")
Back to Journals » International Journal of General Medicine » Volume 15
Determinant of Osteopontin Levels in Microvascular Complications in Patients with Diabetes
Authors Nawaz SS , Siddiqui K , Mujammami M, Alotaibi O , Alanazi SS, Rafiullah M
Received 15 December 2021
Accepted for publication 7 April 2022
Published 27 April 2022 Volume 2022:15 Pages 4433—4440
DOI https://doi.org/10.2147/IJGM.S354220
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Shaik Sarfaraz Nawaz,1,* Khalid Siddiqui,1,* Muhammad Mujammami,1– 3 Obeed Alotaibi,2 Saud Sulaiman Alanazi,1 Mohamed Rafiullah1
1Strategic Center for Diabetes Research, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2University Diabetes Center, King Saud University Medical City, King Saud University, Riyadh, Saudi Arabia; 3Division of Endocrinology, Department of Medicine, College of Medicine, King Saud University, Riyadh, Kingdom of Saudi Arabia
*These authors contributed equally to this work
Correspondence: Khalid Siddiqui, Strategic Center for Diabetes Research, College of Medicine, King Saud University, P.o Box: 245, Riyadh, 11411, Saudi Arabia, Tel +966 114724179 Ext.3106, Fax +966 114725682, Email [email protected]
Background: Osteopontin (OPN) is a 44-kDa multifunctional protein and has a diverse role in biomineralization, tissue remodeling, and chronic inflammation. However, its role in type 2 diabetes (T2D) patients with microvascular complications is not clear. Therefore, the present study aimed to investigate the role of OPN in T2D patients with microvascular complications.
Methods: A total of 324 type 2 diabetes patients in the age group of 38– 66 years were included in this study; 249 T2D patients were diagnosed with microvascular complications. OPN was measured using an enzyme-linked immunosorbent assay kit. Clinical data, such as age, gender, diabetes duration, systolic blood pressure, diastolic blood pressure, were measured. Correlation between OPN levels with different clinical parameters was evaluated.
Results: In patients with microvascular complications, OPN levels were significantly higher than those without microvascular complications (p < 0.05). Moreover, OPN levels were positively associated with systolic blood pressure (SBP), C-reactive protein, and albumin creatinine ratio (ACR). Multiple linear regression analysis showed that OPN levels were independently associated with C-reactive protein (p < 0.045).
Conclusion: The findings in the present study showed that OPN level was more positively associated with C-reactive protein than that with glucose metabolism in patients with microvascular complications. Thus, OPN might serve as a marker in predicting vascular disease.
Keywords: osteopontin, diabetes, microvascular complication, inflammation, C-reactive protein
Introduction
Diabetes is a serious chronic and long-term condition that occurs when there is an elevated level of glucose in the blood because the body cannot produce enough insulin or cannot effectively use the insulin it produces. Currently, it is estimated that nearly 537 million adults (20–79 years) are having diabetes and this number is predicted to rise to 643 million by 2030 and is estimated to reach 784 million by 2045.1 People living with diabetes are at heightened risk of developing several serious and life-threatening complications. The microvascular complications are retinopathy, nephropathy, and neuropathy. However, diabetic patients will have one or more of these subclinical manifestations during the long-term duration of their disease.2 Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) trial study in type 2 diabetes demonstrated that long-term glycemic variability is known to be associated with vascular complication development in type 2 diabetes.3 Recently, reviews have also clarified the adverse glycemic effects inducing several biochemical pathways linking microvascular complications. Molecular mechanisms include non-enzymatic protein glycation and the formation of advanced glycation end products (AGEs); overproduction of reactive oxygen species and chronic endoplasmic reticulum dysfunction and stress; activation of diacylglycerol (DAG)-protein Kinase C (PKC) pathway; activation of polyol pathway; renin–angiotensin system activation; kallikrein–kinin/bradykinin system activation in vascular tissues.4,5 Moreover, subjects with diabetes exhibit pathologically enhanced markers of microvascular complications.
Osteopontin (OPN) is a 44-kDa multifunctional secreted protein with diverse functions in normal physiological as well as pathological conditions including biomineralization, tissue remodeling, and chronic inflammation.6 OPN levels are shown to be associated with prediabetes,7 and type 2 diabetes with cardiovascular autonomic functions.8 Furthermore, OPN levels are associated with diabetic complications such as retinopathy,9,10 nephropathy,11,12 and neuropathy.13 However, its role in microvascular complications in type 2 diabetes patients is less studied. We therefore aimed to investigate the level and role of OPN in type 2 diabetes patients with microvascular complications.
Materials and Methods
Participants
All the participants were diagnosed with type 2 diabetes (T2D). Diabetes was defined using the American Diabetes Association (ADA) criteria.14 The study participants were selected from Saudi Diabetes Kidney Disease (SAUDI-DKD) cohort.15 This study was approved by the College of Medicine's Institutional Review Board and has been conducted in accordance with the principles outlined in the Helsinki Declaration. A research physician interviewed all the participants. Clinical data such as age, gender, diabetes duration, systolic blood pressure, and diastolic blood pressure, were measured. Body mass index (BMI) (kg/m2) was calculated for each participant by dividing weight in (kg) by height squared in (m2). Informed written consent for participation in the research study and biospecimen collection was obtained from all the participants.
Study Design
In this observational case–control study, we initially screened 467 T2D patients from the University Diabetes Center, King Saud University Medical City, King Saud University, Riyadh. All the participants were on treatment with oral hypoglycemic agents and/or on insulin in Saudi Arabia between April 2014 and June 2015. The exclusion and inclusion criteria were as previously reported.15 Patients with macrovascular complications such as ischemic heart disease, cardiovascular disease, peripheral vascular disease, and stroke were excluded from this study. A total of 324 type 2 diabetes patients in the age group 38–66 years were included in this study and are divided into 2 groups according to the presence and absence of microvascular complications. Seventy-five T2D patients had none of the microvascular complications, while 249 T2D patients had microvascular complications as shown in Figure 1. We used Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations to improve the quality of observational studies.16
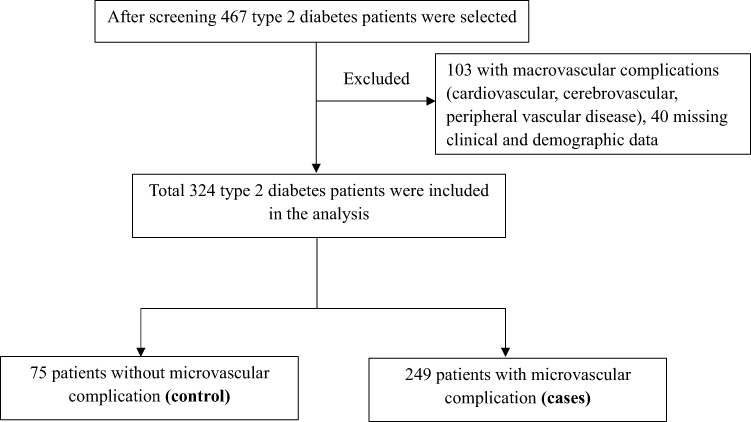 |
Figure 1 Flow chart for patients’ selection and exclusion according to their complications. |
Diagnostic Criteria of Microvascular Complications
During the clinic visit, participants were diagnosed with diabetic complications; either diabetic neuropathy (assessed by 10-g monofilament and reduced vibration perception using 128 Hz tuning fork), diabetic nephropathy (assessed by urine albumin ≥ 30 mg/g of creatinine), or diabetic retinopathy (diagnosed by fundus photographic examination following mydriasis of both eyes) by a retina specialist.17
Laboratory Analysis
After an overnight fast, 10cc of blood was drawn from the cubital vein of all the participants. Blood samples were transported to the Strategic Center for Diabetes Research, College of Medicine, King Saud University, Riyadh. Blood samples were centrifuged at 2000 rpm for 10 min. Serum was collected and stored at −20°C for measurement of fasting blood glucose, glycated hemoglobin (HbA1c), total cholesterol, triglycerides, low-density lipoprotein, and high-density lipoprotein. A 10cc of fresh urine sample was collected and stored at −20°C for measurement of albumin and creatinine using Rx Daytona clinical chemistry analyzer (Randox laboratories, UK). eGFR was calculated using a new equation.18 Serum C-reactive protein was measured using Metabolic syndrome array II assay (Catalog No. EV3758), Randox biochip analyzer. Serum OPN was measured using an ELISA kit (Catalog No. ab100618), Abcam, Cambridge, MA, USA).
Statistical Analysis
A Statistical Package for the Social Science (SPSS) 21.0 IBM, USA, was used to analyze the clinical data. Data with normal distribution were expressed as mean ± standard deviation. Data with skewed distribution were expressed as median (interquartile range). The Chi-square test was used to compare the frequency among groups. The Student’s t-test was used to compare the clinical variables between two groups. Mann–Whitney test for continuous data with skewed distribution. A bivariate correlation was used to analyze the association between OPN and clinical variables. Linear regression analysis was used to determine the association between clinical variables that were significant in the bivariate analysis for OPN protein. A statistical p-value ≤0.05 is considered to be significant.
Results
Table 1 shows the baseline characteristics of controls (T2D without microvascular complication and cases (T2D with microvascular complication). There is no significant difference in their age, gender, DBP, HDL-C, LDL-C among control and cases (P > 0.05). However, the results showed that duration of diabetes, BMI, SBP, FBS, HbA1c%, total cholesterol, triglycerides, C-reactive protein, ACR, and OPN were significantly higher in cases (p < 0.05). While eGFR was significantly lower in cases compared to control (P < 0.05).
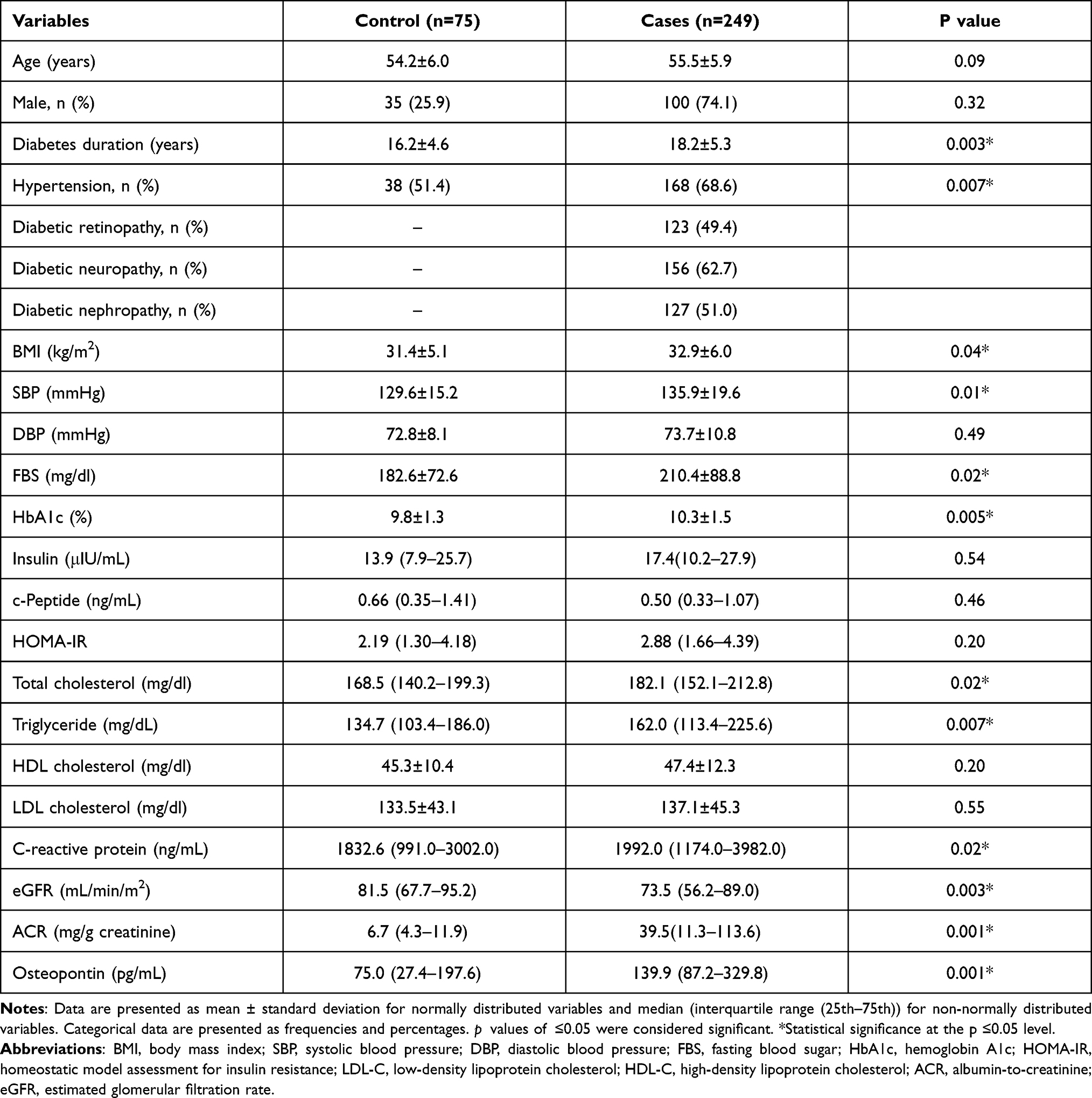 |
Table 1 Baseline Characteristics of T2D without Microvascular Complication (Control) and T2D with Microvascular Complication (Cases) |
Table 2 shows the association of OPN level with different clinical parameters. OPN levels were positively associated with SBP (rho=0.135; p=0.019), C-reactive protein (rho=0.135; p=0.024), and albumin creatinine ratio (ACR) (rho=0.297; p<0.001). However, no significant correlation was observed between OPN and age, diabetes duration, BMI, DBP, FBS, HbA1c%, total cholesterol, triglyceride, and eGFR.
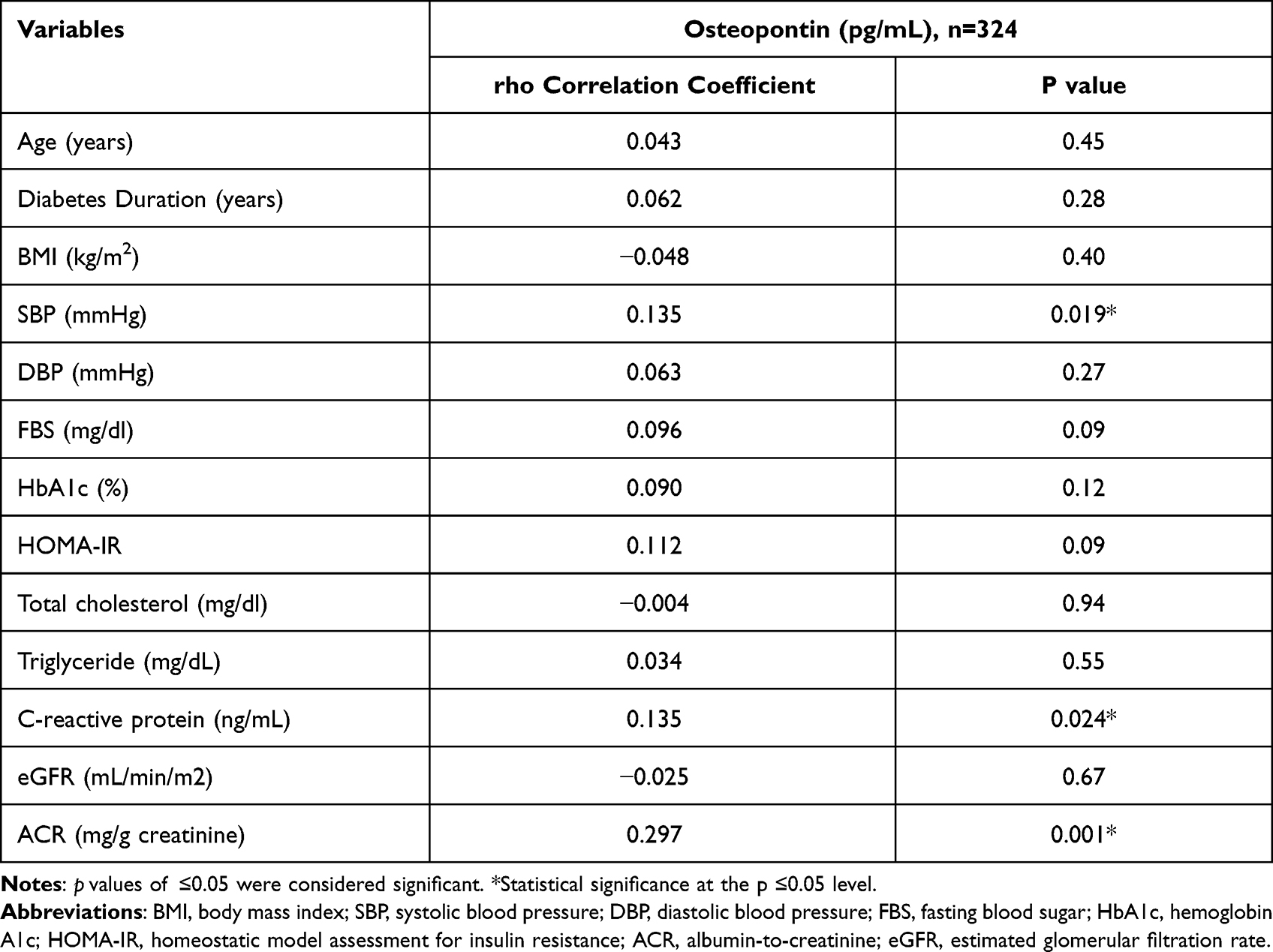 |
Table 2 Association of Osteopontin Level with Different Metabolic Parameters |
In Table 3, multiple linear regression analysis of OPN as dependent variable and SBP, ACR, and C-reactive protein as independent variables was performed to examine the association of OPN level with variables that showed statistical significance in the bivariate analysis. Results from linear regression analysis showed that OPN levels were independently associated with C-reactive protein (p <0.045).
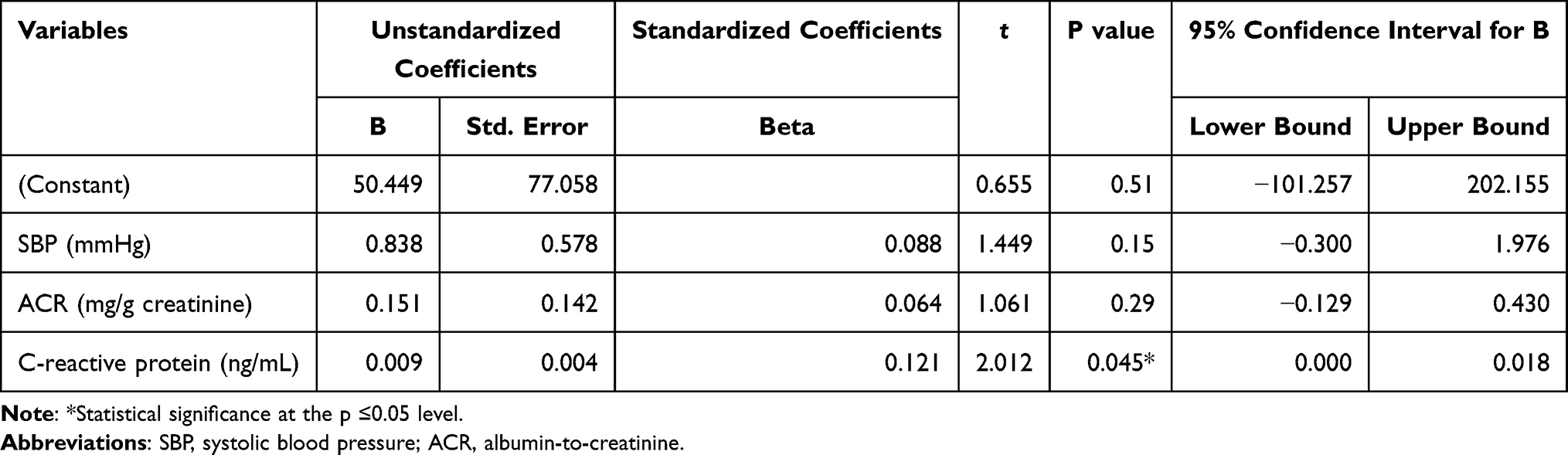 |
Table 3 Multivariable Linear Regression Analysis of Osteopontin (as Dependent Variable) with Independent Variables |
Discussion
In the present study, OPN level was higher in type 2 diabetes patients with microvascular complications. This study also evaluated the association of OPN with different metabolic parameters and showed that OPN level was independently associated with C-reactive protein level and further, demonstrated the role of inflammation in type 2 diabetes patients with microvascular complications. Moreover, we found that metabolic variables such as age, HOMA-IR, diabetes duration, BMI, and eGFR, have no significant role in the upregulation of OPN.
Earlier, studies have shown that OPN is an active player in many physiological and pathological processes, such as atherosclerosis, cancer, chronic inflammatory disease, glomerulonephritis, adipose tissue inflammation, and insulin resistance.19 OPN is expressed in leukocytes and secreted by activated macrophages during acute inflammatory processes. OPN regulates immune cells macrophages, dendritic cells, and T-cells.6,19,20 Daniele G et al measure the circulating cytokines such as TNF-α, IL-6, MCP-1, OPN, fractalkine, and adiponectin involved in the subclinical systemic inflammation and found to be associated with hyperglycemia and insulin resistance.21 OPN has recently emerged as a key factor in both vascular remodeling and atherosclerosis progression. Coronary artery disease (CAD) patients have increased OPN and IL-6 levels. Moreover, IL-6 levels correlated with OPN (r=0.030, P<0.001) levels. Suggesting a possible mechanism linking OPN level with CAD progression through arterial wall stiffening and inflammation.22,23 Thus, inflammation and inflammatory events play an important role in the pathogenesis of microvascular complications.24,25
The results of our previous cross-sectional study in type 2 diabetes patients confirmed that patients with diabetic nephropathy had higher OPN levels. OPN levels were significantly increased according to decreased eGFR and elevated ACR. OPN levels were associated with hyperglycemia, inflammation, insulin resistance, and proteinuria.12 In agreement with our findings earlier Yamaguchi et al, evaluated the plasma and urinary OPN levels in 229 type 2 diabetic microvascular complications such as retinopathy, neuropathy, and nephropathy. OPN levels increased significantly with the progression of nephropathy. However, there was no change in the OPN related to the progression of retinopathy or neuropathy. Thus, indicating that OPN level is a predictor of end-stage renal disease but not for retinopathy and neuropathy.11
In fact, Maser et al demonstrate that OPN is associated with reduced peripheral autonomic nerve function in type 2 diabetes subjects and is involved in the pathogenesis of sudomotor dysfunction.26 Recently, in agreement with our findings, Zhang et al in a multiethnic cohort in Singapore demonstrated that OPN was higher in type 2 diabetes patients with diabetic retinopathy (64.7 [49.7–89.5] ng/mL) than in type 2 diabetes patients without diabetic retinopathy (51.7 [38.9–66.9] ng/mL; p<0.001).10 Furthermore, OPN levels were associated with the presence and severity of diabetic retinopathy, suggesting OPN as a potential biomarker for diabetic retinopathy. In agreement with our results in Table 2. El Dayem et al evaluated the relationship between OPN and diabetic complications in seventy type 1 diabetic patients. OPN levels correlate with Systolic blood pressure (mmHg) (r=0.28; p <0.030); albumin creatinine ratio (ACR) (r=0.48; p<0.0001).27 OPN levels are increased in type 1 diabetes patients and can be used for the early detection of microvascular and macrovascular complications.27 Similarly, Talat et al demonstrate that elevated OPN levels are independently associated with type 1 pediatric patients and support the hypothesis that OPN may have a role in the prediction of microvascular complications. Multivariate logistic regression analysis also revealed an association of increased OPN levels with diabetes (OR=1.73; p=0.004), DR (OR=2.07; p=0.045, and DN (OR=2.20; p=0.026).28 Moreover, Barchetta et al evaluate circulating OPN levels in adult patients with type 1 diabetes mellitus (T1DM) compared to non-diabetic control. T1DM patients had significantly higher serum OPN levels than controls (17.2±12.9 vs 10.5±11.6 μg/l, P=0.009). OPN levels correlated with higher blood pressure, BMI, creatinine, γ-GT, ALP, and lower HDL-C. No correlation was shown between OPN and HbA1c, C-peptide, insulin requirement, co-medications, and diabetes duration.29 In agreement with our findings Momiyama et al investigated the association of C-reactive protein and OPN levels with severities of both coronary and aortic atherosclerosis. OPN and C-reactive protein levels were independent factors in aortic atherosclerosis.30
Li T et al show that OPN is involved in mineral metabolism and is associated with severe and extensive vascular calcification. High glucose induces the expression of OPN in smooth muscles cells (SMCs) and vascular endothelial cells (VECs), which is a key factor in the calcification and dysfunction of the vascular wall in diabetes.31 Similar to the above study, Ito et al also investigated the effect of high glucose and high insulin on human pancreatic duct epithelial cells lines (HPDE-6). High glucose level accelerates cell proliferation and increases the secretion and mRNA expression of OPN.32 Glucose-dependent insulinotropic polypeptide (GIP) induces the expression of the proatherogenic cytokine OPN in mouse arteries via the local release of endothelin-1 and activation of CREB. OPN levels were positively correlated with limb ischemia, stroke, transient ischemic attacks, and amaurosis fugax.33 Considerable evidence has shown that hyperglycemia can stimulate OPN expression in the culture vascular cells leading to the development of microvascular complications. Many of the stimuli are known to enhance OPN expression, including hyperglycemia, angiotensin II (Ang II), glucose-dependent insulinotropic peptide (GIP), oxidized LDL-C, IL-1β, IL-2, IL-3, IL-6, IL-18, INF-γ, TNF-α, and TGF- β.6 Previous study hypothesized the molecular mechanism that underlies vascular complication and demonstrates that hyperglycemia activates nuclear factor of activated T cells (NFATc3) signaling in vascular smooth muscles. NFATc3 activation leads to increased OPN protein expression in arteries, and this leads to vascular disease. Pharmacological treatment of NAFT with inhibitor A-285222 prevented glucose-induced OPN expression in arteries.34 Although monitoring blood glucose levels and current diabetes treatment are still not effective to prevent the development of microvascular complications. In a recent meta-analysis, a paleolithic diet has been shown to decrease blood pressure, inflammation and improve the vasculature in obese subjects.35 In addition, the pleiotropic effect of metformin has been shown to reduce carotid intima-media thickness in humans.36 Therefore, early detection of microvascular complications and effective treatment becomes important issue. Inhibition of OPN may exert favorable effects on microvascular complications.
The major strength of the current study is well-characterized cases with matched age, gender, and duration of diabetes. Furthermore, we include an unequal number of cases and with controls in the ratio (3.3:1) to increase the power of the study. We have also evaluated and identified the most likely associated parameters with OPN. The major limitation is a single-center study. Secondly, we did not measure the vascular markers to assess the vascular dysfunction as the causation of microvascular complications is complex. We also cannot rule out the interference of medications on OPN. These results need to be confirmed in other populations.
Conclusion
OPN levels were significantly elevated in type 2 diabetes microvascular complications and independently associated with C-reactive protein in inflammatory processes. Thus, OPN might serve as a marker in predicting vascular disease.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy reasons.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the College of Medicine Institutional Review Board, College of Medicine, King Saud Universty, Saudi Arabia.
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Acknowledgments
The author would like to acknowledge the Strategic Center for Diabetes Research that is funded by the National Plan for Science, Technology, and Innovation (MAARIFAH), King Abdul-Aziz City for Science and Technology, Kingdom of Saudi Arabia. We also like to thank University Diabetes Center, King Saud University Medical City (KSUMC), King Saud University for patient recruitment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The article processing charges (APC) to publish as open access will be funded by University Diabetes Center, King Saud University Medical City (KSUMC), King Saud University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. International Diabetes Federation. IDF Diabetes Atlas.
2. Vithian K, Hurel S. Microvascular complications: pathophysiology and management. Clin Med. 2010;10(5):505–509.
3. Scott ES, Januszewski AS, O’Connell R, et al. Long-term glycemic variability and vascular complications in type 2 diabetes: post hoc analysis of the FIELD study. J Clin Endocrinol Metab. 2020;105(10):45.
4. Barrett EJ, Liu Z, Khamaisi M, et al. Diabetic microvascular disease: an endocrine society scientific statement. J Clin Endocrinol Metab. 2017;102(12):4343–4410.
5. Găman M-A, Epîngeac ME, Diaconu CC, Găman AM. Evaluation of oxidative stress levels in obesity and diabetes by the free oxygen radical test and free oxygen radical defence assays and correlations with anthropometric and laboratory parameters. World J Diabetes. 2020;11(5):193–201.
6. Kahles F, Findeisen HM, Bruemmer D. Osteopontin: a novel regulator at the cross roads of inflammation, obesity, and diabetes. Molecular Metabolism. 2014;3(4):384–393.
7. Daniele G, Winnier D, Mari A, et al. The potential role of the osteopontin-osteocalcin-osteoprotegerin triad in the pathogenesis of prediabetes in humans. Acta Diabetol. 2018;55(2):139–148.
8. Maser RE, Lenhard MJ, Pohlig RT, Balagopal PB. Osteopontin and osteoprotegerin levels in type 2 diabetes and their association with cardiovascular autonomic function. J Diabetes Complications. 2016;30(3):507–510.
9. Kase S, Yokoi M, Saito W, et al. Increased osteopontin levels in the vitreous of patients with diabetic retinopathy. Ophthalmic Res. 2007;39(3):143–147.
10. Zhang X, Chee WK, Liu S, et al. Association of plasma osteopontin with diabetic retinopathy in Asians with type 2 diabetes. Mol Vis. 2018;24:165.
11. Yamaguchi H, Igarashi M, Hirata A, et al. Progression of diabetic nephropathy enhances the plasma osteopontin level in type 2 diabetic patients. Endocr J. 2004;51(5):499–504.
12. Siddiqui K, Nawaz SS, Mujammami M. SAT-163 association of osteopontin with the risk factors of nephropathy in patients with type 2 diabetes. Kidney International Reports. 2020;5(3):S70.
13. Pizzamiglio C, Ripellino P, Prandi P, et al. Nerve conduction, circulating osteopontin and taxane-induced neuropathy in breast cancer patients. Neurophysiologie Clinique. 2020;50(1):47–54.
14. Association AD. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2019. Diabetes Care. 2019;42(Supplement 1):S13–S28.
15. Al-Rubeaan K, Siddiqui K, Alghonaim M, Youssef AM, AlNaqeb D. The Saudi Diabetic Kidney Disease study (Saudi-DKD): clinical characteristics and biochemical parameters. Ann Saudi Med. 2018;38(1):46–56.
16. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Epidemiology. 2007;18(6):805–835.
17. Association AD. 11. Microvascular complications and foot care: standards of medical care in diabetes—2021. Diabetes Care. 2021;44(Supplement 1):S151–S167.
18. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612.
19. Lund SA, Giachelli CM, Scatena M. The role of osteopontin in inflammatory processes. J Cell Commun Signal. 2009;3(3):311–322.
20. Lund SA, Wilson CL, Raines EW, Tang J, Giachelli CM, Scatena M. Osteopontin mediates macrophage chemotaxis via α4 and α9 integrins and survival via the α4 integrin. J Cell Biochem. 2013;114(5):1194–1202.
21. Daniele G, Mendoza RG, Winnier D, et al. The inflammatory status score including IL-6, TNF-α, osteopontin, fractalkine, MCP-1 and adiponectin underlies whole-body insulin resistance and hyperglycemia in type 2 diabetes mellitus. Acta Diabetol. 2014;51(1):123–131.
22. Maniatis K, Siasos G, Oikonomou E, et al. Osteoprotegerin and osteopontin serum levels are associated with vascular function and inflammation in coronary artery disease patients. Curr Vasc Pharmacol. 2020;18(5):523–530.
23. Găman MA, Cozma MA, Dobrică EC, Bacalbașa N, Bratu OG, Diaconu CC. Dyslipidemia: a trigger for coronary heart disease in Romanian patients with diabetes. Metabolites. 2020;10(5):54.
24. Della Corte V, Tuttolomondo A, Pecoraro R, Di Raimondo D, Vassallo V, Pinto A. Inflammation, endothelial dysfunction and arterial stiffness as therapeutic targets in cardiovascular medicine. Curr Pharm Des. 2016;22(30):4658–4668.
25. Zanoli L, Boutouyrie P, Fatuzzo P, et al. Inflammation and aortic stiffness: an individual participant data meta-analysis in patients with inflammatory bowel disease. J Am Heart Assoc. 2017;6:10.
26. Maser RE, Lenhard MJ, Pohlig RT, Balagopal PB. Osteopontin and clusterin levels in type 2 diabetes mellitus: differential association with peripheral autonomic nerve function. Neurological Sciences. 2017;38(9):1645–1650.
27. Abd El Dayem SM, El Bohy AEM, Battah AA, Hamed M, Abd El Aziz SH. Osteopontin for early detection of microvascular and macrovascular type 1 diabetic complication. Open Access Macedonian j Med Sci. 2019;7(21):3619.
28. Talat MA, Sherief LM, El-Saadany HF, Rass AA, Saleh RM, Sakr MMH. The role of osteopontin in the pathogenesis and complications of type 1 diabetes mellitus in children. J Clin Res Pediatr Endocrinol. 2016;8(4):399.
29. Barchetta I, Alessandri C, Bertoccini L, et al. Increased circulating osteopontin levels in adult patients with type 1 diabetes mellitus and association with dysmetabolic profile. Eur J Endocrinol. 2016;174(2):187–192.
30. Momiyama Y, Ohmori R, Fayad ZA, et al. Associations of plasma C-Reactive Protein and osteopontin levels with the severities of coronary and aortic atherosclerosis. J Cardiovascular Magnetic Resonance. 2009;11(1):1–316.
31. Li T, Ni L, Liu X, Wang Z, Liu C. High glucose induces the expression of osteopontin in blood vessels in vitro and in vivo. Biochem Biophys Res Commun. 2016;480(2):201–207.
32. Ito M, Makino N, Matsuda A, et al. High glucose accelerates cell proliferation and increases the secretion and mRNA expression of osteopontin in human pancreatic duct epithelial cells. Int J Mol Sci. 2017;18(4):807.
33. Berglund LM, Lyssenko V, Ladenvall C, et al. Glucose-dependent insulinotropic polypeptide stimulates osteopontin expression in the vasculature via endothelin-1 and CREB. Diabetes. 2016;65(1):239–254.
34. Nilsson-Berglund LM, Zetterqvist AV, Nilsson-Ohman J, et al. Nuclear factor of activated T cells regulates osteopontin expression in arterial smooth muscle in response to diabetes-induced hyperglycemia. Arterioscler Thromb Vasc Biol. 2010;30(2):218–224.
35. Sohouli MH, Fatahi S, Lari A, et al. The effect of paleolithic diet on glucose metabolism and lipid profile among patients with metabolic disorders: a systematic review and meta-analysis of randomized controlled trials. Crit Rev Food Sci Nutr. 2021;1:1–12.
36. Chen Y, Li H, Ye Z, Găman MA, Tan SC, Zhu F. The effect of metformin on carotid intima-media thickness (CIMT): a systematic review and meta-analysis of randomized clinical trials. Eur J Pharmacol. 2020;886:173458.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.