")
Back to Journals » Cancer Management and Research » Volume 12
Δ133p53/FLp53 Predicts Poor Clinical Outcome in Esophageal Squamous Cell Carcinoma
Authors Tu Q , Gong H , Yuan C, Liu G, Huang J, Li Z, Luo J
Received 19 May 2020
Accepted for publication 25 July 2020
Published 18 August 2020 Volume 2020:12 Pages 7405—7417
DOI https://doi.org/10.2147/CMAR.S263559
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Yong Teng
Qimin Tu,1,2,* Hongjian Gong,3,4,* Chunhui Yuan,3 Gao Liu,5 Jinqi Huang,1 Zhichao Li,4 Jianfei Luo2
1Department of Cardio-Thoracic Surgery, Central Hospital of Enshi Autonomous Prefecture, Enshi Clinical College of Wuhan University, Enshi, Hubei, People’s Republic of China; 2Department of Gastrointestinal Surgery, Renmin Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China; 3Clinical Research Center, Wuhan Medical and Health Center for Women and Children, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 4Department of Rheumatism Immunology, Wuhan Medical and Health Center for Women and Children, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 5Department of Gastrointestinal Surgery, Central Hospital of Enshi Autonomous Prefecture, Enshi Clinical College of Wuhan University, Enshi, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhichao Li
Department of Rheumatism Immunology, Wuhan Medical and Health Center for Women and Children, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China
Tel +86-27-82433423
Email [email protected]
Jianfei Luo
Department of Gastrointestinal Surgery, Renmin Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China
Tel +86-27-88041911
Email [email protected]
Background: p53 isoform Δ 133p53 is directly transactivated by p53 and antagonizes p53 activities in cancer progression. However, its correlation with prognosis and cancer recurrence in esophageal squamous cell carcinoma (ESCC) is still unclear.
Patients and Methods: Expression of Δ 133p53 and Δ 133p53/full-length p53 (FLp53) in tissues and serums of 180 ESCC patients was evaluated using qRT-PCR. Patients were divided into high- and low-expression groups according to the cutoff value determined by X-tile 3.6.1 software. Survival analysis was performed by the Kaplan–Meier method. Univariate and multivariate Cox survival analyses were applied to assess the hazard ratios (HRs).
Results: Tissue Δ 133p53 expression and Δ 133p53/FLp53 ratio were significantly increased in ESCC tissue compared with adjacent normal tissue. Pre-operative Δ 133p53 expression and Δ 133p53/FLp53 ratio in tissue or serum samples were positively associated with TNM stage and post-operative recurrence. Kaplan–Meier curve and multivariate cox regression analyses revealed that the tissue and serum Δ 133p53/FLp53 ratios (cutoff value: 2.9160) were independent prognostic factors for overall survival (OS) and progression-free survival (PFS) in ESCC patients and showed no statistical difference in receiver-operating characteristic curve (ROC) analysis, while serum Δ 133p53 showed no significant prognostic value. More importantly, the serum Δ 133p53/FLp53 ratio in ESCC patients was significantly decreased within 72 h post tumor resection and patients with a consistently high serum Δ 133p53/FLp53 ratio (≥ 2.9160) had higher recurrence rates than those with consistently low ratio values. In addition, dynamic detection in each follow-up timepoint showed that serum Δ 133p53/FLp53 ratios were higher than 2.9160 upon recurrence, and they even increased prior to radiologic progression.
Conclusion: The serum Δ 133p53/FLp53 ratio can be a novel predictor for survival outcome and may serve as a real-time parameter for monitoring recurrence in ESCC patients after surgery.
Keywords: esophageal squamous cell carcinoma, p53, Δ 133p53, prognosis, recurrence
Introduction
Esophageal cancer is the fourth leading cause of cancer-related death in both men and women in China,1 and approximately 90% of Chinese patients with esophageal cancer were diagnosed with esophageal squamous cell carcinoma (ESCC).2 Recently, multiple approaches have been developed to improve the outcome of ESCC, including esophagectomy combined with radiotherapy or chemotherapy. However, the 5-year overall survival rate is still inferior and ranges from 15 to 25% in all patients.3 This is thought to be due to a combination of late stage of diagnosis, rapid development of ESCC and lack of effective therapies.4 Moreover, molecular biomarkers capable of predicting recurrence and metastasis, which frequently developed in ESCC patients diagnosed with localized disease, have not yet been developed and thus treatment decisions regarding systemic therapy have been delayed.
Events involved in driving cancer evolution affect tumor aggressiveness, response to treatment and patient prognosis.5 To identify prognostic biomarkers, several recent large-scale genomic studies have characterized hundreds of somatic mutations, copy number alterations (CNAs) and structural variants (SVs) in ESCC.4,6-10 Mutations in SLC39A6,4 EP300 (10%),9,10 and FAM135B (6.8%)7 as well as amplification or overexpression of EGFR5 were associated with a poor prognosis of ESCC. Moreover, many genes involved in cell cycle regulation, DNA repair and apoptosis were mutated or amplified in 99% of cases, including TP53 (93%), CCND1 (33%), CDK4/CDK6 (23.6%), CDKN2A (20%), NFE2L2 (10%) and RB1 (9%).7,9 As the highest frequency of mutated gene, mutation of TP53 in the DNA binding domain has been regarded as the main cause for p53 inactivation and proposed as a key factor in driving ESCC progression.9 Two compounds (ie, APR-246, COTI-2) that can reactivate missense-mutant p53 protein have been tested in clinical Phase I/II trials.11 However, a growing body of evidence has suggested that abundance of p53 isoforms in cancer tissues, due to alternative splicing or usage of alternative promoters, also modulates the biological processes regulated by full-length p53 (FLp53).12 Importantly, the tumor-promoting functions of p53 mutations also depend on the shorter p53 isoforms from the mutated FLp53 in some specific conditions, like missense mutations.13
The human p53 gene encodes 12 natural p53 isoforms, including Δ133p53, an N-terminally truncated isoform (lacking the first 132 amino acids).14 Δ133p53 is directly transactivated by FLp53 in response to DNA-damaging signals and antagonizes p53 apoptotic activity.15 Furthermore, Δ133p53 also stimulates angiogenesis, metastasis and generation of cancer stem cells regardless of p53 mutations, and its mRNA expression is associated with increased risk of recurrence and poor outcome in various cancers.16–20 Recently, several studies further clarified that elevated Δ133p53 promotes an immunosuppressive and chemoresistant environment by inducing secretion of CCL-2, IL-6 and the recruitment of tumor-associated macrophages.21,22 Thus, Δ133p53 isoform serves as an important oncogene by antagonistically modulating p53 functions.23,24 Previously, we have demonstrated that Δ133p53 promotes DNA double-strand break (DSB) repair and tumorigenesis by coordinating with p73 in a p53-independent manner;12,25 however, the expression level of Δ133p53 and its prognostic performance in ESCC remains unknown.
In the present study, we first measured the levels of Δ133p53 and p53 and calculated their ratio (Δ133p53/FLp53) in cancerous tissue compared to adjacent normal tissues; subsequently, we analyzed their prognostic value in ESCC patients undergoing tumor resection. Circulating p53 mutations were significantly associated with drug resistance and disease progression of patients with metastatic breast cancer.26 Based on promising results in the tissue, we further investigated dynamic changes and prognostic significance of the serum Δ133p53/FLp53 ratio in ESCC patients.
Patients and Methods
Patients and Samples
FFPE cancerous tissue samples and parallel serum samples of 180 ESCC patients with overall survival information were collected from the Central Hospital of Enshi Autonomous Prefecture (China) between January 2009 to December 2012. All cases were pathologically confirmed as ESCC and did not receive chemotherapy and radiotherapy before tumor resection. Serum samples were obtained before and within 72 h following surgery, and then stored at −80°C for further use. FFPE tissue samples were obtained at the time of surgery and adjacent normal tissue samples were also collected from 42 of 180 ESCC patients. Due to the fact that 31 patients had no regular follow-up checks for recurrence or progression after surgery (confirmed by CT scan), 149 in 180 ESCC patients with recurrence information were included for PFS analysis. Patient clinical information, including age, gender, BMI, smoking, clinicopathological features (tumor location, TNM and differentiation stage) were obtained from the clinical or pathologic records. All cases of ESCC were staged based on the 7th edition of the AJCC/UICC TNM classification system. This study was approved by the Ethics Committee of Central Hospital of Enshi Autonomous Prefecture. All participants were informed about the purpose, procedures, benefits and potential risks of the study, and their written or oral consents (if patients are without culture, or culture is very shallow, the informed oral consent process was approved by the Ethics Committee of the Central Hospital of Enshi Autonomous Prefecture) were obtained.
RNA Isolation and cDNA Synthesis
Five 8-μm-thick FFPE tissue samples were cut from each block and placed in sterile 1.5-mL centrifuge tubes ready for extraction. Total RNA was extracted using an RNAprep Pure FFPE Kit (TIANGEN Biotech, Beijing, China) according to the manufacturer’s instructions. Total RNA of 300 µL serum was isolated by using a Liquid Total RNA Isolation Kit (BioTeke, Beijing, China) as we described previously27 and treated with DNase I prior to reverse transcription. The concentration of RNA was measured by Nanodrop 2000 spectrophotometer (Thermo Fisher) following purification with RNeasy mini kit (QIAGEN). First strand cDNA was synthesized using M-MLV Reverse Transcriptase (Invitrogen) and conditions were as follows: 65°C for 5 min, and then 37°C for 50 min, 70°C for 15 min.
Quantitative Real-Time PCR (qRT-PCR)
The expressions of Δ133p53 and full-length p53 (FLp53) were determined on the ABI-7300 (Thermo Fisher) using Maxima SYBR Green/ROX qPCR Master Mix (Thermo Fisher Scientific) according to the manufacturer’s instructions. The primers used were as follows: Δ133p53 (GenBank accession No. NM_001126115.1)15 (Forward: 5ʹ-TGGGTTGCAGGAGGTGCTTAC-3ʹ, Reverse: 5ʹ-CCACTCGGATA AGATGCTGAGG-3ʹ), FLp53 (Forward: 5ʹ-GCTCAAGACTGGCGCTAAA-3ʹ, Reverse: 5ʹ-GTTTTCA GGAAGTAGTTTCCATAGG-3ʹ), and GAPDH (Forward: 5ʹ-GAGTCAACGGATTTGGTCGTAT-3ʹ, Reverse: 5ʹ-ATGGGTGGAATCATATTGGAAC-3ʹ) was used as the endogenous control.28 The reactions were started at 95°C for 5 min, followed by 42 cycles of 95°C for 30 s, 59.3°C for 30 s, and 72°C for 30 s. All experiments were carried out in triplicate for each data point. Relative quantification of Δ133p53 and FLp53 expression was calculated with the 2−ΔCt method.
Statistical Analysis
SPSS software (version 17.0; USA) and Graphpad Prism software (version V.5.00, USA) were used to perform the statistical analyses in this study. Differences in the Δ133p53/FLp53 ratio between ESCC and paired adjacent normal tissues were compared using a paired Student’s t-test. Patients were divided into relatively high- and low-expression groups according to the cutoff value determined by X-tile 3.6.1 software (Yale University, New Haven, CT, USA)29 in serum and tissue samples for survival analysis. The χ2 test or Fisher’s exact test was used to determine the correlations of Δ133p53/FLp53 in tissue or serum samples with the clinicopathological factors of ESCC patients. Pearson’s correlation coefficient analysis was used to determine the association of the Δ133p53/FLp53 ratio in the tissue and in the serum. Survival analysis was carried out by the Kaplan-Meier method, and subjected to the log rank test. Univariate and multivariate Cox survival (Forward Stepwise Likelihood Ratio method) analyses were applied to assess the hazard ratios (HRs). For the Cox proportional hazards regression model, all covariate, including age, gender, BMI, smoking history, tumor location, pathologic M, N and T stage, grade, recurrence, tissue Δ133p53/p53 ratio and serum Δ133p53/p53 ratio were treated as binary variable and adjusted for the multivariate Cox proportional hazard regression model on tissue and serum Δ133p53/p53 ratio. P < 0.05 was considered statistically significant. Receiver operating characteristic (ROC) curve analysis was conducted by MedCalc statistical software (Version 18.11.6, USA) to determine the predictive value of the parameters.
Results
Δ133p53 and Δ133p53/FLp53 Ratio Significantly Increased in ESCC Tissues
As there is no specific antibody for the Δ133p53 isoform,30 we first examined the mRNA abundance of Δ133p53 in 42 pairs of tumor and adjacent normal tissues to determine whether Δ133p53 was associated with ESCC progression. Δ133p53 isoform significantly increased in cancerous tissues (0.10 ± 0.09 vs 0.05 ± 0.03, P = 0.0019) (Figure 1A). We simultaneously detected mRNA expression of FLp53 in these paired samples and confirmed that FLp53 is significantly decreased in cancerous tissues of ESCC patients (0.06 ± 0.04 vs 0.17 ± 0.14, P < 0.0001) (Figure 1B). In addition, we also noticed that the expression ratio of Δ133p53 to FLp53 significantly increased in cancerous tissues (2.40 ± 3.16 vs 0.50 ± 0.64, P = 0.0006) (Figure 1C).
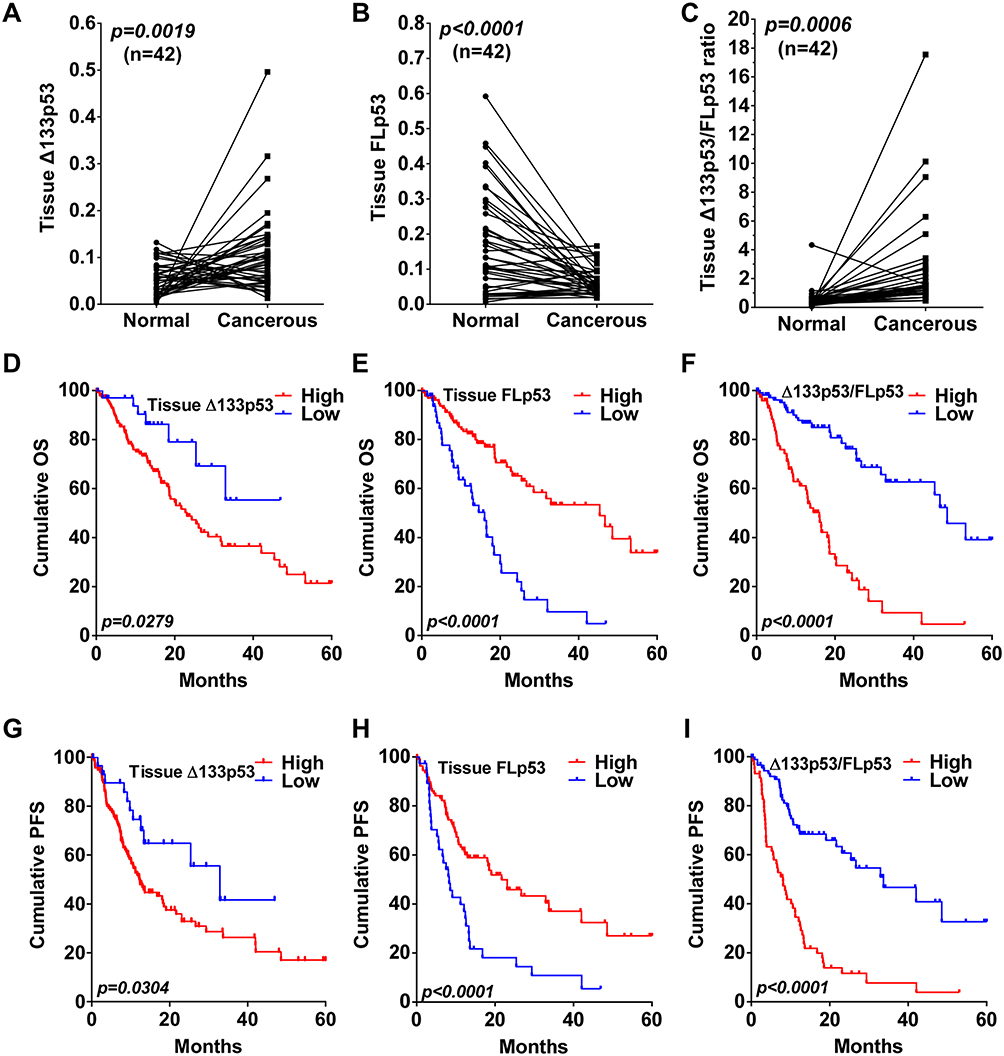 |
Figure 1 Kaplan–Meier curves of tissue Δ133p53, FLp53 and Δ133p53/FLp53 ratio in ESCC. mRNA expression of Δ133p53 (A), FLp53 (B) and Δ133p53/FLp53 ratio (C) in 42 paired adjacent normal and cancerous tissue of ESCC patients. ESCC, esophageal squamous cell carcinoma; FLp53, full-length p53. OS of 180 ESCC patients divided by tissue Δ133p53 (D), FLp53 (E) and Δ133p53/FLp53 ratio (F). PFS of 149 ESCC patients divided by tissue Δ133p53 (G), FLp53 (H) and Δ133p53/FLp53 ratio (I). Abbreviations: OS, overall survival; PFS, progression-free survival. |
Elevated Tissue Δ133p53/FLp53 Ratio Predicts Poor Outcome of ESCC Patients
To confirm the association of Δ133p53 and FLp53 with clinical outcomes of ESCC patients, we then measured Δ133p53 and FLp53 expression in 180 FFPE ESCC tissue samples. The optimal cut-off values of Δ133p53, FLp53 and Δ133p53/FLp53 ratio for predicting the prognosis of ESCC were estimated by X-tile 3.6.1 software (Figure S1). ESCC patients were divided into two groups (Δ133p53 <0.0425 and ≥0.0425; FLp53 <0.0195 and ≥0.0195; Δ133p53/FLp53 ratio <2.6470 and ≥2.6470). The clinicopathological characteristics of the ESCC patients divided by the cut-off values of Δ133p53, FLp53 and Δ133p53/FLp53 ratio are shown in Table 1. Our results indicated that the elevated Δ133p53 was significantly associated with increased TNM stage (P = 0.0011), differentiation grade (P = 0.0030) and recurrence (P = 0.0371), although it had no significant correlations with other clinicopathological features such as age, gender, and BMI index (Table 1). Decreased FLp53 was significantly associated with male gender (P = 0.0166), higher BMI (P = 0.0078), lower tumor location (P = 0.0295), increased TNM stage (P < 0.0001), differentiation grade (P < 0.0001) and recurrence (P < 0.0001) (Table 1). Increased Δ133p53/FLp53 ratio was significantly associated with Lower tumor location (P = 0.0091), increased TNM stage (P < 0.0001), differentiation grade (P < 0.0001) and recurrence (P < 0.0001) (Table 1).
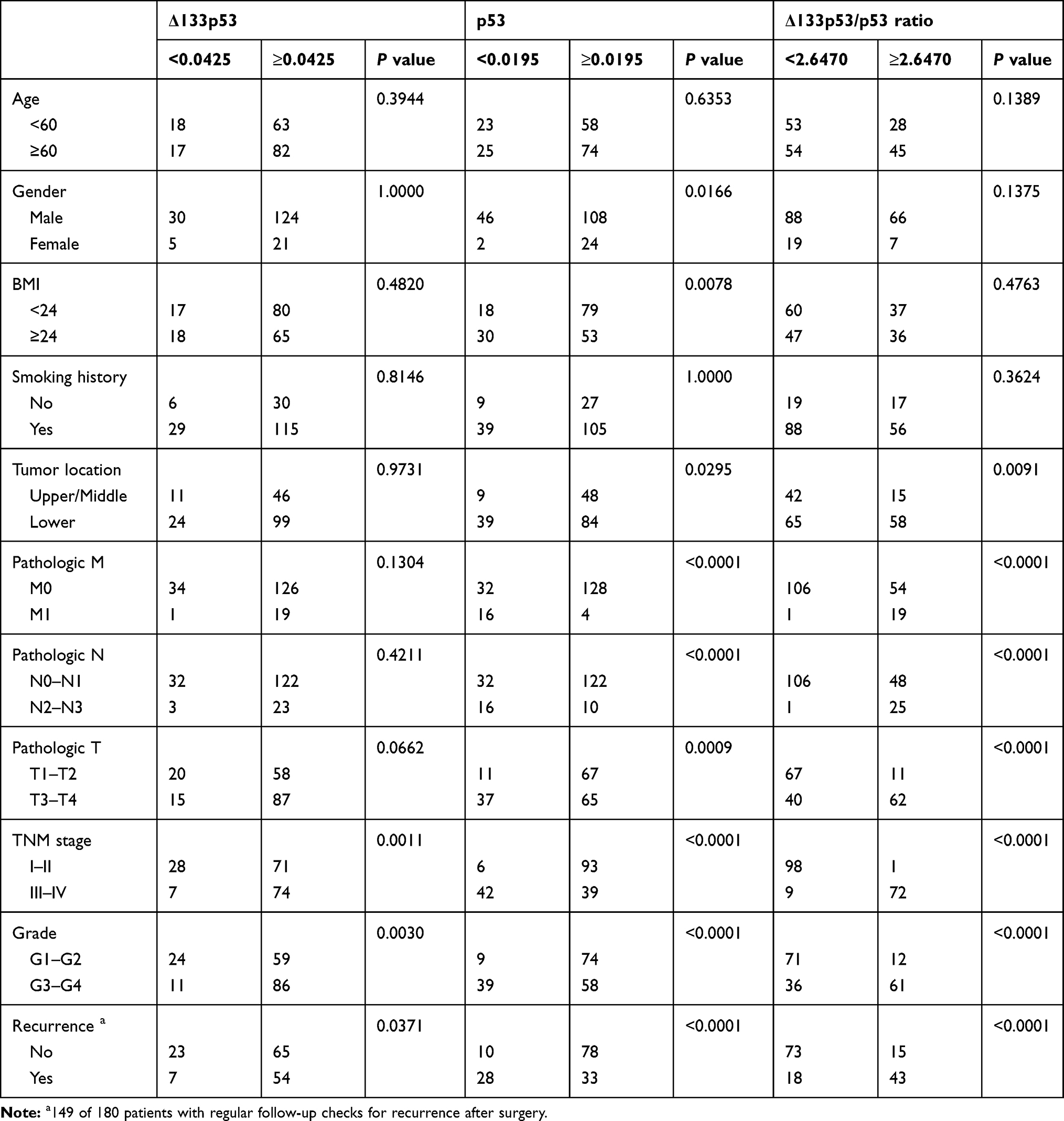 |
Table 1 Associations of Tissue Δ133p53, p53 and Δ133p53/p53 Ratio with Clinicopathological Features in ESCC |
The median survival time of all patients was 25.47 months (range 0.3–60 months), 106 patients (58.89%) were censored and 74 patients (41.11%) died during our follow-up period. Kaplan-Meier analysis revealed that increased tissue abundance of Δ133p53 (χ2 = 4.83, P = 0.0279) (Figure 1D) and decreased p53 expression (χ2 = 27.76, P < 0.0001) (Figure 1E), as well as increased Δ133p53/FLp53 ratio (χ2 = 42.34, P < 0.0001) (Figure 1F) were significantly related to worse OS. By the time of analysis, 149 of 180 ESCC patients had regular follow-up checks for recurrence after surgery. Recurrence occurred in 61 of 149 patients, with a median follow-up time of 13.4 months (range 0.8–42 months), and 88 patients had clear evidence of no recurrence. Tissue Δ133p53 and Δ133p53/FLp53 ratio were significantly increased in recurrent patients compared with non-recurrent ones (P = 0.0032 and P < 0.0001, respectively), and FLp53 was decreased in recurrent patients (P = 0.0023) (Figure S2). Kaplan-Meier analysis revealed that increased Δ133p53 (χ2 = 4.69, P = 0.0304) (Figure 1G), decreased p53 expression (χ2 = 15.53, P < 0.0001) (Figure 1H) and increased Δ133p53/FLp53 ratio (χ2 = 39.18, P < 0.0001) (Figure 1I) were significantly associated with worse PFS. Thus, these results demonstrate that tissue Δ133p53 and FLp53 expression, tissue Δ133p53/FLp53 ratio are associated with OS and PFS of ESCC patients.
Serum Δ133p53/FLp53 Ratio Shows Prognostic Significance in ESCC Patients
p53 could exist as circulating DNA or mRNA in cancers,28,31 we next further evaluated Δ133p53 and FLp53 mRNA expression in serum of 180 ESCC patients. Pearson’s correlation coefficient analysis revealed that serum Δ133p53, FLp53 and Δ133p53/FLp53 ratio were positively correlated with their tissue expression, and Pearson’s correlation coefficients were 0.7019 (P < 0.0001) (Figure 2A), 0.4030 (P < 0.0001) (Figure 2B) and 0.4137 (P < 0.0001) (Figure 2C), respectively. ESCC patients were divided into two groups (Δ133p53 <0.0870 and ≥0.0870; FLp53 <0.0300 and ≥0.0300; Δ133p53/FLp53 ratio <2.9160 and ≥2.9160) by X-tile 3.6.1 software (Figure S3). Correlation analysis revealed that the elevated serum Δ133p53 was significantly associated with male gender (P = 0.0105), increased M stage (P = 0.0086), N stage (P = 0.0184) and TNM stage (P = 0.0008), as well as recurrence (P = 0.0005) (Table 2). Increased Δ133p53/FLp53 ratio was significantly associated with high BMI index (P = 0.0287), increased M stage (P < 0.0001), N stage (P = 0.0133), TNM stage (P < 0.0001), differentiation grade (P = 0.0131) and recurrence (P < 0.0001) (Table 2). Whereas decreased serum FLp53 was only associated with increased TNM stage (P = 0.0276) and recurrence (P = 0.0007) (Table 2).
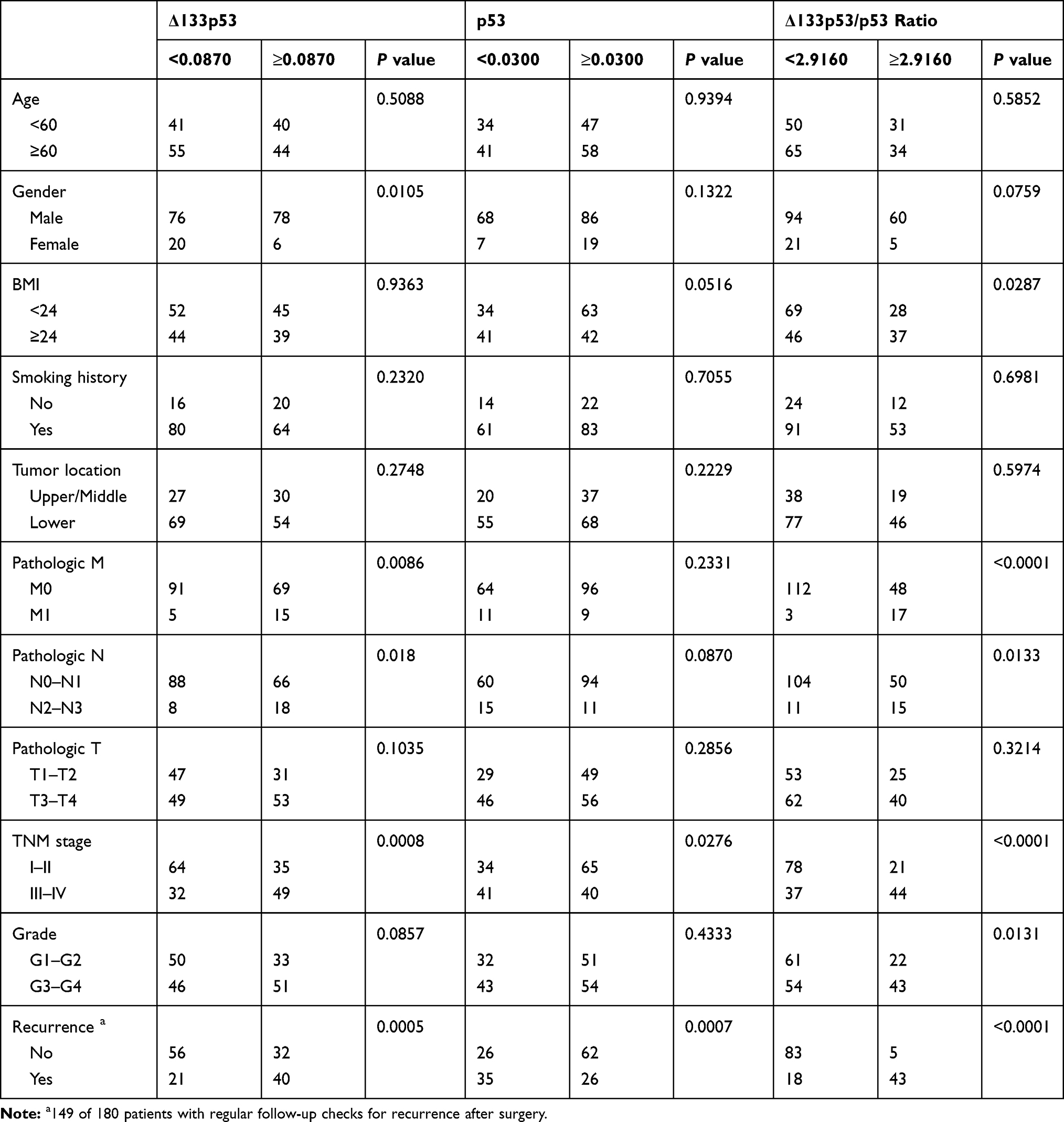 |
Table 2 Associations of Serum Δ133p53, p53 and Δ133p53/p53 Ratio with Clinicopathological Features in ESCC |
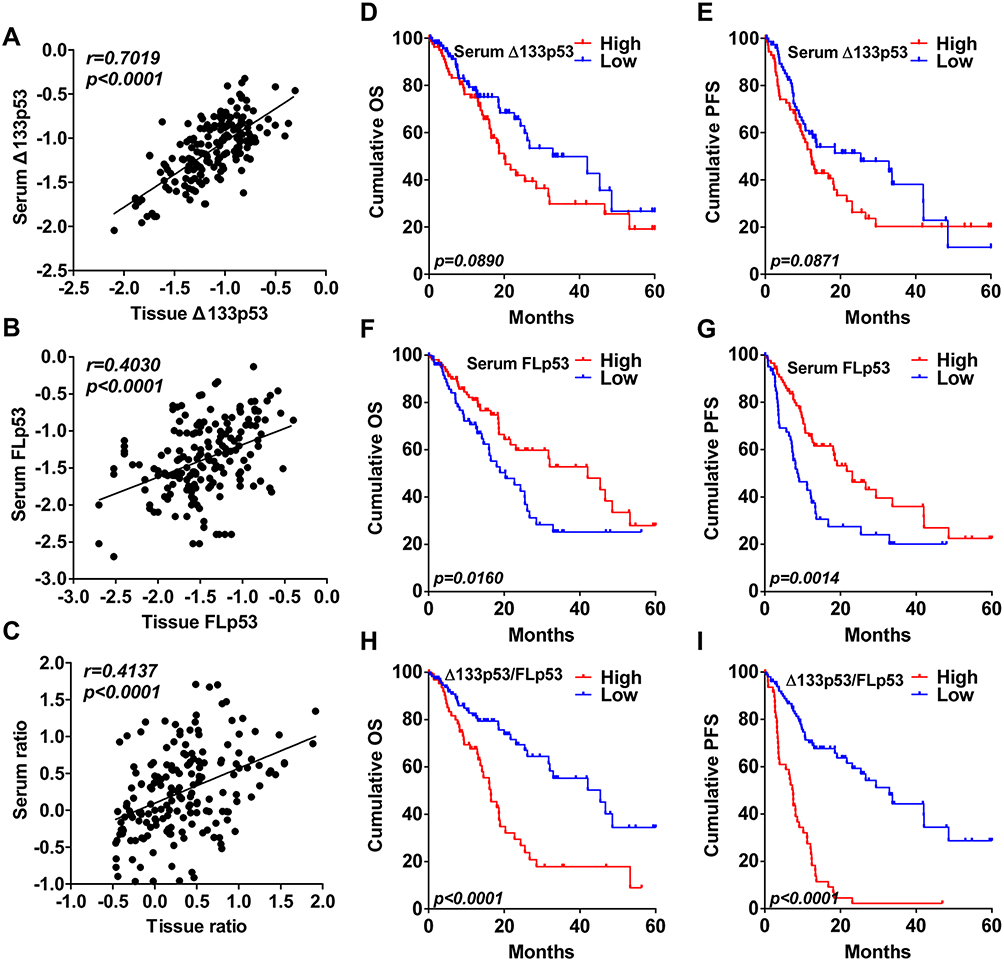 |
Figure 2 Kaplan–Meier curves of serum Δ133p53, FLp53 and Δ133p53/FLp53 ratio in ESCC. Pearson’s correlation analysis between tissue Δ133p53 (A), FLp53 (B), Δ133p53/FLp53 ratio (C) and their respective level in serum of ESCC patients. OS of 180 ESCC patients divided by preoperative serum Δ133p53 (D), FLp53 (F) and Δ133p53/FLp53 ratio (H). PFS of 149 ESCC patients divided by preoperative serum Δ133p53 (E), FLp53 (G) and Δ133p53/FLp53 ratio (I). |
Serum Δ133p53 and Δ133p53/FLp53 ratio were significantly increased in recurrent patients compared with non-recurrent ones (P = 0.0002 and P < 0.0001, respectively) (Figure S4A and S4C), FLp53 was decreased in recurrent patients (P = 0.0001) (Figure S4B). However, survival analysis indicated that increased serum Δ133p53 showed no association with OS (χ2 = 2.89, P = 0.0890) (Figure 2D) and PFS (χ2 = 2.93, P = 0.0871) (Figure 2E). Decreased p53 expression correlated with decreased OS (χ2 = 5.80, P = 0.0160) (Figure 2F) and PFS (χ2 = 10.27, P = 0.0014) (Figure 2G); and increased Δ133p53/FLp53 ratio correlated with poor OS (χ2 = 17.26, P < 0.0001) (Figure 2H) and PFS (χ2 = 56.16, P < 0.0001) (Figure 2I). Taken together, these results suggest that serum FLp53 expression and Δ133p53/FLp53 ratio are associated with OS and PFS of ESCC patients.
Tissue and Serum Δ133p53/FLp53 Ratios are Poor Independent Prognostic Factors for ESCC
The univariate survival analysis indicated that tissue and serum Δ133p53/FLp53 ratio were correlated with OS (Table 3) and PFS (Table 4) of ESCC patients. Furthermore, the multivariate analyses identified that the tissue Δ133p53/FLp53 ratio was an independent prognostic factor for OS (HR = 3.864; 95% CI = 2.293–6.511, P < 0.0001) (Table 3) and PFS (HR = 2.283; 95% CI = 1.387–3.760, P < 0.0001) (Table 4) of ESCC patients. The serum Δ133p53/FLp53 ratio was also an independent prognostic factor for OS (HR = 2.503; 95% CI = 1.465–4.276, P = 0.0011) (Table 3) and PFS (HR = 3.230; 95% CI = 1.947–5.359, P < 0.0001) (Table 3) of ESCC patients. Besides, M stage and recurrence were also predictive indicators for OS and PFS. However, serum Δ133p53 or FLp53 and tissue Δ133p53 were not independent prognostic factors for OS and PFS of ESCC patients, except tissue FLp53 (data not shown).
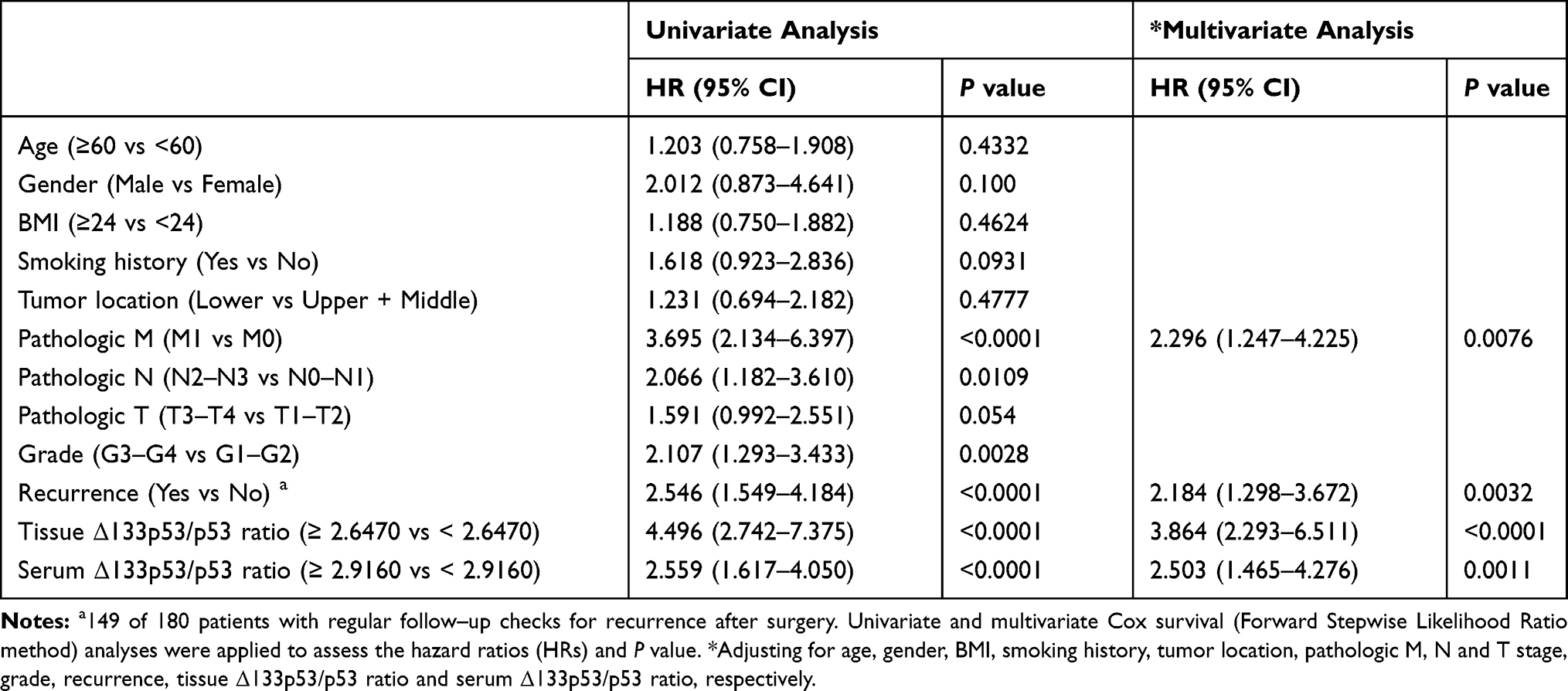 |
Table 3 Univariate and Multivariate Survival Analyses of OS in Patients with ESCC |
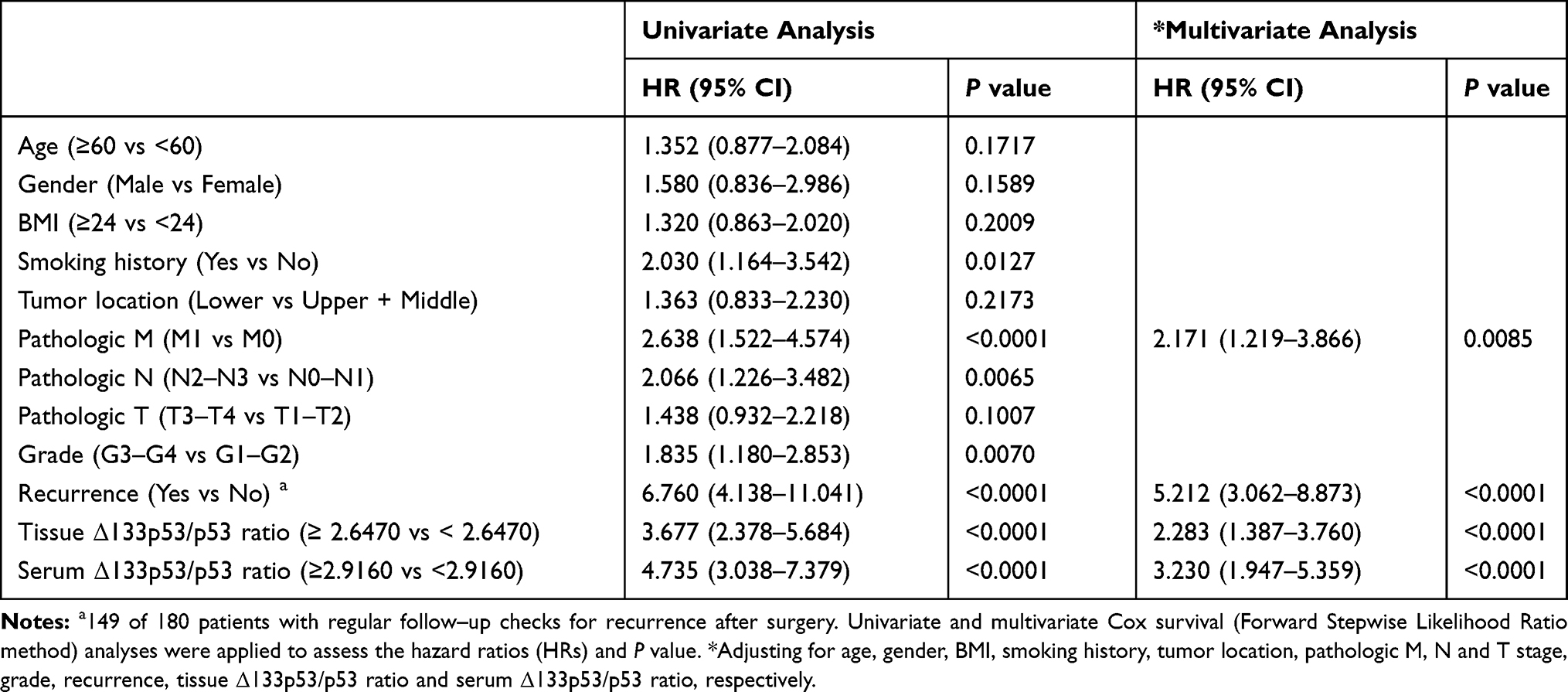 |
Table 4 Univariate and Multivariate Survival Analyses of PFS in Patients with ESCC |
Tissue and Serum Δ133p53/FLp53 Ratios Show No Difference in Prognostic Performance for OS and PFS
We also conducted a ROC analysis of tissue and serum Δ133p53/FLp53 ratio. The AUC values of tissue and serum Δ133p53/FLp53 ratio in the Cox regression model for OS were 0.695 (P = 0.0351) and 0.641 (P = 0.0360), respectively (Figure 3A), and 0.692 (P = 0.0337) and 0.649 (P = 0.0340) for PFS, respectively (Figure 3B). Prognostic performance of tissue and serum Δ133p53/FLp53 ratio showed no statistical difference for OS and PFS (P = 0.2066 and P = 0.3207, respectively).
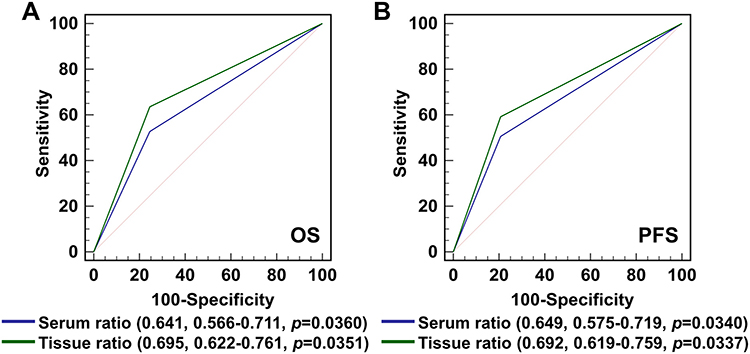 |
Figure 3 The ROC analysis of tissue and serum Δ133p53/FLp53 ratio in Cox regression model. Patients were divided into two groups according to the cutoff value of tissue (2.6470) and serum (2.9160) Δ133p53/FLp53 ratio, separately. (A) Receiver operating curve in the OS model. (B) Receiver operating curve in the PFS model. |
The Dynamic Change of Serum Δ133p53/FLp53 Ratio After Surgery and Its Association with Recurrence
To evaluate whether serum Δ133p53/FLp53 ratio dynamically correlates with treatment response, we further measured its postoperative level in 180 ESCC patients within 72 h after resection. Postoperative serum Δ133p53/FLp53 ratio significantly dropped after surgery (4.31 ± 7.69 vs 2.81 ± 4.12, P = 0.0098) (Figure 4A). Based on changes between preoperative and postoperative serum Δ133p53/FLp53 ratio, patients were divided into four groups: I, persistent high levels at the two time points; II, preoperative high followed by postoperative low; III, preoperative low followed by postoperative high, and IV, preoperative low followed by postoperative low, using the same cutoff value of preoperative serum Δ133p53/FLp53 ratio (2.9160). Persistent high levels of serum Δ133p53/FLp53 ratio predicted poor OS (Figure 4B), higher recurrence rates (Figure 4C) and worse PFS (Figure 4D) in ESCC patients. Patients in group I showed significantly shorter time to relapse (TTR) and higher recurrence rates than group IV (median TTR of 5.57 months vs not reached; recurrence of 27/28 vs 14/88, P < 0.0001), as well as group III (median TTR of 5.57 months vs 29.4 months; recurrence of 27/28 vs 4/13, P < 0.0001), while there was a propensity of increased recurrence compared with group II (median TTR of 5.57 months vs 8.07 months; recurrence of 27/28 vs 16/20; P = 0.0643) (Figure 4C). Compared with group IV, patients in groups I and II had significantly shorter TTR and higher recurrence rates (all P < 0.0001, Figure 4C).
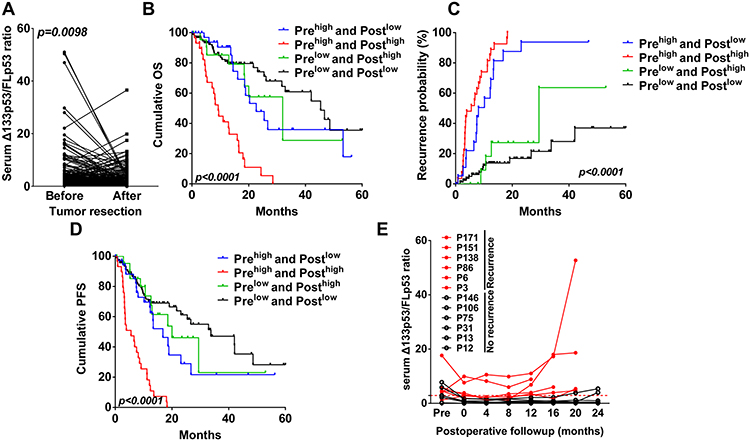 |
Figure 4 Dynamic changes of serum Δ133p53/FLp53 ratio reflect treatment response and recurrence risk of ESCC. (A) Changes of serum Δ133p53/FLp53 ratio before versus after (within 72 h following) resection. (B) OS of 180 ESCC patients divided by pre- and post-operative serum Δ133p53/FLp53 ratio, cutoff value was 2.9160. (C) Prognostic significance for time to recurrence in patients with persistent high serum Δ133p53/FLp53 ratio, conversion of serum Δ133p53/FLp53 ratio from high to low, conversion of serum Δ133p53/FLp53 ratio from low to high, and persistent low (cutoff value was 2.9160). (D) PFS of 149 ESCC patients divided by pre- and post-operative serum Δ133p53/FLp53 ratio, cutoff value was 2.9160. (E) 12 patients were monitored by CT scans every 4 months in a time range of 24 months, serum Δ133p53/FLp53 ratio were measured at each time until recurrence occurred. Dashed line means Y = 2.9160. |
Twelve patients with no history of radio- or chemo-therapies after tumor resection were selected for measurement of real-time changes of serum Δ133p53/FLp53 ratio in each time of follow-up (tumor recurrence was monitored by CT scans every 4 months in the first two years). Six patients were confirmed to have lung, brain or lymph node metastasis, and the other 6 showed no evidence of recurrence. The serum Δ133p53/FLp53 ratios were higher than 2.9160 at the time of detected recurrence in 6 patients and even increased prior to radiologic progression in 2/6 patients, while they were lower than 2.9160 in 4/6 patients with no recurrence (Figure 4E). In addition, healthy donors exhibited significantly lower serum Δ133p53/FLp53 ratios than did ESCC patients preoperatively, mostly lower than 2.9160 (Figure S4D). The best cutoff value of the serum Δ133p53/FLp53 ratio to distinguish ESCC patients from healthy donors was 0.6798 (Sensitivity: 76.11%; Specificity: 77.55%, AUC = 0.8376), which was also less than 2.9160 (Figure S4E). These results indicate the potential usefulness of serum Δ133p53/FLp53 ratio as a prognostic predictor for ESCC and may also reflect recurrence risk in a real-time manner.
Discussion
This investigation provides the novel finding that the pre-operative tissue abundance of Δ133p53 as well as the Δ133p53/FLp53 ratio were significantly elevated in recurrent ESCC patients compared with non-recurrent patients. This finding is consistent with previous reports that Δ133p53 increases risk of cancer recurrence in breast18 and ovarian cancer.32 Furthermore, clinicopathological factor distribution analyses also revealed that Δ133p53 and FLp53 expression, as well as the Δ133p53/FLp53 ratio correlated significantly with TNM stage or recurrence state. Most importantly, the Kaplan-Meier curve revealed that increased tissue Δ133p53 and Δ133p53/FLp53 ratio and decreased FLp53 were correlated to worse OS and PFS in ESCC patients. Thus, Δ133p53 may also play an oncogenic role in ESCC progression.
Δ133p53 constituted an independent prognostic marker in patients with advanced serous ovarian cancer.32 In our study, tissue FLp53 and Δ133p53/FLp53 ratio were shown to serve as independent prognostic factors for OS and PFS, while Δ133p53 was not in a further univariate and multivariate analysis. Although we have previously confirmed that Δ133p53 can act synergistically with p73 to upregulate the transcription of rad51, lig4 and rad52 by joining together to bind to a novel type of Δ 133p53-responsive element in their promoters,12,25 the detailed molecular mechanism of Δ133p53 function is still unclear, the possibility of this inconsistency may result from the fact that Δ133p53 has three isoforms (α, β and γ), which have been shown to have specific functions in a cancer or disease-specific manner and could be regulated by different factors.18 As in breast cancer, Δ133p53β promotes cancer cell invasion and associates with cancer progression, while Δ133p53α and γ are not.18 In human glioblastoma, the Δ133p53 angiogenic effect is due to Δ133p53α and γ, but not the β isoform.16 SRSF1, an essential splicing factor, promotes vascular smooth muscle cell (VSMC) proliferation and injury-induced neointima formation via inducing Δ133p53α, but not the γ and β isoforms.33 It is worth noting that the expression level of SRSF1 differs among 33 cancer types as confirmed by Cancer Genome Atlas (TCGA) Program. The detailed roles of individual Δ133p53 isoforms (α, β and γ) and their functional molecular mechanisms should be investigated in future studies.
Circulating DNA/RNAs are not affected by tissue sampling timing and conditions, and thus are optimal diagnostic or prognostic biomarkers for various cancers, including ESCC.34,35 We previously reported that circulating RNAs could be used as diagnostic biomarkers for non-small cell lung carcinoma.27 In this investigation, we then further measured Δ133p53 and FLp53 expression in serum samples by using GAPDH28 as an internal control. The Pearson’s correlation coefficient of Δ133p53 was 0.7019 between serum and tissue, significantly higher than that of FLp53 (r = 0.4030) and Δ133p53/FLp53 ratio (r = 0.4137), which indicated that cancer cells may be the main source of Δ133p53. Δ133p53 is significantly increased during the progression from premalignant adenoma to malignant carcinoma.36 Similar to results obtained from tissue samples, the serum abundance of Δ133p53 as well as the Δ133p53/FLp53 ratio were significantly increased in recurrent ESCC patients, and were related to TNM stage and recurrence state. Although serum Δ133p53 showed no prognostic value in ESCC patients, the Δ133p53/FLp53 ratio showed a better prognostic performance than FLp53 alone for OS (χ2 value, 17.26 vs 5.80) and PFS (χ2 value, 56.16 vs 10.27) prediction. Furthermore, ROC analysis revealed that prognostic performance of the serum Δ133p53/FLp53 ratio showed no statistical difference from the tissue ratio, both of which were confirmed to be independent prognostic biomarkers for OS and PFS in multivariate analysis.
The clinical utility of monitoring circulating DNA/RNA changes with treatment and recurrence has been reported in various types of cancers.37,38 In this study, we reported for the first time that a significant decrease of serum Δ133p53/FLp53 ratio was observed soon after resection, which may well be attributed to surgical resection of the primary tumor. Patients with consistently high serum Δ133p53/FLp53 ratio (higher than 2.9160 before and after surgery) showed increased recurrence rate and shorter TTR than those with postoperatively or consistently low levels. Furthermore, serum Δ133p53/FLp53 ratios were higher than 2.9160 and even increased prior to the time of radiologically detected recurrence. Based on these results, we propose that serum Δ133p53/FLp53 ratio may be a real-time surrogate indicator for treatment response and recurrence risk following the ESCC curative resection.
Conclusions
In summary, the results of this study demonstrate that preoperative high serum or tissue Δ133p53/FLp53 ratio are independent prognostic factors for OS or PFS in ESCC patients undergoing curative resection. Serum Δ133p53/FLp53 ratio in ESCC patients was significantly decreased within 72 h post tumor resection and patients with a consistently high serum Δ133p53/FLp53 ratio (≥2.9160) (pre- and post-operative) had higher recurrence rates than those with consistently low ratio values. In addition, dynamic detection at each follow-up timepoint showed that serum Δ133p53/FLp53 ratios were increased upon radiologically detected progression. Thus, the serum Δ133p53/FLp53 ratio can be a novel predictor for survival outcome and may serve as a real-time parameter for monitoring recurrence in ESCC patients after surgery.
Abbreviations
ESCC, esophageal squamous cell carcinoma; FLp53, full-length p53; OS, overall survival; PFS, progression-free survival; ROC, receiver-operating characteristic curve; CNAs, copy number alterations; TTR, time to relapse; VSMC, vascular smooth muscle cell.
Data Sharing Statement
We are willing to share anonymized data after required ethical approval by the Ethics Committee of Central Hospital of Enshi Autonomous Prefecture.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of Central Hospital of Enshi Autonomous Prefecture. All participants were informed about the purpose, procedures, benefits and potential risks of the study, and their written or oral consents were obtained. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
2. Deng J, Chen H, Zhou D, et al. Comparative genomic analysis of esophageal squamous cell carcinoma between Asian and Caucasian patient populations. Nat Commun. 2017;8(1):1533. doi:10.1038/s41467-017-01730-x
3. Mariette C, Markar SR, Dabakuyo-Yonli TS, et al. Hybrid minimally invasive esophagectomy for esophageal cancer. N Engl J Med. 2019;380(2):152–162. doi:10.1056/NEJMoa1805101
4. Wu C, Li D, Jia W, et al. Genome-wide association study identifies common variants in SLC39A6 associated with length of survival in esophageal squamous-cell carcinoma. Nat Genet. 2013;45(6):632–638. doi:10.1038/ng.2638
5. Ohashi S, Miyamoto S, Kikuchi O, Goto T, Amanuma Y, Muto M. Recent advances from basic and clinical studies of esophageal squamous cell carcinoma. Gastroenterology. 2015;149(7):1700–1715. doi:10.1053/j.gastro.2015.08.054
6. Hao JJ, Lin DC, Dinh HQ, et al. Spatial intratumoral heterogeneity and temporal clonal evolution in esophageal squamous cell carcinoma. Nat Genet. 2016;48(12):1500–1507. doi:10.1038/ng.3683
7. Song Y, Li L, Ou Y, et al. Identification of genomic alterations in oesophageal squamous cell cancer. Nature. 2014;509(7498):91–95. doi:10.1038/nature13176
8. Lin DC, Hao JJ, Nagata Y, et al. Genomic and molecular characterization of esophageal squamous cell carcinoma. Nat Genet. 2014;46(5):467–473. doi:10.1038/ng.2935
9. Gao YB, Chen ZL, Li JG, et al. Genetic landscape of esophageal squamous cell carcinoma. Nat Genet. 2014;46(10):1097–1102. doi:10.1038/ng.3076
10. Sawada G, Niida A, Uchi R, et al. Genomic landscape of esophageal squamous cell carcinoma in a Japanese population. Gastroenterology. 2016;150(5):1171–1182. doi:10.1053/j.gastro.2016.01.035
11. Bykov VJN, Eriksson SE, Bianchi J, Wiman KG. Targeting mutant p53 for efficient cancer therapy. Nat Rev Cancer. 2017;18:89. doi:10.1038/nrc.2017.109
12. Gong L, Gong H, Pan X, et al. p53 isoform Δ113p53/Δ133p53 promotes DNA double-strand break repair to protect cell from death and senescence in response to DNA damage. Cell Res. 2015;25(3):351–369. doi:10.1038/cr.2015.22
13. Candeias MM, Hagiwara M, Matsuda M. Cancer-specific mutations in p53 induce the translation of Δ160p53 promoting tumorigenesis. EMBO Rep. 2016;17(11):1542–1551. doi:10.15252/embr.201541956
14. Mondal AM, Zhou H, Horikawa I, et al. Δ133p53α, a natural p53 isoform, contributes to conditional reprogramming and long-term proliferation of primary epithelial cells. Cell Death Dis. 2018;9(7):750. doi:10.1038/s41419-018-0767-7
15. Gong L, Pan X, Chen H, et al. p53 isoform Δ133p53 promotes efficiency of induced pluripotent stem cells and ensures genomic integrity during reprogramming. Sci Rep. 2016;6:37281. doi:10.1038/srep37281
16. Bernard H, Garmy-Susini B, Ainaoui N, et al. The p53 isoform, Δ133p53alpha, stimulates angiogenesis and tumour progression. Oncogene. 2013;32(17):2150–2160. doi:10.1038/onc.2012.242
17. Roth I, Campbell H, Rubio C, et al. The Δ133p53 isoform and its mouse analogue Delta122p53 promote invasion and metastasis involving pro-inflammatory molecules interleukin-6 and CCL2. Oncogene. 2016;35(38):4981–4989. doi:10.1038/onc.2016.45
18. Gadea G, Arsic N, Fernandes K, et al. TP53 drives invasion through expression of its Δ133p53beta variant. eLife. 2016;5:e14734. doi:10.7554/eLife.14734
19. Lei J, Qi R, Tang Y, et al. Conformational stability and dynamics of the cancer-associated isoform Δ133p53β are modulated by p53 peptides and p53-specific DNA. FASEB J. 2019;33(3):4225–4235. doi:10.1096/fj.201801973R
20. Arsic N, Gadea G, Lagerqvist EL, et al. The p53 isoform Δ133p53β promotes cancer stem cell potential. Stem Cell Rep. 2015;4(4):531–540. doi:10.1016/j.stemcr.2015.02.001
21. Kazantseva M, Eiholzer RA, Mehta S, et al. Elevation of the TP53 isoform Δ133p53β in glioblastomas: an alternative to mutant p53 in promoting tumor development. J Pathol. 2018;246(1):77–88. doi:10.1002/path.5111
22. Campbell H, Fleming N, Roth I, et al. 133p53 isoform promotes tumour invasion and metastasis via interleukin-6 activation of JAK-STAT and RhoA-ROCK signalling. Nat Commun. 2018;9(1):254. doi:10.1038/s41467-017-02408-0
23. Kastenhuber ER, Lowe SW. Putting p53 in context. Cell. 2017;170(6):1062–1078. doi:10.1016/j.cell.2017.08.028
24. Aoubala M, Murray-Zmijewski F, Khoury MP, et al. p53 directly transactivates Δ133p53α, regulating cell fate outcome in response to DNA damage. Cell Death Differ. 2011;18(2):248–258. doi:10.1038/cdd.2010.91
25. Gong H, Zhang Y, Jiang K, et al. p73 coordinates with Δ133p53 to promote DNA double-strand break repair. Cell Death Differ. 2018;25(6):1063–1079. doi:10.1038/s41418-018-0085-8
26. Hu ZY, Xie N, Tian C, et al. Identifying circulating tumor DNA mutation profiles in metastatic breast cancer patients with multiline resistance. E Bio Medicine. 2018;32:111–118. doi:10.1016/j.ebiom.2018.05.015
27. Luo CL, Xu ZG, Chen H, et al. LncRNAs and EGFRvIII sequestered in TEPs enable blood-based NSCLC diagnosis. Cancer Manag Res. 2018;10:1449–1459. doi:10.2147/CMAR.S164227
28. Li Y, Elashoff D, Oh M, et al. Serum circulating human mRNA profiling and its utility for oral cancer detection. J clin oncol. 2006;24(11):1754–1760. doi:10.1200/JCO.2005.03.7598
29. Camp RL, Dolled-Filhart M, Rimm DL. X-Tile. Clin Cancer Res. 2004;10(21):7252–7259. doi:10.1158/1078-0432.CCR-04-0713
30. Marcel V, Dichtel-Danjoy ML, Sagne C, et al. Biological functions of p53 isoforms through evolution: lessons from animal and cellular models. Cell Death Differ. 2011;18(12):1815–1824. doi:10.1038/cdd.2011.120
31. Vandekerkhove G, Todenhofer T, Annala M, et al. Circulating tumor DNA reveals clinically actionable somatic genome of metastatic bladder cancer. Clin Cancer Res. 2017;23(21):6487–6497. doi:10.1158/1078-0432.CCR-17-1140
32. Hofstetter G, Berger A, Schuster E, et al. Δ133p53 is an independent prognostic marker in p53 mutant advanced serous ovarian cancer. Br J Cancer. 2011;105(10):1593–1599. doi:10.1038/bjc.2011.433
33. Xie N, Chen M, Dai R, et al. SRSF1 promotes vascular smooth muscle cell proliferation through a Δ133p53/EGR1/KLF5 pathway. Nat Commun. 2017;8:16016. doi:10.1038/ncomms16016
34. Hsu FM, Cheng JCH, Chang YL, Lee JM, Koong AC, Chuang EY. Circulating mRNA profiling in esophageal squamous cell carcinoma identifies FAM84B as a biomarker in predicting pathological response to neoadjuvant chemoradiation. Sci Rep. 2015;5:10291. doi:10.1038/srep10291
35. Jin Z, Olaru A, Yang J, et al. Hypermethylation of tachykinin-1 is a potential biomarker in human esophageal cancer. Clin Cancer Res. 2007;13(21):6293–6300. doi:10.1158/1078-0432.CCR-07-0818
36. Fujita K, Mondal AM, Horikawa I, et al. p53 isoforms Δ133p53 and p53beta are endogenous regulators of replicative cellular senescence. Nat Cell Biol. 2009;11(9):1135–1142. doi:10.1038/ncb1928
37. Liu Z, Jiang M, Zhao J, Ju H. Circulating tumor cells in perioperative esophageal cancer patients: quantitative assay system and potential clinical utility. Clin Cancer Res. 2007;13(10):2992–2997. doi:10.1158/1078-0432.CCR-06-2072
38. Khan KH, Cunningham D, Werner B, et al. Longitudinal liquid biopsy and mathematical modeling of clonal evolution forecast time to treatment failure in the prospect-c phase II colorectal cancer clinical trial. Cancer Discov. 2018;8(10):1270–1285. doi:10.1158/2159-8290.CD-17-0891
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.