")
Back to Journals » Clinical Epidemiology » Volume 14
Design for a Multicentre Prospective Cohort for the Assessment of Platelet Function in Patients with Hepatitis-B-Virus-Related Acute-on-Chronic Liver Failure
Authors Jiang X , Chai S, Huang Y, Huang Z , Tan W, Gao Y, Lu X, Meng Z , Zhou H, Kong W, Tang X, Tang Y, Qi T, Liao C, Gan Q, Xiang X, Zhang Y, Wang S, Chen Y, Chen J
Received 4 June 2022
Accepted for publication 15 August 2022
Published 24 August 2022 Volume 2022:14 Pages 997—1011
DOI https://doi.org/10.2147/CLEP.S376068
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Henrik Sørensen
Xiuhua Jiang,1,* Shiqi Chai,1,* Yan Huang,2,* Zuxiong Huang,3,* Wenting Tan,4,* Yanhang Gao,5,* Xiaobo Lu,6,* Zhongji Meng,7,* Huayou Zhou,8 Wenbing Kong,8 Xiaoting Tang,1 Yujun Tang,1 Tingting Qi,1 Chengjin Liao,2 Qiaorong Gan,3 Xiaomei Xiang,4 Yanan Zhang,5 Shuai Wang,6 Yuanyuan Chen,7 Jinjun Chen1,9
1Hepatology Unit, Department of Infectious Diseases, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China; 2Department of Infectious Diseases, Hunan Key Laboratory of Viral Hepatitis, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 3Department of Hepatology, Mengchao Hepatobiliary Hospital of Fujian Medical University, Fuzhou, People’s Republic of China; 4Department of Infectious Diseases, Southwest Hospital, Third Military Medical University (Army Medical University), Chongqing, People’s Republic of China; 5Department of Hepatology, the First Hospital of Jilin University, Changchun, People’s Republic of China; 6Infectious Disease Center, the First Affiliated Hospital of Xinjiang Medical University, Urumqi, People’s Republic of China; 7Department of Infectious Diseases, Hubei Clinical Research Center for Precise Diagnosis and Treatment of Liver Cancer, Taihe Hospital, Hubei University of Medicine, Shiyan, People’s Republic of China; 8Department of Blood Transfusion, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China; 9Hepatology Unit, Zengcheng Branch, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinjun Chen, Hepatology Unit, Department of Infectious Diseases, Nanfang Hospital, Southern Medical University, No. 1838, Guangzhou Dadao Bei, Guangzhou, 510515, People’s Republic of China, Email [email protected]
Background: Acute-on-chronic liver failure (ACLF) has high short-term mortality and lacks sufficient medical therapy. Available algorithms are unable to precisely predict short-term outcomes or safely stratify patients with ACLF as emergent liver transplantation candidates. Therefore, a personalized prognostic tool is urgently needed.
Purpose: Platelet function and its clinical significance in ACLF patients with chronic hepatitis B virus (HBV) infection have not been investigated. This study aimed to assess changes in platelet function using thromboelastography (TEG) and platelet mapping (TEG-PM) in HBV-related ACLF patients.
Methods: Chronic liver disease patients with acute decompensation or acute hepatic injury were recruited. The derivation cohort enrolled HBV-related patients at Nanfang Hospital. HBV-related and non-HBV-related patients were both enrolled in internal and external validation cohorts at seven university hospitals. TEG and TEG-PM were performed at baseline in the derivation cohort and baseline, day 7, and day 14 in the validation cohorts. The primary outcome was all-cause 28-day mortality. Status check and new-onset complications were recorded during the 3-month follow-up, but status check will extend to 5 years.
Conclusion and Future Plans: In this study, 586 participants were enrolled, including 100 in derivation cohort, 133 in internal validation cohort, and 353 in external validation cohort. Biomaterials, including plasma, serum, urine, and some explanted liver tissues, were collected from these patients. A 3-month follow-up with survival status was completed. The baseline characteristics indicated that 51% of the patients had adenosine diphosphate (ADP)-hyporesponsive circulating platelets. The prognostic potential of platelet function will be explored in the derivation cohort (HBV-related ACLF patients) and further substantiated in the validation cohorts (HBV-related and non-HBV-related ACLF patients). Biosamples are currently used to explore the underlying mechanisms related to ADP-hyporesponsive platelets. The ongoing proteomic and metabolic analyses will provide new insights into the pathogenesis of extrahepatic organ failures in ACLF patients.
Keywords: acute-on-chronic liver failure, coagulopathy failure, platelet function, thromboelastography, prognosis, study design
Introduction
Acute-on-chronic liver failure (ACLF) is a condition in which patients with chronic liver diseases develop hepatic and extrahepatic organ failure due to acute insults.1 In Asia and many other developing regions, the majority of ACLF patients have chronic hepatitis B virus (HBV) infections, which are characterized by a high prevalence of coagulation disorder.2 ACLF patients in Europe or North America mostly have non-HBV-related liver cirrhosis in which coagulation disorder is much less frequent than those with HBV-related liver cirrhosis. It has been demonstrated that C5a receptor (C5aR), TNF-a, and fibrinogen-like protein 2 (FGL2) form an integral network that contributes to coagulation and complement activation from FH patients infected by HBV.3 In contrast to the ACLF definition of the European Association for the Study of the Liver (EASL)1 or the American Association for the Study of Liver Diseases (AASLD),4 coagulation disorder is an essential component in the definitions proposed by the Asian Pacific Association for the Study of the Liver (APASL)5 or the Chinese Medical Association (CMA)6 (See Online Supplemental Table 1). APASL and CMA define ACLF as “an acute hepatic insult manifesting as jaundice and coagulopathy, while EASL and AASLD definitions of ACLF require the presence of organ failure.7
Coagulation disorder in ACLF patients is always presented by an elevated international normalised ratio (INR) in the literature. And plasma exchange or plasma transfusion aiming to correct the INR has a controversial role in prognosis modification.7,10,11 Compared with alcoholic and/or hepatitis C-related ACLF patients (the CANONIC study), ACLF patients with hepatitis B virus (the COSSH study) showed a higher incidence of coagulation failure (INR ≥2.5).8,9 However, upper gastrointestinal bleeding in patients with ACLF is mostly variceal bleeding and caused by portal hypertension rather than coagulation disorders.13 And ACLF patients had similar upper gastrointestinal bleeding rates, as 13.5% (37/274)12 in HBV-related ACLF and 13.2% (40/303) in alcoholic and/or hepatitis C-related ACLF patients.9
Recently, impaired but mixed fibrinolysis phenotypes have been found at the time of admission of liver cirrhosis and ACLF patients.14 Elevated D-dimer concentrations indicating active fibrinolysis were found in HBV-related ACLF patients and associated with worse 28-day survival.15 Circulating platelet count and platelet function are also fundamental to the coagulation system. In a prospective multicenter cohort, the declining trend of platelet counts was more significant in ACLF than in non-ACLF patients, indicating exacerbated clinical outcomes. In Kaplan–Meier analysis, the cumulative incidence of 90-day adverse outcomes increased with the decline of platelet counts. However, platelet count alone does not seem to independently predict outcomes of ACLF patients.16 Therefore, a global measurement (instead of INR alone) for coagulation disorder and platelet response to endogenous agonists, in addition to platelet count, might expand the knowledge on coagulation disorder in ACLF patients. As such, these studies might provide insights for further prognostic and therapeutic investigations.
Thromboelastography-platelet mapping (TEG-PM) provides a global and dynamic assessment of coagulation. This measurement reflects the cumulative effect of interactions at various levels between plasma components (clotting proteins) and cellular components (platelets, red and white blood cells, and microparticles) of coagulation. Meanwhile, it is also able to measure platelet reactivity presented as a response to adenosine diphosphate (ADP) or arachidonic acid (AA).17
As there are no previous prospective and multicentre studies aiming to profile the coagulation abnormalities and platelet function using TEG and platelet mapping in HBV-related ACLF patients, we aimed to investigate the alterations in coagulation and platelet function with a global measurement using TEG-PM in our patients. The prognostic potential of platelet function for 28-day mortality would also be explored and validated with this patient cohort.
Methods
Aim and Study Protocol
The primary aim was to explore and validate the prognostic potential of platelet function for 28-day mortality in HBV-related ACLF patients. The study protocol was as follows:
1. To conduct a global evaluation of coagulation abnormalities and platelet response to ADP/AA in hospitalised ACLF patients using TEG-PM.
2. To implement a statistical approach to develop and validate a prognosis model composed of TEG-PM variable(s). A more accurate prognostic algorithm for 28-day mortality than those proposed by national and international liver societies would be pursued.
3. To explore the mechanisms underlying platelet hyporesponsiveness to ADP with multi-omics approaches and relevant validation assays.
The study was approved by ethics committees and registered accordingly (ClinicalTrials.gov Identifiers: NCT03281278, NCT04119973) and conducted in compliance with the Declaration of Helsinki guidelines.
Overview
With promising data in the derivation cohort (NCT03281278), the study was expanded to internal validation and external validation cohorts (NCT04119973). All participants were patients who were hospitalised. Both derivation and validation cohorts enrolled HBV-related patients. In addition, non-HBV participants were also enrolled in the validation cohort to further validate the prognostic algorithm derived from HBV-related patients.
In the derivation cohort, HBV patients with severe liver injury who were at a potential risk of ACLF development were consecutively screened and recruited at Hepatology Unit, Nanfang Hospital, Southern Medical University. Patient enrolment occurred from October 2017 to August 2018. A larger sample size for the validation cohort was estimated to gain enough statistical power for the analysis of primary outcomes (n≥50) in non-HBV patients. Internal validation was conducted from August 2018 to August 2019, and a multicentre external validation study was conducted in six centres from provinces with different geographic distributions.
Data were collected according to case report forms. Patients were followed up for 3 months. Death from any cause was considered the endpoint, and liver transplantation (LT) was considered a censoring event. Figure 1 shows the study design (Figure 1A), TEG measurements and biomaterials collection schedule (Figure 1B), and the flowchart of patient enrolment for the derivation (Figure 1C), internal validation (Figure 1D), and external validation (Figure 1E) cohorts.
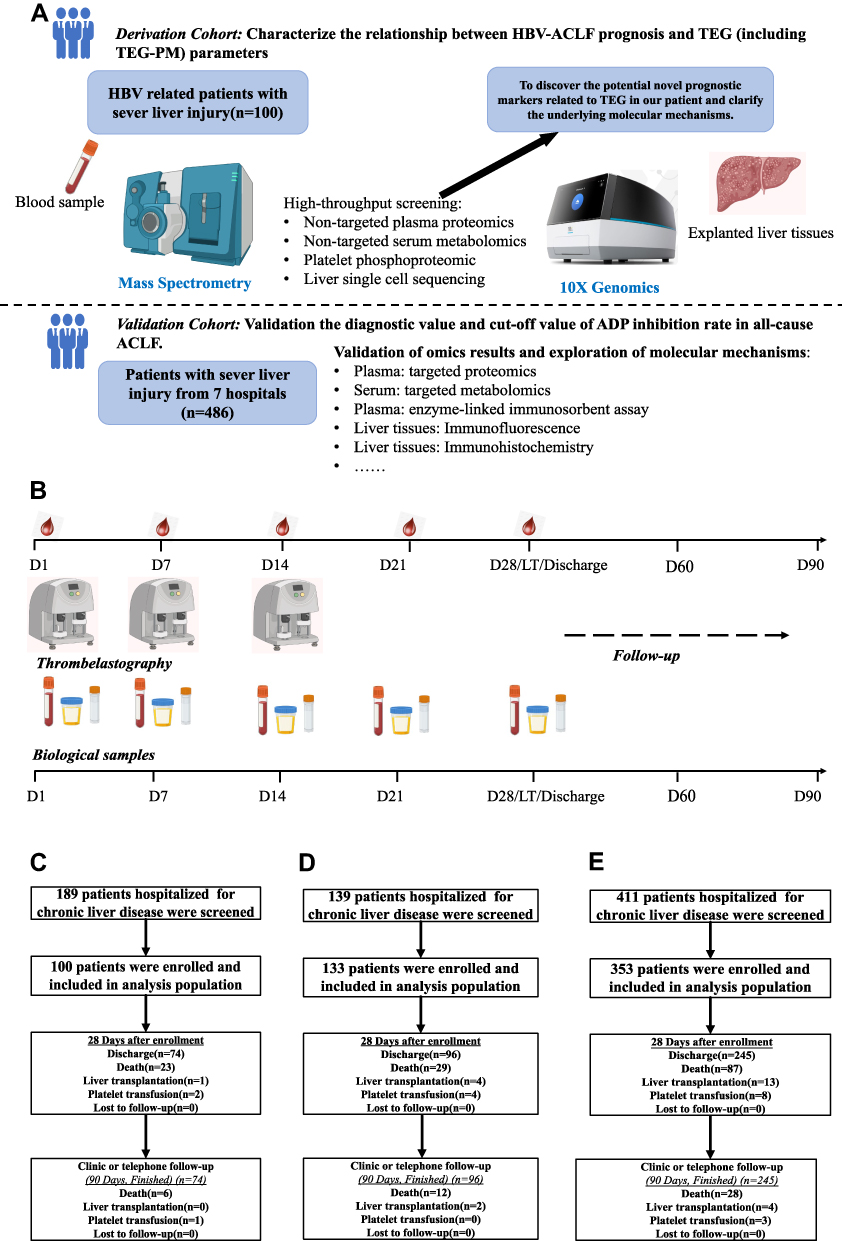 |
Figure 1 Flow chart of patient enrollment, biosamples collection and the study design for related basal studies. And the study design for molecular mechanism exploration with multi-omics approaches (A). Calendar for biosamples collection and follow-ups (B). Flow chart of the derivation cohort (C), internal validation cohort (D) and external validation cohort (E). |
Eligibility Criteria
Derivation Cohort
Patients with an estimated hospital stay >24 hours would be screened on the admission day. The inclusion criteria were as follows: 1) chronic HBV infection was the only cause of chronic liver disease, 2) between 18 and 80 years of age, and 3) having acute and significant liver injury defined as INR >1.5 and total bilirubin >85 μmol/L8 (Online Supplemental Appendix 1). Exclusion criteria were as follows: 1) patients with any types of malignancies, 2) obstructive biliary diseases or other diseases that result in bilirubin evaluation, 3) acute haemorrhage 1 week prior to the hospital admission, 4) received platelet transfusion, cryoprecipitate transfusion, or plasmapheresis therapy within 1 week prior to admission, 5) usage of antiplatelet or anticoagulant drugs within 4 weeks prior to the admission, or receipt of steroids and immunosuppressants, 6) pregnant or breastfeeding, 7) receiver of LT or kidney transplantation, and 8) having other severe extrahepatic diseases, such as heart failure (New York Heart Association Class IV), respiratory failure (partial pressure of oxygen <60 mmHg), renal insufficiency (stage 5 of chronic kidney disease), and conscious disturbance (Glasgow coma scale score of <8), leading to organ failure.
Validation Cohort
The enrolled population included patients aged 18–80 years, with acute and significant liver injury (INR >1.5, total bilirubin >85 μmol/L), irrespective of the aetiology of chronic liver diseases. With the expansion of aetiologies for chronic liver diseases, we expected to validate the prognostic potential of platelet function in ACLF with chronic HBV-infected and non-HBV patients. The exclusion criteria were identical to the derivation cohort (Online Supplemental Appendix 2). Written informed consent was obtained from all participants or their entrusted kins after a full explanation of this study by the investigators.
Selection of Centres
All participating centres met the following qualifications: 1) having a liver division from the Department of Hepatology, Gastroenterology or Infectious Disease with a tertiary university hospital affiliation, 2) the candidate principal investigator is academically active in liver failure and liver cirrhosis research, 3) available staff member(s) and research fellows assigned to this study, 4) TEG measurements were available and performed strictly according to the study protocol, and 5) a representative geographic distribution. Ultimately, seven centres from different provinces (Guangdong, Chongqing, Jilin, Xinjiang, Fujian, Hunan, and Hubei) participated in this study (Figure 2).
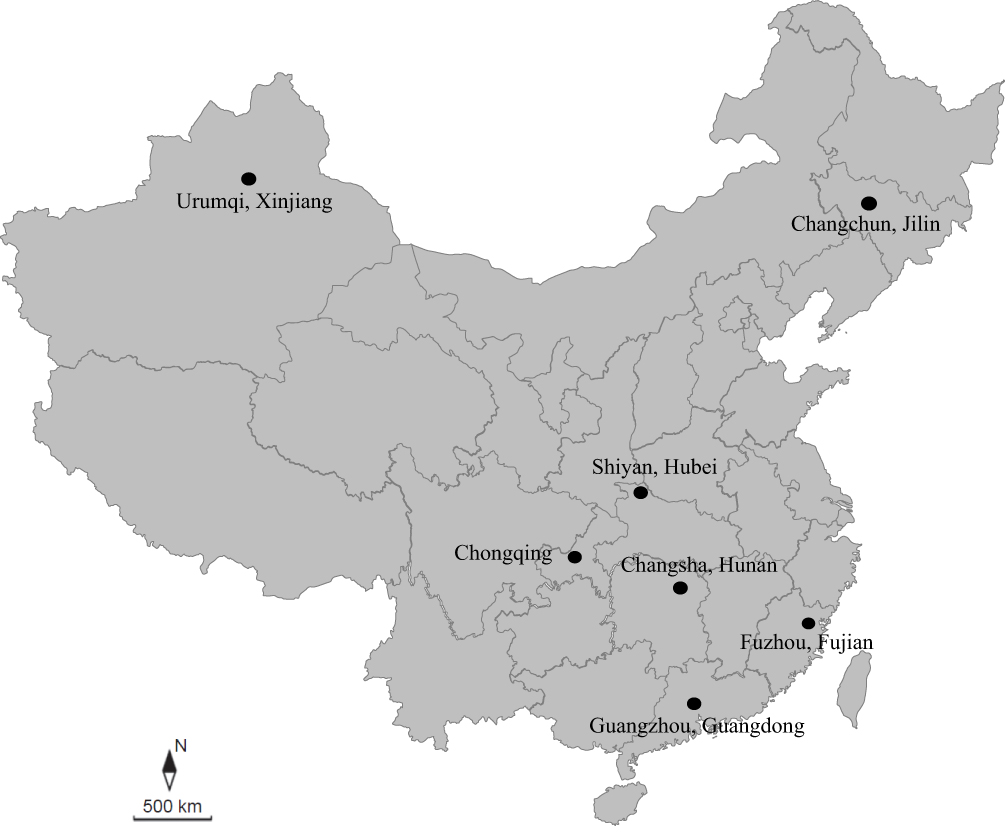 |
Figure 2 The geographical distribution of seven recruitment centres. Approximately 6% of the total population in China resides in the western regions, and 94% of the total population in China resides in the eastern regions. Six of our centres are located in Eastern China and one in Western China. |
Data, TEG Measurements, Biosamples Collection
All measured parameters are listed in Table 1. Demographic data, medical history, physical examinations, and imaging examination(s) on days 1, 4, 7, 14, and 28 after enrolment were collected and recorded according to the case report forms. And clinical outcomes, together with abovementioned parameters, are listed in Table 1 (Online Supplemental Appendix 3-5). Table 2 shows the detailed list of the laboratory parameters during hospitalization and follow-up. Organ failure was assessed according to the EASL-CLIF diagnostic criteria9 (Online Supplemental Table 1). The related therapeutics, including data on antibiotics, antiviral medicines, red blood cell transfusion(s), platelet transfusion(s), plasma transfusion or exchange, and assisted liver support, were all recorded. Patients were followed up until 28 and 90 days after enrolment (Online Supplemental Appendix 6).
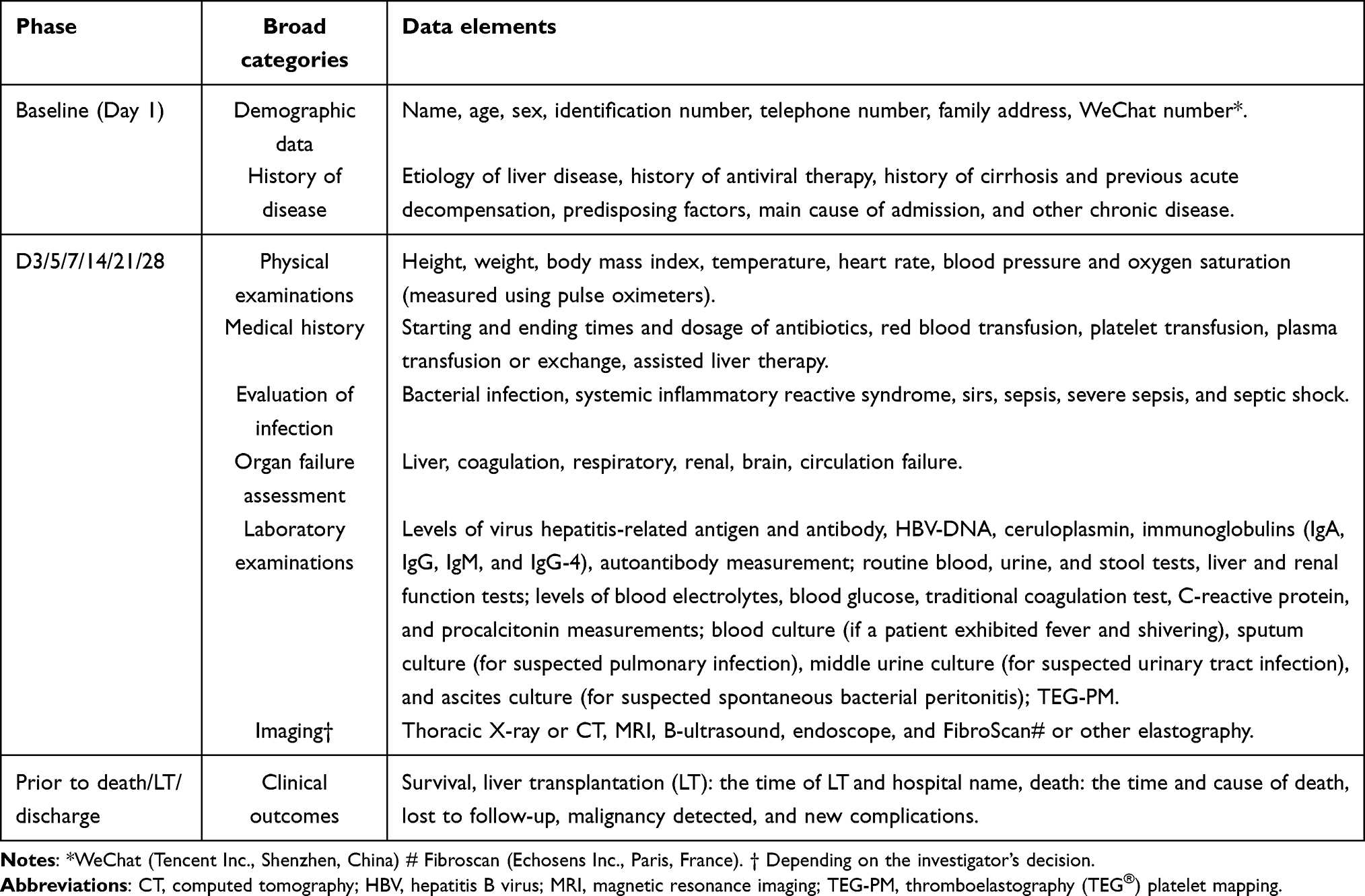 |
Table 1 Parameters of This Study |
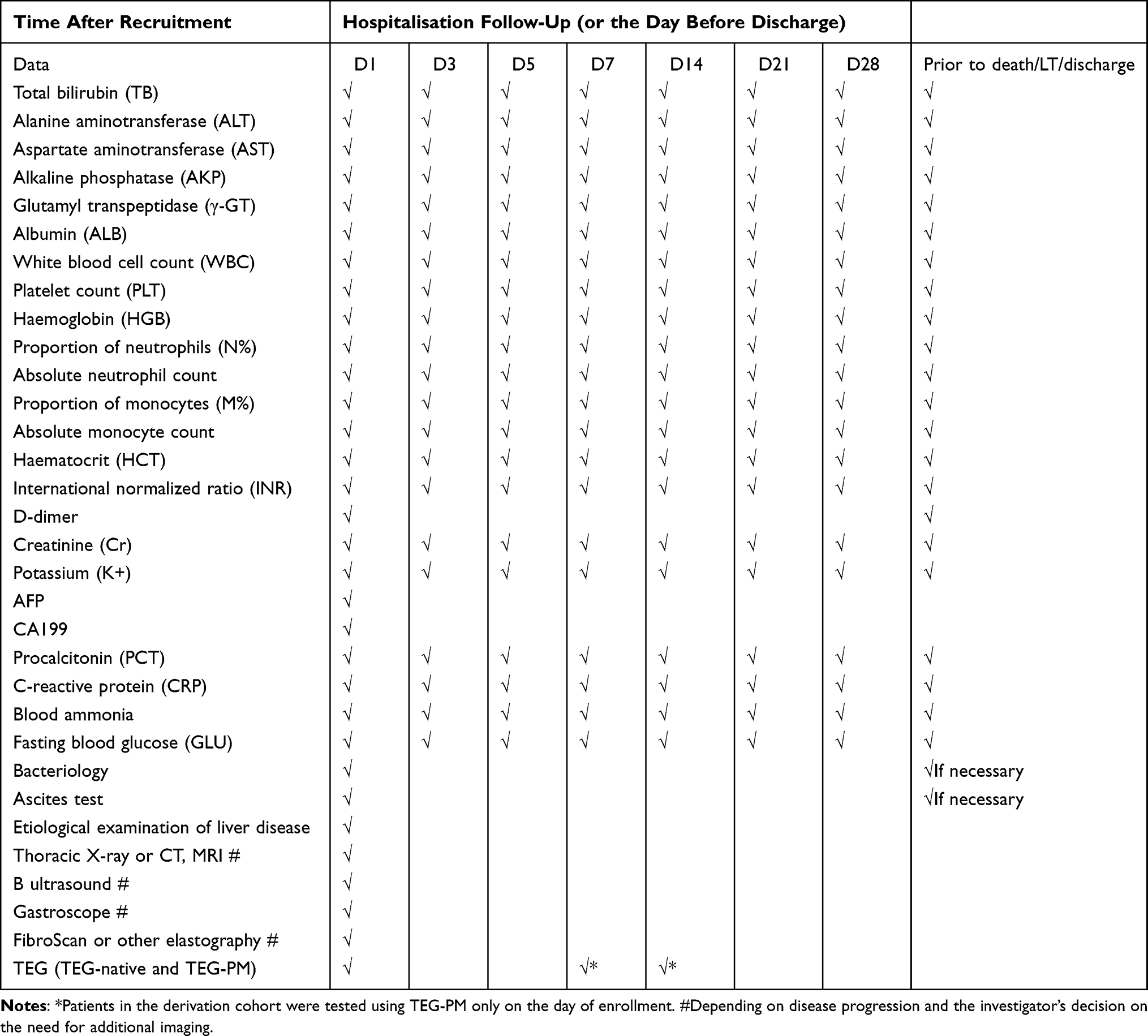 |
Table 2 Data Collection Schedule During 28-Day of the Study |
The participants were scheduled for TEG measurement on days 1, 7, and 14 after enrolment (Figure 1B). Blood samples were drawn from a single clean puncture of a forearm vein and collected into test tubes provided by manufacturers and tested according to the manufacturer’s protocol (TEG ® 5000 Thromboelastography analyser, TEG ®Thromboelastogram ®Haemostasis system, Haemonetics Corporation, USA, or CFMSLEPU-8800 Thromboelastography, LEPU MEDICAL, China). Platelet response to ADP via P2Y12 receptor pathway and to AA via cyclooxygenase pathway was measured and presented as the ADP or AA inhibition rates, respectively. All TEG parameters in this study are presented in Online Supplemental Table 2.
Different types of biosamples, including plasma, serum, peripheral blood mononuclear cell DNA, and urine, were collected and stored at −80°C (Figure 1B). Platelet pellets were collected from patients in the derivation cohort for further proteomic studies. There were 10 explanted liver tissues that were not acquired due to liquid nitrogen shortage at operation unit and 2 without signed explanted organ donation consent from patients and/or their kins, and only 13 explanted liver tissues were collected and cryopreserved appropriately. Explanted liver tissues must be frozen in liquid nitrogen, and held for 1 hour before transferring to −80°C. Proteomics (plasma, platelet pellets), genome-wide association studies (genomic DNA), single-cell transcriptome sequencing (explanted liver tissues), and metabolomics (serum) investigations were planned (Figure 1A).
Follow Up
Each patient had been followed up to 90 days after enrolment as planned. The primary endpoint was 28-day all-cause mortality. The 90-day all-cause mortality and progression to EASL-CLIF-defined ACLF within 28-day were both considered secondary endpoints. LT and loss to follow-up were considered censoring events.
During the study, detailed clinical and laboratory data were collected on days 1, 4, 7, 14, 21, and 28 or till the day of death within 28 days. Afterwards, monthly follow-up was performed by telephone calls, WeChat exchanges with investigators, clinic visits, and hospitalization or re-hospitalization up to 3 months after enrolment. Except for patient status checks (survival, death, or LT), monthly follow-ups also included specific health guidance regarding issues of ascites growth, infection, gastrointestinal bleeding, overt hepatic encephalopathy, jaundice, and malignancy. For patient ceased, the date and cause of death were documented. For patients with LT, the procedure centre and date were recorded accordingly (Online Supplemental Appendix 6). After 3 months, we only recorded patients’ status (survival or death) by telephone calls every 6 months in 5 years. Death of participants with loss of follow-ups would be confirmed or excluded through the civil registration system with the permission of the public security.
Quality Assurance and Control
Electronic Data Capture System
An electronic data capture system was designed, set up, and completed to minimise errors and optimise data accuracy. The system included electronic case report form development, data retention and audit trials, logical verification, source data verification and correction, database locking, data storage, and data export.
Personnel Training
Before the electronic data capture system was implemented, mandatory and timely training of personnel was conducted, and access to the corresponding system rights was granted to those qualified.
Verification
Internal verification: Annual on-site verification of eligibility criteria for all screened and enrolled patients, extreme value verification, logical verification, review of critical medical records, and examination of missing data were performed.
External verification: 1) A third-party company (Unimed Scientific Inc. Wuxi, China) was responsible for data management and inventory. 2) A statistical plan was developed in advance.
Archiving of Traceable Raw Data
Raw data were obtained from medical records, physical examinations, clinical and laboratory data, imaging, pathology, medication orders, clinic notes, and telephone or WeChat follow-up documents. All data were traceable and stored in the corresponding servers at each centre.
TEG and TEG-PM Measurements
To maintain the quality of TEG measurements, personnel training and calibrations were carried out at each centre. TEG tests were performed within 2 hours after blood collection, which was 4 hours from blood collection to TEG measurement as recommended by the manufacturer of the TEG. The time interval between the blood collection and TEG measurement was also documented for each test.
For TEG analysis details, whole blood was collected from citrate tubes (3mL, 0.109 M) and lithium heparin tubes (4mL, 75 USP Units) using BD Vacutainer ® tubes (Becton, Dickinson and Company, Franklin Lakes, NJ, USA). All samples were stored upright at room temperature (20–25°C) for a median time of 60 minutes (range: 15 −180 min) as recommended. Each citrate blood sample was re-calcified and analyzed by a two-channel TEG cartridge, performed using citrated kaolin assay (CK, TEG-native). Heparinized blood sample was used for TEG-PM assay including platelet response to ADP via P2Y12 receptor pathway and to AA via cyclooxygenase pathway.
The Accuracy of TEG and TEG-PM
The tube system was internally validated and specimen handling was in accordance with local protocols with samples checked for clots and to ensure accurate collection volumes. Inadequate samples, including those with clots or those overfilled or underfilled, were discarded and excluded from analysis. The accuracy of the instrument will be checked monthly. In brief, when using the same lot number of reagents to test the same samples, parameters assessed by TEG-native and TEG-PM assays had a coefficient of variation (CV) ≤10%.
Cold Chain (−80°C) Transport
All biochemical samples were cold chain (−80°C) transported to the oversight centre to ensure quality and unified management. At the end of November 2019, all bio-specimens (plasma, serum, platelet pellets, liver tissues, and urine) were transported to the biosample bank at Nanfang Hospital.
Sample Size
To date, there have been no reported data on the relationship between TEG parameters and 28-day mortality among patients with ACLF. The results from the derivation cohort were used to evaluate the sample size of the validation cohort. In the derivation cohort, ADP inhibition rate showed the independent and the best predictive value for 28-day mortality. The sample size statistical analyses were performed using Empower Stats software (www.empowerstats.com, X&Y solutions, Inc Boston MA). The lower limit of the 95% CI of the area under the curve (AUC) of the ADP inhibition rate was 0.9 for the prediction of 28-day mortality (N1=6), and the mortality rate of the derivation cohort was approximately 25% (N2=6/0.25=24). Twenty-four patients with HBV-related ACLF achieved 90% power and detected a difference of 0.4 between the AUC under the null hypothesis of 0.500 and the AUC under the alternative hypothesis of 0.9 using a two-sided z-test at a significance level of 0.05. HBV-related ACLF accounts for approximately 50% of ACLF cases (N3=24*2=48). Considering a 20% loss to follow-up (N4=48/0.8=60), 60 participants were planned to be included in the internal and external validation cohorts. Different centers may represent different populations as the study commenced simultaneously in each center, it was finally decided to include about 60 patients per center, resulting in a total of 420 participants in the validation cohort.
Statistical Analyses
Statistical analyses were conducted using IBM SPSS Statistics (version 22) and R version 3.6.0 (R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics were calculated. Continuous variables were tested for normality using the Shapiro–Wilk test and presented as mean±SD or median and interquartile range (IQR 25–75%), while categorical variables were reported as absolute numbers and percentages. Comparisons would be performed using Student’s t-test, Mann–Whitney U-test, χ2 test, or Fisher’s exact test. All statistical tests were two-sided with a significance level of P<0.05.
As specified in the analysis plan, the optimal cutoff point of the ADP inhibition rate is defined using maximally selected log-rank statistics.18 Mortality rates and differences in 28-day mortality influenced by clinical complications were estimated and displayed using the Kaplan–Meier estimator. Short-term mortality risk prediction equations were explored using logistic regression, Cox proportional hazards models, and competing risk models. Variable selection was performed by applying the LASSO methodology in conjunction with 10-fold cross-validation to prevent overfitting. Variables were selected based on their contribution to the model’s significance, using the likelihood ratio test, and including the least number of variables to facilitate its future usage in clinical practice. Model fit was evaluated (by discrimination C-statistic and calibration Ȥ2 using modified Nam-D’Agostino test,) using the Hosmer–Lemeshow test. The performance of the equations was evaluated in both internal and external validation cohorts using the same statistical methods. As part of the validation process, the predictive capacity of each model was estimated by calculating the receiver operating characteristic curves and the area under the curve (AUC), and comparing the AUC of each model, if necessary. If the models proved valid and accurate enough for prediction purposes, scoring systems permitting simpler use of clinical practice models were defined.
For high-throughput screening (Figure 1A), patients were divided into two groups according to platelet responses to ADP and stratified at the optimal cutoff value, which was adopted in the model for the 28-day survival prediction. Five biological replicates for each group were planned for platelet phosphoproteomic and non-targeted plasma proteomics (tandem mass tags), and 25 biological replicates were planned for non-targeted serum metabolomics (ultra-high-performance liquid chromatography-tandem mass spectrometry). For targeted plasma proteomics (parallel-reaction monitoring) and serum metabolomics (Liquid chromatography-tandem mass spectrometry), more than 50 biological replicates were designed for each group.
In omics analysis, using a p-value <0.05 with a difference of 1.2-fold or more and 0.83-fold or less, we identified biomarkers with high or low expression from proteomics and metabolomics.
Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis or Gene Ontology (GO) was performed to select highlighted pathways from GWAS (400 biological replicates for each group) and SC-Seq (3 biological replicates for each group). Next, the least absolute shrinkage and selection operator (LASSO) approach was used to find biomarkers of interest as explanatory variables to build up a new prognostic score or to uncover underlying molecular mechanisms. Each of those selected biomarkers was subjected to ROC analyses evaluating its sensitivity and specificity in discriminating high mortality patients from enrolled patients. A logistic regression model or multivariate Cox proportional hazards regression model was constructed for the diagnosis score. ROC analysis was used to estimate the performance of the diagnostic score.
Ethics
This study was approved by the Nanfang Hospital Ethics Committee at Southern medical University.
Results
A total of 586 patients were enrolled from seven centres (Figure 2) according to the study design. Among these patients, 100 HBV-related patients were enrolled in the derivation cohort (Figure 1C), in which ADP inhibition rate was found as the most promising variable in the 4-week mortality prediction. As previously planned, 133 patients were enrolled in the internal validation cohort (Figure 1D), and 353 were enrolled in the external validation cohort (Figure 1E).
In overall, 189 HBV-related patients were screened and 100 were enrolled in the derivation cohort at Nanfang Hospital (Figure 3A). For the internal validation cohort, 139 patients were screened, and 100 HBV-related and 33 non-HBV patients were enrolled (Figure 3B). For the external validation cohort, 411 patients were screened, and 277 HBV-related and 76 non-HBV patients were enrolled. In the validation cohort, no alcoholic hepatitis or autoimmune hepatitis patient was excluded due to steroids use prior to enrollment. And 6 patients with acute gastrointestinal bleeding events which might significantly change coagulation parameters were excluded from this entire study. The number of patients screened and enrolled at each centre is shown in Figure 3B, and the number of HBV-related patients enrolled at each centre was further highlighted.
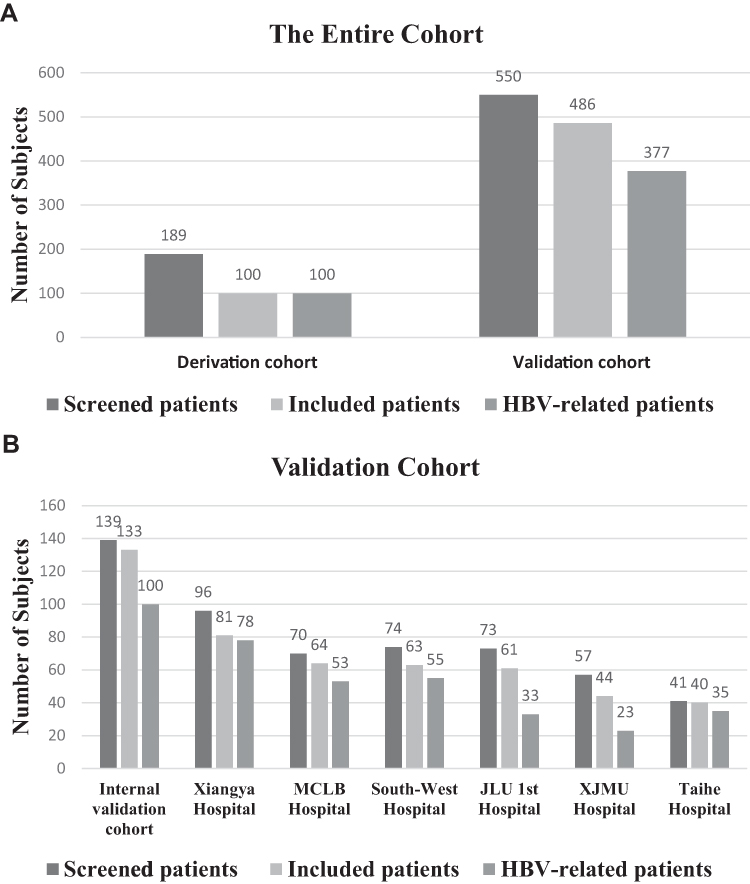 |
Figure 3 The number of patients enrolled in each of the seven centres. The enrolment of the entire cohort (A) and the validation cohort (B). Nanfang Hospital, Southern Medical University (Guangzhou); Xiangya Hospital, Central South University (Changsha); Mengchao Hepatobiliary Hospital (MCLB), Fujian Medical University (Fuzhou); Southwest Hospital, Third Military Medical University (Chongqing); First Hospital of Jilin University (JLU) (Changchun); First Affiliated Hospital of Xinjiang Medical University (XJMU) (Urumqi); Taihe Hospital, Hubei University of Medicine (Shiyan). |
The types and numbers of collected biosamples for the entire study are shown in Figure 4. On the first day of enrolment, 456 plasma (and peripheral blood mononuclear cell DNA), 445 serum, and 323 urine samples were successfully collected. Additionally, explanted liver tissues were collected from 13 patients who underwent LT. Seventy platelet pellet samples were collected from the derivation cohort.
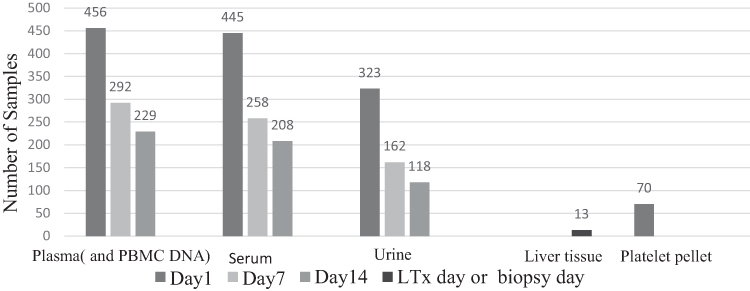 |
Figure 4 The sample collection and storage of the study. |
The baseline characteristics, including the demographic and laboratory data of eligible patients, are summarized in Table 3. Overall, men were the majority in all three cohorts (84.0% in the derivation cohort, 82.7% in the internal validation cohort, and 80.2% in the external validation cohort). The median age of the patients was 45 years.
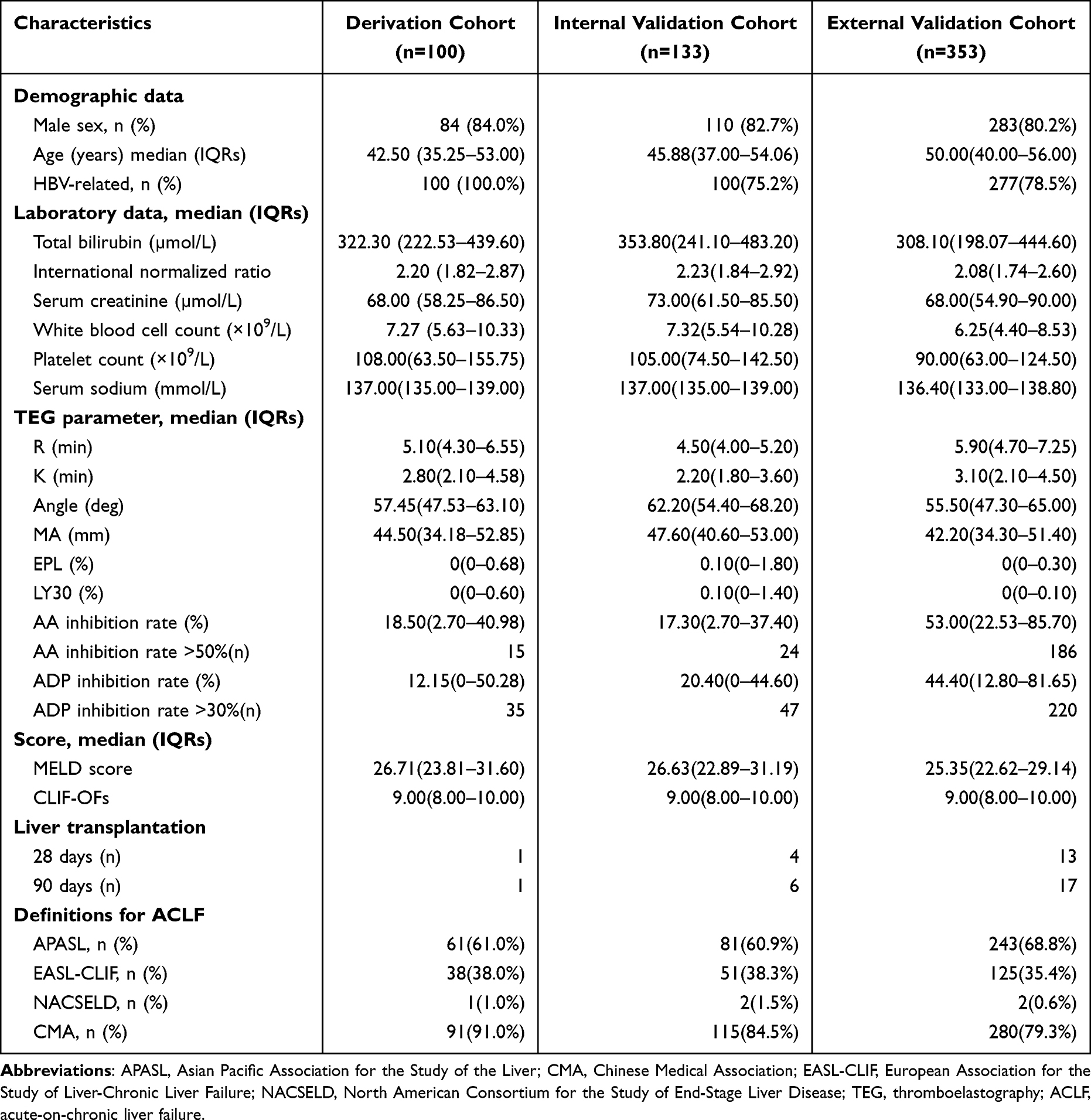 |
Table 3 Baseline Characteristics of Study Participants |
Regarding the aetiology of chronic liver disease, patients with chronic HBV infection accounted for 75.2% (100/133) and 78.5% (277/353) of the internal and external validation cohorts, respectively. Both cohorts reached the expected enrolment numbers of patients with HBV-related diseases. The number of primary outcomes in non-HBV patients was also reached. ACLF diagnoses in our patients were classified as per the definitions of national or international liver societies (Online Supplemental Table 1). The proportion of our ACLF patients was the largest, consistent with the CMA criteria (91.0% in the derivation cohort, 84.5% in the internal validation cohort, and 79.3% in the external validation cohort), followed by the APASL and EASL-CLIF criteria. AASLD criteria were deemed to be obviously unsuitable for our patients (Table 3). The prevalence of ACLF diagnosed with different definitions in the entire population is shown in Figure 5A. Patients who met the EASL-CLIF criteria had the highest 28-day mortality rate (Figure 5A). The parameters of the TEG-PM measurement suggested that 51% (299/586) and 38% (225/586) of the patients had circulating platelets with ADP and AA hyporesponsiveness, respectively, as indicated by an ADP inhibition rate of >30% and an AA inhibition rate of >50%.19–23 ACLF patients met EASL-CLIF criteria had the highest proportion of ADP hyporesponsiveness, followed by the APASL and CMA criteria (Figure 5B). The rates of loss to follow-up at 28 and 90 days were all zero in the three cohorts. For the entire study, the number of patients who underwent LT was 18 within 28 days and 6 within 29–90 days (Figure 1C-E).
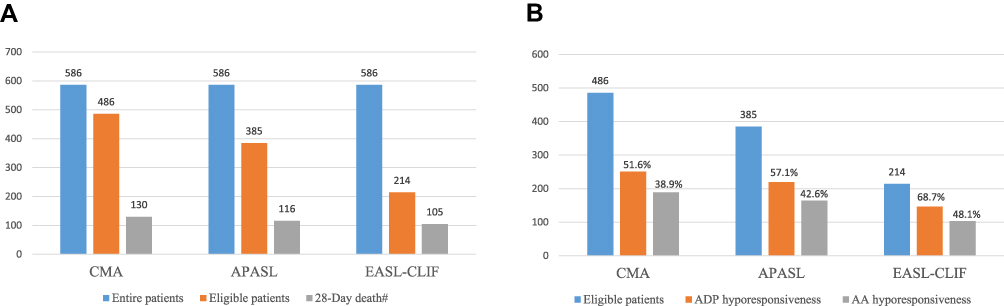 |
Figure 5 The prevalence of ADP hyporesponsiveness and 28-day mortality according to different ACLF definitions. The prevalence of ACLF according to CMA, APASL or EASL-CLIF criteria, and 28-day deaths according to ACLF definitions (A). Prevalence of platelet dysfunction according to ACLF definitions (B). # Liver transplantation patients and platelet transfusion patients were not included in the survival analysis. |
Discussion
This large, prospective and multicenter study has been completed. It focused on the potential prognostic role of TEG measurement and platelet functions in ACLF patients with chronic hepatitis B virus infection. These related omics researches will provide insights for understanding the mechanisms underlying liver failure development and extrahepatic organ injuries or failures.
To date, TEG measurement has been used to explore coagulation abnormalities relating to bleeding and thrombosis complications. It has been reported to be helpful in guiding blood product usage in patients with liver cirrhosis or acute liver failure or those requiring invasive procedures. No such study has been carried out in ACLF patients.
This study makes a considerable contribution to the exploration more precise and accurate prognostic model for ACLF patients with HBV infection. The newly proposed model is expected to more accurately stratify the 28-day survival of ACLF patients defined as COSSH study and CANONIC study, respectively. Our model provided superior overall accuracy compared to the commonly cited prognosis scores including CLIF-OF, MELD and MELD-Na. In both the derivation and validation cohorts, the sensitivity remained at ≥99% in patients with HBV-related ACLF, which was able to be applied to all-cause chronic liver diseases as our validation cohort showed. More importantly, the model owned capacity to differentiate some patients who would develop ACLF patients within 28 days and would facilitate timely and appropriate prophylactic interventions.
Moreover, the already collected biosamples had been investigated with emerging technologies, including metabolomics and proteomics. Those omics researches would obtain molecular insights into the mechanism for extrahepatic organ failures in ACLF patients precipitated with intrahepatic insults. Furthermore, those studies also identified the potential intervention to modify the 28-day mortality of ACLF patients. Previous studies have shown that upon receiving signals of blood vessel damage, platelets reorganize their actin cytoskeleton, which transforms into a spiky dynamic adherent glue.24 Our data showed that over half of EASL-CLIF-defined ACLF patients had hyporeactive circulating platelets, and the dysfunction platelets were supposed to impair the ability of rolling, spreading, adhesion, and contraction in endothelial repair, local coagulation,25 thrombosis,26 and bacterial killing.27 In addition, platelets have been shown to prevent tissue injury during the early phase of inflammatory reactions through GPVI-dependent platelet binding and activation,28 thus preventing bleeding in inflamed tissues. And our retrospective analysis of ACLF patients transfused with platelets had improved 28-day survival (data not shown) which strengthened our hypothesis. Therefore, with the stratification of patients with their platelet responses to ADP, we started platelet transfusion for selected ACLF patients aiming to improve their short-term prognosis (NCT04564651).
In brief, we successfully established a qualified internal and external validation cohort of ACLF patients in HBV high-endemic areas. We used rigorous data quality control strategies to ensure the relatively high validity of the data collection. The loss to follow-up rates at 28 and 90 days were both zero.
Our study has some limitations. Firstly, since it is a prospective cohort study, the absence of data on potential confounding factors can lead to a conclusion bias. Secondly, our inclusion criteria and exclusion criteria would certainly miss some ACLF patients. We excluded patients complicated with acute hemorrhage, as previous studies have elaborated that major bleeding would compromise platelet reactivity,29,30 therefore it would bias the potential prognostic value of TEG-PM in ACLF patients. Even though only six patients were excluded from this entire study, we recognized that prognostic value of TEG-PM in ACLF precipitated by acute upper gastrointestinal bleeding needs further study. Patients with steroids using prior to enrollment would also be excluded due to undetermined effects of steroids on platelet reactivity. Although no patient was excluded for this exclusion in the validation cohort, we recognized that the effects of steroids on platelet reactivity need investigation in ACLF patients with severe alcoholic hepatitis or autoimmune hepatitis both of which are indications for steroids therapy. Finally, our patients were all Chinese ethnic.
In summary, this multicenter, prospective cohort study was to explore and validate the prognostic role of TEG and TEG-PM in chronic liver disease patients with acute severe liver injury. And multiple biosamples were collected to elucidate the mechanism underlying ADP-hyporesponsive platelets and to explore novel therapeutic approaches for ACLF.
Abbreviations
ACLF, acute-on-chronic liver failure; ALI, acute hepatic injury; APASL, Asian Pacific Association for the Study of the Liver; EASL, European Association for the Study of the Liver; HBV, hepatitis B virus; LT, liver transplantation; TEG, thromboelastography; TEG-PM, thromboelastography-platelet mapping.
Data Sharing Statement
The data are kept in private access mode because other researches based on the dataset are still being processed. However, we are ready to provide the credentials to interested readers upon request until the dataset is released.
Acknowledgment
We thank the participants for the contributions to this study: Hepatology Unit, Department of Infectious Diseases, Nanfang Hospital, Southern Medical University—Guotao Zhong, Xiaoge Bei; Department of Infectious Disease, Hunan Key Laboratory of Viral Hepatitis, Xiangya Hospital, Central South University—Zebin Huang; Department of Hepatology, Mengchao Hepatobiliary Hospital of Fujian Medical University-Baorong Liu, Haibing Gao; Infectious Disease Center, The First Affiliated Hospital of Xinjiang Medical University-Xinyi Zhou.
Funding
This work was supported by the National Science and Technology Major Project (2018ZX10723203, 2018ZX10302206), National Natural Science Foundation of China (82070650), National Key Research and Development Program of China (2017YFC0908100), Local Innovative and Research Teams Project of Guangdong Pearl River Talents Program (2017BT01S131), Clinical Research Program of Nanfang Hospital, Southern Medical University (2020CR026), Clinical Research Startup Program of Southern Medical University by High-level University Construction Funding of Guangdong Provincial Department of Education (LC2019ZD006), President Foundation of Nanfang Hospital, Southern Medical University (2019Z003) and Key-Area Research and Development Program of Guangdong Province (2019B020227004).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Moreau R, Gao B, Papp M, Bañares R, Kamath PS. Acute-on-chronic liver failure: a distinct clinical syndrome. J Hepatol. 2021;75(Suppl 1):S27–s35. doi:10.1016/j.jhep.2020.11.047
2. Gu WY, Xu BY, Zheng X, et al. Acute-on-Chronic Liver Failure in China: rationale for Developing a Patient Registry and Baseline Characteristics. Am J Epidemiol. 2018;187(9):1829–1839.
3. Liu J, Tan Y, Zhang J, et al. C5aR, TNF-α, and FGL2 contribute to coagulation and complement activation in virus-induced fulminant hepatitis. J Hepatol. 2015;62(2):354–362.
4. Bajaj JS, O’Leary JG, Lai JC, et al. Acute-on-Chronic Liver Failure Clinical Guidelines. Am J Gastroenterol. 2022;117(2):225–252.
5. Sarin SK, Kedarisetty CK, Abbas Z, et al. Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific Association for the Study of the Liver (APASL) 2014. Hepatol Int. 2014;8(4):453–471.
6. Liver Failure and Artificial Liver Group. Chinese Society of Infectious Diseases, Chinese Medical Association, et al. [Guideline for diagnosis and treatment of liver failure]. Zhonghua Gan Zang Bing Za Zhi. 2019;27(1):18–26.
7. O’Leary JG, Greenberg CS, Patton HM, Caldwell SH. AGA Clinical Practice Update: coagulation in Cirrhosis. Gastroenterology. 2019;157(1):34–43.e31.
8. Wu T, Li J, Shao L, et al. Development of diagnostic criteria and a prognostic score for hepatitis B virus-related acute-on-chronic liver failure. Gut. 2018;67(12):2181–2191.
9. Moreau R, Jalan R, Gines P, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013;144(7):
10. Saraiva IE, Ortiz-Soriano VM, Mei X, et al. Continuous renal replacement therapy in critically ill patients with acute on chronic liver failure and acute kidney injury: a retrospective cohort study. Clin Nephrol. 2020;93(4):187–194. doi:10.5414/CN109983
11. Huang K, Ji F, Xie Z, et al. Artificial liver support system therapy in acute-on-chronic hepatitis B liver failure: classification and regression tree analysis. Sci Rep. 2019;9(1):16462.
12. Chen T, Yang Z, Choudhury AK, et al. Complications constitute a major risk factor for mortality in hepatitis B virus-related acute-on-chronic liver failure patients: a multi-national study from the Asia-Pacific region. Hepatol Int. 2019;13(6):695–705.
13. Magaz M, Baiges A, Hernandez-Gea V. Precision medicine in variceal bleeding: are we there yet? J Hepatol. 2020;72(4):774–784.
14. Blasi A, Patel VC, Adelmeijer J, et al. Mixed Fibrinolytic Phenotypes in Decompensated Cirrhosis and Acute-on-Chronic Liver Failure with Hypofibrinolysis in Those With Complications and Poor Survival. Hepatology. 2020;71(4):1381–1390.
15. Qi T, Zhu C, Lu G, et al. Elevated D-dimer is associated with increased 28-day mortality in acute-on-chronic liver failure in China: a retrospective study. BMC Gastroenterol. 2019;19(1):20.
16. Ouyang R, Li H, Xia J, et al. Lower platelet counts were associated with 90-day adverse outcomes in acute-on-chronic liver disease patients. Ann Palliat Med. 2021;1:854.
17. Craft RM, Chavez JJ, Bresee SJ, Wortham DC, Cohen E, Carroll RC. A novel modification of the Thrombelastograph assay, isolating platelet function, correlates with optical platelet aggregation. J Lab Clin Med. 2004;143(5):301–309.
18. Lausen B, Schumacher M. Evaluating the effect of optimized cutoff values in the assessment of prognostic factors. Comput Stat Data Anal. 1996;21:307–326.
19. Yang Y, Chen W, Pan Y, et al. Effect of ticagrelor versus clopidogrel on platelet reactivity measured by thrombelastography in patients with minor stroke or TIA. Aging. 2020;12(20):20085–20094.
20. Li Y, Zhang X, Guo Z, et al. Standard vs. modified antiplatelet therapy based on thromboelastography with platelet mapping for preventing bleeding events in patients undergoing stent-assisted coil for a ruptured intracranial aneurysm. Front Neurol. 2020;11:615829.
21. Chen WH, Lee PY, Ng W, Tse HF, Lau CP. Aspirin resistance is associated with a high incidence of myonecrosis after non-urgent percutaneous coronary intervention despite clopidogrel pretreatment. J Am Coll Cardiol. 2004;43(6):1122–1126.
22. Bliden KP, DiChiara J, Tantry US, Bassi AK, Chaganti SK, Gurbel PA. Increased risk in patients with high platelet aggregation receiving chronic clopidogrel therapy undergoing percutaneous coronary intervention: is the current antiplatelet therapy adequate? J Am Coll Cardiol. 2007;49(6):657–666.
23. Tantry US, Bliden KP, Gurbel PA. Overestimation of platelet aspirin resistance detection by thrombelastograph platelet mapping and validation by conventional aggregometry using arachidonic acid stimulation. J Am Coll Cardiol. 2005;46(9):1705–1709.
24. Kim K, Shin EK, Chung JH, Lim KM. Arsenic induces platelet shape change through altering focal adhesion kinase-mediated actin dynamics, contributing to increased platelet reactivity. Toxicol Appl Pharmacol. 2020;391:114912.
25. Bender M, Palankar R. Platelet shape changes during thrombus formation: role of actin-based protrusions. Hamostaseologie. 2021;41(1):14–21.
26. Scheller I, Beck S, Göb V, et al. Thymosin β4 is essential for thrombus formation by controlling the G-actin/F-actin equilibrium in platelets. Haematologica. 2021.
27. Palankar R, Kohler TP, Krauel K, Wesche J, Hammerschmidt S, Greinache A. Platelets kill bacteria by bridging innate and adaptive immunity via platelet factor 4 and FcγRIIA. J Thromb Haemost. 2018;16(6):1187–1197.
28. Gros A, Syvannarath V, Lamrani L, et al. Single platelets seal neutrophil-induced vascular breaches via GPVI during immune-complex-mediated inflammation in mice. Blood. 2015;126(8):1017–1026.
29. Wohlauer MV, Moore EE, Thomas S, et al. Early platelet dysfunction: an unrecognized role in the acute coagulopathy of trauma. J Am Coll Surg. 2012;214(5):739–746.
30. Simmons JW, Powell MF. Acute traumatic coagulopathy: pathophysiology and resuscitation. Br J Anaesth. 2016;117(suppl3):iii31–iii43.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.