")
Back to Journals » Patient Preference and Adherence » Volume 9
Detection and correlation analysis of serum cytokines in non-small-cell lung cancer patients with bone and non-bone metastases
Authors Sun Y, Ai X, Shen S, Gu L, Lu S
Received 14 April 2015
Accepted for publication 30 May 2015
Published 12 August 2015 Volume 2015:9 Pages 1165—1169
DOI https://doi.org/10.2147/PPA.S86605
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Naifeng Liu
Yingjia Sun, Xinghao Ai, Shengping Shen, Linping Gu, Shun Lu
Lung Tumor Clinical Medical Center, Shanghai Chest Hospital, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
Objective: To detect and analyze 13 cytokines that may be related to bone metastasis in the serum of non-small-cell lung cancer (NSCLC) patients with bone metastases and NSCLC patients with non-bone metastases.
Patients and methods: The Luminex LiquiChip system was used to detect the concentration of 13 cytokines that may be related to bone metastasis in the serum of 30 NSCLC patients with bone metastases and 30 with non-bone metastases.
Results: The concentration of insulin-like growth factor binding protein-3 (IGFBP-3) in the serum of NSCLC patients with bone metastases was obviously higher than in non-bone metastasis patients (P=0.014). The serum concentration of other cytokines showed no significant difference (P>0.05) between the two groups. The concentration of IGFBP-3 in the serum of the bone metastasis group was positively correlated to VEGF concentration (r=0.804, P=0.009) and monocyte chemotactic protein 1 (MCP-1) concentration (r=0.785, P=0.012), but had no correlation to other factors (P>0.05). No correlation was found between serum concentrations of cytokines in bone metastasis. Concentration of IGFBP-3 in the serum of bone metastasis patients was positively correlated to the presence or absence of pain at diagnosis (r=0.701, P=0.036) and performance status (PS) score (r=0.670, P=0.048), and correlated with the number of bone metastases, sex, age, pathological characteristics, T stage, and N stage (P>0.05).
Conclusion: The findings of this study suggest important clinical implications to detect the concentration of IGFBP-3 in the serum of lung cancer patients so as to evaluate the diagnosis and degree of bone metastasis. Concentration of IGFBP-3 in the serum of bone metastasis patients was positively correlated to concentration of VEGF and MCP-1, which may be highly relevant for the development of new treatments for bone metastasis of lung cancer.
Keywords: metastatic lung cancer, cytokine, liquichip
Introduction
The National Central Cancer Registry of China annual report in 2012 showed that lung cancer ranks first among all cancers in the People’s Republic of China in terms of morbidity and mortality.1 It is difficult to detect, and approximately 50% of the diagnoses are made at the late stage (stage IV). Bone metastasis is one of the major blood metastases.2 With the development of treatment methods and techniques, the median survival time of lung cancer patients in late stages has gradually extended to approximately 1 year.3
The incidence of metastasis of lung cancer is 30%–40%. One study showed that 50% of lung cancer patients were found with bone metastases after death.4 Forty-six percent of lung cancer patients with bone metastases had skeletal-related events (SREs).5 Once lung cancer patients with bone metastasis have SRE, their survival will be significantly shortened. One study has shown that the median survival of lung cancer patients with bone metastases is only approximately 6–10 months.6 If a patient is found with a severe SRE, such as hypercalcemia, pathologic fractures, spinal cord compression, or other complications, his or her life will be further shortened.6,7 Therefore, during the control of primary disease, it is particularly important to prevent and treat bone metastasis and bone-related events.
Bone metastasis of lung cancer is mainly due to resorption caused by osteoclasts, mostly presenting as osteolytic lesions.8 Lung cancer cells move to the bone and release soluble mediators, activating osteoclasts and osteoblasts. Cytokines released by osteoclasts further promote tumor cells to secrete osteolysis media, thus forming a vicious cycle.
In the present study, we analyzed the 13 cytokines that may be related to bone metastasis in the serum of non-small-cell lung cancer (NSCLC) patients with bone metastases and those with non-bone metastases, aiming to evaluate the correlation between and clinical applications of the cytokines and bone metastasis.
Patients and methods
Patients
This study was approved by an ethics committee of Shanghai Chest Hospital, and all participants signed a consent form. NSCLC patients were divided into two groups: those with bone metastasis and those with non-bone metastasis. The two groups had no significant statistical difference in age, sex, smoking history, TNM stage, or pathological type, thus were comparable.
Lung cancer with bone metastasis group
Between April 2008 and July 2008, Shanghai Chest Hospital diagnosed 30 NSCLC patients with multiple bone metastases, consisting of 15 males and 15 females with an average age of 54.5 years. Fifteen cases had a smoking index ≥400 pcs/year (where pcs is number of cigarettes smoked), and 15 had a smoking index <400 pcs/year. There were 15 cases of adenocarcinoma, 12 of squamous cell carcinoma, and three of poorly differentiated carcinoma; all carcinoma types had a TNM stage of IV.
Lung cancer with non-bone metastasis group
Between April 2008 and July 2008, Shanghai Chest Hospital diagnosed 30 NSCLC patients with non-bone metastasis. The TNM stage for all non-bone metastasis NSCLC cases was IIIa–IV, and 18 males and 12 females with an average age of 56.4 years were included. The smoking index was >400 pcs/year in 15 cases and <400 pcs/year in 15 cases. There were 21 cases of adenocarcinoma, six of squamous cell carcinoma, and three of poorly differentiated carcinoma.
Patient inclusion criteria
The pathological diagnosis of NSCLC had no treatment (chemotherapy, radiotherapy, or targeted therapy) before taking blood samples.
Patients with bone metastases had systemic multiple bone transfer (more than two). Entry of patients with distant metastasis was avoided. Criteria for diagnosis of bone metastasis were prompt radiation bone emission computed tomography or positron emission tomography uptake and computed tomography or magnetic resonance imaging to verify the existence of bone destruction. Exclusion criteria were history of malignancy, immune inhibitors in acute and chronic bone-related diseases, autoimmune diseases, and long-term use of glucocorticoids.
Methods
Plasma collection and preservation
Three milliliters of cubital vein blood was collected while the patient was experiencing limosis in the morning, left standing for 1 hour at 4°C, and centrifuged for 20 minutes; 0.5 mL of the upper serum was collected and stored at −80°C for later testing.
Test items
The 13 cytokines in serum that may be related to bone metastasis were tested and divided into two types based on different functions. The first type was homing chemokines and cytokines that make the tumor cells migrate to specific tissues, including a matrix derivative factor (SDF-1), an irregular chemoattractant protein (fractalkine), interferon-inducible protein 10 (IP-10), monocyte chemotactic protein-1 (MCP-1), interferon (IFN), interleukin (IL)-6, IL-10, IL-17α, and IL-23. The other type was growth factors that, after exfoliated cell adhesion, transfer tissue and induce tumor cells to continue to grow, including platelet-derived growth factor-αα (PDGF-αα), fibroblast growth factor (FGF), insulin-like growth factor binding protein-3 (IGFBP-3), and vascular endothelial growth factor (VEGF).
Detection methods
The Luminex detection method, which is based on LiquiChip technology, was employed using a kit purchased from Guangzhou Yi Shan Biotechnology Co. (Guangzhou, People’s Republic of China), and detection equipment for the Luminex 200 (Luminex Co. Ltd., USA), according to the kit instructions, to determine the concentration of serum cytokines (pg/mL).
Statistical analysis
All data were processed using the SPSS 13.0 statistical software package. Quantitative data analysis was conducted using t-tests, and analysis of variance (ANOVA) was used to identify the statistical significance of differences among groups. Statistical significance was evaluated using Student’s t-test for the single or multiple comparisons of experimental groups. Correlation analysis was performed using Pearson’s or Spearman’s correlation. P>0.05 indicated no significant difference; P<0.05 was considered a significant difference; and P<0.01 indicated a very significant difference.
Results
A comparison of cytokine concentrations between the two groups of patients is shown in Table 1. The results show that both groups had a high expression of PDGF-αα, IGFBP-3, IP-10, IFN, and MCP-1, but SDF-1, fractalkine, FGF, and serum IL-23 showed no detected expression in either serum group (the detection range of IL-23 is 48.8–50,000 pg/mL, and that of the other cytokines is 9.77–10,000 pg/mL). Statistical analysis showed that the expression of IGFBP-3 was significantly different (P=0.014) between the bone and non-bone metastasis groups; IFN and IL-6 expression were nearly statistically different between the two groups, with P=0.075 and P=0.073, respectively. Expression of the remaining detected targets – growth factors PDGF-αα and VEGF; chemokines IP-10, MCP-1, fractalkine, and SDF-1; and cytokines IL-6, IL-10, IL-17α, and IL-23 – showed no significant statistical difference between the two groups (P>0.1). Table 1 shows the results of the two groups’ serum concentrations of each cytokine.
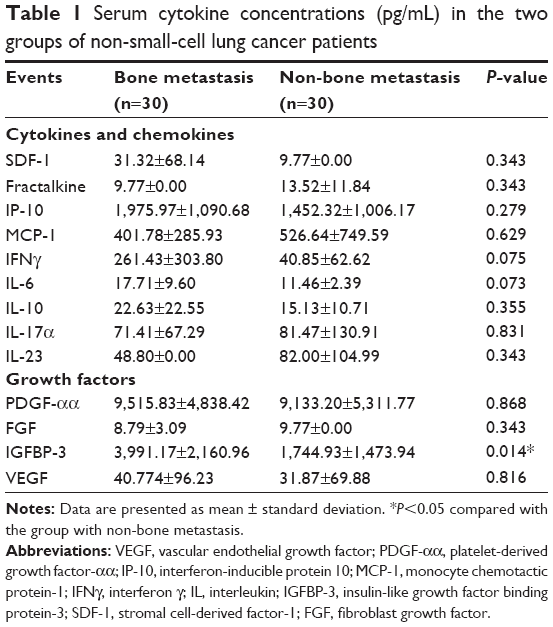 | Table 1 Serum cytokine concentrations (pg/mL) in the two groups of non-small-cell lung cancer patients |
In the bone metastasis group, one patient also had liver metastases; it should be taken into account that liver is one of the major organs for the synthesis of IGFBP-3. To increase the reliability and credibility of the trial, this case was removed, and the concentration of IGFBP-3 in the serum of the two groups of patients was then analyzed. The results showed that the 29 cases of serum from bone metastasis patients had a mean concentration of IGFBP-3 of 3,764.55±2,163.35 pg/mL, which was a statistically significant difference when compared to the non-bone metastasis group (n=30), with P=0.028.
Since the serum concentrations of SDF-1, FGF, IL-23, and fractalkine were too low, these four factors were not involved in the correlation analysis between IGFBP-3 and the other cytokines in serum. The results showed that, in the bone metastasis group, the serum concentration of IGFBP-3 had a positive correlation with VEGF (r=0.804, P=0.009) and MCP-1 (r=0.785, P=0.012) serum concentrations, but no correlation with other factors’ serum concentrations, as shown in Tables 2 and 3. In the non-bone metastasis group, there were no correlations between IGFBP-3 serum concentration and the serum concentrations of the various other factors. Table 2 shows the correlation of IGFBP-3 serum concentration with that of each other factor in the bone metastasis group.
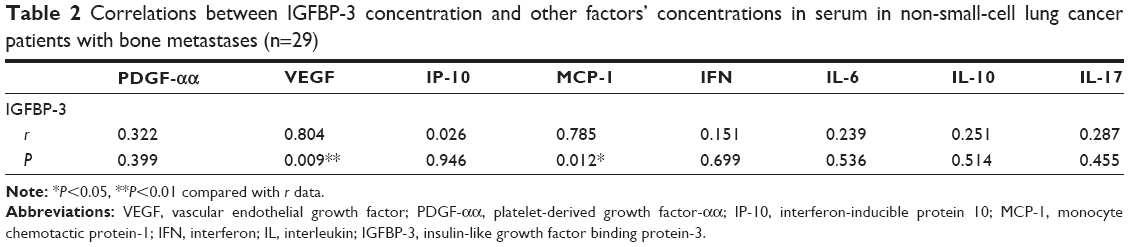 | Table 2 Correlations between IGFBP-3 concentration and other factors’ concentrations in serum in non-small-cell lung cancer patients with bone metastases (n=29) |
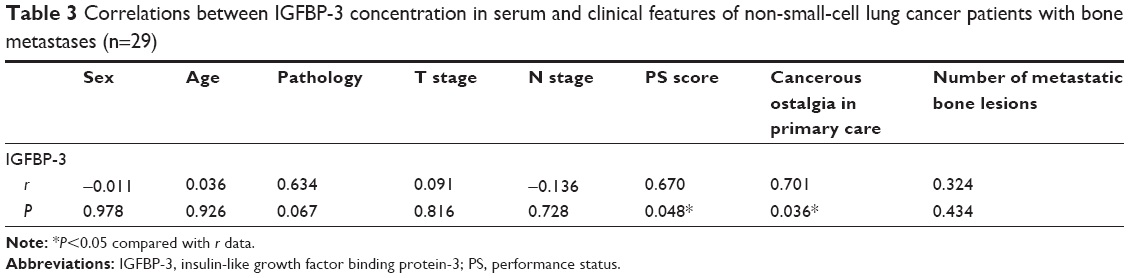 | Table 3 Correlations between IGFBP-3 concentration in serum and clinical features of non-small-cell lung cancer patients with bone metastases (n=29) |
In the bone metastasis group, by using partial correlation analysis between IGFBP-3, VEGF, and MCP-1, no correlation was found between any two of the factors with any one indicator variable fixed, suggesting that a synergistic effect may exist between the three factors.
Table 3 shows the correlation analysis between IGFBP-3 in bone metastasis patients’ serum and the clinical characteristics of the patients. The results show that no correlation was found between IGFBP-3 concentration in bone metastasis patients’ serum and patients’ sex, age, histological type, T stage, N stage, or number of metastatic lesions (P>0.05). A positive correlation was found between serum IGFBP-3 concentration and PS score (r=0.670, P<0.05), and between serum IGFBP-3 concentration and bone pain (r=0.701, P<0.05) in each of the two groups when newly diagnosed.
Discussion
Insulin-like growth factor (IGF) mediates growth hormone and promotes growth of cells and bones. The bone matrix was shown to have a lot of IGF-1 and IGF-2, where content was higher than other tissues.9 Thus, the direct effect of IGF on bone tissue has gradually attracted people’s attention. When IGF-1 or IGF-2 is bonded with IGFBP, it can reach the bone tissue through the capillary barrier. By extending the plasma half-life of IGF-1 and regulating the clearance rate of IGF, the effect of IGF-1 is enhanced. IGFBP-3 is promoted to be phosphorylated in the bone tissue, thus participating in the regulation of bone cell growth, proliferation, and metabolism. In vitro studies showed that IGF-1 stimulates the expression of osteoblast growth and alkaline phosphatase, type I collagen, osteocalcin, and other bone formation markers.10
It is well known that two biomarkers, N-telopeptide of type I collagen (NTx) and type I collagen carboxyterminal telopeptide (ICTP), may serve as aids in the diagnosis of bone metastasis in patients with lung cancer. For one thing, ICTP is a marker of pathological degradation of type I collagen. However, type I collagen does not exist exclusively in the bone, and the elevation of ICTP may be caused also by non-skeletal diseases. Furthermore, NTx is measured in urine or serum, so it is easy to measure and enables frequent testing in the intervals between bone scintigraphy; the results can indicate the need for bone scintigraphy. NTx can be used as a supplemental tool to diagnose bone metastasis from lung cancer.
In addition, Giles and Singh found that in the MDA-MB-231 breast cancer cell culture media, high concentrations of IGFBP-3 in a dose-dependent manner regulated transforming growth factor-β (TGF-β) mitosis to stimulate pro-bone metastasis of breast cancer cells, and TGF-β also had rich content in bone matrix and was an important constituent molecule of the microenvironment of bone metastases.11 In the present study, concentration of IGFBP-3 in lung cancer patients with bone metastases was obviously higher than in the non-bone metastasis group (P=0.014), indicating that the high serum expression of IGFBP-3 could be a sensitive indicator of bone metastasis in lung cancer. It increased the possibility of bone metastasis by enhancing the effects of IGF-1. This result was in line with that of Giles and Singh.11
IGFs and epidermal growth factor receptor (EGFR) on tumor cells bond to promote formation of new arteries. In the presence of IGF-1, mutant expression of EGFR can facilitate the generation of VEGF, thereby stimulating angiogenesis.12 In the present study, serum concentrations of IGFBP-3 showed a significant positive correlation with VEGF in the bone metastasis group (r=0.804, P=0.009), but no correlation in the non-bone metastasis group (r=−0.185, P=0.608), and further illustrated the synergy that may exist between VEGF in patients with bone metastases, IGFBP-3 generation, and the vascular endothelium.
MCP-1 is a representative member of the CC family in the MCP family with a strong lymphocyte chemotaxis. MCP-1 gene upstream had binding and regulatory region of Sp-1. By binding IGF-1 and IGF-1R, the expression of MCP-1 can be induced by cascade activation. Currently, there is no relevant literature reporting synergies that may exist between IGFBP-3 and MCP-1. Correlation analysis in the present study showed a positive correlation between expressions of IGFBP-3 and MCP-1 (r=0.785, P=0.012), suggesting that, as an important combined carrier of IGF-1, IGFBP-3 could stimulate activation of MCP-1; however, this finding requires further experimental support.
The results demonstrate that serum concentration of IGFBP-3 in lung cancer patients with bone metastases was positively correlated with bone pain and PS score, which may be due to these patients having a high baseline serum IGFBP-3 that stimulated osteoclasts to secrete a series of cytokines that 1) did or did not rely on IGFs; 2) strengthened the osteolytic process; 3) disrupted the balance between bone resorption and bone formation; and 4) caused bone destruction and bone pain.
Tumor cells invade the bone matrix to reach the periosteum, causing pain, and stimulate bone stromal cells to secrete excess IGFs, thus indirectly stimulating the secretion of bone matrix IGFBP-3. If it is true that serum concentration of IGFBP-3 in lung cancer patients with bone metastases is positively correlated with bone pain and PS score, then IGFBP-3 may be a new therapeutic target for bone metastases that could reduce stimulation of osteoclast activity by inhibiting the IGF system and reduce osteolytic bone metastases; if the second hypothesis is true, then, with the development of new drugs and widely used bisphosphonates or denosumab, monitoring and evaluation of the severity before and after treatment are likely to reveal the dynamic changes of bone metastasis IGFBP-3 indicators and provide meaningful evidence of treatment efficacy, thus becoming an evaluation index of bone metastases. However, the assertion of any hypothesis as correct needs a larger sample to support it.
We also found that the serum concentration of IGFBP-3 had no positive correlation with the number of bone metastases, indicating that the concentration of IGFBP-3 did not increase with the growth of bone metastases. This suggests that IGFBP-3 might have an important effect in early pathogenesis of bone metastases but be less involved in later progress.
Conclusion
The IGFBP-3 concentration in serum of lung cancer patients with bone metastasis was significantly higher than in that of patients with non-bone metastasis, and the IGFBP-3 concentration in bone metastasis patients was positively correlated with bone pain and PS score when newly diagnosed, but had no correlation with the number of bone metastases. This finding suggests important clinical implications of monitoring IGFBP-3 concentrations in patients’ serum for diagnosis and evaluation of the degree of bone metastasis. In addition, the positive correlation found in this study between IGFBP-3 concentration in bone metastasis patients with VEGF and MCP-1 concentrations might be highly relevant for the development of new treatments for bone metastasis of lung cancer.
Acknowledgment
This research was supported in part by the Shanghai Chest Hospital Technology Development Fund (YZ-13-27).
Disclosure
The authors report no conflicts of interest in this work.
References
National Office for Cancer Prevention and Control, National Center for Cancer Registry, Disease Prevention and Control Bureau, MOH. Chinese Cancer Registry Annual Report (2012). Beijing: Military Medical Science Press, 2012:12. Chinese. | ||
Wang Z. Selection of chemotherapy for non-small cell lung cancer is facilitated by new therapeutic strategies. Int J Clin Exp Med. 2014;7(11):3833–3842. | ||
Delea T, Langer C, McKiernan J, et al. The cost of treatment of skeletal related events in patients with bone metastases from lung cancer. Oncology. 2004;67(5–6):390–396. | ||
Plunkett TA, Rubens RD. The biology and management of bone metastases. Crit Rev Oncol Hematol. 1999;31(1):89–96. | ||
Rosen LS, Gordon D, Tchekmedyian NS, et al. Long-term efficacy and safety of zoledronic acid in the treatment of skeletal metastases in patients with nonsmall cell lung carcinoma and other solid tumors: a randomized, Phase III, double-blind, placebo-controlled trial. Cancer. 2004;100(12):2613–2621. | ||
Tsuya A, Kurata T, Tamura K, Fukuoka M. Skeletal metastases in non-small cell lung cancer: a retrospective study. Lung Cancer. 2007;57(2): 229–232. | ||
Hirsh V. Targeted treatments of bone metastases in patients with lung cancer. Front Oncol. 2014;4:146. | ||
Gesthalter YB, Vick J, Steiling K, Spira A. Translating the transcriptome into tools for the early detection and prevention of lung cancer. Thorax. 2015;70:476–481. | ||
Powell GJ, Southby J, Danks JA, et al. Localization of parathyroid hormone-related protein in breast cancer metastases: increased incidence in bone compared with other sites. Cancer Res. 1991;51(11):3059–3061. | ||
Mohan S, Jennings JC, Linkhart TA, Baylink DJ. Primary structure of human skeletal growth factor: homology with human insulin-like growth factor-II. Biochim Biophys Acta. 1988;966(1):44–55. | ||
Giles ED, Singh G. Role of insulin-like growth factor binding proteins (IGFBPs) in breast cancer proliferation and metastasis. Clin Exp Metastasis. 2003;20(6):481–487. | ||
Samani AA, Yakar S, LeRoith D, Brodt P. The role of the IGF system in cancer growth and metastasis: overview and recent insights. Endocr Rev. 2007;28(1):20–47. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.