")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Detection, diagnosis, and treatment of Alzheimer’s disease dementia stratified by severity as reported by caregivers in Japan
Authors Montgomery W, Goren A , Kahle-Wrobleski K, Nakamura T, Ueda K
Received 22 December 2017
Accepted for publication 12 April 2018
Published 16 July 2018 Volume 2018:14 Pages 1843—1854
DOI https://doi.org/10.2147/NDT.S160591
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
William Montgomery,1 Amir Goren,2 Kristin Kahle-Wrobleski,3 Tomomi Nakamura,4 Kaname Ueda5
1Global Patient Outcomes & Real World Evidence, Eli Lilly Australia, NSW, Australia; 2Real World Evidence, Kantar Health, New York, NY, USA; 3Global Patient Outcomes and Real World Evidence, Eli Lilly and Company, Lilly Corporate Center, Indianapolis, IN, USA; 4Bio-Medicines, Medical Development Unit, Eli Lilly Japan K.K., Tokyo, Japan; 5Health Outcomes, Health Technology Assessment, & Real World Evidence, Medical Development Unit, Eli Lilly Japan K.K., Kobe, Japan
Background: Dementia of Alzheimer’s disease (AD) imposes burdens on patients, caregivers, and society. This cross-sectional study examined caregiver-reported history of disease onset and AD dementia to inform efforts promoting early disease detection and diagnosis.
Methods: An online survey collected self-reported cross-sectional data – demographic characteristics, diagnosis, treatment experiences, and other information on disease detection, diagnosis, and treatment – from caregivers of patients with AD dementia. These characteristics were examined as a function of AD dementia severity.
Results: Three hundred patients with AD dementia were trichotomized by long-term care insurance levels reported by caregivers: 12.3% (n=37) as low severity, 63.7% (n=191) as medium severity, and 24.0% (n=72) as high severity. The Short-Memory Questionnaire and patient dependency scores both varied significantly across severity groups. AD dementia symptoms were most frequently first detected by a caregiver (58.7%) or the patient’s family (45.7%). However, in 13.7% of cases, symptoms were detected by a health care provider during a routine visit. Memory problems were the most frequent first symptoms (77.3%), followed by repetition (55.7%). Patients (73.7%) were taking symptomatic treatment such as acetylcholinesterase inhibitors or memantine. High-severity patients were older, had been diagnosed with AD dementia for a longer time, had more frequent reports of memory problems as the first symptoms detected, and required more hours of care per day, compared with low-severity patients.
Conclusion: Caregivers and families play an integral role in the identification of AD dementia patients, with memory problems being common first symptoms noticed by caregivers that led to a diagnosis of AD dementia. These results provide novel insight into the detection, diagnosis, and treatment of AD dementia in Japan and how these factors differ across the spectrum of disease severity.
Keywords: Alzheimer’s disease dementia, Japan, disease history, caregivers, treatment pattern
Background
Dementia of Alzheimer’s disease (AD) represents the most common form of dementia, and symptoms typically do not present until later in life. Therefore, the prevalence of AD dementia is predicted to rise in the coming years as the median age of the global population continues to increase.1,2 Notably, Japan is among the countries with the highest rates of AD dementia, with a point prevalence of 3.8% in the population older than 65.3,4 Even more concerning, the number of patients in Japan with dementia is expected to rise correspondingly as the population ages,3,5,6 with recent studies predicting that the number of those experiencing dementia will increase from 2.5 to 7.3 million by 2025.6–8 Thus, caring for these individuals and their caregivers is a paramount public health issue.9
AD dementia has been shown to be associated with significant humanistic and economic burden globally. AD is a progressive neurodegenerative disorder that results in impaired cognition (eg, memory difficulties) and impaired ability to complete activities of daily living (ADLs). As symptoms gradually worsen over time, people with AD usually require increased levels of support and care. Informal caregivers (eg, family members) are frequently responsible for the care of AD patients, particularly as the condition worsens over time.10
Informal caregivers play an integral role in the care of patients with AD dementia in Japan and throughout the world. In contrast to diseases for which care is administered primarily by medical professionals in a clinical setting, the slow and progressive nature of AD dementia often results in many patients being cared for in the home by family members. At the same time, informal caregiving without appropriate supportive structures may be associated with a variety of poor outcomes for caregivers11,12 – across physical,13,14 psychological,15,16 social,17 and financial18 domains – both globally and in the country of interest, Japan.19–26 Japan possesses the fastest aging population in the world, with the multifaceted burden associated with AD dementia in this country also continuing to grow.27 As rates of AD dementia increase, the role of caregivers in early detection of disease and providing informal care will increase in importance, as will the potential burden associated with informal caregiving. This research base includes work which found that caregivers experienced significant impairments in health utility scores, quality of life, and work productivity, and had higher rates of mental health issues and health care resource utilization compared with non-caregivers.28 Despite these associated impairments, many caregivers may also derive positive effects through caregiving – most often, in the form of meaning-based outcomes.29–32
Furthermore, formal and informal care of AD dementia patients may entail significant economic consequences.33–36 In Japan, the cost associated with dementia care was recently estimated to be $145 billion, with informal care representing nearly half of this overall cost ($62 billion, where $1=100 yen).37 To address the growing care demands and costs associated with AD dementia, the Japanese government, in 2000, implemented an insurance program and long-term care strategy, with insurance directed to cover medical treatment and nursing care support to provide non-medical services such as daycare. This initiative sought to provide ongoing evaluation of the elderly and enhanced supportive care and financial assistance for family caregivers.38,39 Another national initiative was introduced in 2012 as the “Orange Plan” and was updated as the “New Orange Plan” in 2015, representing a renewed emphasis on supporting families and enabling patients with AD dementia to remain within the home environment for as long as possible,40 with further funding allocated to disease prevention and early detection and diagnosis.40,41 The long-term care insurance (LTCI) provision implemented by the Japanese government has sought to bring increasing care costs under control by utilizing tax revenues and insurance premiums to subsidize home-based care; nevertheless, costs continue to rise.42,43
Despite efforts to provide additional supportive services and to clarify diagnostic criteria (see the National Institute on Aging/Alzheimer’s Association 2011 diagnostic guidelines),44 evidence suggests that more than half of all individuals experiencing symptoms consistent with dementia are never evaluated by a medical professional nor do they receive a formal diagnosis of dementia, especially among patients with less severe memory and cognitive problems.45,46 Barriers to early detection exist, however, including diagnostic uncertainty (eg, difficulty differentiating AD dementia symptoms from symptoms associated with normal aging), stigma surrounding AD dementia, and lack of appropriately trained profressionals.47 Given the availability of treatments and care management options for AD dementia – as well as a robust pipeline of investigative therapeutic agents that depend upon the timely and accurate detection and diagnosis of symptoms – greater awareness, screening, and earlier diagnosis may provide an opportunity for patients to be more involved with decisions concerning their own care and for earlier intervention, with treatment or other support initiatives, which may ultimately lead to an improvement in the patient’s overall quality of life. However, this is not without its challenges, as evidence suggests that significant variation exists in the early signs of this disease among patients.48 It is, therefore, important to understand when and how symptoms are first noticed, particularly from the caregiver and patient perspective.
To help build a better understanding of the role of caregivers in the detection and diagnosis of AD dementia – a group that does not possess exposure to training or diagnostic guidelines – the current study utilized real-world survey data to examine the characteristics and experiences of patients with AD dementia as reported by their informal caregivers in Japan, particularly with regard to disease history and treatment patterns in this group of patients. Further, the relationships between disease severity level and the patient’s diagnosis, symptom identification, and treatment were explored. These results can provide insight into where patients and caregivers are, in terms of identifying disease progression, and inform efforts that could be used to promote earlier detection and diagnosis of AD dementia (especially, in a milder state), which may in turn help reduce this disease’s burden on – and costs to – society.
Methods
Sample
This study collected original data from caregivers identified in the 2012 and 2013 Japan National Health and Wellness Surveys (NHWS), with additional caregivers invited from the Lightspeed Research (LSR) opt-in ailment panels from Japan. Inclusion criteria were as follows: adults (≥18 years) and caring for an individual diagnosed with AD dementia (according to caregiver self-report). This study was reviewed and approved by the Pearl Institutional Review Board. Participants were asked to provide their informed consent before beginning this study via an online survey. The informed consent information provided study details, including the objectives of this study, risks/benefits, and contact information for any questions/concerns.
To maintain the focus of the study on informal caregivers, those who were receiving payment as a form of employment for caregiving duties were excluded as were those who did not provide informed consent. Informal caregivers may detect signs of AD dementia relatively early in the disease’s progression, whereas more formal caregivers (including those providing at-home nursing care and services for pay) may be caring for patients at more severe stages of the disease. Thus, informal caregivers may play a key role to help detect AD dementia at a relatively early stage. Details about NHWS and respondent recruitment are included in Laks et al12 and Goren et al.28
The current study population comprised 300 caregivers – 119 current caregivers who were recruited from the 2012 and 2013 NHWS and an additional 181 current caregivers who were recruited from the separate ailment panel source. Using an online survey, each caregiver provided survey responses for themselves as well as proxy measures on behalf of the AD dementia patient for whom they provided care. In total, 176 caregivers identified from the 2012 and 2013 NHWS entered the survey but were excluded because they were no longer providing care for an AD dementia patient. Reasons for discontinuing care included: patient deceased (n=76, 43.2%); patient receiving care at a hospital/health care facility (n=68, 38.6%, including n=2 who were also receiving at-home nursing care and services); and (exclusive of prior reasons noted) patient receiving at-home nursing care and services, someone else took over responsibilities, other, or none of the above (n=7, n=7, n=8, and n=10, respectively). The online survey protocol and questionnaire were reviewed and approved by Essex Institutional Review Board (Lebanon, NJ, USA), and all participants provided informed consent.
Measures
Sociodemographic and health characteristics and behaviors of caregivers
Demographic characteristics include: sex and age (for both patients and caregivers), marital status, employment, income, education, children in household, smoking, drinking alcohol, exercise, body mass index, health insurance, and change in employment status due to caregiving for the AD dementia patient.
Disease severity
Patient disease severity was assigned on the basis of LTCI levels reported by caregivers with respect to their AD dementia patients. The implementation of LTCI initiatives in Japan required that an accurate and detailed assessment of patients needed to be available to effectively assign care resources. The Government-Certified Disability Index (GCDI) is an 85-item measure which was developed to serve this purpose by providing a score from 0 to 5 that indicates the amount spent on services for a patient in each category and enables the severity of patient disease to be inferred. LTCI status was assessed and categorized according to the actual distribution of patients across levels (don’t know, no long-term nursing care insurance, support levels 1 or 2, or nursing care levels 1, 2, 3, 4, or 5). LTCI levels in the current study were trichotomized for analysis into categories reflecting increasing physical severity of AD dementia, mapping roughly onto the GCDI levels: 1) low severity – no long-term nursing care insurance, support levels 1 or 2, or level unknown; 2) medium severity – nursing care levels 1, 2, or 3; and 3) high severity – nursing care levels 4 or 5. These categorical groups were chosen to differentiate between patients who had relatively more special needs (in the medium- and high-severity groups – with the latter typically requiring institutionalization) and those who had slight impairments or difficulties with daily activities (low-severity group), as well as serving to combine small samples across categories to maximize statistical power for comparisons of interest.
Two additional measures were included to confirm the use of LTCI as a measure of AD dementia severity. First, the Short-Memory Questionnaire (SMQ)49,50 is an informant-based scale used to assess everyday memory problems. Caregivers rated the perceived frequency (“almost never” to “almost always”) of a patient’s memory difficulties and competencies in various situations. A total summary score of 40 or less suggests “disproportionate cognitive difficulties.” The SMQ is highly correlated with other measures of cognitive disease severity among Japanese patients.49,50 Second, caregivers also reported on patients’ level of dependency (no assistance, some assistance, or complete dependence) across 11 tasks in different domains that were generated for this study (eg, self-care, travel, health care, and finance). A total dependency score was calculated, ranging theoretically from 0 (“patient does not need assistance”) to 11 (“patient needs some assistance”) to 22 (“patient is completely dependent on me” across every task).
Patient disease history
Disease history variables include: years since AD dementia diagnosis and since AD dementia symptoms were first noticed, which symptoms were exhibited and who noticed them, diagnosing physician and evaluations, and prescriptions ever and currently taken for AD dementia.
Analysis
Descriptive results were examined for all study variables of interest, including numbers and percentages for categorical variables and means, SDs, medians, and both minimum and maximum values for continuous variables. The LTCI-based severity was trichotomized as described earlier, with low severity used as the reference category in bivariate analysis, to test whether medium AD dementia (where in-home care was still anticipated) was associated with different patterns than high-severity AD dementia (where patients were expected to be institutionalized due to the severity of their disease). Bivariate comparisons examined differences across disease severity (ie, low vs medium severity; low vs high severity) with chi-square and binomial proportion tests for categorical variables and one-way analysis of variance (ANOVA) tests for continuous variables. Bonferroni post hoc tests adjusted for multiple comparisons for all statistically significant omnibus ANOVA results.
Results
Patient severity
Three hundred caregivers were surveyed, and they provided information on their AD dementia patients. The LTCI was used as a surrogate measure of severity of illness, with 12.3% of caregivers (n=37 in the low-severity group) indicating that they did not know their patients’ LTCI (n=3), that their patients had no LTCI (n=15), or were at support level 1 (n=7) or 2 (n=12); 63.7% (n=191 in the medium-severity group) indicated that patients had nursing care level 1 (n=52), 2 (n=75), or 3 (n=64); and 24.0% (n=72 in the high-severity group) indicated that patients had nursing care level 4 (n=43) or 5 (n=29). SMQ total scores (with lower scores indicating greater difficulties with memory) ranged from 19 to 56, with a mean of 25.4 (SD=4.49) and median of 23, reflecting – along with the LTCI groups – a predominantly severe patient sample. The SMQ scores varied significantly across the three LTCI groups (F [2, 297]=22.1, p<0.001): high severity (mean [M] =23.3, SD=2.2) versus medium severity (M=25.4, SD=4.4) versus low (M=29.0, SD=6.1), p values<0.001 for all (Figure 1). Similarly, the mean patient dependency scores varied significantly across the LTCI severity groups (F [2, 297]=27.1, p<0.001): high severity (M=18.2, SD=5.4) versus medium severity (M=15.2, SD=4.2) versus low severity (M=11.7, SD=4.4), p values<0.001. These differences were largely driven by those in the high-severity group reporting complete dependency on caregivers for bathing/grooming/toileting and eating, as well as on logistic tasks (eg, travel and medication management).
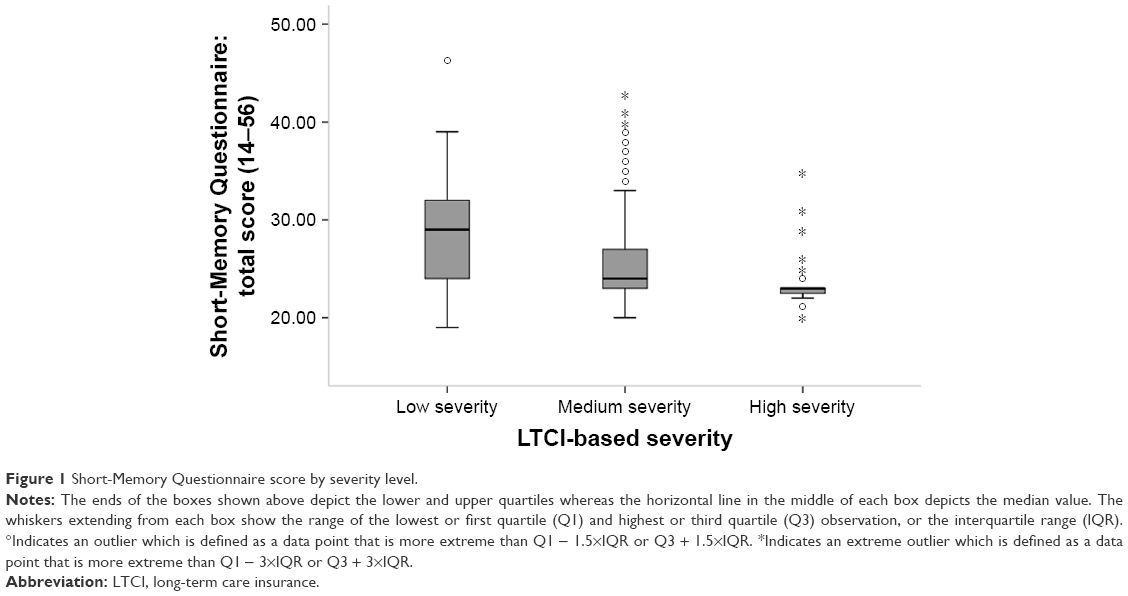 | Figure 1 Short-Memory Questionnaire score by severity level. |
Caregiver and patient demographics
There was no statistical difference for most of the demographics. Caregivers of high-severity patients were more likely to change their employment status due to caregiving, compared with caregivers of low-severity patients (31.9% vs 13.5%, p<0.05). Similarly, patients were more likely to be 90 years old or older in the medium-severity (22.0%) and high-severity (31.9%) LTCI groups as compared with the low-severity group (5.4%) (p values=0.060 and 0.003, respectively; Table 1).
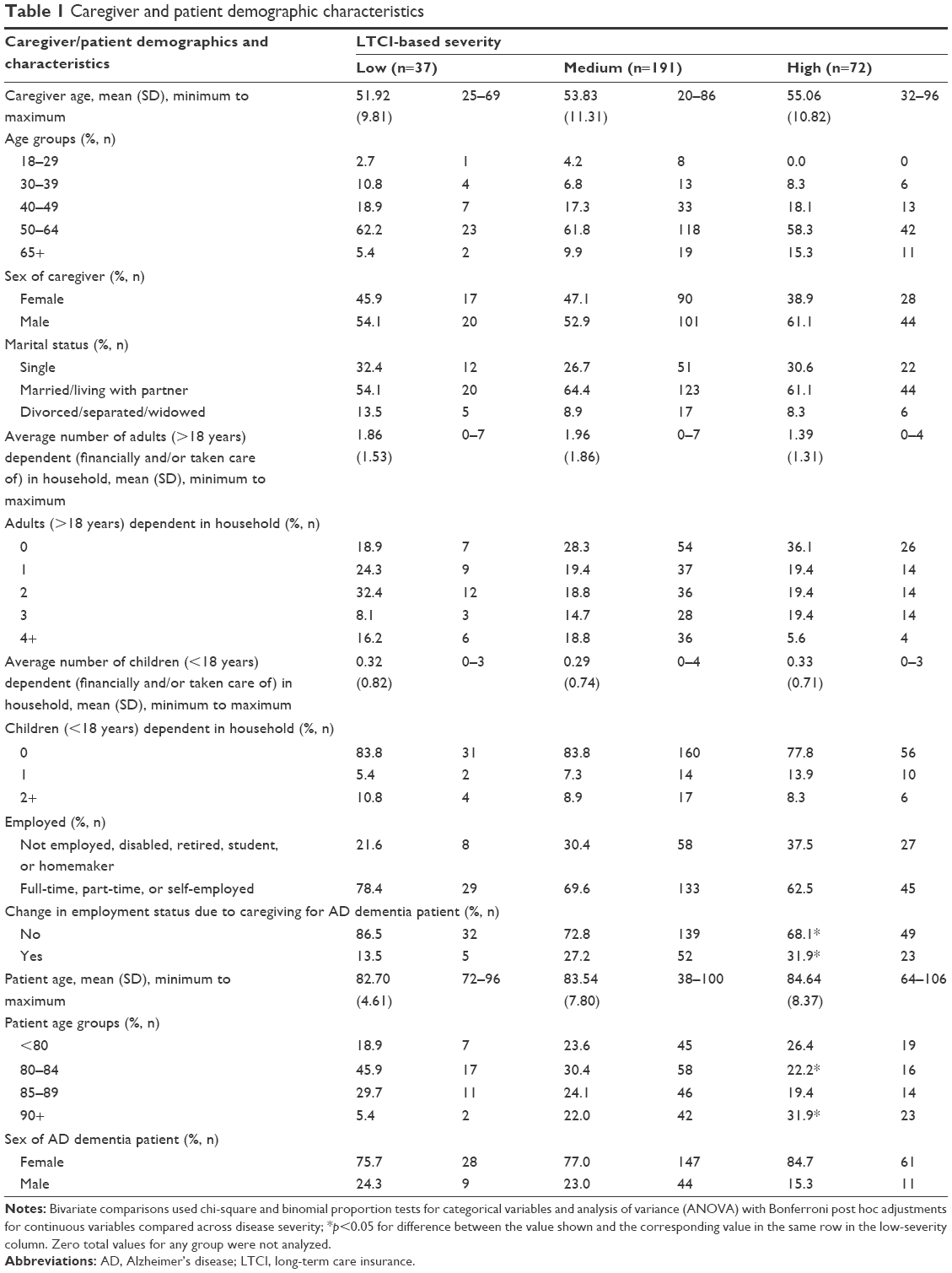 | Table 1 Caregiver and patient demographic characteristics |
Caregiving involvement/intensity
Among all caregivers, 60.3% were the primary caregivers with sole or shared responsibilities, and 39.7% were secondary caregivers; however, there was no statistical difference across AD dementia severity for the caregiving role (Table 2). The average number of hours of care per day varied significantly across AD dementia severity (F [2, 297]=11.9, p<0.001). Caregivers devoted a significantly greater number of average hours of care per day for high-severity (M=16.2, SD=8.1) and medium-severity (M=12.6, SD=7.7) patients as compared with low-severity (M=8.8, SD=7.1) patients (p values=0.020 and <0.001), respectively, as well as other indicators of increasing caregiver involvement across groups, and more years providing care to the patient (Figure 2 and Table 2).
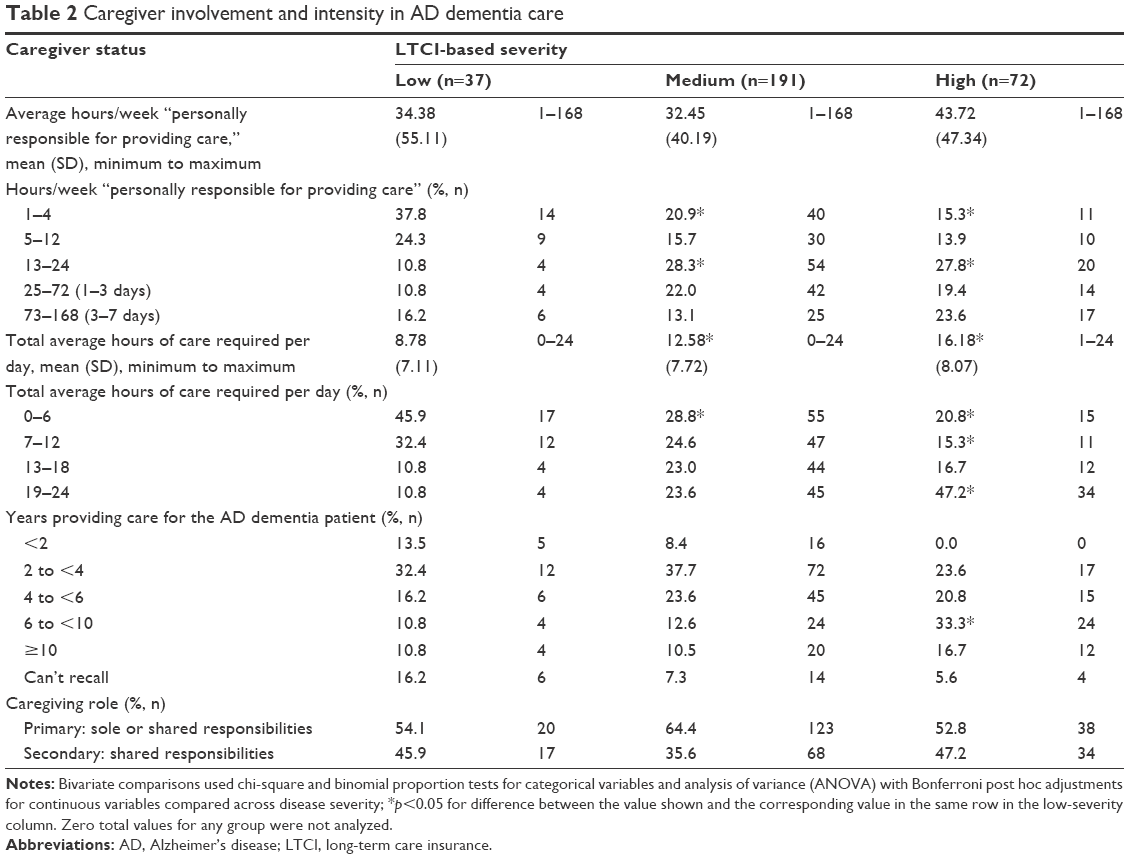 | Table 2 Caregiver involvement and intensity in AD dementia care |
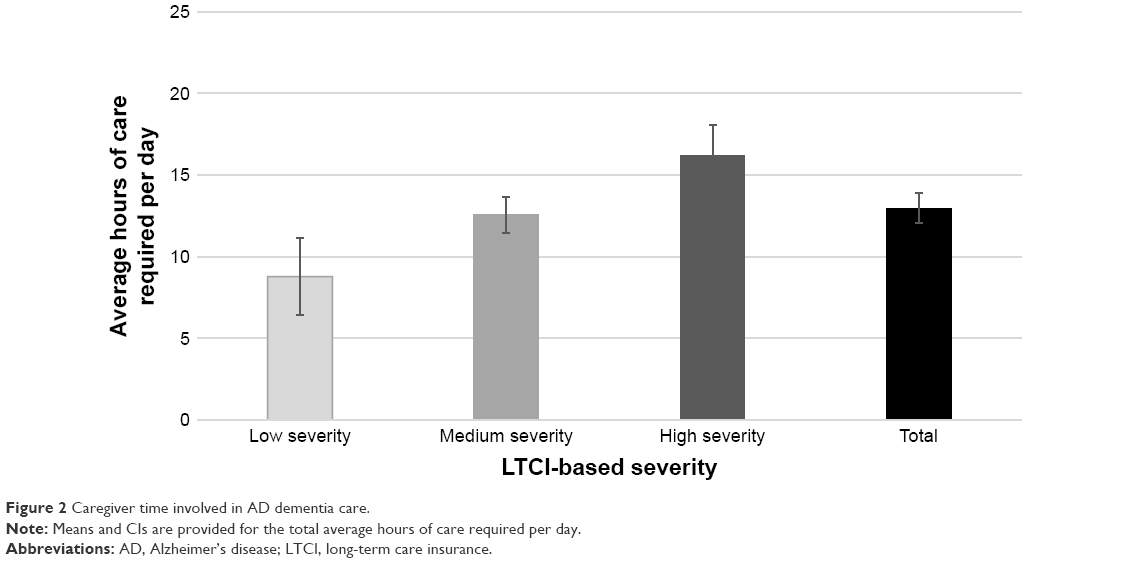 | Figure 2 Caregiver time involved in AD dementia care. |
Disease history
Significantly more patients had been diagnosed between 2 and <4 years prior to the study (13.9%) in the high-severity versus low-severity group (p<0.001), with 0% of patients diagnosed <2 years before the study (Table 3). In addition, a higher proportion of patients had AD dementia symptoms noticed around 10 years or farther prior (18.1%) in the high-severity group versus the low-severity (2.7%) group (p<0.001); however, no significant differences were observed between the low-severity and medium-severity groups (8.4%; p=0.135).
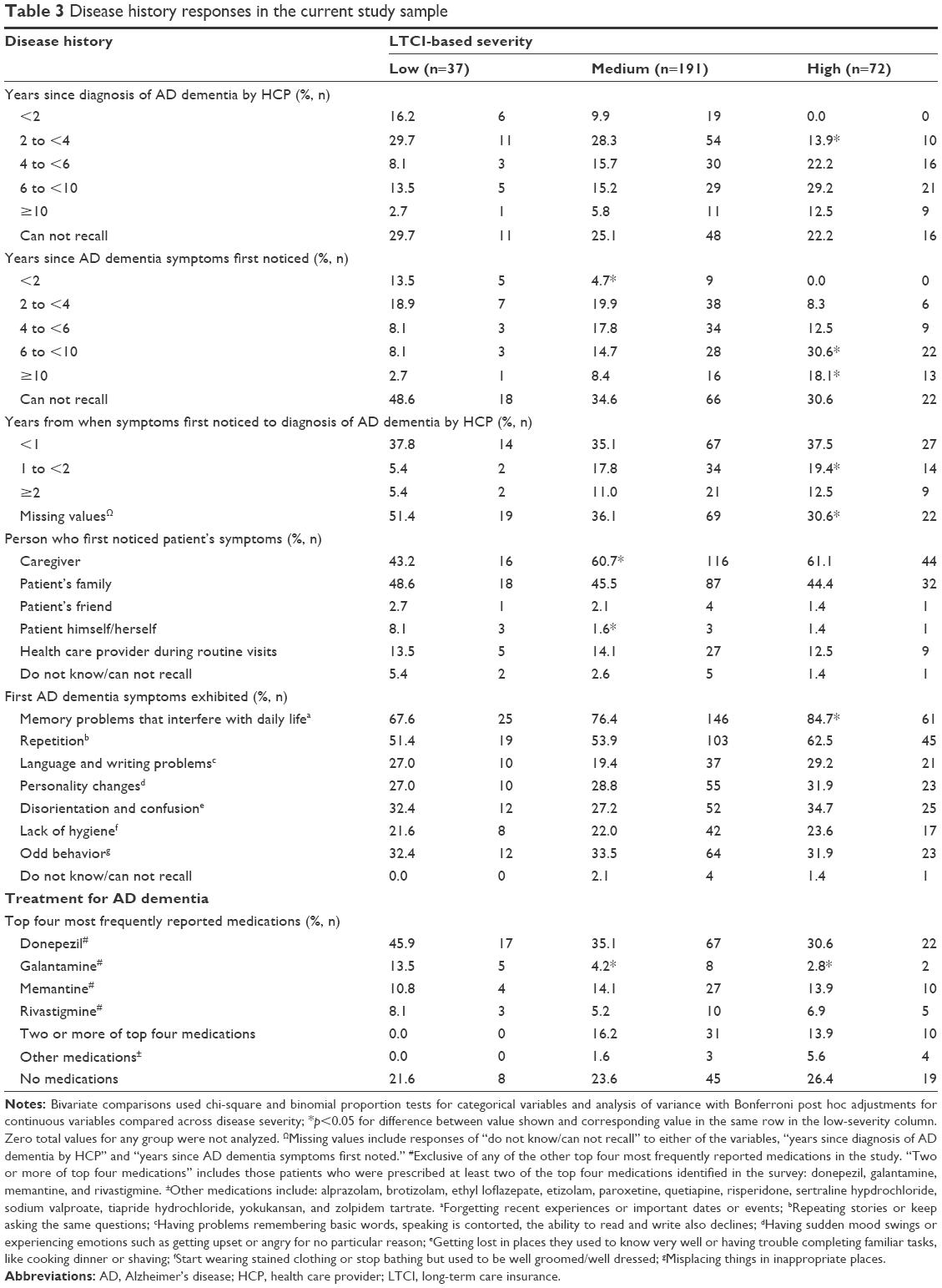 | Table 3 Disease history responses in the current study sample |
Most often, symptoms of AD dementia were first detected by the caregiver (58.7%) or the patient’s family (45.7%), and rarely noticed by the patient himself/herself (2.3%). However, in 13.7% of cases, symptoms were first detected by a health care provider during a routine visit. Memory problems were the most frequent first symptom exhibited (77.3%), followed by repetition (55.7%).
In the medium-severity versus low-severity groups, significantly more caregivers (60.7% vs 43.2%, p=0.049) and fewer patients themselves (1.6% vs 8.1%, p=0.023) were the ones who first noticed the patient’s symptoms. Although the proportions were similar across the medium-severity and high-severity groups, the high-severity group did not differ significantly from the low-severity group. Memory problems were significantly more likely to have been the first AD dementia symptoms exhibited in the high-severity LTCI group (84.7%) compared with the low-severity LTCI group (67.6%). This finding may be driven by a few possible explanations. For example, this result may be an artifact of memory bias. Caregivers of more severe patients may falsely recall detecting more symptoms than those caring for less severe patients (eg, may falsely recall patient’s memory problems). Furthermore, in this study, full-time/part-time employment status tended to be more frequent among caregivers of patients with less severe AD dementia. As memory loss is a subtler symptom of AD dementia compared with symptoms such as repetition, personality changes, and odd behaviors, caregivers of less severe patients may have had fewer opportunities to detect memory loss symptoms given their employment status. There were no significant differences in terms of who first diagnosed patients across severity groups, nor in the evaluations used to confirm diagnosis.
Disease evaluation
Patients were most commonly diagnosed by a neurologist (41.0%), primary care physician or internist (28.3%), or psychiatrist (21.3%). The evaluation to confirm diagnosis most commonly involved brain imaging (65.3%) or a mental status test (62.3%).
AD dementia treatment
The majority of patients (73.7%) were currently taking a symptomatic treatment for AD dementia such as acetylcholinesterase inhibitors (donepezil, galantamine, and rivastigmine) or memantine, regardless of disease severity. Some of the medium- and high-severity patients were on more than one of these symptomatic treatments concurrently (16.2% and 13.9%, respectively), whereas none of the low-severity patients were concurrently on more than one of these treatments (Table 3). Galantamine was used significantly more frequently as the current medication for patients in the low-severity patient group (13.5%) compared with the medium-severity (4.2%) and high-severity groups (2.8%) (Table 3).
Discussion
In the current study, the vast majority of caregivers surveyed had first noticed AD dementia symptoms in the person they were caring for at least 2 years before the survey, if they remembered the timing at all. In the majority (58.7%) of these cases, symptoms were noticed by the caregiver, whereas the patient’s family also noticed symptoms in many cases (45.7%), compared with only 13.7% noticed by a health care provider. Memory problems were the first symptom exhibited most frequently (77.3%), indicating a potential early signal for follow-up testing to rule out reversible causes or other diagnoses. These findings suggest that caregivers and patients’ families are a useful source to facilitate early identification, diagnosis, and treatment of patients with AD dementia. The inclusion of patients with mild disease in the current study can help guide early detection efforts, which are particularly crucial in countries such as Japan with an aging population and an increasing degree of societal burden associated with AD dementia.
The majority of patients were on a symptomatic treatment for AD dementia and some were taking more than one treatment at a time; moreover, these patients were likely to be in a more severe state of disease necessitating such treatment, and this was reflected by the long-term nursing care level. Greater disease severity was associated with several factors. High-severity patients were older, had been diagnosed for a longer duration, more frequently reported memory problems as the first symptoms noticed, and required more hours of care per day, compared with low-severity patients. Given the current understanding of when the disease pathology first develops, as well as a pipeline of potential new therapies focused on use earlier in the trajectory of disease, early detection, diagnosis, and initiation of treatment is essential; disease-modifying therapy may be best suited for patients earlier in the disease course, prolonging the duration of time that the patient can remain independent and delaying the progression to moderate and severe states, which in turn can enable patients to be cared for longer at home.51
As noted earlier, the Japanese government has implemented a range of initiatives to promote home-based care for AD dementia patients and enable them to remain as members of the community, potentially in contrast with other health care systems that have a greater acceptance of institutionalization.38–41 Given these social and cultural goals to enhance home-based care, increased formal assistance programs can support caregivers and reduce their caregiving responsibilities, with corresponding reductions in their overall burden. Despite such efforts to curtail costs through iterations of the New Orange Plan40 and the introduction of supportive measures to enable patients to remain at home, the costs associated with AD dementia care in Japan remain substantial.
The current study forms part of a growing empirical focus on the care trajectory of those diagnosed with a chronic disease. In a recent Canadian study, Carpentier et al utilized a qualitative methodology to explore the trajectory of care among 60 caregivers and their patients with AD dementia.52 The authors noted that many caregivers initiated care through past experience with dementia, whereas other families who were not in close contact or without this past experience required a “watershed” moment to initiate care. Other caregivers reported the initial referral from a health professional upon noticing memory problems, consistent with the early signs reported in the current study. In an earlier study, Devier et al also reported that a decline in memory was the initial symptom reported by those with mild cognitive impairment, and that memory problems were predictive of an eventual diagnosis of AD dementia.53 The current study provides further insight into the disease course of Japanese patients and caregivers.
Strengths and limitations
The current study utilized methodology that enabled a large-scale representative sample to be surveyed. The online survey format, however, limits reporting by patients and family members who are less comfortable with, or lack access to, online technology, or those who are less able to participate due to caregiving duties or health burden. This may be noteworthy given the hyper-aging nature of Japan society and, thus, many caregivers are also elderly. Further, only AD dementia patients for whom care was reported as being provided by informal caregivers were included, leading to an underrepresentation of patients receiving institutionalized care. This may have led to a sample with a less severe disease progression compared with the general AD dementia patient population. Caution is thus warranted in generalizing the current study results beyond those who participated.
Despite the limitations noted herein, the online study format resulted in a large representation of relatively young, employed informal caregivers. These individuals are often expected to maintain dual roles, including as active members of working society and supportive care for their family members. Given this dual-role status, such caregivers may feel increased pressure to maintain their own physical and mental health, and thus it may be especially meaningful to gain insight into the experiences of this subgroup, and to utilize this information to develop and implement effective supportive care services.
There were differences found in the demographic characteristics of those enrolled in this study compared with the general Japanese population, with those enrolled reporting being generally younger (10.7% vs 26.7% >65 years), male (55% vs 48.7%), and socioeconomically advantaged (69% vs 58.6% employed) compared with national estimates.54 These differences may suggest that those enrolled had greater motivation, physical ability, and Internet access than the population at large. Furthermore, there was a high number of patients with severe dementia in the current study, possibly because people did not become caregivers until the patients’ AD dementia progressed to a severe state. There was a high number of male caregivers, especially relative to the percentage of female patients (78.7%), contrasting previous work that examined AD dementia caregivers in which female caregivers were the majority.12
The current study was cross-sectional by design and, thus, precludes longitudinal assessment and the consequent ability to draw causal relationships between study variables. Further, self-report assessments have inherent limitations in that they rely on participants’ memory of events. In the current study, for example, reports of initial symptomatology may be biased toward events that were of particular interest to caregivers. Further, more than one third of caregivers surveyed could not recall when AD dementia symptoms first appeared, suggesting that in these cases other people (eg, other family members or health care providers) may have noticed them first. Such information was not collected as part of the current study and provides fertile ground for further research.
Conclusion
The current findings suggest that caregivers and family members play an integral role in promoting the early identification of symptoms, diagnosis, and treatment of AD dementia. Patients with AD dementia who required informal care were generally identified and diagnosed at least 2 years before the survey, with caregivers being the ones most frequently having detected the symptoms; memory problems were most frequently the first symptoms noticed by caregivers. These results provide novel insight into the diagnosis, treatment, and disease history of AD dementia in Japan, and how experiences may differ based on disease severity. Given that past research has largely focused on those with moderate and severe disease, the inclusion of individuals with mild disease provides important information in guiding efforts for early detection and diagnosis of AD dementia.
This research provides baseline data on symptom presentation, diagnosis, disease severity, and caregiver burden in patients with AD dementia. The potential benefits associated with early and accurate detection and diagnosis of AD dementia reinforce the importance of gaining greater insight into the trajectory of the disease and caregiving experience, and raising awareness among patients, family members, and the medical community at large. Caregivers and family members are a useful place to start in terms of helping get patients identified early, diagnosed, and treated whereas, at the same time, the findings underscore the importance of increasing identification of AD dementia by patients themselves and by health care providers. Early identification of symptoms, and diagnosis, will be important to facilitate the use of new interventions that promise to slow or halt the progression of AD dementia which, in turn, have the potential to moderate the level of caregiving needed and potentially delay institutionalization.
Acknowledgments
The authors acknowledge Errol J Philip, PhD, for assistance with literature review and writing, and Colleen M Carpinella, PhD, and Michael J Doane, PhD, of Kantar Health, for their assistance with writing, analysis, and interpretation. This study, the manuscript writing services, and publication fees were funded by Eli Lilly and Company (Indianapolis, IN, US). Results contained in this paper were presented at the 32nd International Conference of Alzheimer’s Disease International. The presentation was entitled: “Understanding Symptom Presentation, Recognition and Diagnosis for People with Alzheimer’s Disease in Japan.”
Author contributions
All authors contributed to study design, data analysis, and drafting and revision of the paper, and all authors agree to be accountable for all aspects of the work. Amir Goren conducted the statistical analyses.
Disclosure
William Montgomery, Tomomi Nakamura, Kaname Ueda, and Kristin Kahle-Wrobleski were full-time employees of Eli Lilly and Company at the time of this study. Amir Goren is an employee of Kantar Health, which conducted this study with funding from Eli Lilly. The authors report no other conflicts of interest in this work.
References
Brookmeyer R, Johnson E, Ziegler-Graham K, Arrighi HM. Forecasting the global burden of Alzheimer’s disease. Alzheimers Dement. 2007;3(3):186–191. | ||
Carter R. Addressing the caregiving crisis. Prev Chronic Dis. 2008;5(1):A02. | ||
Sekita A, Ninomiya T, Tanizaki Y, et al. Trends in prevalence of Alzheimer’s disease and vascular dementia in a Japanese community: the Hisayama Study. Acta Psychiatr Scand. 2010;122(4):319–325. | ||
Yamada T, Hattori H, Miura A, Tanabe M, Yamori Y. Prevalence of Alzheimer’s disease, vascular dementia and dementia with Lewy bodies in a Japanese population. Psychiatry Clin Neurosci. 2001;55(1):21–25. | ||
Dodge HH, Buracchio TJ, Fisher GG, et al. Trends in the prevalence of dementia in Japan. Int J Alzheimers Dis. 2012;2012:956354. | ||
Ninomiya, et al. Report of “A Study on the Future Estimates of the Elderly Population of Dementia in Japan” (direct translation, not official). 2015 March. Available from: https://mhlw-grants.niph.go.jp/niph/search/Download.do?nendo=2014&jigyoId=141031&bunkenNo=201405037A_upload&pdf=201405037A0003.pdf. Accessed June 19, 2018. Japanese. | ||
Duthey B. Background paper 6.11: Alzheimer disease and other dementias. 2013. Available from: http://www.who.int/medicines/areas/priority_medicines/BP6_11Alzheimer.pdf. Accessed June 7, 2016. | ||
Asada T. [Prevalence of dementia in Japan: past, present and future]. Rinsho Shinkeigaku. 2012;52(11):962–964. Japanese [with English abstract]. | ||
Chaudhuri JD, Das S. The role of caregivers in the management of Alzheimer’s disease: examples from Asian Countries. Sultan Qaboos Univ Med J. 2006;6(2):11–18. | ||
National Institute on Aging. Alzheimer’s Disease Fact Sheet. 2015. Available from: http://www.nia.nih.gov/alzheimers/publication/alzheimers-disease-fact-sheet. Accessed October 15, 2015. | ||
Bergvall N, Brinck P, Eek D, et al. Relative importance of patient disease indicators on informal care and caregiver burden in Alzheimer’s disease. Int Psychogeriatr. 2011;23(1):73–85. | ||
Laks J, Goren A, Dueñas H, Novick D, Kahle-Wrobleski K. Caregiving for patients with Alzheimer’s disease or dementia and its association with psychiatric and clinical comorbidities and other health outcomes in Brazil. Int J Geriatr Psychiatry. 2016;31(2):176–185. | ||
Fuller-Jonap F, Haley WE. Mental and physical health of male caregivers of a spouse with Alzheimer’s disease. J Aging Health. 1995;7(1):99–118. | ||
Schulz R, Beach SR. Caregiving as a risk factor for mortality: the Caregiver Health Effects Study. JAMA. 1999;282(23):2215–2219. | ||
Kolanowski AM, Fick D, Waller JL, Shea D. Spouses of persons with dementia: their healthcare problems, utilization, and costs. Res Nurs Health. 2004;27(5):296–306. | ||
Lu YF, Wykle M. Relationships between caregiver stress and self-care behaviors in response to symptoms. Clin Nurs Res. 2007;16(1):29–43. | ||
Beeson R, Horton-Deutsch S, Farran C, Neundorfer M. Loneliness and depression in caregivers of persons with Alzheimer’s disease or related disorders. Issues Ment Health Nurs. 2000;21(8):779–806. | ||
Langa KM, Chernew ME, Kabeto MU, et al. National estimates of the quantity and cost of informal caregiving for the elderly with dementia. J Gen Intern Med. 2001;16(11):770–778. | ||
Arai A, Matsumoto T, Ikeda M, Arai Y. Do family caregivers perceive more difficulty when they look after patients with early onset dementia compared to those with late onset dementia? Int J Geriatr Psychiatry. 2007;22(12):1255–1261. | ||
Arai Y. [Medical and nursing care of dementia patients. Nursing burden of family caregivers]. Nihon Naika Gakkai Zasshi. 2005;94(8):1548–1554. Japanese [with English abstract]. | ||
Arai Y, Kumamoto K, Washio M, Ueda T, Miura H, Kudo K. Factors related to feelings of burden among caregivers looking after impaired elderly in Japan under the Long-Term Care insurance system. Psychiatry Clin Neurosci. 2004;58(4):396–402. | ||
Arai Y, Zarit SH. Exploring strategies to alleviate caregiver burden: effects of the National Long-Term Care insurance scheme in Japan. Psychogeriatrics. 2011;11(3):183–189. | ||
Kurasawa S, Yoshimasu K, Washio M, et al. Factors influencing caregivers’ burden among family caregivers and institutionalization of in-home elderly people cared for by family caregivers. Environ Health Prev Med. 2012;17(6):474–483. | ||
Sasaki M, Arai Y, Kumamoto K, Abe K, Arai A, Mizuno Y. Factors related to potentially harmful behaviors towards disabled older people by family caregivers in Japan. Int J Geriatr Psychiatry. 2007;22(3):250–257. | ||
Hayashi S, Terada S, Nagao S, et al. Burden of caregivers for patients with mild cognitive impairment in Japan. Int Psychogeriatr. 2013;25(8):1357–1363. | ||
Muraki I, Yamagishi K, Ito Y, et al. Caregiver burden for impaired elderly Japanese with prevalent stroke and dementia under long-term care insurance system. Cerebrovasc Dis. 2008;25(3):234–240. | ||
Montgomery W, Ueda K, Jorgensen M, Stathis S, Cheng Y, Nakamura T. Epidemiology, associated burden, and current clinical practice for the diagnosis and management of Alzheimer’s disease in Japan. Clinicoecon Outcomes Res. 2018;10:13–28. | ||
Goren A, Montgomery W, Kahle-Wrobleski K, Nakamura T, Ueda K. Impact of caring for persons with Alzheimer’s disease or dementia on caregivers’ health outcomes: findings from a community based survey in Japan. BMC Geriatr. 2016;16(1):122. | ||
Cassidy T. Benefit finding through caring: the cancer caregiver experience. Psychol Health. 2013;28(3):250–266. | ||
Cheng ST, Lau RW, Mak EP, Ng NS, Lam LC. Benefit-finding intervention for Alzheimer caregivers: conceptual framework, implementation issues, and preliminary efficacy. Gerontologist. 2014;54(6):1049–1058. | ||
Kim Y, Schulz R, Carver CS. Benefit-finding in the cancer caregiving experience. Psychosom Med. 2007;69(3):283–291. | ||
Lum HD, Lo D, Hooker S, Bekelman DB. Caregiving in heart failure: relationship quality is associated with caregiver benefit finding and caregiver burden. Heart Lung. 2014;43(4):306–310. | ||
Wimo A, Reed CC, Dodel R, et al. The GERAS Study: a prospective observational study of costs and resource use in community dwellers with Alzheimer’s disease in three European countries – study design and baseline findings. J Alzheimers Dis. 2013;36(2):385–399. | ||
Darbà J, Kaskens L, Lacey L. Relationship between global severity of patients with Alzheimer’s disease and costs of care in Spain; results from the co-dependence study in Spain. Eur J Health Econ. 2015;16(8):895–905. | ||
López-Pousa S, Garre-Olmo J, Turon-Estrada A, et al. Análisis de los costes de la enfermedad de Alzheimer en función del deterioro cognitivo y funcional [Cost relation between severity of Alzheimer’s disease and cognitive and functional impairment]. Med Clin (Barc). 2004;122(20):767–772. Spanish [with English abstract]. | ||
Zencir M, Kuzu N, Beşer NG, Ergin A, Catak B, Sahiner T. Cost of Alzheimer’s disease in a developing country setting. Int J Geriatr Psychiatry. 2005;20(7):616–622. | ||
Shikimoto R, Sado M, Mimura M. [The social costs of dementia in Japan: focusing on the informal care cost]. Brain Nerve. 2016;68(8):939–944. Japanese [with English abstract]. | ||
Sugino H, Watanabe A, Amada N, et al. Global trends in Alzheimer disease clinical development: increasing the probability of success. Clin Ther. 2015;37(8):1632–1642. | ||
Social Welfare Bureau. Long-Term Care Insurance Program. 2016. Available from: http://www.city.osaka.lg.jp/contents/wdu020/fukushi/english/kaigo/03_kaigohoken_seido.html. Accessed September 15, 2016. | ||
Awata S. [Medical services for dementia in the Comprehensive Strategy to Accelerate Dementia Measures (New Orange Plan)]. Nihon Rinsho. 2016;74(3):499–504. Japanese [with English abstract]. | ||
Nakanishi M, Nakashima T. Features of the Japanese national dementia strategy in comparison with international dementia policies: how should a national dementia policy interact with the public health- and social-care systems? Alzheimers Dement. 2014;10(4):468–476.e3. | ||
Yong V, Saito Y. National long-term care insurance policy in Japan a decade after implementation: some lessons for aging countries. Ageing Int. 2012;37(3):271–284. | ||
Matsuda S, Yamamoto M. Long-term care insurance and integrated care for the aged in Japan. Int J Integr Care. 2001;1:e28. | ||
Ihara R. [New diagnostic guidelines for Alzheimer’s disease by NIA/AA]. Nihon Rinsho. 2016;74(3):386–394. Japanese [with English abstract]. | ||
Kotagal V, Langa KM, Plassman BL, et al. Factors associated with cognitive evaluations in the United States. Neurology. 2015;84(1):64–71. | ||
Alzheimer’s Disease International. World Alzheimer Report 2011: the Benefits of Early Diagnosis and Intervention. London: Alzheimer’s Disease International; 2011. | ||
Dubois B, Padovani A, Scheltens P, Rossi A, Dell’Agnello G. Timely diagnosis for Alzheimer’s disease: a literature review on benefits and challenges. J Alzheimers Dis. 2016;49(3):617–631. | ||
Barnes J, Dickerson BC, Frost C, Jiskoot LC, Wolk D, van der Flier WM. Alzheimer’s disease first symptoms are age dependent: evidence from the NACC dataset. Alzheimers Dement. 2015;11(11):1349–1357. | ||
Koss E, Patterson MB, Ownby R, Stuckey JC, Whitehouse PJ. Memory evaluation in Alzheimer’s disease. Caregivers’ appraisals and objective testing. Arch Neurol. 1993;50(1):92–97. | ||
Maki N, Ikeda M, Hokoishi K, et al. [Japanese version of the Short-Memory Questionnaire: memory evaluation in Alzheimer’s disease]. No To Shinkei. 1998;50(5):415–418. Japanese [with English abstract]. | ||
Porter CN, Miller MC, Lane M, Cornman C, Sarsour K, Kahle-Wrobleski K. The influence of caregivers and behavioral and psychological symptoms on nursing home placement of persons with Alzheimer’s disease: a matched case-control study. SAGE Open Med. 2016;4:2050312116661877. | ||
Carpentier N, Bernard P, Grenier A, Guberman N. Using the life course perspective to study the entry into the illness trajectory: the perspective of caregivers of people with Alzheimer’s disease. Soc Sci Med. 2010;70(10):1501–1508. | ||
Devier DJ, Villemarette-Pittman N, Brown P, et al. Predictive utility of type and duration of symptoms at initial presentation in patients with mild cognitive impairment. Dement Geriatr Cogn Disord. 2010;30(3):238–244. | ||
Statistics Bureau. Statistics Japan. Tokyo: Ministry of Internal Affairs and Communications; 2016. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.