")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Dementia Care Education Targeting Job Strain and Organizational Climate Among Dementia Care Specialists in Swedish Home Care Services
Authors Fallahpour M , Borell L , Sandberg L , Boström AM
Received 3 May 2019
Accepted for publication 14 November 2019
Published 23 January 2020 Volume 2020:13 Pages 85—97
DOI https://doi.org/10.2147/JMDH.S214378
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mandana Fallahpour, 1, 2 Lena Borell, 1 Linda Sandberg, 1 Anne-Marie Boström 3–5
1Department of Neurobiology, Care Sciences and Society, Division of Occupational Therapy, Karolinska Institutet, Stockholm, Sweden; 2Department of Neurobiology, Care Sciences and Society, Division of Clinical Geriatrics, Karolinska Institutet, Stockholm, Sweden; 3Department of Neurobiology, Care Sciences and Society, Division of Nursing, Karolinska Institutet Stockholm, Solna, Sweden; 4Theme Aging, Karolinska University Hospital, Stockholm, Sweden; 5Department of Nursing, Western Norway University of Applied Science, Haugesund, Norway
Correspondence: Mandana Fallahpour
Department of Neurobiology, Care Sciences and Society, Division of Occupational Therapy, Karolinska Institutet, Fack 23200, Huddinge SE-141 83, Stockholm, Sweden
Tel +46 8 524 838 56
Fax +46 8 34 50 14
Email [email protected]
Introduction: An increasing number of older persons live at home with various limitations, such as dementia, requiring well-educated and trained home care staff to meet their complex care needs. Dementia care specialists working in home care service have reported high levels of job strain in comparison with home care staff in general.
Aim: This pilot study aims to evaluate the effects of a dementia care education model targeting self-reported job strain and organizational climate, among dementia care specialists in home care service.
Methods: A quasi-experimental, one-group pretest–posttest design was applied, with 12 months’ follow-up. Participants were dementia care specialists who worked in home care service (n=34 baseline; n=30 follow-up). The data were collected using the Strain in Dementia Care Scale and Creative Climate Questionnaires, administered pre- and post-intervention. The intervention applied an educational model based on previous research in dementia care and a person-centered approach.
Results: The educational model was implemented in the context of home care services. Of 34 participants at baseline, only 21 responded to the questionnaires, due to a drop off of 13 participants and recruitment of 9 new participants (follow-up=30). A significantly reduced perceived job strain among the participants was detected, indicating perceiving less difficulty in “Balancing competing needs” when caring for the older persons. No significant difference was found in the self-reported creative organizational climate between the two occasions.
Conclusion: The educational model could be integrated into dementia home care and it seemed to reduce job strain among dementia care specialists. Future studies are needed to evaluate the effects of the intervention using a stronger study design and a larger sample.
Keywords: creative climate questionnaire, dementia, home care services, interventions, job strain, national guidelines, strain in dementia care scale
Introduction
Dementia is among the leading causes of disability among older adults.1 There are currently 47.5 million people living with dementia worldwide. This population is expected to increase to over 121 million by 2050.2 More than half of the population of persons with dementia in Sweden, about 94,000 out of 160,000, live at home.3 This high proportion of people with dementia living at home can be seen as a result of the implementation of the ageing-in-place policy aimed at enabling older adults to remain living at home.4 Home care, as opposed to care in an institution, has been suggested as a good way of caring for persons with dementia, because home care is associated with a higher quality of life and higher levels of activity for those with moderate dementia.5 It is also an effective way of maintaining individuals’ independence.6
The Swedish welfare state has a strong and well-established tradition of providing home care services to older persons living at home. According to the Social Services Act, day-to-day life among older persons should be supported by the home care staff in cases when the older person’s needs cannot be met in other ways.7 It can be questioned whether there is a readiness in the home care services, in terms of access to relevant knowledge and education among staff, to provide adequate support in daily living to those persons with dementia, who just 10–15 years ago would have been living in a nursing home.8 Currently, there are urgent challenges to face when many older persons with severe cognitive impairments continue to live at home. A previous study has found that, in eight European countries the home care services for persons with dementia were provided by staff with a low educational level or no specific education or training at all, which could impact the quality of the provided care.9 Staff with formal education working in home care was only found to be common in Sweden and Finland. However, the formal education of nurse aides/assistants in home care is often limited to secondary school in general. Nurse aides/assistants had less than 6 months’ training and provided home care services (supporting IADL and PADL).10 Moreover, home care staff often work alone in the older person’s home, requiring them to be independent and flexible to accomplish tasks.11 In a previous study by the research group,12 dementia care specialists, referring to the nurse aides/assistants who received dementia care education by taking a web-based course focusing on the guidelines for persons with dementia13 in the context of home care service, rated job strain significantly higher than other home care staff. One possible reason for their highly rated job strain could be that dementia care specialists rather than other staff worked more extensively with persons with dementia and those with special needs.12 The dementia care specialists reported higher mean scores on job strain in the study by Sandberg et al12 compared to nursing home staff from a previous study.14 It is important to examine job strain reported by staff as previous studies have shown that well-being among staff is correlated with the quality of their work and the services provided.15 Previous research also found a positive association between organizational factors such as direct and good leadership and psychosocial work environment, in both contexts of nursing home and home care, and satisfaction among both nurse assistants and older adults.16 Research also shows that organizational and environmental support, supportive leadership, and a caring climate are associated with a lower level of job strain and stress.14 These results indicate an essential need for developing and evaluating appropriate interventions providing the educational activities which can create a positive caring and supportive climate, in order to decrease job strain and stress where the nurse assistants are able to provide high-quality care.14 A number of person-centered intervention studies in the field of dementia care have been developed. These studies have shown that person-centered interventions lead to decreased job strain and stress, as well as increased personal and professional satisfaction.17–19 However, all these studies have been performed in the context of nursing homes.
The national guidelines for providing high-quality care for persons with dementia, developed by the Swedish National Board of Health and Welfare, emphasize evidence-based care, building on a person-centered approach to the provision of care regardless of whether the older person lives at home or in a nursing home.13 Providing this type of high-quality care service therefore requires relevant education and training based on evidence. In order to enable and empower the home care staff, there is an essential need for planning appropriate educational activities consisting of the two components of (i) evidence-based care, and (ii) person-centered care. This type of intervention supports changes in ways of working, reflective approaches/attitude, and time management skills, i.e. how to prioritize and complete the tasks. A previous intervention study conducted in a nursing home by our research group reported that educational activities based on the national guidelines for dementia care were beneficial for the staff. The intervention significantly increased the person-centeredness of care and reduced stress among staff.18,20 To provide high quality care for older persons with cognitive impairments and quality of work life for staff, such as less experiences of job strain and more satisfaction, extensive efforts are needed to educate and support staff in caring for persons with dementia, in particular for home care staff who have a limited education and training in health care.
In summary, an increasing number of older persons continue to live at home with multiple limitations, such as impaired cognition. Well-educated and trained home care staff, who can meet the extensive and complex care needs of these older persons are required. However, previous research has shown that high job strain and stress among home care staff is a challenge in many countries worldwide.11,12,21,22 Increased job strain and stress among care staff are related to the quality of their work life, and these factors will also affect the quality of care for the clients. Earlier research conducted in the nursing home has reported that a perceived high level of well-being among the staff is associated with provision of high quality care.15 The findings of previous research show that staff in home care services reported a higher level of job strain compared with nursing homes.12 There is a need to develop interventions to improve the quality of work life among home care staff, by for example decreasing job strain and enhancing the organizational support, thereby increasing the quality of care for the clients. According to the body of literature, care of persons with dementia requires specific and goal-directed education, and training grounded in evidence-based knowledge about how to provide care. This need has been recognized in Sweden, and new initiatives have been launched for education and for the development of home care services for persons with dementia, building on previous studies in the context of nursing home.18,20 However, there is still a knowledge gap whether this type of intervention developed in the context of nursing home can be beneficial to implement in the specific context of home care services for persons with dementia. This pilot study is to our knowledge, one of the first studies aiming to decrease job strain among dementia care specialists in the context of home care. Therefore, the purpose of this pilot study was to evaluate the effects of a dementia care education targeting self-reported job strain and organizational climate, among dementia care specialists in home care service.
Methods
Study Design
A one-group pretest–posttest quasi-experimental design was applied in the study, with 12 months’ follow-up. This study was part of a larger research program focusing on implementing evidence-based practice in home care services. A FORTE-funded research program, implementation of evidence-based knowledge in home care, was developed for implementing the national guidelines for dementia care,13 in home care services through an action research program.18,20 The research program was designed to explore how the translation of knowledge into practice took place within an intervention, including educational activities and to evaluate the outcomes among dementia care specialists, in terms of job strain and organizational climate.
Ethical Approval
The study was approved by the Regional Ethical Review Board in Stockholm No. 2014/1014-31/4 and 2014/1894-32.
Setting and Sample
This study was carried out in a home care agency in a city in Sweden. Participants were recruited as a convenience sample from one agency, including five units in various geographical areas. The data were collected in January and February 2014 (baseline) and then 12 months’ later, in 2015 (follow-up). Four hundred employees provided home care services at the agency to about 1000 persons, among whom 20–30% were likely to have cognitive impairment and/or dementia. The home care services included services 24 hrs a day and 7 days a week. Home care staff are nurse assistants with an education in caring corresponding to secondary school level (not a university education). The services were provided by specialized staff at the agency unit – named as dementia care specialists in this study – who were about 9% of all the staff (34 individuals). The dementia care specialists received dementia care education at the agency, by taking a web-based course23 based on the guidelines for persons with dementia,13 and participating in 1 hr meetings each week, for reflection and guidance. The dementia care specialists provided services broadly to persons with dementia and particularly with persons who had increased special needs.
The inclusion criterion for participants in the study was being a dementia care specialist, providing home care services for persons with dementia. The exclusion criterion was working only night shifts. All participants received written and oral information about the study, which specified that their participation was voluntary and anonymous. If a participant decided to answer the survey questions, it was accepted as written informed consent to participate in the study. The participants who were recruited after the data collection at baseline also received written and oral information as the participants recruited at baseline.
Intervention Program
The intervention program was comprised of an interactive stepwise program of knowledge translation, knowledge generation, and knowledge dissemination based on the participatory action research model.24,25 The intervention program was built on the educational model developed in a previous intervention project in a nursing home,18,20 in which the Swedish national guidelines for care of people with dementia13 were central. The intervention program aimed at (i) translating the guidelines to evidence-based practice for the staff (ii) using the guidelines for developing, implementing, and evaluating practice, and (iii) disseminating the improvement processes and findings among the staff in the home care center.18,20 The three intervention steps have been presented in Table 1. More details about the intervention program can be found elsewhere.18,20
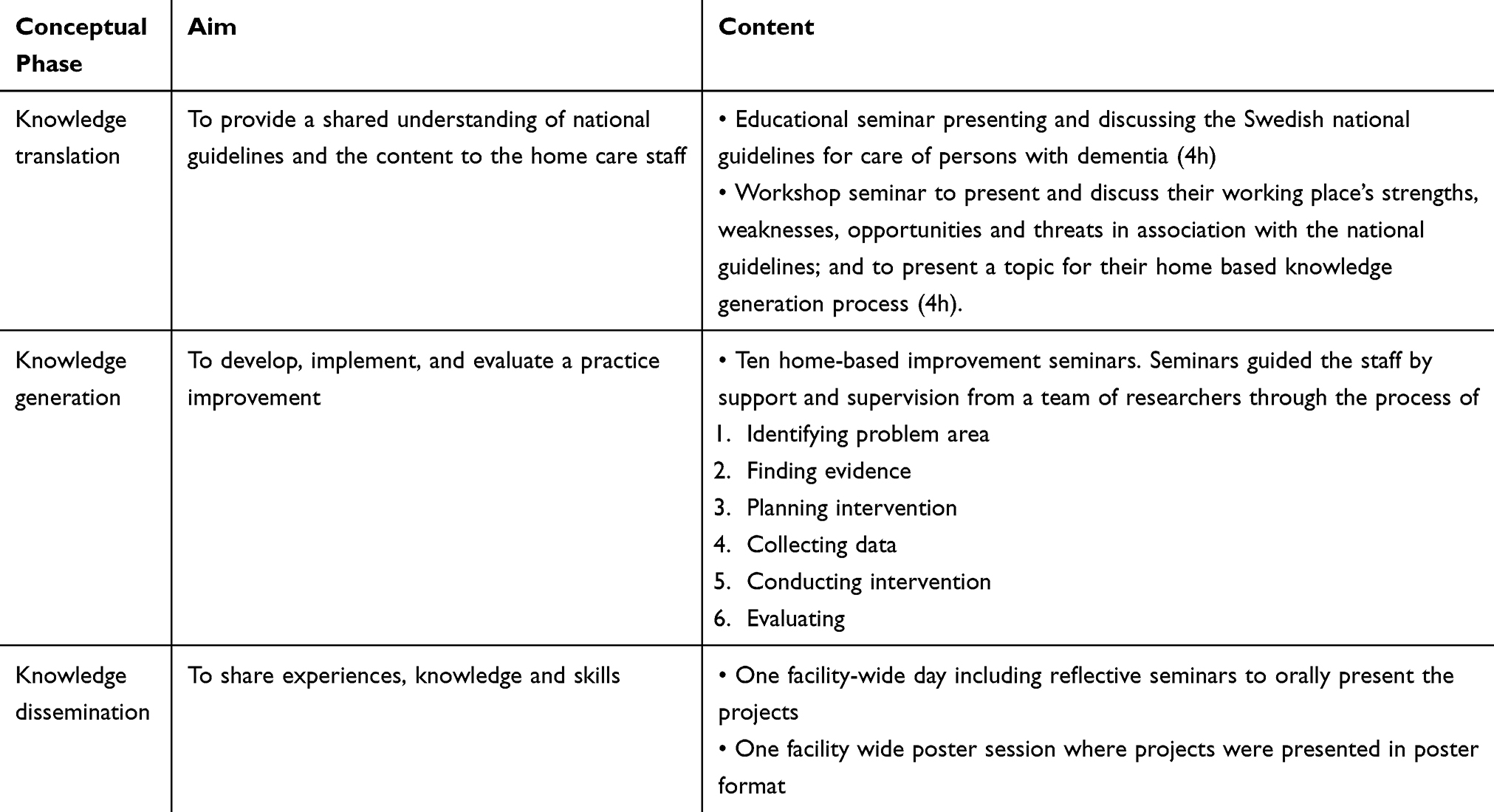 |
Table 1 Conceptual Phases, Aim, and Content of the Intervention |
The educational model consisted of the two components of (i) evidence-based care, and (ii) person-centered care. The education and training was therefore based on using theory (e.g. on dementia care) and previous research findings (e.g. the idea and practice of person-centered care). The novelty of the model is the active engagement of the front-line staff (nurse assistants) in developing new approaches for use and improvement of practice, grounded both in research and the experiences of staff. The model, therefore, applied education and practical training, grounded in the experiences of staff, as a resource for improvements, including a number of learning activities over 12 months, in 2014–2015. The staff were supported and coached by a team of researchers from Karolinska Institutet. The participants worked in five small groups (6–7 individuals in each group) which met 10 times over a year. In the groups, participants took part in discussions about challenges in practice, as well as theory and research in care of persons with dementia that could support finding improvements in practice. The learning activities included trying out new ways of caring for the older persons, in the context of home, based on recommendations from the Swedish national guidelines on dementia care13 (e.g. lectures, poster presentations of all activities related to the needs of persons with dementia). The activities included choosing a topic about one of the challenging situations that they experienced in their work with persons with dementia - and applying theory. The group activities were facilitated by faculty members from Karolinska Institutet with expertise in caring for persons with dementia, including registered nurses and occupational therapists with a PhD.
Instruments
Two instruments were used in this study in order to measure job strain and organizational climate, as described below.
Strain in Dementia Care Scale (SDCS)26 was used to assess job strain in the study. The SDCS is comprised of 27 items measuring job strain in everyday situations, as a total score based on five factors. The factors are Frustrated empathy (7 statements); Difficulty in understanding and interpreting (7 statements); Balancing competing needs (5 statements); Balancing emotional involvement (4 statements); and Lack of recognition (4 statements). Each statement is scored on two 4-point response scales for (i) the frequency of the situations that occur (from 1 = never to 4 = very often), and (ii) the amount of stress caused by the situations occurring (from 1 = none to 4 = high level of stress). Job strain is calculated by multiplying the frequency score by the stress score; all the questions are finally summarized and divided by the number of questions included, thus creating a job strain score ranging from 1 to 16. A high score indicates a high level of job strain. Previous studies found Cronbach’s alpha values for the five factors between 0.65 and 0.82,14 0.66 and 0.7727 and 0.53 and 0.90.12 Cronbach’s alpha values for the total score job strain were reported as 0.91,14 0.9227 and 0.92.12
Creative Climate Questionnaire (CCQ)28 was used to assess organizational climate dimensions. This questionnaire consists of 50 items assessing 10 dimensions of organizational climate, including (i) Challenge (members’ emotional involvement in the organization’s operations and goals), (ii) Freedom (independence of behavior demonstrated by organization members), (iii) Idea support (the ways new ideas are treated), (iv) Trust/Openness (emotional safety in relationships), (v) Dynamism/Liveliness (eventfulness of life in the organization), (vi) Playfulness/Humor (display of spontaneity and ease), (vii) Debates (occurrence of encounters and clashes between viewpoints), (viii) Conflicts (presence of personal and emotional tensions in contrast to conflicts between ideas in the organization), (ix) Risk-taking (tolerance of uncertainty in the organization), and (x) Idea time (time people can, and do use, for elaborating new ideas).
Each dimension includes five statements graded on a 4-point scale ranging from 0 = not at all to 3 = to a high degree. High scores indicate a creative organizational climate except for the dimension “Conflicts”, where unlike the other dimensions, a high score indicates a more stagnated organizational climate. In order to make the scale consistent for calculating the total CCQ score, the response option values for the conflict dimension are reversed when calculating the total score. The CCQ was used in several previous studies in the Swedish context.14,29–31 Previous studies found Cronbach’s alpha value for the dimensions ranged between 0.77 and 0.9132 and 0.55 and 0.86.12
Data Collection
The study comprised three phases, including (i) baseline assessment. (ii) intervention program, and (iii) follow-up assessment. Data were collected at the baseline before the intervention (2014) and at follow-up after the intervention (2015). The intervention program was conducted in the 12 months between 2014 and 2015. The data were collected using the questionnaires of SDCS and CCQ. Before the intervention program started, 34 dementia care specialists at the agency were invited to participate at the meeting. They were informed orally and in writing about the study. The data collection was performed during an introductory meeting. The questionnaire also included some baseline/demographic questions, such as age, sex, education, Swedish as their first language, years of employment, time spent working with people with dementia and working hours which the participants answered in addition to SDCS and CCQ. After 1 year of the intervention at the end of the educational model, the participants were invited to answer the same questionnaire used at the baseline data collection.
Data Analysis
As the first step in the data analysis, missing values in the questionnaires of SDCS, and CCQ were addressed. In a case where ≤50% of the values for each factor/dimension were missing, a mean was calculated based on the numbers for the reported items. Thereafter, the missing value was replaced by the calculated mean.33 Between 0 and 5 respondents completed less than 50% of the response scale for the SDCS factors and CCQ dimensions.
Descriptive analyses were applied in order to describe frequencies and distributions. Data from the SDCS and CCQ were largely normally distributed motivating the use of parametric statistics for analyzing the data. In line with the previous research using the same instruments,12,14 this study applied the parametric statistics to analyze the data to be able to compare the findings with previous literature. The paired samples t-test was used to explore baseline and follow-up differences on mean scores for SDCS and CCQ. The Wilcoxon rank test was also applied as an additional non-parametric analysis to compare the changes between pre- and post-intervention scores in the sample of completers, in order to compare the findings from the parametric analyses. The significance level was set at p-value ≤0.05. The Statistical Package of Social Sciences (SPSS) version 22.034 was used to analyze the data in the study.
Results
The Sample of the Dementia Care Specialists During the Study
The study included 34 participants at baseline. At follow-up after 12 months’ of intervention, the sample consisted of 30 participants. Out of 34 individuals at the baseline, only 21 participants took part at the follow-up assessment, because 13 participants finished their jobs at the agency before the study period was completed. In the process of implementing the intervention program over 12 months, nine new individuals started to work at the agency to fill these vacancies. For this reason, they were not assessed at the baseline. The data analysis therefore included 21 participants (the completers) who took part in the three phases of the study (baseline assessment, intervention program and follow-up assessment) (See Figure 1). The demographic characteristics of the participants are given in Table 2.
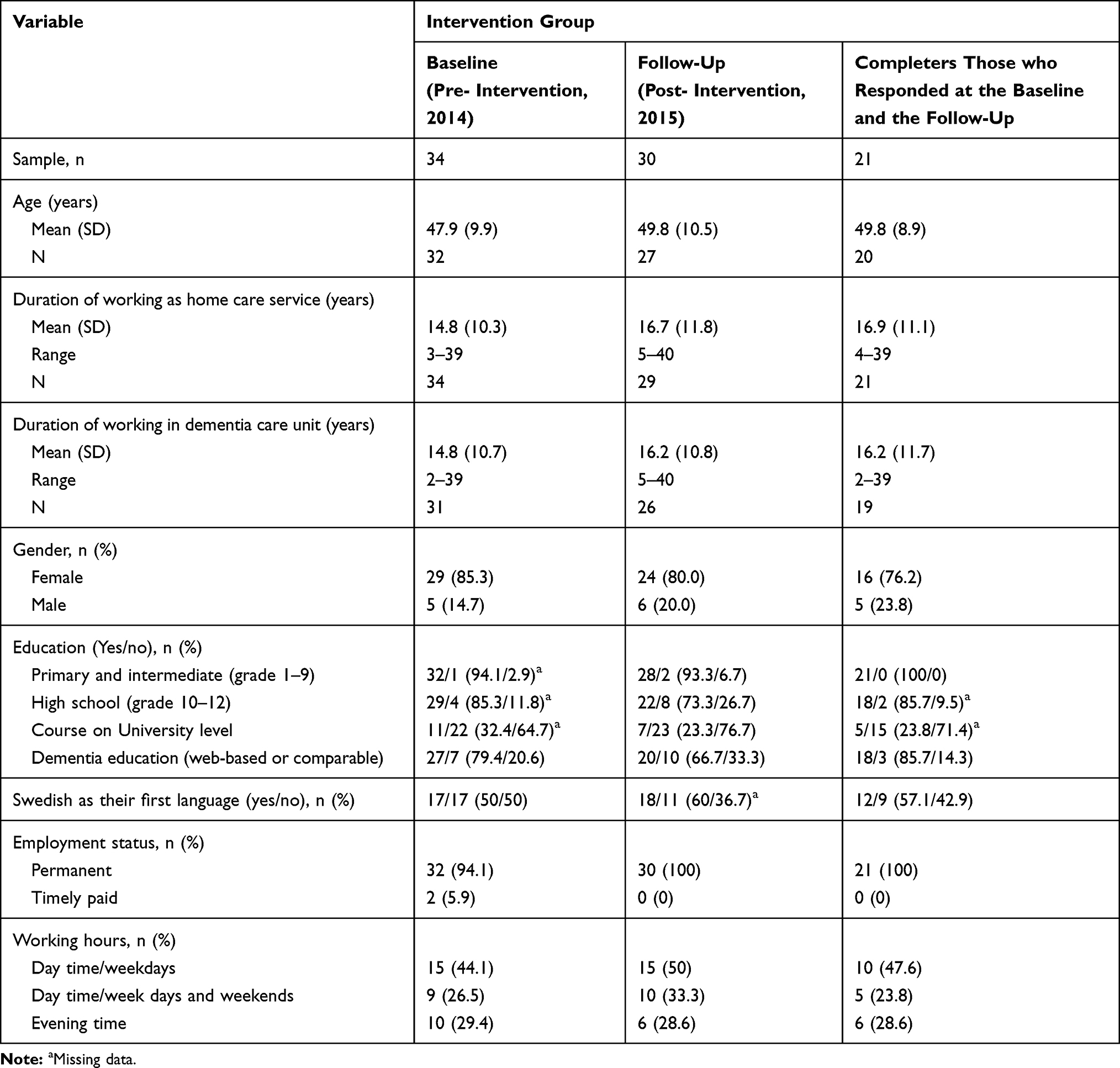 |
Table 2 Demographic Characteristics of the Dementia Care Specialists at Baseline (n=34), Follow-Up (n=30) and Completers (n=21) |
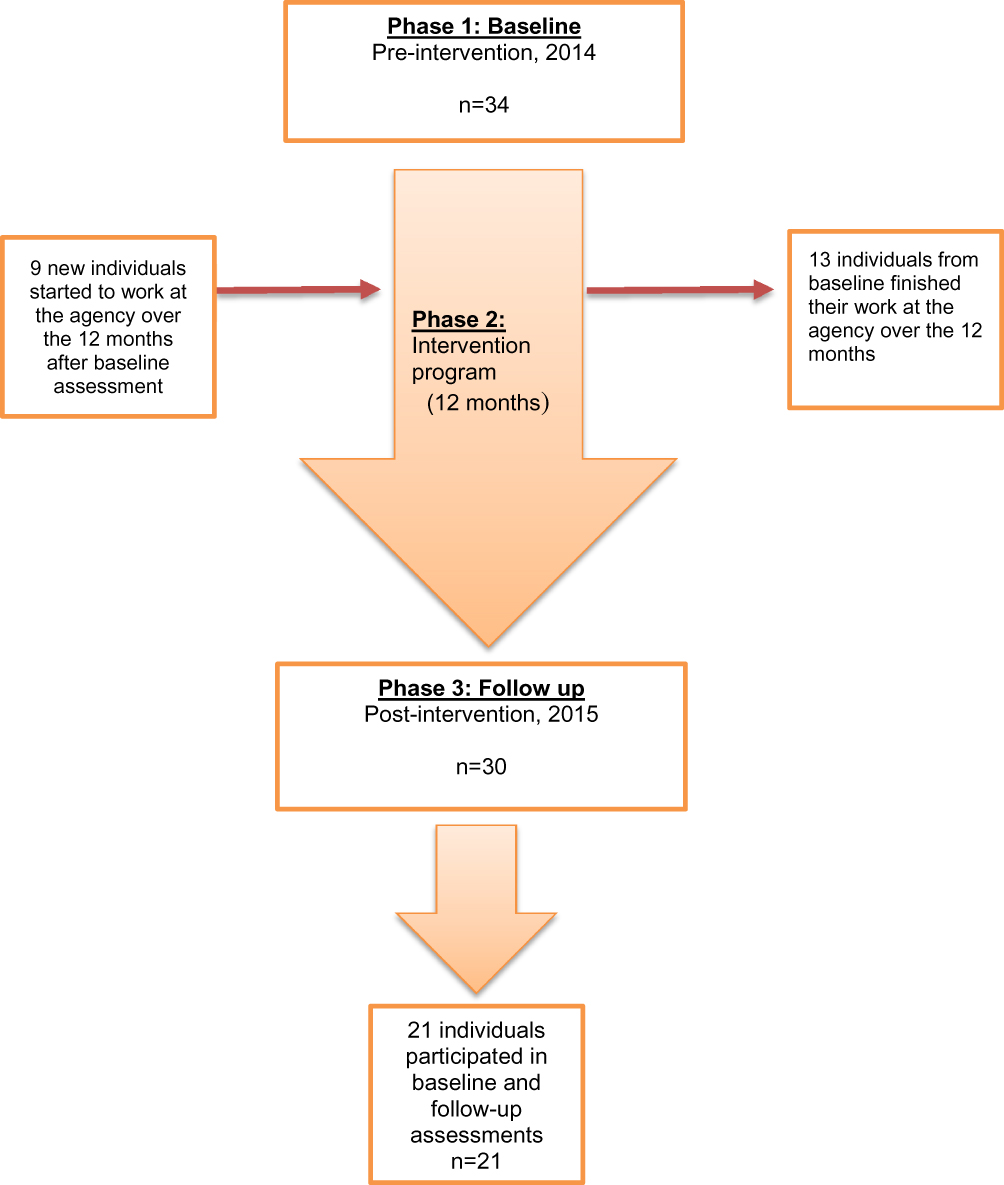 |
Figure 1 Study sample over the study phases. |
Job Strain and Organizational Climate Among Dementia Care Specialists at Baseline and Follow-Up
The mean scores for SDCS and CCQ at baseline (pre-intervention, n=34) and follow-up (post-intervention, n=30) are presented in Table 3. At baseline, the mean value for the SDCS total score was 5.70. The highest mean scores for SDCS factors at the baseline describing the highest job strain among the sample were reported in SDCS Factor 3 Balancing competing needs (M=6.85), Factor 5 Lack of recognition (M=6.59), and Factor 1 Frustrated empathy (M=6.15). At the follow-up, the mean value for the SDCS total score was 4.95. The SDCS Factors with the highest mean values at follow-up were Factor 5 Lack of recognition (M=5.90), Factor 3 Balancing competing needs (M=5.46), and Factor 1 Frustrated empathy (M=5.39).
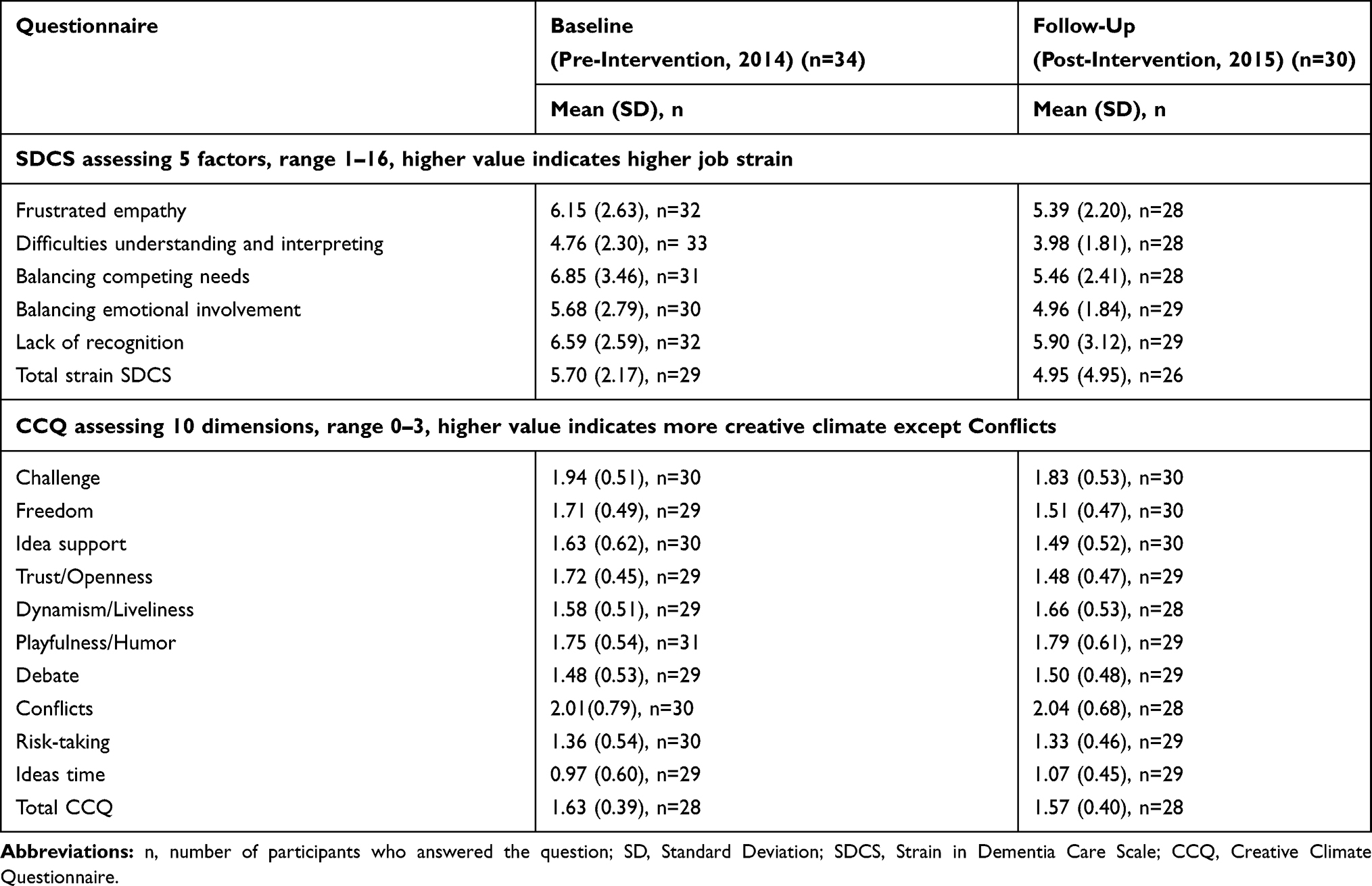 |
Table 3 Presentation of the Baseline and Follow-Up Scores Among the Samples at Baseline (n=34) and Follow-Up (n=30) on Perceived Job Strain and Creative Organizational Climate |
At baseline, the mean value for the CCQ total score was 1.63. The three highest mean values for CCQ dimensions at baseline, indicating more creative organizational climate, were reported by the sample for Challenge (M=1.94), Playfulness/Humor (M=1.75) and Trust/Openness (M=1.72). At follow-up, the mean value for the CCQ total score was 1.57. The CCQ dimensions with the highest mean values were Challenge (M=1.83), Playfulness/Humor (M=1.79) and Dynamism/Liveliness (M=1.66).
Changes in Job Strain and Organizational Climate Reported by Completers
Table 4 presents the findings among the 21 participants (the completers) who took part in the intervention and responded to the questionnaires on both occasions. As it is presented in Table 4, there was a trend that the completers rated lower mean values on the SDCS total score and the five SDCS factors at the follow-up, compared with the baseline. However, the change was only statistically significant for the SDCS Factor 3, Balancing competing needs (p = 0.033), indicating less job strain in balancing needs (See Table 4).
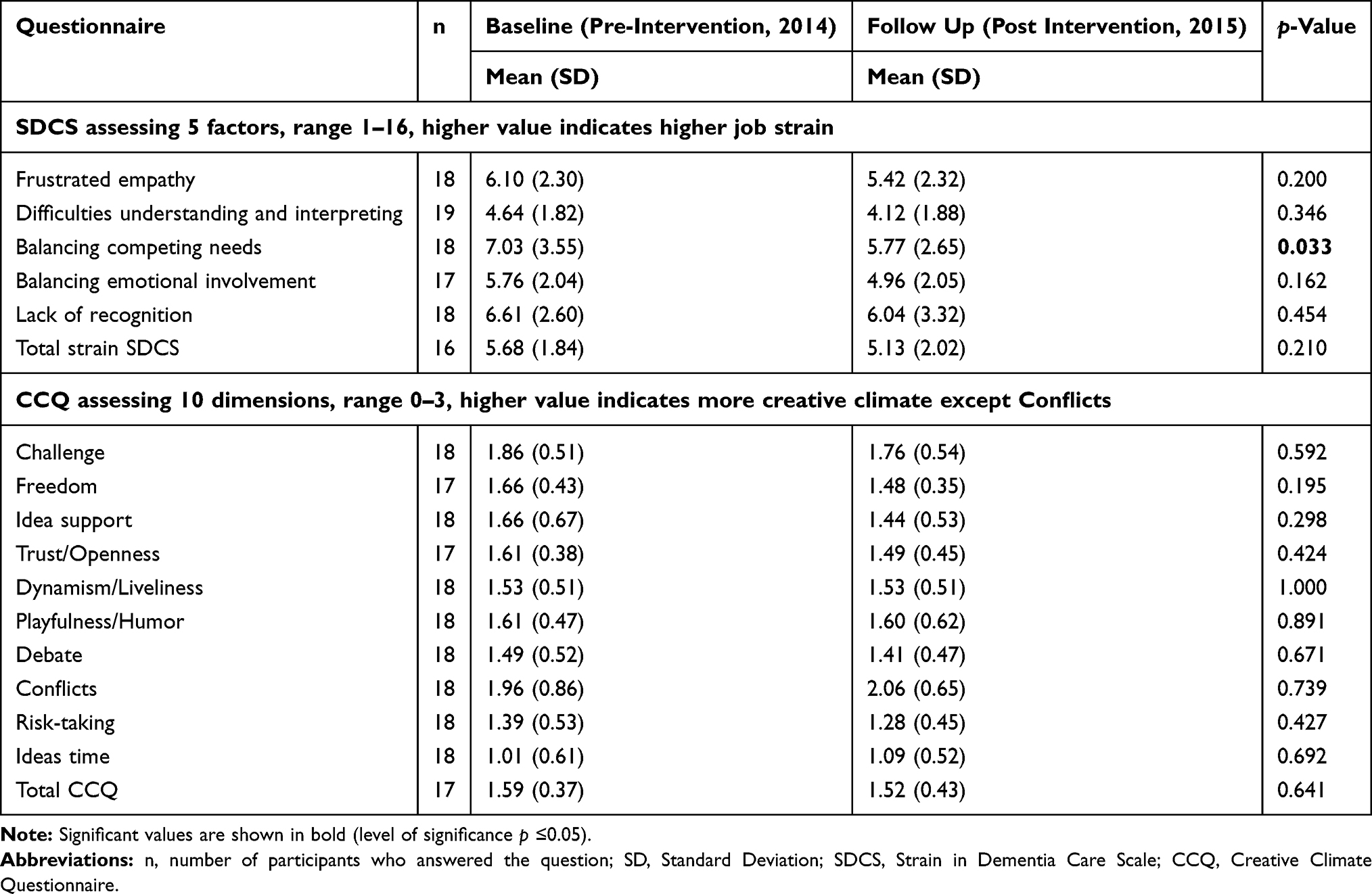 |
Table 4 Presentation of the Baseline and Follow-Up Scores Among the Completers (n=21) on Perceived Job Strain and Creative Organizational Climate |
The five items included in SDCS Factor 3 were analyzed further. Two significant differences between the baseline and the follow-up assessments were identified in the two items: “I have to balance the needs of the older person against the needs of his or her family” (p = 0.038) and, “I have to balance the needs of the older person against the needs of other older persons” (p = 0.029) (see Table 5).
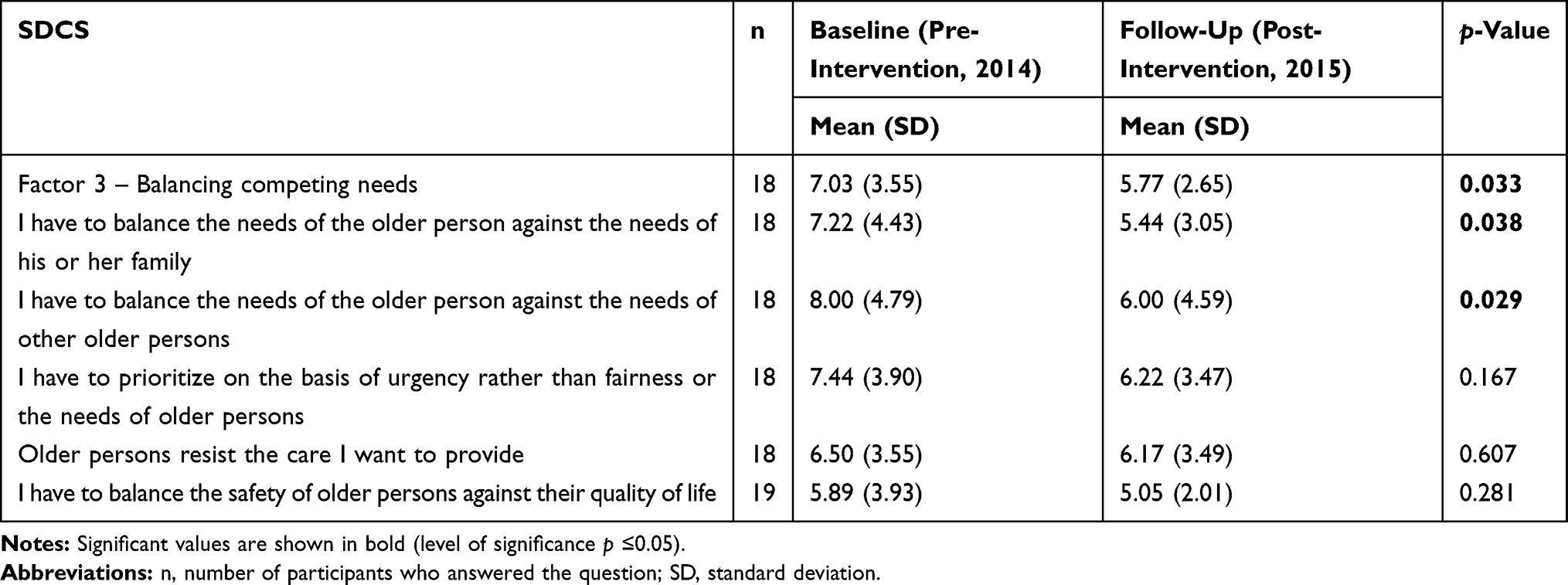 |
Table 5 Presentation of the Baseline and Follow-Up Scores Among the Completers (n=21) on Factor 3 SDCS, “Balancing Competing Needs” |
The trend for the completers’ rating of the CCQ between baseline and follow-up indicated a more stagnated organizational climate. But no significant differences were found in the 10 CCQ dimensions and the total CCQ score between the baseline and follow-up (See Table 4).
The findings from the Wilcoxon rank test, applied as additional non-parametric analyses in the study, were in line with paired samples t-test and did not reveal any different results in the changes between the baseline and follow-up assessments regarding the SDCS scores or the CCQ scores.
Discussion
This pilot study aimed to evaluate the effects of a dementia care education intervention on job strain and organizational climate among dementia care specialists in home care service. Significantly lower scores on job strain were reported by the dementia care specialists at follow-up, regarding Balancing competing needs, thus indicating less job strain in balancing needs of the older persons. Among the five items of Factor 3, significant differences were found in the mean scores for the items: “I have to balance the needs of the older person against the needs of his or her family” and, “I have to balance the needs of the older person against the needs of other older persons”, between the baseline and follow-up assessments. Despite no statistically significant changes in the other four SDCS factors and the SDCS total score, the results show a positive trend showing less job strain when comparing the mean scores of SDCS at baseline and follow-up, among the completers. This result suggests that the intervention may have influenced this outcome. These results are supported by previous research18 which showed that this intervention program grounded in implementing the national guidelines for person-centered care of persons with dementia, applied in the context of residential care, significantly decreased the reported job strain and stress among the residential care staff.
The intervention program in this study seems to provide a useful educational model grounded in person-centered care and applying evidence for developing home care services for older adults with dementia. Accordingly, the educational model in this study may be discussed as having been effective in meeting staffs needs to act on the challenging situations. The significant changes in the SDCS Factor 3 in this study indicate that the educational model may have provided more possibility for the dementia care specialists to manage the competing needs of the persons with dementia. One possible explanation for this finding is that the educational model, applying the person-centered approach13 among the specialized staff, was effective to support staff to identify older persons’ needs, and also to balance these needs against the needs of their families or other older adults. It is also possible that the participants got the opportunity through the intervention program to develop their time management skills to prioritize and complete their tasks in everyday work life, which is in line with previous research in the context of nursing homes.35 The findings can also be understood in light of the stress theory of demand and control.36 It might be assumed that the dementia care specialists experienced high demands in their job when providing care for persons with dementia using a person-centered approach. They potentially also experienced low control over their working situations with the older adults, due to working by themselves without access to, and support from, colleagues when they provide care in the person’s home. The combination of the high demands and low control will, according to the theory of demand and control, contribute to an experience of high levels of stress. The knowledge and practice from the educational activities have supported the dementia care specialists to identify strategies to handle and manage situations to balance the needs from the older persons and thereby experience more control over the situation and lower levels of job strain.
The results of this pilot study can also be discussed with a view to the PARiHS (Promoting Action on Research Implementation in Health Services) framework.37 According to this conceptual framework, successful implementation of research in practice is a function of the interplay between three core elements: (i) the level and nature of evidence, (ii) the context of the environment in which the research is to be performed, and (iii) the method or way in which the process is facilitated. This conceptual framework stresses the equal importance of all three elements in having a successful implementation. The intervention model in this study was an educational model with a number of learning activities and discussions in small groups (6–7 individuals per group) around special themes, on a regular basis. The educational model in this study could be implemented and the participants actively took part in the planned educational activities. This educational model was tested and evaluated in a previous research study with the aim to implement person-centered care for persons with dementia within the context of nursing homes, and in this context showed other findings.18 Even if the educational model was the same as in the present study, the outcome measures and the applied instruments to assess the primary endpoints (person-centeredness of care and the environment) and the secondary endpoints (staff strain and stress of conscience) were not the same as in the present study. The previous study found that applying the educational intervention resulted in significantly higher scores on person-centeredness of care at follow-up, and the facility was rated as being significantly more hospitable at follow-up. The findings also showed a significant reduction of stress of conscience reported by staff at follow-up, suggesting that staff to a larger extent, could provide the care they wanted after the intervention. This finding is also in line with the significantly lower scores reported in SDCS Factor 3 by the participants, after the intervention in the present study.
However, the effects on job strain in the present study compared with the study by Edvardsson and colleagues (2014) could be discussed from different angles.16 Firstly, one possible reason for the non-significant findings in this study might be the different context used in the present study. The previous study18 was conducted in the context of a nursing home, which differs from a home care setting in working conditions for staff regarding opportunities to discuss and learn from each other in their daily work. Compared with staff working in residential care,14 home care staff reported higher scores on job strain, indicating a different working context for the care staff. Previous research studies have shown that home care staff work alone,11 requiring them to rely on their own competence.21,38 Furthermore, home care staff has reported that they experience pressure and violence21,39 which was significantly associated with experiencing stress, depression, sleep problems and burnout.21
Secondly, the previous study18 included all staff working at the nursing home, such as the nurse aides and health professionals (registered nurses, physiotherapists, occupational therapists) in the intervention. However, in the present study, only 34 out of 400 staff members were invited to participate in the intervention, which is less than 10% of the staff members at the home care agency. One might assume that in order to modify outcomes, such as the organizational climate in a workplace, the educational intervention needs to embrace the whole staff group to make a difference. In particular, the managers and leaders need to be involved to support change and implementation of new knowledge and routines according to the PARIHS framework.37 On the other hand, the empirical literature focusing on exploring the effectiveness of the educational programs stresses that changing practice requires changing mental models and creating new ways of thinking.40 According to the spiral model for the process of change, practice gives knowledge that shapes attitude and leads to changed practice.41 Altogether, the process of change through implementation takes time, especially when the outcome variable is individuals’ attitudes, values and beliefs (e.g. CCQ dimensions).
Despite the low number of participants, the findings showed a positive result, as lower levels of job strain reported by the home care staff (Factor 3 SDCS Balancing competing needs) indicated that the intervention influenced the ability of the staff to balance the prioritization of the need of the older person, against the needs of their family. Additionally, it underlined the ability of the staff to prioritize and balance the needs of the older person against the needs of other older persons. One interpretation of this result might be that it is plausible that the intervention provided the required support to the dementia care specialist, in order to balance the needs of the older persons in their work situation.
Limitations
This study was a pilot study to evaluate effects of a dementia care education targeting self-reported job strain and organizational climate, among dementia care specialists in home care services. The quasi-experimental, one-group pretest–posttest design of this study enforces some limitations to be considered when interpreting the results. A one-group sample could increase the possibility of bias from various variables that were not controlled for, which may have impacted the internal validity of the study. Another limitation of the study design was the risk of an under-powered study from the limited sample size and there was a more extensive turnover among the participants than was expected. It was not possible to include all the 34 participants from the baseline in the data analyses since only 21 participants participated in both data collection points. Thirteen individuals left the study over the 12 months of intervention and 9 individuals were newly recruited over the intervention phase, with no report of their assessment at baseline. Excluding these 13 individuals at the baseline, which accounted for 38% of the sample at the baseline, as well as the low number of the participants who completed the study, might have influenced the results. The findings of the power calculation and effect size42 point in the same direction. The power calculation considering a sample of 34 at baseline produced an effect size of 0.5 for the three scales, assuming 81% power at a 5% level of significance. However, since 21 out of 34 individuals took part in the follow-up evaluation, the power was calculated for 21 participants, which produced an effect size of 0.5 in the two scales, assuming 59% power at a 5% level of significance. The power could have increased to 90% if a sample of 44 participants had been recruited pre- and post-intervention.
The findings can also be discussed in relation to the outcome measures used in this study. It was feasible for the participants to use the instruments applied in the study. Some participants did not respond to all items, but the number was not more extensive than in previous studies using the SDCS and CCQ.14,26 Future studies are needed to examine the educational model by applying instruments assessing person-centered care in a home care context. It is, however, important to stress that there is a lack of valid and reliable instruments that are available in the context of home care services which also requires more future research. Despite the present limitations, it is important to stress that this study was only a pilot study, even if it was the first study to develop an intervention program based on national Swedish guidelines,13 aiming to decrease the job strain among home care staff for persons with dementia. One might assume that the findings should be interpreted cautiously. Future studies are needed to further development of the intervention program applying a randomized controlled trial (RCT) design, with a larger sample of intervention and control groups, preferably from several agencies among dementia care specialists in the home care context.
Conclusion
The findings of this study showed that the educational model could be integrated into dementia home care services. The intervention seems to be able to reduce the perceived job strain among the dementia care specialists indicating less job strain in Balancing competing needs. Because home care staff, and particularly dementia care specialists, rate high levels of job strain, it is important that interventions aiming to reduce job strain tailored to these staff groups are developed and evaluated. Future studies are needed to evaluate the intervention in a larger sample, applying RCT designs, and also to explore the effects among older persons with dementia who are supported by the dementia care specialists.
Acknowledgments
The study was funded by the FORTE (The Swedish Research Council for Health, Working Life and Welfare), 2014-04674; Implementation of evidence-based knowledge in home care (PI: Lena Borell). We are grateful to the participants for the valuable participation in this study as well as the home care services agency for providing us with the support we needed.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Colantuoni E, Surplus G, Hackman A, Arrighi HM, Brookmeyer R. Web-based application to project the burden of Alzheimer’s disease. Alzheimer’s Dementia. 2010;6(5):425–428. doi:10.1016/j.jalz.2010.01.014
2. Alzheimer’s Disease International. World Alzheimer Report 2016: The Global Impact of Dementia Online 2016. Available from: https://www.alz.co.uk/research/world-report-2015.
3. Wimo A, Jönsson L, Fratiglioni L, Sandman P, Gustavsson A, Sköldunger A. Demenssjukdommarnas Samhällskostnader I Sverige 2012 [Societal Costs for Dementia in Sweden in 2012]. Stockholm: National Board of Health and Welfare; 2014. Available from: http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/19444/2014-6-3.pdf.
4. World Health Organization. World report on ageing and health; 2015. Available from: http://www.who.int/ageing/events/world-report-2015-launch/en/.
5. Olsen C, Pedersen I, Bergland A, et al. Differences in quality of life in home-dwelling persons and nursing home residents with dementia - a cross-sectional study. BMC Geriatr. 2016;16:137. doi:10.1186/s12877-016-0312-4
6. Genet N, Boerma WG, Kringos DS, et al. Home care in Europe: a systematic literature review. BMC Health Serv Res. 2011;11:207. doi:10.1186/1472-6963-11-207
7. Socialtjänstlagen [Social Services Act] SFS 2001:453. Stockholm: Socialdepartmentet. Swedish.
8. Ulmanen P, Szebehely M. From the state to the family or to the market? Consequences of reduced residential eldercare in Sweden. Int J Soc Welfare. 2015;24:81–92. doi:10.1111/ijsw.12108
9. Bokberg C, Ahlstrom G, Leino-Kilpi H, et al. Care and service at home for persons with dementia in Europe. J Nurs Scholarsh. 2015;47(5):407–416. doi:10.1111/jnu.12158
10. Hallberg IR, Cabrera E, Jolley D, et al. Professional care providers in dementia care in eight European countries; their training and involvement in early dementia stage and in home care. Dementia (London). 2016;15(5):931–957. doi:10.1177/1471301214548520
11. Lundgren D, Ernsth-Bravell M, Kareholt I. Leadership and the psychosocial work environment in old age care. Int J Older People Nurs. 2016;11(1):44–54. doi:10.1111/opn.12088
12. Sandberg L, Borell L, Edvardsson D, Rosenberg L, Bostrom AM. Job strain: a cross-sectional survey of dementia care specialists and other staff in Swedish home care services. J Multidiscip Healthc. 2018;11:255–266. doi:10.2147/JMDH.S155467
13. The Swedish National Board of Health and Welfare. Nationella Riktlinjer För Vård Och Omsorg Vid Demenssjukdom 2010 [National Guidelines for Care and Nursing in Dementia 2010]. Stockholm: National Board of Health and Welfare; 2010. Available from: http://www.demenscentrum.se/globalassets/utbildning_pdf/nationella_riktlinjer_vard_omsorg_vid_demens.pdf.
14. Orrung Wallin A, Jakobsson U, Edberg AK. Job strain and stress of conscience among nurse assistants working in residential care. J Nurs Manag. 2015;23(3):368–379. doi:10.1111/jonm.12145
15. Edvardsson D, Sandman PO, Nay R, Karlsson S. Associations between the working characteristics of nursing staff and the prevalence of behavioral symptoms in people with dementia in residential care. Int Psychogeriatr. 2008;20(4):764–776. doi:10.1017/S1041610208006716
16. Lundgren D, Ernsth Bravell M, Borjesson U, Kareholt I. The impact of leadership and psychosocial work environment on recipient satisfaction in nursing homes and home care. Gerontol Geriatr Med. 2019;5:2333721419841245.
17. Jeon YH, Luscombe G, Chenoweth L, et al. Staff outcomes from the caring for aged dementia care resident study (CADRES): a cluster randomised trial. Int J Nurs Stud. 2012;49(5):508–518. doi:10.1016/j.ijnurstu.2011.10.020
18. Edvardsson D, Sandman PO, Borell L. Implementing national guidelines for person-centered care of people with dementia in residential aged care: effects on perceived person-centeredness, staff strain, and stress of conscience. Int Psychogeriatr. 2014;26(7):1171–1179. doi:10.1017/S1041610214000258
19. McCormack B, Dewing J, Breslin L, et al. Developing person-centred practice: nursing outcomes arising from changes to the care environment in residential settings for older people. Int J Older People Nurs. 2010;5(2):93–107. doi:10.1111/j.1748-3743.2010.00216.x
20. Vikstrom S, Sandman PO, Stenwall E, et al. A model for implementing guidelines for person-centered care in a nursing home setting. Int Psychogeriatr. 2015;27(1):49–59. doi:10.1017/S1041610214001598
21. Hanson GC, Perrin NA, Moss H, Laharnar N, Glass N. Workplace violence against homecare workers and its relationship with workers health outcomes: a cross-sectional study. BMC Public Health. 2015;15:11. doi:10.1186/s12889-014-1340-7
22. Edberg AK, Bird M, Richards DA, Woods R, Keeley P, Davis-Quarrell V. Strain in nursing care of people with dementia: nurses’ experience in Australia, Sweden and United Kingdom. Aging Ment Health. 2008;12(2):236–243. doi:10.1080/13607860701616374
23. The Swedish Dementia Centre. Avgiftsfria webutbildningar. Available from: http://www.demenscentrum.se/Utbildning/Webbutbildningar1/.
24. Freire P. Pedagogy of the Oppressed. New York: Herder and Herder; 1993.
25. Taylor RR, Braveman B, Hammel J. Developing and evaluating community-based services through participatory action research: two case examples. Am J Occup Ther. 2004;58(1):73–82. doi:10.5014/ajot.58.1.73
26. Edberg AK, Anderson K, Orrung Wallin A, Bird M. The development of the strain in dementia care scale (SDCS). Int Psychogeriatr. 2015;27(12):2017–2030. doi:10.1017/S1041610215000952
27. Orrung Wallin A, Edberg AK, Beck I, Jakobsson U. Psychometric properties concerning four instruments measuring job satisfaction, strain, and stress of conscience in a residential care context. Arch Gerontol Geriatr. 2013;57(2):162–171. doi:10.1016/j.archger.2013.04.001
28. Ekvall G. Organizational climate for creativity and innovation. Eur J Work Organ Psychol. 1996;5(1):105–123. doi:10.1080/13594329608414845
29. Orrung Wallin A, Jakobsson U, Edberg AK. Job satisfaction and associated variables among nurse assistants working in residential care. Int Psychogeriatr. 2012;24(12):1904–1918. doi:10.1017/S1041610212001159
30. Carlfjord S, Festin K. Association between organizational climate and perceptions and use of an innovation in Swedish primary health care: a prospective study of an implementation. BMC Health Serv Res. 2015;15:364. doi:10.1186/s12913-015-1038-2
31. Soderlund M, Norberg A, Hansebo G. Validation method training: nurses’ experiences and ratings of work climate. Int J Older People Nurs. 2014;9(1):79–89. doi:10.1111/opn.2014.9.issue-1
32. Bostrom AM, Wallin L, Nordstrom G. Evidence-based practice and determinants of research use in elderly care in Sweden. J Eval Clin Pract. 2007;13(4):665–673.
33. Tabachnick BG, Fidell LS, editors. Using Multivariate Statistics.
34. IBM Corp. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp; 2013.
35. Kagwa SA, Bostrom AM, Ickert C, Slaughter SE. Optimising mobility through the sit-to-stand activity for older people living in residential care facilities: a qualitative interview study of healthcare aide experiences. Int J Older People Nurs. 2018;13:e12169. doi:10.1111/opn.12169
36. Karasek R, Theorell T. Healthy Work. Stress, Productivity, and the Construction of Working Life. New York: Basic books; 1990.
37. Kitson A, Harvey G, McCormack B, Kitson A, Harvey G, McCormack B. Enabling the implementation of evidence based practice: a conceptual framework. Qual Health Care. 1998;7(3):149–158. doi:10.1136/qshc.7.3.149
38. Gleason HP, Boerner K, Barooah A. Supporting home health aides through a client’s death: the role of supervisors and coworkers. Geriatr Nurs. 2016;37(4):278–283. doi:10.1016/j.gerinurse.2016.04.001
39. Quinn MM, Markkanen PK, Galligan CJ, et al. Occupational health of home care aides: results of the safe home care survey. Occup Environ Med. 2016;73(4):237–245. doi:10.1136/oemed-2015-103031
40. Dall’Alba G. Understanding professional practice: investigations before and after an an educational programme. Stud Higher Educ. 2004;29:679–692. doi:10.1080/0307507042000287195
41. Diwan VK, Sachs L, Wahlstrom R. Practice-knowledge-attitudes-practice: an explorative study of information in primary care. Soc Sci Med. 1997;44(8):1221–1228. doi:10.1016/S0277-9536(96)00310-3
42. Cohen J. Statistical Power Analysis for the Behavioural Sciences. New Jersy: Lawrence Erlbaum Associates Inc.; 1988.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.