")
Back to Journals » Infection and Drug Resistance » Volume 16
Demographic Characteristics and Hot-Spot Areas of Recent Infections Among New HIV Diagnoses in Sichuan, China, Between 2018 and 2020
Authors Yang H , Li Y , He F, Yuan F, Liu L , Li L, Yuan D , Ye L, Zhou C, Zhang Y, Su L, Liang S
Received 14 November 2022
Accepted for publication 18 January 2023
Published 5 February 2023 Volume 2023:16 Pages 779—789
DOI https://doi.org/10.2147/IDR.S394828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Hong Yang, Yiping Li, Fang He, Fengshun Yuan, Lunhao Liu, Ling Li, Dan Yuan, Li Ye, Chang Zhou, Yan Zhang, Ling Su, Shu Liang
Center for AIDS/STD Control and Prevention, Sichuan Center for Disease Control and Prevention, Chengdu, People’s Republic of China
Correspondence: Shu Liang; Ling Su, Email [email protected]; [email protected]
Background: Sichuan Province is severely affected by the HIV epidemic in China. Little is known about the characteristics of recent infections among new HIV diagnoses, which is critical to prevention strategies, evaluation of the HIV epidemic and health resource allocation. Meanwhile, individuals at primary stages of infection are related to the hot-spot areas of ongoing transmission in new HIV diagnoses, which is also rarely known.
Objective: This article aimed to report the proportion of recent infections among new HIV diagnoses, and to reveal demographic characteristics associated with HIV recent infections, and finally, to indicate the hot-spot areas of ongoing transmission in Sichuan province between 2018 and 2020.
Methods: Limiting Antigen (LAg)-Avidity assay was performed to detect recent infection within new HIV diagnoses reported in odd months between 2018 and 2020. Results were reclassified according to the data on CD4 cell count, antiretroviral treatment and the existence of an AIDS-defining illness. Logistic regression was used to determine characteristics associated with HIV recent infections. The spatial analysis was conducted with ArcGIS 10.7 to figure hot-spot areas of HIV recent infections.
Results: 42,089 newly diagnosed HIV-1 cases were tested using the LAg-Avidity EIA. In total, 5848 (13.89%) of those were classified as HIV recent infections. Female, age between 18– 25 years and men who had sex with men were related to higher proportion of HIV recent infections. Logistic regression revealed that MSM aged between 18– 25 years were more likely to be classified as recent infection. Spatial analysis demonstrated significant clustering in Chengdu, Yibin, Luzhou city between 2018 and 2020. Hot spots were mainly clustered in the center of Sichuan in 2018, but gradually spread to southwest and northwest between 2019 and 2020.
Conclusion: Enhanced preventive measures among relevant risk groups and areas where the potential HIV-1 transmission is ongoing is urgently needed to curb further spread.
Keywords: human immunodeficiency virus, HIV, HIV recent infection, Sichuan, hot spots
Background
In 2018, it was estimated that 1.25 million people were living with HIV in China.1 In many regions, an unequal distribution of the HIV epidemic is obvious, especially in certain areas and populations with high HIV prevalence.2 The number of people living with HIV-1 in Sichuan Province increased from 0.13 million at 2018 to 0.17 million at 2020, ranked first in China [unpublished data]. The prevalence increased from 0.16% at 2018 and 0.20% at 2020 [unpublished data]. The number of newly diagnoses HIV-1 cases attributable to heterosexual contact gradually increased, representing 70.44% of all cases at 2018 to 76.2% at 2020 [unpublished data]. In this context, we suspected that there was an upsurge of HIV epidemic in newly diagnosed HIV-1 cases. And some study and targeted interventions should be taken, which has been demonstrated to be effective at the lowest cost.3
It is complicated to evaluate the incidence of HIV infection among new HIV diagnoses per year, owing to the time between infection and diagnosis varies widely among individuals.4 So we chose the proportion and demographic characteristics of HIV recent infection among newly diagnosed to reflect the development of HIV-1 epidemic to a certain extent.
Spatial analysis measures were used to identify hot-spot areas where HIV recent infections relatively increased, relaying on the geographic data of HIV recent infections.
This article aimed to report the proportion of recent infections among new HIV diagnoses, and to reveal demographic characteristics associated with HIV recent infections, and finally, to indicate the hot-spot areas of ongoing transmission in Sichuan province between 2018 and 2020.
Methods
Sample Collection
The blood samples of newly diagnosed HIV-1 cases, which were the residual plasma/serum from HIV-1 diagnostic tests in odd months between 2018 and 2020 were collected from 73 reporting laboratories in Sichuan. Based on the National Guideline on Detection of HIV/AIDS,5 there are three steps for confirmation of HIV-1 antibody: first of all, blood samples are screened for HIV-1 antibody by using Chemiluminescence immunoassay, Enzyme-linked immunosorbent-assay (ELISA), and rapid testing. Secondly, positive samples in the screening tests were confirmed by Western blot (WB). At last, positive samples in the confirmatory tests were considered as HIV-1 sero-positive. Information about age at diagnosis, gender, transmission route, sample source and ethnicity were collected from the national database of HIV/AIDS cases.6 Data quality was ensured by multiple logic checks, which meant that all completed case report forms were dispatched to the National Center for AIDS/STD Control and Prevention after ascertainment of new cases.7 Local CDC staffs double-checked ID numbers, names, addresses and other relevant information at the field-level for avoiding the likelihood of duplication of reported cases.7 Age below 18 years, any documented AIDS defining illnesses, the mother–infant transmission, unknown information on gender or age, or blood samples from double-notified HIV-1 cases were excluded from the analysis.
Ethics Statement
No patient informed consent was given, for the blood samples were residuals from routine HIV diagnostic tests. In addition, due to the national database of HIV/AIDS cases is strictly anonymous, the blood samples cannot connect with an individual. Moreover, the LAg-Avidity EIA is only licensed for research use only and not for clinical use or for use in HIV infection diagnosis. Thus, no extra benefit can be obtained by informing persons about positive LAg-Avidity EIA test results. The study was approved by the Ethics Committee of the Sichuan Center for Disease Control and Prevention and conducted following the Helsinki Declaration of 1964.
Limiting Antigen Avidity Assay and HIV Recent Infection Algorithm
All blood samples in the survey were tested for evidence of recent infection by the Sichuan CDC laboratory using the LAg-Avidity assay from the Maxim Biomedical, Inc, Rockville, USA.8 The tests were performed completely following manufacturers’ instruction manuals. A normalized optical density (ODn) of <1.5 was considered to represent recent infection.
We applied a RITA to reduce misclassification of the LAg-Avidity assay. The criteria we used to reclassify recent cases as long-term cases: a report of an AIDS defining illness, or viral load less than 1000 copies/mL,9 CD4 cell counts less than 200 cells/mm3.10–12 Because the blood samples were collected before the time of HIV diagnosis, all newly diagnosed cases did not participate any antiretroviral therapy. Therefore, in the study the information about CD4 cell counts was used to minimize false recent classification.
In brief, a recent infection case from new HIV diagnoses in our study was defined as: (1) the ODn of the specimen is ≤1.5 in the LAg-Avidity assay (2) CD4 cell counts>200 cells/mm3 (3) without any documented AIDS defining illnesses and antiretroviral therapy. In contrast, a long-term infection case was defined as the ODn>1.5 in the LAg-Avidity assay or CD4 cell counts≤200 cells/mm3. By using above methods, the misclassification of recent cases can be identified and corrected; however the misclassification of long-term cases was not corrected.
Spatial Analysis for HIV Recent Infections
The spatial analysis was conducted with ArcGIS 10.7 (ESRI, Redlands, CA, USA) to visualize hot-spot areas and geographical distribution where HIV recent infection occurred and to create map of distribution of participating laboratories in Sichuan.
Statistical Analysis
Data analysis was conducted in SPSS version 23.0 (IBM, Armonk, New York, USA). The chi2 test was used to analyze the proportion of recent infections among new HIV diagnoses for bivariate comparison and the logistic regression was used to assess the odds ratio for recent infections. The demographic and behavioral factors associated with recent infections classified by RITA were examined by univariable and multivariable analysis using logistic regression. A Mann–Whitney (Wilcoxon) rank sum test of medians was used to compare the age and the CD4 cell counts of the two groups.
Results
Characteristics of New HIV Diagnoses Between 2018 and 2020
Between 2018 and 2020, a total of 42,089 newly diagnosed HIV-1 cases were reported by 73 laboratories province wide (Figure 1). Those cases consisted mostly of men (74.48%; n=3,1346/42,089). The major mode of HIV transmission was HET (92.75%; n=3,9037/42,089), followed by MSM (5.82%; n=2448/42,089), an unknown mode of transmission (0.83%; n=349/42,089) and IDU (0.61%; n=255/42,089).The median age of new HIV diagnoses was 56 years old. One half (53.29%; n=22,431/42,089) was older than 55 years old and one third (23.31%; n=9812/42,089) was between 45 and 54 years old. Most cases were Han (96.46%; n=40,601/42,089). Two half (61.05%; n=25,694/42,089) of the newly diagnosed HIV-1 cases were from medical institution.
 |
Figure 1 Distribution of participating laboratories (n=73) in Sichuan, 2018–2020. |
Data about CD4 cell count was available from 91.15% (n =38,364/42,089). Of those cases, 67.87% (n =26,038/38,364) presented CD4 cell counts below 350 cells, the median of CD4 cell counts was 268 cells/mm3.
The number of new HIV diagnoses were varied from 2018 to 2020, separately 1514, 1872 and 1463. The proportion of HIV recent infections per year varied from 11.10% to 11.87%, No significant trend over time (chi2 p =0.278).
Characteristics of Recent Infections Among New HIV Diagnoses Between 2018 and 2020
In total, 5848 (13.89%; n=5848/42,089) cases were classified as recent infections by the LAg-Avidity assay, of which 999 (17.08%; n=999/5848) were reclassified according to the CD4 cell counts below 200 cells. Finally, RITA determined 4849 new HIV diagnoses to be recent (11.52%, n=4849/42,089,).The proportion of HIV recent infections among men was lower than that among women (10.96% vs.13.15%, chi2 p<0.001). In different transmission routes, MSM produced a highest proportion of recent infections (21.160%) (Table 1). The proportion of recent infections (21.63%) was highest among young persons aged between 18 and 25 years (Table 1).
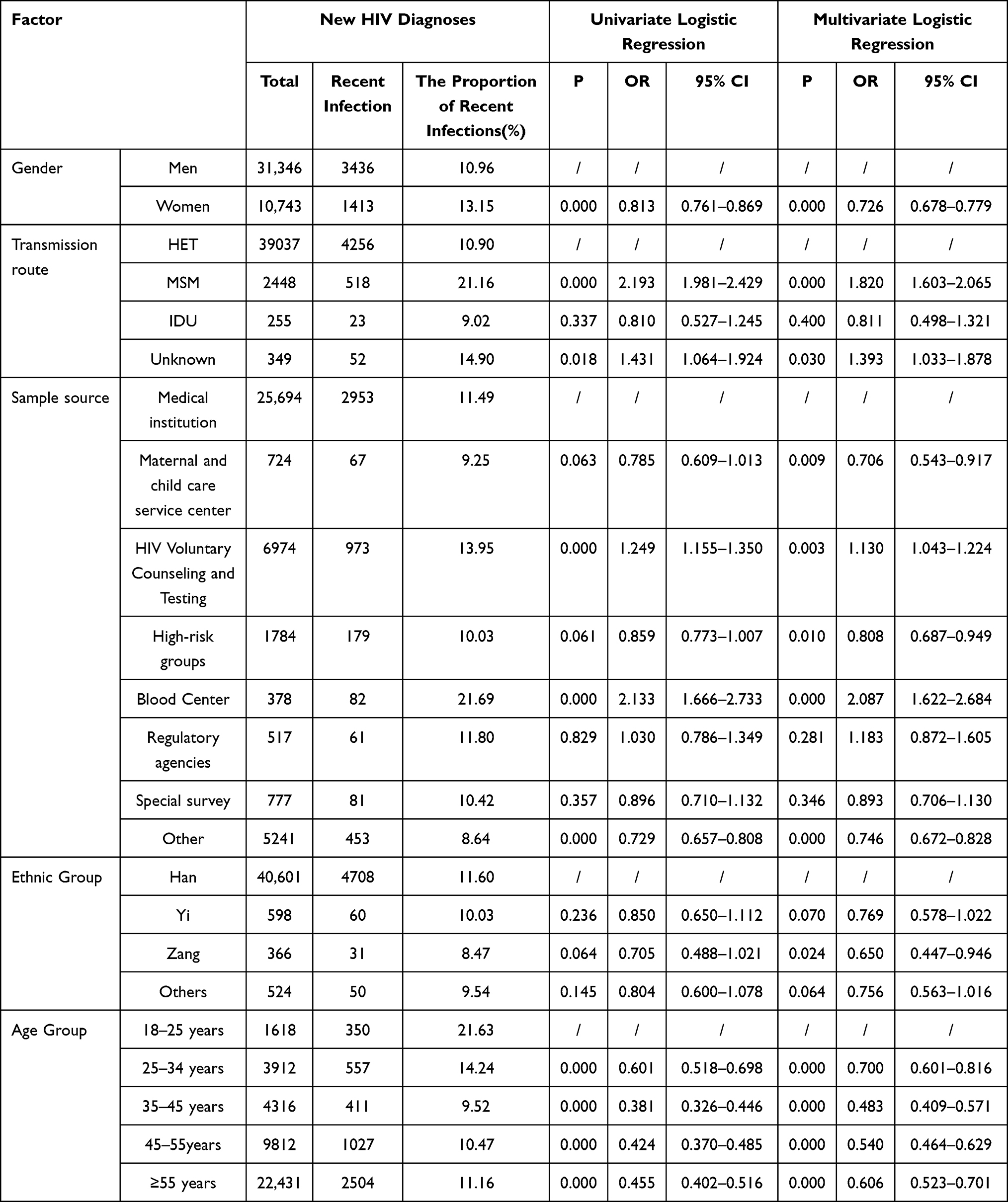 |
Table 1 Factors Associated with HIV Recent Infection Among New HIV Diagnoses in Sichuan, 2018–2020 |
All recently infected individuals were slightly younger than those with a long-term infection (median age 55 vs.56 years; p < 0.001 Wilcoxon). MSM with HIV recent infection had a younger age than those with a long-term infection (median age 26 vs 29 years; p < 0.001 Wilcoxon). There was no difference in age found among HET (median age 57 vs 57; p = 0.215 Wilcoxon) and IDU (median age 36 vs 38; p = 0.121 Wilcoxon). Han was more likely classified as recent infection (11.60% chi2 p < 0.05). The median of CD4 cell counts among recent infections was significantly higher than that among long-term infections (Median 382 vs 251 CD4 cells/mm3; p < 0.001 Wilcoxon).
Factors Associated with HIV Recent Infections
Several factors were associated with HIV recent infection through the univariate logistic regression, like gender, transmission route, age, ethnic group and sample source, which are displayed in Table 1. It showed that MSM were more likely to acquire a HIV recent infection, which was verified both by univariate logistic regression and multivariable logistic regression (OR 2.19; 95% CI 1.98–2.43;OR 1.82; 95% CI 1.60–2.07). Individuals between 18 and 25 years old had a higher chance of being classified as HIV recent infection (Table 1). Medical institution was the major place to catch recent infection cases (Table 1).
Spatial Analysis
Local spatial correlation was applied to the year-wise distribution of hot spots at district levels throughout Sichuan (Figure 2). Hot spots were generally clustered in center of Sichuan in 2018 (Figure 2A), but gradually spread to southwest and northwest between 2019 (Figure 2B) and 2020 (Figure 2C) in Chengdu, Yibin, Luzhou, Zigong, Neijiang, Mianyang, Deyang.
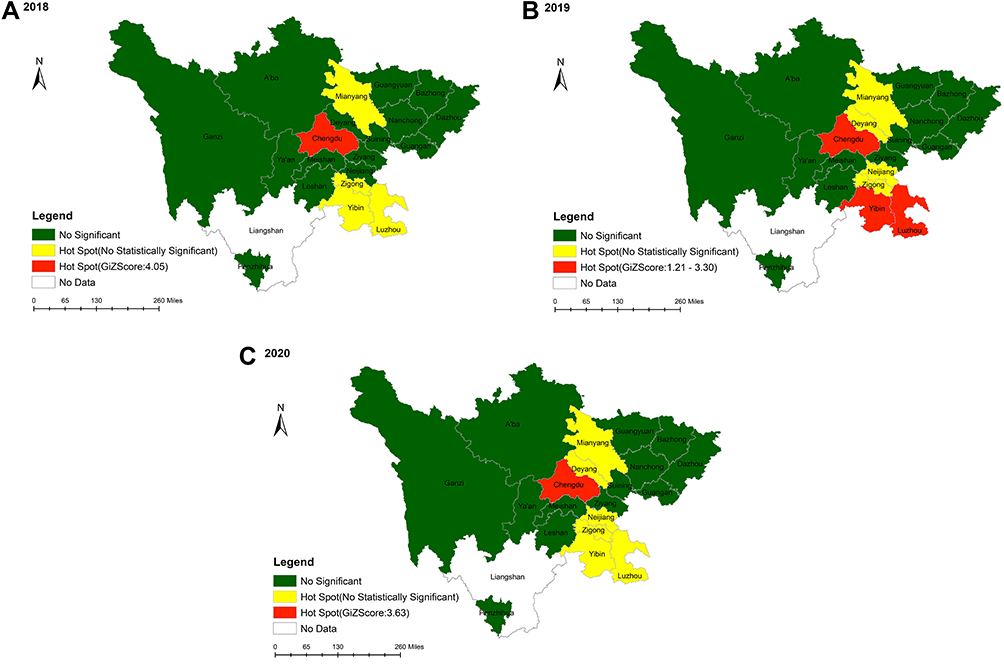 |
Figure 2 2018–2020 Hot spots of HIV recent cases at city level by year.(A) Sichuan province, 2018. (B) Sichuan province, 2019. (C) Sichuan province, 2020. |
To show the relationship between recent infected cases and long-term infected cases in Chengdu, Luzhou, Yibin, respectively, we marked 2267 (1264+453+550) recent infected cases and 17,056 (8043+3281+5732) long-term infected cases by different colors and different sizes of purple circles, separately, thereby the relationship between two groups could be visualized (Figure 3). Different colors indicated the differentiation in numbers of recent infected cases, and different sizes of purple circles indicated the differentiation in numbers of long-term infected cases.
Figure 3 Continued. Figure 3 Continued. Figure 3 Geographical distribution of the total number of HIV recent cases at city level in the years 2018, 2019 and 2020. (A) Chengdu city, 2018. (B) Chengdu city, 2019. (C) Chengdu city, 2020. (D) Luzhou city, 2018. (E) Luzhou city, 2019. (F) Luzhou city, 2020. (G) Yibin city, 2018. (H) Yibin city, 2019. (I) Yibin city, 2020.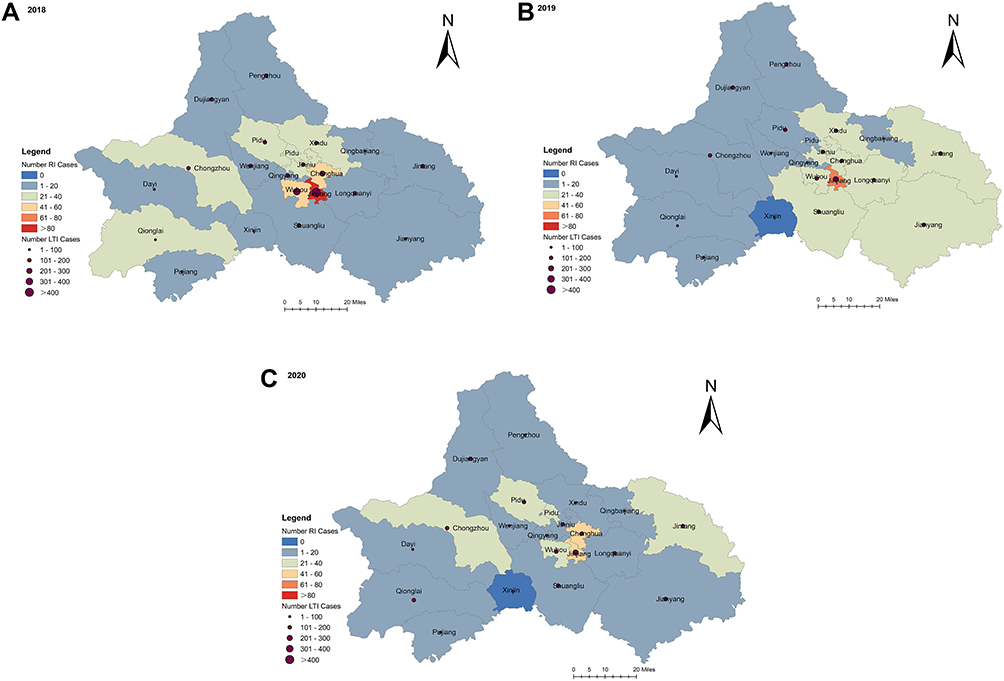
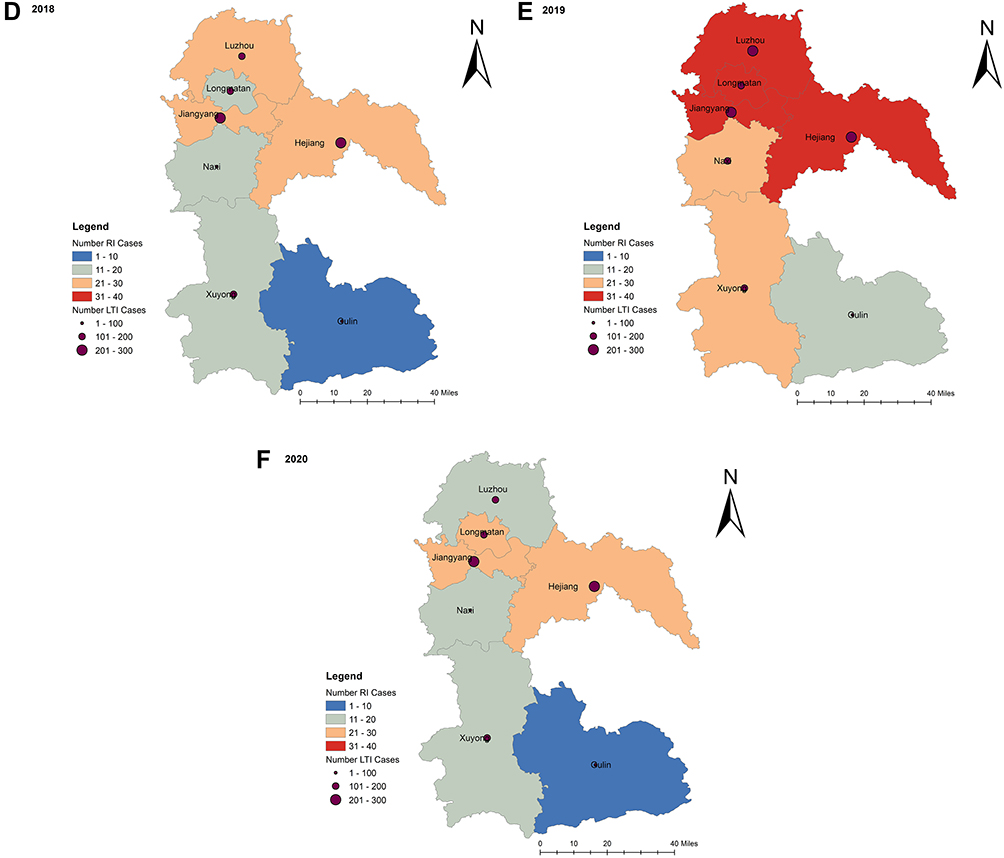

On a whole, the local spatial correlation showed noticeable geographic changes of numbers of recent infection throughout Sichuan during 2018 and 2020.The number of new hot spots varied slightly over the years. These were mainly localized in Chengdu, Yibin, Luzhou. Later these hot spots shifted toward southwest. Significant cluster of recent infected cases were identified in Chengdu (Figure 3A–C), Luzhou (Figure 3D–F), Yibin (Figure 3G–I) from 2018 and 2020, which was a strong signal of high HIV transmission in the recent past.
During 2018 and 2020, the number of recent infected cases and long-term cases were sustainably high in Jinjiang district (Figure 3A–C), Jiangyang district (Figure 3D–F), Hejiang district (Figure 3D–F) and Cuiping (Figure 3G–I) district, separately in Chengdu, Luzhou and Yibin, which suggested that the clustering of recent infected cases accompanied with the high number of long-term cases in those area. Besides, in other areas where numbers of long-term cases was stable, clusters of recent infected cases emerged, such as Longmatan district (Figure 3D–F), which suggested a potential increase of recent infected cases and needs more attention. On the map, there are several areas where long-term cases coupled with only a few recent infected cases, like Gaoxian and Gongxian in Ybin (Figure 3H), which suggested that these areas might exist a certain degree of delay in finding individuals infected with HIV-1. The local CDC should pay more attention to those areas, because the delay might trigger a hidden HIV-1 transmission and need closer attention.
Discussion
To our knowledge, this is the first province-wide study to reveal the characteristics of recent infections among new HIV diagnoses by using RITA, and to determine the hot spots at district levels in China three years in a row.
In our study, the overall proportion of HIV recent infection was 11.52%, which was lower compared with that in other countries such as Sweden13 and England,12 but higher than Yunnan.14 The proportion of recent-infected cases was much lower than that of long-term infections among new HIV diagnoses (11.52%.vs.88.48%). This is probably an alarm from the perspective of prevention, for long-term infection individuals among new HIV diagnoses could lead to potent HIV-1 transmission due to the unawareness of their own HIV-1 infection statue.4,14 Consequently, early detection and intervention of HIV infection are crucial to the prevention.14–16 As a strategy for reducing infections, the accessibility and scale of testing must be taken into consideration, and immediate sustainable treatment must be followed, regardless of the immune status.17,18
MSM was the group most vulnerable to HIV infection in our study, as well as in the Yunnan, England and Germany.4,14,19 MSM was also the group in the study with the highest proportion of HIV recent infection cases among newly diagnosed cases. The national data20 and Sichuan’s data,21 respectively, revealed that HIV-1 incidence among MSM was highest among all sub-population in the sentinel surveillance (5.0, 95% CI:4.1–5.8% and 5.16, 95% CI: 4.65–5.66%). High incidence consequentially lead to high proportion. On the other hand, some studies22,23 recommended MSM should increase the frequency of HIV testing, according to their risk manner. Furthermore, the knowledge, awareness and individual risk behavior for HIV infection among MSM is high.21,24,25 The sensitive health consciousness and more concerns of their infection status might be another reason for the high proportion of HIV recent infection we found in this group.
This study clearly indicated that young residents (aged 18–25) in Sichuan accounted for a substantial proportion of recent infection cases during 2018 and 2020. There were several factors leading to the high proportion of recent infection in this group. Behavioral patterns and societal shifts coupled with unique development changes were known to increase vulnerability to HIV infection faced by young people.26 Inconsistent condom use and risk-taking behaviors were also reported among young African-Americans in United States (aged 18–21), Uganda and China.7,27–30 Lack of comprehensive knowledge about HIV and low self-perceived risk might be the primary risk factors associated with this rising burden of HIV among young people.31–33 Thus, strategies must be tailored to the developmental needs of this age group. Enhanced coverage of HIV testing, improved access to quality services provided by clinicians trained to work with this population and sustained prevention and support services specific for adolescents might bring positive effect with further decrease in high-risk activities among this susceptible group.7,34
Spatial analysis in our study demonstrated significant clustering in Chengdu, Yibin, Luzhou city with a stable situation in number of recent infection cases over time (Figure 2). Many factors influencing the clustering of HIV recent infections: local HIV burden, as shown in Figure 3, the number of long-term infection was sustainably high, which raised the difficulty of HIV control. Density of population, the resident population (year-end, 2020) of Chengdu was almost 21 million, accounting for 25% of that in Sichuan province, and the density of population was 1461 (person/sq.km), which was the highest in Sichuan province.35 That of Luzhou and Yibin was respectively 348 (person/sq.km) and 346 (person/sq.km), ranking tenth and eleventh.35 The high density of population provided the convenience for HIV spread. Chengdu is the provincial capital of Sichuan, with two airports and four railway stations, connecting across the country. Yibin and Luzhou also has one airport and two railway stations. Traffic convenience also provided the convenience for HIV spread.
Though not confirmed, it was still reasonable to speculate that, as most of the universities are sited in those cities, where a variety of students were enrolled each year. The college environment which offered great opportunity for HIV high-risk behaviors, including unsafe sex and multiple partnerships, might be another contributing factor to the appearance of hot spots areas.7,32
Limitation
There were several limitations in our study. First, it was difficult to obtain the exact number of individuals tested over the study period, so we could not immediately estimate the HIV incidence, which is essential to the estimation of HIV epidemic. Second, data of Liangshan were absence, which made this study incomplete, but it has stimulated further research. Finally, since a part of this study was a record-based study, the number of newly diagnosed cases might be affected by accessibility and uptake of HIV-antibody testing as well as the possible impact of prevention efforts.
Conclusion
We demonstrate for the first time significant HIV-1 hot spots in Sichuan province, especially in central and southwestern areas. There is an obvious sign of ongoing HIV transmission in those areas. To distinguish recent infections from new HIV diagnoses and highlight their demographic characteristics and hot-spot areas is a necessary complement to routine HIV-1 surveillance. All findings of this study should receive sufficient consideration, and enhanced preventive measures among appropriate risk groups and areas where the HIV epidemic was concentrated.
Abbreviations
LAg-Avidity EIA, Limiting Antigen Avidity enzyme immunoassay; RITA, recent infection testing algorithm; HIV, Human immunodeficiency virus; HET, Heterosexual contact; MSM, Men who have sex with men; IDU, Intravenous drug user; CDC, Center for Disease Control and Prevention.
Data Sharing Statement
The study database used and/or analyzed during the current study available from the corresponding author on reasonable request.
Acknowledgments
We are very grateful to the staff at the local Centers for Disease Control and Prevention for their assistance in coordinating samples collection and data acquisition.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation; took part in drafting, revising the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the Natural Science Foundation of Sichuan Province (2022NSFSC1547) and Sichuan Science and Technology Program(2019YFS0369).
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Lyu F, Chen F. National HIV/AIDS epidemic estimation and interpretation in China. Chin J Epidemiol. 2019;40:1191–1196. doi:10.3760/cma.j.issn.0254-6450.2019.10.004
2. Zhu Q, JiKe C, Chengdong X, et al. A new strategy to quantitatively identify hot-spot areas in growth of new HIV infections for targeted interventions. Front Public Health. 2021;9:680867. doi:10.3389/fpubh.2021.680867
3. Anderson SJ, Cherutich P, Kilonzo N, et al. Maximising the effect of combination HIV prevention through prioritization of the people and places in greatest need, a modelling study. Lancet. 2014;384:249–256. doi:10.1016/S0140-6736(14)61053-9
4. Hofmann A, Hauser A, Zimmermann R, et al. Surveillance of recent HIV infections among newly diagnosed HIV cases in Germany between 2008 and 2014. BMC Infect Dis. 2017;17(1):484. doi:10.1186/s12879-017-2585-4
5. National Guideline on Detection of HIV/AIDS 2015 . Chinese center for disease control and prevention.
6. Sun LN, Fu SG, Wang L. The history and situation of HIV/AIDS case reporting. Mod Prev Med. 2011;4:70.
7. Xiayan ZHANG, Weiming TANG, Yinge LI, et al. HIV/AIDS epidemic among young people in China between 2005 and 2012, results from spatial temporal analysis. HIV Med. 2017;18(3):141–150. doi:10.1111/hiv.12408
8. Biomedical M. Maxim HIV-1 Limiting Antigen Avidity EIA, Single Well Avidity Enzyme Immunoassay for Detection of Recent HIV-1 Infection. Rockville, Maryland USA: Maxim Biomedical, Inc; 2013.
9. Kassanjee R, Pilcher CD, Keating SM, et al. Independent assessment of candidate HIV incidence assays on specimens in the CEPHIA repository. AIDS. 2014;28(16):2439–2449. doi:10.1097/QAD.0000000000000429
10. Robinson E, Moran J, O’Donnell K, et al. Integration of a recent infection testing algorithm into HIV surveillance in Ireland, improving HIV knowledge to target prevention. Epidemiol Infect. 2019;147:e136. doi:10.1017/S0950268819000244
11. Romero A, Gonzalez V, Esteve A, et al. Identification of recent HIV-1 infection among newly diagnosed cases in Catalonia, Spain (2006–08). Eur J Public Health. 2012;22(6):802–8.doi. doi:10.1093/eurpub/ckr179
12. Aghaizu A, Murphy G, Tosswill J, et al. Recent infection testing algorithm (RITA) applied to new HIV diagnoses in England, Wales and Northern Ireland, 2009 to 2011. Euro Surveill. 2014;19(2):20673. doi:10.2807/1560-7917.es2014.19.2.20673
13. Widgren K, Skar H, Berglund T, Kling AM, Tegnell A, Albert J. Delayed HIV diagnosis common in Sweden, 2003–2010. Scand J Infect Dis. 2014;46(12):862–867. doi:10.3109/00365548.2014.953575
14. Chen M, Yanling M, Chen H, et al. Demographic characteristics and spatial clusters of recent HIV-1 infections among newly diagnosed HIV-1 cases in Yunnan, China, 2015. BMC Public Health. 2019;19:1507. doi:10.1186/s12889-019-7557-8
15. Granich RM, Gilks CF, Dye C, De Cock KM, Williams BG. Universal voluntary HIV testing with immediate antiretroviral therapy as a strategy for elimination of HIV transmission, a mathematical model. Lancet. 2009;373:48–57. doi:10.1016/S0140-6736(08)61697-9
16. Zhao B, Qiu Y, Wei S. Undiagnosed HIV infections may drive HIV Transmission in the Era of “Treat All”, A deep-sampling molecular network study in Northeast China during 2016 to 2019. Virus. 2022;14(9):1895. doi:10.3390/v14091895
17. Maheu-Giroux M, Vesga JF, Diabate S, et al. Population-level impact of an accelerated HIV response plan to reach theUNAIDS 90- 90-90 target in cote d’Ivoire, insights from mathematical modeling. PLoS Med. 2017;14:e1002321. doi:10.1371/journal.pmed.1002321
18. Iwuji C, Newell ML. HIV testing, the ‘front door’ to the UNAIDS 90- 90-90 target. Public Health Action. 2017;7:79. doi:10.5588/ijtld.17.0046
19. De Cock KM, Jaffe HW, Curran JW. The evolving epidemiology of HIV/AIDS. AIDS. 2012;26(10):1205–1213. doi:10.1097/QAD.0b013e328354622a
20. Feng Y, Bu K, Li M, Zhang X, Jin S, Wang L. Meta-analysis of HIV infection incidence and risk factors among men who have sex with men in China. Chin J Epidemiol. 2015;36:752–758.
21. Hong Y, Ling S, Li Y, et al. Incidence rates of HIV-1 epidemics among 4 high risk groups in Sichuan province during 2011–2015. Chin J Epidemiol. 2017;38(12):1649–1654. doi:10.3760/cma.j.issn.0254-6450.2017.12.014
22. Gokengin D, Geretti AM, Begovac J, et al. 2014 European guideline on HIV testing. Int J STD AIDS. 2014;25(10):695–704. doi:10.1177/0956462414531244
23. Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften, Deutsche STI-Gesellschaft, Robert Koch-Institut, Bundeszentrale für gesundheitsliche Aufklärung, Landeszentrum Gesundheit, Nordrgein-Westfalen. S1 Guidline, STI/STD- Counselling, Diagnostic and Therapy; 2015. Available from: http://www.awmf.org/uploads/tx_szleitlinien/059-006l_S1_STI_STD-Beratung_2015-07.pdf.
24. Hong Y, Ye L, Ling S, et al. An analysis on incidence of HIV-1 epidemics among men who have sex with men in Sichuan Province during 2011–2015. Chin J Prev Med. 2019;53(03):327–329. doi:10.3760/cma.j.issn.0253-9624.2019.03.018
25. Yang L, Chen M, Yanling M, et al. The changing trends of HIV-1 prevalence and incidence from sentinel surveillance of five sub-populations in Yunnan, China, 2001–2010. BMC Public Health. 2015;15:376. doi:10.1186/s12889-015-1722-5
26. Bearinger LH, Sieving RE, Ferguson J, et al. Global perspectives on the sexual and reproductive health of adolescents, patterns, prevention, and potential. Lancet. 2007;369:9568. doi:10.1016/S0140-6736(07)60367-5
27. Song Y, Ji CY. Sexual intercourse and high-risk sexual behaviors among a national sample of urban adolescents in China. J Public Health. 2010;32(3):312–321. doi:10.1093/pubmed/fdp123
28. Xiao Z, Palmgreen P, Zimmerman R, et al. Adapting and applying a multiple domain model of condom use to Chinese college students. AIDS Care. 2010;22(3):332–338. doi:10.1080/09540120903193609
29. Kogan SM, Brody GH, Chen YF, et al. Risk and protective factors for unprotected intercourse among rural African American young adults. Public Health Rep. 2010;125(5):709. doi:10.1177/003335491012500513
30. Chimoyi LA, Musenge E. Spatial analysis of factors associated with HIV infection among young people in Uganda, 2011. BMC Public Health. 2014;14(1):555. doi:10.1186/1471-2458-14-555
31. Idele P, Gillespie A, Porth T, et al. Epidemiology of HIV and AIDS among adolescents, current status, inequities, and data gaps. J Acquir Immune Defic Syndr. 2014;66(Suppl2):S144–53. doi:10.1097/qai.0000000000000176
32. Adefuye AS, Abiona TC, Balogun JA, et al. HIV sexual risk behaviors and perception of risk among college students, implications for planning interventions. BMC Public Health. 2009;9:281. doi:10.1186/1471-2458-9-281
33. Nogues D, David A, Falcou Briatte R. Comparative studies of the access HCV Ab plus assay. Biochim Clin. 2013;37:S458.
34. Bearinger LH, Sieving RE, Ferguson J, et al. Global perspectives on the sexual and reproductive health of adolescents: patterns, prevention, and potential. Lancet. 2007;369(9568):1220–1231. doi:10.1016/S0140-6736(07)60367-5
35. Sichuan Provincial Bureau of Statistics. Sichuan statistical yearbook; 2021. Available from: http://tjj.sc.gov.cn/.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.