")
Back to Journals » Clinical Interventions in Aging » Volume 15
Delirium: A Frequent Manifestation in COVID-19 Older Patients
Authors Mattace-Raso F , Polinder-Bos H, Oosterwijk B, van Bruchem-Visser R , Goudzwaard J, Oudshoorn C, Ziere G , Egberts A
Received 10 September 2020
Accepted for publication 22 November 2020
Published 1 December 2020 Volume 2020:15 Pages 2245—2247
DOI https://doi.org/10.2147/CIA.S280189
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Walker
Francesco Mattace-Raso, Harmke Polinder-Bos, Barbara Oosterwijk, Rozemarijn van Bruchem-Visser, Jeannette Goudzwaard, Christian Oudshoorn, Gijsbertus Ziere, Angelique Egberts
Division of Geriatric Medicine, Department of Internal Medicine, Erasmus MC University Medical Center, Rotterdam, the Netherlands
Correspondence: Francesco Mattace-Raso
Division of Geriatric Medicine, Department of Internal Medicine, Erasmus MC University Medical Center, Office RG 534, Dr. Molewaterplein 40, Rotterdam, GD 3015, the Netherlands
Tel +31 10 703 59 79
Email [email protected]
Abstract: The authors report a high prevalence of delirium in COVID-19 old patients admitted in an academic hospital. During the recent COVID-19 period, delirium was present in 38% of old patients admitted with delirium at the COVID ward of the Erasmus MC University Medical Center of Rotterdam. We do not know in which patients COVID-19 can cause delirium; however, considering the high prevalence of delirium in COVID-19 old patients and the potential serious consequences, attention is needed in order to reduce disability and mortality in this vulnerable category of patients.
Keywords: delirium, old patients, COVID-19
From March until April 2020, 123 patients aged 60 years and older were admitted at the COVID ward of the Erasmus MC University Medical Center of Rotterdam, after the onset of coronavirus disease 2019 (COVID-19), the disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
During this period, 47 patients (38%), 37 men and 10 women, mean age 71.3 years presented signs and symptoms of delirium. Of these, 39 patients developed a delirium during admission at the intensive care unit. Delirium screening was performed using the Delirium Observation Screening Scale (DOSS). A DOSS score ≥3 suggesting a delirium, was followed by a delirium assessment by the ward physician according the DSM-5 criteria.1 At the ICU, the Intensive Care Delirium Screening Checklist (ICDSC), based on the DSM-5 criteria, is used 3 times daily for screening for delirium.2 Information on comorbidities was obtained from the medical records. Differences in baseline characteristics in patients with and without delirium were investigated by the analysis of covariance adjusted for age and sex, where appropriate (Table 1).
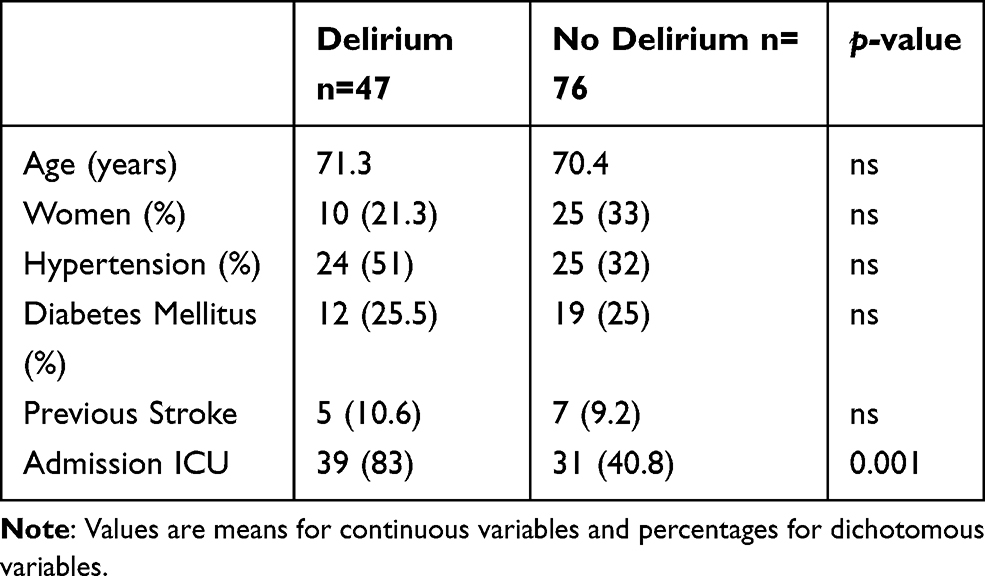 |
Table 1 Characteristics of Patients with and without Delirium |
This prevalence of delirium is high in this novel disease which frequently presents with nasal secretions, cough, dyspnea, fever, myalgia, occasionally diarrhea and in about 15% of the patients with acute respiratory distress syndrome.
The high prevalence of delirium in COVID-19 patients at the ICU might be due to serious illness of these patients, the presence of traditional risk factors, but possibly also due to withdrawal of prolonged treatment with midazolam or clonidine. Besides, severely ill COVID-19 patients develop thromboembolic episodes, myocardial damage, kidney and liver disease. It was reported that several patients with ARDS showed cerebral hypoperfusion or small acute ischemic strokes, even with no focal neurological signs.3 Neurological features such as Guillain–Barré syndrome are also described in COVID-19 positive patients;4 the virus can enter the central nervous system and increase inflammatory cytokines which can be expected to lead to delirium. With the activation of brain parenchymal cells, which might express inflammatory cytokines and other inflammatory mediators in the central nervous system, the inflammatory process can lead to neuronal and synaptic dysfunction which can be expected to lead to delirium.5
Another possible explanation could be the distinct presence of hypoxia in COVID-19 patients. Studies in surgical patients found a strong correlation between intraoperative O2 saturation and postoperative cognitive dysfunction.6 Hypoxia and decreased brain oxygenation causes a failure in oxidative metabolism, which is associated with a strong release of neurotransmitters, especially glutamate and dopamine.7 The strong release of dopamine might explain the hyperactive form of delirium with agitation and hallucinations. Hypoxia can also lead to reduced synthesis and release of acetylcholine. Cholinergic neurotransmission is sensitive to metabolic events, such as diminished availability of glucose and oxygen. Reduction in cerebral oxygen may induce delirium by impairing acetylcholine production.8
The prevalence of delirium reported in the present study is similar to the prevalence observed in other studies which have included patients of the same age but also older patients9,10 and is slightly higher than the prevalence of delirium (25–31%) reported in old patients admitted with non-COVID-19 pneumonia11,12 and in patients admitted with severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS).13 At the moment we do not know in which patients COVID-19 can cause delirium; it might be speculated that decline in physiological capacity in organ systems, with an increased susceptibility to stressors such as frailty, can play a role in these vulnerable older persons. Frailty impairs organ reserves also at biomolecular level, due to inflammaging, immunosenescence, reduced oxygen uptake and altered energy balance which can be crucial in determining the onset of delirium in older vulnerable COVID-19 patients. Moreover, additional sensory and social deprivation, because of the specific care procedures associated with the treatment of this condition and extreme diminished, or lost, contact with relatives may have negative impact on the severity and duration of the delirium.
Delirium is an acute neuropsychiatric syndrome characterized by disturbances in attention, awareness and cognition – is a frequent disorder in older hospitalized patients. It is associated with poor clinical outcomes including prolonged hospital stay, loss of independence, admission in nursing homes and mortality. Considering the dramatic consequences of delirium and the high prevalence of delirium in COVID-19 older patients we must pay attention to early recognition of neuropsychiatric disorders in order to start with delirium-related treatment to reduce disability and mortality in this vulnerable category of patients.
Ethics Statement
This study was conducted in accordance with the principles expressed in the Declaration of Helsinki. In The Netherlands, ethical approval and patient consent are not required for retrospective chart review studies in which data collected during routine clinical care are extracted and analyzed anonymously.
Disclosure
The authors report no conflicts of interest.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
2. Bergeron N, Dubois MJ, Dumont M, Dial S, Skrobik Y. Intensive care delirium screening checklist: evaluation of a new screening tool. Intensive Care Med. 2001;27:859–864. doi:10.1007/s001340100909
3. Combes A, Hajage D, Capellier G, et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. New Engl J Med. 2018;378:1965–1975. doi:10.1056/NEJMoa1800385
4. Toscano G, Palmerini F, Ravaglia S, et al. Guillain-barre syndrome associated with SARS-CoV-2. N Engl J Med. 2020;382(26):2574–2576. doi:10.1056/NEJMc2009191
5. Maldonado JR. Delirium pathophysiology: an updated hypothesis of the etiology of acute brain failure. Int J Geriatr Psychiatry. 2018;33:1428–1457. doi:10.1002/gps.4823
6. Morimoto Y, Yoshimura M, Utada K, Setoyama K, Matsumoto M, Sakabe T. Prediction of postoperative delirium after abdominal surgery in the elderly. J Anesth. 2009;23:51–56. doi:10.1007/s00540-008-0688-1
7. Siesjo BK. Cerebral circulation and metabolism. J Neurosurg. 1984;60:883–908.
8. Maldonado JR. Delirium in the acute care setting: characteristics, diagnosis and treatment. Crit Care Clin. 2008;24:657–722, vii. doi:10.1016/j.ccc.2008.05.008
9. De Smet R, Mellaerts B, Vandewinckele H, et al. Frailty and mortality in hospitalized older adults with COVID-19: retrospective observational study. J Am Med Dir Assoc. 2020;21:928–32 e1. doi:10.1016/j.jamda.2020.06.008
10. McLoughlin BC, Miles A, Webb TE, et al. Functional and cognitive outcomes after COVID-19 delirium. Eur Geriatr Med. 2020;11:857–862. doi:10.1007/s41999-020-00353-8
11. Aliberti S, Bellelli G, Belotti M, et al. Delirium symptoms during hospitalization predict long-term mortality in patients with severe pneumonia. Aging Clin Exp Res. 2015;27:523–531. doi:10.1007/s40520-014-0297-9
12. Pieralli F, Vannucchi V, Mancini A, et al. Delirium is a predictor of in-hospital mortality in elderly patients with community acquired pneumonia. Intern Emerg Med. 2014;9:195–200. doi:10.1007/s11739-013-0991-1
13. Rogers JP, Chesney E, Oliver D, et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. 2020;7:611–627. doi:10.1016/S2215-0366(20)30203-0
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.