")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Determinants of Home Delivery Among Women in Rural Pastoralist Community of Hamar District, Southern Ethiopia: A Case–Control Study
Authors Wondimu MS , Woldesemayat EM
Received 23 June 2020
Accepted for publication 11 September 2020
Published 15 October 2020 Volume 2020:13 Pages 2159—2167
DOI https://doi.org/10.2147/RMHP.S268977
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Mebratu Shite Wondimu,1 Endrias Markos Woldesemayat2
1South Nations Nationalities and Peoples Regional State Health Bureau, South Omo Zone Health Department, Jinka, Ethiopia; 2Hawassa University, College of Medicine and Health Science, School of Public Health, Hawassa, Ethiopia
Correspondence: Endrias Markos Woldesemayat Email [email protected]
Purpose: Studies addressing determinants of home delivery in pastoralist areas are scarce in Ethiopia. In this study, we aimed to assess determinants of home delivery in rural pastoralist communities of Hamar District, Southern Ethiopia.
Patients and Methods: In April 2018, we conducted a community-based case–control study. Of 35 rural kebeles (lowest level of administration) in the district, 8 were randomly selected. Ninety-nine randomly selected cases (mothers who gave birth at home) and 193 controls (mothers who gave birth at health facility) were included in the study. We used structured questionnaires to collect data. Through face-to-face interview, data on place of delivery, socio-demographic characteristics, obstetric history knowledge and attitude of mothers were collected. We used logistic regression model to measure association between variables.
Results: Late initiation of antenatal care (AOR = 4.6, 95% CI = 1.2, 17.1), husbands only decision-making (adjusted odds ratio [AOR] =7.2, 95% CI = 2.1, 24.5), women’s preference for traditional birth attendants (TBAs) (AOR = 3.9, 95% CI = 1.2, 12.5), and not involving in women’s development army (WDA), (AOR = 3.3, 95% CI = 1.0, 10.5) increased the risk of home delivery. Moreover, low maternal knowledge on danger signs of pregnancy (AOR = 6.5, 95% CI = 1.5, 29.0) and negative maternal attitudes towards institutional delivery (AOR = 4.4, 95% CI = 1.4, 14.1) were other factors that increased the risk of home delivery.
Conclusion: Among our study participants, a number of factors increased the risk of home delivery. Improving women’s awareness on the importance of institutional delivery, establishing systems for integration between TBAs and health facilities, empowering women and promoting them to participation in WDA were recommended.
Keywords: determinants, home delivery, pastoralist community, Hamar District, Southern Ethiopia
Introduction
Pregnancy is a physiological state which most women aspire to have at some point in life.1 Women give birth into two mutually exclusive places; home or health institutions. Home deliveries increase the likelihood of maternal and newborn morbidity and mortality.2 In-order to prevent this, increasing the proportion of deliveries attended at health institutions; where women obtain health care by skilled professionals are recommended.
Globally, every year about 303,000 women die due to complications of pregnancy or childbirth. Developing countries accounted for nearly 99% of the global maternal deaths.3 Ethiopia is 4th among the top ten countries in terms maternal death burden with annual number of maternal deaths of 13,000.3 The complication of pregnancy and childbirth does not end by the loss of maternal life only. It may result in devastating effects on the family she leaves behind.4
The global effort to address maternal mortality was started as Safe Motherhood Initiatives in 1987.5 Attention to the problem has increased since 2000 when the United Nations targeted the reduction of maternal mortality by 75% by the year 2015. The Sustainable Development Goals, which was endorsed in 2015 calls for bringing maternal mortality rate down from 216 deaths per 100,000 live births to 70 deaths per 100,000 live births by 2030.6,7
Though 75% or more of maternal deaths could be averted by skilled birth attendants (SBA) during labor, delivery and after childbirth,8 almost 60% of African women give birth without SBAs at home in contrast to less than 1% in developed countries.9 The 2016 Ethiopian Demographic and Health Survey (EDHS) showed that the national prevalence of home delivery was 73%, with significant variations across regions ranging from 3% in Addis Ababa to 85% in Afar.10 In Southern Ethiopia, the prevalence of home delivery ranged from 49.3% in Anlemo District of Hadiya Zone to 84% in rural area of Kembata-Tembaro Zone.11–13
Ethiopian pastoralist communities occupy 61% of the land mass in over 122 districts.14 Studies revealed that the proportion of home delivery is more common in the pastoralist communities. For instance, findings from studies conducted in pastoralist districts in Dubti, Afar Region, Ethiopia indicated 92.6% of births took place at home.15 Similarly, the magnitude of home delivery reported in semi-pastoralist community of Malie District, Southern Ethiopia was 83.3%.16 Several factors could hinder women’s utilization of institutional deliveries in the pastoralist communities; which includes, poor access to transportation,10,17 cultural norms15,16 and low socio-economic status of women.18 The Ministry of Health in Ethiopia has been addressing such challenges by building maternity homes for term pregnant women who come from peripheries and provision of institutional deliveries and ambulance service free of charge. According to Hamar District Health Office 2017 Annual Report, about two-thirds of childbirths in the district were attended at home. However, there is no study which focuses on determinants of home delivery in a rural-pastoralist context in the Southern Ethiopia. Therefore, in this study we aimed to assess determinants of home delivery among women who gave birth 12 months preceding the survey in Hamar District of pastoralist community.
Patients and Methods
Study Design, Setting and Population
We conducted a community-based case–control study in rural pastoralist comminutes of Hamar district, Southern Ethiopia. The district is sub-divided in to 38 kebeles (of which 35 are rural kebeles) with an estimated population of 75,758. A Kebele is the lowest administrative unit in Ethiopia. Nearly 97% of the population in the study area is pastoralists. Hamar district has three Health Centers and 32 Health Posts. However, delivery services are not rendered at health posts in the study area.
All women who gave birth in rural kebeles of the district in the year preceding the survey were considered as our source population. Randomly selected cases and controls in the same period from the selected kebeles were our study populations. Cases were mothers who gave birth at home; while controls were mothers who gave birth at health institution in the district. All women who gave birth in a year preceding the survey living in the study area were included, while women with serious health problems during the interview period were excluded from the study.
Home delivery refers to a non-skilled delivery which took place in non-clinical setting. Institutional delivery refers to deliveries which took place at health centers or hospitals, where women receive skilled birth care by a health professional.10 Traditional birth attendant (TBA) is a woman who assists delivering mother during childbirth at home, who initially acquired her skills by delivering her own babies or through apprenticeship to other TBAs.19 Women development army (WDA) refers to a group of 25 to 30 women household heads organized based on settlement or proximity, they share experiences and take practical actions to improve health of individuals, families and community.20
Sampling
Sample size was determined using Epi Info version 7 statistical software. Time to reach health facility was used as exposure variable taken from a study report from northern Ethiopia.21 Proportion of exposure among controls and cases considered were 13% and 28.2%, respectively. Considering 95% confidence interval (CI), 80% power of the study, a case to control ratio of 1:2 (which was done to increase the power), and 15% contingency for non-response rate, we calculated a sample size of 309 mothers (103 cases and 206 controls) to be included in the study. Of 35 rural kebeles found in the district eight were randomly selected. Five hundred and nine mothers who gave birth in the year preceding the survey were enumerated. This was used as a sampling frame. Based on the sampling frame, we allocated sample size proportionally to the number of women in each of the selected kebeles. Systematic sampling technique was used to select women from the sampling frame. The sampling interval was obtained by dividing the sample size to the total number of participants found in all the selected kebeles.
Data Collection
Data were collected in April 2018 through a face-to-face interview. We used a structured questionnaire adapted from another study.17 Data collection tool used in the study was annexed as supporting information. Place of delivery was the outcome measure evaluated in the study. We selected data collectors and supervisor, from health facilities found in the same district. The supervisor has a training background of Bachelor of Science (B.Sc.) in public health. Enumerators were four women with a diploma level training in health science. Prior experience and fluency of local language were considered in selection of the data collectors and the supervisor. The principal investigator delivered training to both the data collectors and the supervisor on issues related to the study.
Enumerators asked the study participants questions about socio-demographic characteristics like age, marital status, maternal and educational status of the study participants. Past obstetric history related characteristics like parity, gestational age (GA) at first antenatal care (ANC) visit, decision-making power on place of delivery, knowledge of mothers on danger signs of pregnancy and attitude of mothers towards institutional deliveries were other variables measured. Women’s need for ritual celebrations during childbirth at home, worrying about the gender of SBAs, the desire to bury placenta of newborn at home, time to reach the nearest health facility, being a member of the WDA were additional exposure characteristics measured in the study.
Women’s knowledge on danger signs of pregnancy and complications of labor or complications of delivery were measured using eleven questions with a minimum score of 0 and a maximum score of 11. Responding correct answers for at least 75%, 50–74.9% and less than 50% of the questions were considered as having of good, fair and poor knowledge, respectively.21 Attitude towards institutional delivery was measured with 10 attitude related questions. The response of each item had three choices agree, neutral and disagree. We gave points for each of the responses. The points were ‘0’ if the participant disagrees, ‘1’ if the participant responds as neutral and ‘2’ if the participant agrees. Then the points were summed which eventually gave a minimum response of ‘0’ and a maximum response of ‘20’ points. The final score was dichotomized into positive attitude if a woman scored at least 50% and negative attitude if a woman scored below 50%.22
Data Quality Control
We prepared a structured questionnaire in English then translated it to Amharic, and re-translated it back to English. The principal investigator gave training to the supervisor and the data collectors on the objective of the study, techniques of the interview and confidentiality related to the information. We did pre-test in a kebele not included in the study. Based on the pre-test result, essential modification was done to the questionnaire. Data collection was supervised by the principal investigator and the supervisor.
Data Processing and Analysis
The data were first checked for completeness, then coded, entered, cleaned and analyzed using Statistical Package for Social Science (SPSS) Version 20. The outcome variable (place of delivery) was dichotomized into case, if the delivery took place at home and control, if the delivery place was at a health facility. To estimate the rural households’ asset levels, a wealth ranking was developed based on having the following type and number of cattle. Poor households were households with less than 5 cows or oxen or 5–9 sheep or goats. Middle level asset was considered if their households owned 5–9 cows or oxen or 1–5 camels or 10–19 sheep or goats. Rich households were households with at least 10 cows or oxen or 5–9 camels or having at least 20–49 sheep or goats. A similar type of wealth ranking was used in a previous study.23
We calculated frequencies and Chi-square test. Logistic regression model was used to examine the relation between the dependent variable and independent variables. Variables with P-value less than 0.20 in bivariate logistic regression analysis were entered into the multivariable logistic regression model, which showed independent determinants of home delivery. Adjusted Odds Ratio (AOR), along with the 95% CI were used to present statistically significant associations. The fitness of the model was checked by Hosmer-Lemeshow goodness of fit test.
Results
Socio-Demographic Characteristics
Of the eligible 309 mothers, 292 (99 cases and 193 controls) participated in the study making a response rate of 94.5%. The mean (SD) age for cases and controls were 29.20 (6.3) and 29.1 (7.0) years, respectively. Illiterates constituted 93 (93.9%) of cases and 175 (90.7%) of controls. The proportion of participants who visited ANC during the recent pregnancy was 176 (91.2%) for cases and 72 (72.7%) for controls. As illustrated in Table 1, there was no significant difference among cases and controls by socio-demographic characteristics.
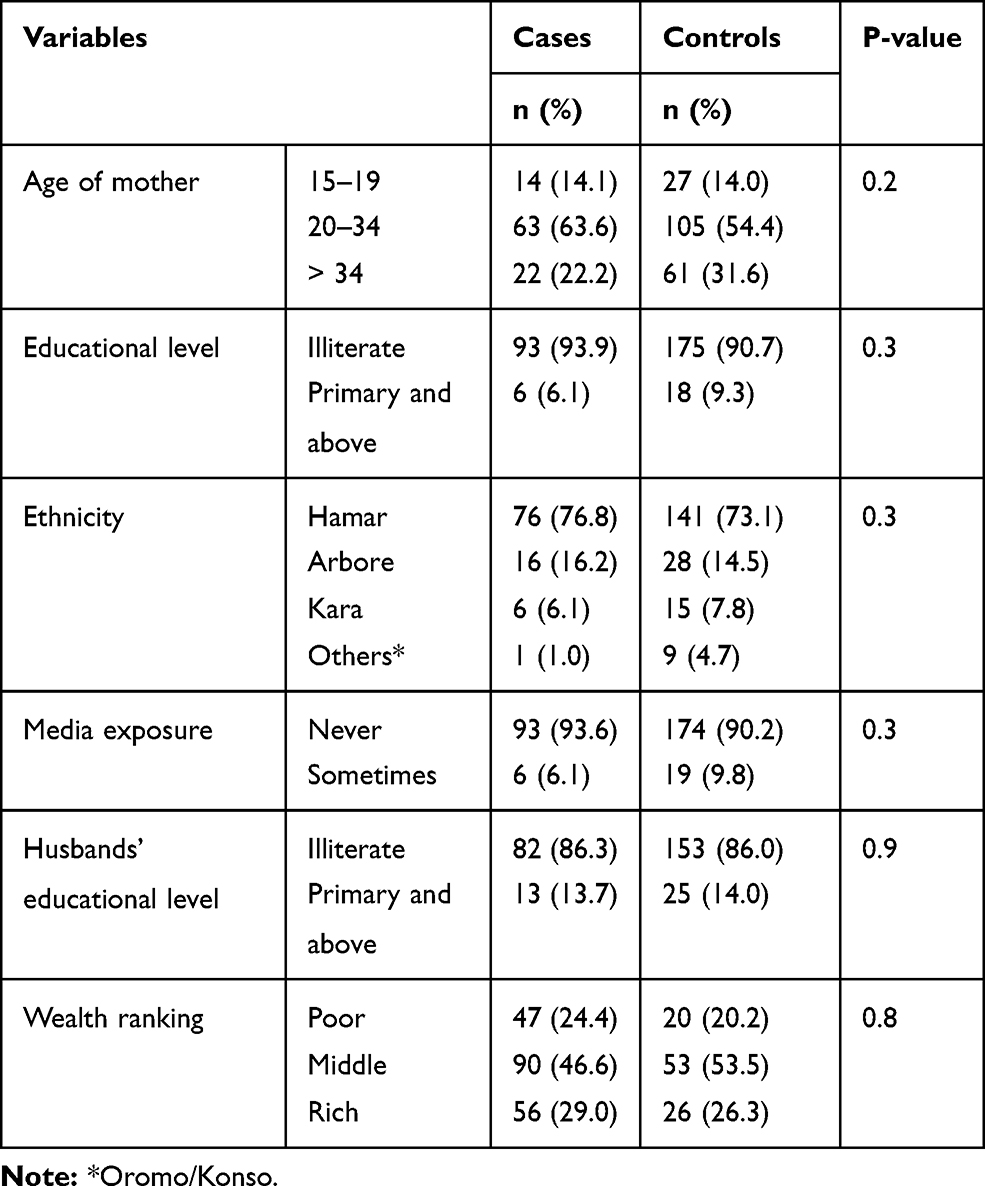 |
Table 1 Socio-Demographic Characteristics of the Study Participants, Hamar District, Southern Ethiopia |
Obstetric History, Knowledge, Attitude and Other Characteristics
The majority (80; 80.8%) of cases and 142 (73.5%) of controls had given childbirth more than one time. The mean (SD) GA during their first ANC visit was 21.4 (+6.5) weeks for cases and 14.4 (+5.9) weeks for controls. Mothers with poor knowledge on danger signs of pregnancy were 65 (65.7%) for cases and 65 (33.7%) for controls. Fifty-nine (59.6%) cases and 46 (23.8%) controls had negative attitude towards institutional delivery. There was significant difference between cases and controls in the number of ANC visit, GA at first ANC visit, decision-making power on place of delivery, place of birth preceding the most recent birth, preference of birth attendant, preference of sex of the SBA and active participation in WDA (p < 0.001) (Tables 2 and 3).
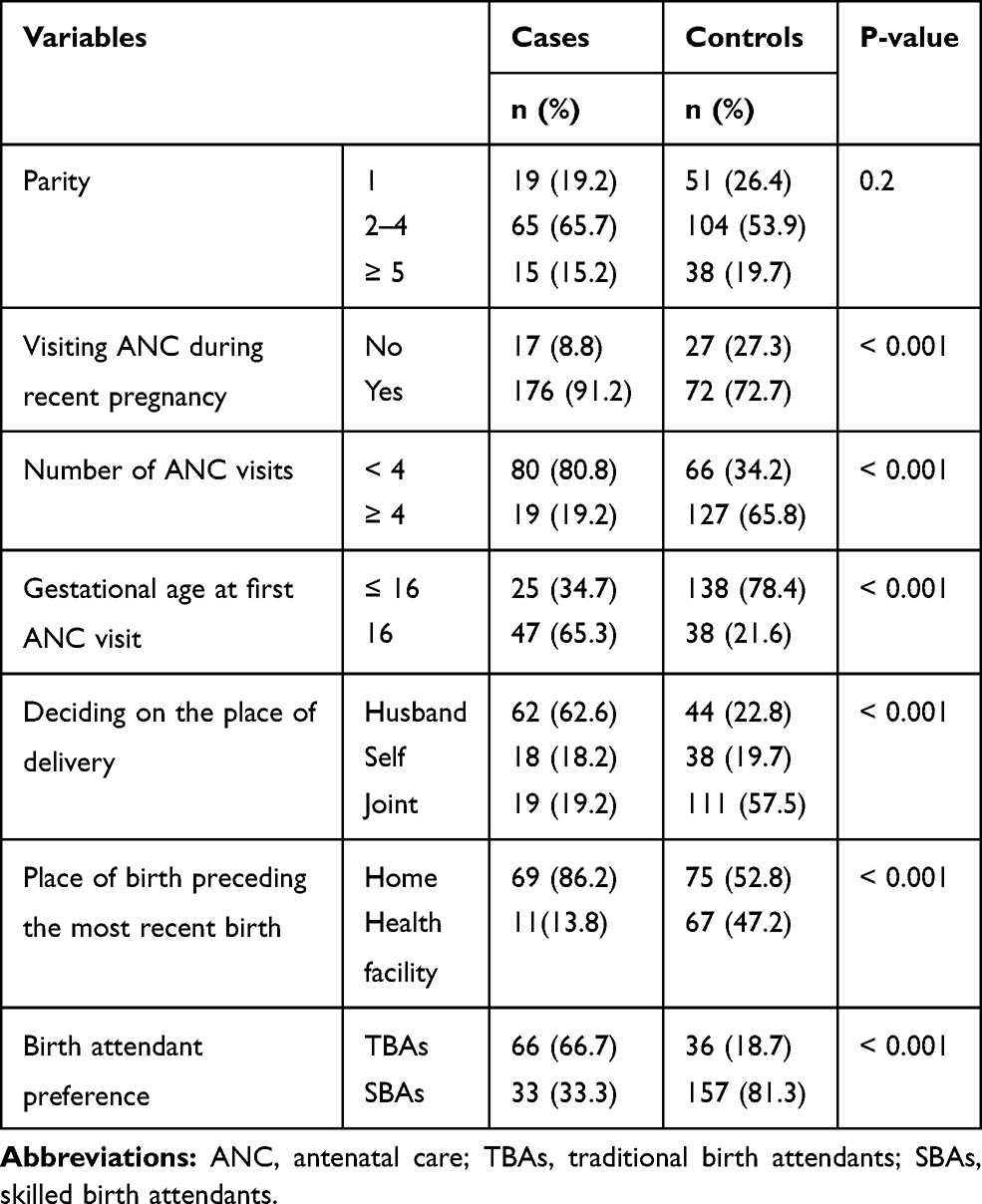 |
Table 2 Obstetric Characteristics of Women in Hamar District, Southern Ethiopia |
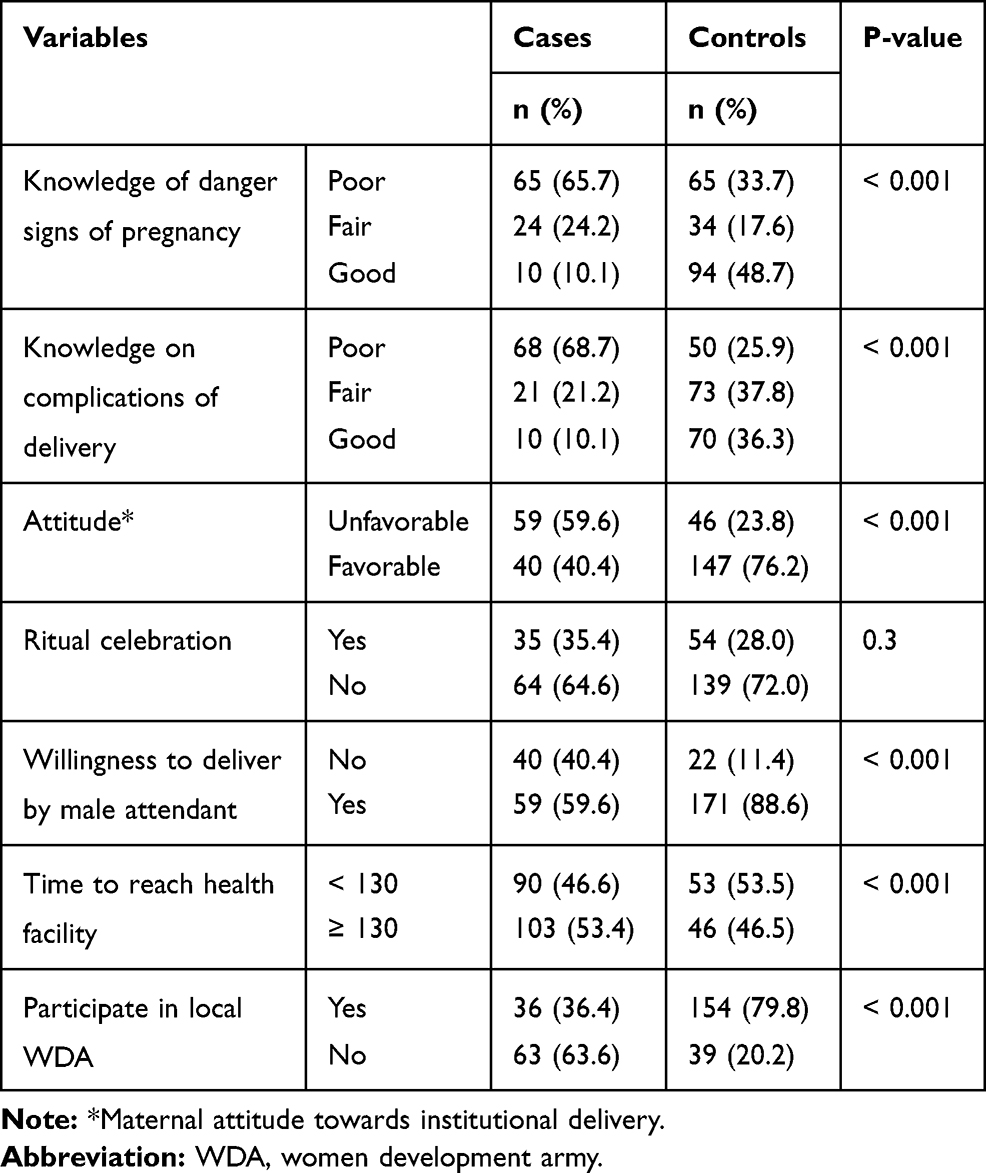 |
Table 3 Knowledge, Attitude and Other Characteristics of Women in Hamar District, Southern Ethiopia |
Determinants of Home Delivery
Table 4 shows results of logistic regression analysis of the study variables. Of 21 variables included in a bivariate analysis, 13 had P-value below 0.20. These were considered in the multivariate analysis. According to the latter analysis, the likelihood of delivering at home was more than four times higher among women who started their 1st ANC visit after 16th weeks of GA than women who started before 16 weeks of GA (AOR = 4.6, 95% CI = 1.2, 17.1). Women whose husbands made the final decision on where to give birth were more than seven times higher to give birth at home than women who make with a joint husband–wife decision (AOR =7.2, 95% CI = 2.1, 24.5). The probability of home delivery was nearly four times greater among women who preferred TBAs during childbirth than women who preferred SBAs (AOR = 3.9, 95% CI = 1.2, 12.5). Mothers with poor knowledge of the danger signs of pregnancy were more than six times likely to deliver at home compared to mothers with good knowledge (AOR = 6.5, 95% CI = 1.5, 29.0). Moreover, having negative attitude towards institutional delivery had significantly increased the odds of home delivery (AOR = 4.4, 95% CI = 1.4, 14.1). The AOR for women who did not participate in WDA was more than three times higher to give childbirth at home than women who were members of WDA (AOR = 3.3, 95% CI = 1.0, 10.5).
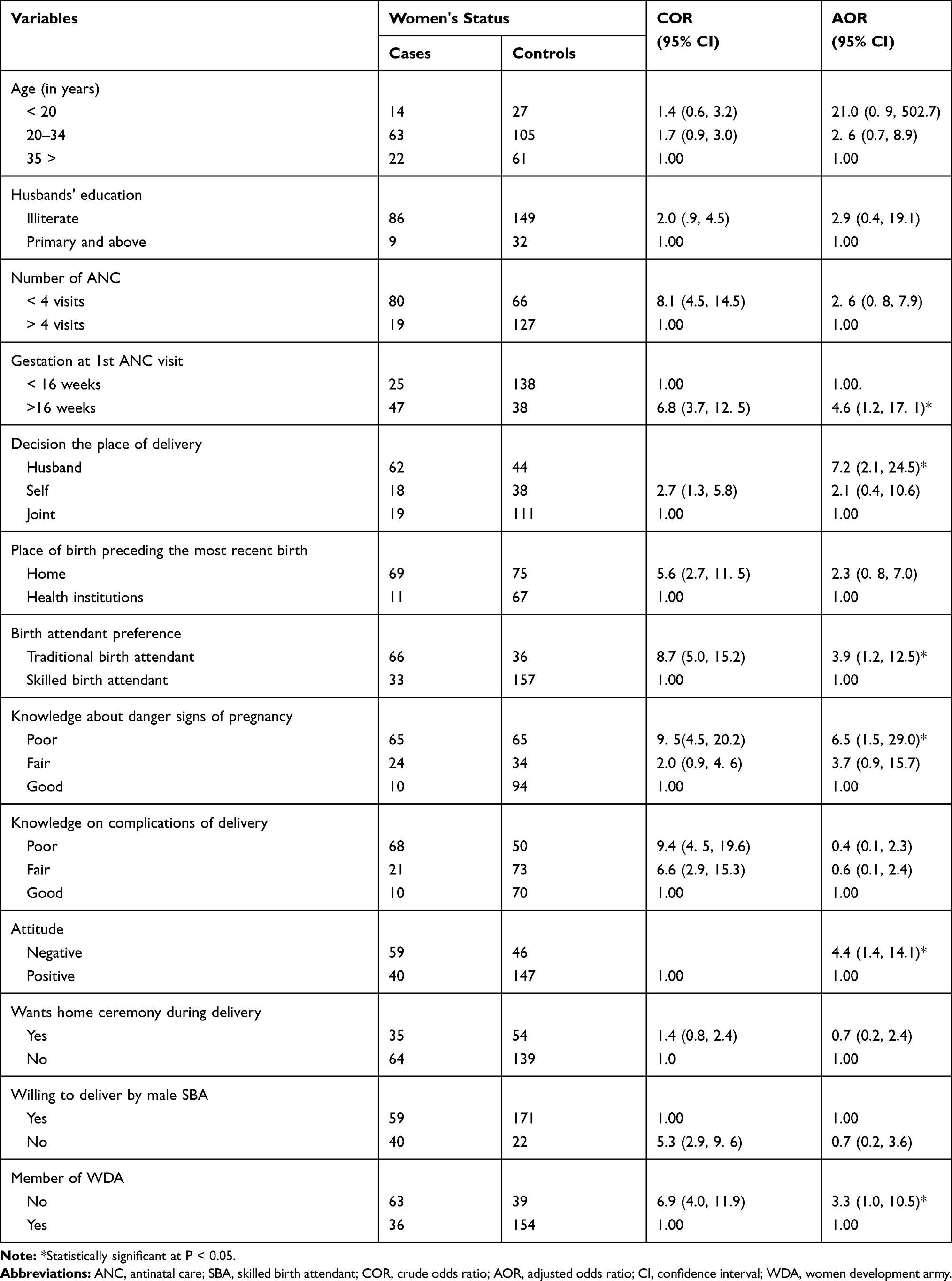 |
Table 4 Logistic Regression Analysis of the Study Variables, Hamar District, Southern Ethiopia |
Discussion
This study showed important determinants of home delivery in rural pastoralist communities of Hamar district, Southern Ethiopia. GA at starting of ANC, knowledge of mothers on the danger signs of pregnancy, women’s attitude towards institutional delivery, decision-making power on place of delivery, mothers preference of who attends the delivery and women’s involvement at WDA predicted place of delivery.
In this study, mothers who started their ANC visit before 17 weeks of GA were about five times less likely to deliver at home than their counter part. This is in agreement with reports from Northern Ethiopia21,24 which showed women with delayed initiation of ANC attendance until the end of the second trimester were more likely to deliver at home than those who attended the services earlier. This could be due to an increased chance of accepting and implementing the advices rendered by the health professional if a woman starts ANC earlier. Therefore, tracing pregnant women at early stage of pregnancy and timely initiation of ANC is important to minimize the risk of home delivery.
Husbands play a significant role in deciding where their wife should give birth. Women whose husbands made the final decision regarding the place of childbirth were roughly seven times more likely to give birth at home compared to women who make a husband–wife joint decision. In contrast to this, a couple of studies conducted in Ethiopia21,25 showed no supporting evidence of association between the place of delivery and decision-making role. The discrepancy might be due to difference in methodology, study population, and/or sample size. However, the current study finding is in agreement with the report from Boricha District, South Ethiopia.26 In pastoralist communities, it is the husband’s role making every decision about his wife including her own health. If women do not get the good will of their husbands, they will not get financial and other supports to go to health institutions, so they give birth at home. To change this trend it is important establishing women empowerment and teaching husbands on the importance of collaborative decision-making. Moreover, involving husbands in ANC visits may help them to prevent home deliveries.27,28
Our data showed women who preferred TBAs were more likely to deliver at home compared to women who preferred SBAs. This finding is supported by studies conducted in Afar, Ethiopia,23 Buta-Jira district Ethiopia29 and in the rural district of Ibanda, Uganda.30 The preference of TBAs over SBAs might be due to their closeness, sympathy and cultural sensitivity of the TBAs and the provision of more psychological and physical support to the women than the health care workers might do. We suggest the importance of conducting studies to explore these factors and apply interventions to minimize home deliveries.
As expected, women in the Hamar District who had little knowledge of the danger signs of pregnancy were more likely to have a home delivery. This result is in agreement with the reports from other settings.21,24,31 This could be due to low socioeconomic status of the women in these settings and the absence or late initiation of ANC which could be related to inaccessibility of the health facilities. Delayed or absence of ANC visit could prevent mothers from getting appropriate information regarding obstetric danger signs of pregnancy.
Our result indicated that the majority (60%) of women who had a home birth had negative attitudes towards institutional deliveries. Home delivery was 4.4 times more common among mothers with negative attitudes than among mothers with positive attitudes. This finding is in agreement with reports from previous Ethiopian studies.17,32 The negative attitude towards institutional delivery could be related to women’s poor knowledge of the danger signs of pregnancy. This diminishes the likelihood of seeking ANC and delivery service at health institutions. Providing health education to pregnant women on the danger signs of pregnancy and the advantages of attending institutional deliveries could be important to improve the knowledge and attitude of women.
The instances of home deliveries was lower among mothers who were WDA members compared to women who were not. Evidence shows that in areas with advanced WDA networks, the coverage of key health interventions including institutional delivery has improved.33 Women who were members of WDAs were more likely to discuss their health, including where to give birth and hear other women's experiences. Moreover, full-term pregnant woman in a WDA can be referred to maternity waiting homes (rooms built to admit full-term pregnant women coming a long way).
Unlike the findings in previous studies,34–36 the age of women was not associated with home delivery in the Hamar district. In rural Ethiopia and in pastoralist comminutes in particular, most women do not remember their accurate date of birth. This may lead to recall bias. In a crude analysis of our result, the number of ANC visits showed association with home delivery. However, the association did not continue in the adjusted analysis. This finding is consistent with other reports.37 However, a study in Dallocha town, SNNPR, Ethiopia, confirmed the association between the number of ANC visits and home delivery in other settings.37,38 Women with fewer ANC visit might be less likely to get more information about risks and problems that they might encounter during childbirth.
Strengths and Limitations of the Study
We conducted a community-based study in rural settings and involved population-based controls. These could be considered as strengths of the study. Recall bias; a bias that may arise due to not remembering some of the measured characteristics, for example, age of mothers may be the main limitation of our study.
Conclusions
This study confirmed that the odds of home delivery were considerably higher among women with late initiation of ANC, low knowledge of the danger signs of pregnancy and women with a negative attitude towards institutional deliveries. Moreover, women for whom their husbands alone decided their place delivery, those who preferred TBAs to SBA, and those who were not member of locally established WDAs had higher chance of delivering at home. Health workers in the district need to initiate ANC at the right time through providing intensive information education communication to improve women’s awareness on the importance of institutional deliveries and improve women attitude towards institutional delivery. To promote joint decision-making on the place of delivery, we suggest the importance of female empowerment and providing health education for their partner. More studies could be done to explore why women prefer TBAs than SBAs, husband’s understanding and attitude regarding institutional delivery and implementation of interventions to minimize home deliveries in these settings. Moreover, promoting women to participate in the locally established WDA is vital.
Abbreviations
ANC, Antenatal care; AOR, Adjusted odds ratio; CI, Confidence interval; COR, Crude odds ratio; DHS, Demographic and health survey; SD, Standard deviation; SPSS, Statistical package for social science; TBAs, Traditional Birth Attendants; WDA, Women Development Army.
Data Sharing Statement
The data sets used in this study are available from the corresponding author on reasonable request.
Ethics Statement
The study was approved by Institutional Review Board (IRB) of Hawassa University College of Medicine and Health Sciences (Reference No. IRB/068/10). We received official support letter from South Omo Zone Health Department and Hamar District Health Office. Informed verbal consent was obtained after appropriate information was provided for each study participants or their husbands (for mothers below 18 years of age). Study participants were informed that they have full right not to participate in the study. The study was conducted in accordance with the Declaration of Helsinki. The IRB office in Hawassa University College of Medicine and Health Sciences approved the consent process.
Acknowledgment
We thank Hawassa University for the financial support and we extend our gratitude to the data collectors, the supervisor and the study participants for their time and courtesy.
Funding
Hawassa University, Ethiopia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. FMOH. Maternal Death Surveillance and Response Technical Guideline. Addis Ababa, Ethiopia; 2014.
2. Thind A, Mohani A, Banerjee K, Hagigi F. Where to deliver? Analysis of choice of delivery location from a national survey in India. BMC Public Health. 2008;8(1):29. doi:10.1186/1471-2458-8-29
3. WHO. Trends in Maternal Mortality: 1990 to 2013. Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Geneva, Swizerland: WHO; 2015.
4. Moucheraud C, Worku A, Molla M, Finlay JE, Learning J, Yamin AE. Consequences of maternal mortality on infant and child survival: a 25-year longitudinal analysis in Butajira Ethiopia (l987–2011). Reprod Health. 2015;12(Supp S1):S4. doi:10.1186/1742-4755-12-S1-S4
5. Mahler H. The safe motherhood initiative a call action. Report on safe motherhood conference 1987 preventing the tragedy of maternal death; a report on the international safe motherhood conference, Nairobi, Kenya. Lancet. 1997;1:668–670.
6. WHO. Global, regional, and national levels of maternal mortality, 1990–2015: a systematic analysis for the global burden of disease. Lancet Glob Health. 2016.
7. Say L, Chou D, Gemmil A, Tuncalp O, Moller AB, Daniels J. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2015;p2.
8. Harvey S, Ayabaca P, Bucagu M, et al. Skilled birth attendant competence: an initial assessment in four countries, and implications for the safe motherhood movement. Int J Gynecol Obstet. 2004;87(2):203–221. doi:10.1016/j.ijgo.2004.06.017
9. Fact sheet: maternal MORTALITY. Available from: http://wunrn.com/2015/05/maternal-mortality-key-facts-who/.
10. CSA. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia: Central Statistical Agency; 2016.
11. Ibrajim SA, Handiso TB, Jifar MS, Yoseph E. Analyzing prevalence of home delivery and associated factors in Anlemo District, Southern Ethiopia. Int Ann Med. 2017;1(6).
12. Ayele G, Tilahun M, Merdokiyos B, Animaw W, Taye W. Prevalence and associated factors of home delivery in Arbaminch Zuria district, southern Ethiopia: community based cross sectional study. Sci J Public Health. 2015;3(1):6. doi:10.11648/j.sjph.20150301.12
13. Shiferaw S, Spigt M, Godefrooij M, Melkamu Y, Tekie M. Why do women prefer home births in Ethiopia? BMC Pregnancy Childbirth. 2013;13(5). doi:10.1186/1471-2393-13-5
14. Abduselam MA. Pastoralism and development policy in Ethiopia: a review study. BIRCI J. 2019;2(4):1–11.
15. Nejimu B, Mohammed H. Pastoralism and antenatal care service utilization in Dubti District, Afar, Ethiopia: a cross-sectional study. Springer Open. 2016;6(15).
16. Gebeyehu D, Hailemariam T. Utilization of institutional delivery services and associated factors among mothers in semi-pastoralist, Southern Ethiopia. J Womens Health. 2015;4(7).
17. Bedilu K, Nigussei M. Delivery at home and associated factors among women in child bearing age, who gave birth in the preceding two years in Zala District, southern Ethiopia. J Public Health Epidemiol. 2017;9(6):177–188. doi:10.5897/JPHE2017.0921
18. Ogolla J. Factors associated with home delivery in West Pokot County of Kenya. Adv Public Health. 2015;2014(6).
19. WHO. Traditional Birth Attendants: A Joint WHO/UNFPA/UNICEF Statement. Geneva, Swizelnd: World Health Organization; 1992.
20. Damtew ZA, Karim AM, Chekagn CT, et al. Correlates of the women’s development army strategy implementation strength with household reproductive, maternal, newborn and child healthcare practices: a cross-sectional study in four regions of Ethiopia. BMC Pregnancy Childbirth. 2018;18(S1):373. doi:10.1186/s12884-018-1975-y
21. Tsegay R, Aregay A, Kidanu K, Alemayehu M. Determinant factors of home delivery among women in Northern Ethiopia: a case control study. BMC Public Health. 2017;17(1). doi:10.1186/s12889-017-4159-1
22. Mohammed M. Institutional delivery service utilization and associated factors among mothers in Afambo district, Ethiopia. Med Res Chronicles. 2017;4(4):363–379.
23. Medhanit E, Mekonnen G, Yalew KN, Umer JY, Melese M. Determinants of delivery practices among Afar pastoralists of Ethiopia. Pan Afr Med J. 2012;13(Supp 1).
24. Abebe FE, Berhane Y, Girma B. Factors associated with home delivery in Bahirdar, Ethiopia: a case control study. BMC Res Notes. 2012;5(1):653. doi:10.1186/1756-0500-5-653
25. Wako G, Kassa H. Institutional delivery service utilization and associated factors among women of reproductive age in the mobile pastoral community of the Liban District in Guji Zone, Oromia, Southern Ethiopia: a cross sectional study. BMC Pregnancy Childbirth. 2017;17(1):144. doi:10.1186/s12884-017-1325-5
26. Kasaye HK, Endale ZM, Desta MS, Desta MS. Home delivery among antenatal care booked women in their last pregnancy and associated factors: community-based cross sectional study in Debremarkos town, North West Ethiopia. BMC Pregnancy Childbirth. 2017;17(1). doi:10.1186/s12884-017-1409-2
27. Teklesilasie W, Deressa W. Husbands’ involvement in antenatal care and its association with women’s utilization of skilled birth attendants in Sidama zone, Ethiopia: a prospective cohort study. BMC Pregnancy Childbirth. 2018;18:315.
28. Suandi D, Williams P, Bhattacharya S. Does involving male partners in antenatal care improve healthcare utilisation? Systematic review and meta-analysis of the published literature from low- and middle-income countries. Int Health. 2019;1–15.
29. Zepro N, Ahmed T. Determinants of institutional delivery service utilization among pastorals of Liben Zone, Somali Regional State, Ethiopia. Int J Womens Health. 2016;8:705–712. doi:10.2147/IJWH.S123189
30. Regassa N, Melaku F. Skilled delivery care service utilization in Ethiopia: analysis of rural-urban differentials based on national demographic and health survey data. Afr Health Sci. 2014;14(4).
31. Habte F, Demissie M. Magnitude and factors associated with institutional delivery service utilization among childbearing mothers in Cheha district, Gurage zone,Ethiopia: a community based cross sectional study. BMC Pregnancy Childbirth. 2016;15(1):299. doi:10.1186/s12884-015-0716-8
32. Hagos S, Shaweno D, Assegid M, Mekonnen A, Afework MF, Ahmed S. Utilization of institutional delivery service at Wukro and Butajera districts in the northern and south central Ethiopia. BMC Pregnancy Childbirth. 2014;14(178):1–11. doi:10.1186/1471-2393-14-178
33. FMOH. Health Sector Transformation Plan 2008–2012 EFY (2015–2020). Addis Ababa, Ethiopia: Federal Ministry of Health; 2015.
34. Umbel T, Kunna A, Salah I, sulman MM. Why women choose to deliver at home in Omdurman, Sudan. J Med Med Sci. 2014;2(8).
35. Wodaynew T, Fekecha B, Abdisa B. Magnitude of home delivery and associated factors among antenatal care booked mothers in Delanta District, South Wollo Zone, North East Ethiopia: a cross-sectional study. Int J Women Health. 2018;4:086.
36. Chernet AG, Dumga KT, Cherie KT. Home delivery practices and associated factors in Ethiopia. J Reprod Infertil. 2019;20(2):102–108.
37. Yilkal M, Mekonnen A, Dejenu G. Prevalence and determinants of home birth after antenatal care attendance in Gozamin District, Northwest Ethiopia. Health Sci J. 2015;9(6).
38. Assefa M, Fite RO, Taye A, Belachew T. Institutional delivery service use and associated factors among women who delivered during the last 2 years in Dallocha town, SNNPR, Ethiopia. Nurs Open. 2020;7(1):186. doi:10.1002/nop2.378
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.