")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
Delayed Inflammatory Reactions to Hyaluronic Acid Fillers: A Literature Review and Proposed Treatment Algorithm
Authors Artzi O , Cohen JL, Dover JS, Suwanchinda A , Pavicic T, Landau M , Goodman GJ , Ghannam S, Al Niaimi F, van Loghem JAJ , Goldie K, Sattler S, Cassuto D , Lim TS, Wanitphakdeedecha R, Verner I , Fischer TC , Bucay V , Sprecher E, Shalmon D
Received 26 January 2020
Accepted for publication 18 April 2020
Published 18 May 2020 Volume 2020:13 Pages 371—378
DOI https://doi.org/10.2147/CCID.S247171
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Ofir Artzi,1,2 Joel L Cohen,3 Jeffrey S Dover,4– 6 Atchima Suwanchinda,7,8 Tatjana Pavicic,9 Marina Landau,10 Greg J Goodman,11 Sahar Ghannam,12 Firas Al Niaimi,13 Jani AJ van Loghem,14 Kate Goldie,15 Sonja Sattler,16 Daniel Cassuto,17 Ting Song Lim,18 Rungsima Wanitphakdeedecha,19 Ines Verner,20,21 Tanja C Fischer,22,23 Vivian Bucay,24 Eli Sprecher,1,2,25 Dana Shalmon1,2
1Department of Dermatology, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel; 2Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel; 3AboutSkin Dermatology and AboutSkin Research, , Greenwood Village and Lone Tree, CO, USA; 4SkinCare Physicians, Chestnut Hill, MA, USA; 5Dermatology, Yale University School of Medicine, New Haven, CT, USA; 6Dermatology, Brown Medical School, Rhode Island, USA; 7Department of Dermatology, School of Anti-Aging and Regenerative Medicine, Mae Fah Luang University, Bangkok, Thailand; 8Division of Dermatology, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 9Private Practice for Dermatology and Aesthetics Dr. Tatjana Pavicic, Munich 80539, Germany; 10Dermatology, Private Practice, Herzliya, Israel; 11Monash University, Clayton, Victoria, Australia; 12Associate Prof. of Dermatology, Alexandria University, Alexandria, Egypt; 13 152, Harley street, London, UK; 14UMA Institute, Amsterdam 1017, TX, Netherlands; 15Medical Director European Medical Aesthetics Ltd, London W1G 8QN, UK; 16Rosenpark Klinik, Darmstadt, Germany; 17Private Practice, Milan, Italy; 18Clique Clinic, Kuala Lumpur, Malaysia; 19Department of Dermatology, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand; 20Verner Clinic, Tel Aviv, Israel; 21Department of Dermatology, University of Rome, Guglielmo Marconi, Italy; 22Skin and Laser Center, Potsdam, Germany; 23School of Medicine, University of Frankfurt, Germany; 24Bucay Center for Dermatology and Aesthetics, UTHSC, San Antonio, TX, USA; 25Department of Human Molecular Genetics & Biochemistry, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Correspondence: Ofir Artzi
Tel Aviv Sourasky Medical Center, Weizman 6, Tel Aviv, Israel
Tel +972-54-5968961
Fax +972-77-2001801
Email [email protected]
Background and Objectives: There is a wide diversity of opinions regarding the management of delayed inflammatory reactions (DIRs) secondary to hyaluronic acid (HA)-based fillers. The plethora of approaches has led the authors to conduct a review regarding management and treatment of DIRs as well as establish therapeutic guidelines for this purpose.
Materials and Methods: A review of the literature was performed through databases such as PubMed using keywords including HA-fillers and complications, delayed HA filler sequelae and therapy, soft tissue and dermal filler reactions and management. Additionally, a survey comprised of questions regarding the management and treatment of DIRs was sent to 18 physicians highly experienced with soft-tissue filler injections in 10 countries. Their answers and recommendations were analyzed and debated amongst these panelists.
Results: Sixteen panelists favored antibiotic therapy as first-line treatment for DIRs, specifically dual antibiotic therapy consisting of a fluoroquinolone along with a tetracycline or macrolide for a period of 3– 6 weeks. The majority refrained from the use of intralesional (IL) or systemic steroids except in the case of disfiguring or recalcitrant reactions. IL hyaluronidase was recommended by 13 panelists; however, some preferred a watchful waiting approach for a period of 48 hours to 2 weeks prior to IL hyaluronidase, and in cases where antibiotics did not lead to improvement.
Conclusion: A consensus was reached and summarized to propose a clear, easy-to-follow, stepwise algorithm for the treatment of DIRs.
Keywords: cosmetic techniques, dermal fillers/adverse effects, hyaluronic acid/adverse effects
Introduction
Delayed inflammatory reactions (DIRs) to hyaluronic acid (HA)-based fillers are widely discussed and debated at many conferences as well as in the scientific literature. A recent Israeli survey illustrated extensive variations in DIRs definition and management protocols.1 The aim of the current study is to provide a clear, easy-to-follow, stepwise approach to the therapeutic management of DIRs.
Methods
A questionnaire comprising open questions on the management of DIRs was sent to 18 physicians highly experienced with soft-tissue filler injections in 10 countries. The research questionnaire was approved by the Tel Aviv Medical Center institutional review board in accordance with the principles of the Declaration of Helsinki and the participants’ consent was provided in a written form. The first questions focused on demographic data, including the responders’ specialties, number of years they had been performing HA-based filler injections, number of 1 mL syringes used per week, and the average number of DIRs they encountered in a year. The second part of the questionnaire aimed at assessing their approach to DIRs management. The physicians were asked to specify treatment options, including oral antibiotics, oral corticosteroids, intralesional (IL) corticosteroids, non-steroidal anti-inflammatory drugs (NSAIDs), IL hyaluronidase, IL 5-fluorouracil (5-FU), topical therapy with a corticosteroid or calcineurin inhibitor, laser therapy, and excision. They were also asked to provide the exact name of the drug/drug combination, dose, and duration of treatment, and to add any pearls and tips they would recommend. Finally, they were asked to propose a stepwise, easy-to-follow algorithm containing specific first-line and second-line recommendations. The last three questions dealt with recurrent DIR episodes, subsequent filler injections following such reactions, as well as precautions taken to avoid DIRs.
Results
Eighteen physicians including 14 dermatologists, 1 plastic surgeon and 3 aesthetic physicians responded to the questionnaire. Missing data or information were filled-in by direct correspondence to the specific physicians. The average number of years of experience with HA-based filler injections was 17.88 ± 5.86 (range: 7–29). The average number of injected HA-filled 1 mL syringes per week was 46.83 ± 25.43 (range: 15–90). The average number of DIRs per year was 6.94 ± 4.59 (range: 2–15).
Table 1 provides a summary of the panelists’ questionnaire answers. Sixteen out of the 18 expert panelists agreed that antibiotics should be given as first-line therapy, and 11 of them believed that dual antibiotic therapy should be used, whereas five favored monotherapies. Among those who preferred monotherapy, the antibiotic of choice was a tetracycline, a macrolide, or a fluoroquinolone. Those antibiotics were chosen due to their broad-spectrum activity as well as their anti-inflammatory properties. Moreover, panelists who supported the use of one antibiotic regarded dual antibiotic therapy as more likely to cause pseudomembranous colitis. First-line antibiotic monotherapy treatment regimens included doxycycline 100 mg daily for 1 month, minocycline 100 mg daily for 2–4 weeks, azithromycin 500 mg TID for 3–6 weeks, or amoxicillin/clavulanic acid 875 mg BID for 2–4 weeks. Of note, three responders emphasized the concomitant use of probiotics when they prescribed long-term antibiotic treatment. Furthermore, three physicians rejected the use of clindamycin or amoxicillin/clavulanic acid based on the risk of developing bacterial resistance. Panelists who supported the use of dual antibiotic therapy recommended combining a fluoroquinolone (ie, ciprofloxacin) with either a tetracycline (ie, minocycline) or a macrolide (ie, clarithromycin, azithromycin). Fluoroquinolones, macrolides, and tetracyclines were recommended due to their anti-inflammatory properties. First-line dual antibiotic treatment approaches included a regimen of ciprofloxacin 500 mg BID + minocycline 100 mg daily or clarithromycin 500 mg BID for 3–6 weeks, or azithromycin 500 mg daily for 3 days per week (and 4 days off) in conjunction with levofloxacin 500 mg daily for 5 days per week (and 2 days off) for a period of 3–6 weeks. One of the panelists recommended first-line dual antibiotic therapy consisting of a 14-day course of clindamycin (300 mg TID) with ciprofloxacin (500 mg BID). One of the panelists did not support the use of fluoroquinolones based on the risk of tendon rupture as well as on the evidence in recent reports of rupture of aortic aneurysms.26.
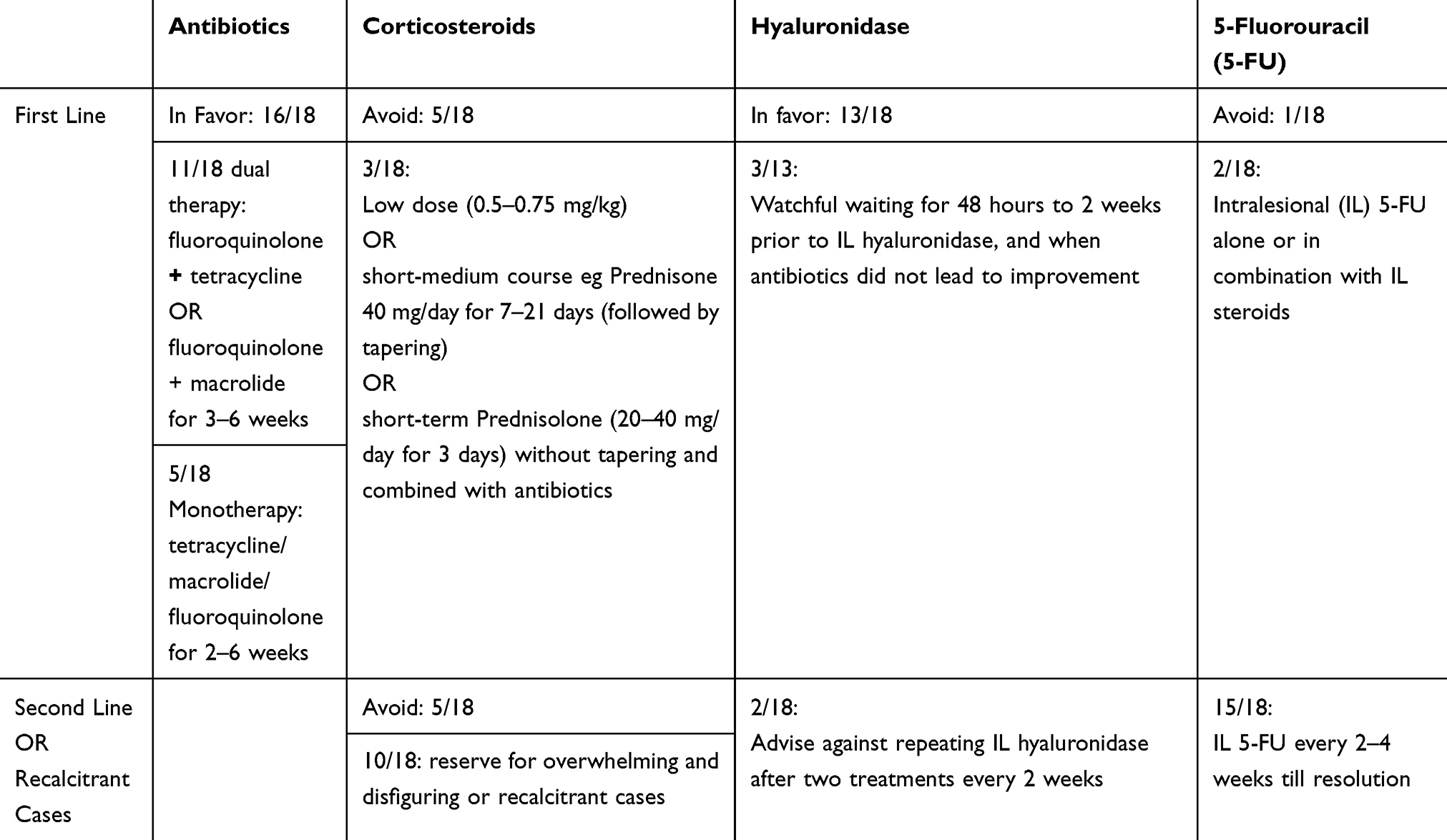 |
Table 1 Panelist Survey Response Summary |
Systemic corticosteroid treatment of DIRs stirred considerable debate among the panelists. Five of the 18 participating physicians advised avoiding the use of corticosteroids altogether in the treatment of DIRs. Masking of symptoms, rebound of infection upon discontinuation of corticosteroids, dependence upon systemic corticosteroid use, as well as the well-documented side effects of systemic corticosteroids were the reasons most cited. Only three panelists supported treatment with a low-dose (0.5–0.75 mg/kg) or a short-medium course of systemic corticosteroid as first-line therapy (eg, a course of prednisone 40 mg daily for 7–21 days followed by tapering). Ten panelists considered that the role of systemic corticosteroids in the management of DIRs depended on the severity and the extent of the inflammatory reaction and reserved the use of corticosteroids to overwhelming and disfiguring inflammatory reactions or for recalcitrant cases. One panelist favored only short-term use of 20–40 mg prednisolone for 3 days with no tapering but in combination with antibiotics. Eleven of the physicians agreed that the use of gastric protectors (H2-blockers or proton pump inhibitors) was indicated when administering systemic corticosteroid therapy.
IL 5FU alone or in combination with IL corticosteroids as first-line therapy was supported by two of the panelists, one panelist rejected their use, and the remaining 15 recommended their use every 2–4 weeks until resolution for recalcitrant cases. The use of IL hyaluronidase for soft-tissue filler removal as first-line therapy was favored by 13 of the 18 panelists. However, three of those 13 advised watchful waiting from 48 hours to 14 days prior to the injection of hyaluronidase and to use it only when the initial course of antibiotics did not lead to improvement. Two panelists stated they would not repeat IL hyaluronidase injections more than twice every 2 weeks. Those in favor of using hyaluronidase reasoned that its use would help break down the cluster of hyaluronic acid and the surrounding inflammatory matrix in order to potentially increase the efficacy of the antibiotic therapy. Five panelists refrained from the use of IL hyaluronidase as first-line therapy in order to maintain the benefit of the soft-tissue filler. The hyaluronidase dosage was also an issue of debate among the panelists. Ten panelists recommended the use of 50–250 units or more if needed, depending upon the size and number of the DIRs, whereas five advised using 30 units of hyaluronidase only 24–48 hours after commencing antibiotic therapy.
Sixteen panelists agreed that they would treat recurrent episodes in the same manner as they would an initial episode. Four panelists suggested switching from antibiotics to systemic corticosteroids in the event of a relapsing episode.
Discussion
The incidence of adverse events has escalated in parallel to the continuing rise in popularity of soft-tissue filler procedures. Different HA-based fillers are associated with different incidences of DIRs. Recent reports in the literature have revealed an incidence of DIRs to Juvederm Volbella of 1.0% per patient and 0.8% per syringe, which is higher than the previously reported incidence of 0.02%,2 and more compatible with the 4.25% incidence of DIRs to Juvederm Volbella reported by Artzi et al.3 It is has been speculated that HA-based fillers with a low-molecular weight-degraded products have higher proinflammatory activity.4
DIRs following HA-based filler injections manifest as discoloration (most commonly as erythema), painful nodules, induration or tissue hardening, and solid edema.5,6 In past publications, “late” reactions were mostly defined as the ones occurring 14 days to 1-year post-injection, whereas “delayed” complications were those occurring 1 year or longer after treatment.7–14 To clearly differentiate between early and delayed reactions, the panel recommended that delayed and late-onset reactions should be considered as one entity under the term delayed inflammatory reactions (DIRs), because their cause is usually not well defined and, more importantly, the initial treatment is similar regardless of etiology. Notably, a DIR arises from a quiescent state 2–4 weeks or longer post-injection.
It is unclear whether DIRs should be considered as true “hypersensitivity” reactions. As such, the panel strongly supported an infectious etiology or trigger, and rejected the word “hypersensitivity” in the context of DIRs.
Triggers that might be associated with the onset of DIRs include viral infection, active sinusitis, low-quality products, combinations of different products, improper technique, past and current dental procedures.8,15
Diagnostic tests to guide the management of delayed-onset nodules have been proposed in the literature by numerous authors. Most of them support the initial need to rule out a fluctuant nodule that requires incision and drainage of content to be sent for aerobic and anaerobic bacterial, mycobacterial, and fungal cultures before initiating any treatment.7,16–18 Of note, the lab must be informed of any suspicion of a mycobacterial process since it can be more challenging to grow and often requires longer culture periods. Polymerase chain reaction (PCR), fluorescent in-situ hybridization, and electron microscopy of tissue specimens may be contributory in establishing the infectious agent.19 A biopsy and tissue culture should be obtained if there is no resolution following treatment.8,16,17,19 Ultrasound imaging is considered as diagnostic “gold standard” in several publications,10 based on its abilities to specify the exact location of delayed-onset nodules in relation to other structures, as well as to demonstrate the density of the filler composition. Blood tests for evaluating inflammatory markers, such as C-reactive protein, have also been suggested.8
There are numerous treatment options for DIRs,8,20 however, stepwise algorithmic approaches for the management of DIRs are lacking. The treatment modalities most frequently described are antibiotic therapy, IL or oral corticosteroids, and hyaluronidase injections. According to the literature, the first-line treatment of choice is antibiotics,7,13,16–22 and the use of dual or triple antibiotic therapy is favored.7,13,18–21 Several authors recommend combining therapy with broad-spectrum antibiotics (ie, fluoroquinolones) and a macrolide, such as clarithromycin,7,17–21 to be taken over a period of several weeks. Macrolides are considered especially effective due to their ability to restrain quorum sensing along with their ability to accumulate in adipose tissue, bearing in mind that fillers are mostly located in fat.18 Other reported regimens included clarithromycin 500 mg and moxifloxacin 400 mg BID for 10 days, ciprofloxacin 500–750 mg BID for 2–4 weeks, or minocycline 100 mg daily for 6 months.16 Antibiotic treatment should be based on results of cultures, and a macrolide may be considered for 2–4 weeks in the event that no laboratory diagnosis has been reached. Other first-line options include IL hyaluronidase,12,18,19 IL steroids,5,22 or the combination of both.5,18,22,23 Hyaluronidase enables the bond between C4 of the glucuronic acid and C1 of the glucosamine to disintegrate, whereupon the HA undergoes hydrolysis.24 It is usually recommended to initiate treatment with five units of hyaluronidase. The dose should be doubled in more resistant fillers (eg, the Vycross family by Juvederm).25,26 The IL hyaluronidase dosage recommended by a consensus group,17 is 10–20 U single injection for an area <2.5 mm, and 2–4 injection points with a 10–20 U per injection point for areas from 2.5 mm to 1 cm in size. Repeated injections may be necessary in both cases, and higher doses will be required in resistant cases.12
The most popular choice for second-line therapy is IL steroids.12,13,16–21,23 To further reduce the number of complications secondary to IL steroids as well as temporary skin atrophy, many authors have suggested reconstitution of steroids with other agents, such as 5-FU, lidocaine, or saline. Alternative options for second-line treatments are antibiotic therapy,12,23 IL hyaluronidase,7,16,17 IL 5-FU,22,23 radiofrequency therapy,18,21 laser therapy,21,23 human platelet-rich plasma,12 or extraction of the material with a 16-gauge needle and a syringe while applying negative pressure.22 Surgical excision of nodules was considered only as a last resort by many,7,13,16,17,21,22,24 especially when a granuloma is suspected.12,18,21
Panel Recommendations
This panel has proposed the following therapeutic approach for a DIR. The treating physician must first consider whether the nodules that appear after HA-based filler injections are likely to improve spontaneously, are small in size with no or minimal pain, or, alternatively, if they are relatively large (usually >0.5 cm), not improving, painful, edematous, and erythematous. The former call for a watchful waiting approach, whereas the latter are considered true DIRs and require intervention. It should be considered that small and short-lived edematous nodules are frequently observed in conjunction with or following a brief illness (eg, viral infections or post-dental procedures) and tend to heal spontaneously.
The second step in the evaluation of a DIR is to consider the presence or absence of fluctuation on palpation. A soft-tissue ultrasound study should be performed for fluctuant nodules, along with incision and drainage. The aspirants should be cultured. Once fluctuation has been ruled out, the first-line treatment of DIRs should consist of antibiotics. The expert panel has divided opinions regarding the appropriate antibiotic regimen, but the majority favor dual antibiotic treatment consisting of a fluoroquinolone (eg, ciprofloxacin 500 mg BID) with either a tetracycline (eg, doxycycline or minocycline 100 mg/day) or a macrolide (eg, clarithromycin 500 mg BID) for a period of 3–6 weeks. Importantly, patients must be informed about a recent correlation that had been found between ciprofloxacin and aortic aneurysms.27 Additionally, ciprofloxacin should not be taken with dairy products, and probiotic treatment is highly recommended in order to prevent Clostridium difficile infections resulting from the long duration of antibiotic use.28 Furthermore, five of the participating experts recommend avoiding the use of amoxicillin/clavulanic acid or clindamycin for the treatment of DIRs, except in the case of oral cavity or dental-associated infections.
Dissolution of a filler by means of IL hyaluronidase may be postponed by 24 hours to 2 weeks after starting the antibiotic treatment, unless a more resistant HA (ie, Vycross) has been injected, in which case IL hyaluronidase must be given as early as possible. A dose of 30–300 units of IL hyaluronidase should be given per nodule. A fine needle with a low gauge (ie, 18 or 21G) is preferred in order to disrupt an encapsulated (filler) organization by allowing for more penetrations. Subsequent dissolution via IL hyaluronidase with increasing dosages should be repeated after 2–3 weeks; however hyaluronidase injections should be limited to 2–3 cycles.
Intralesional steroids alone or combined with 5-FU and saline/lidocaine may be considered for second-line therapy. A low dose of IL corticosteroids should be used to prevent atrophy. The panel recommends the use of a combination of IL triamcinolone (10–20 mg/mL), 5-FU, and saline or lidocaine 1% in a 1:1:1 ratio. It also emphasizes the need for caution when injecting IL corticosteroids into periorbital lesions.
Most participating experts recommended refraining from the use of systemic corticosteroids, with the exception of cases of extremely inflammatory or disfiguring edema and recalcitrant nodules. When oral steroids are prescribed, a low-to-moderate dose and a short-to-medium-term regimen is recommended (ie, 0.5–0.75 mg/kg/day for 7–21 days with tapering).
To the best of our knowledge, the current literature does not address the issues of how a physician should approach recurrent DIRs or the risk of developing recurrent DIRs. This led the panel to address two additional questions that physicians may encounter in their daily practice. The first is whether physicians should choose a different therapeutic scheme if a patient returns with a recurrent episode several months after a previous episode has subsided. The second concern how one should pursue future injections: for example, should the same filler technology or brand be used at the same site of injection, and how long should the interval be in relation to the initial reaction? In response to the first question, 16 of the 18-panel members agreed that they would treat recurrent episodes in the same manner as they would an initial episode. Three of them, however, stated that they would make minor adjustments, such as initiating treatment with steroids, increasing the IL hyaluronidase dosage, or using a mixture of IL steroids/5FU/lidocaine. In response to the second question, the panel unanimously agreed they would perform future injections, but with the caveat of opting for a different HA filler technology or a non-HA filler, such as calcium hydroxyapatite, while three panelists opted for the use of fat transfer instead. The recommended waiting time before performing another injection was 3 months to 1-year post-remission in areas other than those where a DIR had occurred, along with performing the procedure with concomitant steroid therapy. Eight panelists advised using smaller quantities of HA and not exceeding a total of 1 cc or more than 0.1 cc per test site for first re-injection post DIR.
Conclusion
There is a multitude as well as a wide diversity of opinions regarding the management of DIRs in the literature. Our panel emphasizes the need to establish an easy-to-follow and uniform algorithm (Figure 1) for the injecting physician who encounters a DIR.
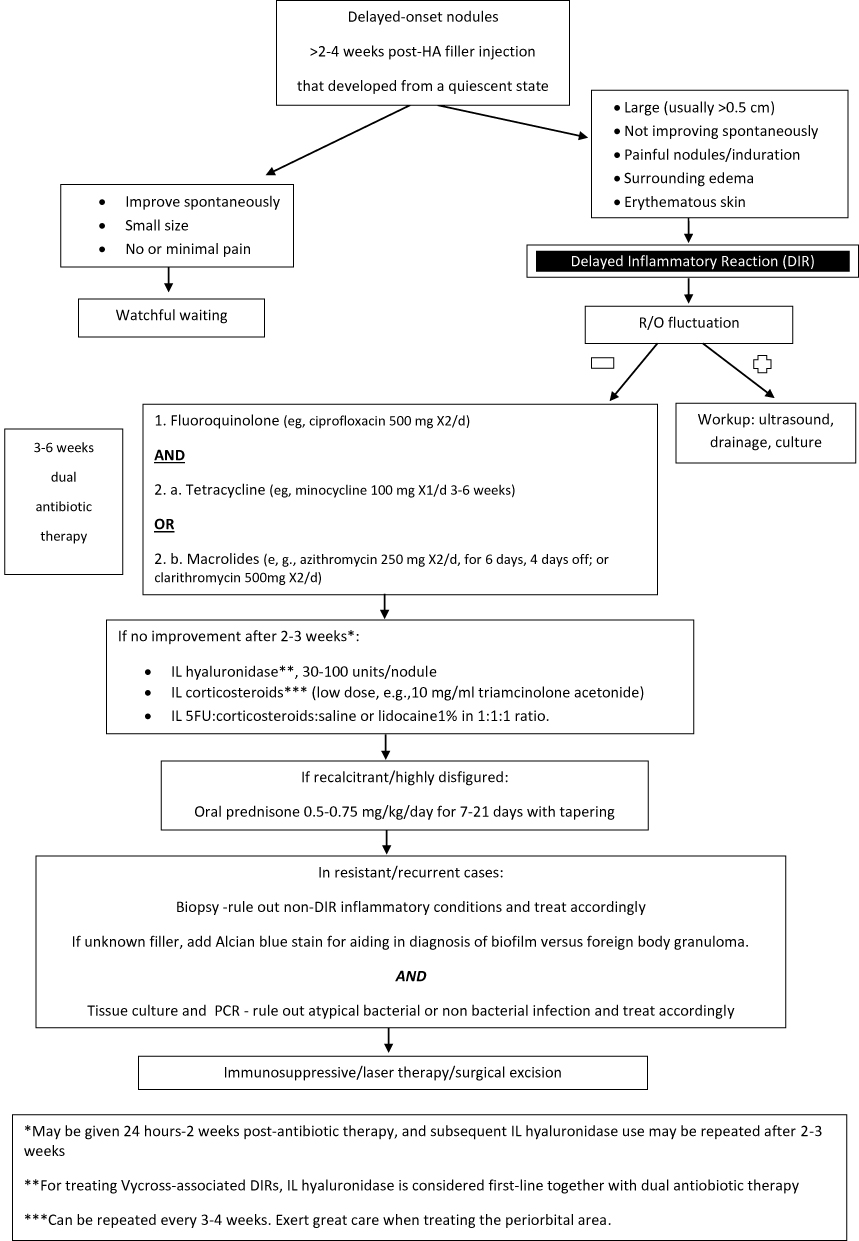 |
Figure 1 Algorithm for treating DIRs secondary to HA filler injections. |
Disclosure
Joel L. Cohen, MD has served as a clinical trial participant and/or consultant for Allergan, Galderma, Merz. He reports personal fees from Allergan, grants, personal fees from Galderma, Merz, Revance, and CROMA, during the conduct of the study. Jeffrey S. Dover, MD has served as a consultant and conducted research funded by Allergan, Galderma, Sunera, Merz. Daniel Cassuto, MD is a speaker and trainer for IBSA and MATEX LAB. Vivian Bucay, MD is a speaker and consultant for Allergan, Galderma, and Merz. Tingsong Lim MD is a speaker and trainer for Allergan CoolSculpting, Merz Aesthetics, Sinclair Pharma and Teoxane. Sonja Sattler, MD reports personal fees from Pharm Allergan, MERZ Aesthetics, and CROMA, as a speaker or in research projects, outside the submitted work. Tanja Fischer reports grants from Merz, Croma, Riemser, and PromoItalia, outside the submitted work. Tatjana Pavicic reports personal fees from and is a speaker and consultant for Merz Aesthetics and AAT, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Shalmon D, Cohen J, Landua M, Verner I, Sprecher E, Artzi O. Management of delayed inflammatory reactions to hyaluronic acid fillers: an online survey in Israel. In press 2020.
2. Sadeghpour M, Quatrano NA, Bonati LM, Arndt KA, Dover JS, Kaminer MS. Delayed-onset nodules to differentially crosslinked hyaluronic acids: comparative incidence and risk assessment. Dermatol Surg. 2019;45(8):1085–1094. doi:10.1097/DSS.0000000000001814
3. Artzi O, Loizides C, Verner I, Landau M. Resistant and recurrent late reaction to hyaluronic acid–based gel. Dermatol Surg. 2016;42(1):31–37. doi:10.1097/DSS.0000000000000562
4. Farwick M, Gauglitz G, Pavicic T, et al. Fifty-kDa hyaluronic acid upregulates some epidermal genes without changing TNF-α expression in reconstituted epidermis. Skin Pharmacol Physiol. 2011;24(4):210–217. doi:10.1159/000324296
5. Lemperle G, Rullan PP, Gauthier-Hazan N. Avoiding and treating dermal filler complications. Plast Reconstr Surg. 2006;118(3S):92S–107S. doi:10.1097/01.prs.0000234672.69287.77
6. Kim H, Cho SH, Lee JD, Kim HS. Delayed onset filler complication: two case reports and literature review. Dermatol Ther. 2017;30(5):e12513. doi:10.1111/dth.12513
7. Rohrich RJ, Monheit G, Nguyen AT, Brown SA, Fagien S. Soft-tissue filler complications: the important role of biofilms. Plast Reconst Surg. 2010;125(4):1250–1256.
8. Beleznay K, Carruthers JD, Carruthers A, Mummert ME, Humphrey S. Delayed-onset nodules secondary to a smooth cohesive 20 mg/mL hyaluronic acid filler: cause and management. Dermatol Surg. 2015;41(8):929–939. doi:10.1097/DSS.0000000000000418
9. Monheit GD, Rohrich RJ. The nature of long-term fillers and the risk of complications. Dermatol Surg. 2009;35:1598–1604. doi:10.1111/j.1524-4725.2009.01336.x
10. Cassuto D, Sundaram H. A problem-oriented approach to nodular complications from hyaluronic acid and calcium hydroxylapatite fillers: classification and recommendations for treatment. Plast Reconst Surg. 2013;132(4S–2):48S–58S.
11. Alsaad SM, Fabi SG, Goldman MP. Granulomatous reaction to hyaluronic acid: a case series and review of the literature. Dermatol Surg. 2012;38(2Part 1):271–276. doi:10.1111/j.1524-4725.2011.02214.x
12. Urdiales-Gálvez F, Delgado NE, Figueiredo V, et al. Treatment of soft tissue filler complications: expert consensus recommendations. Aesth Plast Surg. 2018;42(2):498–510. doi:10.1007/s00266-017-1063-0
13. Narins RS, COLEMAN III WP, Glogau RG. Recommendations and treatment options for nodules and other filler complications. Dermatol Surg. 2009;1(35):1667–1671. doi:10.1111/j.1524-4725.2009.01335.x
14. Lemperle G, Gauthier-Hazan N. Foreign body granulomas after all injectable dermal fillers: part 2. Treatment options. Plast Reconst Surg. 2009;123(6):1864–1873. doi:10.1097/PRS.0b013e3181858f4f
15. De Boulle K, Heydenrych I. Patient factors influencing dermal filler complications: prevention, assessment, and treatment. Clin Cosmet Invest Dermatol. 2015;8:205. doi:10.2147/CCID.S80446
16. Chiang YZ, Pierone G, Al‐Niaimi F. Dermal fillers: pathophysiology, prevention and treatment of complications. J Eur Acad Dermatol Venereol. 2017;31(3):405–413. doi:10.1111/jdv.13977
17. Signorini M, Liew S, Sundaram H, et al. Global aesthetics consensus: avoidance and management of complications from hyaluronic acid fillers—evidence-and opinion-based review and consensus recommendations. Plast Reconst Surg. 2016;137(6):961. doi:10.1097/PRS.0000000000002184
18. Hartmann D, Ruzicka T, Gauglitz GG. Complications associated with cutaneous aesthetic procedures. J Dtsch Dermatol Ges. 2015;13(8):778–786.
19. Ibrahim O, Overman J, Arndt KA, Dover JS. Filler nodules: inflammatory or infectious? A Review of biofilms and their implications on clinical practice. Dermatol Surg. 2018;44(1):53–60. doi:10.1097/DSS.0000000000001202
20. Snozzi P, van Loghem JA. Complication management following rejuvenation procedures with hyaluronic acid fillers—an algorithm-based approach. Plas Reconst Surg Glob Open. 2018;6(12).
21. Kulichova D, Borovaya A, Ruzicka T, Thomas P, Gauglitz GG. Understanding the safety and tolerability of facial filling therapeutics. Expert Opin Drug Saf. 2014;13(9):1215–1226. doi:10.1517/14740338.2014.939168
22. Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol. 2013;6:295.
23. Ozturk CN, Li Y, Tung R, Parker L, Piliang MP, Zins JE. Complications following injection of soft-tissue fillers. Aesthet Surg J. 2013;33(6):862–877. doi:10.1177/1090820X13493638
24. Rohrich RJ, Ghavami A, Crosby MA. The role of hyaluronic acid fillers (Restylane) in facial cosmetic surgery: review and technical considerations. Plast Reconst Surg. 2007;120(6S):41S–54S. doi:10.1097/01.prs.0000248794.63898.0f
25. Jones D, Tezel A, Borrell M. In vitro resistance to degradation of hyaluronic acid dermal fillers by ovine testicular hyaluronidase. Dermatol Surg. 2010;36:804–809. doi:10.1111/j.1524-4725.2010.01550.x
26. Vartanian AJ, Frankel AS, Rubin MG. Injected hyaluronidase reduces restylane-mediated cutaneous augmentation. Arch Facial Plast Surg. 2005;7(4):231–237. doi:10.1001/archfaci.7.4.231
27. Pasternak B, Inghammar M, Svanström H. Fluoroquinolone use and risk of aortic aneurysm and dissection: nationwide cohort study. BMJ. 2018;360:k678. doi:10.1136/bmj.k678
28. Madoff SE, Urquiaga M, Alonso CD, Kelly CP. Prevention of recurrent Clostridioides difficile infection: a systematic review of randomized controlled trials. Anaerobe. 2020;61:102098.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.