")
Back to Journals » Infection and Drug Resistance » Volume 15
Delayed Clearance of Viral RNA in Sputum for Severity COVID-19 Patients with Initial High Viral Load
Authors Zhao H , Tu H, Yu X, Su J, Zhang X, Xu K, Shi Y, Qiu Y , Sheng J
Received 12 December 2021
Accepted for publication 1 April 2022
Published 20 April 2022 Volume 2022:15 Pages 1971—1979
DOI https://doi.org/10.2147/IDR.S353688
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Hong Zhao,* Huilan Tu,* Xia Yu,* Junwei Su, Xuan Zhang, Kaijin Xu, Yu Shi, Yunqing Qiu, Jifang Sheng
State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, National Medical Center for Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jifang Sheng; Yunqing Qiu, State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, National Medical Center for Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310003, People’s Republic of China, Tel +86 571 8723 6491, Fax +86 571 8723 6491, Email [email protected]; [email protected]
Aim: To analyze the possible risk factors of delayed virus clearance in hospitalized patients with coronavirus disease 2019 (COVID-19).
Methods: Retrospective analysis of patients with COVID-19 admitted to the isolation wards from our hospital from 19th Jan 2020 to 18th March 2020. We were collected patient’s data including demographic, epidemiologic, and clinical information, as well as laboratory and radiologic findings. The possible confounding risk factors for prolonged viral RNA shedding of COVID-19 during hospitalization were explored by univariate analysis and any variables with a p value less than 0.05 after univariate analysis were included in a subsequent multivariate logistic regression model analysis.
Results: The 104 patients included 30 mild patients and 74 severe or critically ill patients. The median duration of viral RNA positivity in sputum was 11 days, and the longest duration of viral RNA positivity was 49 days after admission. Multivariate analysis shown that the used with darunavir/cobicistat treatment (odds ratio [OR]: 4.25, 95% confidence interval [CI]: 1.25– 14.42, p = 0.020), duration of fever (OR: 1.15, 95% CI: 1.03– 1.30, p = 0.015) and time to radiological improvement (OR: 1.14, 95% CI: 1.01– 1.30, p = 0.033) were associated with delayed clearance of SARS-CoV-2 in sputum from COVID-19 patients. Then adjusted in the multivariate binary logistic regression analysis model in severe COVID-19 and found that critical COVID-19 patients (OR: 13.25, 95% CI: 1.45– 12.07, p = 0.022), lower virus cycle threshold (CT) values of RT-PCR (OR: 0.96, 95% CI: 0.93– 0.99, p = 0.004) and used with darunavir/cobicistat treatment (OR: 8.44, 95% CI: 2.21– 32.28, p = 0.022) were associated with delayed clearance of SARS-CoV-2 in sputum from COVID-19 patients.
Conclude: Clearance of viral RNA in sputum was delayed in severe COVID-19 patients, especially with lower virus CT value. And antivirals with darunavir/cobicistat has little advantage in eliminating SARS-CoV-2.
Keywords: COVID-19, SARS-CoV-2, clearance, critical disease, viral load
Introduction
The coronavirus disease 2019 (COVID-19) has been controlled, however, sporadic cases are still reported in China.1–3 Meanwhile, even if imposing stringent controls and promotion of vaccination among all the world, according to WHO reported as of 6 December, more than 2021, 265 million confirmed cases of COVID-19 and more than 5.2 million deaths.
As we known that sputum SARS-CoV-2 viral higher load and diseases severity correlates with risk of COVID-19 progression.4–6 And viral shedding has been reported to persist 12 days in COVID-19 patients; however, viral shedding varies greatly among individuals, with the longest duration reported to be 25 days.7,8 A recent study reported no difference in the temporal profiles of viral load in saliva samples between patients with mild and severe disease, but only 23 patients were enrolled and the viral loads are generally higher in the lower respiratory tract.8 But there are little analyzed about the risk factors of delayed clearance of viral RNA in sputum of patients with COVID-19.
To clarify the issue, we performed a retrospective, observational cohort study consisting of patients admitted in our center to analyze these possible influencing factors of virus clearance in sputum or throat swabs of hospitalized COVID-19.
Patients and Methods
Patient
All patients with confirmed COVID-19 were retrospectively enrolled from 19th Jan 2020 to 18th March 2020 in our center. COVID-19 was diagnosed with positive of severe acute respiratory syndrome- coronavirus - 2 (SARS-Cov-2) nucleic acid on sputum specimens from the lower respiratory tract or throat swab samples after deep cough. Viral RNA was defined as negative if absent in two consecutive tests over a 24-h interval.
Mild, severe and critically ill COVID-19 patients were defined as previously described:9 Mild ill COVID-19 was defined with the patients with clinical symptoms mild and respiratory symptoms with radiological findings of pneumonia. Severe ill COVID-19 was defined with patients meeting any of the following criteria: Respiratory distress (≥30 breaths/min); Oxygen saturation ≤93% at rest; Arterial partial pressure of oxygen (PaO2)/fraction of inspired oxygen (FiO2) ≤ 300 mmHg (1mmHg = 0.133 kPa). Patients with chest imaging that shows obvious lesion progression within 24–48 hours >50% shall be managed as severe cases. And critically ill COVID-19 was defined with patients with any of the following criteria: respiratory failure and requiring mechanical ventilation, shock or with another organ failure that requires ICU care. We performed a subgroup analysis grouping by different disease severity groups. All hospitalized participants received a standard treatment based on the New Coronavirus Pneumonia Prevention and Control Program (7th edition).9
The study was approved by the Ethics Committee of the First Affiliated Hospital of Zhejiang University School of Medicine (No: 2020-IIT-39) and was conducted in compliance with the “Ethical Principles for Medical Research Involving Human Subjects” of the Helsinki Declaration. All study participants or their legal representatives provided informed consent.
SARS-CoV-2 Testing
The presence of SARS-CoV-2 viral RNA was determined using real-time polymerase chain reaction (RT-PCR), as previously described.6 And the presence of viral RNA of SARS-Cov-2 in sputum samples was indicated by the cycle threshold (CT) values of RT-PCR assays as previously described.4,6 The tests were performed daily in sputum or throat swab samples after deep cough. Sputum will be tested if the patient could produce sputum, and others were tested with throat swab samples after deep cough.
Data Collection
Data of patients diagnosed with COVID-19 admitted to the isolation wards from our hospital were collected including demographic, epidemiologic, and clinical information, as well as laboratory and radiologic findings. All the data was reviewed medical records and input into a prespecified electronic data sheet. Two experienced radiologists of our hospital reviewed the chest computed tomography (CT) testing and radiographic features of chest CT were described as lobar, unilateral, bilateral, GGO, consolidation and interstitial changes. Two doctors reviewed the data from electronic medical record in order to ensure concordance. Some data would be confirmed through communication with patients if the data was not clear.
Statistical Analyses
SPSS software for Windows version 26.0 (SPSS Inc, Chicago, IL) was used to analyze the data. Continuous variables were represented as mean ± standard deviations (SD), median with inter-quartile. And nominal variables were expressed as number (percentage). The differences between two groups of all potential factors were assessed with univariate analyses, using Chi-square, Student’s t test or Mann–Whitney U-test. The multivariable logistic regression analysis was performed to identify risk factors associated with prolonged viral RNA shedding of COVID-19. The possible confounding risk factors for prolonged viral RNA shedding of COVID-19 during hospitalization were explored by univariate analysis and any variables with a p value less than 0.05 after univariate analysis were included in a subsequent multivariate logistic regression model analysis. Then, we adjusted the multivariate logistic regression analysis model including sex(male), age, history of hypertension, diabetes, leukocyte count increased, lymphocyte decreased, creatinine increased, lower virus CT values (less than 25), time to radiological improvement delay (longer median 9 days), treated with glucocorticoid, glycyrrhizin acid, immunoglobulins, arbidol, lopinavir/ritonavir, darunavir/cobicistat, and favipiravir. The risk factors related to the delay of virus clearance are represented Metanalysis Forest plot using Graph Pad Prism software (Graph Pad Software, Inc., San Diego, CA). In all analyses, statistical significance was formed by p <0.05.
Results
The Clinical Characteristics of COVID-19 Disease Severity
The 104 patients included 30 mild patients and 74 severe or critically ill patients (Table 1). Compared to mild patients, severe or critically ill patients were older (55.58 ± 15.98 vs 47.07 ± 13.87 years; p = 0.013), male (49.0% vs 12.5%; p = 0.015), and more often had hypertension (31.7% vs 3.8%; p = 0.003), tachypnea (19.2% vs 6.7%; p = 0.021), and dyspnea (13.7% vs 0%; p = 0.025). The leukocyte count was higher (8.24 ± 5.01 vs 5.43 ± 3.59; p = 0.002), with fewer lymphocytes (0.77 ± 0.43 vs 1.06 ± 0.45; p = 0.002) and virus CT values (26.07 ± 5.43 vs 29.55 ± 6.03; p = 0.009) in severe and critically ill patients than mild patients. Notably, the median duration of viral RNA positivity in sputum was 11 days in all COVID-19 patients. The longest duration of viral RNA positivity was 49 days after admission. The mean duration of viral RNA positivity in sputum or throat swab samples was much longer in severe or critically ill patients than mild patients (median: 12.0 vs 7 days; p = 0.003). Delayed clearance of SARS-CoV-2 was defined as the time of viral RNA in sputum of COVID-19 patients > 11 days (Table 1).
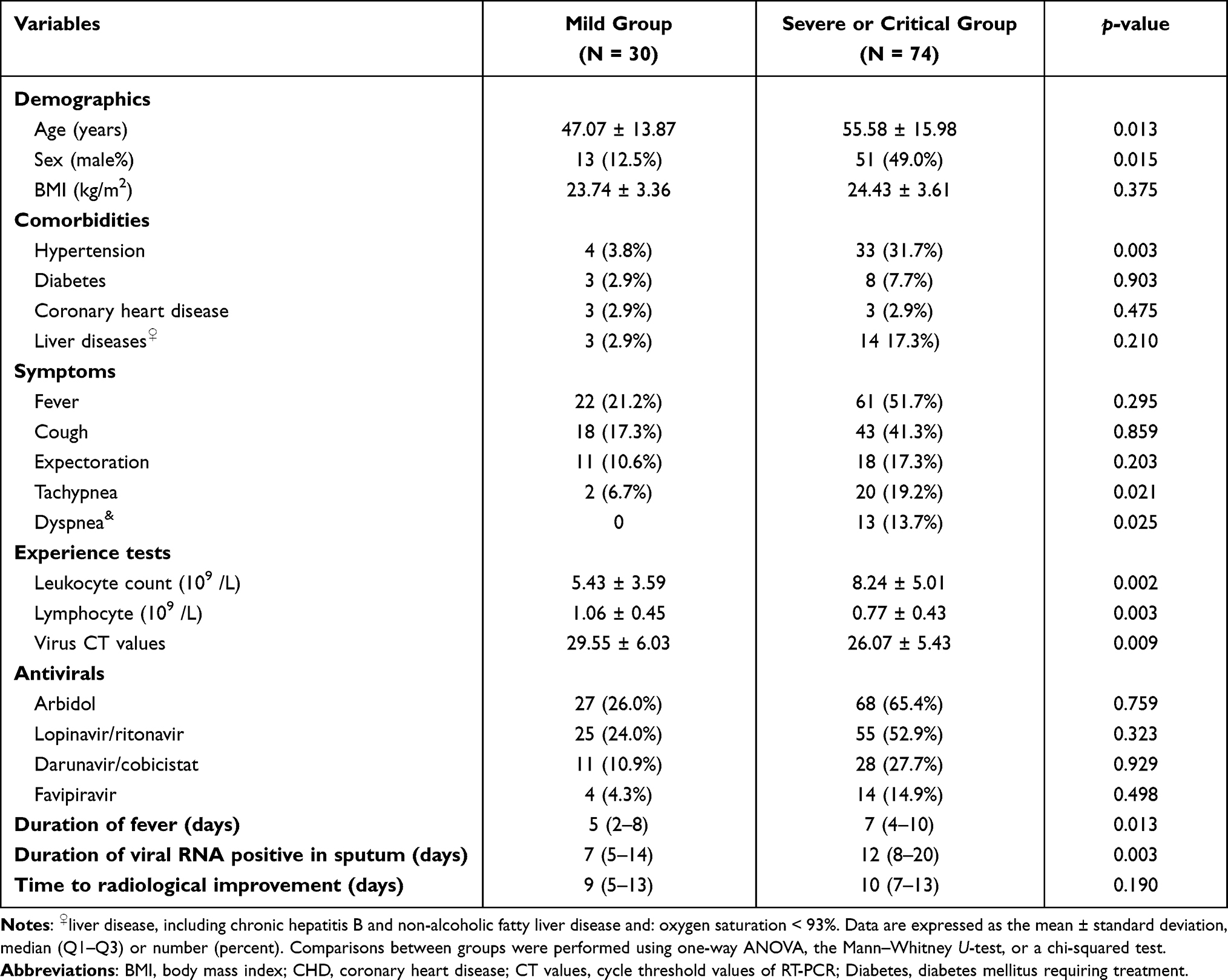 |
Table 1 Demographic and Clinical Characteristics of COVID-19 Patients in Different Disease Severity Groups |
The Clinical Characteristics of Delayed Clearance of SARS-CoV-2
As shown in Table 2, the patients with delayed clearance of SARS-CoV-2 were elderly patients (56.80 ± 17.46 VS 49.83 ± 13.64, p = 0.028), male (72.9% vs 51.8%, p = 0.028), with critical COVID-19 (27.1% vs 1.8%, p = 0.001), used with favipiravir (30.2% vs 9.8%, p = 0.012), little used with darunavir/cobicistat (13.9% vs 25.5%, p = 0.003), used immunoglobulin (60.4% vs 37.5%, p = 0.020) compared in patients without delayed clearance of SARS-CoV-2. Meanwhile, the duration of temperature fever (median: 8 vs 5 days, p < 0.001) and time to radiological improvement were significant prolonged (median: 13 vs 8 days, p < 0.001).
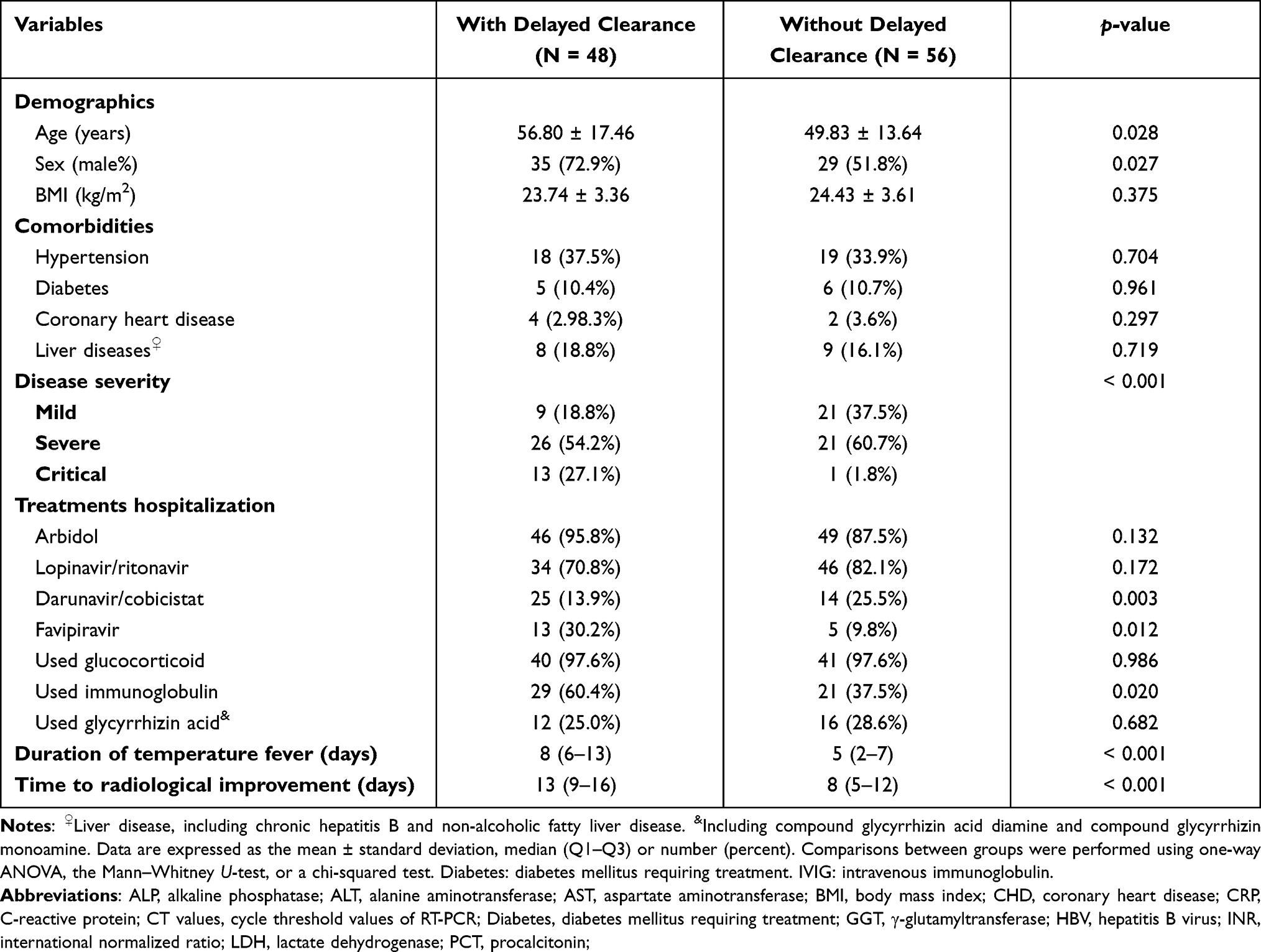 |
Table 2 Characteristics of Patients with or without Delayed Clearance of SARS-CoV-2 in COVID-19 Patients |
Among experience tests for COVID-19 patients with SARS-CoV-2 delayed clearance, the leukocyte count (median: 7.8 vs 5.2, p = 0.011), neutrophil count (median: 5. 6 vs 3.6, p = 0.032) and creatinine (median: 79 vs 21, p = 0.030) were increased and lymphocyte (median: 0.6 vs 0.9, p = 0.001), virus CT values (24.91 ± 5.11 vs 29.30 ± 5.65, p < 0.001) (Supplemental Table 1 and Figure 1).
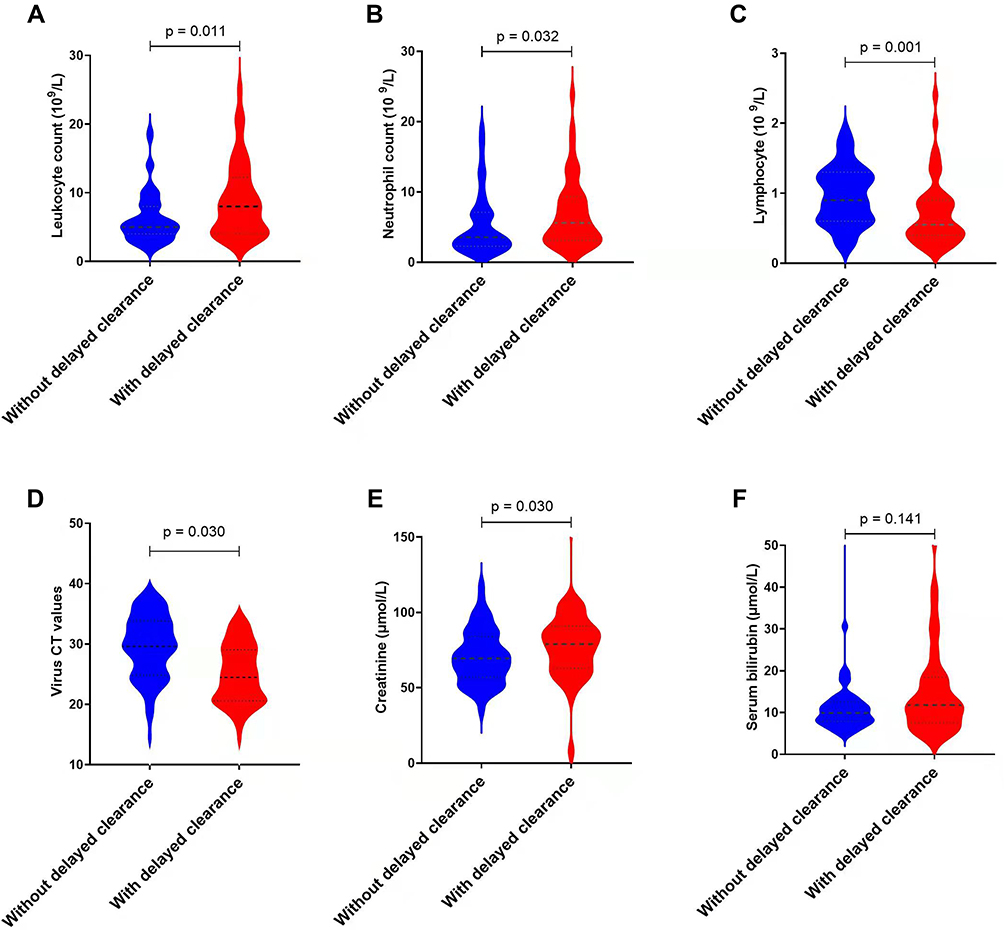 |
Figure 1 Comparison of experience tests in COVID-19 patients with or without delayed clearance of SARS-CoV-2 during hospitalization. (A) The leukocyte count increased significantly (p = 0.011) in the group with delayed virus clearance. (B) The neutrophil count increased significantly (p = 0.032) in the group with delayed virus clearance. (C) The lymphocyte decreased significantly (p = 0.001) in the group with delayed virus clearance. (D) The virus CT values decreased significantly (p = 0.030) in the group with delayed virus clearance. (E) The levels of creatinine increased significantly (p = 0.030) in the group with delayed virus clearance. (F) The difference between the two groups were not significant (p = 0.141) in serum bilirubin. |
Susceptibility Factors Associated With Delayed Clearance of SARS-CoV-2
Univariate analysis showed that the elderly (p = 0.032), male patients (p = 0.029), critical COVID-19 patients (p = 0.004), elevated leukocyte count (p = 0.008), lymphocytopenia (p = 0.010), lower virus CT value (p = 0.004) delayed time to radiologic improvement, and used with darunavir/cobicistat and favipiravir treatment had delayed clearance of SARS-CoV-2 in sputum (Table 3). Meanwhile, duration of temperature fever (p = 0.001) and time to radiological improvement (p < 0.001) were associated with delayed clearance of SARS-CoV-2 in sputum from COVID-19 patients (Figure 2A). Based on multivariate analysis shown that the used with darunavir/cobicistat treatment (odds ratio [OR]: 4.25, 95% confidence interval [CI]: 1.25–14.42, p = 0.020), duration of fever (OR: 1.15, 95% CI: 1.03–1.30, p = 0.015) and time to radiological improvement (OR: 1.14, 95% CI: 1.01–1.30, p = 0.033) were associated with delayed clearance of SARS-CoV-2 in sputum from COVID-19 patients (Table 3 and Figure 2B). Then adjusted in the multivariate binary logistic regression analysis model and found that critical COVID-19 patients (OR: 10.39, 95% CI: 1.08–99.78, p = 0.042), lower virus cycle threshold (CT) values of RT-PCR (OR: 0.30, 95% CI: 0.10–0.94, p = 0.039) and used with darunavir/cobicistat treatment (OR:4.92, 95% CI: 1.56–16.55, p = 0.007) were associated with delayed clearance of SARS-CoV-2 in sputum from COVID-19 patients (Supplemental Table 2).
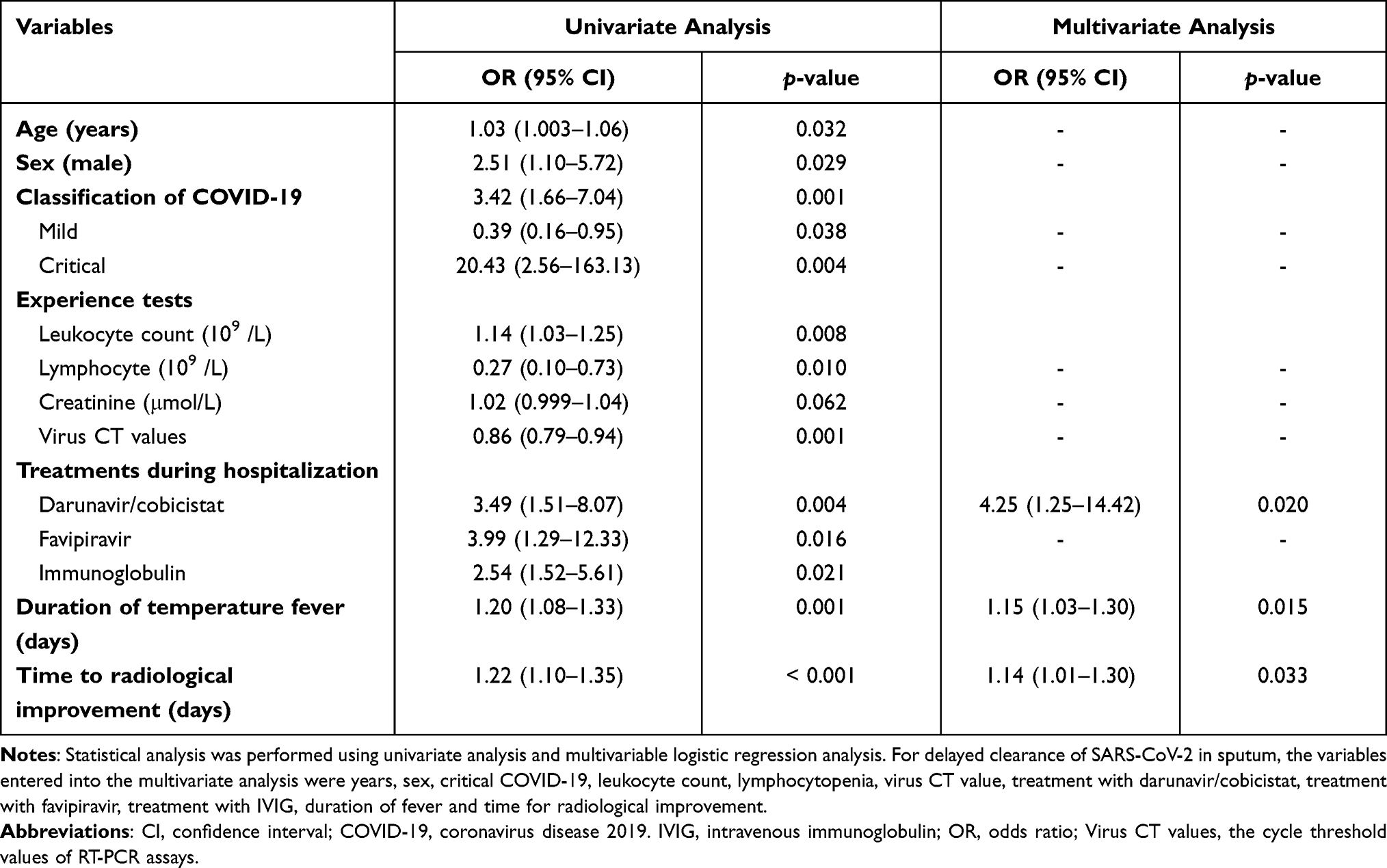 |
Table 3 Susceptibility Risk Factors Associated with Delayed Clearance of SARS-CoV-2 in Sputum |
 |
Figure 2 Used univariate analysis and multivariate analysis for susceptibility factors associated with delayed clearance of SARS-CoV-2 during hospitalization. (A) Univariate analysis for susceptibility factors associated with delayed clearance of SARS-CoV-2 during hospitalization; (B) multivariate analysis for susceptibility factors associated with delayed clearance of SARS-CoV-2 during hospitalization. |
Discussion
In the study, we found that the severity of diseases, higher level of virus copies was associated with virus clearance. And used antivirals with darunavir/cobicistat has little advantage in eliminating SARS-CoV-2. We did not find coronary heart disease (HR 0.619, 95% CI 0.411–0.933; p = 0.022), albumin levels (HR 1.027, 95% CI 1.005–1.049; p = 0.014) associated with SARS-CoV-2 RNA shedding.10 Actually, patients with coronary heart disease and decreased albumin levels mean the servers of disease.10,11 Some reports supported that severity of disease was associated with the duration of fever and time to radiological improvement.12 As professor B Recalde-Zamacona et al descripted that chronic rhinosinusitis is associated with prolonged SARS-CoV-2 RNA shedding in upper respiratory tract samples.13 Although we analyzed the impact of common clinical concomitant diseases on SARS-CoV-2 RNA shedding, but other diseases, such as chronic rhinosinusitis, asymptomatic immunocompromised individual with cancer et al should be further observation and follow-up.4,14
In agreement with a recent study, we report a considerable proportion of patients with detectable viral RNA in sputum or throat swabs > 20 days after admission (longest duration = 49 days). Although it was not ascertained that these patients were shedding live virus, they were isolated until viral RNA was undetectable. Indeed, if such a long viral shedding duration existed, it would be a challenge to establish isolation strategies (suspected cases were isolated for 14 days) for the public.9
Another finding was that the persistence of sputum viral RNA was closely related to disease severity and the virus CT value on admission, although the absence of viral RNA in sputum was correlated with a delay in radiologic improvement. As we know that lower virus CT value means the higher copy of virus. Actually, radiologic improvement was in accordance with the severity of COVID-19 and delayed in patients with persistent viral RNA.15,16 Therefore, the absence of viral RNA was in accordance with the critically ill patients. It is likely that the failure to clear the virus promptly contributes to disease progression and the exacerbation of the disease itself hinders viral clearance, resulting in a vicious circle.
Finally, we observed that the virus clearance time of COVID-19 patients treated with darunavir/cobicistat was prolonged. As reported by Chen et al, 5 days of darunavir/cobicistat did not increase the proportion of negative conversion compared with standard care alone.17 It is quite possible that darunavir/cobicistat may not match potential targets in the four main viral proteins of SARS-CoV-2. In vitro data with normal oral administration of darunavir/cobicistat did not exhibit significant anti-SARS-CoV-2 activity.18 We observed that the virus clearance of COVID-19 patients with darunavir/cobicistat was prolonged, as the same with the reported form doctor Augusto Di Castelnuovo et al.19 In this study, there were no statistical differences between the two groups that were treated and not treated with darunavir/cobicistat with respect to disease severity and other confounders. Our study was a single center retrospective observational study. Therefore, whether there is a causal relationship needs further RCT studies.
In conclusion, we found that clearance of viral RNA in sputum was delayed in severe COVID-19 patients, especially with lower virus CT value. And antivirals with darunavir/cobicistat has little advantage in eliminating SARS-CoV-2.
Abbreviations
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; CHD, coronary heart disease; CI, confidence interval; COVID-19, coronavirus disease 2019; Diabetes, diabetes mellitus requiring treatment; OR, odds ratio; CRP, C-reactive protein; GGT, γ-glutamyltransferase; INR, international normalized ratio; LDH, lactate dehydrogenase; IVIG, intravenous immunoglobulin; OR, odds ratio; PCT, procalcitonin; RT-PCR, real-time polymerase chain reaction; SARS-Cov-2, acute respiratory syndrome-coronavirus-2; viral CT values, cycle threshold values of RT-PCR.
Data Sharing Statement
All datasets generated for this study are included in the article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Key R&D Program of China (2021YFC2301804), National Natural Science Foundation of China (grant numbers 81971982); National Major Science and Technology Projects of China (grant numbers 2017ZX10204401001002) and Zhejiang Province Education Foundation (grant numbers Y202043368).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Guan WJ, Ni Z-Y, Hu Y, et al. clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. doi:10.1056/NEJMoa2002032
2. Xu XW, Wu -X-X, Jiang X-G, et al. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: retrospective case series. BMJ. 2020;368:m606. doi:10.1136/bmj.m606
3. Huang C, Huang L, Wang Y, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2021;397(10270):220–232. doi:10.1016/S0140-6736(20)32656-8
4. Yu X, Sun S, Shi Y, et al. SARS-CoV-2 viral load in sputum correlates with risk of COVID-19 progression. Crit Care. 2020;24(1):170. doi:10.1186/s13054-020-02893-8
5. Zheng S, Fan J, Yu F, et al. Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang province, China, January-March 2020: retrospective cohort study. BMJ. 2020;369:m1443. doi:10.1136/bmj.m1443
6. Zou L, Ruan F, Huang M, et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020;382(12):1177–1179. doi:10.1056/NEJMc2001737
7. Young BE, Ong SWX, Kalimuddin S, et al. Epidemiologic features and clinical course of patients infected with SARS-CoV-2 in Singapore. JAMA. 2020;323(15):1488–1494. doi:10.1001/jama.2020.3204
8. To KK, Tsang OT-Y, Leung W-S, et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. Lancet Infect Dis. 2020;20(5):565–574. doi:10.1016/S1473-3099(20)30196-1
9. National Health Commission & National Administration of Traditional Chinese Medicine. Diagnosis and treatment protocol for novel coronavirus pneumonia (Trial Version 7). Chin Med J. 2020;133(9):1087–1095. doi:10.1097/CM9.0000000000000819
10. Fu Y, Han P, Zhu R, et al. Risk factors for viral RNA shedding in COVID-19 patients. Eur Respir J. 2020;56:1. doi:10.1183/13993003.01190-2020
11. Peng Y, Meng K, He M, et al. Clinical characteristics and prognosis of 244 cardiovascular patients suffering from coronavirus disease in Wuhan, China. J Am Heart Assoc. 2020;9(19):e016796. doi:10.1161/JAHA.120.016796
12. Tu H, Zhao H, Su J, et al. Predictors of COVID-19 infection: a prevalence study of hospitalized patients. Can J Infect Dis Med Microbiol. 2021;2021:6213450. doi:10.1155/2021/6213450
13. Recalde-Zamacona B, Tomás‐Velázquez A, Campo A, et al. Chronic rhinosinusitis is associated with prolonged SARS-CoV-2 RNA shedding in upper respiratory tract samples: a case-control study. J Intern Med. 2021;289(6):921–925. doi:10.1111/joim.13237
14. Avanzato VA, Matson MJ, Seifert SN, et al. Case study: prolonged infectious SARS-COV-2 shedding from an asymptomatic immunocompromised individual with cancer. Cell. 2020;183(7):1901–1912.e9. doi:10.1016/j.cell.2020.10.049
15. Chang D, Mo G, Yuan X, et al. Time kinetics of viral clearance and resolution of symptoms in novel coronavirus infection. Am J Respir Crit Care Med. 2020;201(9):1150–1152. doi:10.1164/rccm.202003-0524LE
16. Nasiri MJ, Haddadi S, Tahvildari A, et al. COVID-19 clinical characteristics, and sex-specific risk of mortality: systematic review and meta-analysis. Front Med. 2020;7:459. doi:10.3389/fmed.2020.00459
17. Chen J, Xia L, Liu L, et al. Antiviral activity and safety of darunavir/cobicistat for the treatment of COVID-19. open forum. Infect Dis. 2020;7(7):ofaa241.
18. Wu C, Liu Y, Yang Y, et al. Analysis of therapeutic targets for SARS-CoV-2 and discovery of potential drugs by computational methods. Acta Pharm Sin B. 2020;10(5):766–788. doi:10.1016/j.apsb.2020.02.008
19. Di Castelnuovo A, Costanzo S, Antinori A, et al. Lopinavir/ritonavir and darunavir/cobicistat in hospitalized COVID-19 patients: findings from the multicenter Italian CORIST study. Front Med. 2021;8:639970. doi:10.3389/fmed.2021.639970
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.