabetes develop hypertension. It is clear that the co-existence of these two diseases in a patient carries an excessive risk for both micro- and macro-vascular complications, and mortality.12
A study conducted in Uganda and Libya showed that the prevalence of hypertension among diabetic patients was 61.9% and 85.6, respectively.13,14
According to studies conducted in Ethiopia, diabetes mellitus accounts for 2% of deaths related to non-communicable diseases (NCDs), while NCDs accounted for almost 39% of all deaths in Ethiopia and the greatest proportion (15%) of these deaths are directly linked to cardiovascular diseases.15 Compared with other cardiovascular disorders, HTN is the most common comorbid disease in patients with diabetes and its effects are devastating if uncontrolled.7 Cross-sectional studies in Ethiopia conducted at Jimma University Medical Center and Nigist Ellen Mohamed Memorial Hospital, Hosanna, with a much smaller sample size (140), show the magnitude of hypertension among diabetic patients is 37.4% and 55%, respectively.16,17
The determinants of hypertension among patients with diabetes have been studied and reported in many studies. These include socio-demographic and socio-economic, behavioral and lifestyle, clinical and anthropometric factors.18 There are also other important factors that have not been studied and described in the literature, in which this study tried to assess their possible relation in determining the development of hypertension in patients with diabetes mellitus such as knowledge about DM and service-related factors such as cost of diabetic drugs, payment source for the cost of diabetic treatment, availability and attending of diabetes education in the facility. Many hospitals organized chronic care clinics to follow-up patients with diabetes.19 However information on HTN in patients with DM and its contributing factors is not clearly understood. The determinants of HTN in the general population have been well studied. However, there are few studies conducted on the determinants of hypertension among patients with diabetes in this study area. Knowing about the determinants of hypertension among patients with diabetes can help to prepare specific intervention plans in resource-scarce countries such as Ethiopia.
Therefore, by applying an unmatched case control study design, this study aimed to identify the determinants of hypertension among patients with diabetes in public hospitals of Kambata Tambaro Zone.
Methods and Materials
Study
Area and Period
The study was conducted from June 17 to August 19, 2021 for two months in public hospitals of the Kambata Tambaro Zone, SNNPR Ethiopia. The Kambata Tambaro Zone has eight8 districts with four4 town administrations and is located 350 km from Addis Ababa, the capital of Ethiopia.20 The study area contains 33 health centers, 138 health posts, 1 general hospital and 4 primary hospitals.21 According to the 2007 Ethiopian census projection the total population of Kambata Tambaro Zone was estimated to be 962,813 of which 49% were male and 51% were female.22 All the hospitals provide inpatient, outpatient, emergency, delivery and many other services including care for chronic illnesses. There were about 1006 diabetic patients in follow-up in all five hospitals (Durame General Hospital: 182 cases and 250 controls; Shinshicho Primary Hospital: 71 cases and 85 controls; Mudula Primary Hospital: 42 cases and 92 controls; Doyogena Primary Hospital: 47 cases and 99 controls; and Angecha Primary Hospital: 46 cases and 92 controls (report from each hospital - 2020 G.C)).21
Study Design
A hospital-based unmatched case control study design was conducted in a population of patients with diabetes mellitus and hypertension comorbidity who were on follow-up on chronic care outpatient departments as cases and diabetes mellitus patients without hypertension comorbidity as controls in order to assess the exposure status of determinant factors between the two groups.
Source and Study Population
The source population for this study was diabetic patients age greater or equal to 18 who had follow-up for at least for 6 months in chronic outpatient care in public hospitals of Kambata Tambaro Zone. The study population was
cases were hypertensive patients with hypertension and diabetes comorbidities who were followed up in the chronic care outpatient department were randomly selected.
Controls were patients with diabetes who were followed up in the chronic care outpatient department without hypertension (who came to the same health facility following the cases).
The inclusion criteria for cases were all hypertensive patients with DM age greater or equal to 18 who were on outpatient chronic care follow-up for at least 6 months and for controls all diabetic patients without HTN age greater or equal to 18 who were on outpatient chronic care follow-up for at least 6 months. While patients who were critically ill, patients who had repeated visits during the data collection period (to avoid double interviews), pregnant mothers (due to pregnancy induced HTN) and patients who were hypertensive prior to being diagnosed with diabetes during data collection period was excluded from the study.
Sample Size Determination and Sampling Procedure
The sample size was determined by the double population proportion formula for unmatched case control study using EpiInfo 7.2.4.0 stat calc. The calculation was computed by taking the assumption of a variable “body mass index” percent of controls exposed as 53.71% and percent of cases exposed as 69.9%23 with 95% confidence interval, power being 80%, case to control ratio of 1:1 and by adding 10% non-response rate, the final sample of study participants on one to one (1:1) case to control ratio becomes 336 with 168 cases and 168 controls.
The study was carried out in all public hospitals of the Kambata Tambaro Zone. The total sample size was proportionally allocated to each hospital based on the follow-up of the previous 3 months. Study participants were included using a systematic random sampling technique by calculating the sampling interval (k) based on the chronic care clinic registration follow-up book for each hospital case.  , 388/168 = 2.3 ≈ 2, where
, 388/168 = 2.3 ≈ 2, where
N = number of all HTN among DM patients, n = 168 sample size for cases and 168 sample size for controls since there were 336 cases and controls. Cases were selected by a systematic random sampling technique where every second person was included and controls were patients who came to the same health facility following the cases (Risk Set sampling technique). The first participant in the case group was selected by lottery method while Risk Set sampling was used for controls.
Data Collection Tools and Procedures
An exit interview was conducted in a quiet space by trained data collectors using a structured interviewer administered questionnaire. The questionnaire was prepared after reviewing different peer reviewed published literatures on the determinants of hypertension.8,10,12,14,15,18–21 The questionnaire contained items on socio-demographic and economic factors, clinical and anthropometric factors, lifestyle and behavioral factors, service related factors and knowledge related factors. The Morisky Green Levine Scale which assesses self-reported measures of medication-taking behavior of the patient using four questions each with a yes (1) or no (0) response and total sum scores of (0–4) was used to assess medication adherence. Knowledge was assessed using a 9-item tool, by assigning a score of one to each correct response and zero to the wrong response. All the tools were administered as a part of a single questionnaire. The questions were closed ended. The questionnaire was developed in English and translated into local languages by a language expert (Kambatisa) and translated back into English.
Secondary data (type of DM, type of diabetic drugs patient currently taking and the most recent three fasting blood sugar levels) were reviewed from the chart.
Data Quality Assurance
Data collectors and supervisors were recruited from health professionals in hospitals and nearby health centers and were trained for one day prior to the data collection process to ensure data quality. The prepared tool was pre-tested with 5% of the sample outside the study area (Kulito hospital). Amendments were made accordingly and a question that clearly differentiated a case from a control from the chart was added to the tool. Height was measured using a stadiometer using the average of three measurements in centimeters to the nearest 0.1 cm and recorded. Weight was measured using a digital weighing scale (United Nations International Children’s Emergency Fund seca) and recorded in kilograms to the nearest 0.1 kg. Height of the participants was measured in the upright standing position with no shoes. The weight of the participants was measured while they wore light clothes. The data collectors with the close observation of the doctors and nurses in chronic clinic measured the weight and height of the participants. Body Mass Index was calculated based on the weight and height measurements of the respondents. Moreover, supervisors cross checked the data collectors randomly every day for questionnaire consistency and completeness and the filled questionnaires were checked daily.
Data Processing and Analysis
Data collected through structured interviewer administered questionnaires were entered into EpiData version 3.1, and then exported to SPSS software version 25.0 for data cleaning and analysis. First descriptive analysis (such as frequencies and percentages) were performed for each variable. Subsequently, a bi-variable analysis was performed to identify candidate variables for multi- variable binary logistic regression. Accordingly, variables with a p-value ≤0.25 in bi-variable analysis were included in the final multi-variable logistic regression model to determine the association between the dependent and each independent variable and to adjust for the effect of confounders on the determinants of hypertension. Multi-collinearity was checked using variance inflation factor (VIF) and variables with values less than 10 were included in the model. Hosmer-Lemshow’s goodness-of-fit test was used to check model fitness. The Adjusted Odds ratio (AOR) with 95% confidence intervals was computed to identify the presence and strength of association and statistical significance was set at p-value <0.05.
Operational and term definitions: Cases – patients with hypertension and diabetes mellitus comorbidity who have follow-up in a chronic care outpatient department.
Diabetes mellitus – Occasional plasma glucose value of ≥ 200 mg/dl (≥ 11.1 mmol/l), Fasting plasma glucose of ≥ 126 mg/dl ( 7.0 mmol/l) (fasting time 8–12 h) or an oral glucose tolerance test 2-h value in venous plasma ≥ 200 mg/dl (≥11.1 mmol/l).24
Hypertension – defined as mean systolic blood pressure (SBP) and diastolic blood pressure (DBP) of 140/90 mmHg or greater, confirmed by two measures taken at least 5 minutes apart and hypertensive patients on regular drug therapy or follow-up for hypertension.
Controls – patients with diabetes mellitus and without hypertension who were followed up in the chronic care outpatient department without hypertension.
Good glycemic control – if the patients had 70–130 mg/dl of fasting blood glucose (FBG) upon measurement at three consecutive visits.24
Poor glycemic control – if the patients had FBG >130 or <70 mg/dl upon measurement at three consecutive visits.25
Regular monitoring of blood glucose – self-monitoring of FBS at home at least once every week.26
Alcohol consumption – ever drinking of any type of alcohol (response was either “yes” or “no”) and the frequency of drinking beer or other alcohol was used to evaluate the drinking status. Participants who answered “almost every day and 3–4 times a week” were coded as a frequent drinker; “once or twice a week” were included as less-frequent drinker; and “once or twice a month” were regarded as barely drinking.27
Smoking status – current cigarette smokers were those who smoke at least one cigarette per day for at least 6 months. Former smokers were those who stopped smoking more than 6 months prior to the study.28
BMI – 18.5–24.9 is considered as normal while BMI ≥ 25 kg/m2 is considered as overweight or obese.20
Physically active – an individual who performs physical exercise for at least 30 min per day for at least 5 days per week.29
Physically inactive (sedentary) – an individual who performs physical exercise for less than 30 min per day for less than 5 days per week.29
Adherence to medications – Was assessed using the four items of the Morisky, Green, Levine Scale which assesses self-reported measures of medication-taking behavior of the patient using four questions each with yes (1) or no (0) responses and total sum scores of (0–4, 33). Patients with a score of ≥ 3 (range: 0–4) showed good adherence. Otherwise they were non-adherent.30
Adherence diet – was assessed by practices related to eating a healthy, low fat and low-salt diet. The response options ranged from 0 to 7 days. The patient was adherent if he/she practice low salt and diet technique in at least 6 out of 7 days (scores >54 points out of 63). Otherwise non-adherent.31
Knowledge-related factor – were assessed by assigning a score of one to each correct response and zero to the wrong response. Thus for 9 items, with 32 multiple responses the maximum attainable score was 32 and the minimum was zero. Knowledge level was classified based on the mean score. Poor knowledge was considered if an individual scored < 11.8 mean score whereas good knowledge was considered if an individual scored ≥11.8 mean score.32
Fasting and random blood sugar – WHO and International Diabetic Association (IDA) define diabetes as fasting blood sugar ≥126 mg/dl or random blood sugar ≥200 mg/dl.33
Results
Socio-Demographic and Economic Characteristics of Participants
In this study, 326 patients with diabetes (163 cases and 163 controls) were interviewed, resulting in a response rate of 97%. The mean age of the participants among cases was 51.8 (11.9 Standard Deviation) and the mean age of controls was 42.9 (12.7 SD). The majority 124 (76.1%) of the cases and 121 (74.2%) controls were married. More than one-third of cases, 57 (35%), and 65 (39.9%) controls had secondary education level. Nearly half, 83 (50.9%), of the cases and 96 (58.9%) of the controls were rural residents. Regarding the income of respondents, 50 (30.7%) and 55 (33.7%) among the cases and controls, respectively earn less than 1000 Ethiopian Birr (Table 1).
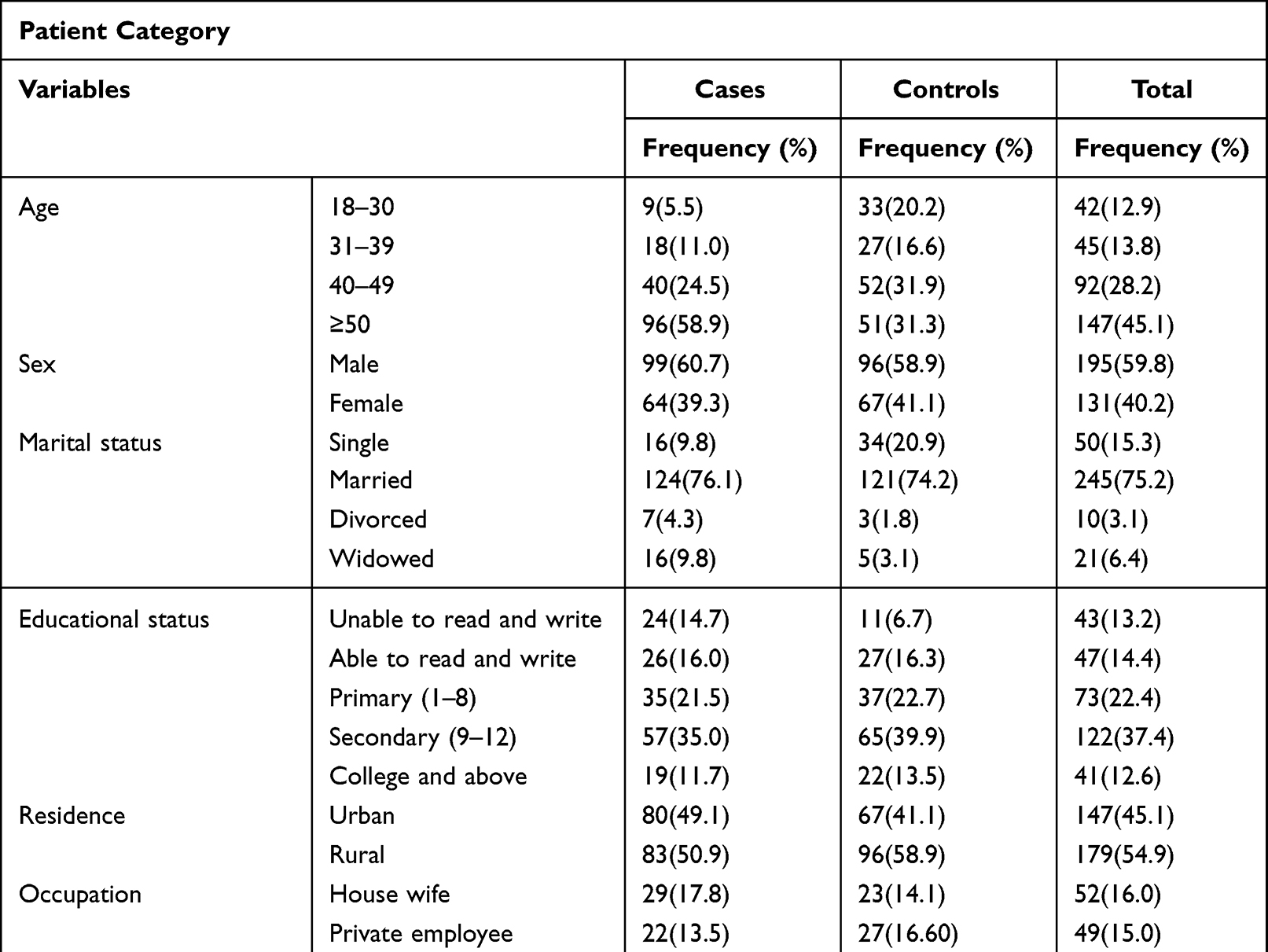 |
Table 1 Socio-Demographic and Socio-Economic Characteristics of Study Participants for a Study on Determinants of Hypertension Among DM Patients in All Public Hospitals of Kambata Tambaro Zone, 2021 (n = 326). |
Clinical and Anthropometric Characteristics
The median duration of DM was 5 years with Inter Quartile Range of 3.8 years. Regarding duration of DM, respondents who have DM for ≥ 5 years among cases numbered 94 (57.7%) and duration of DM for <5 years among respondent controls were 99 (60.7%). There was 46 (28.2%) family history of hypertension among cases, and 137 (84%) controls had no family history of hypertension. Nearly two-thirds of the cases, 106 (65.0), and 100 (61.3%) of controls had poor glycemic control. The body mass indices of the majority of cases and controls were in the normal body weight category, 124 (76.1%) and 122 (74.8%), respectively (Table 2).
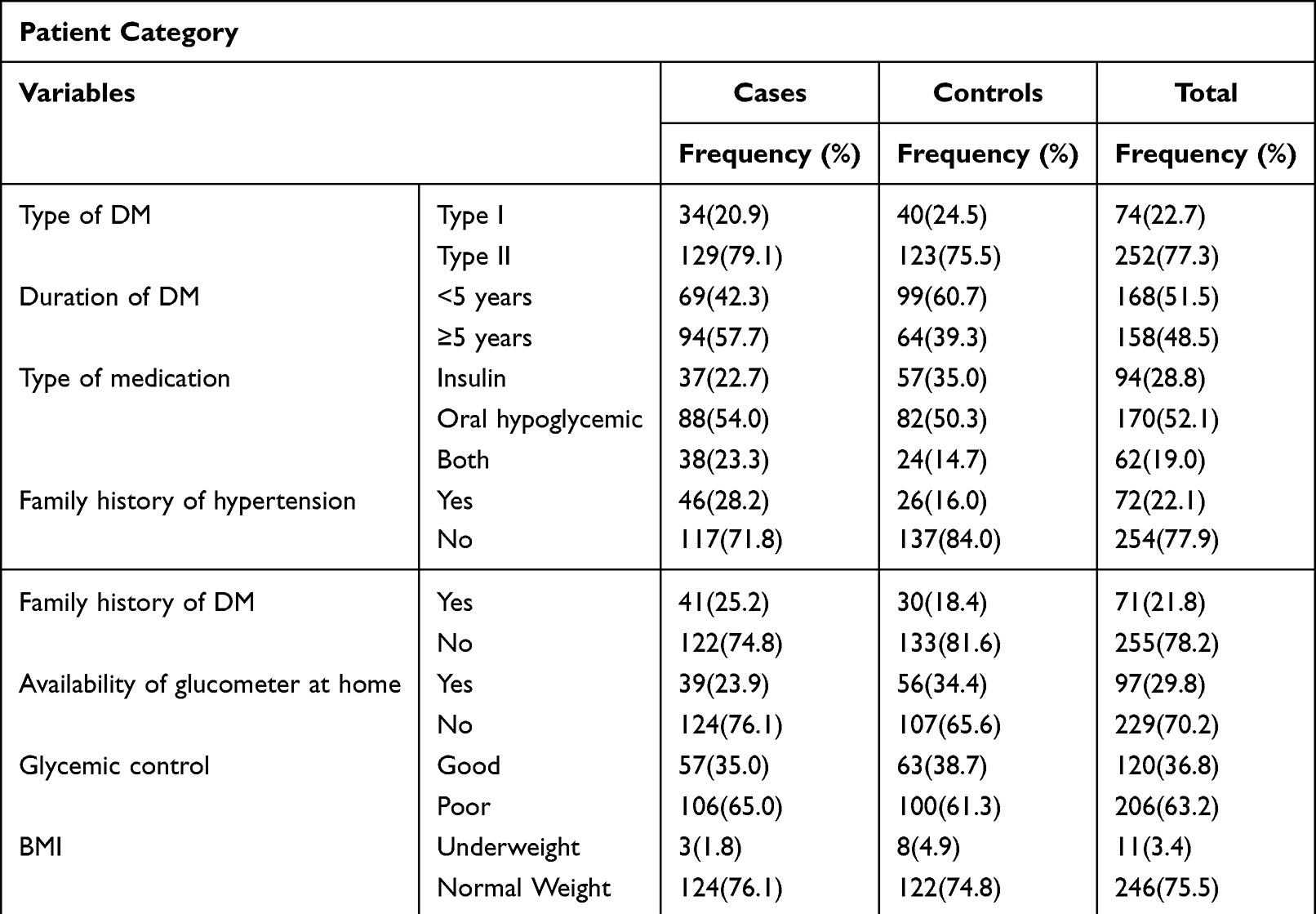 |
Table 2 Clinical Characteristics of Determinants of Hypertension Among DM Patients in All Public Hospitals of Kambata Tambaro Zone, 2021 (n = 326). |
Lifestyle and Behavioral Characteristics
Among the respondents 107 (65.6%) cases were adherent to diet recommendations and 97 (59.5%) controls were adherent to diet recommendations. Most of the cases, 153 (93.9%), and 114 (69.9%) controls were inactive in physical exercise. The majority, 106 (65%), of cases and 134 (82.2%) controls had no history of alcohol consumption (Table 3).
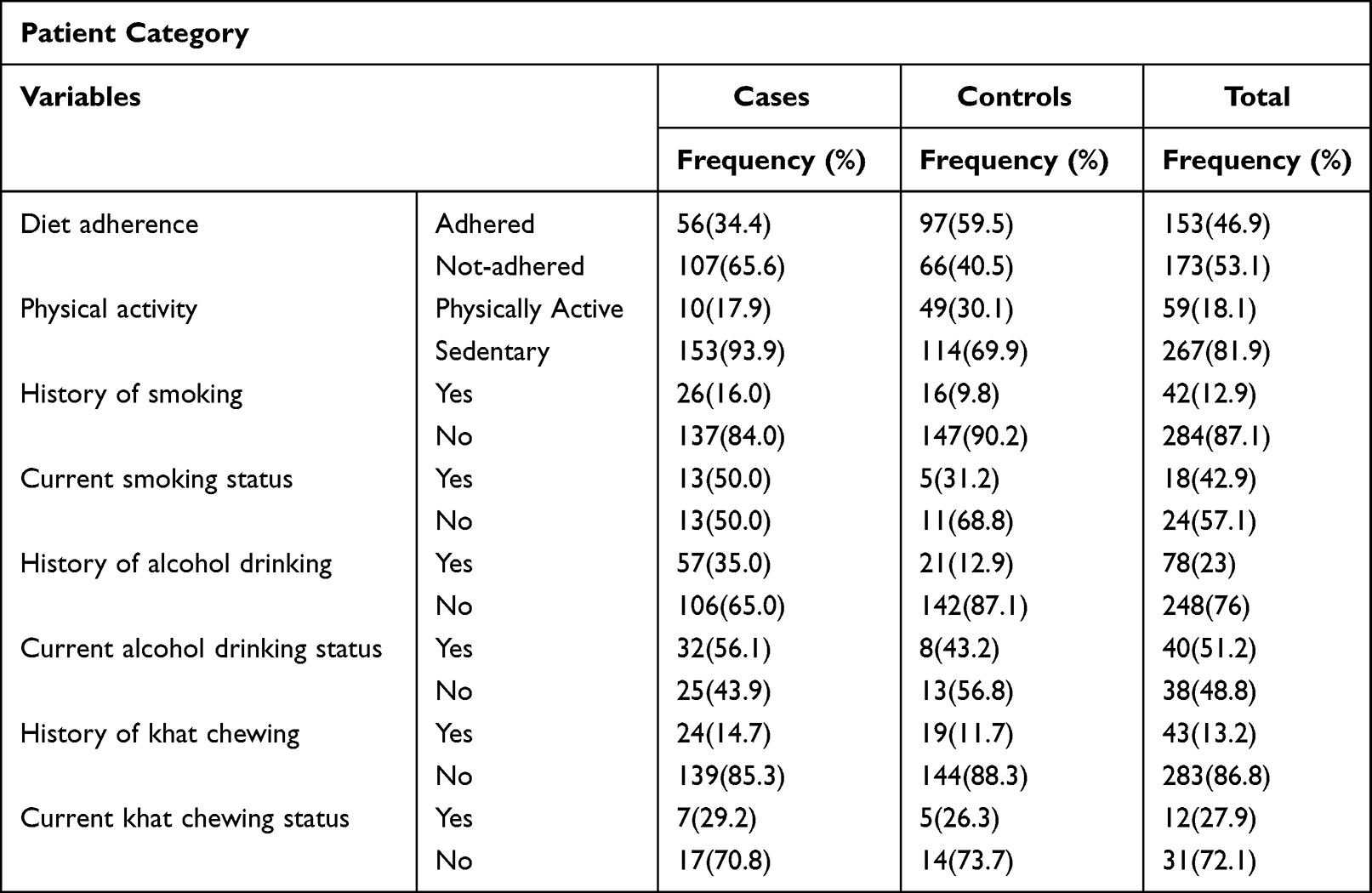 |
Table 3 Lifestyle Determinants of Hypertension Among DM Patients in All Public Hospitals of Kambata Tambaro Zone, 2021 (n = 326). |
Diabetic drug adherence was measured using the 4-item Morisky, Green, Levine scale. More than half of the cases (55.3%) did not adhere to medication and 73.0% of controls did adhere to medication.
Service-Related Factors
More than half (55.2%) of cases and the majority (67.5%) of the controls attended diabetes education. The majority of the cases, 144 (88.3%), and controls, 136 (83.4%), were not members of a diabetic association. Among the cases, 81 (49.7%) and 67 (41.1%) controls covered their medication cost by themselves. About two-thirds of the cases, 109 (66.9%), and nearly half of the controls, 75 (46%), responded that the medication cost was difficult to afford (Table 4).
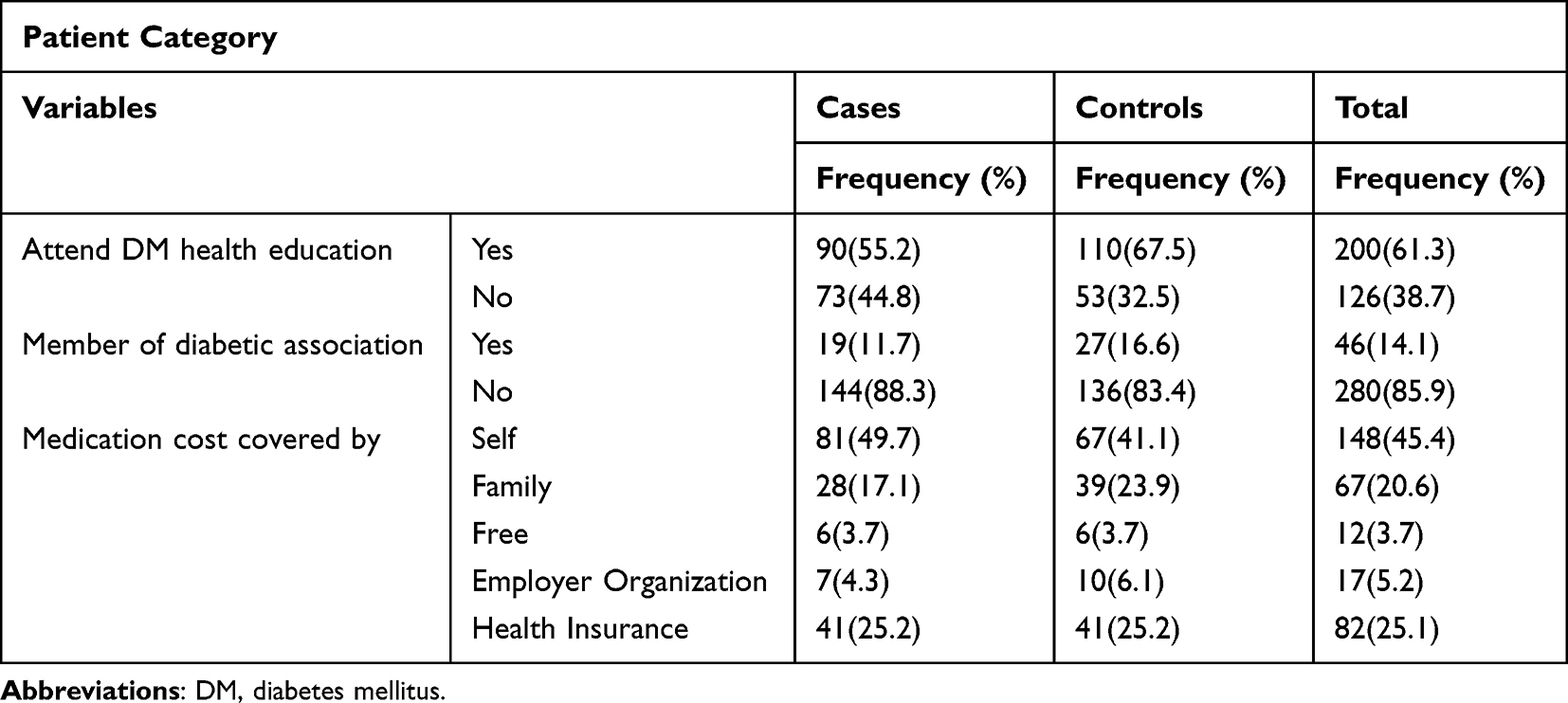 |
Table 4 Service-Related Factors of Determinants of Hypertension Among DM Patients in Public Hospitals of Kambata Tambaro Zone, 2021 (n = 326). |
Knowledge-Related Factors
The mean score of knowledge about DM symptoms, prevention, cutoff point of RBS and FBS and complications among cases and controls was 11.8 (±4.6 SD). More than half of cases, 112 (68.7%), had poor knowledge while more than half of the controls, 108 (66.8%), had good knowledge. The majority of respondents, 131 (80.4%) cases and 114 (69.9%) controls, did not know the cutoff point for RBS. The majority, 113 (69.3%) cases and 88 (54.0%) controls, did not know the cutoff point of FBS. Among the symptoms of diabetes, the majority, 98 (60.1%) of cases and 123 (75.5%) controls, knew increased thirst as a symptom. The less known symptom when compared with others was blurred vision. The majority, 102 (62.6%) of cases and 135 (82.8%) of controls, were aware of excessive weight gain as a risk factor for DM. The least known risk factor was psychological stress. Approximately one-third, 51 (31.3%) of cases and nearly half, 76 (46.6%), of controls knew that heart disease is one of the complications of DM. Foot problems were the least known complications when compared with others. In total, 78 (47.9%) cases and controls knew that avoiding fatty foods could prevent DM. Among the respondents, 63 (38.7%) cases and 29 (17.8%) controls responded that diabetic medication causes ill health respectively.
Factors Associated with HTN Among DM Patients
Age, marital status, family history of hypertension, availability of glucometer at home, physical activity, history of drinking alcohol, attending diabetes mellitus health education, duration of diabetes mellitus, adherence to diabetes mellitus medication, adherence to diet and knowledge about diabetes were the factors that showed possible association in the bi-variable logistic regression. In the final multi-variable logistic regression model, age, physical exercise, history of alcohol consumption and knowledge about DM were statistically significant variables with a p-value <0.05. Among the socio-demographic factors age was a significantly associated variable in developing HTN among patients with DM. The odds of developing HTN among patients with DM were 7 times higher in the age group ≥50 years (AOR = 7.00, 1.69–28.9) than in age group of 18–30. Regarding physical exercise, patients who were inactive in physical exercise were 5 times (AOR = 5.84, 2.47–13.81) more likely to develop hypertension when compared with physically active diabetic patients. Patients with a history of alcohol consumption were 2 times more likely to develop hypertension than their counterparts (AOR = 2.61, 1.35–5.03). Patients who had poor knowledge were 3 times (AOR = 3.04, 1.69–5.47) more likely to develop HTN than those who had good knowledge (Table 5).
 |
Table 5 Factors Associated with Determinants of Hypertension Among DM Patients in Multivariable Logistic Regression in Public Hospitals of Kambata Tambaro Zone, 2021 (n = 326). |
Discussion
According to this study, age, physical exercise, history of alcohol consumption and knowledge about diabetes were significantly associated variables with the development of hypertension among patients with diabetes.
This study revealed that as age increases the odds of developing hypertension increase; however age is a non-modifiable risk factor. The odds of developing HTN among patients with DM were 7 times higher in diabetic patients who are aged ≥50 years than in those age group 18–30. This result was in line with studies conducted in Jimma University Medical Center Ethiopia, Debre Tabor Ethiopia, Adama Ethiopia, Libya (Benghazi). This may be due to aging as generally various physiological functions decline with age.16 Furthermore, increasing age has been linked to a higher incidence of this disease. Moreover, aging induces macro-circulatory changes that promote tissue hypoxia, reduce arteriolar and capillary density, and increase peripheral vascular resistance.34,35 Aging is a physiological process with no direct impact on disease. However, in this period, the passage of time, environmental factors and unhealthy lifestyles negatively impacted the prevalence of chronic diseases.16,35 Aging is accompanied by significant hemodynamic changes, leading to an ever-increasing prevalence of hypertension. Arterial stiffness is the major cause of elevated systolic blood pressure and lower diastolic blood pressure in older adults.35,36
This study also revealed that respondents who were inactive in physical exercise were 5 times more likely to develop hypertension than those who were active in physical exercise. This finding was consistent with those of previous studies, a case control study conducted in Tigray, Ethiopia18 and a cross-sectional study conducted in Libya.14 Physical exercise has been recommended by many professional committees and organizations such as the American College of Sports Medicine, American Heart Association, Canadian Hypertension Education Program, and the European Society of Hypertension/European Society of Cardiology, as a cornerstone of non-pharmacological therapy for hypertension.37 An increasing number of reports suggest that physical exercise can also improve vascular function by reducing arterial stiffness and improving the balance between the vasoconstrictor and vasodilator systems.38 The United States Preventive Services Task Force recently highlighted that patients with risk factors for hypertension should be encouraged to attend physical exercise programs to improve their health.38,39
Among lifestyle and behavioral factors, alcohol intake was a significantly associated variable in this study. Respondents who had a history of drinking alcohol were 2 times more likely to develop hypertension when compared with respondents who had no history of drinking alcohol. This finding was in line with a cross-sectional study conducted in South Africa.40 Healthy lifestyle choices can prevent or delay the onset of hypertension and can reduce cardiovascular risk. Since alcohol consumption is a lifestyle factor, modifications in lifestyle can also prevent hypertension occurrence.41 Studies have shown that a reduction in alcohol intake is effective in lowering the blood pressure both in hypertensive and normotensives and may help to prevent the development of hypertension. There is increasing evidence that alcohol initiates central as well as peripheral reactions which in a synergistic manner have a hypertensive action.42 Excessive alcohol consumption is clearly responsible for adverse health outcomes, mainly various types of cardiovascular diseases especially HTN. Heavy alcohol consumption specifically increases the risk of cardiomyopathy, hypertension and stroke.43 Drinkers who cut back to non-drinking levels can lower their systolic blood pressure by 2–4 mmHg and their diastolic blood pressure by 1–2 mmHg.42
Regarding knowledge of respondents there were limited similar studies before that assessed knowledge of diabetic patients related to hypertension among diabetes in this area. Respondent’s knowledge was a significantly associated variable to develop hypertension among diabetic patients. Respondents who have poor knowledge had 3 times higher odds of developing hypertension than respondents who had good knowledge. The possible explanation could be respondents who had good knowledge may practice and follow counseling and instruction from their doctors and other health professionals about prevention of hypertension and complication of diabetes. Knowledge of diabetes and its management may have a positive impact on prevention of hypertension among diabetic patients.
Limitation of the Study
This study may have introduced social desirability bias on some variables that are sensitive to the respondents such as current alcohol intake and current smoking status. Factors that need laboratory investigation were not included in the study such as lipid profile of the study participants.
Conclusion
This study concludes that age, inactivity in physical exercise, alcohol intake and poor knowledge of diabetes were determinants of hypertension among diabetic patients. Since comorbidity of diabetes mellitus and hypertension put patients at a higher risk of complications and death, taking care for advanced age, promoting physical exercise, education about the impact of alcohol consumption and creating awareness to patients with diabetes by health-care workers are recommended to prevent development of hypertension in patients with diabetes.
Abbreviations
AOR, Adjusted Odd Ratio; BMI, Body Mass Index; CI, Confidence Interval; COR, Crude Odd Ratio; DM, Diabetes Mellitus; ETB, Ethiopian Birr; FBG, Fasting Blood Glucose; FMOH, Federal Ministry of Health; HTN, Hypertension; LMIC, Low and Middle Income Countries; NCD, Non-Communicable Disease; OPD, Outpatient Department; PEN, Package of Essential NCD; RBS, Random Blood Sugar; SNNPR, Southern Nations, Nationalities and Peoples of Region; SPSS, Statistical Package for Social science; WHO, World Health Organization.
Data Sharing Statement
All data are already described and included in the manuscript. Additional data will be made available on request.
Ethical Consideration
Ethical clearance was obtained from the Institute Review Committee from Wolaita Sodo University, College of Health Science and Medicine (Ref. No.CRCSD 12/09/13) before conducting the study. During data collection, each respondent was informed through study participant information sheet about the purpose, scope, expected outcome of the research, potential benefits and harms, confidentiality and their right to withdraw at any time. Anyone who is not willing to participate was not forced to participate in the study. Informed written consent was taken from each participant just before data collection. To keep the confidentiality of the study subjects’ information, personal identifiers were not included in the data collection format and all recorded data were kept in a very secure area where only the principal investigator can access it. This research manuscript compiles with the Declaration of Helsinki.
Acknowledgments
We are very grateful to Wolaita Sodo University College of Health Sciences and Medicine, Kembata Tambaro Zonal Health Office and Hospitals for their cooperation and to all study participants for their willingness and commitment in participating in our study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Mancia G, Dominiczak A, Cifkova R, et al. The task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Blood Press. 2013;22(4):193–278.
2. Bell KTJ, Olin BR. Hypertension: the silent killer: updated JNC-8 guideline recommendations. Alabama Pharm Assoc. 2015;334:4222.
3. Liu JZD, Liu J, Qi Y, Sun J, Wang W, Wang W. Prevalence of diabetes mellitus in outpatients with essential hypertension in China. BMJ Open. 2013;3(11):e003798. doi:10.1136/bmjopen-2013-003798
4. World Health Organization. Global Non-Communicable Diseases Target: Reduce High Blood Pressure. Geneva, Switzerland: World Health Organization; 2016.
5. Lopez-Jaramillo P-L-LJ, Lopez-Lopez C, RodriguezAlvarez MI, Rodriguez-Alvarez MI. The goal of blood pressure in the hypertensive patient with diabetes is defined: now the challenge is go from recommendations to practice. Diabetol Metab Syndr. 2014;6(1):31. doi:10.1186/1758-5996-6-31
6. Alam K, Hankey GJ, Collaborators GRF. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1345–1422.
7. Hurst CTB, Thinkhamrop B, Tran HT. The association between hypertension comorbidity and microvascular complications in type 2 diabetes patients:. Diabetes Metab J. 2015;39(5):395. doi:10.4093/dmj.2015.39.5.395
8. Atlas. IDF Diabetes Atlas.
9. Andualem A, Gelaye H, Damtie Y. Adherence to lifestyle modifications and associated factors among adult hypertensive patients attending chronic follow-up units of Dessie referral hospital, North East Ethiopia, 2020. Integr Blood Press Control. 2020;13:145. doi:10.2147/IBPC.S275575
10. Fan W. Epidemiology in diabetes mellitus and cardiovascular disease. Cardiovasc Endocrinol. 2017;6:8. doi:10.1097/XCE.0000000000000116
11. Peter L-S. Stroke in Developing Countries: Epidemiology, Impact and Policy Implications. Norwich: School of International Development, University of East Anglia; 2009.
12. Kahya E, Harman E, Dolek D, Dolek D, et al. Rate of blood pressure control and antihypertensive treatment approaches in diabetic patients with hypertension. Turk Kardiyol Dern Ars. 2014;42(8):733.
13. Muddu M, Mutebi E, Ssinabulya I, Kizito S, Mondo CK. Hypertension among newly diagnosed diabetic patients at mulago national referral hospital in Uganda: a cross sectional study. Cardiovasc J Afr. 2018;29(4):218–224. doi:10.5830/CVJA-2018-015
14. Nouh FOM, Younis M, Younis M. Prevalence of hypertension among diabetic patients in Benghazi: a study of associated factors. AJMAH. 2017;6(4):1–11. doi:10.9734/AJMAH/2017/35830
15. World Health Organization. Noncommunicable diseases country profiles; 2018.
16. Abdissa D, Kene K. Prevalence and determinants of hypertension among diabetic patients in Jimma University Medical Center, Southwest Ethiopia, 2019. Diabetes Metab Syndr Obes. 2020;13:2317. doi:10.2147/DMSO.S255695
17. Tadesse K, Amare H, Hailemariam T, Gebremariam T. Prevalence of hypertension among patients with type 2 diabetes mellitus and its socio demographic factors in Nigist Ellen Mohamed Memorial Hospital Hosanna, Southern Ethiopia. J Diabetes Metab. 2018;9(4):4–10. doi:10.4172/2155-6156.1000792
18. Mariye T, Girmay A, Tasew H, et al. Determinants of hypertension among diabetic patients in Public Hospitals of the Central Zone, Tigray, Ethiopia 2018: unmatched case-control study. Pan Afr Med J. 2019;33:1.
19. Shiferaw F, Letebo M,Misganaw A, et al. Non-communicable diseases in Ethiopia: disease burden, gaps in health care delivery and strategic directions. Ethiop J Health Dev. 2018;32(3):1.
20. Helelo TGY, Gelaw YA, Adane AA, et al. Prevalence and associated factors of hypertension among adults in Durame Town, Southern Ethiopia. PLoS One. 2014;9(11):e112790. doi:10.1371/journal.pone.0112790
21. Report KTzph. Kambata Tambaro zonal public hospitals report; 2020.
22. Statistical C, Authority. Population and housing census of Ethiopia; 2007.
23. Dedefo A, Galgalo A, Jarso G, Mohammed A. Prevalence of hypertension and its management pattern among type 2 diabetic patients attending, Adama Hospital Medical College, Adama, Ethiopia. J Diabetes Metab. 2018;9(10). doi:10.4172/2155-6156.1000808
24. Petersmann A, Müller-Wieland D, Müller UA, et al. Definition, classification and diagnosis of diabetes mellitus. Exp Clin Endocrinol Diabetes. 2019;127(S 01):S1–S7. doi:10.1055/a-1018-9078
25. Ahmed M, Ejigu SH, Zeleke AZ, et al. Glycemic control, diabetes complications and their determinants among ambulatory diabetes mellitus patients in Southwest Ethiopia: a prospective cross-sectional study. Diabetes Metab Syndr Obes. 2020;13:1089.
26. Gebremichael GB, Berhe KK, Beyene BG, Gebrekidan KB. Self-care practices and associated factors among adult hypertensive patients in Ayder Comprehensive Specialized Hospital, Tigray, Ethiopia, 2018. BMC Res Notes. 2019;12(1):1–6. doi:10.1186/s13104-019-4502-y
27. Gao K, Shi X, Wang W. The life-course impact of smoking on hypertension, myocardial infarction and respiratory diseases. Sci Rep. 2017;7(1):4330. doi:10.1038/s41598-017-04552-5
28. Li GWH, Wang K, Wang K, et al. The association between smoking and blood pressure in men: a cross-sectional study. BMC Public Health. 2017;17(1):797. doi:10.1186/s12889-017-4802-x
29. Muleta S, Melaku T, Chelkeba L, Assefa D. Blood pressure control and its determinants among diabetes mellitus comorbid hypertensive patients at Jimma University medical center, South West Ethiopia. Clin Hypertens. 2017;23(1). doi:10.1186/s40885-017-0085-x
30. Destaw Fetene Teshome1* AFD BMZ. Determinants of blood pressure control amongst hypertensive patients in Northwest Ethiopia. PLoS One. 2018;13(5):e0196535.
31. Warren-Findlow JBDDM, Tapp H, Kuhn L, Tapp H, Kuhn L. Preliminary validation of the Hypertension Self-Care Activity Level Effects (H-SCALE) and clinical blood pressure among patients with hypertension. J Clin Hypertension. 2013;15(9):637–643. doi:10.1111/jch.12157
32. Raj CP, Angadi M. Hospital-based KAP study on diabetes in Bijapur, Karnataka. Indian J Med Spec. 2010;1(2):8083.
33. Shore Hs, Merid M, Beyene AS, et al. Prevalence of hypertension and associated factors in Dire Dawa City, Eastern Ethiopia: a community-based cross-sectional study. Int J Hypertens. 2019;2019:1.
34. De Moraes RTE, Tibirica E. Early functional and structural microvascular changes in hypertension related to aging. Curr Hypertens Rev. 2017;13(1). doi:10.2174/1573402113666170413095508
35. Rizzoni DRM, Nardin M, Chiarini G, et al. Vascular aging and disease of the small vessels. High Blood Press Cardiovasc Prev. 2019;26:183–189. doi:10.1007/s40292-019-00320-w
36. Dominguez L, Veronese N, Barbagallo M. Magnesium and hypertension in old age. Nutrients. 2020;13(1):139. doi:10.3390/nu13010139
37. Pescatello LSMH, Lamberti L, Johnson BT, Johnson BT. Exercise for hypertension: a prescription update integrating existing recommendations with emerging research. Curr Hypertens Rep. 2015;17(87). doi:10.1007/s11906-015-0600-y
38. Bruno C. Lifestyle and hypertension: an evidence-based review. Hypertens Manag. 2018;4(1):1.
39. Sreedhara MSV, Rosal MC, Waring ME, Lemon SC, Lemon SC. Does provider advice to increase physical activity differ by activity level among US adults with cardiovascular disease risk factors? Fam Pract. 2018;35(4):420–425. doi:10.1093/fampra/cmx140
40. Adeniyi OV, Yogeswaran P, Longo-Mbenza B, Goon DT. Uncontrolled hypertension and its determinants in patients with concomitant type 2 diabetes mellitus (T2DM) in rural South Africa. PLoS One. 2016;11(3):e0150033. doi:10.1371/journal.pone.0150033
41. FMOH. National strategic action plan for the prevention and control of NCDs in Ethiopia, 2014 review of selected approaches. Ethiop J Health Dev. 2015;15:1–2.
42. Husain K. Alcohol-induced hypertension: mechanism and prevention. World J Cardiol. 2014;6(5):245.
43. McManus DDYX, Gladstone R, Vittinghoff E, Vasan RS, Larson MG, Benjamin EJMG. Alcohol consumption, left atrial diameter, and atrial fibrillation. Am Heart Assoc. 2016;5. doi:10.1161/JAHA.116.004060
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.