")
Back to Journals » Nutrition and Dietary Supplements » Volume 12
Determinants of Acute Malnutrition Among Children Aged 6–59 Months Visiting Public Health Facilities in Gambella Town, Southwest Ethiopia: Unmatched Case–Control Study
Received 29 March 2020
Accepted for publication 31 July 2020
Published 17 August 2020 Volume 2020:12 Pages 147—156
DOI https://doi.org/10.2147/NDS.S256000
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chandrika J Piyathilake
Gatjiek Tut Wie, Dereje Tsegaye
Department of Public Health, Faculty of Public Health and Medical Sciences, Mettu University, Ethiopia
Correspondence: Dereje Tsegaye
Department of Public Health, Faculty of Public Health and Medical Sciences, Mettu University, Ethiopia
Email [email protected]
Background: Malnutrition is one of the main health problems facing children under five years of age in developing countries. Undernutrition imposes significant costs on the Ethiopian economy as well as impacting the well-being of the society. The aim of this study was to assess determinants of acute malnutrition among children aged 6– 59 months attending public health facilities in Gambella Town, Southwest Ethiopia, 2019.
Methods: An institution-based unmatched case–control study was conducted among children aged 6– 59 months with and without acute malnutrition visiting public health facilities in Gambella town from June 7 to July 21, 2019. Data were collected using an interviewer-administered structured questionnaire and anthropometric measurement was done by standardized calibrated instruments. The collected data were entered onto EpiData™ version 3.1 and then exported to SPSS version 20 for analysis. Both bivariate and multivariable logistic regression analyses were used to identify determinants of acute malnutrition. Statistical significance was declared at P-value of < 0.05.
Results: A total of 342 children (114 cases and 228 controls) with mother/care giver pair were interviewed making the response rate 100%. Maternal education (AOR=2.55, 95%CI: 1.02– 6.37), birth order of the child (AOR=3.65, 95%CI: 1.21– 11.03), number of under-five children in the family (AOR=3.40, 95%CI: 1.03– 11.22), immunization status (AOR=4.60, 95%CI: 1.51– 13.99), IYCF counseling (AOR=6.02, 95%CI: 2.91– 12.46), time of initiation of breastfeeding after birth (AOR=2.43, 95%CI: 1.14– 5.17), and diarrhea in the last two weeks preceding the survey (AOR=2.74, 95%CI: 1.32– 5.68) were significantly associated with acute malnutrition among children aged 6– 59 months.
Conclusion: This study identified the basic, underlying, and immediate determinants of acute malnutrition among children aged 6– 59 months. Multisectoral collaboration to improve women’s education, IYCF counseling, environmental sanitation, vaccination completion, and prompt seeking of diarrhea treatment to reduce acute malnutrition is required.
Keywords: acute malnutrition, children aged 6– 59 months, case–control study
Background
Malnutrition is a universal problem holding back development with unacceptable human consequences. It affects all geographies, all age groups, rich people and poor people, and all sexes.1 Malnutrition is broad term commonly used as an alternative to “undernutrition” but which technically refers to any dysfunction of nutrition, including inadequate, excessive or unbalanced nutrition. Undernutrition covers a range of disorders including growth failure and micronutrient deficiencies.2
Acute malnutrition is a recent and severe weight loss (wasting) as a result of acute food shortage and/or illness and is measured by weight for height or mid upper arm circumference (MUAC).3 Wasting is usually is a consequence of insufficient food intake or a high incidence of infectious diseases, especially diarrhea. Wasting in turn impairs the functioning of the immune system. It can lead to increased severity, duration, and susceptibility to infectious diseases and an increased risk of death. It is considered the best indicator of acute malnutrition and a strong predictor of mortality among children under five years of age.1,4,5
Childhood malnutrition is a major health problem contributing to child morbidity, mortality, impaired intellectual development, suboptimal adult work capacity and increased risk of diseases in adults.6–8 Malnourished children have lower resistance to infection and are more likely to die from common childhood ailments such as diarrheal diseases and respiratory infections. In addition to this, malnourished children that survive are likely to suffer from frequent illness, which adversely affects their nutritional status. These lock them into a vicious cycle of recurring sickness, faltering growth and diminished learning ability.2,7
Acute malnutrition is not only a condition that kills,but also has long-term health and developmental consequences, which include an increased risk of stunted growth, impaired cognitive development and a greater chance of developing noncommunicable diseases in adulthood.8,9 For current and succeeding generations, good nutrition is the cornerstone for survival, health and development.2 Better nutritional status of children reflects a healthy and a productive generation in the future. When the population is well nourished the results are higher individual productivity, lower health-care costs and greater economic output2,10 Suboptimum breastfeeding, especially nonexclusive breastfeeding in the first six months of life results in 1.4 million deaths and 10% of disease burden in children younger than five years.8
Malnutrition affects every country and its rates remain alarming. In 2017, nearly 51 million children under five were wasted and 16 million were severely wasted globally. Africa and Asia bear the greatest share of all forms of malnutrition. Asia is home to the majority of children under five suffering from wasting and severe wasting. In 2017, more than two thirds (69%) of all wasted children under five lived in Asia that is more than half of all wasted children in the world lived in Southern Asia, while more than one quarter (27%) lived in Africa. Wasting in children is life-threatening. In Asia and Oceania, wasting is putting nearly one in ten children under five at increased risk of death.11
Ethiopia is one of the poorest among the developing countries. It has one of the highest undernutrition rates within Sub-Saharan Africa. According to the Ethiopian Demographic and Health Survey (EDHS), the trend of stunting and being underweight decreased over a 16-year period (2000–2016) from 58% to 38% for stunting and 41% to 24% for being underweight, but wasting changed little over the same period.12 There is variation in prevalence of all forms of malnutrition and their determinants across regions, localities and place of residence in Ethiopia. Gambella region where the study was conducted has a wasting and severe wasting rate of 14.1% and 3.4%, respectively which slightly exceeds the national severe wasting rate of 3%.12
As acute malnutrition (wasting) remains among the top causes of morbidity and mortality among children under five years of age, it is indicated that it is still a serious public health problem that requires attention. Development of effective policies and programs to alleviate acute malnutrition require an understanding of its determinants. A few studies were conducted in different parts of Ethiopia but limited to address a few of the determinants. In addition to this, those studies are not specific to this study area. It is necessary to channel research projects toward identifying the determinants of acute malnutrition (wasting) in various areas across the country to promote and strengthen effective prevention strategy to reduce wasting prevalence so that it will no longer be a public health threat. Therefore, this study was conducted to identify determinants of acute malnutrition (wasting) among children aged 6–59 months attending public health facilities in Gambella town so that Gambella Regional Health Bureau (GRHB), UNICEF and partners working on prevention and treatment of acute malnutrition in the region will use it to improve effectiveness and efficiency of their intervention strategies.
Methods
Study Setting and Design
This institution based unmatched case–control study was conducted in two public health facilities of Gambella town, the capital of Gambella National Regional State. Gambella town is located at a distance of 766 km from the center to Southwest direction. Gambella town comprises of five administrative kebeles and only two public health facilities providing community based management of acute malnutrition (CMAM). According to 2011 Ethiopian Fiscal year (EFY) population projection, the town has a total population of 59,462 (30,326 females and 29,136 males) and 12,927 households. The total population of children below five years of age are 8473 and 95% (8027) are children 6–59 months of age. This study was conducted in Gambella town health center and Gambella hospital from June 7- July 21, 2019.
Study Population
All children aged 6–59 months with mother/care giver pair who attended public health facilities in Gambella town for different health-care services during the study period were the study population. The study has two groups of participants (cases and controls). Cases were all selected children aged 6–59 months with acute malnutrition (weight-for-height z-score <–2 SD or <80% median of the WHO child growth standard or a MUAC <120 mm). Controls were all selected children aged 6– 59 months without acute malnutrition (weight-for-height z-score ≥−2 SD or ≥80% median of the WHO child growth standard or a MUAC ≥120 mm).
Inclusion and Exclusion Criteria
Children aged 6–59 months with and without acute malnutrition were included. Children aged 6–59 months with acute malnutrition and known chronic illnesses like TB, HIV, renal disease, cardiac diseases and congenital abnormalities were excluded. In addition, a child who has edema or was seriously ill or lived in Gambella town for less than six months was excluded.
Sample Size Determination and Sampling Procedures
Sample size was calculated using Epi InfoTM version 7 for window-Stat Calc for calculating sample size for unmatched case–control study by assuming proportion of febrile illness preceding two weeks before developing SAM was used to obtain a minimum sample size of 312 (104 cases and 208 controls), 95% confidence level, 80% power and control to case ratio of two. Considering the nonresponse rate of 10%, the total sample size was 342 (114 cases and 228 controls). The sample was allocated to the two public health facilities proportional to their acutely malnourished children reported.
Since the numbers of acute malnourished children seen per month in each of the two public health facilities were less than the sample allocated to it, all acutely malnourished children were included in the study except those excluded as previously described. Once an acutely malnourished child aged 6–59 months was selected as a case and his or hermother/caretaker interviewed, two non-acutely malnourished children aged 6–59 months were selected as controls and their mothers/caretaker interviewed until the samples allocated to each facility were obtained.
Data Collection Tools and Procedures
An interviewer administered structured questionnaire, which was adapted after a thorough review of different literature, was used to collect data related to the objectives of the study. The questionnaire covered a range of topics including sociodemographic factors, child characteristics, child feeding and caring practices, maternal characteristics, and environmental health conditions. The questionnaire was prepared first in English and translated into local language (Nuer) then back to English by another person who was blinded for the English version to check clarity of the questionnaire. Three data collectors and two supervisors were trained for two days about the objectives of the study, interview, skipping pattern, techniques of measurement and classification. Questionnaire was pretested on 10 acutely malnourished and 10 nonmalnourished children in other health facility to check the clarity of questionnaire, sequence of questions and competence of data collectors. Discussion was held based on the result of the pretest and necessary correction was done. Data were checked for completeness by supervisors on a daily basis during data collection. Regarding anthropometric measurement, calibration of instruments was done on a daily basis. Data were collected by data collectors from all eligible children with mothers or caretakers using a pretested interviewer-administered structured questionnaire and anthropometric measurements. Anthropometric data were collected using measurement tools (MUAC tape, stadiometer, weight scale or salter scale) following standard procedures.
Weight was measured using electronic measuring scale (SECA) to the nearest 0.1 kg in bare feet and with the minimum possible light clothes. Length was measured in the standing position to the nearest 0.1 cm using a measuring board with an upright base and movable headpiece made by Seca, Hamurg, Germany. Length was measured in laying position (recumbent position) using height measuring board or stadiometer to the nearest 0.1 cm for children under 24 months of age. MUAC was measured using easily portable measurement device armband/tape on left arm.
The food security status of the households was determined based on nine standard household food insecurity access scale (HFIAS) questions that were developed for this purpose by food and nutrition technical assistance (FANTA) in 2007 for a developing country. Based on HFIAS, households were categorized as food secure, mild food insecure, moderate food insecure, and severe food insecure.
Data collected on dietary consumption were based on qualitative data collection on dietary recall of seven food groups consumed over the 24 h preceding the survey. These data were used to calculate the dietary diversity score (DDS), the minimum dietary diversity (MDD), the minimum meal frequency (MMF), and the minimum acceptable diet (MAD) classifications. DDS was computed based on the seven food groups which contains grains, roots and tubers; legumes and nuts; dairy products; flesh foods; eggs; vitamin A rich fruits and vegetables; other fruits and vegetables; with one being the minimum score and seven the maximum score. MMD was a consumption of four or more food groups out of the seven food groups for children aged 6–23 months. MMF was defined as receiving solid or semisolid food at least twice a day for breastfed infants 6–8 months; three times a day for breastfed children 9–23 months, and receiving solid or semisolid food or milk feeds at least four times a day for nonbreastfed children 6–23 months. Children aged 6–23 months who have MAD met all three IYCF criteria:1 breastfeeding, or not breastfeeding and receiving two or more feeds of commercial infant formula; fresh, tinned, or powdered animal milk; or yogurt;2 MDD; and3 MMF according to their age and breastfeeding status.
Data Processing and Analysis
Data were entered onto EpiData™ version 3.1 Odense, Denmark and exported to SPSS version 20 (IBM Corporation, Armonk, NY, USA), for descriptive and inferential analyses. Anthropometric data were analyzed using WHO Anthro version 3.2.2. In the analysis, plausibility of anthropometric Z scores were checked using the WHO protocol recommendations (2006), which provide standard deviation cut points for anthropometric Z-scores as a data quality assessment tool.13 Accordingly, implausible z-scores data were excluded if a child’s HAZ was below –6 or above +6, WAZ below –6 or above +5, WHZ below –5 or above +5, or BMIZ below –5 or above +5. Descriptive analysis was used to describe the percentages and number of distributions of the respondents by sociodemographic characteristics and other relevant variables in the study. Binary logistic regression analysis was performed on the independent variables and the dependent variable. Variables with P-value <0.25 in bivariate logistic analysis were entered into final multivariable logistic regression model to control for potential confounders and to identify significant factors associated with outcome variables. The candidate variables were entered into multivariable logistic regression model using Enter method to get significant and insignificant variables in the model. Multicollinearity was checked. Adequacy of the model to fit the outcome variable with the predictors was checked using Hosmer and Lemeshow test for goodness of fit. Finally, adjusted odds ratio (AOR) along with 95%CI was estimated to assess the strength of the association and a P-value <0.05 was considered to declare the statistical significance in the multivariable analysis in this study.
Results
Sociodemographic Characteristics
In this study, a total of 342 children (114 cases and 228 controls) aged 6–59 months with mothers or caretakers were interviewed making the response rate 100%. The mean age of children in this study was 24 months. Protestant was the predominant religion of the respondents (52.6% and 43.4% among respondents with cases and controls respectively). About one third (31.5%) of mothers of cases have no job while 48.2% of mothers of controls were government employees. The principal occupation of fathers of cases and controls was government employment (30.8% and 60.4% respectively). About 13.5% of decision-makers were relatives of cases compared to 7.5% among controls. The mean age of mother at delivery of index child was 23 years. Among households with cases, 10.5% of them had more than three children under five years of age compared to only 3.9% of households with controls (Table 1).
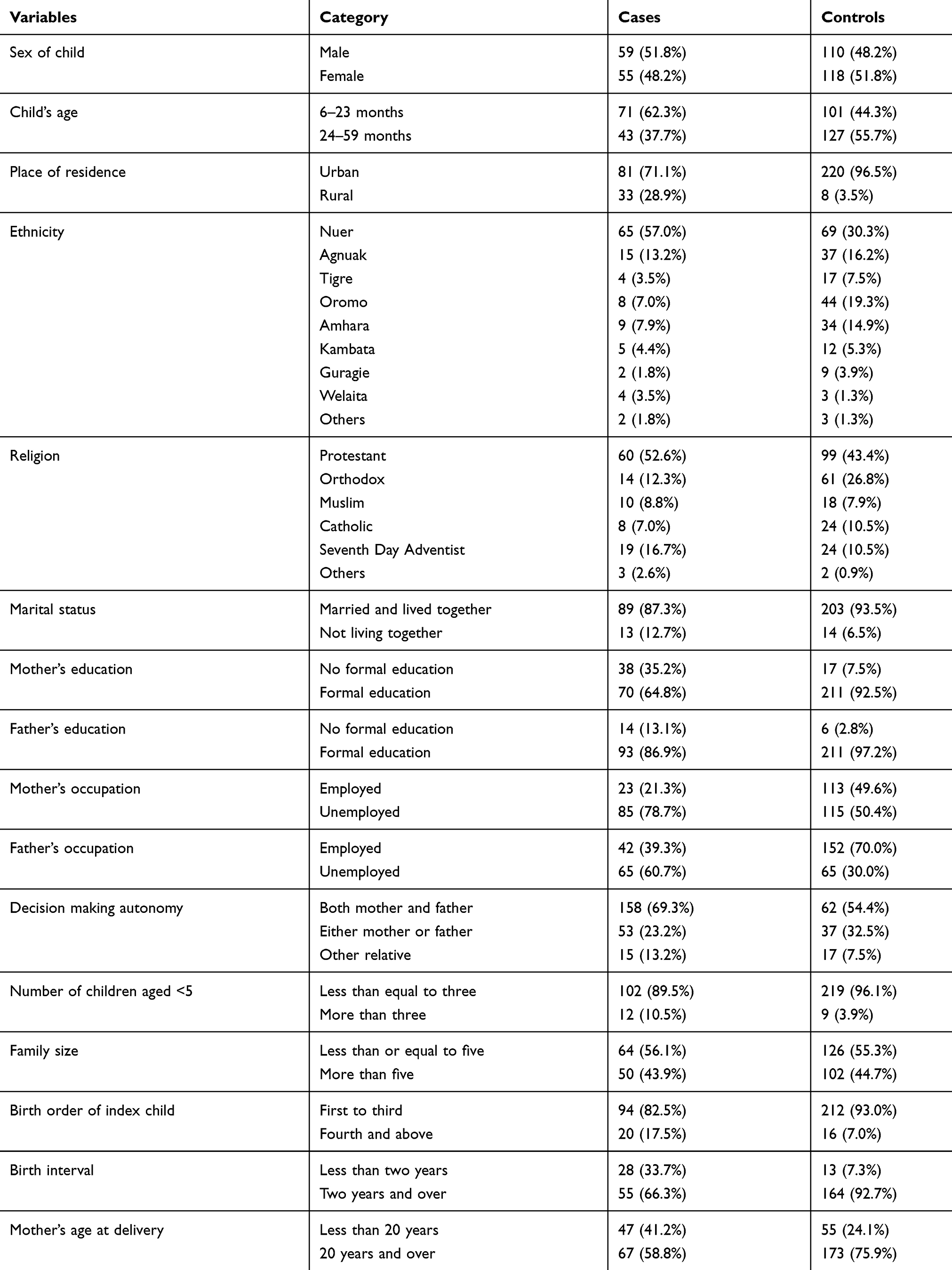 |
Table 1 Sociodemographic Characteristics Among Cases and Controls in Gambella Town, Southwest Ethiopia, July 2019 |
Dietary Diversity of the Children
Dietary recall of seven food groups consumed over the 24 h preceding the survey was assessed. The common food groups consumed were cereals (grains) and vitamin A rich fruits and vegetables. The lowest consumed food groups were legumes and eggs. When comparing the consumption of individual food groups among cases and controls, controls consumed each type of food group more than cases consumed (Figure 1).
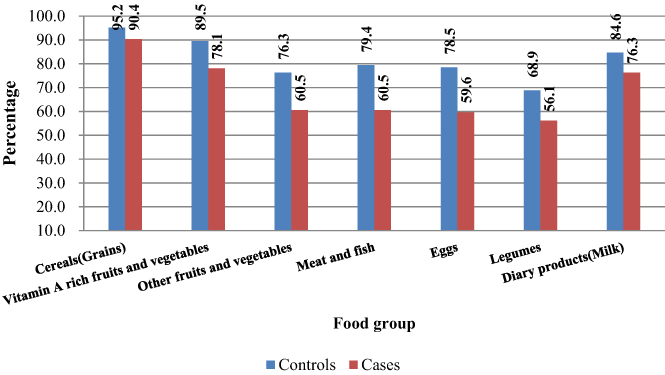 |
Figure 1 Food groups consumed by children 6–59 months in the past 24 h before the survey in Gambella town, Southwest Ethiopia, July 2019. |
Determinants of Acute Malnutrition
In multivariable logistic regression analysis, children whose mothers had no formal education were 2.6 times more likely to have acute malnutrition than their counterparts (AOR=2.55, 95%CI: 1.02–6.37). Likewise, in order of birth, fourth-born children and above were 3.6 times more likely to be acutely malnourished than the first to third children (AOR=3.65, 95%CI: 1.21–11.03). Children from households with more than three children under five years were 3.4 times more likely to have acute malnutrition than children from households with three or fewer children under five years (AOR=3.3.40, 95%CI: 1.03–11.22). Furthermore, children who did not complete vaccination according to their age were 4.6 times more likely to be acutely malnourished than their counterparts (AOR=4.60, 95%CI: 1.51–13.99). Children who were not breastfeeding within one hour of birth were 2.4 times more likely to have acute malnutrition than children who initiated breastfeeding within one hour of birth (AOR=2.43, 95%CI: 1.14–5.17). Likewise children whose mothers have not received IYCF counseling were six times more likely to be acutely malnourished than children whose mothers have received IYCF counseling (AOR=6.02, 95%CI: 2.91–12.46). Children who had diarrhea in the last two weeks before the survey were 2.7 times more likely to be malnourished than those children who did not have diarrhea in the last two weeks before the survey (AOR=2.74, 95%CI: 1.32–5.68) (Table 2).
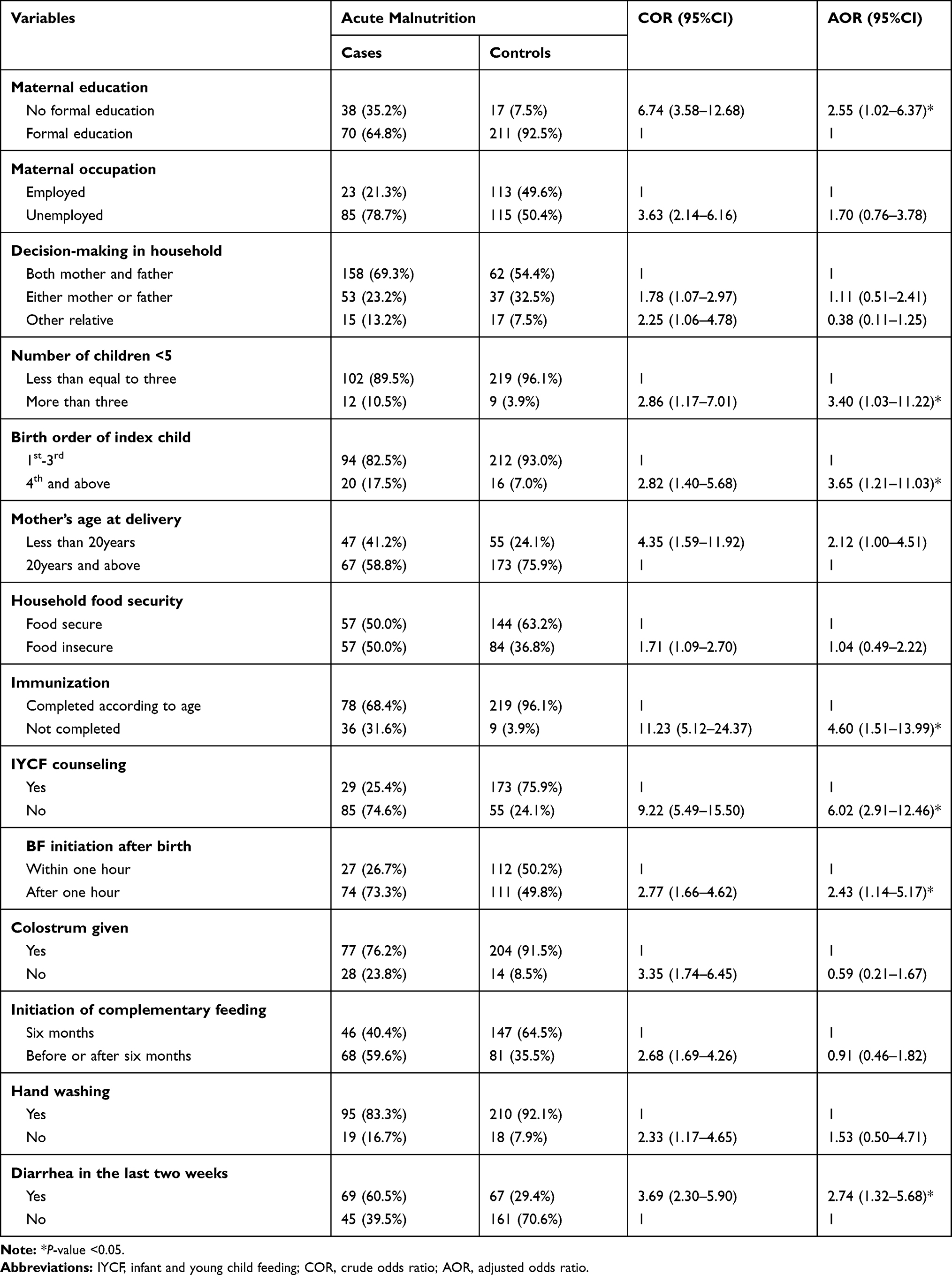 |
Table 2 Predictors of Acute Malnutrition Among Children Aged 6–59 Months in Gambella Town, Southwest Ethiopia, July 2019 |
Discussion
The study revealed that educational status of the mothers/ caretakers, number of children underfive years old in the family, order of birth of the index child, immunization status of the child, IYCF counseling of the mothers/carers, time of breastfeeding initiation after birth and diarrhea in the last two weeks prior to the survey were determinants of nutritional status of the children.
The study revealed that children whose mothers had no formal education were more likely to have acute malnutrition compared to their counterparts. This is consistent with findings of other studies in South Asian countries such as Bangladesh, India, the Maldives, Nepal, Pakistan, and Afghanistan.14–16 It is also in line with findings of other studies in Ethiopia.17–21 This might be due to the fact that mothers with formal education acquire knowledge which helps them to understand and obtain information on optimal child feeding and care practice through education, advice and media.
Number of children under five in the family was another factor significantly associated with acute malnutrition among children 6–59 months. In this study households with more than three children under five years of age were more likely to have acute malnutrition than children from households with fewer than three children under five. This confirms the findings of other studies in Ethiopia, Malaysia, and India.17,21-23 This could probably be due to increased competition for food among children. Beside this, mothers as the main carers for children under five might have also been busy with other household tasks. They could be exhausted while providing the necessary care for more children, which might result in poor childcare practice.
This study further identified that children with higher birth order had higher odds of acute malnutrition than those children with lower birth order. This is icontrary to other studies in Ethiopia21,24 but confirms the findings of studies in South Asian countries such as Bangladesh, India, the Maldives, Nepal, Pakistan, and Afghanistan.15,22,25 The explanation for this might be due to cultural practices in this study area which gives more emphasis to relatively older siblings who stopped breastfeeding and complaint on family about food than the younger one still breastfeeding which might result in less time for feeding and care of younger children.
Children who did not complete immunization for their age were more likely to be acutely malnourished than their counterparts. This is in line with findings of studies in Ethiopia, Nigeria, Pakistan, and India.10,14,21,22,26 This might be due to the fact that complete vaccination helps protect children against most common childhood illnesses which have a negative effect on their nutritional status.
In this study, children whose mothers did not have IYCF counseling were more likely to be acutely malnourished than their counterparts. This is in line with findings of other studies in Ethiopia.17,27 The reason could be due to the fact that counseling on feeding of infants and young children increases awareness on optimal child feeding and care practices.
Time of initiation of breastfeeding after birth was significantly associated with acute malnutrition. Children who were not initiated on breastfeeding within an hour after birth were more likely to develop acute malnutrition when compared to those who were initiated on breastfeeding within an hour of birth. This confirms the finding of a study in Ethiopia.28 It also confirms the finding of a study conducted by analysis of DHS data of 20 countries.29 The association of acute malnutrition and late initiation of breastfeeding after delivery in this study was probably because late initiation of breastfeeding predisposes child to prelacteal feeding and squeezing out of first milk (colostrum) which is full of antibodies that provide first immunization against many diseases. In addition to this, early initiation of breastfeeding also stimulates breast milk production which is crucial for successful subsequent exclusive breastfeeding practices.
Diarrhea in the last two weeks before the survey was found to be significantly associated with acute malnutrition in this study. Those children who had diarrheal diseases in the two weeks prior to the survey were more likely to develop acute malnutrition when compared to their counterparts. Similar findings were found in other studies in Ethiopia,18,20,28,30-33 Chad, Afghanistan, and Pakistan.14,16,34 This is probably due to the fact that diarrhea results in increased needs and high energy expenditure, lower appetite, nutrient losses, poor digestion, malabsorption and the utilization of nutrients resulting metabolic imbalance (loss of body fluids and electrolyte).
Strengths and Limitations of the Study
In this study an attempt was made to use the largest sample size obtained from calculation of sample from different variables to have a representative sample. The study was prone to selection bias since cases were selected from institutions but an attempt was made to include all wasting subjects with no concurrent disease known to cause acute malnutrition. In addition to this, selection of controls was based only on being a nonacute malnourished child from 6–59 months which also minimized selection bias. Selection of controls from institutions also minimized nonresponse bias and recall bias but generalizability may not be possible. In addition to this, controls were not healthy individuals; this might alter the direction of association or mask a true association. Recall bias was also minimized by minimum recall questions and data collectors helped carers to recall events.
Conclusions
This study identified different determinants of acute malnutrition in accordance with other studies in Ethiopia, Africa and other parts of the world. It provided clue on the possible determinants of acute malnutrition in Gambella town. The determinants found were the possible basic, underlying and immediate determinants of acute malnutrition among children aged 6–59 months in Gambella town. The basic determinants found were sociodemographic factors such as no formal education of mothers, number of children under five years of age more than three and higher birth order than three. The underlying determinant found was health service related factors such as incomplete vaccination status of children whereas the immediate determinants found were feeding and care practice related factors such as lack of IYCF counseling, breastfeeding initiation within an hour of delivery, and child health related condition such as diarrhea within the two weeks before the survey. Hence, Gambella Regional Health Bureau (GRHB), Gambella town Health Office and all NGOs working in the nutrition program need to work collaboratively with partners to improve primary and higher education attainment by women and girls, counseling on infants and young children, improve prevention and early treatment of diarrheal diseases through health education.
Abbreviations
AOR, adjusted odds ratio; BMI, body mass index; CMAM, Community Based Management of Acute Malnutrition; COR, crude odds ratio; DDS, dietary diversity score; EDHS, Ethiopian Demographic Health Survey; EFY, Ethiopian fiscal year; FANTA, Food and Nutrition Technical Assistance; HFIAS, household food insecurity access scale; GRHB, Gambella Regional Health Bureau; IYCF, infant and young child feeding; MAD, minimum acceptable diet; MAM, moderate acute malnutrition; MMF minimum meal frequency; MUAC, mid upper arm circumference; SAM, severe acute malnutrition; TB, tuberculosis; UNICEF, United Nations Children’s Fund; WHO, World Health Organization.
Data Sharing Statement
Data will be available upon request from the corresponding author.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki. Ethical clearance was obtained from the Research Review Committee of Mettu University and submitted to Gambella Regional Health Bureau. Prior to the start of data collection, parental/legal guardian written informed consent was obtained after information was provided about the nature and objective of the study. Participants were informed that they have the right not to participate in the study or can withdraw at any time with no repercussion on the quality of any services they receive. Confidentiality was assured at all levels of the study.
Acknowledgments
We would like to express our gratitude to Mettu University. We also appreciate all those involved in materials support and technical guidance for the study. We would also like to thank supervisors and data collectors for taking their precious time to collect the data. We are glad to thank the mothers of children who participated in this study and took their time to provide information.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Development Initiatives. 2018 Global Nutrition Report: Shining a Light to Spur Action on Nutrition. Bristol, UK: Development Initiatives; 2018.
2. UNICEF. Progress for Children: A Report Card on Nutrition. Vol. 4. Progress for children; 2006.
3. Myatt M, Khara TCS, Collins S. A review of methods to detect cases of severely malnourished children in the community for their admission into community-based therapeutic care programs. Food Nutr Bull. 2009;27(3_suppl3):7–23. doi:10.1177/15648265060273S302
4. IOM. Nutrition Surveillance Reports; 2013.
5. Provo A, Atwood S, Sullivan EB, Mbuya N. Malnutrition in Timor-Leste: A review of the burden, drivers, and potential response. Washington DC: World Bank Group. 2017;176.
6. The Lancet. Maternal and child nutrition- executive summary of the lancet maternal and child nutrition series. Lancet. 2013;5(1):1–11.
7. Black RE, Morris SS, Bryce J. Where and why are 10 million children dying every year? Lancet. 2003;361(9376):2226–2234. doi:10.1016/S0140-6736(03)13779-8
8. Black RE, Allen LH, Zulfi Gar A, et al. Maternal and child undernutrition: global and regional exposures and health consequences. lancet. 2008;371(9608):243–260.
9. Sphere P Minimum standards in food security and nutrition. Humanit Chart Minim Stand Humanit response. 2011;140–238.
10. Zewdie T, Abebaw D. Determinants of Child Malnutrition: empirical Evidence from Kombolcha District of Eastern Hararghe Zone, Ethiopia. Q J Int Agric. 2013;52(4):357–372.
11. UNICEF, World Health Organization (WHO), World Bank Group (WB). Levels and Trends in Child Malnutrition 2018; 2018.
12. Central Statistical Agency and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia and Rockville, Maryland, USA; 2016.
13. Mei ZG-SL. Standard deviation of anthropometric Z-scores as a data quality assessment tool using the 2006 WHO growth standards: a cross country analysis. Bull World Health Organ. 2007;85(6):441–448. doi:10.2471/BLT.06.034421
14. Sand A, Kumar R, Shaikh BT, Somrongthong R, Hafeez A, Rai D. Determinants of severe acute malnutrition among children under five years in a rural remote setting: A hospital based study from district Tharparkar-Sindh, Pakistan. Pakistan J Med Sci. 2018;34(2):260–265.
15. Harding KL, Aguayo VM, Webb P. Factors associated with wasting among children under five years old in south asia: implications for action. PLoS One. 2018;13(7):1–17. doi:10.1371/journal.pone.0198749
16. Kamel Frozanfar M, Yoshida Y, Yamamoto E, et al. Acute malnutrition among under-five children in Faryab, Afghanistan: prevalence and causes. Nagoya J Med Sci. 2016;78(1):41–53.
17. Eshetu A, Agedew E, Worku A, Bogale B. Determinant of severe acute malnutrition among children aged 6–59 months in konso, southern ethiopia: case control study. Qual Prim Care. 2016;24(4):181–186.
18. Abuka T, Jembere D, Tsegaw D, Jembere D, Tsegaw D. Determinants for acute malnutrition among under-five children at public health facilities in Gedeo Zone, Ethiopia: a case-control study. Pediatr Ther. 2017;07(02):02. doi:10.4172/2161-0665.1000317
19. Seid A, Seyoum B, Mesfin F. Determinants of acute malnutrition among children aged 6 – 59 months in public health facilities of pastoralist community, afar region, northeast ethiopia: a case control study. Hindawi J Nutr Metab. 2017;2017:1–7. doi:10.1155/2017/7265972
20. Dereje N. Determinants of severe acute malnutrition among under five children in shashogo woreda, southern ethiopia: a community based matched case control study. Nutr Food Sci. 2014;4(05):5. doi:10.4172/2155-9600.1000300
21. Haile A, Amboma A. Children’s nutritional status and its determinants in small towns, Sebeta Hawas district, Oromia, Ethiopia. J Food Sci Nutr. 2018;1(1):33–47. doi:10.35841/food-science.1.1.33-47
22. Shukla N, Toppo NA, Thakur A, Kasar PK, Sharma B. ORIGINAL ARTICLE A study of malnutrition and associated risk factors among children of age 06–59 months in rural area of Jabalpur district, Madhya Pradesh. Indian J Community Heal. 2018;30(01):2–7.
23. Wong H, Moy FM, Nair S. Risk factors of malnutrition among preschool children in Terengganu, Malaysia: a case control study. BMC Public Health. 2014;14(1):785. doi:10.1186/1471-2458-14-785
24. Demissie S, Worku A. Magnitude and factors associated with malnutrition in children 6–59 months of age in pastoral community of dollo ado district, somali Region, Ethiopia. Sci J Public Heal. 2013;1(4):175–183. doi:10.11648/j.sjph.20130104.12
25. Angadi N, Mahabalaraju D. Study to Assess the Maternal Factors Influencing Undernutrition among 3 to 6 Year Old Children of Davangere City. Natl J Commun Med. 2016;7:11.
26. Owoaje E, Onifade O, Desmennu A, Access O. Family and socioeconomic risk factors for undernutrition among children aged 6 to 23 Months in Ibadan, Nigeria. PanAfrican Med J. 2014;8688:1–7.
27. Liben ML, Abuhay T, Haile Y. Acad J ped neonatol factors associated with dietary diversity among children of agro pastoral households in afar regional state, Northeastern Ethiopia. Acad J Ped Neonatol. 2017;5:2.
28. Awoke A, Ayana M, Gualu T. Determinants of severe acute malnutrition among under five children in rural Enebsie Sarmidr District, East Gojjam Zone, North West Ethiopia, 2016. BMC Nutr. 2018;4(1):4. doi:10.1186/s40795-018-0211-5
29. Kerac M, Frison S, Connell N, Page B, McGrath M. Informing the management of acute malnutrition in infants aged under 6 months (MAMI): risk factor analysis using nationally-representative demographic & health survey secondary data. Peer J. 2019;6:e5848. doi:10.7717/peerj.5848
30. Gezahegn Y, Kassahun W, Dube L. Factors Associated with Acute Malnutrition among South Sudanese Children in Tierkidi Refugee Camp: A Case-Control Study. Quality Primary Care. 2017;25(4):253–258.
31. Asfaw M, Wondaferash M, Taha M, Dube L. Prevalence of undernutrition and associated factors among children aged between six to fifty nine months in Bule Hora district, South Ethiopia. BMC Public Health. 2015;15(1):1–9. doi:10.1186/s12889-015-1370-9
32. Andarge B, Kumar A, Quadri J, et al. Major determinants of severe acute malnutrition in under five children in jimma town of Southwest Ethiopia. Int J Manag Econ Soc Sci. 2012;1(1):1–12.
33. Ayana AB, Hailemariam TW, Melke AS. Determinants of acute malnutrition among children aged 6–59 months in Public Hospitals, Oromia region, West Ethiopia: a case–control study. BMC Nutr. 2015;1(1):34. doi:10.1186/s40795-015-0031-9
34. Tesfai C, Ratnayake R, Myatt M. Measuring local determinants of acute malnutrition in Chad: a case-control study. Lancet. 2013;381:S144. doi:10.1016/S0140-6736(13)61398-7
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.