")
Back to Journals » Clinical Epidemiology » Volume 11
Delay in surgery, risk of hospital-treated infections and the prognostic impact of comorbidity in hip fracture patients. A Danish nationwide cohort study, 2005–2016
Authors Glassou EN , Kjørholt KKE, Hansen TB , Pedersen AB
Received 4 January 2019
Accepted for publication 14 March 2019
Published 10 May 2019 Volume 2019:11 Pages 383—395
DOI https://doi.org/10.2147/CLEP.S200454
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Henrik Sørensen
Eva N Glassou,1,2 Kaja KE Kjørholt,3 Torben B Hansen,1 Alma B Pedersen3
1University clinic for hand, hip and knee surgery, Regional Hospital West Jutland, Aarhus University, Holstebro 7500, Denmark; 2Department of Quality, Regional Hospital West Jutland, Holstebro 7500, Denmark; 3Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus N 8200, Denmark
Purpose: We examined the association between delay in surgery and hospital-treated infections in hip fracture patients with and without known comorbidities.
Patients and methods: All hip fracture patients aged ≥65 years registered in the Danish Multidisciplinary Hip Fracture Registry from 2005 to 2016 were included (n=72,520). Delay in surgery was defined as the time in hours from admission to surgery and was divided into 3 groups (12, 24 and 48 hrs). The outcomes were hospital-treated pneumonia, urinary tract infection and reoperation due to infection 0–30 days after surgery. As a measure of comorbidity, we used the Charlson Comorbidity Index (CCI): none (no registered comorbidities prior to the fracture), medium (1–2 points) and high (≥3 points).
Results: Overall, there was an association between a delay of 12 hrs and pneumonia. A delay of 12 hrs was associated with an increased risk of pneumonia in patients with no comorbidities (adjusted hazard ratio (HR) 1.20, confidence interval (CI) 1.03–1.40) and a delay of 24 hrs was associated with an increased risk of pneumonia in patients with a medium level of comorbidity (HR 1.12, CI (1.02–1.23)). Overall, delay was associated with reoperation due to infection, particularly among patients with comorbidities, although the confidence intervals of some of the estimates were wide. A delay of 48 hrs was associated with an increased risk of reoperation due to infection in patients with a high level of comorbidity (HR 2.36, CI 1.19–4.69).
Conclusion: Delay in surgery was associated with an increased risk of hospital-treated pneumonia and reoperations due to infection within 30 days of surgery. The number of postoperative hospital-treated infections within 30 days may be reduced by continuously targeting pre-, per- and postoperative optimization not only for patients with high level of comorbidity but also for hip fracture patients without known comorbidities prior to surgery.
Keywords: hip fracture, delay in surgery, pneumonia, urinary tract infection, reoperation, surgical site infection
Introduction
Hip fractures, with an annual incidence rate in Denmark of approximately 4.2 per 1,000 person-years, are a leading cause of hospital admissions, disability and increased mortality risk in the elderly population.1 The typical hip fracture patient is often frail, elderly and multicomorbid; is in polypharmacy treatment; has underlying cognitive discords; and is dehydrated due to a significant time lapse from trauma to admission.2 Therefore, these patients are vulnerable to both trauma and subsequent surgery, as well to the potential complications that may occur in relation to surgery and immobilization.
In addition to the patients’ own medical state, a delay in surgery may be associated with an increased risk of complications such as pressure wounds, urinary tract infections (UTIs), pneumonia and mortality.3–11 However, a delay in surgery may be favorable in some hip fracture patients, allowing time for a beneficial stabilization of the patient’s medical condition and a proper discontinuation of anticoagulant drugs, commonly used in this patient group.4
The recommendation from the National Institute for Health and Care Excellence is surgery on the day of admission, or the day after.12 Additionally, studies have shown that 24 hrs may represent a threshold in relation to mortality and complications.13 In Denmark, the national guidelines recommend that at least 75% of hip fracture patients receive surgery within 24 hrs,14 but this recommendation has recently become an object of debate. To reduce the mortality risk, which is associated with a delay in surgery, several argue for a further reduction in the delay in surgery. As hip fracture patients compete with other surgery patients for a limited amount of resources at the hospital, including clinical staff and operation rooms, better risk stratification of this patient group is needed. A potential association between delay in surgery and risk of infections may, in this context, be of importance. Therefore, our aim was to examine how delay in surgery affects the risk of an infection in hip fracture patients with and without known comorbidities.
Materials and methods
Study population
Through the Danish Multidisciplinary Hip Fracture Registry (DMHFR) we included all first-time hip fracture patients 65 years or older who underwent primary hip replacement or open reduction and internal fixation between January 1, 2005, and December 31, 2016 (n=74,791). In total, 2,271 patients were excluded due to either missing follow-up (20 patients), missing information about delay (170 patients) or delay of more than 75 hrs (2,081 patients), which we interpreted as a result of registration errors. In total, 72,520 patients met the inclusion criteria and were included in the final analyses.
Data sources
Based on each resident’s unique 10-digit personal identification number encoding age, sex and date of birth, data were collected from four databases and linked to a final dataset on an individual level.
The DMHFR is a nationwide clinical quality database holding individual data on all patients ≥65 years old with femoral neck, per-trochanteric or sub-trochanteric fractures treated surgically since 2003 (see appendix 1 for codes according to the International Classification of Diseases (ICD), revision 10). Reporting in the DMHFR is mandatory, and data are collected prospectively during hospital admission using standardized registration forms in the electronic patient records.15,16 Detailed definitions of data elements are provided to ensure uniform registration of data across departments. Due to the registration method, the completeness is >95%.14 The DMHFR was used to identify the study population and obtain information about fracture type, time of hospitalization and surgery (and by that delay in surgery), type of surgery, body mass index (BMI) and marital status.
The Danish Civil Registration System was initiated in 1968 and contains records of all Danish residents, among other records of residence and date of death. The CRS is updated daily.17 The Danish Civil Registration System provided information about the date of death.
The Danish National Patient Register contains information on surgical procedures and primary discharge diagnoses and up to 20 secondary discharge diagnoses on all inpatient admissions and outpatient visits to Danish hospitals.18 Diagnoses are coded according to the ICD. The Danish National Patient Register provided information about infections during the index hospitalization or re-admission. Additionally, the register provided information about comorbidities at the time of surgery and 10 years prior to surgery, based on the ICD codes.
The Danish National Health Service Prescription Database contains complete data on all reimbursed prescriptions dispensed from community pharmacies and hospital-based outpatient pharmacies in Denmark since 2004.19 The drugs are coded according to the Anatomical Therapeutic Chemical classification system. The database provided information about drug use prior to the hip fracture.
Exposure - delay in surgery
Delay in surgery was defined as time in hours from the hospital admission to the start of surgery. Patients are classified as those with delays in surgery within 12 hrs, 24 hrs or 48 hrs. We compared patients with and without delay within 12 hrs, as well as patients with and without delay within 24 hrs and 48 hrs. This approach is taken to reduce the potential for unmeasured confounding. Thus, prolonged waiting time for surgery may indicate medical rather than administrative reasons for delay and may introduce confounding factors. In addition, the time of admission during the day may be considered a confounder. Further, with this comparison, we can potentially define the threshold for delayed surgery in relation to infection risk.
Outcome - hospital treated infection
The outcome was the presence of any of the following 3 conditions: hospital-treated UTI, hospital-treated pneumonia and reoperation due to infection, all 3 between 0 (day of surgery) and 30 days after surgery. For all 3 infections, the first hospital-treated infection during either the index hospitalization or a re-admission or an outpatient clinic visit at a private or a public hospital forms the basis of the analyses. The follow-up period of 0–30 days was chosen to represent the early postoperative period and the first period after discharge. This period represents a clinically important and, from the patients’ point of view, a vulnerable period where the health-related effect of hip surgery may be maintained or lost.
Covariates
We measured the following covariates as of the surgery date: age (in categories; 65–74, 75–79, 80–84, 85–90 and 90+ years), sex, BMI (in categories; underweight: BMI <18.5 kg/m2, normal weight: BMI ≤18.5–24.9 kg/m2, overweight: BMI 25.0–29.9 kg/m2 and obese: BMI ≥30.0 kg/m2), comorbidity level, marital status (married, not married), type of fracture (femoral neck and sub-/per-trochanteric fractures), type of surgery (osteosynthesis and hemi/total arthroplasty) and surgery year (biannual). Furthermore, we included the use of corticosteroids, anti-osteoporotic medicine, non-steroidal anti-inflammatory drugs, oral anticoagulants, statins, selective serotonin reuptake inhibitors and antibiotics due to the potential association between these drugs and infection risk. Patients were categorized into nonusers (no redemption of a prescribed specific drug in the year prior to surgery), former users (redemption of at least one prescription drug 91–365 days prior to hip fracture surgery) and current users (at least one prescription drug ≤90 days prior to hip fracture surgery).
The comorbidity level was measured with the Charlson Comorbidity Index (CCI) score. We defined three comorbidity levels; none, given to patients with no previous record of diseases included in the CCI; a medium level of comorbidity and a high level of comorbidity, given to patients with a record of diseases equaling CCI-index scores at 1 to 2 and 3 or more, respectively. All primary and secondary diagnoses included in the CCI (see appendix 1 for ICD, revision 10 codes) and registered in relation to hospitalizations and outpatient visits over a ten-year period before the hip fracture formed the basis of the CCI calculation. In addition to the CCI, we included the presence of an alcoholism-related disease as an individual comorbid condition.
All relevant ATC codes and ICD codes used to define the study population, infections and comorbidities are available in appendix 1. The distribution of diseases from the Charlson index according to delay in surgery is also available in appendix 1.
Statistics
Patient characteristics were tabulated as proportions by delay in surgery. We calculated the incidence rates (IRs) per 1,000 person-years with 95% confidence intervals (CIs) for each of the 3 infections. Using the Cox proportional hazards regression model censoring at death, we calculated crude and adjusted hazard ratios (HRs) with corresponding 95% CIs to evaluate the impact of delay in surgery on the risk of infections within 0–30 days. HRs were adjusted for age, sex, comorbidity level, type of fracture and year of surgery. The impact of delay in surgery on the risk of infections was examined by stratifying for comorbidity level, leaving this covariate out of the adjustment. The proportional hazards assumptions were controlled graphically and by log-minus log plot, and found to be fulfilled.
All statistical analyses were performed using STATA Version 15.0 (Stata Corp LP, College Station, TX, USA).
Ethics
The study was approved by the Danish Data Protection Agency (Region of Central Denmark journal number 1–16-02–444-15).
Results
Patient characteristics according to delay in surgery are presented in Table 1. Patients who were delayed more than 24 or 48 hrs were slightly more comorbid, sustained a femoral neck fracture, were treated with a hemi- and total arthroplasty and were current users of oral anti-coagulation. The absolute difference in the proportion of these variables was less than 4%. In general, the proportion of patients with a delay of more than 24 hrs decreased during 2005–2016 with a turning point between 2010 and 2011. The presence of specific comorbidities at the time of surgery was not associated with surgery delay. Of the 19 disease topics included in the CCI, only congestive heart failure and cerebrovascular disease had a small impact on the delay in surgery. We observed only slightly (2–3%) more patients with congestive heart disease and cerebrovascular disease in patients with a delay in surgery of more than 24 hrs or 48 hrs compared to 12 hrs (Appendix 1).
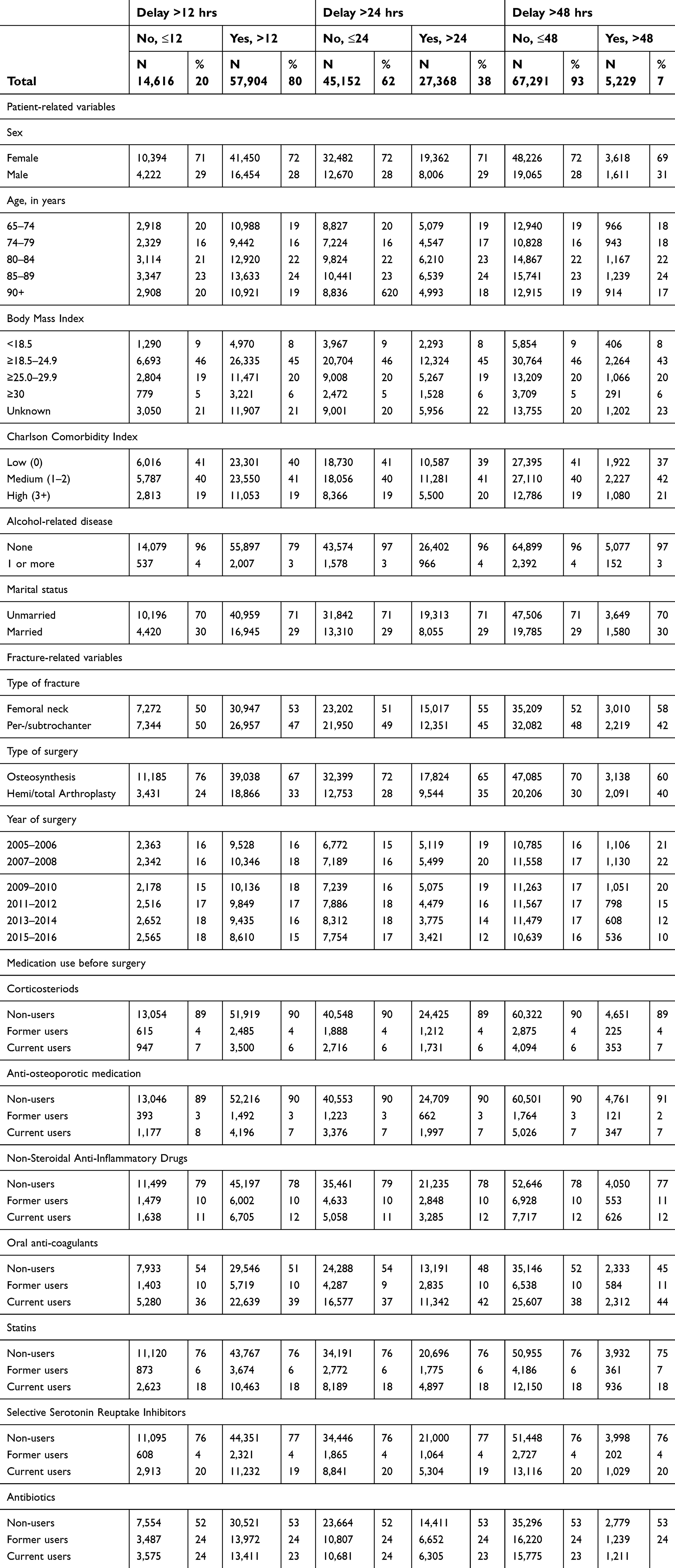 | Table 1 Patient characteristics according to delay of surgery |
Hospital treated infections
In total, 7,287 (10%) of the patients experienced a hospital-treated infection within 0–30 days after surgery. UTI accounted for 4,205 (45%) of all infections, pneumonia accounted for 3,805 (41%) and reoperations due to infection accounted for 253 (3%). The number of infections, incidence rates and hazard ratios for the hospital-treated infections are presented in Table 2.
 | Table 2 Incidence rate and hazard ratios (HR with 95% confidence interval (CI) for the 3 specific hospital-treated infections within 0–30 days following hip fracture surgery. HRs were adjusted for age, sex, comorbidity burden (CCI), type of fracture and year of surgery. When stratifying for comorbidity, the CCI-variable was left out of the analysis |
Delay in surgery was associated with hospital-treated pneumonia. Overall, a delay of >24 hrs resulted in an increased risk of hospital-treated pneumonia (HR 1.09, CI: 1.02–1.16). A similar association was observed between a delay of >24 hrs and patients with a medium comorbidity burden (HR 1.12, CI: 1.02–1.23). In addition, delays of >12 hrs and >24 hrs were associated with a HR of 1.20 (CI: 1.03–1.40) and a HR of 1.11 (CI: 0.98–1.26) for hospital-treated pneumonia in patients with no previous comorbidity.
Overall, a delay of more than 12 hrs was associated with an increased risk of reoperation due to infection within 30 days (HR 1.41, CI: 1.00–1.99). In addition, a delay of 48 hrs was associated with an increased risk of reoperation due to infection within 30 days (HR 1.51, CI: 1.01–2.26). Stratification on comorbidity suggests that delays of 12 hrs, 24 hrs and 48 hrs among patients with moderate and high comorbidity burden were associated with an increased risk of reoperation. However, due to the small sample size and number of outcomes, these estimates should be interpreted with caution.
UTI was the most frequent hospital-treated infection. The incidence rate was approximately 2.1 per 1,000 person-years regardless of delay in surgery. We found no associations between delay and UTI, either overall or in regard to the comorbidity burden.
Discussion
Delay in surgery was associated with an increased risk of hospital-treated pneumonia and reoperations due to infection. A delay of only 12 hrs increased the risk of pneumonia in patients with no known comorbidity prior to surgery. For patients with a medium level of comorbidity, a delay of 24 hrs increased the risk of pneumonia and for patients with a high level of comorbidity, a delay of 48 hrs increased the risk of reoperation due to infection.
The best design when evaluating the effect of delay in surgery would be a randomized controlled trial. However, this is not possible due to ethical and practical reasons, and a large cohort study with the advantages of prospectively and independently collected data is the second best design. This study is, to the best of our knowledge, the largest cohort study evaluating the effect of delay in surgery on the risk of specific hospital-treated infections.
A comparison of studies is in general difficult due to a great variability in both delay cut-offs and the definitions of postoperative complications. Delay cut-offs of more than 24 hrs are not comparable with Danish conditions as more than 60% of patients are treated within 24 hrs. Additionally, an outcome of only early in-hospital complications is not applicable, as we leave out the infections causing readmissions. Nevertheless, both Simunovic et al and Klestil et al concluded in their reviews that early surgery is associated with fewer peri- and postoperative complications including pneumonia.6,10 These findings are supported by Pincus et al who, in a large cohort study from Canada, showed that increased delay in surgery (>24 hrs) was associated with an increased risk of postoperative complications (within 30 days of surgery) including pneumonia.13 As both the exposure and the outcome in Pincus et al are comparable to those in our study, our results add further evidence to the association between early surgery and reduced risk of postoperative pneumonia.
In relation to UTI, our findings support the general impression that delay in surgery does not affect the risk of early postoperative UTI.20–22 Smektala et al found no effect of delay on the risk of UTI in a prospective cohort study of 2,916 hip fracture patients from Germany.22 Similar findings were made by Majumdar et al in a Canadian retrospective cohort study. Here, they found that a delay of 24 or 48 hrs had no effect on the risk of in-hospital UTI.21
We found that the association between delay of surgery and risk of postoperative pneumonia was most distinct for patients with no known comorbidities or a medium level of comorbidities at the time of the hip fracture. This is not intuitive and not identical to earlier findings. Klestil et al suggest in a recent review that patients with comorbidities often benefit from surgery within 24 hrs.10 Since patients with a number of comorbidities prior to the hip fracture are more susceptible to a longer hospital stay than are patients without known comorbidity prior to the hip fracture, it is possible that registration of hospital-treated infections during the index hospitalization is more likely underestimated among high vs low comorbidity patients. However, any underestimation of infection registration during index hospitalization, as well as any underestimation of infection during the follow-up period, will most likely be nondifferential, thus independent of the delay in surgery. On the other hand, if hip fracture in less comorbid patients is the first apparent proof of a medical deterioration, then the findings about an association between surgery delay and risk of infection in less comorbid patients is not that surprising. Here, further studies are needed.
As mentioned, the international recommendations regarding surgery after hip fracture are surgery on the day of admission, or the day after.12 Additionally, 24 hrs may represent a threshold defining complications.13 According to Kelly-Pettersson et al, there is no safe time frame, and additionally, the risk of serious adverse events may increase for every 10 hrs of delay of surgery.9 In view of this and our results, it seems reasonable to assume that the number of hospital-treated infections within 30 days can be reduced if one complies with the guidelines or even better ensures surgery within 12 hrs.
Limitations
Delay in surgery may be due to several reasons. Organizational reasons may delay surgery. This affects patients with femoral neck fractures and therefore patients in need of hemi- or total arthroplasties as these surgeries demand skilled surgeons who are not always on duty. Additionally, the patient’s medical condition may call for a physiological optimization after the fracture, thus delaying surgery. This affects patients with a high comorbidity burden and with current use of oral anti-coagulation. Hypothetically, poor use of the delay in the less vulnerable patients, compared to that in patients with a known high comorbidity level at the time of surgery, could lead to an association between delay in surgery and hospital-treated pneumonia in the less vulnerable patients. Unfortunately, we have no information about why surgery is delayed (medical or organizational reasons) and if the time is well spent. Therefore, we cannot rule out residual confounding. Inclusion of both pathological and nonpathological fractures may have biased our estimates. However, patients with longer surgery delays were not more likely to have a diagnosis of “any tumor” and “metastatic tumor” than patients with shorter surgery delays (Appendix 1). Therefore, we do not believe this would have had a strong impact on our findings. Additionally, we have no exact knowledge about how many patients with a high energy trauma hip fracture were included in our study population, but we expect it to be minimal.
Stratification for comorbidity burden is made with the CCI. The index has been developed to summarize complex medical histories, offering statistical efficiency and straightforward interpretation compared with the inclusion of individual comorbid diseases in statistical models or stratified analyses. The index is frequently used in studies based on register data. The limitation of the index is that it precludes the estimation of the effects of individual comorbid diseases. However, stratifying on the CCI rather than specific comorbid diseases provides an overall and crude effect of delay on infection risk in comorbid and healthy patients. Since the index does not take the severity of a disease into account, residual confounding may still be present. Additionally, since the CCI does not capture diseases treated only by general practitioners, we might have underestimated the number of hip fracture patients with a comorbidity burden. We lacked measurements of frailty and nutrition status, as well as other lifestyle factors, and socioeconomic factors that have previously been reported as risk factors for infection. These factors could also be related to surgery delay.
Conclusion
Delay in surgery was associated with an increased risk of hospital-treated pneumonia and reoperations due to infection. Delays in surgery of 12 hrs and 24 hrs increased the risk of hospital-treated pneumonia in patients with no known and medium levels of comorbidity prior to surgery. A delay of 48 hrs increased the risk of reoperation due to infection in patients with a high level of comorbidity prior to surgery.
However, the association was modest, and one can argue that time from hospitalization to surgery is used for beneficial stabilization of the patient’s medical condition. When held against the current national and international guidelines, the number of hospital-treated infections within 30 days may, however, be reduced if delay in surgery is shortened. Additionally, an increased focus on the less comorbid patients seems beneficial. These patients may, in fact, be patients with a hip fracture as the first apparent proof of a medical deterioration. To balance confounding, further studies looking at the association between delay of surgery and infection need to be conducted with prospective registration of the reason for the delay.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pedersen AB, Ehrenstein V, Szepligeti SK, et al. Thirty-five-year trends in first-time hospitalization for hip fracture, 1-year mortality, and the prognostic impact of comorbidity: a Danish nationwide cohort study, 1980-2014. Epidemiology. 2017;28(6):898–905. doi:10.1097/EDE.0000000000000729
2. Pedersen AB, Ehrenstein V, Szepligeti SK, Sørensen HT. Hip fracture, comorbidity, and the risk of myocardial infarction and stroke: a Danish nationwide cohort study, 1995-2015. J Bone Miner Res. 2017;32(12):2339–2346. doi:10.1002/jbmr.3242
3. Rademakers LM, Vainas T, van Zutphen SW, Brink PR, van Helden SH. Pressure ulcers and prolonged hospital stay in hip fracture patients affected by time-to-surgery. Eur J Trauma Emerg Surg. 2007;33(3):238–244. doi:10.1007/s00068-007-6212-8
4. Khan SK, Kalra S, Khanna A, Thiruvengada MM, Parker MJ. Timing of surgery for hip fractures: a systematic review of 52 published studies involving 291,413 patients. Injury. 2009;40(7):692–697. doi:10.1016/j.injury.2009.01.010
5. Garcia-Alvarez F, Al-Ghanem R, Garcia-Alvarez I, Lopez-Baisson A, Bernal M. Risk factors for postoperative infections in patients with hip fracture treated by means of Thompson arthroplasty. Arch Gerontol Geriatr. 2010;50(1):51–55. doi:10.1016/j.archger.2009.01.009
6. Simunovic N, Devereaux PJ, Sprague S, et al. Effect of early surgery after hip fracture on mortality and complications: systematic review and meta-analysis. Cmaj. 2010;182(15):1609–1616. doi:10.1503/cmaj.092220
7. Moja L, Piatti A, Pecoraro V, et al. Timing matters in hip fracture surgery: patients operated within 48 hrs have better outcomes. A meta-analysis and meta-regression of over 190,000 patients. PLoS One. 2012;7(10):e46175. doi:10.1371/journal.pone.0046175
8. Cordero J, Maldonado A, Iborra S. Surgical delay as a risk factor for wound infection after a hip fracture. Injury. 2016;47(Suppl 3):S56–S60. doi:10.1016/S0020-1383(16)30607-6
9. Kelly-Pettersson P, Samuelsson B, Muren O, et al. Waiting time to surgery is correlated with an increased risk of serious adverse events during hospital stay in patients with hip-fracture: a cohort study. Int J Nurs Stud. 2017;69:91–97. doi:10.1016/j.ijnurstu.2017.02.003
10. Klestil T, Roder C, Stotter C, et al. Impact of timing of surgery in elderly hip fracture patients: a systematic review and meta-analysis. Sci Rep. 2018;8(1):13933. 018-32098-7. doi:10.1038/s41598-018-32098-7
11. Byun SE, Shon HC, Kim JW, Kim HK, Sim Y. Risk factors and prognostic implications of aspiration pneumonia in older hip fracture patients: a multicenter retrospective analysis. Geriatr Gerontol Int. 2019;19(2):119–123. doi:10.1111/ggi.13559
12.
13. Pincus D, Ravi B, Wasserstein D, et al. Association between wait time and 30-day mortality in adults undergoing hip fracture surgery. JAMA. 2017;318(20):1994–2003. doi:10.1001/jama.2017.17606
14.
15. Mainz J, Hansen AM, Palshof T, Bartels PD. National quality measurement using clinical indicators: the Danish National Indicator Project. J Surg Oncol. 2009;99(8):500–504. doi:10.1002/jso.21192
16. Kristensen PK, Thillemann TM, Søballe K, Johnsen SP. Are process performance measures associated with clinical outcomes among patients with hip fractures? A population-based cohort study. Int J Qual Health Care. 2016;28(6):698–708. doi:10.1093/intqhc/mzw093
17. Schmidt M, Pedersen L, Sørensen HT. The Danish civil registration system as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
18. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish national patient registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
19. Johannesdottir SA, Horvath-Puho E, Ehrenstein V, Schmidt M, Pedersen L, Sørensen HT. Existing data sources for clinical epidemiology: the Danish national database of reimbursed prescriptions. Clin Epidemiol. 2012;4:303–313. doi:10.2147/CLEP.S37587
20. Moran CG, Wenn RT, Sikand M, Taylor AM. Early mortality after hip fracture: is delay before surgery important? J Bone Joint Surg Am. 2005;87(3):483–489. doi:10.2106/JBJS.D.01796
21. Majumdar SR, Beaupre LA, Johnston DW, Dick DA, Cinats JG, Jiang HX. Lack of association between mortality and timing of surgical fixation in elderly patients with hip fracture: results of a retrospective population-based cohort study. Med Care. 2006;44(6):552–559. doi:10.1097/01.mlr.0000215812.13720.2e
22. Smektala R, Endres HG, Dasch B, et al. The effect of time-to-surgery on outcome in elderly patients with proximal femoral fractures. BMC Musculoskelet Disord. 2008;9:171. 2474-9-171. doi10.1186/1471-2474-9-87
Appendix 1
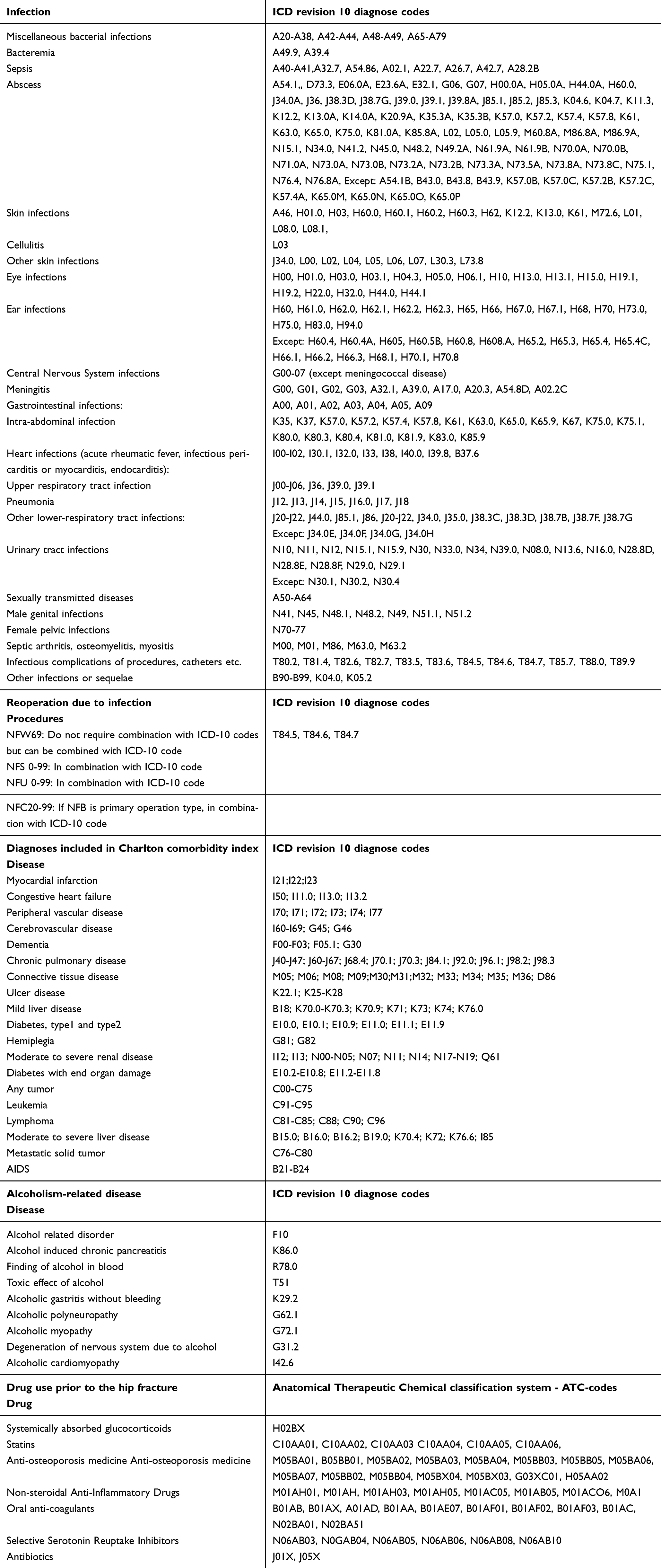 | Any hospital-treated (inpatient or outpatient) infections, collected from The Danish National Patient Register. |
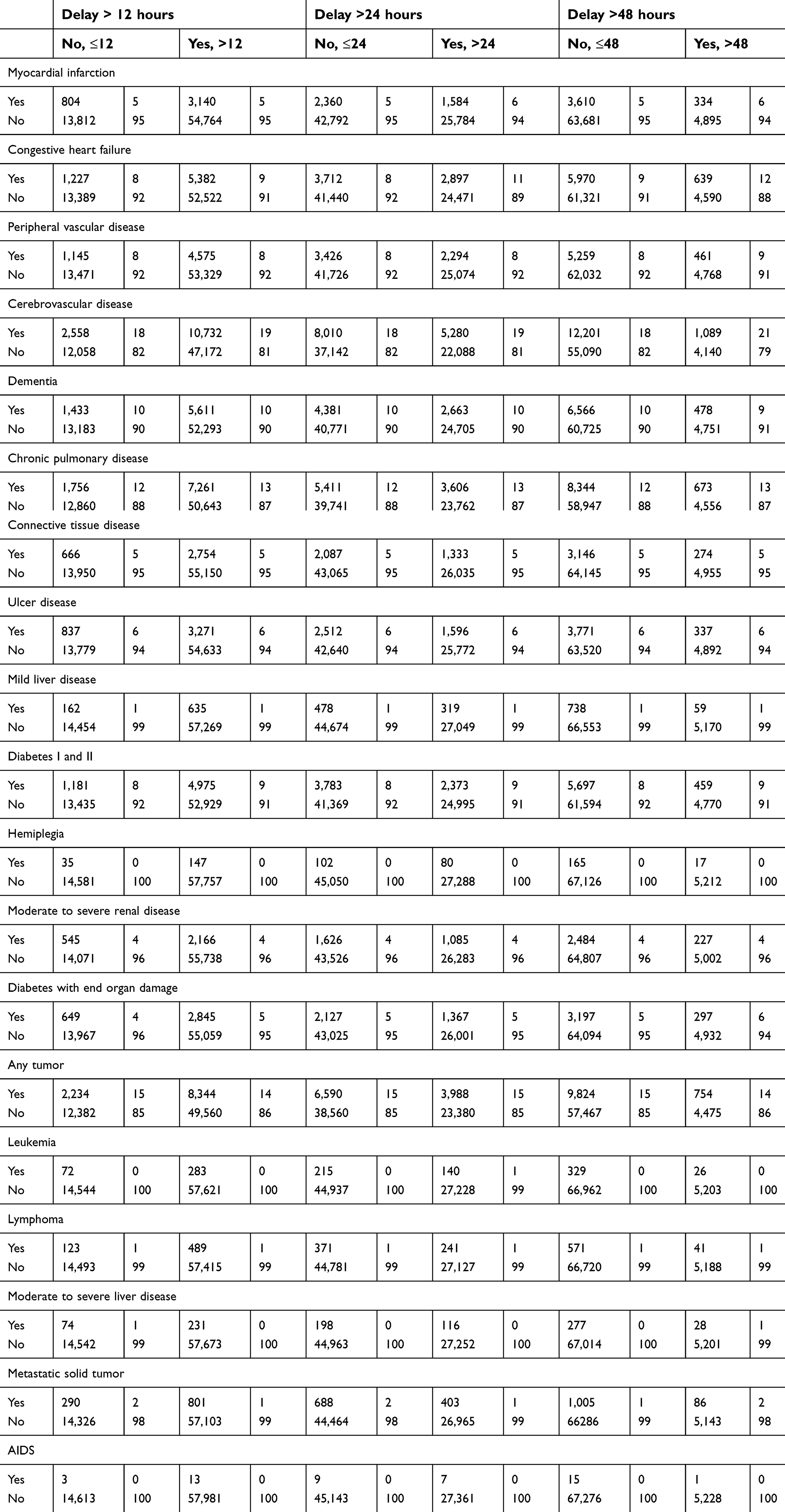 | The distribution of diseases from the Charlson index according to delay in surgery. All primary and secondary diagnoses included in the CCI and registered in relation to hospitalizations and outpatient visits over a ten-year period before the hip fracture form the basis for having (yes) og not having (no) a specific comorbid disease at the time of surgery. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.