")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Delayed Inflammatory Reactions After Hyaluronic Acid Filling of Neck Lines: A Case Report
Authors Li Z , Zhao P, Xu Q, Bi J , Huo R
Received 28 October 2022
Accepted for publication 23 December 2022
Published 14 January 2023 Volume 2023:16 Pages 99—102
DOI https://doi.org/10.2147/CCID.S394141
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Zhiyu Li,1 Pu Zhao,2 Qing Xu,3 Jianhai Bi,1,4,5,* Ran Huo1,4,5,*
1Department of Plastic and Aesthetic Surgery, Shandong Provincial Hospital, Cheeloo College of Medicine, Shandong University, Jinan, Shandong Province, People’s Republic of China; 2Department of Plastic Surgery, Liaocheng Hospital of Traditional Chinese Medicine, Liaocheng, People’s Republic of China; 3Department of Plastic and Aesthetic Surgery, Maternity and Child Health Care of Zaozhuang, Zaozhuang, People’s Republic of China; 4Department of Plastic and Aesthetic Surgery, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, People’s Republic of China; 5Medical Science and Technology Innovation Center, Shandong First Medical University & Shandong Academy of Medical Sciences, Jinan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianhai Bi; Ran Huo, Email [email protected]; [email protected]
Abstract: The incidence of adverse events after hyaluronic acid filling is gradually increasing. In addition to acute reactions in the early postoperative period, there have been some cases of delayed inflammatory reactions. However, such events are rarely reported in Asia, which may be due to atypical symptoms, long intervals, and misidentification of the product quality. Herein, we present a case in which erythema of the neck appeared three weeks after hyaluronic acid injection into the neck lines and a delayed inflammatory reaction was diagnosed. Watchful waiting was performed, and the erythema subsided spontaneously after two weeks. This case suggests that in patients with a history of hyaluronic acid injections who develop allergic and inflammatory reactions after an interval, it is important to consider whether the reaction is a delayed inflammatory reaction, and if aggressive intervention is necessary.
Keywords: delayed inflammatory reactions, hyaluronic acid, neck lines, root canal, COVID-19 vaccination
Introduction
Hyaluronic acid (HA) is globally the second most common non-surgical aesthetic procedure after botulinum toxin. As such, complications from HA injections are increasing. Delayed inflammatory reactions (DIRs) are a relatively rare complication and often mistaken for common infections or not related to HA due to an insidious onset and diverse manifestations. Herein, we present a case of DIRs after HA injection three weeks. The patient developed transient erythema on the neck that spontaneously resolved within two weeks, which deserves our attention and consideration.
Case Presentation
A 30-year-old female patient had received a HA (Hearty 1.5; Imeik Technology Development Co., ltd., Beijing, China.) injection in the neck at a private clinic three weeks previously, with no adverse reactions. The patient suddenly noticed erythema on the neck (Figure 1A) but made no timely visits due to work commitments. We instructed the patient to take neck photographs daily (Figure 1B and C). The patient was treated with alcohol and erythromycin ointment which was applied externally and monitored daily. She visited our hospital on the fourth day. The patient reported a previous HA (Restylane; Q-Med AB, Uppsala, Sweden) injection in the chin at a private clinic five years ago, and that no adverse reactions had occurred within five years. Moreover, she had received the third dose of the COVID-19 vaccine (Changchun Institute of Biological Products Co., Ltd., Jilin, China) five months ago, and experienced no adverse reactions after the three vaccinations. A month ago, she reported having a fever due to cold and recovered within a few days. She had undergone root canal therapy 10 days prior, during which time minocycline ointment was used. Recently, she reported no exposure to special substances or local application of drugs. Physical examination revealed linear erythema on the neck with pruritus, which was soft and painless (Figure 1D). Ultrasonography (US) revealed no subcutaneous abnormalities. Blood tests revealed normal immunoglobulin E (IgE) levels and erythrocyte sedimentation rates. The patient was instructed to continue erythromycin ointment application. After two weeks, the erythema resolved spontaneously (Figure 1E–H). At follow-up after six months, the patient had no recurrence.
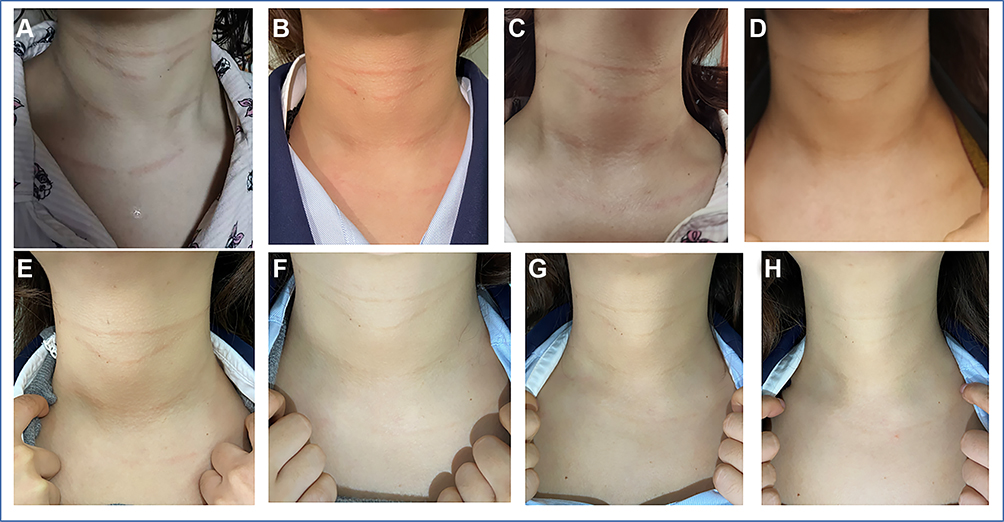 |
Figure 1 Changes in neck erythema in the patient. (A). Neck erythema on the 1st day; (B). Neck erythema on the 2nd day; (C). Neck erythema on the 3rd day; (D). Neck erythema on the 4th day; (E). Neck erythema on the 5th day; (F). Neck erythema on the Day 8; (G). Neck erythema on day 10; (H). Neck erythema on day 14. |
Discussion
DIRs caused by HA injection have been reported since the 1990s. However, only a few cases have been reported in China and Asia. Recently, two cases of DIRs after neck-line injections have been reported in China.1,2 Clinically, DIRs after HA injection manifest as discoloration, erythema, local tissue sclerosis, painful nodules, and edema. However, many cases are considered to be hypersensitivity reactions.3 Some scholars have defined the onset time of DIRs as reactions occurring 2–4 weeks or more after HA injection. While experts favored viral or bacterial infectious triggers, the term hypersensitivity was rejected in favor of inflammation for broader coverage, with prevalence ranging from 0.3% to 4.25%.4 Moreover, they reported other potential triggers for DIRs including previous or recent dental procedures, low-quality products, combinations of different products, active sinusitis, and inappropriate techniques.4,5
In this case, the patient had a fever a month ago, combined with root canal therapy ten days earlier, both of which may have induced DIRs. However, the patient had also been injected with HA 5 years prior and had fever or flu during this period without experiencing any abnormality. Therefore, we speculated that root canal therapy is more likely to cause DIRs. Although root canal therapy is currently recognized as a good method for the treatment of dental pulp and periapical diseases, it may also release toxins and bacteria, which can cause systemic diseases.6
Due to the particularity of neck-line injection, diagnosis is not easily influenced by other factors, thus indicating HA. However, in the event of an uncertain diagnosis or failed treatment attempts, the search for a definitive diagnosis is warranted, often requiring biopsies with histological examination, tissue cultures, and polymerase chain reaction analysis of tissue samples. Fluorescent in situ hybridization may also be used,7 and US is useful for clarifying the extent of the lesions.8 Blood tests, such as routine blood tests, total serum IgE, erythrocyte sedimentation rate, and C-reactive protein, are helpful to further clarify the diagnosis.9
In the three years since the global outbreak of COVID-19, more than ten cases of DIRs have been reported internationally. During a period ranging from 4 months to 3 years after HA filling, COVID-19 vaccination or COVID-19 infection resulted in DIRs at the filling site. DIRs can occur after the first COVID-19 vaccination and can present following the booster injection, despite the patients having been fine after the previous vaccination.10 Although the correlation and regularity between the vaccine and DIRs cannot be elucidated thus far, the time of onset of DIRs and time of vaccination are highly suggestive. These cases have drawn international attention and are yet to be reported in the Chinese population. In addition, there have been reports of DIRs following vaccination for rabies and tetanus.11 This event was not considered related to the vaccine as the vaccination time had exceeded 5 months, and no adverse events occurred in any of the three vaccinations. However, this case needs to be of concern to researchers in China, especially for patients who have not been filled with HA. Patients can consider filling after a sufficient period following vaccination to avoid DIRs. For such patients, oral administration of angiotensin-converting enzyme inhibitors may have unexpected efficacy; however, the safety and feasibility of this treatment requires further study.12
A relatively well-established treatment process for DIRs has been proposed by experts.13 For those with relatively mild symptoms that improve on their own, especially superficial ones, watchful waiting can be performed, as reported by Li et al1, and in this case. In contrast, for patients with more severe symptoms that do not subside, antibiotics, glucocorticoids, hyaluronidase, immunosuppressive agents, and surgical treatment can be used. Due to the rare incidence and reports of DIRs, symptoms may be mistaken for a general infection and treated too positively with medication. Some articles in China consider DIRs to be product-related and recommend positive use of antibiotics or glucocorticoids.14 Therefore, more studies are needed for the diagnosis and treatment of DIRs in the Chinese population.
Abbreviations
HA, Hyaluronic acid; DIRs, Delayed inflammatory reactions.
Informed Consent
The patient has signed the informed consent and agreed to publish it. She gave her consent for the publication of identifiable details, which can include photograph(s) and/or case history and/or details within the text to be published in the article.She confirmed that she have seen and been given the opportunity to read the article.
Consent for Publication
Approval for the publication of the patient’s case details was obtained from Shandong Provincial Hospital.
Acknowledgments
We would like to thank Editage for English language editing.
Funding
This work was supported by the Taishan Scholars(No.ts201511100).
Disclosure
Jianhai Bi and Ran Huo are co-correspondence authors for this study. The authors report no conflicts of interest in this work.
References
1. Li A, Fang R, Sun Q. Delayed inflammatory reactions to hyaluronic acid filler injection: should be treated but should not be overtreated. J Cosmet Dermatol. 2022;21:3625–3626. doi:10.1111/jocd.14924
2. Lai D, Liu H, Kong L, Cheng S. Delayed complication of botulinum toxin and hyaluronic acid filler injections: a case report. J Cosmet Dermatol. 2022;21:2374–2378. doi:10.1111/jocd.15016
3. Jordan DR. Delayed inflammatory reaction to hyaluronic acid (Restylane). Ophthalmic Plast Reconstr Surg. 2005;21:401–402. doi:10.1097/01.iop.0000173194.18050.b8
4. Michon A. Hyaluronic acid soft tissue filler delayed inflammatory reaction following COVID-19 vaccination - A case report. J Cosmet Dermatol. 2021;20:2684–2690. doi:10.1111/jocd.14312
5. Beleznay K, Carruthers JD, Carruthers A, Mummert ME, Humphrey S. Delayed-onset nodules secondary to a smooth cohesive 20 mg/mL hyaluronic acid filler: cause and management. Dermatol Surg. 2015;41:929–939. doi:10.1097/DSS.0000000000000418
6. Kulacz DR, Levy MD. The Toxic Tooth: How a Root Canal Could Be Making You Sick. Nevada(NV): Medfox Publishing; 2014.
7. Ibrahim O, Overman J, Arndt KA, Dover JS. Filler nodules: inflammatory or infectious? A review of biofilms and their implications on clinical practice. Dermatol Surg. 2018;44:53–60. doi:10.1097/DSS.0000000000001202
8. Cassuto D, Sundaram H. A problem-oriented approach to nodular complications from hyaluronic acid and calcium hydroxylapatite fillers: classification and recommendations for treatment. Plast Reconstr Surg. 2013;132:48S–58S. doi:10.1097/PRS.0b013e31829e52a7
9. Wu L, Liu X, Jian X, et al. Delayed allergic hypersensitivity to hyaluronidase during the treatment of granulomatous hyaluronic acid reactions. J Cosmet Dermatol. 2018;17:991–995. doi:10.1111/jocd.12461
10. Munavalli GG, Guthridge R, Knutsen-Larson S, Brodsky A, Matthew E, Landau M. COVID-19/SARS-CoV-2 virus spike protein-related delayed inflammatory reaction to hyaluronic acid dermal fillers: a challenging clinical conundrum in diagnosis and treatment. Arch Dermatol Res. 2022;314:1–15. doi:10.1007/s00403-021-02190-6
11. Sarigul GS. A case of delayed inflammatory filler reaction following vaccination with successful response to colchicine. J Cosmet Laser Ther. 2021;23:52–54. doi:10.1080/14764172.2021.1967997
12. Munavalli GG, Knutsen-Larson S, Lupo MP, Geronemus RG. Oral angiotensin-converting enzyme inhibitors for treatment of delayed inflammatory reaction to dermal hyaluronic acid fillers following COVID-19 vaccination-a model for inhibition of angiotensin II-induced cutaneous inflammation. JAAD Case Rep. 2021;10:63–68. doi:10.1016/j.jdcr.2021.02.018
13. Artzi O, Cohen JL, Dover JS, et al. Delayed inflammatory reactions to hyaluronic acid fillers: a literature review and proposed treatment algorithm. Clin Cosmet Investig Dermatol. 2020;13:371–378. doi:10.2147/CCID.S247171
14. Aesthetic Injection Subcommittee of Chinese Dermatology Association. Consensus recommendations from Chinese expert for preventing and treating hyaluronic acid filler induced adverse effects. J Clin Dermatol. 2019;48:518–521.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.