")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Depressive Symptoms in Older versus Younger People with Epilepsy: Findings from an Integrated Epilepsy Self-Management Clinical Research Dataset
Authors Khalid Z, Momotaz H , Briggs F , Cassidy KA , Chaytor NS , Fraser RT, Janevic MR , Jobst B, Johnson EK, Scal P, Spruill TM, Wilson BK, Sajatovic M
Received 14 August 2019
Accepted for publication 1 November 2019
Published 3 December 2019 Volume 2019:12 Pages 981—988
DOI https://doi.org/10.2147/JMDH.S227184
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Zaira Khalid,1 Hasina Momotaz,2 Farren Briggs,3 Kristin A Cassidy,1,2 Naomi S Chaytor,4 Robert T Fraser,5 Mary R Janevic,6 Barbara Jobst,7 Erica K Johnson,8 Peter Scal,9 Tanya M Spruill,10 Betsy K Wilson,2 Martha Sajatovic1,2
1Department of Psychiatry, Case Western Reserve University School of Medicine, University Hospitals Cleveland Medical Center , Cleveland, OH, USA; 2Department of Neurology, Case Western Reserve University School of Medicine, Neurological and Behavioral Outcomes Center, University Hospitals Cleveland Medical Center, Cleveland, OH, USA; 3Department of Population Health and Quantitative Science, School of Medicine, Case Western Reserve University, Cleveland, OH, USA; 4Department of Medical Education and Clinical Sciences, Elson S. Floyd College of Medicine, Washington State University, Spokane, WA, USA; 5Department of Rehabilitation Medicine, University of Washington, Seattle, WA, USA; 6Center for Managing Chronic Disease, University of Michigan School of Public Health, Ann Arbor, MI, USA; 7Department of Neurology, Geisel School of Medicine at Dartmouth, Dartmouth College, Lebanon, NH, USA; 8Health Promotion Research Center, University of Washington, Seattle, WA, USA; 9Department of Pediatrics and Adolescent Health, University of Minnesota, Minneapolis, MN, USA; 10Department of Population Health, NYU School of Medicine, New York, NY, USA
Correspondence: Martha Sajatovic
Prevention Research Center, Case Western Reserve University School of Medicine, University Hospitals Cleveland Medical Center, 10524 Euclid Avenue, Cleveland, OH 44106, USA
Tel +1 216 844-2808
Fax +1 216 844-2742
Email [email protected]
Aim: There are limited data on psychological outcomes in older people with epilepsy (PWE). This analysis, from a large pooled dataset of clinical studies from the Managing Epilepsy Well (MEW) Network, examined clinical variables including depressive symptom severity, quality of life and epilepsy self-management competency among older (age 55+) vs younger (<age 55) PWE. We were particularly interested in differences between older vs younger individuals with clinically significant depression.
Methods: Analyses used baseline data from 9 MEW Network studies and examined demographic and clinical variables. Older vs younger individuals were compared and then we assessed groups with clinically significant depression vs those without clinically significant depression using the PHQ-9 and QOLIE-10 as a measure of quality of life.
Results: The sample included 935 individuals. Compared to younger adults (n=774), the older group (n=161) had a better quality of life (p= 0.041) and more individuals without clinically significant depression (p=0.038). There was a trend for slightly lower depression severity scores (PHQ-9 total) (p=0.07) in the older group and a trend for fewer seizures (p=0.055) in older adults relative to younger adults.
Conclusion: Compared to younger PWE, older PWE have less clinically significant depression and better quality of life. Future research needs to identify possible mechanisms underlying these differences.
Keywords: epilepsy, self-management, depression, quality of life, database
Introduction
Epilepsy has a prevalence of approximately 1.2% in the United States, and in 2015, epilepsy affected roughly 2.9 million adults. Nearly one million of those adults are age 55 years or older.1 Some risk factors for epilepsy are more common as people age including stroke and cardiovascular disease, neurodegenerative disorders, brain tumor and long-term sequelae of alcohol abuse.2
Current demographic trends project a growing number of older individuals with epilepsy (both new-onset cases and those who have long-standing epilepsy)3 and thus, it is important to better understand the clinical features that may occur in later-life among people with epilepsy (PWE), including the presence of common comorbidities like depression. The reported prevalence of depression in PWE varies, with a range of 15–37%.4 Depressive symptoms have a pronounced impact on the quality of life among PWE, greater so than short-term seizure control.5 In general, there are limited data on psychological outcomes in older PWE,3 and little is known on how depressive symptom severity and other clinical characteristics relevant to depression may compare in older vs younger PWE.
This analysis, from a large pooled dataset of clinical studies from the Centers for Disease Control and Prevention (CDC)-funded Managing Epilepsy Well (MEW) Network, examined clinical variables including depressive symptom severity, quality of life and epilepsy self-management competency among older (≥55 years of age) versus younger PWE.6 The limited literature on older PWE suggests that individuals may, over time, learn coping skills that minimize seizure frequency and improve quality of life. We thus expected to find more positive health outcomes in older vs younger PWE. In line with this expectation of better outcomes in older PWE, and in spite of the fact that rates of suicide are higher among older vs younger adults in the United States,7 we expected that suicidality as measured by a standardized depression assessment instrument would be lower in older vs younger PWE.
In younger PWE, there are a variety of risk factors for depression comorbidity including sociodemographic variables such as low income and limited social support as well as epilepsy-specific variables such as poor seizure control or refractory epilepsy.8,9 We were particularly interested in whether the same sociodemographic and epilepsy-specific characteristics that are associated with clinically significant depressive symptom severity in younger PWE are the same in older PWE. We expected that older people, who might learn to self-manage their epilepsy over time, might be less impacted by some social factors, such as income, as a possible risk factor for depression. Taken together, we expected that findings have potential to inform care planning and delivery across the full age range of PWE.
Methods
Overview
This analysis used baseline data from 9 studies of the MEW Network integrated research database (MEW DB), details of which are described elsewhere.10 All studies that were analyzed were approved by local Institutional Review Boards (IRBs) and the integrated dataset infrastructure and analysis was approved by a local IRB. Data access is based upon approval from a MEW DB Steering group composed of representatives from research sites that have contributed to the data pool and with appropriate data use agreements (DUAs) between research institutions.
The pooled MEW DB sample for this analysis included 935 individuals, consisting of 161 older adults (≥55 years; 17.2%), and 774 younger adults (age 18–54 years; 82.8%). We examined baseline demographic variables of self-reported gender, race, marital status, education level, income, as well as standardized rating scales for depressive symptom severity and quality of life in older vs younger individuals and then compared groups with clinically significant depressive symptom severity based on established thresholds on a standardized depression measure (the 9-item Patient Health Questionnaire, the PHQ-9)18 versus those without clinically significant depressive severity in the younger vs older groups.
Studies included in this MEW DB analysis:
HOBSCOTCH
The study evaluated the effects of home-based cognitive and behavioral self-management program to improve memory complaints and quality of life for PWE. The HOBSCOTCH study included 66 adults (age 18–65 years) who had a diagnosis of epilepsy and reported subjective cognitive symptoms.11
FOCUS
The FOCUS program study (Figure out the problem, Observe your routine, Connect your observations and choose a change goal, Undertake a change strategy, Study the results) tested an 8-week hybrid in-person workshop and telephone coaching program to develop self-regulation skills among PWE and a support person (a family member or friend). A pilot study of FOCUS included 21 PWE (age >21 years).12 A subsequent RCT of FOCUS included 159 PWE.13
SMART
Self-management for people with epilepsy and a history of negative health events (SMART) study tested a group-format, remotely delivered (web or telephone) self-management approach in a prospective, 6-month randomized controlled trial that compared SMART vs a 6-month waitlist control in 120 PWE.14
Time
Targeted Self-Management for Epilepsy and Mental Illness (TIME) was tested in a 16-week prospective randomized controlled trial that evaluated TIME vs treatment as usual in 44 PWE.15
FACES
The FACES study looked to identify psychosocial and disease-related factors affecting Chinese American PWE. It included 16 PWE (age ≥18 years) and examined demographic variables such as race, education, gender, relationship status, as well as PHQ-9 scores and number of seizures in the past month.
PEARLS
PEARLS (Program to Encourage Active and Rewarding Lives) in Epilepsy was a prospective, randomized controlled trial of a home-based depression management program, which included 80 adults (age ≥18 years) who had a diagnosis of epilepsy as well as a PHQ-9 score of ≥10.16
PACES
The PACES study was a randomized controlled trial of a self-management program for adults with epilepsy.17 PACES includes both medical and psychosocial self-management in adults (age ≥18 years) with epilepsy.
YESS
Data included a cross-sectional survey administered to inform the implementation of Youth Epilepsy & Successful Self-Management (YESS), an online epilepsy self-management intervention for teens (age 13–19 years), which provides education and teaching regarding interpersonal connections, decision-making and epilepsy self-management skills along with peer support.
Standardized Measures
Standardized rating scales included Quality of Life in Epilepsy (QOLIE-10), the 9-item Patient Health Questionnaire (PHQ-9) for depressive symptoms and the Epilepsy Self-Management Scale (ESMS).
Depression
The PHQ-9 is a self-administered questionnaire that reflects the Diagnostic and Statistical Manual 5 (DSM-5) diagnostic criteria for major depressive disorder.18 Scoring ranges from 0 to 27. A score of 0–4 is considered non-depressed, a score of 5–9 is considered mild depression, a score of 10–14 is considered moderate depression and a score of ≥15 is considered severe depression.18
Quality of Life
The QOLIE-10 is a 10-item questionnaire that has been developed from the original QOLIE-89 to assess various domains of quality of life in PWE including working, social limitations, and worrying about seizures.19 For this analysis, scoring was calibrated on a 1–5 scale with higher scores indicating a worse quality of life.
Epilepsy Self-Management Scale
The ESMS is a 38-item questionnaire that evaluates self-reported epilepsy self-management competency. In addition to a total score, the ESMS is subdivided into 5 sub-scales which are safety, lifestyle, medications, seizures and information management.20 Higher scores indicate greater use of self-management strategies.
Statistical Analysis
Statistical analysis was performed using SPSS software version 22 (IBM Corporation, NY) and SAS (version 9.4, The SAS Institute, Cary, NC); a p-value less than 0.05 was set for statistical significance. We first conducted descriptive statistics of the demographic variables and clinical characteristics comparing older versus younger groups overall (Table 1) and then using the cut-point of ≥10 on the PHQ-9 as indicating clinically significant depressive symptom severity,18 compared the older versus the younger groups without clinically significant depressive symptoms to those with clinically significant depressive symptoms (Table 2). Item 9 on the PHQ-9 evaluates the specific symptom of suicidality. In Tables 1 and 2, continuous variables are presented with mean (standard deviation/SD) and independent samples t-tests/non-parametric Wilcoxon tests; categorical variables were presented with count (percent) and Chi-square tests/Fisher’s exact tests. Spearman correlations and comparisons of standardized rating scores across the sample age groups were conducted using non-parametric methods for categorical variables and ANOVA for continuous variables. Linear regression analyses examined the associations between total PHQ-9 scores and age, both as a continuous and categorical variable (older group versus younger group).
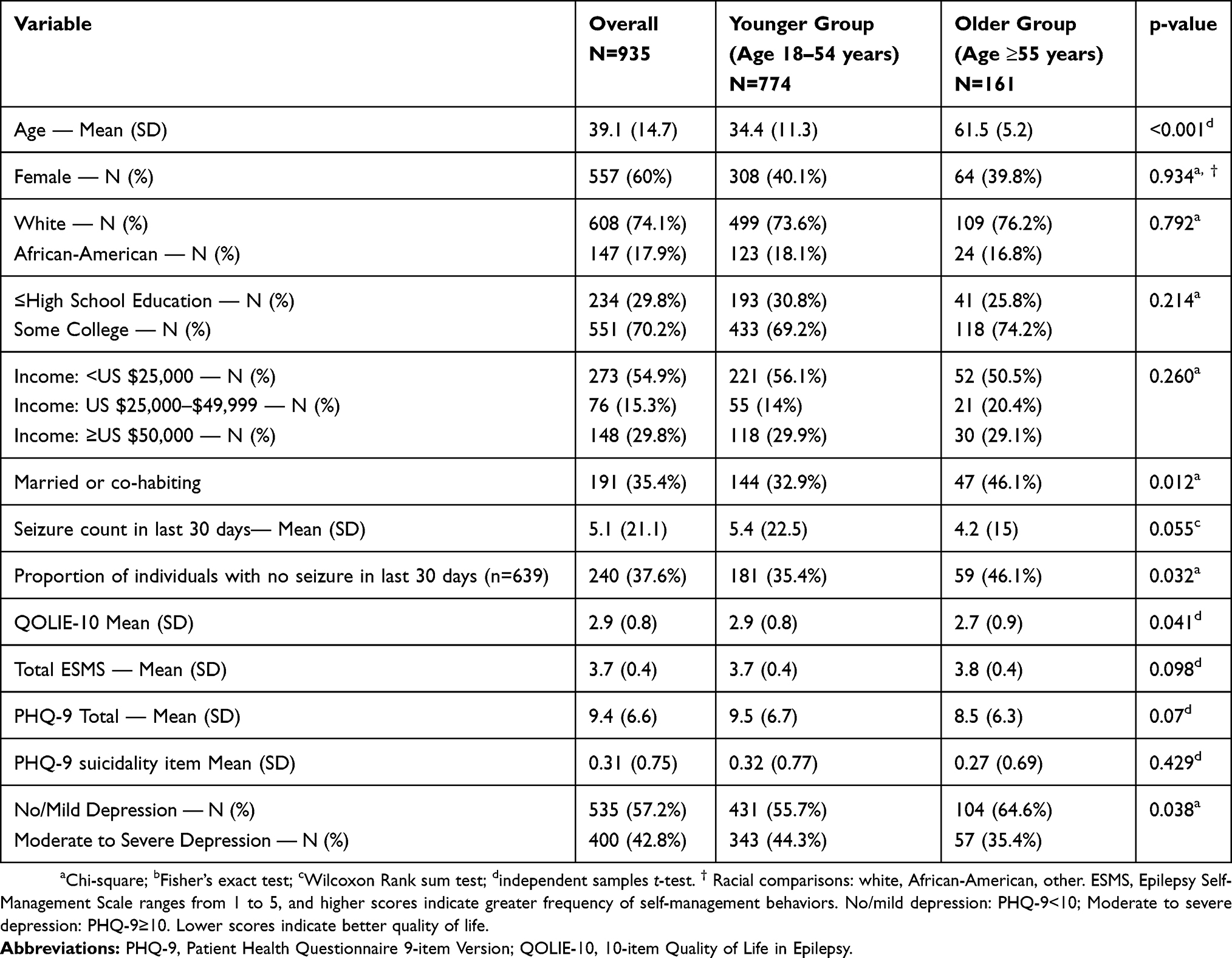 |
Table 1 Comparison of Baseline Demographic and Clinical Variables Between Older (≥55 Years) and Younger (<55 Years) PWE |
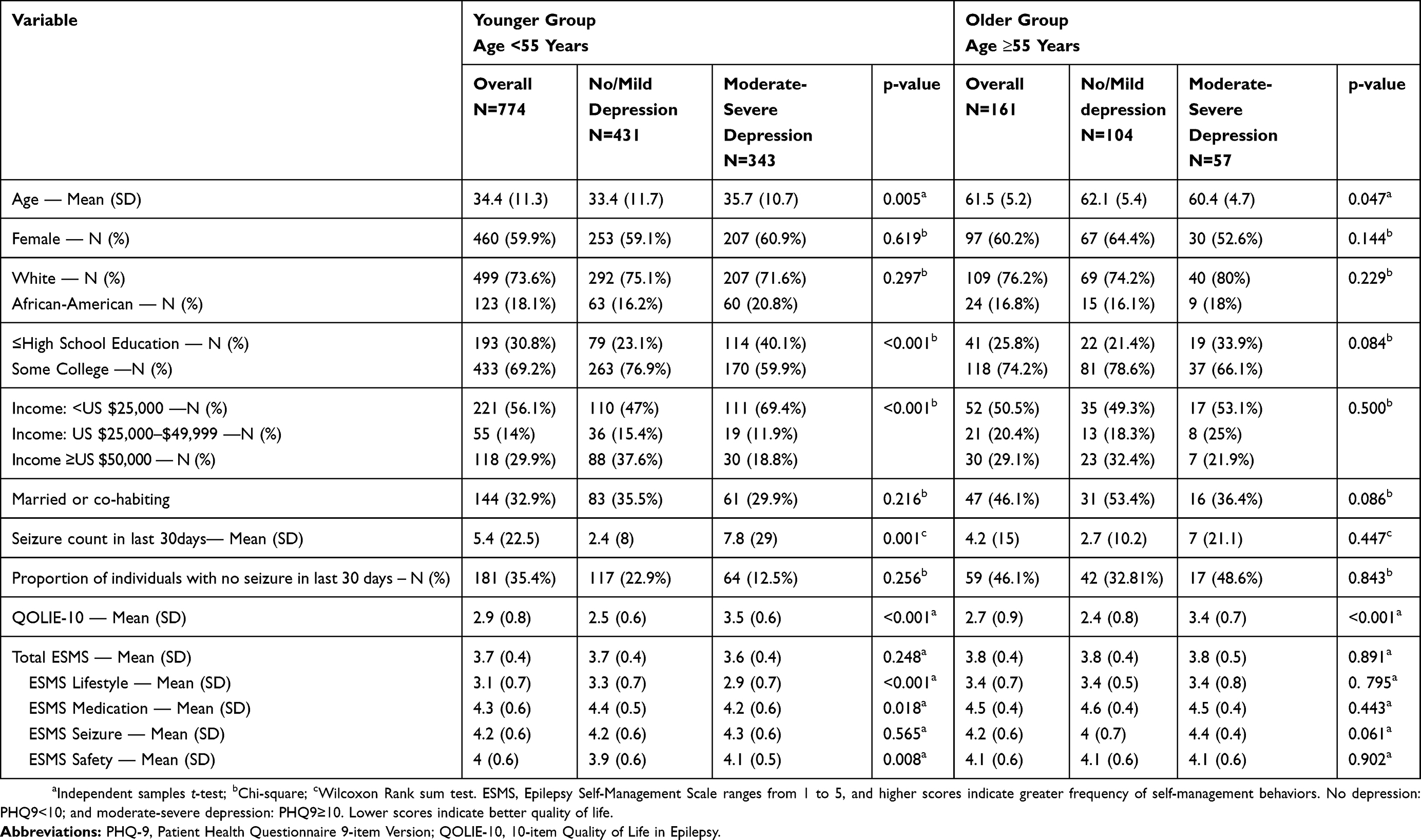 |
Table 2 Comparison of Demographic and Clinical Characteristics of Older (≥55 Years) vs Younger (<55 Years) People with Epilepsy and Clinically Signification Depressive Symptom Severity as Defined by Established Cut-Points on the PHQ-9 |
Results
Overall Sample Descriptive Analysis
As noted in Table 1, the overall mean age of the 935 patients was 39.1 (standard deviation [SD] 14.7 years), 557 (60%) female. The majority were white (N=608, 74.1%), and 17.9% (N=147) were African American. This was a relatively well-educated sample, with 551 PWE (70.2%) having at least some college education. Of this sample, 400 (43%) of individuals had clinically significant depressive symptoms.
Health Outcomes in Younger versus Older PWE
As shown in Table 1, mean age was 61.5 (SD 5.2 years) for older PWE, and 34.4 (SD 11.3 years) for younger PWE. As noted in Table 1, demographic and clinical variables were generally similar; however, the older group had a slightly better quality of life (p=0.041) and fewer individuals with clinically significant depressive symptoms (p=0.038) compared to the younger group. With respect to the suicidality item on the PHQ-9, we found no significant difference between older vs younger PWE. There was a trend for slightly lower depression severity scores (PHQ-9 total) (p=0.07) in the older group, as well as a trend for fewer seizures (p=0.055). Additionally, older patients were more likely to have been seizure free in the past 30 days (p=0.032) and reported significantly better epilepsy self-management competency on the medication-taking (p=0.010) and the lifestyle (p=0.036) sub-domains of the ESMS (data not shown).
Correlates of Depression in Younger versus Older PWE
As shown in Table 2, using established cut-points of depression on the PHQ-9, within the younger age group, those with a lower level of education (p<0.001) and lower income level (p<0.001) had a greater likelihood of clinically significant depressive symptoms. In younger PWE, higher seizure frequency (p<0.001), lower quality of life (p< 0.001) and selected sub-scales of the ESMS (lifestyle p <0.001, medication p=0.018, safety p=0.008) and lifestyle, p=0.036) were also associated with clinically significant depression. Correlations with PHQ-9 total scores in younger individuals included higher PHQ-9 scores in those who were unmarried/not-cohabitating (p=0.049), racial group other than white or African American (p=0.017) and those with lower self-management competency (p=0.013). In the older age group, no demographic or clinical variables were associated with clinically significant depressive symptoms.
Linear regression analyses examining the association between total PHQ-9 scores with age as a continuous variable and with age as a categorical variable (older group versus younger group) identified some significant findings. Bivariate associations between clinical variables and PHQ-9 total scores found that depressive symptom severity was significantly associated with education, income, marital status, seizure frequency, quality of life and epilepsy self-management competency (all p<0.05). However, adjusting for multiple predictors found that only quality of life (total QOLIE-10 p<0.0001) and the lifestyle sub-scale in epilepsy self-management competency (ESMS lifestyle p <0.03) were significant.
Discussion
This analysis of 935 PWE from an integrated dataset of epilepsy self-management studies compared older (age ≥ 55) vs younger (<age 55) individuals on depressive symptom severity, quality of life and epilepsy self-management competency with a particular focus on factors associated with clinically significant depressive symptoms. Consistent with the limited literature and aligned with what we expected to find, our results suggested that older PWE have better quality of life, less severe depressive symptoms, and higher ratings of epilepsy self-management competency in medication-taking and on lifestyle management compared to younger PWE. While there were some demographic and clinical correlates of clinically significant depression in younger PWE, there were no demographic or clinical correlates associated with clinically significant depressive symptoms in the older group.
Both Devinsky and colleagues21 and May and colleagues3 have noted that psychological and emotional constructs in older PWE have not been well studied. Some studies3,22 suggest that people who have lived with epilepsy for many years may learn coping skills over time. Escoffery and colleagues reported a lower seizure count and lower reports of being bothered by seizures in those that were over 50 compared to their younger counterparts.23 This is in line with our findings that note less clinically significant depressive symptoms, better quality of life and some improved epilepsy self-management skills which shows that learning to live with epilepsy is a skill that can be learned and once learned, it translates into improved health. Alternatively, the finding of relatively better functioning and mood in older PWE could be a result of a “survivor effect” in which those PWE who have poorly controlled seizures and more epilepsy-related complications die prematurely or are less likely to participate in research. The lower rate of clinically significant depressive symptoms in older PWE in this sample could also be explained by the overall lower prevalence of depression in elderly populations compared to younger patients in the general public.24
Our analysis findings have potentially important clinical implications given the fact that the number of older PWE appears to be increasing.3 Epilepsy self-management skills and quality of life are key factors that impact the association of age and depressive symptoms. Our data suggest that PWE may become better at managing their health as they get older. The literature on evidence-based epilepsy self-management programs is increasing6 and younger people with epilepsy are clearly ideal targets for epilepsy self-management training. Given that evidence-based epilepsy self-management interventions are a relatively new addition to the treatment armamentarium, it seems likely that at least some of the older PWE in our sample did not have this training in their earlier years, and perhaps had to learn their self-management skills through trial and error. Additionally, it is possible that epilepsy self-management training begun in early life or shortly after an epilepsy diagnosis is first received, could change a variety of health outcomes further downstream into mid-life and beyond, including quality of life and depressive symptoms. Future studies might include evaluation of whether PWE have had exposure to evidence-based epilepsy self-management programs in evaluating whole-health and epilepsy-specific outcomes.
A caveat that needs to be noted is that this dataset provides cross-sectional data; therefore, we are not able to assess if the severity of depression changes over time in the same individual. This dataset also did not provide data regarding the duration or age of onset of epilepsy in these individuals. Other investigators have reported differences within older samples with epilepsy based on late vs early age of onset. May et al found that elderly with late-onset epilepsy had fewer seizures, better tolerance of antiepileptic drugs and less epilepsy-related fears compared to those with more long-standing epilepsy.3
In younger PWE we found several correlates of clinically significant depressive symptom severity including education, income, quality of life, seizure frequency and selected epilepsy self-management domains, while we did not find any significant correlations with clinically significant depressive symptoms in older PWE. It is possible that older PWE may be more likely to have additional supports, such as Medicare coverage which could minimize healthcare access problems that may have attenuated the relationship between socioeconomic variables and health outcomes. It is also possible that some of our older sample had epilepsy that began relatively later in life and this could have contributed to relatively better socioeconomic outcomes in the older group. Epilepsy onset that occurs after educational and career attainment could potentially translate to having retirement savings or financial resources available. Analysis of larger samples of older PWE with varying age of epilepsy onset and varying types of health insurance coverage would be needed to explore this idea.
Given our findings of relatively better health outcomes in older PWE vs younger PWE, it might be reasonable to consider how resilient older individuals who have learned to cope with their illness might potentially help and support those who are earlier in their recovery journey. For example, some MEW Network interventions use Peer Educators or PWE to serve as experiential guides to others in self-management learning.6,15
Other limitations of this study include a small older-adult sample of 161 people with an average age of 61.5 years, which falls on the lower age spectrum of geriatric patients. The data set may not represent those that are “old-old” who present with higher comorbidities. Additionally, those that do participate in clinical research may not represent the full spectrum of people with epilepsy across the age span. There are a number of strengths to off-set these limitations, however including the fact that both younger and older groups of PWE were largely similar in their demographic and clinical variables, aiding in reducing confounding factors. The sample also was racially and ethnically diverse. The later-life focus of our paper does not facilitate conclusions on the youngest adults with epilepsy and indeed, the MEW DB has until recently not had a large sampling of young adults. However, more recently completed research and new research funding from the CDC is expected to substantially expand the MEW Network’s ability to assess and address epilepsy outcomes across the full lifespan.25
In conclusion, this large sample of PWE found that older PWE had less significant depressive symptoms and better quality of life. Future studies need to collect data longitudinally, as well as sample more elderly PWE including the “old-old” and those with more extensive medical comorbidity.
Acknowledgment
Portions of these data were presented at the American Association for Geriatric Psychiatry (AAGP) Annual Meeting, Atlanta, Georgia, USA; March, 2019
Disclosure
KAC reports a grant from the Center for Disease Control, during the conduct of the study. NSC reports personal fees from Eli Lilly, outside the submitted work. BJ reports non-financial support from the Centers for Disease Control and Prevention (CDC), the Defense Advanced Research Projects Agency (DARPA), the Diamond Foundation, Eisai, Inc., the National Science Foundation, Neuropace, Inc., and Sunovion, outside the submitted work. MS reports grants from the Centers for Disease Control and Prevention (CDC), during the conduct of the study; grants from Otsuka, Alkermes, Janssen, the International Society for Bipolar Disorders, the Reuter Foundation, the Woodruff Foundation, the Reinberger Foundation, and the National Institutes of Health (NIH); personal fees from Alkermes, Bracket, Otsuka, Janssen, Neurocrine, Health Analytics, and Frontline Medical Communications; royalties from Springer Press, Johns Hopkins University Press, Oxford Press, UpToDate, compensation for the preparation of continuing medical education (CME) materials from American Physician’s Institute, MCM Education, CMEology, Potomac Center for Medical Education, Global Medical Education, Creative Educational Concepts, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Sapkota S, Kobau R, Pastula DM, et al. Close to 1 million US adults aged 55 years or older have active epilepsy—National Health Interview Survey, 2010, 2013, and 2015. Epilepsy Behav. 2018;87:233–234. doi:10.1016/j.yebeh.2018.06.030
2. Pugh MJ, Knoefel JE, Mortensen EM, et al. New-onset epilepsy risk factors in older veterans. J Am Geriat Soc. 2009;57(2):237–242. doi:10.1111/(ISSN)1532-5415
3. May TW, Pfäfflin BC, Füratsch N, et al. Epilepsy in the elderly: restrictions, fears, and quality of life. Acta Neurol Scand. 2014;131:176–186. doi:10.1111/ane.12317
4. Fiest KM, Dykeman J, Patten SB, Wiebe S, Kaplan GG, Maxwell CJ. Depression in epilepsy: a systematic review and meta analysis. Neurology. 2013;80:590–599. doi:10.1212/WNL.0b013e31827b1ae0
5. Kwan P, Yu E, Leung H, et al. Association of subjective anxiety, depression, and sleep disturbance with quality‐of‐life ratings in adults with epilepsy. Epilepsia. 2015;50:1059–1066. doi:10.1111/epi.2009.50.issue-5
6. Sajatovic M, Jobst BC, Shegog R, et al. The managing epilepsy well network:: advancing epilepsy self-management. Am J Prev Med. 2017;52:241–245. doi:10.1016/j.amepre.2016.07.026
7. Wang Z, Yu C, Wang J, Bao J, Gao X, Xiang H. Age-period-cohort analysis of suicide mortality by gender among white and black Americans, 1983-2012. Int J Equity Health. 2016;15(1):107. doi:10.1186/s12939-016-0400-2
8. Wang HJ, Tan G, Deng Y, et al. Prevalence and risk factors of depression and anxiety among patients with convulsive epilepsy in rural West China. Acta Neurol Scand. 2018;138(6):541–547. doi:10.1111/ane.13016
9. Lacey CJ, Salzberg MR, D’Souza WJ. Risk factors for depression in community-treated epilepsy: systematic review. Epilepsy Behav. 2015;43:1–7. doi:10.1016/j.yebeh.2014.11.023
10. Sahoo SS, Ramesh P, Welter E, et al. Insight: an ontology-based integrated database and analysis platform for epilepsy self-management research. Int J Med Inform. 2016;94:21–30. doi:10.1016/j.ijmedinf.2016.06.009
11. Caller TA, Ferguson RJ, Roth RM, et al. A cognitive behavioral intervention (HOBSCOTCH) improves quality of life and attention in epilepsy. Epilepsy Behavior. 2016;57:111–117. doi:10.1016/j.yebeh.2016.01.024
12. Diiorio CK, Bamps YA, Edwards AL, et al. The prevention research centers’ managing epilepsy well network. Epilepsy Behav. 2010;19:218–224. doi:10.1016/j.yebeh.2010.07.027
13. Sajatovic M, Tatsuoka C, Welter E, et al. Correlates of quality of life among individuals with epilepsy enrolled in self-management research: from the US centers for disease control and prevention managing epilepsy well network. Epilepsy Behav. 2017;69:177–180. doi:10.1016/j.yebeh.2016.12.005
14. Sajatovic M, Colon-Zimmermann K, Kahriman M, et al. A 6-month prospective randomized controlled trial of remotely delivered group format epilepsy self-management versus waitlist control for high-risk people with epilepsy. Epilepsia. 2018;59:1684–1695. doi:10.1111/epi.14527
15. Sajatovic M, Tatsuoka C, Welter E, et al. Targeted self-management of epilepsy and mental illness for individuals with epilepsy and psychiatric comorbidity. Epilepsy Behav. 2016;64:152–159. doi:10.1016/j.yebeh.2016.08.012
16. Ciechanowski P, Chaytor N, Miller J, et al. PEARLS depression treatment for individuals with epilepsy: a randomized controlled trial. Epilepsy Behav. 2010;19(3):225–231. doi:10.1016/j.yebeh.2010.06.003
17. Fraser RT, Johnson EK, Lashley S, et al. PACES in epilepsy: results of a self-management randomized controlled trial. Epilepsia. 2015;56:1264–1274. doi:10.1111/epi.13052
18. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–613. doi:10.1046/j.1525-1497.2001.016009606.x
19. Cramer JA, Perrine K, Devinsky O, Meador K. A brief questionnaire to screen for quality of life in epilepsy: the QOLIE-10. Epilepsia. 1996;37(6):577–582. doi:10.1111/j.1528-1157.1996.tb00612.x
20. Bautista RED. Understanding the self-management skills of persons with epilepsy. Epilepsy Behav. 2017;69:7–11. doi:10.1016/j.yebeh.2016.11.022
21. Devinsky O. Quality of life in the elderly. Epilepsy Behav. 2005;6:1–3. doi:10.1016/j.yebeh.2004.09.011
22. Baker GA, Jacoby A, Buck D, Brooks J, Potts P, Chadwick DW. The quality of life of older people with epilepsy: findings from a UK community study. Seizure-Eur J Epilepsy. 2001;10(2):2–99. doi:10.1016/S1059-1311(00)90465-5
23. Escoffery C, McGee RE, Bamps Y, Helmers SL. Differences in epilepsy self-management behaviors among young and older adults. Austin J Neurol Disord Epilepsy. 2016;3(1):1015.
24. Haigh EA, Bogucki OE, Sigmon ST, Blazer DG. Depression among older adults: a 20-year update on five common myths and misconceptions. Am J Geriatric Psychiatry. 2018;26(1):107–122. doi:10.1016/j.jagp.2017.06.011
25. Managing Epilepsy Well Network. 2019. Available from: https://managingepilepsywell.org/.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.