")
Back to Journals » International Journal of Women's Health » Volume 13
Depression in Ugandan Rural Women Involved in a Money Saving Group: The Role of Spouse’s Unemployment, Extramarital Relationship, and Substance Use
Authors Kaggwa MM , Namatanzi B, Kule M, Nkola R , Najjuka SM , al Mamun F , Hosen I , Mamun MA , Ashaba S
Received 7 June 2021
Accepted for publication 4 September 2021
Published 22 September 2021 Volume 2021:13 Pages 869—878
DOI https://doi.org/10.2147/IJWH.S323636
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Mark Mohan Kaggwa,1 Brendah Namatanzi,2 Moses Kule,3 Rahel Nkola,1 Sarah Maria Najjuka,4 Firoj al Mamun,5,6 Ismail Hosen,5,6 Mohammed A Mamun,5,6 Scholastic Ashaba1
1Department of Psychiatry, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda; 2Faculty of Health Sciences, Lira University, Lira, Uganda; 3Department of Psychiatry, Mbarara Regional Referral Hospital, Mbarara, Uganda; 4College of Health Sciences, Makerere University, Kampala, Uganda; 5CHINTA Research Bangladesh, Savar, Dhaka, 1342, Bangladesh; 6Department of Public Health and Informatics, Jahangirnagar University, Savar, Dhaka, 1342, Bangladesh
Correspondence: Mark Mohan Kaggwa
Department of Psychiatry, Faculty of Medicine, Mbarara University of Science and Technology, P.O. Box 1410, Mbarara, Uganda
Email [email protected]
Background: Rural women are highly prevalent to depression, where spouse-related factors, including extramarital affairs and poverty, intensify its likelihood of occurrence. However, women engaged with a Money-Saving Group (MSG) are financially self-dependent, which can reduce the risk of depression suffering. Despite this, there is less study among this cohort, which led us to investigate the prevalence and associated factors of depression among the Ugandan women involved in MSG.
Methods: This was a cross-sectional study in Uganda among rural married or cohabiting women aged 18 to 45 years engaged in MSG. The survey was carried out within a total of 153 participants (33.3 ± 6.7 years) in April 2021. Information related to socio-demographic of the participants, their spouse characteristics, and depression were collected.
Results: About 65.4% of the participants had depressive symptoms (based on the cutoff 10/27 at the PHQ-9). But, 8.15 times (CI: 2.83– 23.44, p< 0.001) and 16.69 times (CI: 4.85– 57.39, p< 0.001), higher risk of depression were observed, if the participants’ spouses were using an addictive substance and had been involved in an extramarital relationship, respectively. Similarly, there was an increased likelihood of depression when the participant or spouse was unemployed.
Conclusion: This study observed a higher prevalence of depression, which suggests paying attention to this cohort. Thus, there should be routine screening for depression among married women involved in MSG at lower-level health facilities in rural settings, especially those with spouses engaged in substance use, having an extramarital relationship, and being unemployed.
Keywords: depression, married women, spouse extramarital affairs, rural Uganda, women’s mental health, extramarital relationship, money-saving group, substance use, spouse substance use, poverty, addiction
Introduction
Depression is a mood disorder characterized by feelings of sadness, emptiness, or irritability, accompanied by reduced functionality due to cognitive and somatic changes.1,2 Worldwide, over 322 million people are affected with depression, and it is prevalent among females (that is, 5.1% female and 3.6% male respectively).3 The burden of depression and its extreme complications, such as suicidality, is persistently higher among women residing in rural areas compared to the urban.4–6 With substandard mental health services and limited expertise among the available health workers in most rural settings, mental health problems, including depression, remain prevalently untreated, contributing to their functional decline.7
The vulnerability of rural women to depression is associated with a number of personal factors that include the higher number of children, lower levels of education, increasing number of years in marriage, use of addictive substances, and mental illness history, especially depression.7–9 Marriage is an essential part of life, where women’s risk for depression depends on many of the spouse-related factors. Lack of support from spouses or in-laws, and their substance use behaviors, current mental illness, lower levels of education, and extramarital relationships are the noteworthy risk factors for women’s depression.8–11 In addition, a spouse’s extramarital relationship leads to a higher risk of domestic violence, substance misuse, familial conflicts, and ultimately turns into negligence behaviors toward the woman, where these factors are being reported worsening depression in married women.9,10,12
Depression among married women has detrimental effects, including increasing the risk of familial dysfunctionality and poverty.13–16 While money-generating activities keep women economically active, help in reducing poverty, and make their finances independent from their spouses, which may reduce the likelihood of depression.14,17 Poverty-related depression is being reported consistently, where it is prevalent in the low- and middle-income countries (LMICs).18 Women, especially from rural settings, are reported as suffering from both issues (ie, poverty and depression),19,20 while empowerment can be a protective factor of their depression, which leads to them involving in income-generating activities such as micro-credit, small business earnings, assets accumulation, and so forth.13,16,21,22
Given the vulnerability of rural married women to depression, it is unknown how depression affects those involved in the income-generating activity (eg, Money-Saving Group, MSG) in the context of Uganda. MSG's have been set up in various areas of the country to help economically deprived groups by learning how to save money and improve their incomes through an approach to support saving and borrowing by forming Village Savings and Loan Associations.23–25 Women dominate the majority of the MSG, such as AVSI Foundation supported groups (an international NGO that carries out cooperation projects for development).26 The MSG is set up by poor women who cannot access formal money lending and saving services, lack stable jobs or money-generating activities, or have the collateral needed for loans.23 Members of the groups manage these with limited support from external organizations, thus empowering women.26 However, this study investigates the prevalence of depression and its associated factors among the rural married women involved in MSG from Uganda.
Methods
Study Design and Setting
The present study was cross-sectional in nature, conducted in April 2021, among the married or cohabiting women in Isingiro Town Council in Isingiro district in southwestern Uganda. Isingiro district is located 309.2 KM from the capital city, Kampala, with a total estimated population of 18,045 women.27 Data were collected from Mabona parish (note: a parish is the second-lowest administrative unit of the Uganda government, made up of many villages and consisted of a population of about 4000 people28), which was purposively selected because it had a group of married or cohabiting women organized in a MSG (“Bataka Kweyamba Group”). In addition, this group had a list of all married or cohabiting women, 292. Women aged 18–45 years who were part of the MSG and were willing to consent to participate in the study were included in this study. But, these women who had a physical illness that could have impaired their ability to stand the interview length were excluded. Besides, pregnant women and postpartum women were excluded because hormonal changes can increase the depression rate.29 Lastly, eligible participants aged 45 years and above were excluded because these women experience premenopausal or menopausal symptoms that may present as symptoms of depression hence overestimating the prevalence.30
Sample Size
A pilot study involving 50 married women was done in a similar setting to determine the prevalence of depression among married women. The prevalence of depression among women in that pilot study was 23%, and this rate was used to determine the sample size of the current study using the Kish-Leslie formula.31 A sample of 153 participants was reached based on a 95% confidence interval and a margin of error of 5%. Consecutive recruitment was done until the required sample size was reached.
Data Collection
Data were collected by female research assistants who were trained in data collection methods and handling sensitive topics (eg, extramarital affairs). They administered the questionnaire in the local language (Runyakole), and each interview took about 30 minutes to complete. The questionnaire consisted of four parts; that is, (i) participants sociodemographic characteristics such as age in years, level of education, monthly income, number of children, employment status, alcohol and substance use history, and history of mental illness; (ii) the spouse’s reported characteristics of the participating women, such as age, level of education, employment status, extramarital relationship, alcohol and substance use history, and history of mental illness; and (iii) depression assessed by the Patient Health Questionnaire 9 (PHQ-9).
Patient Health Questionnaire (PHQ-9)
The PHQ-9 is a 9-item self-administered tool that was used to assess depression symptoms in this study. It is a 4-point Likert scale, where the responses are recorded as not at all = 0, several days = 1, more than half the days = 2, and nearly every day = 3. The PHQ-9 is internationally used to screen for depression because of its excellent psychometric properties.32,33 The PHQ-9 is also used in the context of Uganda; excellent psychometric properties are found.34–36 The severity of depression based on the total score is as follows: 1–4 for minimal depression, 5–9 for mild depression, 10–14 for moderate depression, 15–19 for moderately severe depression, and 20–27 for severe depression.37 The cutoff score (≥10) of major depressive disorder has reported a sensitivity of 88%, and specificity of 85%, as per a recent meta-analysis study by Levis et al.33 Therefore, this cutoff is used to assess to determine the presence of depression in this study. Like the prior studies,33 Cronbach’s alpha in this study was excellent (0.94) for a translated version of Runyankole/Rukiga.
Ethical Considerations
The study was conducted according to the ethical guidelines of the Declarations of Helsinki. Besides, it was approved by the Mulago Hospital Research and Ethics Committee (MHREC 2044). Permission to collect data was obtained from the district, local councils of the parish, and villages. The participants’ partners (head of the family) permitted the research team to interview their wives about mental wellness. The spouses were not given the details of the study and what information may be asked. All participants were interviewed in a private place either within the home environment or away from home or any other place of their choice not accessed by another person to ensure privacy and confidentiality. Participants were informed about the study, and they provided written informed consent before enrollment in the study. Counseling was provided to all the women diagnosed with depression by the psychologist on the team (BN). Those with moderate to severe depression were referred to the psychiatrists of the research team (MMK, RN, and SA) for further management.
Data Analysis
Initially, data were entered into Excel and exported to STATA version 16.0 for final analysis. Descriptive statistics were summarized using mean and standard deviations for continuous data and percentages for categorical variables. Inferential statistics (t-tests and chi-square tests) were performed to identify relationships between depression and independent variables. Logistic regression analysis was used to determine the association between depression and independent variables, which were statistically significant at the first-order analyses. All significant factors at bivariate logistic regression were taken into the adjusted model to adjust for confounding. A p-value of less than 0.05 for the level of significance was considered at a 95% confidence interval.
Results
A total of 153 participants were recruited, whereas 65.4% (n=100) had scored being depressed based on the PHQ-9 cutoff score (10 out of 27). However, the severity of depression was as follows: minimal 28.76% (n = 44), mild 5.88% (n = 9), moderate 13.07% (n = 20), moderately severe 27.45% (n = 42), and severe 24.84% (n = 38).
Relationship Between Depression and Participant’s Characteristics
Of the total participants, 33.3 (± 6.7) years was the mean age. The majority of the participants had primary level education (47.7%), were unemployed (60.8%). About 70.0% of the unemployed women had depression, which was higher than the employed ones (vs 30.0%; χ2 = 10.29 p < 0.001). Depression was predominantly observed among these women not reporting addictive substance use compared with those used (67.0% vs 33.0%; χ2 = 10.31, p < 0.001). Similarly, participants being older and having more children were at an increased risk of depression (p=0.021 and p<0.001, respectively) (Table 1).
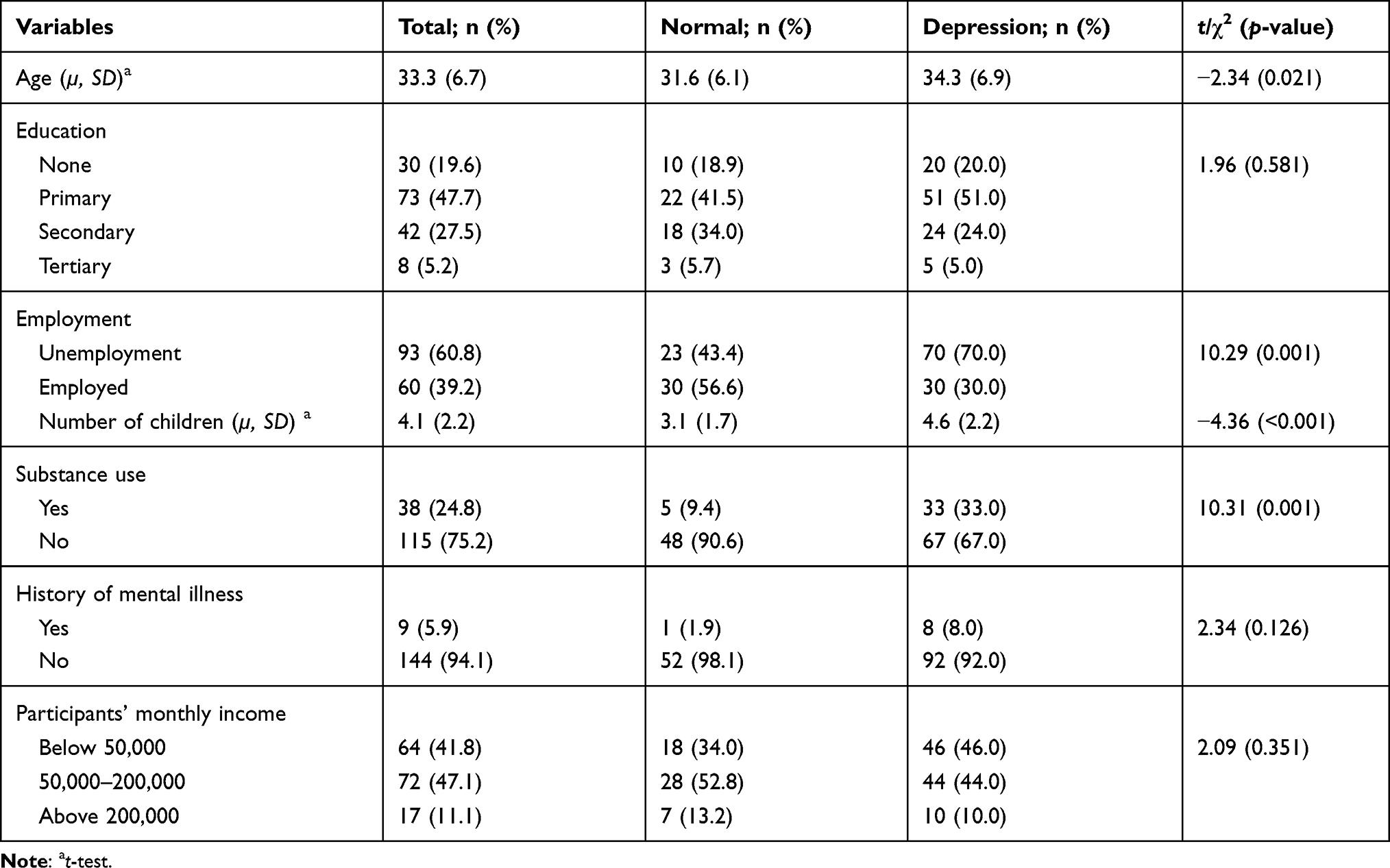 |
Table 1 The Association Between Participants’ Variables and Depression |
Relationship Between Depression and Spouse’s Characteristics
The reported mean age for the participant’s spouse was 43.4 (± 9.5) years, and 46.4% of spouse had achieved secondary level education. Nearly half (49.7%) of the partners were involved in extramarital relationships. The prevalence of depression was higher among women who reported their spouses using addictive substances (75.0% vs 25.0%; χ2=44.20, p < 0.001). In addition, the women whose husbands had extramarital affairs were more depressed compared to those whose husbands had not (71.0% vs 29.0%; χ2=52.52, p < 0.001) (Table 2).
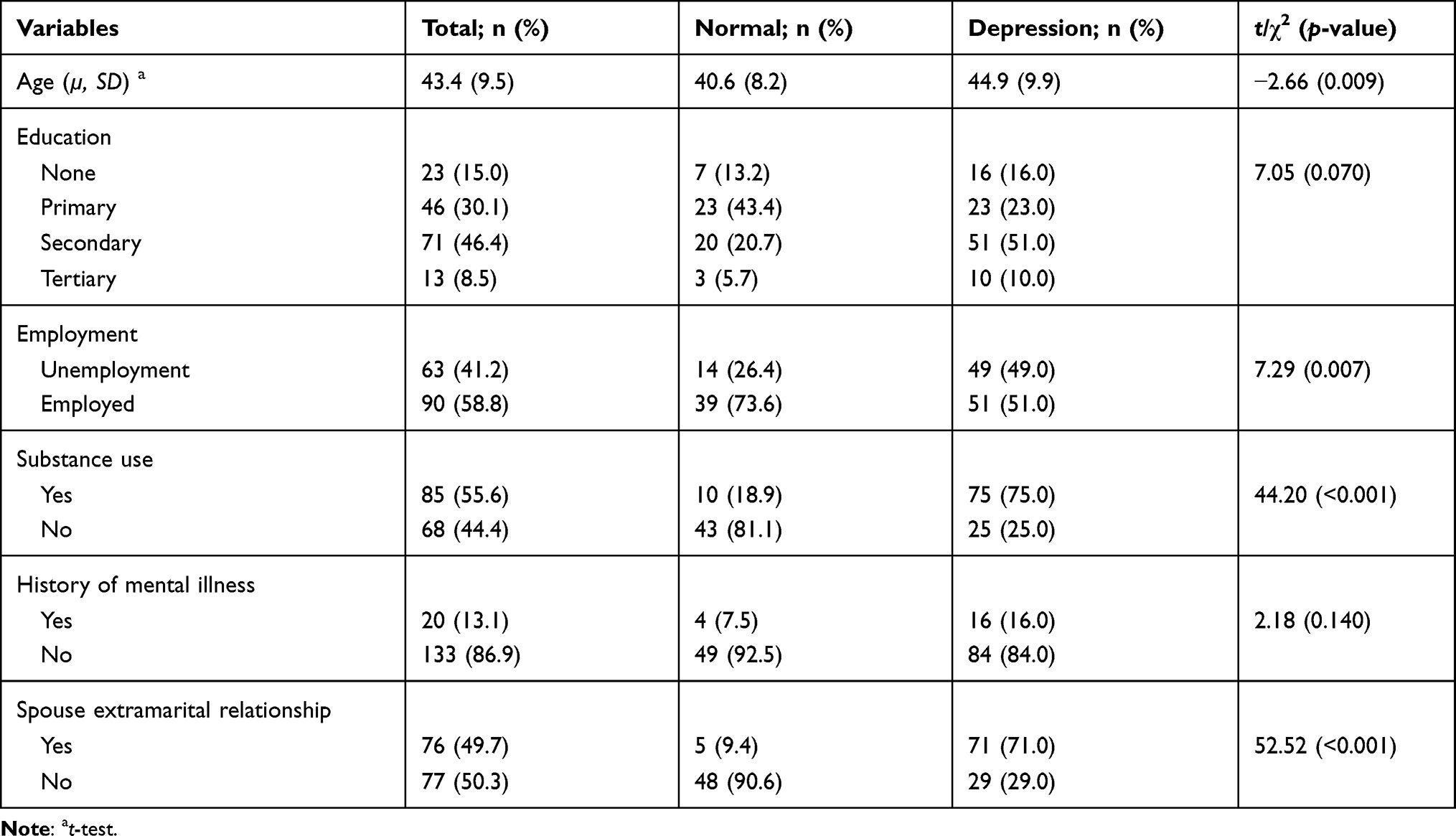 |
Table 2 The Association Between Spouse Characteristics as Reported by the Participants |
Factors Associated with Depression Among Women in Rural Uganda
Factors with statistical significance at the chi-square test or t-test were used to perform logistic regression to obtain the factors associated with depression, included: age, employment, number of children, and history of substance use, for participants. While their reported spouse’s characteristics were age, employment, history of substance use, and having an extramarital relationship. The factors were tested for collinearity, and the reported age of the spouse was dropped because it has a variance inflation factor (VIF) above 3. The remaining variables were checked for collinearity, with all having a VIF below 2, and mean VIF was 1.32. These were used to build the model using a backward stepwise selection method. The model had a sensitivity of 92.0%, specificity of 77.4%, and correctly classified 86.9% of depression. The goodness-of-fit p-value of 0.028 for the six variables.
The identified factors associated with depression were participant spouse reported substance abuse and involvement in extramarital relationships at multivariable analysis. The likelihood of having depression was 8.15 (CI 2.83–23.44) times if the participant spouses were using substances of addiction. However, the likelihood of depression, if the spouse was reported to be involved in an extramarital relationship, was higher at 16.69 (CI 4.85–57.39) folds (Table 3).
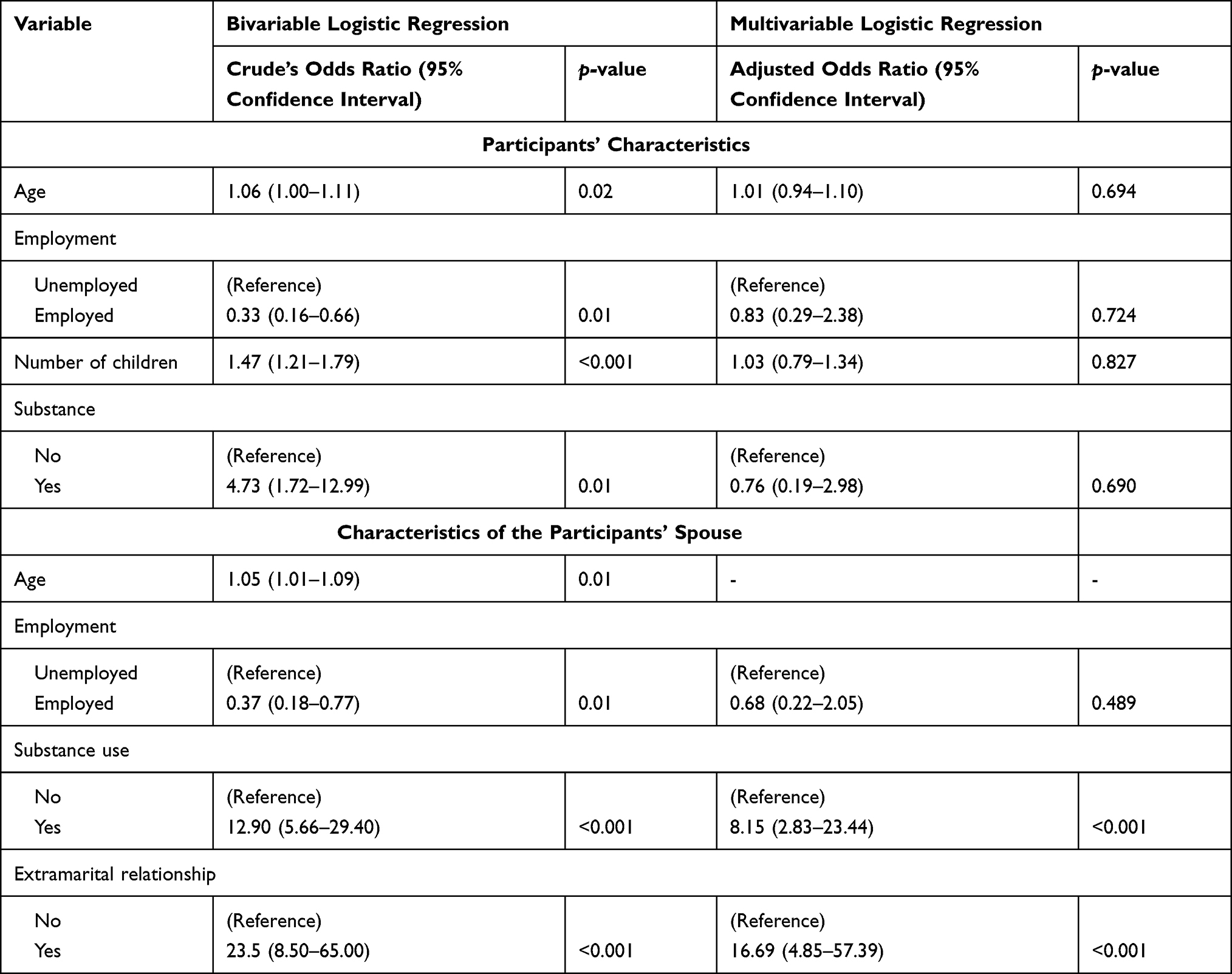 |
Table 3 Logistic Analysis for Factors Associated with Depression Among Married Women |
Discussion
This is the first study that assesses depression among the rural Ugandan women involved in a Money-Saving Group (MSG) and found 65% of them had moderate to extremely severe depression. The rate is slightly lower than a hospital-based study among young adult women in Kisoro (75% based on the Self-Reporting Questionnaire [SRQ-20] at a cutoff of 7 out of 20), another rural district in southwestern Uganda.8 The difference may be due to the study population recruited in the two studies. The study in Kisoro recruited women from a hospital setting who had various medical conditions and somatic symptoms. Individuals with medical conditions and somatic symptoms are at higher risk of depression suffering,8,38 which may rationalize the prevalence rate differences across two studies. In addition, a high prevalence of depression has consistently been found in the economically deprived groups in Uganda using the PHQ-9 at a cutoff of 10, such as refugees (range from 47% to 96%).36,39,40 Individuals with depression who are involved in activities such as MSG to transition from poverty show a significant reduction in depressive symptoms (40.5% had recovered from depression in six weeks).41 Despite this study recruiting women from an MSG, the prevalence of depression was high, a possible indicator of higher depression among women was not part of the MSG. But this could not be the case because in a study conducted in Pakistan (an LMIC like Uganda), no difference in depression prevalence was found between economically deprived women and those with high socioeconomic status.11
The prevalence of depression found in our study was much higher than that 38% found among women in a study involving 1603 participants (men and women) involved in water insecurity and depression study conducted in an urban setting (Mbarara) using the Hopkins Symptom Checklist-Depression Subscale at a threshold value of >1.75.42 The difference may be due to the study settings, where Mbarara is more developed with more economic opportunities for women to thrive than Isingiro, which is more rural.36 In addition, women in urban areas are more economically empowered, which favors them mentally.11 The difference in the prevalence of depression may also be explained by variations in the study tools used, due to differences in psychometric properties in terms of specificity and sensitivity.43 However, the prevalence of depression in our study was similar to that found in a study, done among women in Pakistan, 65%;11 and this is likely because both studies recruited women of reproductive age, excluding other possible etiologies such as menopausal-related factors that have the ability to influence feelings and shifts in the mood.29 Additionally, polygamy is highly practiced in both communities, and polygamous men are highly respected, hence the similarities.44,45
This study participant had a statistically significant association between depression and spousal extramarital affairs, as echoed in the previous studies conducted from LMICs.10,12,46 Usually, men involving in extramarital relationships show inadequate love and offer no emotional support and care to their wives, which increases the risk of separation and divorce, and ultimately turns mental instabilities among couples.12,47 Culturally, divorce is not common in Uganda, with only 7% of the population getting a divorce.48 As such, most women choose to stay in these relationships with increased exposure to stress and hence depression. Such relationships are characterized by reduced intimacy and increased risk of violence, which comes in the form of physical, psychological, and sexual violence that ultimately increases the risk of depression. In most Ugandan cultures, extramarital relationships are accepted, and polygamous relationships are considered normal in most communities, which explains the high prevalence of extramarital affairs found in our study because most women do not accept these practices is seen as a breach of marital trust.49
Despite the fact that the majority of the studies about the effect of spouse’s addictive substance uses being qualitative,50–52 this study, one of very few, found a statistically significant relationship between participants’ depression and their spouse’s use of addictive substances. This can be explained by the previously reported correlation between spouse’s substance addiction and extramarital relation – a known risk factor of depression.53 In addition, spouses using addictive substances are reported to show negative and devastating relationships, such as criticism, blaming, humiliation and anger themselves, and express a low level of empathy in solving family problems.51 The effect is not only on married women but also on their children. Parents’ use of addictive substances is associated with adverse childhood events, poor school grades, low quality of life, malnutrition, and childhood use of the substance of addiction.54–56 Effect on children worsens women’s depression due to their strong attachments to their children.57 Spouses who use addictive substances are reported to divert most of the family financial resources to acquire addictive substances.58 This makes women belonging to MSG secure a future for their children, which causes depression to such women. Spouse addiction is reportedly associated with domestic violence that also worsens depression.
The high prevalence of depression among women involved in MSG may be due to the circumstances of poverty experienced in a rural setting (most women earned less than SHS 50,000 [approximately 13 USD]) or disability that makes patients less economically active, thus keeping them in poverty; or the increased healthcare expenditure associated with depression leads individuals to deprive their finances, hence remaining in poverty.18,19 Financial empowerment or activities that reduce poverty are integral in reducing the risk of depression; no wonder in this study, women who were employed or had spouses employed were less likely to have depression, though the relationships were not significant (Table 3).
Unfortunately, depression in such communities goes undetected, and individuals may resist seeking mental health care due to cultural stigma for mental illness.8 Coupled with reduced care from their spouse due to extramarital affairs, depression symptoms are seen as a sign of attention-seeking and hence ignored, making many affected women not seek care. The untreated depression is associated with a reduced level of functioning among women who are the backbone of most families in rural settings.16 Women live in a cycle involving spouse addiction, poverty, adverse events to children, spouse extramarital relationships, domestic violence, all interlinked, and worsened depression. Thus, this causes family deterioration in all aspects of social, psychological, economic, and lack of respect since most families in rural communities in Uganda thrive on the functionality and productivity of women.16
Recommendations
We recommend that policymakers at different levels use the following methods to combat depression among women involved in MSG: (i) incorporate mental health services among the MSG such as counseling, group therapy for the affected, and expert opinion for those who have experienced depression before; (ii) preventative methods through the use of methods to empower women; (iii) creating job opportunities for women and their spouses and (iv) handling qualitative studies to explore the reasons for depression and solutions to the experiences. The mental health community teams should assess and pass on messages to promote mental wellness at the service level.
Limitations
Our cross-sectional study is bias-prone and confounding rich due to the inadequate sample size and extended confidence intervals; thus, the results should be interpreted cautiously. We also did not separate cohabiting from married, yet they may have different reasons for their depression, such as not being wedded or being a second wife to someone. Mental health, including depression, is a culturally sensitive subject, with associated stigma and discrimination. Most women are unwilling to talk about it, leading to recall bias and social desirability where women could have chosen not to disclose their true feelings, which may affect the generalizability of our findings. Wecollected data from one rural setting, limiting generalizability of this study's findings for all women in rural Uganda. The study was also liable to selection bias since we excluded women at higher risk of depression, such as menopause, pregnant, and postpartum women. Lastly, this being a cross-sectional study, we cannot confirm the causality effect relationship between extramarital affairs and depression among our study participants.
Conclusions
Relatively, a higher prevalence of depressive symptoms among married rural women in this study was significantly associated with reported spouse extramarital relationships and substance use, and woman or spouse unemployment. This high prevalence of depression should be a cause for concern since most women are not treated, yet depression carries an increased risk of mortality through suicide and additional social and psychological effects on the family. In addition, depression causes functional impairment and when it affects women and impairs their functionality. It may have detrimental effects on the whole family since women are the backbone of the family in most rural settings in Uganda. Community mental health services should be strengthened to enable routine screening for depression among married women at lower-level health facilities so that they can be referred for appropriate care to maintain their functionality and stability of their families. Also, social support interventions should be formed for rural women to promote peer support which may reduce the risk of depression despite the challenges of spouse substance use and involvement in extramarital relationships, which are common in rural settings in Uganda.
Data Sharing Statement
Data are available on request from the corresponding author.
Ethics Approval and Consent to Participate
The study was approved by the Mulago Hospital Research and Ethics Committee (MHREC 2044), and all participants provided the written informed consent to participate in the study. The consent form translated to the local language (Runyankole) was read aloud to individuals who could not read and write, signed in the presence of a participant trusted witness (fluent in reading and writing) who countersigned.
Consent for Publication
Participants consented to the publication of the information obtained from them.
Acknowledgment
We appreciated the local government of the Isingiro district, the local leaders, and the participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that the study did not receive any financial support to support the compilation of this report.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). Washington, DC: American Psychiatric Publishing; 2013.
2. Rasheduzzaman M, Al Mamun F, Faruk MO, Hosen I, Mamun MA. Depression in Bangladeshi university students: the role of sociodemographic, personal, and familial psychopathological factors. Perspect Psychiatr Care. 2021. doi:10.1111/ppc.12722
3. World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; 2017. Available from: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf.
4. Bolton JM, Pagura J, Enns MW, Grant B, Sareen J. A population-based longitudinal study of risk factors for suicide attempts in major depressive disorder. J Psychiatr Res. 2010;44(13):817–826. doi:10.1016/j.jpsychires.2010.01.003
5. Deyessa N, Berhane Y, Alem A, et al. Intimate partner violence and depression among women in rural Ethiopia: a cross-sectional study. Clin Pract Epidemiol Ment Health. 2009;5:8. doi:10.1186/1745-0179-5-8
6. Fleischer NL, Fernald LC, Hubbard AE. Depressive symptoms in low-income women in rural Mexico. Epidemiology. 2007;18(6):678–685. doi:10.1097/EDE.0b013e3181567fc5
7. Sharma VK. Organization of mental health services in rural areas. In: Chaturvedi SK, editor. Mental Health and Illness in the Rural World. Singapore: Springer Singapore; 2020:169–181.
8. Fischer M, Ramaswamy R, Fischer-Flores L, Mugisha G. Measuring and understanding depression in women in Kisoro, Uganda. Cult Med Psychiatry. 2019;43(1):160–180. doi:10.1007/s11013-018-9604-9
9. Zahidie A, Jamali T. An overview of the predictors of depression among adult Pakistani women. J Coll Phys Surg Pak. 2013;23(8):574–580.
10. Kamali S, Ameri F, Khosravi Z, Ramezani MA. Lived experience of women of their husbands’ extramarital relationships: a phenomenological study. J Fam Res. 2018;14(1):95–112.
11. Zainab S, Fatmi Z, Kazi A. Risk factors for depression among married women belonging to higher and lower socioeconomic status in Karachi, Pakistan. J Pak Med Assoc. 2012;62(3):249–253.
12. Azhar A, Wenhong AJ, Akhtar T, Aqeel M. Linking infidelity stress, anxiety and depression: evidence from Pakistan married couples and divorced individuals. IJHRH. 2018;11:214–228. doi:10.1108/IJHRH-11-2017-0069
13. Burke L. The impact of maternal depression on familial relationships. Int Rev Psychiatry. 2003;15(3):243–255. doi:10.1080/0954026031000136866
14. Maselko J, Bates L, Bhalotra S, et al. Socioeconomic status indicators and common mental disorders: evidence from a study of prenatal depression in Pakistan. SSM Population Health. 2018;4:1–9. doi:10.1016/j.ssmph.2017.10.004
15. Wachs TD, Black MM, Engle PL. Maternal depression: a global threat to children’s health, development, and behavior and to human rights. Child Dev Perspect. 2009;3(1):51–59. doi:10.1111/j.1750-8606.2008.00077.x
16. Camalin M, Setiawan I. The Role of Women Farmer Group in Increasing Family Welfare. Vol. 33. Bandung Islamic University; 2017.
17. Patel V. Poverty, gender and mental health promotion in a global society. Promot Educ. 2005;Suppl 2:26–29, 62, 68. doi:10.1177/10253823050120020104x
18. Lund C, Cois A. Simultaneous social causation and social drift: longitudinal analysis of depression and poverty in South Africa. J Affect Disord. 2018;229:396–402. doi:10.1016/j.jad.2017.12.050
19. Hailemichael Y, Hanlon C, Tirfessa K, et al. Catastrophic health expenditure and impoverishment in households of persons with depression: a cross-sectional, comparative study in rural Ethiopia. BMC Public Health. 2019;19(1):930. doi:10.1186/s12889-019-7239-6
20. Smith MV, Mazure CM. Mental health and wealth: depression, gender, poverty, and parenting. Annu Rev Clin Psychol. 2021;17(1):181–205. doi:10.1146/annurev-clinpsy-071219-022710
21. Dutta A, Banerjee S. Does microfinance impede sustainable entrepreneurial initiatives among women borrowers? Evidence from rural Bangladesh. J Rural Stud. 2018;60:70–81. doi:10.1016/j.jrurstud.2018.03.007
22. Kermode M, Herrman H, Arole R, White J, Premkumar R, Patel V. Empowerment of women and mental health promotion: a qualitative study in rural Maharashtra, India. BMC Public Health. 2007;7(1):225. doi:10.1186/1471-2458-7-225
23. Burt M Savings groups, mobile phones, and a new solution for rural women; 2014. Available from: https://www.centerforfinancialinclusion.org/savings-groups-mobile-phones-and-A-new-solution-for-rural-women.
24. Food and Agriculture Organization of the United Nations. Village Savings and Loan Schemes empower women in Karamoja; 2021. Available from: https://reliefweb.int/sites/reliefweb.int/files/resources/Uganda-VSLA-empowers-women-farmers.pdf.
25. Karlan D, Savonitto B, Thuysbaert B, Udry C. Impact of savings groups on the lives of the poor. Proc Natl Acad Sci USA. 2017;114:201611520. doi:10.1073/pnas.1611520114
26. Vegezzi C. In Uganda, a women’s savings group combats the Coronavirus. [News]; 2020; Available from: https://www.avsi.org/en/news/2020/05/06/in-uganda-A-womens-savings-group-combats-the-coronavirus/2048/.
27. Isingiro district planning unit. Five Year District Local Government Development Plan II 2015/2016-2019/2020. Isingiro local government; 2014. Available from: http://npa.go.ug/wp-content/uploads/2017/05/ISINGIRO-District-5-Year-LGDP-Final.pdf.
28. Kavuma RM Explainer: local government structures in Uganda. The Guardian; 2009. Available from: https://www.theguardian.com/katine/2009/dec/14/local-government-explainer.
29. Thériault RK, Perreault ML. Hormonal regulation of circuit function: sex, systems and depression. Biol Sex Differ. 2019;10(1):12. doi:10.1186/s13293-019-0226-x
30. Shea AK, Sohel N, Gilsing A, Mayhew AJ, Griffith LE, Raina PJM. Depression, hormone therapy, and the menopausal transition among women aged 45 to 64 years using Canadian longitudinal study on aging baseline data. Menopause. 2020;27(7):763–770.
31. Kish L. Statistical Design for Research. Vol. 83. John Wiley & Sons; 2004.
32. Carroll HA, Hook K, Perez OFR, et al. Establishing reliability and validity for mental health screening instruments in resource-constrained settings: systematic review of the PHQ-9 and key recommendations. Psychiatry Res. 2020;291:113236. doi:10.1016/j.psychres.2020.113236
33. Levis B, Benedetti A, Thombs BD. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ. 2019;365:l1476.
34. Gelaye B, Williams MA, Lemma S, et al. Validity of the Patient Health Questionnaire-9 for depression screening and diagnosis in East Africa. Psychiatry Res. 2013;210(2):653–661. doi:10.1016/j.psychres.2013.07.015
35. Nakku JEM, Rathod SD, Kizza D, et al. Validity and diagnostic accuracy of the Luganda version of the 9-item and 2-item Patient Health Questionnaire for detecting major depressive disorder in rural Uganda. Global Mental Health. 2016;3:e20. doi:10.1017/gmh.2016.14
36. Ronald B, Herbert Elvis A, Cathy Denise S, Godfrey Zari R. Association between stigma and depression among urban refugees in Mbarara Municipality, Southwestern Uganda. Res Square. 2021. doi:10.21203/rs.3.rs-17932/v1
37. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
38. Shim E-J, Hwang H, Lee K-M, et al. Somatic symptoms and sleep quality as indicators of depression and suicide risk among Korean military conscripts. Psychiatry Res. 2020;287:112912. doi:10.1016/j.psychres.2020.112912
39. Amir K, Lucas A. Depression and associated factors among refugees amidst Covid-19 in Nakivale Refugee Camp in Uganda. J Neurol Res Rev Rep. 2021;3(1):1–5. doi:10.47363/JNRRR/2021(3)132
40. Logie C, Okumu M, Simon M, Hakiza R, Chemutai D, Kyambadde P. Contextual factors associated with depression among urban refugee and displaced youth in Kampala, Uganda: findings from a cross-sectional study. Confl Health. 2020;14. doi:10.1186/s13031-020-00289-7
41. Ali A, Hawkins RL, Chambers DA. Recovery from depression among clients transitioning out of poverty. Am J Orthopsychiatry. 2010;80(1):26–33. doi:10.1111/j.1939-0025.2010.01004.x
42. Cooper-Vince CE, Arachy H, Kakuhikire B, et al. Water insecurity and gendered risk for depression in rural Uganda: a hotspot analysis. BMC Public Health. 2018;18(1):1143. doi:10.1186/s12889-018-6043-z
43. El-den S, Chen TF, Gan YL, Wong E, O’Reilly CL. The psychometric properties of depression screening tools in primary healthcare settings: a systematic review. J Affect Disord. 2018;225:503–522. doi:10.1016/j.jad.2017.08.060
44. Grace A, Ayebare E, Olwit C, Ndeezi G, Nankabirwa V, Tumwine J. Intimate partner violence among pregnant teenagers in Lira district, northern Uganda: a cross-sectional study. Afr J Midwifery Women’s Health. 2020;14:1–11. doi:10.12968/ajmw.2020.0011
45. Muhammad Roy P, Tamyiz M, Syibly MR, Ahmad N Polygamy in Muslim countries: a comparative study in Tunisia, Saudi Arabia, and Indonesia.
46. Abramsky T, Watts CH, Garcia-Moreno C, et al. What factors are associated with recent intimate partner violence? findings from the WHO multi-country study on women’s health and domestic violence. BMC Public Health. 2011;11(1):109. doi:10.1186/1471-2458-11-109
47. Conroy AA, McKenna SA, Comfort ML, Darbes LA, Tan JY, Mkandawire J. Marital infidelity, food insecurity, and couple instability: a web of challenges for dyadic coordination around antiretroviral therapy. Soc Sci Med. 2018;214:110–117. doi:10.1016/j.socscimed.2018.08.006
48. HiiL user friendly justice. Deep Dive into Divorce and Separation in Uganda; 2020. Hiil user friendly justice; 2020. Available from: https://www.hiil.org/wp-content/uploads/2020/10/HiiL-Uganda-Deep-Dive-Divorce-and-separation_Online.pdf. Accessed September 12, 2021.
49. Parikh SA. The political economy of marriage and HIV: the ABC approach, “safe” infidelity, and managing moral risk in Uganda. Am J Public Health. 2007;97(7):1198–1208. doi:10.2105/AJPH.2006.088682
50. Church S, Bhatia U, Velleman R, et al. Coping strategies and support structures of addiction affected families: a qualitative study from Goa, India. Fam Syst Health. 2018;36(2):216–224. doi:10.1037/fsh0000339
51. Mancheri H, Alavi M, Sabzi Z, Maghsoudi J. The effects of addiction on children and women: a qualitative study. Int J Pediatr. 2020;8(10):12165–12176. doi:10.22038/IJP.2019.45214.3718
52. Moriarty H, Stubbe M, Bradford S, Tapper S, Lim BT. Exploring resilience in families living with addiction. J Prim Health Care. 2011;3(3):210–217. doi:10.1071/HC11210
53. Sharifinia A, Nejati M, Bayazi M, Motamedi H. Investigating the relationship between addiction to mobile social networking with marital commitment and extramarital affairs in married students at Quchan Azad University. Contemp Fam Ther. 2019;41:401–407. doi:10.1007/s10591-019-09507-8
54. Ashaba S, Rukundo GZ, Beinempaka F, Ntaro M, LeBlanc JC. Maternal depression and malnutrition in children in southwest Uganda: a case control study. BMC Public Health. 2015;15:1303. doi:10.1186/s12889-015-2644-y
55. Lander L, Howsare J, Byrne M. The impact of substance use disorders on families and children: from theory to practice. Soc Work Public Health. 2013;28(3–4):194–205. doi:10.1080/19371918.2013.759005
56. Satinsky EN, Kakuhikire B, Baguma C, et al. Adverse childhood experiences, adult depression, and suicidal ideation in rural Uganda: a cross-sectional, population-based study. PLoS Med. 2021;18(5):e1003642–e1003642. doi:10.1371/journal.pmed.1003642
57. Crnic K, Ross E. Parenting stress and parental efficacy. In: Deater-Deckard K, Panneton R, editors. Parental Stress and Early Child Development: Adaptive and Maladaptive Outcomes. Cham: Springer International Publishing; 2017:263–284. doi:10.1007/978-3-319-55376-4_11
58. Arlappa P, Jha S. Impact of addiction on family: an exploratory study with reference to slums in Kolkata. Current Res J Soc Sci Humanities. 2019;2:58–71. doi:10.12944/CRJSSH.2.1.07
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.