")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Design, Development, and Evaluation of the Blood Collection Management Workstation
Authors Huang H , Yin H, Xu W, Wang Q, Xiao M , Zhao Q
Received 3 August 2022
Accepted for publication 18 October 2022
Published 31 October 2022 Volume 2022:15 Pages 2015—2022
DOI https://doi.org/10.2147/RMHP.S384866
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Huanhuan Huang,1 Huimei Yin,2 Wenxin Xu,1 Qi Wang,3 Mingzhao Xiao,4 Qinghua Zhao1
1Department of Nursing, the First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Neurology, the First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 3Department of Medical Informatics, the First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 4Department of Urology, Urologist, the First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Qinghua Zhao, Department of Nursing, the First Affiliated Hospital of Chongqing Medical University, 1st Youyi Road, Chongqing, 400016, People’s Republic of China, Tel +86 023 89012206, Email [email protected]
Purpose: To design and develop a blood collection management workstation with high usability to reduce the risk of preanalytical errors and improve patient safety.
Methods: A five-phase mobile application development lifecycle model (MADLC) and experience-based co-design (EBCD) were used for design and development. Subsequently, the blood collection management workstation was evaluated using the Chinese System Usability Scale (SUS) in a general ward setting from January to June 2021.
Results: It was used on 2593 in-patients who underwent phlebotomy with 12,378 tubes being labeled. The rate of errors and meantime for blood sampling were decreased compared with the same period in the previous year. A total of 14 nurses agreed to participate in the evaluation, and the overall raw SUS score was 69.26 ± 10.39, which indicated above average results.
Conclusion: The blood collection management workstation has shown the potential to decrease errors and improve working efficiency in a clinical setting. The study also identified some weaknesses, which will be amended in the future.
Keywords: patient safety, identification, pre-analytical phase, phlebotomy, technology
Introduction
Biological specimens play an irreplaceable role in the diagnosis, assessment, and monitoring of disease in precision medicine.1 Specimens’ quality and accreditation are of great significance to ensure reliable results and also promote patient safety. Despite evidence of highly accurate test results, many hurdles remain to be overcome.2 Experts and scholars gradually reached a consensus that unqualified or inappropriate specimens were mainly generated from the pre-analytical phase (PRE),3,4 which encompassed all procedures from the clinician’s request to the laboratory.5 It was reported that PRE accounted for 46% to 84.5% of total errors, and a high error rate (18.5–47%) was found in the PRE.6 Venous blood sampling (phlebotomy) is the most common invasive procedure performed in patient care and the most common source of preanalytical variability.4 Therefore, it is essential to raise awareness and take immediate improvements to manage it in the PRE.7
Although commonly considered as a simple clinical practice, the standard procedure of a phlebotomy is complex and contains up to 15 steps in the PRE,8 from the initial preparing to sending the properly labeled blood collection tubes to the appropriate laboratories.9 A study conducted in 12 European countries by the European Federation of Clinical Chemistry and Laboratory Medicine Working Group for the Preanalytical Phase (EFLM WG-PRE) found that the highest risk steps during a phlebotomy in the PRE were patient identification and subsequent tube labeling.10,11 Medical errors have been considered as the third leading cause of death in the United States, and identification errors are prominent.12 Improper identification leads to delayed diagnoses and treatments, additional tests and costs, or even severe transfusion reactions that threaten life. Since 2002, the Joint Commission named improving the accuracy of patient identification as the first of its National Patient Safety Goals.13 There is room for improvement, and harmonization of the preanalytical step is necessary.
Recently, emerging innovative technologies, such as barcodes, radio frequency identification (RFID) chips, and even fingerprints,14 have shown a promising scenario for nurses, which could improve patient safety and nursing efficiency.15,16 Besides, at the hospital level, it was demonstrated that information construction levels had a large impact on the performance of caring quality.17 Automation and standard protocols in the PRE are fundamental to support or extend clinical nursing.18 Nevertheless, in each health system, there may be different workloads, competencies, and job specifications.19 Thus, a tailor-made management process and technology assists are necessary in each context. In this study, we aimed to design and develop a blood collection management workstation to improve phlebotomy efficiency and decrease identification errors in the general wards.
Methods
Design and Management Part
Design
The blood collection management workstation was designed and developed under the guidance of the five phases of the mobile application development lifecycle model (MADLC),20 which brought out a six-step lifecycle (Identification, Design, Development, Prototyping, Testing, and Maintenance) for software development. This method has been previously used to develop a mobile application for student-teacher cooperation.21 In addition, the experience-based co-design, which emphasized the cooperative relationships between end-users and researchers,22 was applied to design a user-centered tool. All stakeholders, which included designers from the hospital’s department of medical informatics, clinical nurses, nursing assistants, and managers, participated in the design and development process by gathering their responses and suggestions.23 The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)24 guidelines were followed. The Ethics Committee of the First Affiliated Hospital of Chongqing Medical University where the current study took place reviewed and approved the study (Approval No. 20211001). All participants provided written informed consent.
Methodology
In the identification phase (I), ideas were collected from existing literature and guidelines. Using techniques before and during the process of venous blood was recognized as best practice,25,26 and recommended by the EFLM.27 Thus, there was a need to design a novel system for phlebotomy. In the design phase (II), the expected functions were collected, discussed, and identified. The architecture of the system was created, and the prototypes and related modules were initially defined by software developers. In the development phase (III), different prototypes and similar modules were coded and integrated. In the prototyping phase (IV), the required functions were tested and analyzed, and continued changes were implemented according to the feedback of the interactions between the designers and related users. The testing phase (VI) was the most important stage of development. The prototype’s suitability, feasibility, and usability were assessed in the laboratory and subsequently evaluated in a general ward setting after the protocol was reviewed and approved by the hospital’s research ethics committee.
Data Collection and Analysis
The raw data of the time for blood sampling (referred to the procedure from patient identification to sample checkout) and reported errors were collected directly from the blood collection management workstation and Hospital Information System (HIS). The rate and meantime were provided to assess the difference in the performance of a phlebotomy with the same period in the previous year (from January to June 2020).
Evaluation Part
Design
This descriptive study had two measurement points in one department. The blood collection management workstation was applied in the Department of Neurology to evaluate its performance in general ward settings from January to June 2021. Mixed-methods were applied to evaluate its usability.
Methods
Setting
The department was selected via convenience sampling, with 208 beds, and was divided into three wards (two general units and one intensive care unit). The department was a large, national key clinical specialty, and provincial key laboratory of neurobiology as well as focused on basic and clinical research of cerebrovascular diseases, epilepsy, central nervous system infections, and neurodegenerative diseases. It was estimated that the annual number of hospitalized patients was more than 7000. In this study, two workstations were installed in two general wards and the eight most used types of serum separating tubes were applied.
Participants
A total of 18 registered nurses from in two general wards participated. The fixed staff allocations were 13 for the day shift, two for the night shift, two for the overnight shift, and one for the emergency shift. Those who could correctly understand the contents of the questionnaire and had used the blood collection management workstation were included in the investigation.
Tools
Usability, recognized as a key indicator of application performance, has been included in the evaluation criteria or guidance documents for health applications or digital tools by many industries or organizations.28–30 It referred to the extent to which the system, product, or service could be used effectively, efficiently, and satisfactorily by target users to achieve specific goals in a specific use environment.31 Presently, methods are used to evaluate the usability of application programs. Among these, the System Usability Scale (SUS)32 is most widely used.33 In this study, the Chinese System Usability Scale34 was applied, which including 10 items. The content validity and Cronbach’s α were 0.83 and 0.81, respectively.
Responses were scored on a 5-point Likert scale, with a score of 1 for completely disagree and 5 for completely agree. For odd numbers items, the score contribution was the scale position minus 1. For even numbers items, the score contribution was 5 minus the scale position. The overall SUS score contribution was the sum of the scores of each item multiplied by 2.5, which ranged from 0 (very poor perceived usability) to 100 (excellent perceived usability). According to Usability.gov (https://measuringu.com/interpret-sus-score/, accessed on 10 September 2021), a raw SUS score above 68 was above average.35 Moreover, after the scale, there was an open-ended question that asked the limitations of the blood collection platform. This method had been previously applied in designing a bed-cleaning mobile application by Hung et al.36
Data Collection and Analysis
Data were distributed electronically via a free questionnaire website (https://www.wjx.cn/). The link to the questionnaire along with posters that promoted the study was sent to all the participants. To ensure the quality of the study, each IP address was only allowed to submit once after all the questions had been completed. SPSS version 26.0 was used to analyze the data. Averages, standard deviations, minimum and maximum scores, and percentiles were used for descriptive statistics. Content analysis was conducted on the answers to the open-ended question.
Results
Characterization of the Workstation
The blood collection management workstation was a moveable tool used for the patients or at any phlebotomy point for patient identification, tube labeling, and sample management in the pre-analytical phase. It mainly consisted of six components, such as the color touch screen display interface, label print port, exit and entrance of tubes, storage, and sorting drawers. An overview of the workstation is shown in Figure 1. In addition, the blood collection management workstation was a closed system linked to the Hospital Information System (HIS), nurse station, and Laboratory Information System (LIS). It could identify patients and their required tests by Radio Frequency Identification Devices (RFID) and barcode reading technologies, provide automatically print and label tubes tasks, and support instant record and upload data. Moreover, the tool also required face recognition to confirm the practice qualification and ensure the safety of the transfer process. In general, these technologies effectively shortened the workflow. The key workflows are shown in Figure 2.
 |
Figure 1 An overview of the blood collection management workstation. |
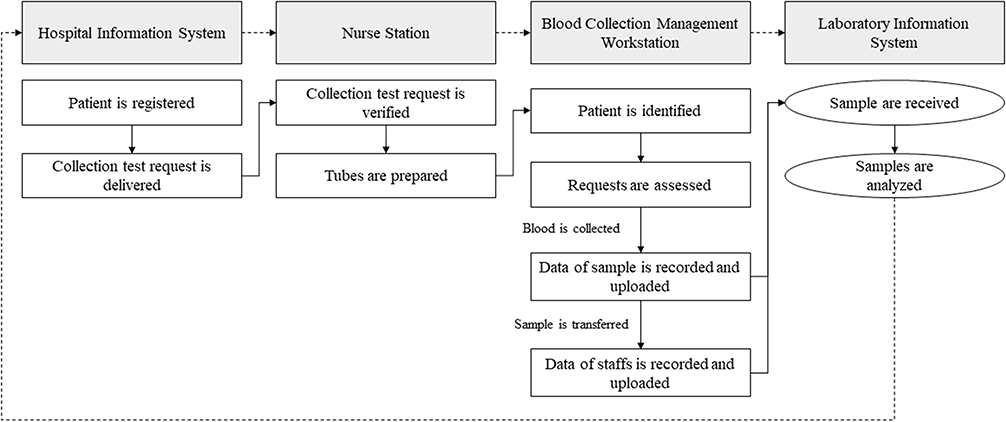 |
Figure 2 The key workflows of the blood collection management workstation. |
Management of the Workstation
The blood collection management workstation was used for 2593 in-patients who underwent a phlebotomy with 12,378 tubes labeled from January to June 2021. The rate of errors and meantime for blood sampling were decreased compared with the same period in the previous year, as shown in Table 1.
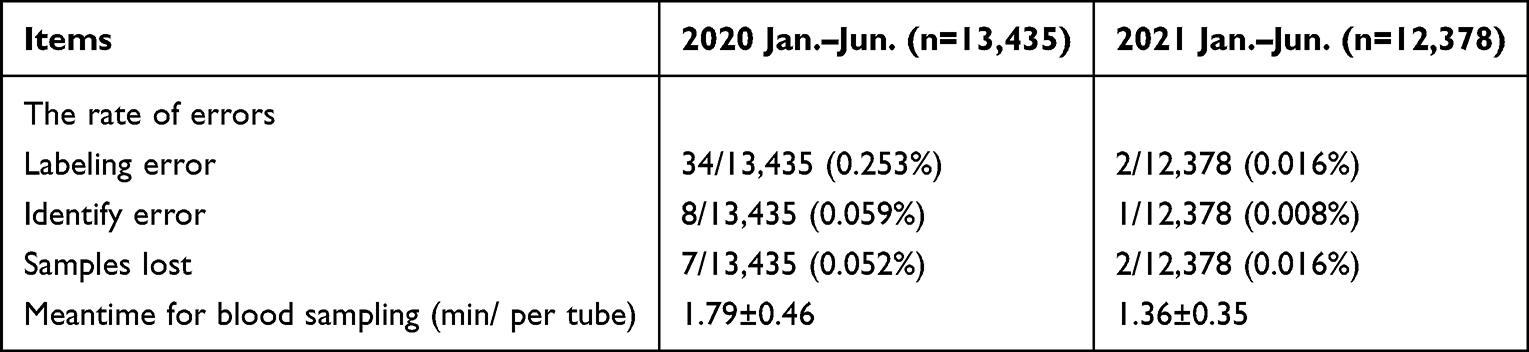 |
Table 1 Comparison of the Rate of Errors and Meantime for Blood Sampling |
Evaluation of the Workstation
A total of 14 nurses agreed to participate in the evaluation. All participants were female, with an average age of 33.07±4.38 years and an average job tenure of 12.71±7.77 years. Most (12, 85.71%) participants had a bachelor’s degree. The overall raw SUS score was (69.26±10.39), which indicated an above average score. The items with the positive response were “I think that I would like to use this system frequently”, “I would imagine that most people would learn to use this system very quickly”, and “I felt very confident using the system.” The item that had the most negative response was “I thought there was too much inconsistency in this system.” Feedback from the open-ended question indicated that respondents were generally satisfied with the system; however, some weaknesses existed and were required to be amended in the future. These mainly included: (a) limited types of tubes that could not meet the clinical need and (b) system-related errors, sometimes tube could not move forward normally (device failure) and had problems in HIS communication.
Discussion
Phlebotomy, a common procedure performed during hospital care, contains multiple steps, and is recognized as a great contributor to pre-analytical phase errors, which depends on correct identification and labeling.37 A specimen’s quality and accreditation depends on multiple phlebotomy processes, in which many steps are undertaken on an exclusively manual basis. Those potential human-related factors pose great challenges to patient safety, and the COVID-19 pandemic has made the shortage of health workers particularly worse.38 Recently, the use of emerging technology (artificial intelligence, the Internet of things, information and communications technology, simulation technology, and e-learning) have shed light on patient safety and nursing management.39,40 In this study, inspired by this concept, we designed and developed a blood collection management workstation with high usability to reduce the risk of preanalytical errors and improve patient safety.
Our results showed that the blood collection management workstation decreased the rate of errors and meantime for blood sampling when compared with the same period in the previous year, which implied that it may be an important tool for ensuring patient safety and enhancing efficiency in the pre-analytical process. These results were consistent with another innovative device named ProTube.41 In contrast, technology was instrumental in pre-analytical error reduction.42 In our study, we used the RFID, barcode reading, and facial recognition technologies in the labeling, and to support nurses in preparing, delivering, documenting, and reviewing procedures, which ensured optimized traceability and also improved workflow to reduce turnaround time. Similar studies also reported positive results. A study observed significant decrease in specimen-labeling errors after application of the RFID to an endoscopy unit.43 Gutierrez et al reported a 83% and 10% reduction in process errors and labor expenses within a payback period of 2.5 years after using the RFID system in blood products tracking, respectively.44
In contrast, the introduction of semi- or full automation was not meant to replace nurses; however, support their specialized skills and release burden.45 Some studies reported that the lack of knowledge of the practice (doctors or nurses) in several parts of the phlebotomy process was also the leading cause of error in the pre-analytical phase.46,47 Another national study revealed that the knowledge on phlebotomy among Chinese nurses was unsatisfactory in some areas.48 Thus, although innovative technology is required, standardized phlebotomy education programs were also highlighted. Furthermore, nurse shortage, brain drain, and the lack of career advancement were persistent issues in China and other middle- and low-income countries.49 Thus, emerging technologies could be leveraged to support professional health workers or non-specialists to increase workforce capacity for existing health systems in low-resource settings.
The results of the system’s evaluation were encouraging. The overall raw SUS score was (69.26±10.39), which indicated an above average score. Scholars reported that usability was an essential element for system development and eventual acceptance by target users, such as patients and healthcare workers. Furthermore, it should be used to guide the development of applications in the health field.33 However, we also identified some weaknesses. The item “I thought there was too much inconsistency in this system” had the lowest score, and participants repeatedly mentioned that the types of the tubes were limited. Due to the variety of tubes manufacturer and development of manufacturers, up to 25 different types of tubes are used in the clinical setting. Although only eight of the most used types of serum separating tubes were included, further modification of the system is still required. Besides, our study only included female nurses with bachelor ‘s degree from one comprehensive hospital, which may create certain bias. A study investigated the physicians’ gender and their performance on electronic health records and showed that females reported a significant higher level of SUS scores50 compared to males. In addition, education level, age, and working experience were also factors that influenced the SUS scores.51 Thus, understanding the feedback from different stakeholders is necessary to continually improve the blood collection management workstation.
Overall, this study has some limitations. First, the blood collection management workstations were only applied in one department for half a year. Thus, additional data are required to further increase multiplicity and enhance conclusion consistency. Second, the participants in the system evaluation part were all female nurses, which may result in bias. Future studies should include more users. Third, this was the first system designed for pre-analytical phase management in a general department setting. Although the system was developed through multi-iterative process, both inter- and intra-rater reliabilities and usability assessments of the products is required before public use.
Implications for Policy, Practice, and Research
Phlebotomy management in the pre-analytical phase is of great significance to patient safety. However, the heterogeneity of knowledge and shortage of medical workers often hinder major healthcare reforms that potentiate major leaps in service delivery accuracy and efficiencies. Technologies should support nurses in preparing, delivering, documenting, and reviewing procedures. Therefore, we hope that our work could evoke further discussions and initiatives on the development and implementation of innovative technologies to provide clinical solutions.52 In addition, we also highlight that, tools are always just a booster for clinical work and could never replace nurses. Thus, nurse leaders have an obligation to provide standard and evidence-based strategies to educate and train nurses to promote specialized skills.
Conclusion
In this study, we designed, developed, and evaluated the blood collection management workstation, which showed potential to decrease errors and improve working efficiency in a clinical setting. Although some weaknesses are to be improved in future versions, the system is a stepping-stone to future efforts seeking to empower clinical workers with technology. We hope that data from this study will provide health care managers with a new conception of how technologies can support nurses in preparing, delivering, documenting, and reviewing during clinical care.
Acknowledgments
The authors would like to thank supports provided by Chong Hu and Juan Liu.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lippi G, Bassi A, Bovo C. The future of laboratory medicine in the era of precision medicine. J Lab Precision Med. 2016;1(3):7. doi:10.21037/jlpm.2016.12.01
2. Lippi G, Plebani M. A Six-Sigma approach for comparing diagnostic errors in healthcare-where does laboratory medicine stand? Ann Transl Med. 2018;6(10):180. doi:10.21037/atm.2018.04.02
3. Fei Y, Kang F, Wang W, et al. Preliminary probe of quality indicators and quality specification in total testing process in 5753 laboratories in China. Clin Chem Lab Med. 2016;54(8):1337–1345. doi:10.1515/cclm-2015-0958
4. Lippi G, Baird GS, Banfi G, et al. Improving quality in the preanalytical phase through innovation, on behalf of the European Federation for Clinical Chemistry and Laboratory Medicine (EFLM) Working Group for Preanalytical Phase (WG-PRE). Clin Chem Lab Med. 2017;55(4):489–500. doi:10.1515/cclm-2017-0107
5. Carey RB, Bhattacharyya S, Kehl SC, et al. Practical Guidance for Clinical Microbiology Laboratories: implementing a Quality Management System in the Medical Microbiology Laboratory. Clin Microbiol Rev. 2018;31(3):e00062–17. doi:10.1128/CMR.00062-17
6. Lee NY. Reduction of pre-analytical errors in the clinical laboratory at the University Hospital of Korea through quality improvement activities. Clin Biochem. 2019;70:24–29. doi:10.1016/j.clinbiochem.2019.05.016
7. van Dongen-Lases EC, Cornes MP, Grankvist K, et al. Patient identification and tube labelling - a call for harmonisation. Clin Chem Lab Med. 2016;54(7):1141–1145. doi:10.1515/cclm-2015-1089
8. National Health Commission of the People’s Republic of China. Guidelines of venous blood specimen collection; 2020. Available from: http://www.nhc.gov.cn/wjw/s9492/202004/31b4fa14ee174bb1999142525ceba608/files/fd630f2e64cd4060aae826e07d00f562.pdf.
9. Lima-Oliveira G, Lippi G, Salvagno GL, Montagnana M, Picheth G, Guidi GC. The effective reduction of tourniquet application time after minor modification of the CLSI H03-A6 blood collection procedure. Biochem Med (Zagreb). 2013;23(3):308–315. doi:10.11613/bm.2013.037
10. Cornes M, Ibarz M, Ivanov H, Grankvist K. Blood sampling guidelines with focus on patient safety and identification - a review. Diagnosis. 2019;6(1):33–37. doi:10.1515/dx-2018-0042
11. Simundic AM, Church S, Cornes MP, et al. Compliance of blood sampling procedures with the CLSI H3-A6 guidelines: an observational study by the European Federation of Clinical Chemistry and Laboratory Medicine (EFLM) working group for the preanalytical phase (WG-PRE). Clin Chem Lab Med. 2015;53(9):1321–1331. doi:10.1515/cclm-2014-1053
12. Makary MA, Daniel M. Medical error-The third leading cause of death in the US. BMJ. 2016;353:i2139. doi:10.1136/bmj.i2139
13. Huang H, Xiao L, Chen Z, et al. A National Study of Patient Safety Culture and Patient Safety Goal in Chinese Hospitals. J Patient Saf. 2022. doi:10.1097/PTS.0000000000001045
14. Sohn JW, Kim H, Park SB, et al. Clinical Study of Using Biometrics to Identify Patient and Procedure. Front Oncol. 2020;10:586232. doi:10.3389/fonc.2020.586232
15. Lee TY, Sun GT, Kou LT, Yeh ML. The use of information technology to enhance patient safety and nursing efficiency. Technol Health Care. 2017;25(5):917–928. doi:10.3233/THC-170848
16. Ruppel H, Funk M. Nurse-Technology Interactions and Patient Safety. Crit Care Nurs Clin North Am. 2018;30(2):203–213. doi:10.1016/j.cnc.2018.02.003
17. Duan M, Kang F, Zhao H, et al. Analysis and evaluation of the external quality assessment results of quality indicators in laboratory medicine all over China from 2015 to 2018. Clin Chem Lab Med. 2019;57(6):812–821. doi:10.1515/cclm-2018-0983
18. Peck Palmer OM, Wheeler SE, Plebani M, Patterson PD, Korpi-Steiner NL, Martin C. Recognition of the Prehospital Preanalytical Phase: collaborative Efforts between Laboratory Medicine and Emergency Medicine to Ensure Quality Testing. Clin Chem. 2020;66(8):998–1005. doi:10.1093/clinchem/hvaa140
19. Bellini C, Guerranti R, Cinci F, Milletti E, Scapellato C. Defining and Managing the Preanalytical Phase With FMECA: automation and/or “Human” Control. Hum Factors. 2020;62(1):20–36. doi:10.1177/0018720819874906
20. Vithani T, Kumar A, Rajesh NG, Nandhakumar S. Modeling the mobile application development lifecycle. Toxicology Reports. 2014;1:596–600. doi:10.1016/j.toxrep.2014.08.006
21. Strandell-Laine C, Leino-Kilpi H, Löyttyniemi E, et al. A process evaluation of a mobile cooperation intervention: a mixed methods study. Nurse Educ Today. 2019;80:1–8. doi:10.1016/j.nedt.2019.05.037
22. Raynor DK, Ismail H, Blenkinsopp A, Fylan B, Armitage G, Silcock J. Experience-based co-design-Adapting the method for a researcher-initiated study in a multi-site setting. Health Expect. 2020;23(3):562–570. doi:10.1111/hex.13028
23. Greenhalgh T, Hinton L, Finlay T, et al. Frameworks for supporting patient and public involvement in research: systematic review and co-design pilot. Health Expectations. 2019;22(4):785–801. doi:10.1111/hex.12888
24. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
25. Giavarina D, Lippi G. Blood venous sample collection: recommendations overview and a checklist to improve quality. Clin Biochem. 2017;50(10–11):568–573. doi:10.1016/j.clinbiochem.2017.02.021
26. Jain S, Chraiti MN, Pittet D, Mclaws ML. Blood collection guidelines for inpatients and outpatients, home-based care and long-term care facilities. J Hospital Infection. 2020;104(4):600–602. doi:10.1016/j.jhin.2019.10.017
27. Simundic AM, Bölenius K, Cadamuro J, et al. Joint EFLM-COLABIOCLI recommendation for venous blood sampling. Ann Biol Clin (Paris). 2019;77(2):131–154. doi:10.1684/abc.2019.1419
28. NHS Digital. How we assess health apps and digital tools; 2019. Available from: https://digital.nhs.uk/services/nhs-apps-library/guidance-for-health-app-developers-commissioners-and-assessors/how-we-assess-health-apps-and-digital-tools.
29. the Medicines and Healthcare products Regulatory Agency. Applying Human Factors and Usability Engineering to Medical Devices. U.S. Food and Drug Administration; 2018. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/applying-human-factors-and-usability-engineering-medical-devices.
30. ORCHA. Health App Reviews & Prescription Services. Available from: https://www.orcha.co.uk/about-us/.
31. Maramba I, Chatterjee A, Newman C. Methods of usability testing in the development of eHealth applications: a scoping review. Int J Med Inform. 2019;126:95–104. doi:10.1016/j.ijmedinf.2019.03.018
32. Jordan PW, Thomas B, McClelland IL, Weerdmeester B. Usability Evaluation in Industry. CRC Press; 1996.
33. Klaassen B, van Beijnum BJF, Hermens HJ. Usability in telemedicine systems—A literature survey. Int J Med Inform. 2016;93:57–69. doi:10.1016/j.ijmedinf.2016.06.004
34. Wang Y, Lei T, Liu X. Chinese System Usability Scale: translation, Revision, Psychological Measurement. Int J Human. 2020;36(10):953–963. doi:10.1080/10447318.2019.1700644
35. Lewis JR. The System Usability Scale: past, Present, and Future. Int J Human. 2018;34(7):577–590. doi:10.1080/10447318.2018.1455307
36. Hung LC, Yang JY, Chen MC, Chang HL, Ku CY, Hou TW. Design and evaluation of the bed-cleaning mobile application. J Nurs Manag. 2020;28(4):771–776. doi:10.1111/jonm.12900
37. Fanshawe TR, Glogowska M, Edwards G, et al. Pre-analytical error for three point of care venous blood testing platforms in acute ambulatory settings: a mixed methods service evaluation. PLoS One. 2020;15(2):e0228687. doi:10.1371/journal.pone.0228687
38. Pawar SD, Kode SS, Keng SS, Tare DS, Abraham P. Steps, implementation and importance of quality management in diagnostic laboratories with special emphasis on coronavirus disease-2019. Indian J Med Microbiol. 2020;38(3& 4):243–251. doi:10.4103/ijmm.IJMM_20_353
39. Huang F, Brouqui P, Boudjema S. How does innovative technology impact nursing in infectious diseases and infection control? A scoping review. Nurs Open. 2021;8(5):2369–2384. doi:10.1002/nop2.863
40. Lu ZX, Qian P, Bi D, et al. Application of AI and IoT in Clinical Medicine: summary and Challenges. Curr Med Sci. 2021;41(6):1134–1150. doi:10.1007/s11596-021-2486-z
41. Piva E, Tosato F, Plebani M. Pre-analytical phase: the automated ProTube device supports quality assurance in the phlebotomy process. Clin Chim Acta. 2015;451(Pt B):287–291. doi:10.1016/j.cca.2015.10.010
42. Norgan AP, Simon KE, Feehan BA, et al. Radio-Frequency Identification Specimen Tracking to Improve Quality in Anatomic Pathology. Arch Pathol Lab Med. 2019;144(2):189–195. doi:10.5858/arpa.2019-0011-OA
43. Francis DL, Prabhakar S, Sanderson SO. A quality initiative to decrease pathology specimen-labeling errors using radiofrequency identification in a high-volume endoscopy center. Am J Gastroenterol. 2009;104(4):972–975. doi:10.1038/ajg.2008.170
44. Gutierrez A, Levitt J, Reifert D, et al. Tracking blood products in hospitals using radio frequency identification: lessons from a pilot implementation. ISBT Sci Series. 2013;8(1):65–69. doi:10.1111/voxs.12015
45. Cherkaoui A, Renzi G, Viollet A, et al. Implementation of the WASPLabTM and first year achievements within a university hospital. Eur J Clin Microbiol Infect Dis. 2020;39(8):1527–1534. doi:10.1007/s10096-020-03872-1
46. Banković Radovanović P. Quality improvement project: reducing non-conformities of the samples for haemostasis testing in a secondary healthcare centre through the nurses’ education in phlebotomy. Biochem Med (Zagreb). 2020;30(2):020708. doi:10.11613/BM.2020.020708
47. Cadamuro J, von Meyer A, Wiedemann H, et al. Hemolysis rates in blood samples: differences between blood collected by clinicians and nurses and the effect of phlebotomy training. Clin Chem Lab Med. 2016;54(12):1987–1992. doi:10.1515/cclm-2016-0175
48. Cai Q, Zhou Y, Yang D. Nurses’ knowledge on phlebotomy in tertiary hospitals in China: a cross-sectional multicentric survey. Biochem Med (Zagreb). 2018;28(1):10703. doi:10.11613/BM.2018.010703
49. Turale S, Nantsupawat A. Clinician mental health, nursing shortages and the COVID-19 pandemic: crises within crises. Int Nurs Rev. 2021;68(1):12–14. doi:10.1111/inr.12674
50. Khairat S, Coleman C, Ottmar P, Bice T, Koppel R, Carson SS. Physicians’ gender and their use of electronic health records: findings from a mixed-methods usability study. J Am Med Inform Assoc. 2019;26(12):1505–1514. doi:10.1093/jamia/ocz126
51. Wang SW, Chiou CC, Su CH, et al. Measuring Mobile Phone Application Usability for Anticoagulation from the Perspective of Patients, Caregivers, and Healthcare Professionals. Int J Environ Res Public Health. 2022;19(16):10136. doi:10.3390/ijerph191610136
52. Ng ZQP, Ling LYJ, Chew HSJ, Lau Y. The role of artificial intelligence in enhancing clinical nursing care: a scoping review. J Nurs Manag. 2021. doi:10.1111/jonm.13425
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.