")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Determinants of Drug-Induced Hepatotoxicity Among Patients with Human Immunodeficiency Virus Taking a High Dose of Rifapentine Plus Isoniazid Drugs at the All Africa Leprosy Tuberculosis Rehabilitation and Training Center in Addis Ababa, Ethiopia
Authors Lisanwork Arage L, Deybasso HA , Yilma Gebremichael D, Gintamo Nuramo B, Negash Mekuria Z
Received 8 January 2021
Accepted for publication 26 February 2021
Published 16 March 2021 Volume 2021:13 Pages 307—314
DOI https://doi.org/10.2147/HIV.S300135
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bassel Sawaya
This paper has been retracted.
Leuel Lisanwork Arage, 1 Haji Aman Deybasso, 2 Delelegn Yilma Gebremichael, 3 Binyam Gintamo Nuramo, 4 Zelalem Negash Mekuria 4
1The Ohio State University Global One Health, Addis Ababa, Ethiopia; 2Adama Hospital Medical College, Adama, Ethiopia; 3Ambo University, College of Medicine and Health Sciences, Department of Public Health, Ambo, Ethiopia; 4Addis Ababa Medical and Business College, Department of Research and Community Service, Addis Ababa, Ethiopia
Correspondence: Haji Aman Deybasso Tel +251 911386781
Email [email protected]
Purpose: The drugs for the treatment of latent Tuberculosis are potentially hepatotoxic and can lead to drug-induced hepatotoxicity. The current study aimed at identifying the determinants of anti-tuberculosis drug-induced hepatotoxicity among patients living with Human Immunodeficiency Virus taking Isoniazid and rifapentine at All Africa Leprosy Tuberculosis Rehabilitation and Training Center in Addis Ababa, Ethiopia.
Methods: An unmatched case–control study was conducted from March, 21, to April 21, 2020, at All Africa Leprosy Tuberculosis Rehabilitation and Training Center. A total of 65 cases and 130 controls were interviewed. Data were collected using a data extraction tool from clinical reporting forms, follow-up charts, and patients’ logbooks. Binary and multiple logistic regressions were conducted to check the association between independent and dependent variables. Adjusted odds ratios and the corresponding 95% confidence intervals were estimated to assess the strength of association. P-values < 0.05 were used to declare statistical significance.
Results: The prevalence of anti-TB drug-induced hepatotoxicity was 8%. Body mass index < 18.5 Kg/m2 (AOR = 5.8 [95% CI: 2.2– 8.9]), low CD4 count (AOR = 4.9 [95% CI: 1.6– 15.8]), and the presence of comorbid illnesses (AOR = 3.9 [95% CI: 1.7– 8.9]) were identified as independent predictors of drugs-induced hepatotoxicity among Human Immunodeficiency Virus positive patients taking Isoniazid and rifapentine.
Conclusion: The prevalence of anti-TB drug-induced hepatotoxicity was higher compared to standard references. BMI< 18 kg/m2, low CD4 count, and comorbid illness were positively associated with anti-tuberculosis drug-induced hepatotoxicity among patients with HIV.
Keywords: isoniazid and rifapentine, TPT, hepatotoxicity, HIV patients, Ethiopia
Introduction
Tuberculosis (TB) is a chronic infection of a global health concern due to the burden of high incidence, medical expenses, drug resistance, and co-infections.1 The World Health Organization (WHO) in 2018 estimated that worldwide, around 10 million people still fall ill with the disease each year and there were 1.5 million TB deaths.2 Latent tuberculosis infection (LTBI) is defined as a state of the persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifest active TB.3,4 Nearly one-third of the world’s population is estimated to be infected with M. tuberculosis and once infected, the individual is at the highest risk of developing TB disease within the first two years but can remain at risk for their lifetime.5 The risk of developing TB is between 20 and 37 times greater in people living with HIV than among those who do not have HIV infection.6
TB preventive therapy (TPT) entails using one or more Anti-tuberculous drug to treat persons with latent TB infection who are at high risk of progressing to TB disease.7 Prevention of active TB disease by treatment of LTBI is a critical component of the WHO End TB Strategy,5 and TPT has been demonstrated to prevent TB disease among persons who might be infected with TB and are at risk for TB disease.8 Accordingly,; WHO recommends at least six months of isoniazid (6H) for persons living with HIV.2
The World Health Organization currently recommends the following regimens as options for LTBI treatment: 6 months of daily Isoniazid (INH) (6H), 9 months of daily INH (9H), INH and rifapentine once weekly for 12 weeks (3HP), 3–4 months daily INH plus rifampin (INH/RFMP 3–4), and 3–4 months daily rifampin alone (RFMP 3–4 months).5
Hepatotoxicity is one of the most important adverse drug reactions associated with these drugs during the treatment of LTB that may limit their use and is also one of the most prevalent drug-induced liver injuries (DILI) or also known as drug-induced hepatotoxicity.9,10 In medical practice and about 9% of patients taking first-line ant-TB drugs to develop major adverse drug effects.11
A previous study indicated that 5.1% of patients living with HIV had reactions to Anti-tuberculosis drugs requiring modification of treatment.12 Drug-induced hepatotoxicity may occur with all currently recommended regimens for the treatment of LTBI13 and is the commonest of all adverse effects leading to drug discontinuation in 11% of patients treated with isoniazid alone or in combination with rifapentine.14
Various studies have suggested that a high alcohol intake, older age, slow acetylation status, pre-existing chronic liver disease, chronic viral infection due to hepatitis B and hepatitis C, HIV infection, advanced tuberculosis, Asian ethnicity, female sex, concomitant administration of enzyme-inducers (eg barbiturates and anesthetic agents), inappropriate use of drugs and poor nutritional status increase the risk of anti-tuberculosis drug-induced hepatitis.15–18
To the best of our knowledge, there is no study on DIH in Ethiopia as the 3HP regimen is recently being implemented in the county’s health system. The current study aimed at identifying the determinants of anti-tuberculosis drug-induced hepatotoxicity among patients living with HIV taking Isoniazid and rifapentine at ALERT Hospital in Addis Ababa, Ethiopia. The findings will contribute to bridging the information gap and subsequently serves as evidence to improve local TB control through improving LTBI treatment.
Patients and Methods
Setting
ALERT hospital is one of the referral hospitals in Addis Ababa town under the administration of the Federal Ministry of health. The Hospital currently has 6400 patients living with HIV out of which a cohort of 870 HIV infected patients commenced a high dose Rifapentine plus Isoniazid anti-TB preventive drug as a single round or given annually at ALERT hospital.
The study was conducted in the ALERT Hospital from March, 21, to April 21, 2020.
Study Design
An unmatched case–control study of patients living with HIV was conducted to identify the determinants of Isoniazid and rifapentine-induced hepatotoxicity.
Study Population
The study populations were patients living with HIV treated for the full duration of latent TB treatment with regular follow-up at the ART clinic by the physician, nurse, and pharmacist at baseline and throughout their treatment.
Sample Size Determination
The sample was calculated using Stat-Calc using the determinants of hepatotoxicity from a previous study done in Ethiopia.19 With a power of 90%, a confidence level of 95%, a 1:2 ratio of cases to controls, the sample size was 195 (65 cases and 130 controls).
Sampling Procedure
Cases were patients living with HIV who were diagnosed with drug-induced hepatotoxicity after four days of a standard dose of TPT during the course. Controls were patients treated for the full duration of latent TB treatment with regular follow-up at the ART clinic of the hospital taking the same regimen but without clinical or biochemical evidence of hepatotoxicity. From a compiled list of 870 patients living with HIV who commenced three months of high dose Rifapentine plus Isoniazid during the study period, 65 patients fulfilled the criteria of having hepatotoxicity, ie cases. From the remaining 805 patients, 130 controls were selected using simple random sampling. Each case was matched with randomly selected two controls.
Inclusion and Exclusion Criteria
The inclusion criteria for cases were being on ART for at least three months, diagnosed to have DIH after at least four days of a standard dose of 3HP regimen, age above 18 years. The criteria for controls were similar to the cases except that controls did not develop DIH throughout the course.
The exclusion criteria were patients who on a different regimen other than 3HP, patients’ elevated liver enzymes caused by other causes of liver injury (ie Other than TPT), presumptive or confirmed TB disease, and the participant with incomplete data.
Data Collection Procedures and Measurements
Data were collected by trained BSc Nurses. Data were collected using a data extraction tool from clinical reporting forms, follow-up charts, and patients’ logbooks. The collected information comprises age, sex, weight, height, CD4 count, associated medical conditions, other medications, baseline aspartate aminotransferase (AST) and alanine aminotransferase (ALT), peak AST, peak ALT, peak bilirubin, the onset of side effects or hepatotoxicity, presence or absence of symptoms associated with hepatotoxicity, the latency period between the start of treatment and development of DILI, resolution status, hospitalization, and treatment completion status. Diagnostic criteria for hepatotoxicity were taken to be the presence of one or more of the following biochemical criteria and clinical judgment abnormalities between four and 90 days after the start of the standardized anti-TB drugs excluding other possible causes.10,20–23
(1) A rise of serum AST and/or ALT to three times of the normal upper limit (2) a rise in the level of serum total bilirubin >1.5 mg/DL; (3) Any increase in AST and/or ALT compared to pre-treatment levels accompanied by anorexia, nausea, vomiting, and jaundice; (4) absence of serologic evidence of infection with hepatitis viruses.
Operational Definitions
Upper limit normal values (for both ALT and AST) of liver enzymes: 29 to 33μ/l for males, 19 to 25μ/l for females, and 1mg/dl for total bilirubin.22
Anti-TB DIH: a clinical diagnosis of exclusion fulfilling the above diagnostic criteria.13
CD4 count: the most recent (within the last 6 months) CD4 count documented in the participant’s medical record with two levels (below and above 200 cells/µL).
BMI: the body mass index of a participant measured at the enrollment visit with two levels (below and above 18.5 kg/m2).
Comorbidity: The presence of more than one distinct health condition in an individual.23
Mild hepatotoxicity: elevation of ALT/AST less than 3 times ULN. Moderate hepatotoxicity: elevation of ALT/AST less than 3 to 5 times ULN. Severe hepatotoxicity: elevation of ALT/AST less than 5 to 10 times ULN. Very severe hepatotoxicity (potentially life-threatening): elevation of ALT/AST above 10 times ULN or elevations more than 250 IU/L with symptoms of fulminant hepatitis as evidenced by jaundice and/or lethargy.24
Quality Assurance
Data collectors and supervisors were trained on how to fill in the information according to the prepared tool to make sure that the data collectors and supervisors understood the detailed elements of the tool. Throughout the data collection, there was strict supervision of data quality. The data were retrieved by reviewing records from clinical reporting forms, follow-up charts, and patients’ logbooks by using a data extraction form. The extraction form pretested using similar patients’ medical record and improvement made on question format, order, skip patterns and categories in response list.
Data Management and Analysis
Data were coded and entered into the EPI info version7, and transported to SPSS software version 24. Categorical variables were presented in frequencies and percentages, whereas numerical variables were expressed in descriptive statistics. Binary and multiple logistic regressions were conducted to check the association between independent and dependent variables. Multicollinearity was checked at ≥5 variance inflation factor (VIF). Adjusted odds ratios and the corresponding 95% confidence intervals were estimated to assess the strength of association. P-values <0.05 were used to declare statistical significance.
Results
Prevalence of Anti-TB Drug-Induced Hepatotoxicity
In the study population, the prevalence of anti-TB drug-induced hepatotoxicity was 8%. The onset of hepatotoxicity ranged from 15 days to 78 days (median, 28 days) after treatment was initiated. The majority of 35 (53.9.0%) of the cases occurred during the first 28 days while most of the cases 54 (83.1%) occurred during the first 42 days.
Socio-Demographic and Clinical Characteristics of the Study Participants
A total of 195 participants, 65 cases, and 130 controls were included in this study. The mean (±SD) age of cases was 46.81 (±10.20) and that of controls was 46.96 (±8.56) years [P=0.946]. On the other hand, 39 (60.0%) cases, and 77 (59.2%) controls were females. All study participants were on ART before LTBI treatment and the mean (±SD) duration was 7.95 [±3.74] and 7.92 [±3.26] years for cases and controls, respectively, when the anti-TB drug was started. Study participants took two different types of ART regimens; the majority (75.9%) were on Tenofovir (TDF), Lamivudine (3TC), and Efavirenz (EFV). Two-third of cases 44 (67.7%) and 63 (48.5%) of controls were on cotrimoxazole prophylaxis. Besides, 26 (40.0%) of cases and 23 (17.7%) of controls had CD4 count less than 350 cells/μL. Seventeen (26.2%) of cases and 11 (8.4%) of controls were found to have co-morbid illnesses where Diabetes Mellitus and Hypertension being the commonest. In addition, 27 (41.5%) of cases and 18 (13.8%) of controls had a body mass index (BMI) <18.5 Kg/m2 (Table 1).
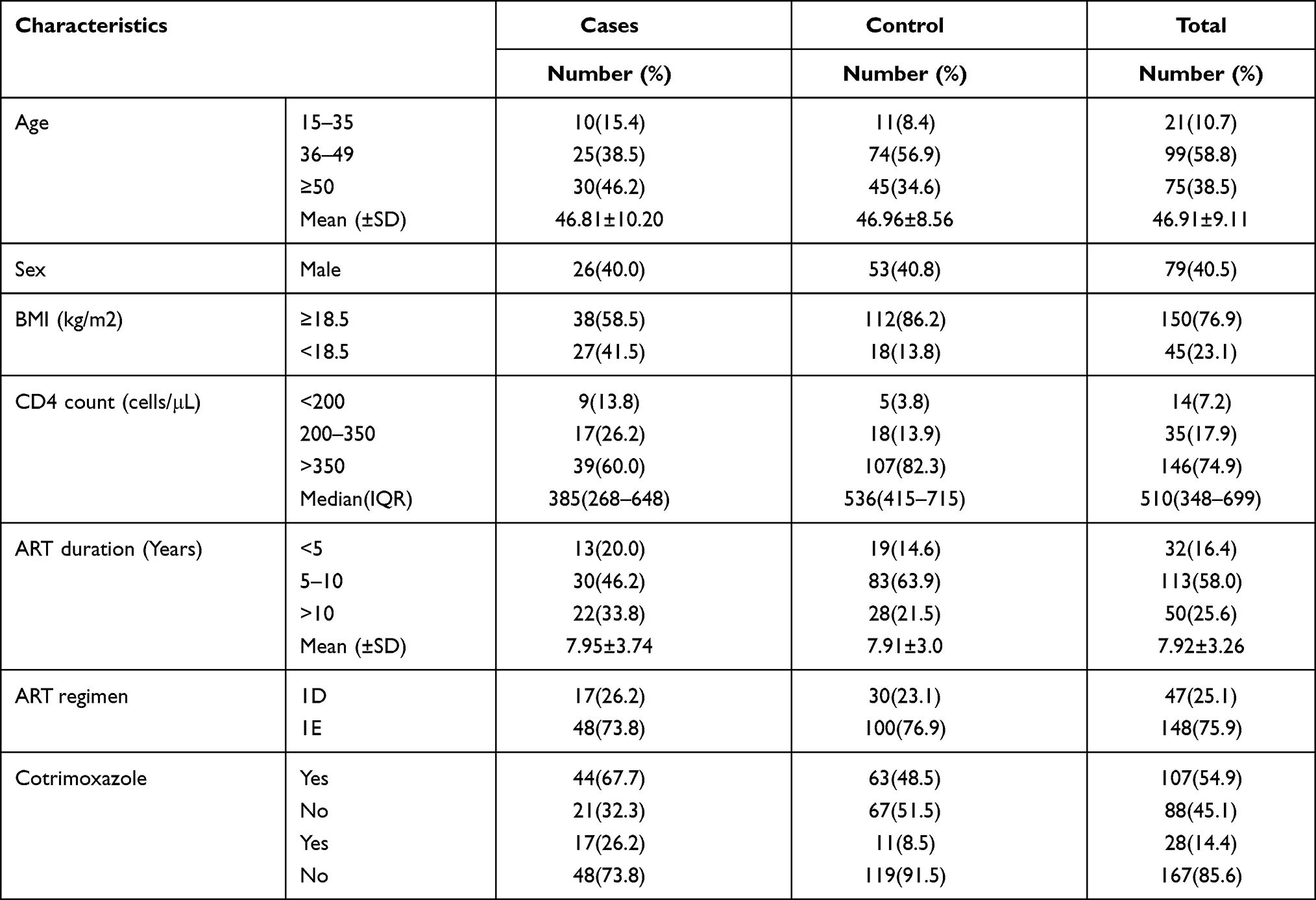 |
Table 1 Socio-Demographic and Clinical Characteristics of HIV Patients in ALERT Hospital, Addis Ababa, Ethiopia, 2020 |
Changes in Liver Function Tests of the Participants
AST and ALT in patients with anti-TB drug-induced hepatotoxicity ranged from 36 to 587 IU/L [mean of 184±111.37] and 83 to 711 IU/L [mean of 187±105.12], respectively. The mean Total Bilirubin in cases and controls was 0.96±0.61 and 0.34±0.23, respectively (Table 2).
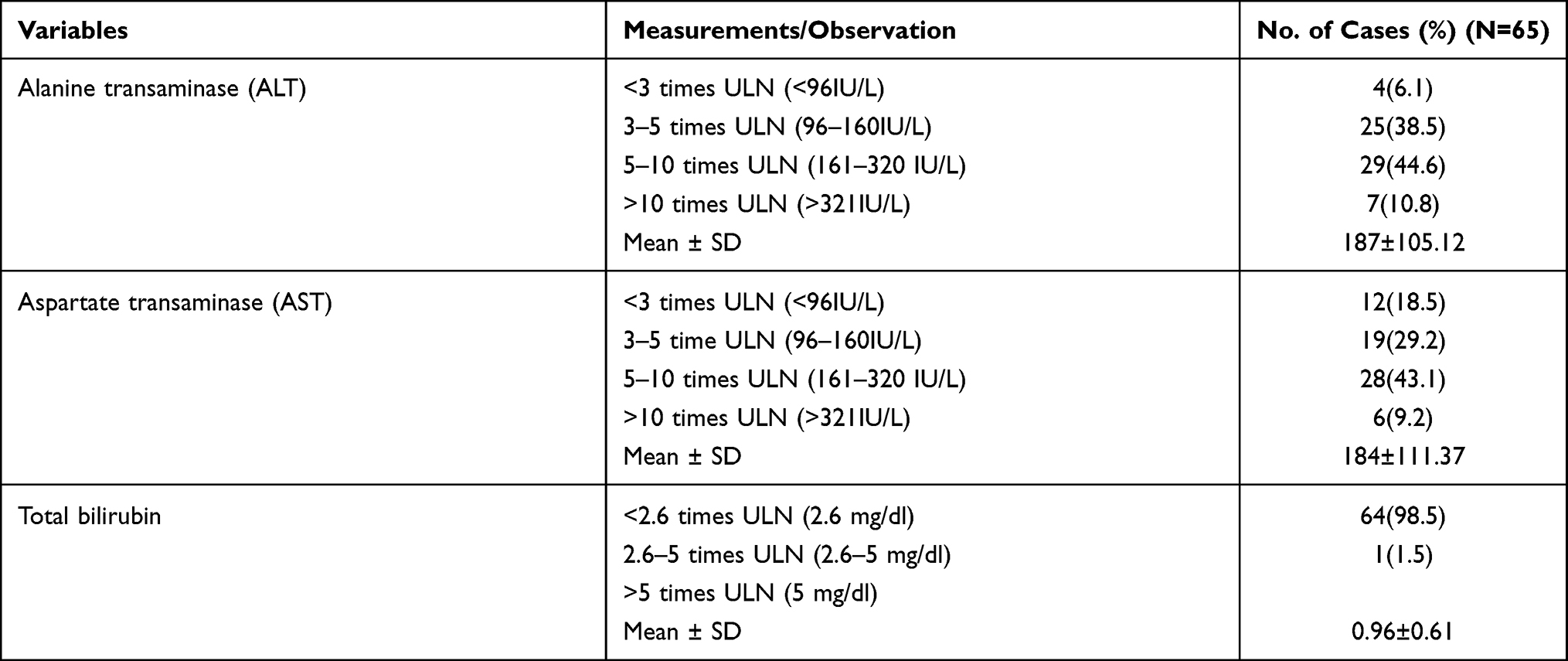 |
Table 2 Changes in Liver Function Tests of HIV Infected Patients Who Developed Anti-TB Drugs-Induced Hepatotoxicity |
The Severity of Anti-TB Drug-Induced Hepatotoxicity
Among 65 total cases, 37 (56.9%) of them were moderate hepatotoxicity, 24 (36.9%) of them were severe hepatotoxicity, whereas the remaining 4 (6.2%) were very severe (potentially life-threatening) hepatotoxicity cases (Table 3).
 |
Table 3 Degree of Severity of Anti-TB Drug-Induced Hepatotoxicity, According to the US National Institute of Allergy and Infectious Diseases, Division of AIDS Classification of Drug Toxicity |
Factors Associated with Anti-TB Drug-Induced Hepatotoxicity
BMI < 18.5 kg/m2 (COR = 4.5 [95% CI 2.2–8.9]), lower CD4 count (<200 mm3) (COR = 4.9 [95% CI 1.6–15.8]) and below 350 mm3 (COR = 2.6 [95% CI 1.2–5.6]), CPT prophylaxis (COR = 2.2 [95% CI 1.2–4.1]) and presence of comorbidity (COR = 3.9 [95% CI 1.7–8.9]) were significantly associated with anti-TB DIH from bivariate model analysis.
In multivariable analysis, body mass index (BMI) <18.55 kg/m2 (AOR = 5.8 [95% CI 2.6–12.8]), lower CD4 count (<200 mm3) (AOR = 4 [95% CI 1.1–15.4]) and below 350 mm3 (AOR = 4.4 [95% CI 1.8–10.7]) as well as presence of comorbidity (AOR = 5.2 [95% CI 2.1–12.8]) were identified as independent predictors of Anti-TB drug-induced hepatotoxicity (Table 4).
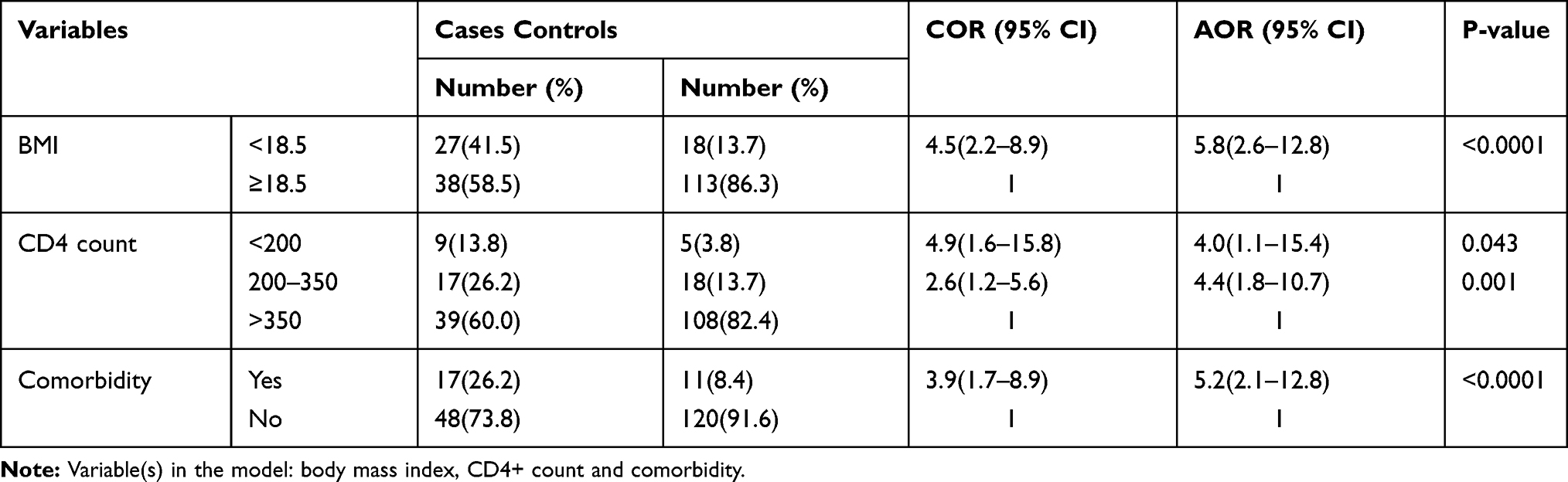 |
Table 4 Multivariate Regression Analysis of Factors Associated with (Predictive Factors of) Anti-TB DIH Among HIV Patients in ALERT Hospital, Addis Ababa, Ethiopia, 2020 |
Discussion
In the present study, the prevalence of anti-TB drugs-induced hepatotoxicity among TB/HIV co-infected patients was 8%. The finding is comparable with results reported by Wondwossen A. et al (8%) in Ethiopia,25 Rajani S et al (8%) from Nepal,26 and Alsina N et al (8.8%) from Brazil.27 However, this prevalence is lower than other studies in Ethiopia (20.2%),28 and (11%),11 as well in Brazil (36.7%),29 and higher than that of the western world (4.3%).31 The variation in the prevalence of anti-TB-DIH worldwide may be attributed to the differences in patients’ characteristics, indiscriminate use of drugs, and the definition criteria of hepatotoxicity as different countries use their guidelines.27
In this study, patients whose BMI<18.5 kg/m2 were more likely to develop hepatotoxicity compared to patients who had BMI ≥18.5, a finding which is consistent with others.17,28,30 The possible explanation of anti-TB drugs-induced hepatotoxicity in malnutrition may be due to depletion of glutathione stores, which makes patients more vulnerable to oxidative injuries, and the slower pace at which the liver metabolizes drugs.26,31
In a previous study conducted in Ethiopian HIV positive and negative TB patients, the development of anti-TB drugs-induced hepatotoxicity had a significant association with a decrement in the immune status of the patients as measured by the CD4 count32 Similarly, this study revealed a statistically significant association between low CD4 counts and the development of hepatotoxicity among the participants with decreased immune status. This phenomenon was not shown in previous studies and may suggest the presence of an immunologic mechanism for the development of anti-TB DIH although the exact mechanism has not yet been elucidated.33 The other possible explanation for this could be since patients with low CD4 count are more prone to acquiring opportunistic infections, this might necessitate the consumption of different drugs, leading to subclinical liver damage and thereby increase susceptibility for hepatotoxicity while taking anti TB.32,34
This study also showed that the presence of comorbid illness (such as diabetes mellitus, hypertension, and anemia) was positively associated with increased risk for anti-TB-DIH. Limited information is available regarding this association, but a prior investigation reported that drug toxicity might result in these patients due to abnormal drug metabolism, which could increase the possibility of adverse events and fatty liver disease.35
It has been reported that advanced age can be a risk factor for anti-TB drug-induced hepatotoxicity,10,14 in the present study, however, no association was found between age of the participants and the risk of developing anti-TB drugs-induced hepatotoxicity similar to previous studies.17,28,30,32
Strengths and Limitations
The major strength of this study is that it is the first study that identified the determinants of drug-induced hepatotoxicity among patients living with HIV on new regimens for the prevention of tuberculosis.
This study had some limitations. The study was conducted in a single hospital; therefore, a generalization of the finding must be made with caution. Secondly, since the data is based on secondary data the reliability of the data relies on the information on the patient card. Thirdly, as the study design is a case–control, it cannot yield population-level incidence. Fourthly, the present study has limitations inherent in retrospective case–control analysis, such as the inability to directly compute the risk. It is the suggestion of the present study to carry out a multi-center population-based prospective cohort study of anti-TB drugs-induced hepatotoxicity to provide data on the incidence, clinical features, and its impact on TB treatment.
Conclusions
The prevalence of anti-TB drug-induced hepatotoxicity was higher compared to the incidence in standard references like America Thoracic Society, 1–4%. BMI<18 kg/m2, low CD4 count, and comorbid illness were the independent predictors of anti-tuberculosis drug-induced hepatotoxicity among HIV-positive patients. We recommend to health care providers that patients with HIV having lower BMI, low CD4 count and comorbid illness should be identified by clinicians so as to closely monitor their liver enzyme levels during the first few weeks of LTB treatment for greater quality of care.
Abbreviations
ALT, alanine aminotransferase; ART, antiretroviral therapy; AST, aspartate aminotransferase; BMI, body mass index; DIH, drug-induced hepatotoxicity; DILI, drug-induced liver injuries; HIV, human Immune deficiency virus; INH, isoniazid; LTBI, latent tuberculosis infection; REFMP, Rifampin; TB, tuberculosis; TPT, TB preventive therapy; VIF, variance inflation factor; WHO, World Health Organization.
Data Sharing Statement
The datasets supporting the conclusions of this article are included in the article.
Ethical Consideration
This study was conducted in accordance with the Declaration of Helsinki. As the study was conducted through reviewing of patients’ medical records, informed consents were waived through the permission from ALERT hospital. Approval for conducting the study was obtained from the institutional review board of, Addis Ababa Medical, and Business College as well as. The confidentiality of the data was maintained by avoiding personal identifiers on the data extraction form. The recorded data was not accessed by a third person, except the principal investigator, and confidentiality was ensured.
Acknowledgments
The authors would like to thank Addis Ababa Medical and Business College, Dr. Getnet Yimer, Kaitlyn Humphrey, and also ALERT hospital team for their kindly cooperation during conducting this study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There was no funding for this work.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Mao Q, Zhang K, Yan W, Cheng C. Forecasting the incidence of tuberculosis in China using the seasonal auto-regressive integrated moving average (SARIMA) model. J Infect Public Health. 2018;11(5):707–712. doi:10.1016/j.jiph.2018.04.009
2. World Health Organization. Global Tuberculosis Report 2019. Geneva: World health organization; 2019.
3. Getahun H, Matteelli A, Chaisson R, Raviglione M. Latent Mycobacterium tuberculosis Infection. N Engl J Med. 2015;372(22):2127–2135. doi:10.1056/NEJMra1405427
4. Truer J, Moyo N, Tay E, et al. Risk of Active Tuberculosis in the Five Years Following Infection [Internet]. Chest Chest. 2016;149(2):516.
5. World Health Organization. Latent TB Infection: updated and consolidated guidelines for programmatic management [Internet]. WHO; [cited Dec 2, 2020]. Available from: http://www.who.int/tb/publications/2018/latent-tuberculosis-infection/en/.
6. Churchyard GJ, Swindells S. Controlling latent TB tuberculosis infection in high-burden countries: a neglected strategy to end TB. PLoS Med. 2019;16(4):e1002787. doi:10.1371/journal.pmed.1002787
7. World Health Organization. Guidelines for intensified tuberculosis case-finding and isoniazid preventative therapy for people living with HIV in resource-constrained settings [Internet]. Geneva, Switzerland: Department of HIV/AIDS: Stop TB Department, World Health Organization; 2011 [
8. Badji A, Moh R, Gabillard D, et al. Effect of isoniazid preventive therapy on risk of death in west African, HIV-infected adults with high CD4 cell counts: long-term follow-up of the Temprano ANRS 12136 trial [Internet]. Lancet. 2017;5(11):1080.
9. Yu Y, Tsao S, Yang W, et al. Association of drug metabolic enzyme genetic polymorphisms and adverse drug reactions in patients receiving rifapentine and isoniazid therapy for latent tuberculosis [Internet]. Vol. 17, International journal of environmental research and public health. Int J Environ Res Public Health. 2019;17(1):210. doi:10.3390/ijerph17010210
10. Bliven-Sizemore E, Sterling T, Shang N, et al. Three months of weekly rifapentine plus isoniazid is less hepatotoxic than nine months of daily isoniazid for LTBI [Internet]. Vol. 19, The international journal of tuberculosis and lung disease: the official journal of the International Union against Tuberculosis and Lung Disease. Int J Tuberc Lung Dis. 2015;19(9):
11. Guidelines for the clinical and operational management of drug-resistant tuberculosis | the union [Internet]. [cited Dec 2, 2020]. Available from: https://theunion.org/technical-publications/guidelines-for-the-clinical-and-operational-management-of-drug-resistant-tuberculosis.
12. Ormerod L, Horsfield N. Frequency and type of reactions to antituberculosis drugs: observations in routine treatment [Internet]. Vol. 77, Tubercle and lung disease: the official journal of the International Union against Tuberculosis and Lung Disease. Tuber Lung Dis. 1996;77(1):37–42. doi:10.1016/S0962-8479(96)90073-8
13. Saukkonen J, Cohn D, Jasmer R, et al. An official ATS statement: hepatotoxicity of antituberculosis therapy. Am J Respir Crit Care Med. 2006;174(8):935.
14. Schaberg T, Rebhan K, Lode H. Risk factors for side-effects of isoniazid, rifampin and pyrazinamide in patients hospitalized for pulmonary tuberculosis. Eur Respir J. 1996;9(10):2026.
15. Huang Y, Chern H, Su W, et al. Cytochrome P450 2E1 genotype and the susceptibility to antituberculosis drug-induced hepatitis [Internet]. Vol. 37, Hepatology (Baltimore, Md.). Hepatology. 2003;37(4):924–930. doi:10.1053/jhep.2003.50144
16. Sharma SK, Balamurugan A, Saha PK, Pandey RM, Mehra NK. Evaluation of Clinical and Immunogenetic Risk Factors for the Development of Hepatotoxicity during Antituberculosis Treatment. Am J Respir Crit Care Med. 2002;166(7):916–919. doi:10.1164/rccm.2108091
17. Hassen A, Belachew T, Yami A, Ayen W. Anti-tuberculosis drug induced hepatotoxicity among TB/HIV co-infected patients at Jimma University Hospital, Ethiopia: nested case-control study. PLoS One. 2013;8(5):e64622.
18. Ungo J, Jones D, Ashkin D, et al. Antituberculosis drug-induced hepatotoxicity. The role of hepatitis C virus and the human immunodeficiency virus. Am J Respir Crit Care Med. 1998;157(6 Pt 1):1871–1876. doi:10.1164/ajrccm.157.6.9711039
19. Devarbbavi H. Antituberculous drug-induced liver injury: current perspective. Trop Gastroenterol off J Dig Dis Found. 2011;32(3):167–174.
20. Babalik A, Arda H, Bakirci N, et al. Management of and risk factors related to hepatotoxicity during tuberculosis treatment. Tuberk Ve Toraks. 2012;60(2):136–144.
21. Gaude GS, Chaudhury A, Hattiholi J. Drug-induced hepatitis and the risk factors for liver injury in pulmonary tuberculosis patients. J Fam Med Prim Care. 2015;4(2):238. doi:10.4103/2249-4863.154661
22. Kwo PY, Cohen SM, Lim JK. ACG clinical guideline: evaluation of abnormal liver chemistries. Off J Am Coll Gastroenterol ACG. 2017;112(1):18–35. doi:10.1038/ajg.2016.517
23. Valderas JM, Starfield B, Sibbald B, Salisbury C, Roland M. Defining comorbidity: implications for understanding health and health services. Ann Fam Med. 2009;7(4):357–363. doi:10.1370/afm.983
24. National Institutes of Health. Division of AIDS (DAIDS) Table for grading the severity of adult and pediatric adverse events. 2017. Corrected Version 2.1: 35.
25. Abera W, Cheneke W, Abebe G. Incidence of antituberculosis-drug-induced hepatotoxicity and associated risk factors among tuberculosis patients in Dawro Zone, South Ethiopia: a cohort study. Int J Mycobacteriology. 2016;5(1):14–20. doi:10.1016/j.ijmyco.2015.10.002
26. Shaky R, Shrestha B. Evaluation of Risk Factors for Antituberculosis-drug-induced hepatotoxicity in Nepalese Population. Kathmandu Univ J Sci Eng Tech. 2006;1(2):353.
27. Alsina Nader L, Alves de Mattos A, Dornelles Picon P, Luis Bassanesi S, Zambam De Mattos A, Pineiro Rodriguez M. Hepatotoxicity due to rifampicin, isoniazid and pyrazinamide in patients with tuberculosis: is anti-HCV a risk factor? Ann Hepatol. 2010;9(1):70–74. doi:10.1016/S1665-2681(19)31682-5
28. Zeleke A, Misiker B, Yesuf TA. Drug-induced hepatotoxicity among TB/HIV co-infected patients in a referral hospital, Ethiopia. BMC Res Notes. 2020;13(1):2. doi:10.1186/s13104-019-4872-1
29. Steele M, Burk R. DesPrez Rm. Toxic hepatitis with isoniazid and rifampin. A meta-analysis. Chest. 1991;99(2):465–471.
30. Assob JC, Nde PF, Nsagha DS, Njunda AL, Ngum NM, Ngowe MN. Incidence and risk factors of anti-tuberculosis drugs induced hepatotoxicity in HIV/AIDS patients attending the limbe and buea regional hospitals. J AIDS Clin Res. 2014;5(3):6.
31. Walter-Sack I, Klotz U. Influence of diet and nutritional status on drug metabolism. Clin Pharmacokinet. 1996;31(1):47–64.
32. Yimer G, Aderaye G, Amogne W, et al. Anti-tuberculosis therapy-induced hepatotoxicity among ethiopian HIV-positive and negative patients. Myer L, editor. PLoS One. 2008;3(3):e1809. doi:10.1371/journal.pone.0001809
33. Pol S, Lebray P, Vallet-Pichard A. HIV infection and hepatic enzyme abnormalities: intricacies of the pathogenic mechanisms. Clin Infect Dis off Publ Infect Dis Soc Am. 2004;38(Supplement_2):S65.
34. Pukenyte E, Lescure F, Rey D, et al. Incidence of and risk factors for severe liver toxicity in HIV-infected patients on anti-tuberculosis treatment. Int J Tuberc Lung Dis off J Int Union Tuberc Lung Dis. 2007;11(1):78–84.
35. Chung-Delgado K, Revilla-Montag A, Guillen-Bravo S, et al. Factors associated with anti-tuberculosis medication adverse effects: a case-control study in lima, Peru. Pai M, editor. PLoS One. 2011;6(11):e27610. doi:10.1371/journal.pone.0027610
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.