")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Depression and Associated Factors Among Men Living with HIV/AIDS Aged 50 Years and Over in Chongqing, China
Authors Tan T, Zhou C, Lu R, Chen C, Bai C, Li L, Wu G
Received 1 July 2022
Accepted for publication 2 September 2022
Published 9 September 2022 Volume 2022:15 Pages 2033—2040
DOI https://doi.org/10.2147/JMDH.S378956
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Tianyu Tan,1 Chao Zhou,1 Rongrong Lu,1 Cheng Chen,2 Chongyang Bai,1 Long Li,1 Guohui Wu1
1Chongqing Center for Disease Control and Prevention, Chongqing, 400042, People’s Republic of China; 2Chongqing Jiulongpo District Center for Disease Control and Prevention, Chongqing, 400039, People’s Republic of China
Correspondence: Guohui Wu, Chongqing Center for Disease Control and Prevention, No. 8, Changjiang 2nd Road, Chongqing, 400042, People’s Republic of China, Tel +8602368801491, Email [email protected]
Purpose: This study aimed to assess the proportion of depression and its associated factors among men living with HIV/AIDS and aged 50 and over in Chongqing, China.
Methods: This cross-sectional study included 774 men diagnosed as HIV/AIDS and aged 50 and over in four regions. Data were collected through face-to-face interviews with a structured questionnaire. Multivariate logistic regression analysis was performed to identify factors associated with depression. A two-tailed P-value less than 0.05 was considered as statistical significance.
Results: A total of 293 participants (37.9%) reported depressive symptoms. Results from multivariate logistic regression suggested that individuals aged ≥ 70 (AOR = 1.99, 95% CI: 1.28– 3.08) and those living in rural areas (AOR = 2.79, 95% CI: 1.96– 3.97) were associated with higher odds of depression, while those being employed (AOR = 0.50, 95% CI: 0.32– 0.80) and with monthly income > 3000 CNY (AOR = 0.47, 95% CI: 0.30– 3.74) had lower odds of depression.
Conclusion: Our findings indicate a high prevalence of depression among older men living with HIV/AIDS in Chongqing, China. Age, residence, employment, and income have been identified as potential risk factors of depressive symptoms. Mental-health intervention initiatives should be tailored to target adults with a higher risk of depression.
Keywords: depression, China, older male, HIV/AIDS, influencing factors
Introduction
As a severe sexually transmitted disease, acquired immune deficiency syndrome (AIDS) is induced by the human immunodeficiency virus (HIV) and has threatened global population health.1 China has more than 1.053 million individuals living with HIV/AIDS and has recorded 351,000 HIV/AIDS-related deaths by 2020.2 Older adults have been increasingly and disproportionately affected by HIV/AIDS over the past decade in China.3 From 2007 to 2018, the rate of newly-diagnosed HIV/AIDS increased 10.4 times among older adults in China.4 And the proportion of newly-reported HIV positive cases among males aged 60 and over increased from 7.4% in 2010 to 18.2% in 2020 in China.5 The disproportionate increase among older men is particular of concern in Chongqing, China: men aged 50+ have accounted for over 60% of the newly-diagnosed HIV/AIDS cases (N ~8000) in this city in 2021, according to China National Center for AIDS/STD Control and Prevention (NCAIDS). In addition to the increasing incidence of HIV/AIDS among older adults,6 life expectancy has significantly increased among HIV/AIDS cases with the progress of antiretroviral therapy, leading to a larger number of aging populations living with HIV/AIDS.
Compared with the younger generation, older adults with HIV/AIDS may have a higher risk of mental health problems such as depression,7,8 as they may experience more HIV-driven psychological challenges due to social stigma and discrimination.9 Existing studies have found that individuals with HIV/AIDS have a higher prevalence of depression compared to the general population.10,11 Another research with a meta-analysis based on populations in western countries found that individuals with HIV/AIDS have a nearly two times higher prevalence of depression than HIV-negative population.12 Current studies have also suggested that the prevalence of depression among HIV/AIDS patients could be higher in low- and middle-income countries compared with high-income countries,13 ranging from 47% in the US14 to 80% in Pakistan.15 To be noted, initiative evidence from China has indicated that the prevalence of depressive symptoms is 74.2% among older adults with HIV/AIDS,16 significantly higher than that among the general HIV/AIDS population (53.8%).17
As one of the most common mental illnesses worldwide, depression has affected approximately 121 million people.18 Depression may incorporate a variety of symptoms, such as sadness, lack of interest, and feelings of low self-worth, and could lead to thoughts of death and suicide, with a total of global 800,000 depression-related suicide cases per year.19,20 Depression has been associated with an increased risk of morbidity and mortality, lower adherence to antiretroviral therapy,21 and worse quality of life including health-related parameters among individuals with HIV/AIDS.22,23 A comprehensive understanding of depression status and its risk factors may help to maintain quality of life among older adults with HIV/AIDS.24
This study aimed to examine the prevalence of depression and its potential influencing factors among older males with HIV/AIDS in Chongqing, China. Our findings might be promising to support depression intervention initiatives among individuals with HIV/AIDS in China.
Materials and Methods
This cross-sectional study was conducted in Chongqing, one of the largest cities in southwest China. Chongqing consists of four regions, including two districts in urban areas (Yubei and Shapingba District), one in suburban area (Kaizhou District), and one in rural–urban fringe area (Jiangjin District). From June to December 2021, participant recruitment was conducted in the local Centers for Disease Control and Prevention and designated medical institutions for AIDS treatment in each of these four regions. The inclusion criteria were (1) males aged 50 and above, (2) diagnosed as HIV/AIDS, and (3) followed-up with the HIV/AIDS-related services and management. We excluded HIV/AIDS individuals with other serious diseases and cognitive impairment. Overall, we included a total of 800 individuals with each region accounting for 200 participants.
Study recruits were usually patients on medication or regular CD4 testing. If the survey object meets the research object conditions, physicians will explain the purpose and significance of the survey to the patient and invite them to participate in the research. All investigators are well-trained health professionals such as outpatient physicians for voluntary HIV counseling and testing. Once the participants agreed to participate in this survey, investigators would conduct face-to-face interviews using the structured questionnaire including socioeconomic characteristics, AIDS-related characteristics, antiretroviral treatment information and Self-rating Depression Scale. The interviewers would read out loud each of the questions to the participants and recorded answers. Finally, the investigator checked the completeness and logic of the answers.
Ethical Consideration
This study conformed to the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Chongqing Center for Disease Control and Prevention. Participants were informed that the information collected for this research project would be kept confidential and information collected would be coded with a unique identification number. Written informed consent has been obtained from all study participants. Interviews were taken place in a silent place separately from others to avoid influencing others.
Questionnaire
The questionnaire was formulated through the Delphi method, and a pre-investigation was carried out before the formal investigation to further improve the questionnaire. Finally, the contents of the questionnaire were divided into four parts: Socio-demographic characteristics, AIDS-related characteristics, antiretroviral treatment information and depression status.
Self-Rating Depression Scale (SDS)
The self-rating depression scale consists of 20 items with four categorical options: always, often, sometimes, and rarely.25 We standardized raw scores (ranging from 1 to 4) by multiplying 1.25 and identified standardized scores over 53 as the presence of depression. According to the results of the Chinese norm, a score of 53 to 62 is considered as mild depression with scores between 63 and 72 classified as moderate depression and scores over 72 as severe depression. The SDS was tested and showed good reliability and validity (the Cronbach’s alpha coefficient was 0.80).
Statistical Analysis
We collected data using Epi Data 3.1 and performed data analyses in SPSS 23.0. Socio-demographic characteristics were described using frequencies for categorical variables and mean as well as standard deviation (SD) for continuous variables. We estimated crude odds ratios (ORs) with 95% confidence interval (CI) from univariate logistic regression models to investigate the association between each of these independent variables and the depression. We then performed multivariate logistic regression models and conducted backward stepwise method to identify risk factors of depression, independent of other covariates. The adjusted ORs with 95% CI were computed to measure the strength of the association. A two-tailed p-value <0.05 was considered as statistical significance. We tested multicollinearity among independent variables using variance inflation factors (<2), indicating mild and acceptable collinearity.
Results
Socio-Demographic Characteristics of Participants
A total of 800 questionnaires were issued with 774 effective questionnaires completed (effective rate: 96.8%). The mean age of the participants was 62.5 years old (SD = 8.6, range: 50–92). Among the participants, 466 (60.2%) lived in urban areas and 521 (67.3%) of them were married. A total of 327 (42.4%) and 224 (29.1%) had primary school and secondary school education. About three-fourths (73.1%) of the participants were unemployed and 581 (75.1%) had a monthly income less than 3000 CNY. Table 1 provides socio-demographic characteristics of the study.
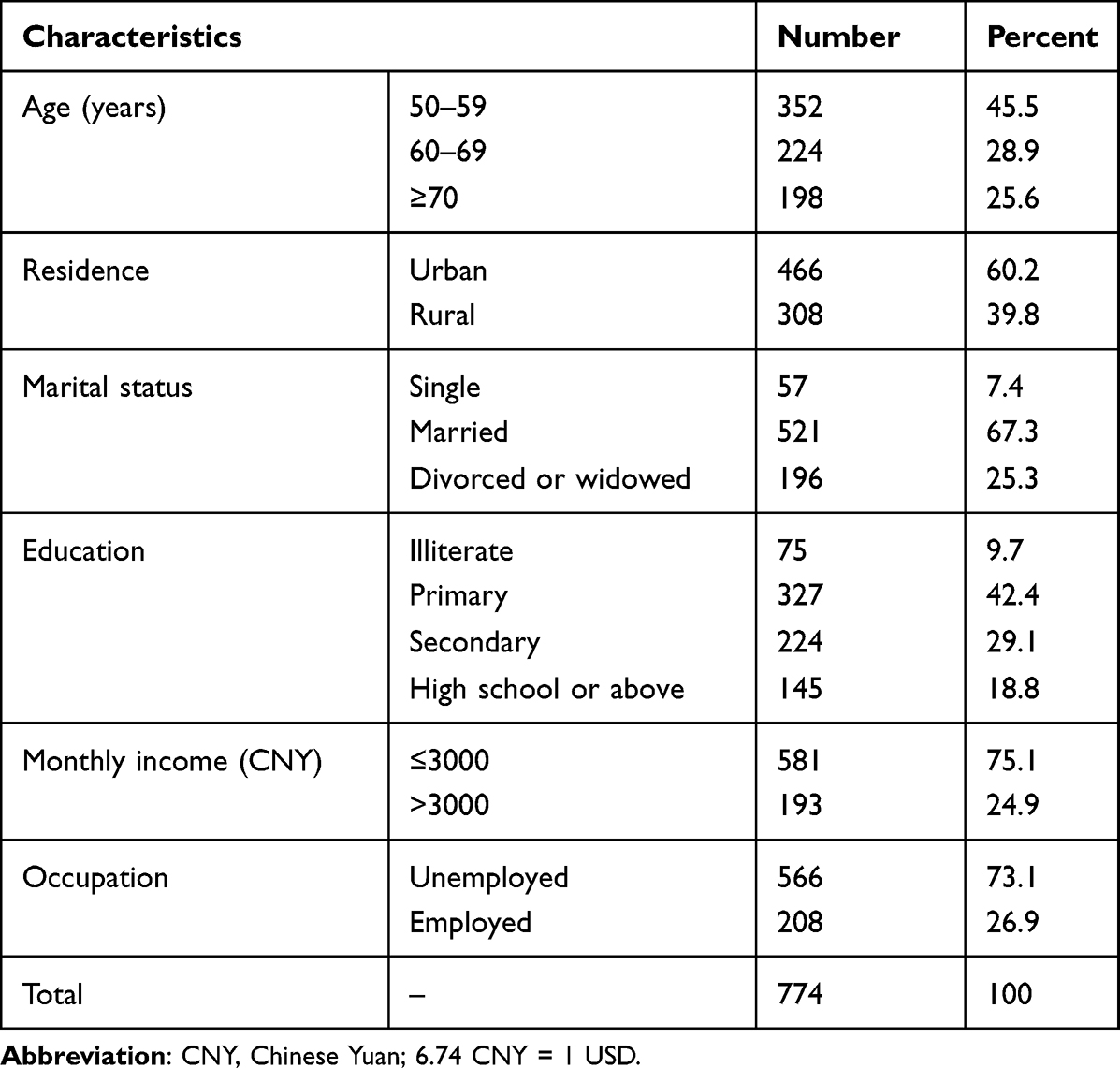 |
Table 1 The Socio-Demographic Characteristics of Men Living with HIV/AIDS and Aged 50 and Above in Chongqing, China |
HIV/AIDS Status-Related Characteristics of Participants
A majority of sexual orientation and transmission routes were heterosexual contact (88.0%) and heterosexual contact (87.7%), respectively. A total of 491 (63.4%) participants maintained ART for three years or more. In the most recent test, 600 (77.5%) had a CD4 count greater than 200 cells/mm3 and 598 (77.2) had a viral load less than 50 copies/mL. There are 508 (65.6%) participants who reported awareness of HIV/AIDS. HIV/AIDS status-related characteristics of all participants are shown in Table 2.
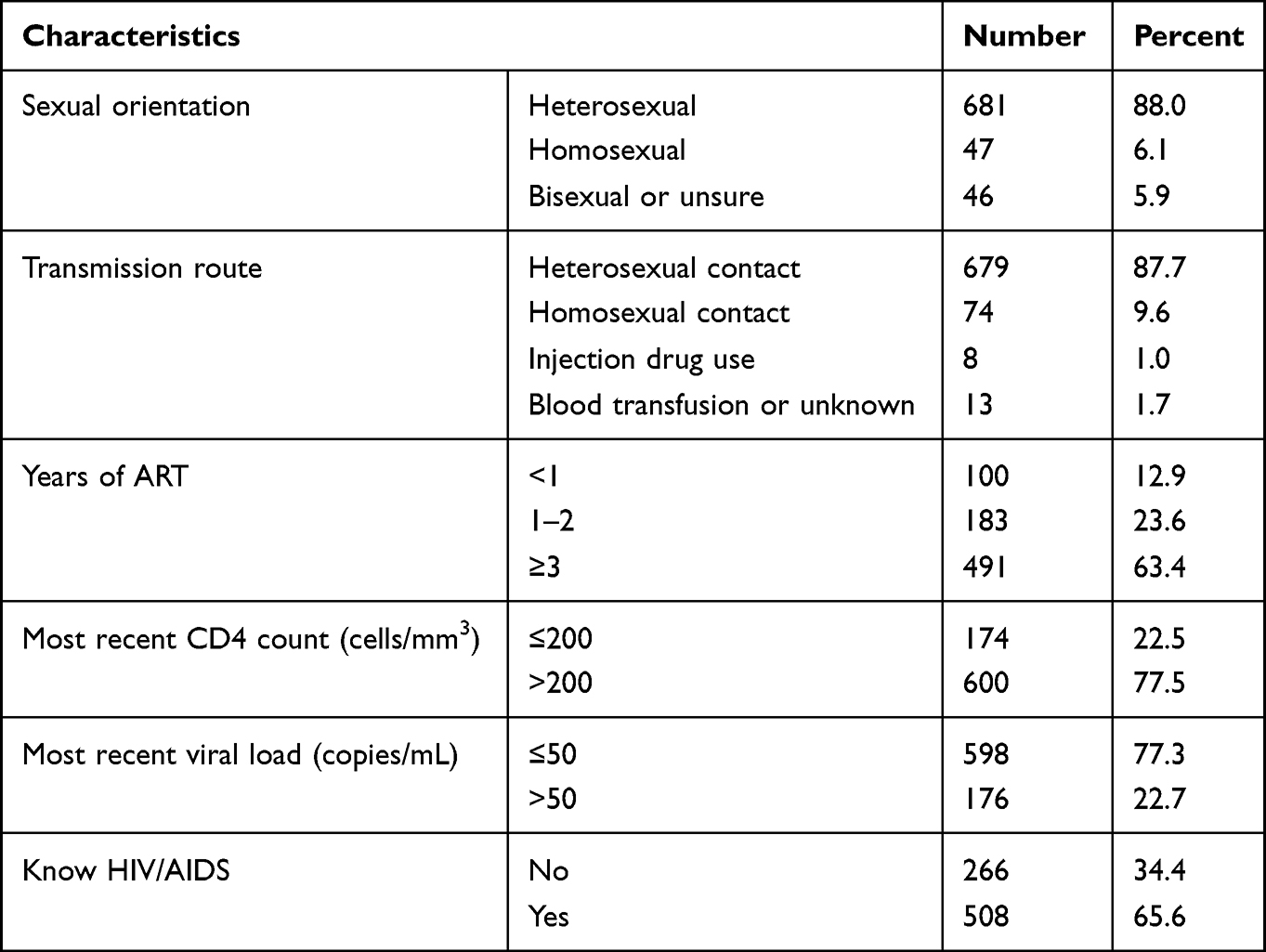 |
Table 2 HIV/AIDS Status-Related Characteristics of Men Living with HIV/AIDS and Aged 50 and Above in Chongqing, China |
Prevalence of Depression
We identified 37.9% of the study participants as being depressed (n = 293) through the Self-Rating Depression Scale (SDS). The prevalence of mild, moderate and severe depression was 17.6%, 19.3% and 1.0%, respectively.
Factors Associated with Depression Among Participants
Table 3 provides estimates and 95% CIs from logistic regression analyses. Results from univariate logistic regression analyses showed that age, residence, education, employment status, and monthly income were associated with depression and therefore were considered as candidates for multivariable analyses. Results from the multivariable logistic regression suggested that age, residence, occupation, and monthly income were significantly associated with depressive symptoms. Participants aged ≥70 had higher odds of having depressive symptoms than those aged 50–59 years (AOR = 1.99, 95% CI: 1.28–3.08). Compared to those with monthly income ≤3000 CNY, individuals with monthly income >3000 CNY (AOR = 0.47, 95% CI: 0.30–3.74) were less likely to have depressive symptoms. Rural residents (AOR = 2.79, 95% CI: 1.96–3.97) were 2.79 times more likely to develop depressive symptoms compared to their urban counterparts. Last, employees had lower the odds of depressive symptoms (AOR = 0.50, 95% CI: 0.32–0.80) than those unemployed.
 |
Table 3 Factors Associated with Depression Among Men Living with HIV/AIDS and Aged 50 and Above in Chongqing, China |
Discussion
In this cross-sectional study, we assessed the prevalence of depressive symptoms and their potential risk factors among men living with HIV/AIDS aged 50 and over in Chongqing, China. Several socioeconomic characteristics including age, residence, employment status, and monthly income could be potential risk factors of depressive symptoms among older men living with HIV/AIDS, providing empirical evidence for mental health intervention initiatives in this region.
The observed prevalence of depressive symptoms (37.9%) is higher than the general older population,26 indicating additional mental health burden among older men living with HIV/AIDS in Chongqing. Although the observed depression prevalence in our study is lower than that observed in studies conducted in China’s other cities such as Nanning,16 Wuhan,27 it is higher than that in Nanjing,28 Sichuan29 and similar to Shanghai30 and Guangzhou,31 potentially due to the variations in the employment of depression assessment tools. We used the Zung Self-Rating Depression Scale (SDS) to measure depressive symptoms, while others have used the Beck Depression Inventory (BDI), the Geriatric Depression Scale (GDS), and Patient Health Questionnaire (PHQ).32–34 Compared with these scales, the SDS is more sufficient to identify clinically meaningful depressive symptoms among older adults.35
Several socioeconomic characteristics including age, residence, occupation, and monthly income were significantly associated with depressive symptoms in this study. Consistent with a study in north-central Ethiopia,36 increased age was positively associated with depression, potentially due to a higher prevalence of chronic illnesses such as diabetes, hypertension, and heart disease, which have been theorized as important predictors of depressive symptoms.37 We also found that monthly income was associated with depression, potentially because financial hardship may induce psychological distress and frustration, leading to increasing risk of depression.38 Living in rural areas may have poorer living conditions and limited access to mental health care services than those living in urban areas,28 leading to the observed variations. Additionally, a cross-sectional study including 7966 older adults suggested that socioeconomic status (SES) was associated with depression.39 In this SES model, variables such as occupation, income, and education are considered as intermediate variables that jointly affect the SES which was negatively correlated with depression. Therefore, we hypothesized that people being employed had better socioeconomic status and lower rates of depression than being unemployed, ultimately presenting the results in this study.
Different from existing studies,40,41 the CD4 level and viral load are not associated with depression in this study. High viral load and low CD4 level have been considered as the markers of poor disease progression and immune functioning, which may result in depression.42 As an indicator of individuals’ immunity function, the CD4 level is lower among older adults compared to that of the younger generation. Therefore, the decline in immune function among older HIV/AIDS individuals may not be as obvious as that among younger ones in the absolute scale,43 which may partially explain the reason as to why high viral load and low CD values were not associated with depression in our study.
However, several limitations to our findings should be taken into account. First, the nature of cross-sectional study design could not provide strong evidence to infer causality. Second, the study relied on self-reported data, which may be subject to recall bias. Furthermore, the potential misclassification of outcome measures may bias the true association under study. Last, we are unable to control for potential confounders such as perceived discrimination, antiretroviral therapy side effects, and social capital, leading to residual confounding.16,29,39
Conclusion
The findings suggest that the prevalence of depression among men living with HIV/AIDS aged 50 and over is prominent in Chongqing, China. Age, residence, employment status, and monthly income are significantly associated with depressive symptoms. Mental-health intervention initiatives should be tailored to target adults at high risk of depression.
Acknowledgments
The authors are grateful to the staff from Shapingba District Center for Disease and Control, Jiangjin District Center for Disease and Control, Yubei District Center for Disease and Control, and Kaizhou District Center for Disease and Control for participation in the study. The authors are also grateful to the study participants who voluntarily agreed to be interviewed and participated in the study. Special thanks to Dr. Zhao BH of Oxford University and Dr. Yu XX of the University of Michigan.
Funding
This study was supported by Chongqing Natural Science Foundation Project (cstc2021jcyj-msxmX1171), Chongqing Talents Program for Innovative and Entrepreneurial Pioneers (cstc2021ycjh-bgzxm0097), Chongqing medical scientific research project (2022WSJK022) and Chongqing medical scientific research project of Chongqing Health Commission and Science and Technology Bureau (2022GDRC017).
Disclosure
The authors declare that they have no conflicts of interest for this work or regarding the publication of this paper.
References
1. GDB. 2017 HIV Collaborators. Global, regional, and national incidence, prevalence, and mortality of HIV, 1980–2017, and forecasts to 2030, for 195 countries and territories: a systematic analysis for the Global Burden of Diseases, Injuries, and Risk Factors Study 2017. Lancet HIV. 2019;6(12):e831–e859. doi:10.1016/S2352-3018(19)30196-1
2. He N. Research progress in the epidemiology of HIV/AIDS in China. China CDC Wkly. 2021;3(48):1022–1030. doi:10.46234/ccdcw2021.249
3. Chen H, Wu X, Chen L, et al. Rapidly spreading human immunodeficiency virus epidemic among older males and associated factors: a large-scale prospective cohort study in rural Southwest China. Sex Transm Dis. 2019;46(4):234–239. doi:10.1097/OLQ.0000000000000957
4. Zhang Y, Cai C, Wang X, Li Y, Tang H, Ma J. Disproportionate increase of new diagnosis of HIV/AIDS infection by sex and age – China, 2007–2018. China CDC Wkly. 2020;2(5):69–74. doi:10.46234/ccdcw2020.020
5. National Center for AIDS & STD Control and Prevention, The Chinese Center for Disease Control and Prevention (CDC). Annals of Information on Comprehensive Prevention and Treatment for AIDS, STD and Hepatitis C; 2020.
6. Ma Y, Cui Y, Hu Q, et al. Long-term changes of HIV/AIDS incidence rate in China and the U.S. population from 1994 to 2019: a join-point and age-period-cohort analysis. Front Public Health. 2021;9:652868. doi:10.3389/fpubh.2021.652868
7. Remien RH, Stirratt MJ, Nguyen N, et al. Mental health and HIV/AIDS: the need for an integrated response. AIDS. 2019;33(9):1411–1420. doi:10.1097/QAD.0000000000002227
8. Guan Y, Zhu H, Qi T, et al. HIV/AIDS strategies should focus on outcomes and the psychological status of older patients diagnosed with HIV. Biosci Trends. 2022;16(1):91–98. doi:10.5582/bst.2021.01437
9. Brown MJ, Cohen SA, DeShazo JP. Psychopathology and HIV diagnosis among older adults in the United States: disparities by age, sex, and race/ethnicity. Aging Ment Health. 2020;24(10):1746–1753. doi:10.1080/13607863.2019.1636201
10. Charlson FJ, Baxter AJ, Cheng HG, et al. The burden of mental, neurological, and substance use disorders in China and India: a systematic analysis of community representative epidemiological studies. Lancet. 2016;388(10042):376–389. doi:10.1016/S0140-6736(16)30590-6
11. Pappin M, Wouters E, Booysen FL. Anxiety and depression amongst patients enrolled in a public sector antiretroviral treatment programme in South Africa: a cross-sectional study. BMC Public Health. 2012;12:244. doi:10.1186/1471-2458-12-244
12. Ciesla JA, Roberts JE. Meta-analysis of the relationship between HIV infection and risk for depressive disorders. Am J Psychiatry. 2001;158(5):725–730. doi:10.1176/appi.ajp.158.5.725
13. Rezaei S, Ahmadi S, Rahmati J, et al. Global prevalence of depression in HIV/AIDS: a systematic review and meta-analysis. BMJ Support Palliat Care. 2019;9(4):404–412. doi:10.1136/bmjspcare-2019-001952
14. Bengtson AM, Pence BW, Crane HM, et al. Disparities in depressive symptoms and antidepressant treatment by gender and race/ethnicity among people living with HIV in the United States. PLoS One. 2016;11(8):e0160738. doi:10.1371/journal.pone.0160738
15. Ahmed A, Saqlain M, Umair MM, et al. Stigma, social support, illicit drug use, and other predictors of anxiety and depression among HIV/AIDS patients in Pakistan: a cross-sectional study. Front Public Health. 2021;9:745545. doi:10.3389/fpubh.2021.745545
16. Liu H, He X, Levy JA, et al. Psychological impacts among older and younger people living with HIV/AIDS in Nanning, China. J Aging Res. 2014;2014:576592. doi:10.1155/2014/576592
17. Yuan QQ, Li FR, Ruan YH, et al. Meta-analysis of the prevalence of depression among Chinese HIV/AIDS patients. Chin J AIDS STD. 2021;27(1):5.
18. GBD. 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–1259. doi:10.1016/S0140-6736(17)32154-2
19. Tao J, Vermund SH, Qian HZ. Association between depression and antiretroviral therapy use among people living with HIV: a meta-analysis. AIDS Behav. 2018;22(5):1542–1550. doi:10.1007/s10461-017-1776-8
20. Bachmann S. Epidemiology of suicide and the psychiatric perspective. Int J Environ Res Public Health. 2018;15(7):1425. doi:10.3390/ijerph15071425
21. Camargo CC, Cavassan NRV, Tasca KI, et al. Depression and coping are associated with failure of adherence to antiretroviral therapy among people living with HIV/AIDS. AIDS Res Hum Retroviruses. 2019;35(11–12):1181–1188. doi:10.1089/aid.2019.0050
22. Shim EJ, Hahm BJ, Lee SH, et al. The relationships among fear of disease progression, anxiety, depression and medication adherence in persons with HIV/AIDS. J Psychosom Res. 2018;109:135. doi:10.1016/j.jpsychores.2018.03.143
23. Ntshakala TT, Mavundla TR, Dolamo BL. Quality of life domains relevant to people living with HIV and AIDS who are on antiretroviral therapy in Swaziland. Curationis. 2012;35(1):87. doi:10.4102/curationis.v35i1.87
24. Rosenfeld D, Catalan J, Ridge D; HIV and Later Life (HALL) Team. Strategies for improving mental health and wellbeing used by older people living with HIV: a qualitative investigation. AIDS Care. 2018;30:102–107. doi:10.1080/09540121.2018.1468016
25. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12:63–70. doi:10.1001/archpsyc.1965.01720310065008
26. Liu K, Chen Y, Zhou XL, et al. Influencing factors of depressive disorder among the elderly in the community. Int J Gerontol. 2022;43(2):5.
27. Rong H, Nianhua X, Jun X, et al. Prevalence of and risk factors for depressive symptoms among people living with HIV/AIDS receiving antiretroviral treatment in Wuhan, China: a short report. AIDS Care. 2017;29(12):1524–1528. doi:10.1080/09540121.2017.1327649
28. Wei HX, Bai CQ, Huan XP, et al. Analysis of medication compliance and influencing factors among HIV/AIDS patients in Nanjing. Chin J AIDS STD. 2018;24(1):4.
29. Han J, Jia P, Huang Y, et al. Association between social capital and mental health among older people living with HIV: the Sichuan Older HIV-Infected Cohort Study (SOHICS). BMC Public Health. 2020;20(1):581. doi:10.1186/s12889-020-08705-6
30. Jiang M, Yang J, Song Y, et al. Social support, stigma, and the mediating roles of depression on self-reported medication adherence of HAART recipients in China. AIDS Care. 2019;31(8):942–950. doi:10.1080/09540121.2019.1587360
31. Zeng C, Li L, Hong YA, et al. A structural equation model of perceived and internalized stigma, depression, and suicidal status among people living with HIV/AIDS. BMC Public Health. 2018;18(1):138. doi:10.1186/s12889-018-5053-1
32. Taylor WD. Clinical practice. Depression in the elderly. N Engl J Med. 2014;371(13):1228–1236. doi:10.1056/NEJMcp1402180
33. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
34. Beard C, Hsu KJ, Rifkin LS, et al. Validation of the PHQ-9 in a psychiatric sample. J Affect Disord. 2016;193:267–273. doi:10.1016/j.jad.2015.12.075
35. Jokelainen J, Timonen M, Keinänen-Kiukaanniemi S, et al. Validation of the Zung self-rating depression scale (SDS) in older adults. Scand J Prim Health Care. 2019;37(3):353–357. doi:10.1080/02813432.2019.1639923
36. Damtie Y, Kefale B, Yalew M, et al. Depressive symptoms and associated factors among HIV positive patients attending public health facilities of Dessie town: a cross-sectional study. PLoS One. 2021;16(8):e0255824. doi:10.1371/journal.pone.0255824
37. Abadiga M. Depression and its associated factors among HIV/AIDS patients attending ART clinics at Gimbi General hospital, West Ethiopia, 2018. BMC Res Notes. 2019;12(1):527. doi:10.1186/s13104-019-4553-0
38. Getaye A, Cherie N, Bazie GW, et al. Proportion of depression and its associated factors among youth HIV/AIDS clients attending ART clinic in Dessie town government health facilities, Northeast Ethiopia. J Multidiscip Healthc. 2021;14:197–205. doi:10.2147/JMDH.S296849
39. Domènech-Abella J, Mundó J, Leonardi M, et al. The association between socioeconomic status and depression among older adults in Finland, Poland and Spain: a comparative cross-sectional study of distinct measures and pathways. J Affect Disord. 2018;241:311–318. doi:10.1016/j.jad.2018.08.077
40. Shearer K, Evans D, Xhosa B, et al. Low prevalence of depressive symptoms among stable patients on antiretroviral therapy in Johannesburg, South Africa. PLoS One. 2018;13(9):e0203797. doi:10.1371/journal.pone.0203797
41. Aibibula W, Cox J, Hamelin AM, et al. Association between depressive symptoms, CD4 count and HIV viral suppression among HIV-HCV co-infected people. AIDS Care. 2018;30(5):643–649. doi:10.1080/09540121.2018.1431385
42. Prasithsirikul W, Chongthawonsatid S, Ohata PJ, et al. Depression and anxiety were low amongst virally suppressed, long-term treated HIV-infected individuals enrolled in a public sector antiretroviral program in Thailand. AIDS Care. 2017;29(3):299–305. doi:10.1080/09540121.2016.1201194
43. Ferrando-Martínez S, Ruiz-Mateos E, Romero-Sánchez MC, et al. HIV infection-related premature immunosenescence: high rates of immune exhaustion after short time of infection. Curr HIV Res. 2011;9(5):289–294. doi:10.2174/157016211797636008
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.