")
Back to Journals » Substance Abuse and Rehabilitation » Volume 10
Depot Buprenorphine Injection In The Management Of Opioid Use Disorder: From Development To Implementation
Authors Ling W , Shoptaw S, Goodman-Meza D
Received 19 July 2019
Accepted for publication 8 October 2019
Published 29 November 2019 Volume 2019:10 Pages 69—78
DOI https://doi.org/10.2147/SAR.S155843
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles Parry
Walter Ling, 1 Steve Shoptaw, 1 David Goodman-Meza 2
1UCLA Department of Family Medicine, Center for Behavioral and Addiction Medicine, Los Angeles, CA, USA; 2UCLA Department of Medicine, Division of Infectious Diseases, Los Angeles, CA, USA
Correspondence: Walter Ling Email [email protected]
Abstract: Buprenorphine has pharmacologic advantages over methadone, especially buprenorphine’s better safety profile. The true significance of buprenorphine’s introduction lies in returning the care of those suffering from opioid use disorder (OUD) to the hands of the physician. The clinical success of buprenorphine has been meager, in part because most physicians have not been exposed to treating these patients. For physicians inclined to treat OUD, the barriers to buprenorphine’s implementation have been onerous and largely counter to the norms of medical practice. Some notable concerns pertain to buprenorphine’s clinical pharmacology like street diversion, unintended use and accidental poisoning. Recently, injectable buprenorphine preparations have been introduced to mitigate these latter shortcomings. Yet, the injectable preparations’ clinical and commercial success has fallen far short of expectation. Here, we review the clinical pharmacology of these products and their expected clinical advantages for the manufacturers, clinicians, policy makers and patients, and offer our perspective, as clinicians and researchers, on how things can improve. Questions remain whether clinicians are willing to overcome barriers to treat OUD using these medications.
Keywords: opioid use disorder, injectable buprenorphine, treatment barriers, stakeholders
Corrigendum for this paper has been published
Introduction
The availability of buprenorphine for opioid pharmacotherapy is the most significant event in addiction medicine since the introduction of methadone maintenance in the 1960s.1,2 Its true clinical significance was not in having another safe and effective medication to treating Opioid Use Disorder (OUD), but in bringing OUD pharmacotherapy to mainstream medicine.3,4 Likewise, the coming of injectable buprenorphine formulations marks another watershed event in the treatment of OUDs. This article reviews where we started and imagines the future as the story unfolds.
While by no means a panacea, buprenorphine is pharmacologically a vast improvement over methadone. Its safety profile and its Drug Enforcement Administration (DEA) Schedule III status enable medical practitioners to prescribe it in their usual practice setting. However, it is an opioid and like all opioids have the potential for street diversion, unintended use and accidental poisoning.5,6 While desirable therapeutically, the marketed forms need rather high doses–daily or more often–unencumbered by Schedule II constraints, which added more worries. Naloxone was added to the most common marketed formulation to partially address its abuse potential.7 Clinicians today are generally aware that the preferred dosage form in clinical use is the combination product, and that the mono-product containing only buprenorphine is reserved for use in pregnancy to avoid prolonged exposure of the fetus to naloxone.
It is not surprising, then, that from the beginning of its approval for clinical use there was a felt need to develop sustained-release formulations that can greatly reduce or eliminate having a large amount of medications taken away from the clinics or the physicians’ offices. Reckitt Benckiser Group (RBP), now Indivior, began to develop its sustained-release injectable formulation (Sublocade) in 2007, the year after it began to develop its buccal film. Braeburn Pharmaceuticals has developed two separate products: A subcutaneous implant (Probuphine) and a sustained release injectable (Brixadi).
Besides the obvious public health demand to mitigate diversion, abuse and accidental poisoning, there were considerations that sublingual buprenorphine will have inter-dose fluctuation of blood levels, and by inference fluctuating receptor occupancy, which would consciously or unconsciously lead to craving and use of illicit opioids. A sustained release formulation that can produce a sufficient steady-state blood level would obviate these fluctuations and relieve the patient from the daily preoccupation with their medications and worries over withdrawal.
The first sustained release buprenorphine formulation available to clinicians was Probuphine. It is perhaps a good place to begin this review. See Table 1 for a comparison of available products.
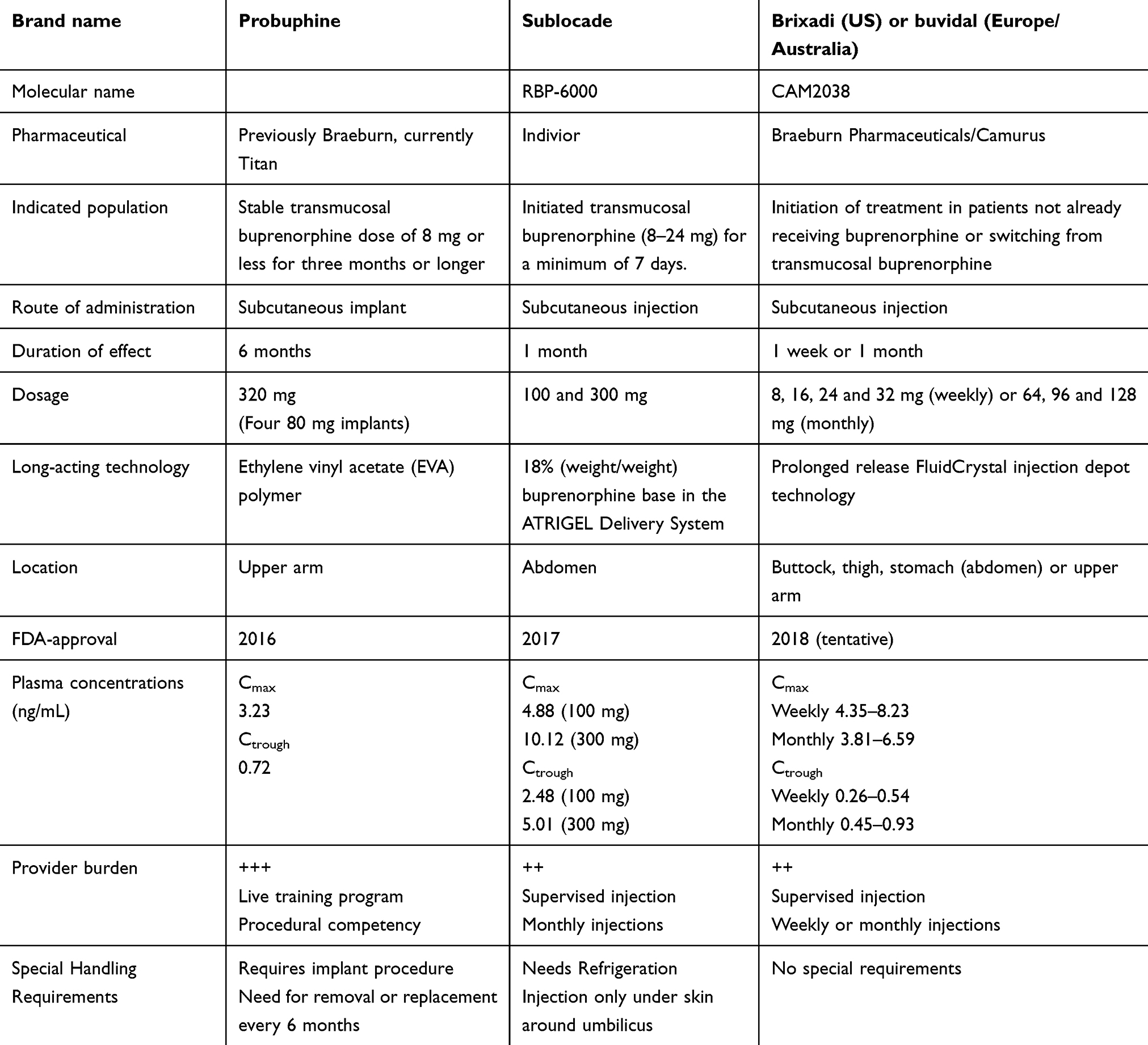 |
Table 1 Comparison Of Long-Acting Formulations Of Buprenorphine FDA-Approved For Treatment Of Opioid Use Disorder |
Probuphine
Probuphine is a subcutaneous implant formulation of buprenorphine. Each implant, a 2.5 mm in diameter and 26 mm in length rod, contains 80 mg of buprenorphine HCl blended and extruded with an ethylene vinyl acetate (EVA) polymer. Four implants are inserted sub-dermally into the inner side of the upper arm in a brief office procedure under local anesthesia, and provides a sustained non-fluctuating buprenorphine blood level over 6 months. Probuphine is not biodegradable and at the end of each 6-month period, the implants are removed in a similar brief in-office procedure. Reducing the risk of diversion, improving medication adherence, obviating the daily fluctuating blood levels and reducing overall drug exposure to patients were some of the anticipated advantages of Probuphine over the sublingual preparations in treating OUD.
In early human trials, two and four implant rods of 90 mg buprenorphine each achieved plasma concentrations (Cmax) of 2.00 ng/mL and 3.23 ng/mL approximately 17 and 16 hrs respectively post implant. The plasma concentrations reached a plateau 21–28 days after implant and were sustained through 6 months, averaging 0.37 ng/mL and 0.72 ng/mL, respectively, for the 2 and 4 implants.8
The critical study to establish Probuphine clinical efficacy and safety was an 18-site double-blind placebo-controlled trial of 163 adults meeting DSM-IV criteria for opioid dependence, randomly assigned, after a 12–16 mg/day sublingual buprenorphine induction and stabilization over 3 days, in a 2:1 ratio to the active buprenorphine or placebo implants. The active implant group had better retention, less opioid use, fewer withdrawal symptoms; lower craving scores, and better global clinical improvement rated by patients and investigators.9 In a subsequent phase III randomized, double-blind, placebo-controlled trial, subjects received either 4 buprenorphine implants (80 mg/implant) (n=114), 4 placebo implants (n=54), or open-label buprenorphine/naloxone (12–16 mg/d) (n=119). The results showed that, compared to placebo, the buprenorphine implant group used significantly less opioids and was clinically similar to those receiving sublingual buprenorphine/naloxone.10
The common side effects and adverse events of the buprenorphine implant, except for those relating to the insertion and removal of the implants, were unsurprisingly similar to those of sublingual buprenorphine: headache, drowsiness, nausea, anxiety, depression, insomnia, and constipation are common. Less common side effects include weight gain, irregular menstruation, diminished libido, sweating, itching, and dental caries. Those relating to implant insertion and removal were pain, local swelling, bruising, bleeding, scarring, itching and infection. Most adverse effects proved to be minor; the procedure was modified and improved considerably during the implant’s clinical roll-out.8–10 Probuphine became clinically available in 2016. Braeburn Pharmaceuticals undertook its clinical marketing.
Still, the launching of Probuphine was not a commercial success. The biggest problem involves a simple surgical procedure: something the majority of the addiction medicine specialists, mostly psychiatrists, had no inclination for. Fewer than one in ten of those who attended the trainings did even a single implant. An added barrier to its clinical success was the needed implant removal after 6 months.11 The general impression among clinicians is that the benefits were by and large not worth the hassle of being trained to perform a surgical procedure, the need for recertification for the procedure and the fact that only well-managed patients on low stable buprenorphine can use the implant. Furthermore, there remains little demand from patients for the product that could shape provider interests.12,13 There was no marketing addressing the growing cadre of primary care clinicians who treat OUD using medications, and who may be much more comfortable with simple office procedures. Instead, demand grew for the existing treatment, sublingual buprenorphine, which was working quite well.14 The marketing of Probuphine has reverted to Titan, its eventual success remains uncertain.
Sublocade
RBP-6000 (Indivior) is a drug-device combination product with 18% (weight/weight) buprenorphine base in the ATRIGEL Delivery System, designed to be subcutaneously injected monthly in the abdominal area.15 ATRIGEL contains a biodegradable polymer dissolved in a biocompatible solvent. When the liquid polymer system is injected with a conventional syringe it solidifies on contact with body fluids to form a solid implant and entraps within it the incorporated buprenorphine into the polymer matric as it solidifies and is slowly released as the polymer biodegrades. Formulations are available in 100 and 300 mg once monthly injections.
Sublocade was designed to deliver a level of plasma buprenorphine that translates into at least a 70% sustained mu-opioid receptor occupancy in the brain over 1 month.16 The developer emphasized the product’s ability to generate a sustained average plasma drug concentration of 2–3 ng/mL which had been shown to be associated with mu-opioid receptor occupancy ≥70% and the reduction of illicit opioid use. Sublocade 300 mg delivers average buprenorphine plasma levels of approximately 2 ng/mL after the first injection. The average concentration of Sublocade at steady-state was 3.21 ng/mL and 6.54 ng/mL for the 100 mg and 300 mg doses, respectively.16
Indivior conducted an Opioid Blockade Study (RB-US-13-0002) which investigated the ability of Sublocade 300 mg to block the subjective effects of illicit opioids, including drug-liking. In the 12-week trial evaluating the blocking effect, Sublocade 300 mg fully blocked the drug-liking effects of hydromorphone, a potent opioid commonly used in human studies to evaluate opioid drug-liking.17
The critical phase III efficacy and safety trial involved 36 treatment centers across the US enrolling 504 treatment-seeking adults aged 18–65 who were randomly assigned to receive BUP-XR 300 mg/300 mg: 6 monthly BUP-XR 300 mg injections (n=201); BUP-XR 300 mg/100 mg: 2 monthly 300 mg followed by 4 monthly 100 mg injections (n=203); or monthly placebo injections (n=100). The primary outcome for efficacy was the participants’ percentage of negative urine samples and self-reports of illicit opioid use from week 5 to week 24. The mean participants’ percent abstinence was 41.3% (SD 39.7) for the 300 mg/300 mg group, 42.7% (SD 38.5) for the 300 mg/100 mg group, and 5% (SD 17.0) for the placebo group (p ˂0.0001 for both BUP-XR groups). Common side effects were headache, constipation, nausea, and injection site pruritus, consistent with other buprenorphine products except for the site-injection reactions – mostly mild and not treatment-limiting – reported by over 5% of the BUP-XR recipients.18
The US Food and Drug Administration (FDA) approved Sublocade in November 2017, for the treatment of moderate to severe OUD in patients who have initiated treatment with a transmucosal buprenorphine-containing product followed by dose adjustment for a minimum of 7 days.19 It became available to patients in the US in 2018. Since its roll out more than a year ago and despite its promise, few patients have received Sublocade. That is not a success story. So what happened? Did the product fail to deliver what it promises? Are there problems getting the medications to the patients? Have the right messages been delivered to those who can benefit from the product and those who were to provide them?
Brixadi (CAM 2038)
In December 2018, the US FDA approved a second injectable buprenorphine product, CAM 2308, now named Brixadi (Braeburn Pharmaceuticals and Camurus).20 Brixadi is a once weekly or once monthly extended-release, prefilled small volume, injectable buprenorphine, that uses the FluidCrystal injection depot technology which comprises a low volume lipid-based liquid with a dissolved active ingredient. Upon injection and contact with tissue fluids, the solution transforms into a nanostructured liquid-crystalline gel effectively encapsulates the buprenorphine and subsequently releases it at a controlled and steady rate over the one-week or one-month period as the depot slowly biodegrades in the subcutaneous tissue.21,22 Brixadi is delivered with a thin 23-gauge needle and administered in the buttock, thigh, stomach (abdomen) or upper arm. Brixadi does not require refrigeration and therefore facilitates reduced storage logistics. Having different compositions and doses should facilitate flexible and individualize treatment from its initiation.
In a pivotal Phase 3 efficacy and safety trial evaluating the range of weekly and monthly doses, Brixadi was titrated to effect in a blinded fashion. Brixadi met the primary endpoint of non-inferiority for responder rate (p<0.001) versus daily sublingual buprenorphine/naloxone (SL BPN/NX). The trial included real-world patients: 26% tested positive for fentanyl prior to study randomization, 71% were using heroin at study initiation and 52% were using injectable opioids at study initiation. For the trial’s key secondary endpoint, Brixadi demonstrated superiority to SL BPN/NX in the percentage of negative opioid assessments from week 4 through 24 (p=0.004). Brixadi is the only injectable buprenorphine studied against the standard of care (SL BPN/NX), with no opioid overdoses in patients receiving Brixadi during clinical trials.23
The safety profile of Brixadi was generally consistent with the known safety profile of oral buprenorphine with the exception of mild-to-moderate injection-site reactions. The most common adverse reactions (occurring in ≥5% of patients) included injection-site pain, headache, constipation, nausea, injection-site erythema, injection-site pruritus, insomnia and urinary tract infections.
The FDA’s tentative approval to Braeburn Pharmaceuticals of Brixadi follows the recent approvals granted to Camurus for Buvidal® by the European Commission and the Australian Therapeutic Goods Administration in November 2018.
What is In It For Me? Stakeholders’ Perspectives
To this point, this review presented medical and potential treatment advantages and disadvantages for the different medications. This section presents stakeholder’s perspectives on the medication. The three long-acting formulations all posit they will improve treatment outcomes for OUD. Still there has been no demonstrated superiority of outcomes using extended-release formulations over oral daily product. More there is little to no uptake of long-acting products. So the bottom-line benefit to using extended release formulations depends on which stakeholder you talk to: the patients, the providers, the society at large and the manufacturer. Let us consider their respective interest in the reverse order; as they are not necessarily the same.
For the manufacturer, regardless of what else may motivate them, is the need for success in the market place. So far neither Probuphine nor Sublocade have shown broad commercial success, and it is too soon to make a call for Brixadi. Commercial success is important for the manufacturer and should not be understated. Commercial success incentivizes the current players in the market and others in the pharmaceutical industry to continue research and development of better and newer products for OUD and other substance use disorders where pharmacological management is scarce (i.e., stimulant use disorder).
For the society, the interest is, rightfully, to reduce social harm, especially in the context of the current opioid epidemic. We want to see overdose deaths diminished, if not gone completely, especially when such deaths involve someone we know or someone we love. Beyond that, society has a strong interest in safe communities. We want a reduction in public injection, petty thefts and more serious property crimes. On the other side, society wants their constituents to return to be productive members of the society. We also welcome new treatments that increase the number of people in care and who stay in care.
Clinicians have complex interests–including treatment adherence and improvements in their patients’ outcomes, like reducing emergency room visits and hospitalizations. However, clinicians are also concerned for more litigious aspects of care that include medication mismanagement (diversion, loss and replacement, misuse and accidental poisoning), and the threat of law suits and DEA inspections that can be levied against a provider at any time and with no cause.24 Medication formulations that are administered by clinicians, obviating the need of taking away medications, would seem like a blessing indeed. But that reassurance is countered by the hassle involved to administer the medications.
For Probuphine the burden is more than trivial, including the need for initial training and later re-certification for implant insertion and removal. The training takes away productive time from clinicians in community. The procedure is not easily incorporated into routine practice, especially in psychiatric offices. Only patients stabilized on 8 mg daily buprenorphine or less are qualified for the implants, there are limits to two implantable sites, and patients must be located for implant removal at the end of 6 months. There are complexities involved in getting the implant from the supplier to the physician placing it, plus the prep work for the implant requires support and coordination. Finally, since roll-out for Probuphine has been limited, most patients have little knowledge about the new formulation and few clinicians have the time or expertise to explain to patients the risks and potential benefits to new formulations. Clinicians with patients whose lives have changed from stable sublingual preparations may decide that the potential benefit from switching to long-acting injectables is simply not worth the bother.
Patients, not surprisingly, have most at stake. After all, they are the ones who actually get the injections or implants and tolerate unpleasant injection site irritations and other side effects. True enough, the safety data have been reassuring; side effects have been inconveniences and annoyances rather than actual harm. Still, there is the real, unspoken risks for patients switching from their predictable, stable lives made possible by buccal daily medication to an unknown routine using long-acting treatment, which may mean losing hard-earned gains during treatment. Early survey-based research on patients’ perspectives on depot formulations had been favorable with high ratings on topics such as the ability for depot medications to make life easier, avoid stigma, and free-up time for other activities.25 Yet, a series of in-depth qualitative studies have raised concerns.12,13,26,27 These include issues with a surgical procedure, the invariability of the daily dose, concerns for infection, and social isolation – due to no longer frequenting the methadone clinic.12,26 The granular subjective experiences when patients use buprenorphine as treatment for OUD appear more powerful in making decisions about injectable formulations that extend beyond simple calculations of costs or of coverage that can vary for 1 week, 1 month and 6 months. These studies clearly highlight the complexity in selecting an injectable formulation from the patient’s perspective. Likely the most important perspective.
As members of the community, patients share the acknowledged benefits to long-acting injectables as described: improved adherence, no medication diversion, resolution of need for daily treatment for opioid use disorder. But at the end of the day, patients still want to know: What is in it for me? To be sure, there are benefits. Long-acting injectable formulations reduce the number of required clinic visits, eliminate the need for take home medications, protect against loss of privacy or of being stigmatized from attending treatment programs, and facilitate the ability to travel freely (at least for a week or a month on the injectable formulations, and 6 months on the implant). Finally, and importantly, these injectable formulations are new in the marketplace and introduce significant costs compared to sublingual buprenorphine. Even for those who have health insurance, out-of-pocket co-pays, frequent office visits and documentation required for pre-authorizations can dampen the willingness of patients to use injectable products when they know well how to use a cheaper, predictable oral daily product.
For scientists and researchers, the new formulations promise a higher level of opioid receptor occupancy, and a higher steady blood level, which should reduce craving and provide consistent blockade of the effects of street opioids. Yet, people do not feel greater “receptor blockade” in their brains from the long-acting products. Few stop using opioids due to receptor blockade. If they did, naltrexone, the mother of all receptor blockers would be used far more often than is currently the case. The part about craving is easier to understand. Craving is mostly triggered by something that brings back memories of drugs. Once craving starts, it grows and usually leads to use.28 So a medication that keeps people from craving opioids should help stop use. But there is no signal that tells us we are not having craving. So the unique benefit to long-acting injectables may be helping patients not to think about street drugs or the treatment medications, independent of craving. That represents freedom, liberty. The question, then, is this: What to do with this new found freedom and liberty?
The Bigger Picture
Perhaps it is good to step back and think about the overall goal when treating OUD. Many terms have been used, from Detox to Relapse Prevention to Rehabilitation (Rehab for short), all of which is equated with getting off drugs, staying off drugs and getting (back) a life. To put it simply, the whole idea of treating people with an OUD is to make a difference in their lives – not just stop using drugs. People who seek treatment have resolved ambivalence over the positive aspects of opioids; they are having a hell of a time and want change.
A major issue with recovery involves the blocks of time that were prior allotted to finding drug, using drug and recovering from drug. Before addiction, people filled their lives with work, families and friends, and activities that had low reinforcing value, but generally anchored people in their lives. With resolution of the medical and biological aspects of OUD, many patients find the skills involved in maintaining their lives before drugs have been retired for so long that the behavioral steps to “getting their lives back” are either gone or require so much work that people become demoralized.
“Getting ones’ lives back” as part of recovery slowly reentered thinking only of late.29,30 This involves patients RE-building their lives – not simply not resuming active drug use. Long-term treatment success for OUD is simply life: boring, low-reinforcing, routine. And it requires work and commitment from patients, their families and their clinicians. For example, if you dropped out of your life for say 5 or 10 years because of OUD, your chances of getting back your life solely by getting off and staying off drugs are pretty close to nil. Most need a program that helps them to re-enter their lives. The treatment system, with rare exceptions, does little of that sort. There are shared beliefs that talks with counselors, mindfulness and meditations and going to 12-step meetings will get you on track to returning to your life as an airplane mechanic, assembly line worker, tech expert or movie star. Yet, these activities reinforce skills needed to succeed in treatment settings. Few programs teach patients how to succeed with their recovery in their lives when they engage anew with remnants from former lives (if still possible) with spouses, families, jobs, careers. The retraining that can help patients make a real difference in their lives is mostly absent. At the end of the day, the most significant benefit to injectable medications may be to keep patients from constantly being preoccupied with their medications. If the injectable frees patients from that constant pre-occupation, that would be true Liberty.
Who Is Likely To Benefit From Long-Acting Formulations?
There is little science to guide us on what patients the new formulation might be best for: Patients who are ready to make life changes, patients already stabilized and maintained on certain dosages, patients who have trouble resisting street opioids, patients who are incarcerated or are on the verge of being released, patients with insurance. Such classifications implied that different patient groups will respond differently to distinct agents and formulations. The rationale has never been made clear. After all, all that the medications can do is to change the physiology of people who take them. The implication is that people in different circumstances have different physiological responses to the same medication. There is zero evidence that such is the case. Instead, any treatment outcome differences depend on what patients do with the energy and time to get their life back. Anyone with an OUD who can benefit from oral buprenorphine can benefit from the injectable. Any artificial attempt to define who is suitable and who is not simply raising barriers to the treatment. The reality is that long-acting injectables are not a cure-all, they are another tool for the clinician, or another option on the menu for the patient. Choice tends to be good.
One of the main behavioral advantages of why a long-acting injectable will be superior to a daily oral medication is that the patient does not have to remember to take the medication every day for the medication to be effective. Forgetfulness as a barrier to adherence may be true for contraceptives, antipsychotics, rheumatology drugs, and medications for HIV treatment and prevention. These are other fields with proven or emerging experience with long-acting formulations. In those areas, there may not be much of a change from day-to-day if the patient’s life if he forgets or decides not to take a daily dose of oral medication. Yet, for people living with an OUD this is not the case. As the opioid – be it heroin, fentanyl, methadone, buprenorphine, you name it – is eliminated or metabolized, the patient is obsessed with taking his next dose due to his/her/their fear of withdrawal. Just drive past a methadone clinic at five in the morning to see people with OUD lined up awaiting their next dose to prove our point.
Viewed in the context of the current opioid epidemic the availability of the injectable buprenorphine formulations should add a very powerful tool to communities’ fight against the epidemic. Sublocade has now been available for over a year. Word on the street is that its uptake has been way slower than anticipated. The reasons are legion but they have little to do with the medication itself and much to do with responses by the stakeholders. Recent work31 shows that despite the opioid crisis, patients may sign up for medication-assisted therapy but leave that care within the first 6 months. Why are we not more successful in using the tools we have to combat the opioid crisis? Why do they keep dying?
The System Issue
The opioid treatment system is mostly rooted in methadone. The system is over 60 years old and we have made little effort to change and improve on it. While other countries have expanded the use of methadone for the treatment of OUD to primary care clinics, in the US we have restricted it to difficult to access opioid treatment programs (OTP). Due to this, training physicians get little exposure to methadone; thus, practicing physician’s fear its use, leading to a dearth of physician workforce willing to prescribe methadone. In turn, the OTP’s major effort has been to negotiate reductions in physician involvement. Clinical decision making is increasingly driven by counselors and managers, and physician’s signoff without ever having discussions with patients.
Recently, several state Medicaid programs have expanded coverage for provision of buprenorphine at the OTP. The OTP may be an ideal setting for expansion of injectable long-acting buprenorphine formulations. This could avoid the mingle within the OTP’s waiting room that leads to uptake of new substances as the patient would only have to come for their long-acting dosing and units of counseling. However, two things must happen. Drug prices for these products must come down, and the system needs to reimburse clinics adequately to incentive the provision of this service. Society (better said the government) needs to invest in treating addiction adequately, especially in OUD, where we actually have treatments that have been proven to work.
New providers must be targeted to provide long-acting injectables. As the opioid epidemic has devastated different parts of the US, providers that had never had an interest in providing addiction care are slowly getting engaged. Yet, the Drug Addiction Treatment Act – 2000 (DATA2000), continues to be a barrier to physicians willing to prescribe buprenorphine – requirements like a course to get an “X-waiver”, a limit on the number of patients to be treated, and open door for “no-cause” inspections by the DEA – slow down uptake and provision of buprenorphine. Physicians from low paying specialties that include family and internal medicine and infectious diseases are leading the charge for expanding access to buprenorphine. These physicians could receive an additional incentive to provide “procedures” for implantable and injectable buprenorphine, hence, providing higher reimbursement rates.
We keep talking patient-centered and individualized treatment but insist that we know what is best for them and what we advocate is good for everybody. In a study comparing buprenorphine with simple medical management, with and without added psychosocial treatment, the majority of patients found medication most helpful; only 1% found psychosocial treatment most helpful.32 Yet we label what the World Health Organization called psychosocial assisted medical treatment “medication assisted treatment”, delegating medication to a secondary therapeutic role.
This is not to say that psychosocial supports are not important, but they must be of practical use to the patients—things like transacting tasks of getting back their children, driver’s license and jobs, instead of depth psychotherapy approaches. Many patients in the current opioid crisis have had a life that they can return to; it makes little sense to insist on having them come for therapy. Give them medications to keep them from dying and let them get on with their lives. Many people in the current crisis live in the rural areas, providing supports such as transportation are far more useful than psychotherapy.
Let us transform “detox” into long-term recovery. There is no evidence that “detox” works. However, it is still the most commonly promoted treatment for OUD in this country. We promote “detox” as if it will cure OUD in the fashion we promote destination weddings, as if it will reduce divorced rates. There is a strong bias in the treatment system for patients to be “drug-free” in recovery in spite of all the data to the contrary.33,34 In many recovery settings, patients stable on buprenorphine are not considered “sober,” to the detriment of patients. Yet it is these medications that let patients ignore the power of opioid withdrawal and conditioned cues and triggers to remain free of street opioids. “Detox” has the highest rates of relapse of any treatment modality and one of the most vulnerable times for overdose.35 Clinicians let patients leave “detox” without medications that might keep them alive; instead we give them memorials when they are dead. Long-acting injectables offer a stable bridge back into the community after inpatient programs or when leaving the structure of outpatient programs.
Conclusion
Long-acting injectable formulations of buprenorphine are novel additions to the repertoire of tools for the treatment of OUD. Their efficacy in clinical trials has been proven, yet, their uptake has lagged in the US. Stakeholders have different motivations for the success of these long-acting formulations. However, without real system change, it may be that the impact of these medications will be missed in the future.
Models for that system change are available internationally, where policy makers emphasize efforts to reduce barriers to medications for persons with OUD. Medications, even full agonists like methadone and prescribed heroin, are delivered regularly in primary care or pharmacy settings. Since the FDA approved methadone as the first real medical treatment for heroin addiction in 1972, the rest of the world learned from us and evolved and modified their treatment systems to best serve their patients accordingly to their societal values. Meanwhile, we continue to conduct methadone treatment with virtually no change for the last 50 years. That is in itself astounding but nobody in leadership seems bothered by it.
We supported the methadone treatment system to grow into a self-serving profit-making industry while we kowtow to the non-medical philosophy of the “recovery” industry. We are complicit by tolerating well-intentioned stakeholders who critique medication for OUD as swapping a “drug for a drug,” with the clear inference that patients maintained successfully on medication are not “in recovery.” We make it worse when we promote non-opioid-based treatments that have little clinical utility36 or of antagonist treatments that work only for a select segment of patients living with OUD.
Long-acting depot buprenorphine medications likely have a place in the toolkit for recovery, what place, is yet to be known. The efficacy is there, the question remains who is most likely to benefit, and how can we best get these medications to them. There is a dearth of systematically collected knowledge regarding patient-, physician-, clinic-, and systems-based factors that support and/or inhibit the prescription of buprenorphine. Research needs to be undertaken to understand these factors, and systematically review these studies to best understand how to maximize these novel depot medications.
In the US, we can do better at using evidence to guide efforts to stem the nearly 50,000 lives lost annually to opioid dependence.37 We know what the problems are. We have the tools to fix the problems. We absolutely have the resources to turn these problems around. The remaining question is whether we have the resolve to do this. So far the answer appears to be that we do not.
Disclosure
Dr Walter Ling reports personal fees from Indivior Pharmaceuticals, outside the submitted work. Dr David Goodman-Meza was supported by the National Institute of Mental Health (grant number DA-2T32MH080634-11) and the National Institute on Drug Abuse (grant number 1K08DA048163-01), during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Greene P. Outpatient Drug Utilization Trends for Buprenorphine Years 2002–2009. FDA Office of Surveillance and Epidemiology. 2010. Presentation Archived by WebCite®. Available from: http://www.webcitation.org/6OJVKGwyg. Accessed October 15, 2019.
2. Fiellin DA. The first three years of buprenorphine in the United States: experience to date and future directions. J Addict Med. 2007;1(2):62–67. doi:10.1097/ADM.0b013e3180473c11
3. Ling W. A perspective on opioid pharmacotherapy: where we are and how we got here. J Neuroimmune Pharm. 2016;11(3):394–400. doi:10.1007/s11481-016-9663-z
4. Ling W. Buprenorphine for opioid dependence. Expert Rev Neurother. 2009;9(5):609–616. doi:10.1586/ern.09.26
5. Lugoboni F, Zamboni L, Cibin M, Tamburin S; Gruppo Inter SdCS. Intravenous misuse of methadone, buprenorphine and buprenorphine-naloxone in patients under opioid maintenance treatment: a cross-sectional multicentre study. Eur Addict Res. 2019;25(1):10–19. doi:10.1159/000496112
6. Moratti E, Kashanpour H, Lombardelli T, Maisto M. Intravenous misuse of buprenorphine: characteristics and extent among patients undergoing drug maintenance therapy. Clin Drug Investig. 2010;30 Suppl 1:3–11. doi:10.2165/11536020-000000000-00000
7. Webster LR, Smith MD, Unal C, Finn A. Low-dose naloxone provides an abuse-deterrent effect to buprenorphine. J Pain Res. 2015;8:791–798. doi:10.2147/JPR.S90780
8. White J, Bell J, Saunders JB, et al. Open-label dose-finding trial of buprenorphine implants (Probuphine) for treatment of heroin dependence. Drug Alcohol Depend. 2009;103(1–2):37–43. doi:10.1016/j.drugalcdep.2009.03.008
9. Ling W, Casadonte P, Bigelow G, et al. Buprenorphine implants for treatment of opioid dependence: a randomized controlled trial. JAMA. 2010;304(14):1576–1583. doi:10.1001/jama.2010.1427
10. Rosenthal RN, Ling W, Casadonte P, et al. Buprenorphine implants for treatment of opioid dependence: randomized comparison to placebo and sublingual buprenorphine/naloxone. Addiction. 2013;108(12):2141–2149. doi:10.1111/add.12315
11. Administration FD. PROBUPHINE (buprenorphine) implant for subdermal administration CIII. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/204442Orig1s000lbl.pdf. Published 2016.
12. Neale J, Tompkins CNE, Strang J. Prolonged-release opioid agonist therapy: qualitative study exploring patients’ views of 1-week, 1-month, and 6-month buprenorphine formulations. Harm Reduct J. 2019;16(1):25. doi:10.1186/s12954-019-0296-4
13. Neale J, Tompkins CNE, McDonald R, Strang J. Implants and depot injections for treating opioid dependence: qualitative study of people who use or have used heroin. Drug Alcohol Depend. 2018;189:1–7. doi:10.1016/j.drugalcdep.2018.03.057
14. Alderks CE. Trends in the use of methadone, buprenorphine, and extended-release naltrexone at substance abuse treatment facilities: 2003–2015 (update). In: The CBHSQ Report. Rockville, MD: Substance Abuse and Mental Health Services Administration (US); 2013:1–8.
15. Dunn R. The atrigel drug delivery system. In: Rathbone M, Hadgraft J, Editors. Modified-Release Drug Delivery Technology. Boca Raton, FL: CRC Press; 2002.
16. Laffont CM, Gomeni R, Heidbreder C, Jones JP
17. Nasser AF, Greenwald MK, Vince B, et al. Sustained-release buprenorphine (RBP-6000) blocks the effects of opioid challenge with hydromorphone in subjects with opioid use disorder. J Clin Psychopharmacol. 2016;36(1):18–26. doi:10.1097/JCP.0000000000000434
18. Haight BR, Learned SM, Laffont CM, et al. Efficacy and safety of a monthly buprenorphine depot injection for opioid use disorder: a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2019;393(10173):778–790. doi:10.1016/S0140-6736(18)32259-1
19. Hertz S Approval package for: SUBLOCADE extended-release injection for subcutaneous use, 100 and 300 mg. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/209819Orig1s000Approv.pdf. Published 2017.
20. Hertz S Tentative approval of BRIXADI. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2018/210136Orig1s000TALtr.pdf. Published 2018.
21. Albayaty M, Linden M, Olsson H, Johnsson M, Strandgarden K, Tiberg F. Pharmacokinetic evaluation of once-weekly and once-monthly buprenorphine subcutaneous injection depots (CAM2038) versus intravenous and sublingual buprenorphine in healthy volunteers under naltrexone blockade: an open-label Phase 1 study. Adv Ther. 2017;34(2):560–575. doi:10.1007/s12325-016-0472-9
22. Frost M, Bailey GL, Lintzeris N, et al. Long-term safety of a weekly and monthly subcutaneous buprenorphine depot (CAM2038) in the treatment of adult out-patients with opioid use disorder. Addiction. 2019;114(8):1416–1426. doi:10.1111/add.14636
23. Lofwall MR, Walsh SL, Nunes EV, et al. Weekly and monthly subcutaneous buprenorphine depot formulations vs daily sublingual buprenorphine with naloxone for treatment of opioid use disorder: a randomized clinical trial. JAMA Intern Med. 2018;178(6):764–773. doi:10.1001/jamainternmed.2018.1052
24. Mendoza S, Rivera-Cabrero AS, Hansen H. Shifting blame: buprenorphine prescribers, addiction treatment, and prescription monitoring in middle-class America. Transcult Psychiatry. 2016;53(4):465–487. doi:10.1177/1363461516660884
25. Gilman M, Li L, Hudson K, et al. Current and future options for opioid use disorder: a survey assessing real-world opinion of service users on novel therapies including depot formulations of buprenorphine. Patient Prefer Adherence. 2018;12:2123–2129. doi:10.2147/PPA.S180641
26. Neale J, Tompkins CNE, Strang J. Depot buprenorphine injections for opioid use disorder: patient information needs and preferences. Drug Alcohol Rev. 2019;38(5):510–518. doi:10.1111/dar.12939
27. Tompkins CNE, Neale J, Strang J. Opioid users’ willingness to receive prolonged-release buprenorphine depot injections for opioid use disorder. J Subst Abuse Treat. 2019;104:64–71. doi:10.1016/j.jsat.2019.06.007
28. Preston KL, Kowalczyk WJ, Phillips KA, et al. Before and after: craving, mood, and background stress in the hours surrounding drug use and stressful events in patients with opioid-use disorder. Psychopharmacology (Berl). 2018;235(9):2713–2723. doi:10.1007/s00213-018-4966-9
29. Ray LA, Lim AC, Shoptaw S. What defines a clinically meaningful outcome in the treatment of substance use disorders: ‘Getting your life back’. Addiction. 2019;114(1):18–20. doi:10.1111/add.v114.1
30. Ling W. Mastering the Addicted Brain: Building a Sane and Meaningful Life to Stay Clean. Novato, CA: New World Library; 2017.
31. Morgan JR, Schackman BR, Leff JA, Linas BP, Walley AY. Injectable naltrexone, oral naltrexone, and buprenorphine utilization and discontinuation among individuals treated for opioid use disorder in a United States commercially insured population. J Subst Abuse Treat. 2018;85:90–96. doi:10.1016/j.jsat.2017.07.001
32. Ling W, Hillhouse M, Ang A, Jenkins J, Fahey J. Comparison of behavioral treatment conditions in buprenorphine maintenance. Addiction. 2013;108(10):1788–1798. doi:10.1111/add.12266
33. Burns RM, Pacula RL, Bauhoff S, et al. Policies related to opioid agonist therapy for opioid use disorders: the evolution of state policies from 2004 to 2013. Subst Abus. 2016;37(1):63–69. doi:10.1080/08897077.2015.1080208
34. Nowotny KM. Race/ethnic disparities in the utilization of treatment for drug dependent inmates in U.S. state correctional facilities. Addict Behav. 2015;40:148–153. doi:10.1016/j.addbeh.2014.09.005
35. Kleber HD. Pharmacologic treatments for opioid dependence: detoxification and maintenance options. Dialogues Clin Neurosci. 2007;9(4):455–470.
36. Juurlink DN. Lofexidine for opioid withdrawal: small effects at an exorbitant price. J Addict Med. 2019;13(3):167–168. doi:10.1097/ADM.0000000000000473
37. Hedegaard H, Miniño AM, Warner M. Drug Overdose Deaths in the United States, 1999–2017. Hyattsville, MD: National Center for Health Statistics; 2018.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.