")
Back to Journals » Infection and Drug Resistance » Volume 12
Deep-sequencing study of HCV G4a resistance-associated substitutions in Egyptian patients failing DAA treatment
Authors Amer F , Yousif MM , Hammad NM , Garcia-Cehic D, Gregori J , Rando-Segura A , Nieto-Aponte L, Esteban JI, Rodriguez-Frias F , Quer J
Received 7 May 2019
Accepted for publication 23 July 2019
Published 10 September 2019 Volume 2019:12 Pages 2799—2807
DOI https://doi.org/10.2147/IDR.S214735
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Fatma Amer,1 Monkez M Yousif,2 Noha M Hammad,1 Damir Garcia-Cehic,3,4 Josep Gregori,3–5 Ariadna Rando-Segura,6 Leonardo Nieto-Aponte,6 Juan Ignacio Esteban,3,4 Francisco Rodriguez-Frias,4,6 Josep Quer3,4
1Department of Medical Microbiology and Immunology, Faculty of Medicine, Medical College, Zagazig University, Zagazig, Egypt; 2Internal Medicine Department , Faculty of Medicine, Medical College, Zagazig University, Zagazig, Egypt; 3Liver Unit, Liver Disease Laboratory-Viral Hepatitis, Internal Medicine Department, Vall d’Hebron Institut Recerca (VHIR)-Hospital Universitari Vall d’Hebron (HUVH), Barcelona 08035, Spain; 4Centro de Investigación Biomédica en Red (CIBER) de Enfermedades Hepáticas y Digestivas (CIBERehd) del Instituto de Salud Carlos III, Madrid 28029, Spain; 5Business Development Department, Roche Diagnostics SL, Sant Cugat del Vallès, Barcelona 08174, Spain; 6Liver Pathology Unit, Department of Biochemistry and Microbiology, HUVH, Barcelona 08035, Spain
Correspondence: Josep Quer
Liver Unit, Liver Disease Laboratory-Viral Hepatitis, Internal Medicine Department, Vall d’Hebron Institut Recerca (VHIR-HUVH), Barcelona 08035, Spain
Tel +34 93 489 4034
Email [email protected]
Fatma Amer
Medical Microbiology and Immunology Department, Zagazig Faculty of Medicine, 9A, Road 275, New Maadi, Cairo, Zagazig, Egypt
Tel +20 122 313 4810
Email [email protected]
Purpose: To study resistance-associated substitutions using next-generation sequencing in Egyptian hepatitis C virus-infected patients failing direct-acting antiviral treatment.
Methods: The current study describes three cases of treatment failure in patients referred to Zagazig Viral Hepatitis Treatment Center (ZVHTC), Sharkia Governorate, Egypt. RAS were identified and characterized using deep sequencing. The first patient had breakthrough while receiving a daclatasvir (DCV)+sofosbuvir (SOF) regimen, patient 2 relapsed after treatment with DCV+SOF+ribavirin (RBV), and patient 3 relapsed after DCV+SOF therapy. A serum sample was collected from each patient at failure and sent to Vall d’Hebron Research Institute at Hospital Universitari Vall d’Hebron in Barcelona (Spain) for deep-sequencing study to identify and characterize the RAS present in the samples.
Results: The following were identified: L28M, L30S and L28M+L30S in patient 1, L30R in patient 2, and R155C, D168E, L28M, L30H, L30S, L28M+L30H, and L28M+L30S in patient 3.
Conclusion: To the best of our knowledge, this is the first report from Egypt of patients failing DAA-based therapy, describing the associated RAS. This information will be of help to understand the natural history of HCV in Egyptian patients and guide the proper choice of retreatment protocols.
Keywords: resistance-associated substitutions, RAS, subtype 4a, treatment failure, Egypt, direct acting antivirals, DAA
Introduction
Egypt has one of the highest prevalence rates of hepatitis C virus (HCV) infection worldwide. In 2008, the Egypt Demographic and Health Survey (EDHS) reported that nearly 10 million Egyptians were infected with this virus, whereas the 2015 EDHS identified a clear decline, reporting chronic HCV infection in only 6 million individuals.1 Nonetheless, this is a large number of cases, and it indicates that HCV remains a serious national health problem.2 A systematic review of HCV genotypes has reported limited diversity in Egypt, with dominance of genotype (GT) 4, accounting for 92.5% of cases (12.1% subtype 4a and 82.3% unknown subtypes), followed by 3.6% of GT1 cases, and 3.2% of mixed infections.3
It has become clear that the root causes for this high prevalence (4.5–6.7%) are strongly associated with poor compliance with infection prevention and control in both the hospital and community settings.4 In 2006, the Egyptian National Committee for Control of Viral Hepatitis (NCCVH) was established to set up and implement a national HCV control program. One of the Committee’s strategies was to provide affordable and accessible treatment, based at that time on pegylated interferon/RBV. In 2014, after successful negotiation between Gilead and the Egyptian Government represented by the NCCVH, the first direct-acting antiviral (DAA) drug, sofosbuvir (SOF) was introduced. Treatment regimens using this agent led to a sustained virological response (SVR) rate of 90%. In 2015 to 2016, new combinations were approved in Egypt to improve antiviral treatment and cover all patients chronically infected with HCV.5 The HCV program is continuously updated to open the prospect of future elimination of the disease in Egypt.
Real-life studies using DAA-based regimens in the Egyptian population have reported very few cases of the breakthrough and relapse categories of treatment failure. In this study, we report on 3 HCV subtype 4a-infected Egyptian patients who failed to respond to regimens of daclatasvir (DCV) + SOF with/without RBV. A RAS study was performed using deep-sequencing to investigate the patients’ RAS profile in targeted and non-targeted regions of the HCV proteins, NS3, NS5A, and NS5B.
Materials and methods
Patient samples
The original three serum samples were from HCV-infected patients who had failed DAA-based antiviral treatments in the Zagazig Viral Hepatitis Treatment Center (ZVHTC), Sharkia Governorate, Egypt. The study was approved by ZVHTC and the three patients signed an informed consent for participation. The RAS analysis was approved by the clinical research ethic committee of Hospital Universitari Vall d’Hebron. To perform the study of resistance-associated substitutions (RAS), one sample from each patient taken during 2018 at the time of failure was delivered on dry ice to Vall d’Hebron Research Institute at Hospital Universitari Vall d’Hebron (VHIR-HUVH) in Barcelona, for characterization using a next-generation sequencing (NGS) technique adapted to the MiSeq platform.
Definitions
For the present study, HCV viral breakthrough was defined as an increase in viral load at the end of antiviral treatment, even though HCV RNA had been undetectable during the treatment period. Viral relapse was defined as confirmed detectable HCV RNA levels during the post-treatment follow-up period in patients who had an undetectable HCV RNA level at the end of treatment.
Patient 1
Patient 1 was a 65-year-old diabetic woman with hypertension. She was receiving gliclazide and metformin to manage diabetes mellitus, and amlodipine and torsemide for hypertension. On ultrasound study, her gall bladder showed a thickened wall and internal calculi. There was no ascites, but splenomegaly was visualized (16.7 cm, superior to inferior axis). The superior mesenteric vein and splenic vein were enlarged (>10 mm), and the diameter of the portal vein was 13 mm. The portal venous flow was slow (<15 cm/sec), and showed reversal or to-and-fro flow. The patient was diagnosed with compensated liver cirrhosis and splenomegaly. Her condition was classified as Child Class A, with a Child Pugh (CP) score of 5 and MELD score of 9. The signs of liver cirrhosis included the following: surface nodularity, a generally coarse echotexture, segmental atrophy, caudate width:right lobe width ratio >0.65, and a reduction (<30 mm) in the transverse diameter of the medial segment (segment IV) of the left lobe. The body mass index (BMI) was 26.4, hemoglobin measured 13.3 g/dL, platelet count was 120×109/L, and total leucocyte count was 4.8×109/L. The international normalized ratio (INR) was 1.23. Serum albumin, total bilirubin, alanine transaminase (ALT), and aspartate transaminase (AST) levels were 3.9 g/dL, 0.91 mg/dL, 95 U/L, and 165 U/L, respectively. Alpha fetoprotein (AFP) concentration was 16 ng/mL, antinuclear antibodies (ANA) tested negative, and serum creatinine was 0.6 mg/dL.
On virological testing, HBsAg was negative and the virus was identified as HCV genotype 4a (G4a). HCV viral load in serum was 1,959,000 IU/mL, as determined by the TaqMan Real Time PCR assay (Roche Applied Science, Basel, Switzerland), which had a lower limit of detection of 15 I U/mL.
The patient had never received antiviral treatment (naïve) and was cirrhotic. She was referred to ZVHTC for treatment and was prescribed SOF (400 mg daily) plus DCV (60 mg daily) for 12 weeks (12 W), reporting good treatment adherence.
On HCV RNA monitoring at week 4 (4 W) of treatment, the virus was undetectable. At 12 W, the end of treatment (EOT), HCV RNA measured 393 IU/mL and at 12 weeks follow-up after stopping therapy (12 WFU), HCV RNA level was 707,999 IU/mL. The patient was retreated with SOF/DCV/RBV for 24 weeks and attained SVR.
Patient 2
Patient 2 was a 48-year-old man with a diagnosis of HCV cirrhosis and a history of liver encephalopathy attacks. He was referred to ZVHTC for treatment. The patient was treatment-experienced and had failed a 6-month course of SOF+RBV.
Ultrasonography showed an enlarged spleen (18 cm, superior to inferior axis), portal vein diameter of 11 mm, and signs of hepatic cirrhosis (surface nodularity, overall coarse and heterogeneous echotexture, segmental hypertrophy/atrophy, caudate width:right lobe width ratio >0.65, and a reduction in the transverse diameter (<30 mm) of segment IV of the left lobe. The BMI was 36.3. Blood tests showed a hemoglobin level of 13.6 g/dL, platelet count 88×109/L, and total leucocyte count 2.7×109/L. The INR was 1.28. Liver function tests yielded the following results: serum albumin 3.7 g/dL, total bilirubin 0.84 mg/dL, ALT 174 U/L, and AST 168 U/L. AFP measured 22 ng/mL, ANA tested negative, and serum creatinine was 0.93 mg/dL. The patient received a diagnosis of portal hypertension with splenomegaly and was classified as Child Class A, with a CP score of 6 and MELD Score of 9
On virological testing, HBsAg was negative and the virus was identified as HCV G4a. Prior to designing a second therapy, serum HCV viral load, measured with the same real-time PCR method described above, was found to be 725,245 IU/mL.
The patient was prescribed SOF (400 mg daily) plus DCV (60 mg daily) plus RBV (600–1000 mg daily, with dose adjustment according to tolerability) for 24 weeks. The patient reported good treatment adherence.
HCV Monitoring at 4 W, 12 W, and 16 W during treatment, 24W EOT, and 12 W after EOT (12 WFU) yielded the following viral load data: 132 IU/mL, undetectable viral load, undetectable viral load, undetectable viral load, and 865,000 IU/mL, respectively. The patient, who was diagnosed as having a relapse, ultimately died because of deteriorating liver function.
Patient 3
Patient 3 was a 58-year-old diabetic man receiving Humalog insulin. He had mild ascites. Ultrasonography showed an enlarged spleen (15.7 cm, superior to inferior axis), portal vein diameter of 14 mm, and signs of hepatic cirrhosis, including surface nodularity, overall coarse and heterogeneous echotexture, segmental hypertrophy/atrophy, caudate width:right lobe width ratio >0.65, and a reduction in the transverse diameter (<30 mm) of segment IV of the left lobe. The BMI was 29.5. Blood tests showed a hemoglobin level of 9.6 g/dL, platelet count 52×109/L, and total leucocyte count 1.4×109/L. The INR was 1.3. Liver function tests yielded the following results: serum albumin 2.5 g/dL, total bilirubin 1.8 mg/dL, ALT 35 U/L, and AST 73 U/L. AFP concentration was 9 ng/mL, ANA tested negative, and serum creatinine was 1 mg/dL. The patient was diagnosed as having decompensated cirrhosis, portal hypertension, splenomegaly, and mild ascites, and was classified as Child Class B, with a CP score of 8 and MELD score of 12.
On virological testing, HBsAg was negative and the virus was identified as HCV G4a. Prior to the start of retreatment, serum HCV viral load, measured with the same real-time PCR method described above, was found to be 9,285,197 IU/mL.
The patient had never received antiviral treatment (naïve). At ZVHTC he was prescribed SOF (400 mg daily) plus DCV (60 mg daily) plus RBV (600–1000 mg, with dose adjustments according to tolerability) for 12 weeks. He reported good treatment adherence.
HCV-RNA was monitored at 4 W, 12 W EOT, and 12 and 24 W follow-up after stopping therapy (12 and 24 WFU). On RT-PCR monitoring, HCV RNA was undetectable at 4 W, 12 W EOT, and 12 WFU. At 24 WFU, viral load was 402,020 IU/mL. He was diagnosed as having HCV relapse.
The patient’s clinical condition worsened, with recurrent attacks of hepatic encephalopathy, increasing ascites, and development of hepatic hydrothorax. The patient could not afford the cost of a liver transplantation. He has not been retreated and is currently under conservative treatment for liver failure.
Methods
A serum sample was collected from each patient at treatment failure and sent to Vall d’Hebron Research Institute at Hospital Universitari Vall d’Hebron (VHIR-HUVH, Barcelona) for deep-sequencing study. HCV RNA was obtained from 140 µL of serum by manual extraction using the QIAmp Viral RNA Mini Kit (Qiagen, Hilden, Germany) following the manufacturers’ instructions and avoiding contamination.6 A high-resolution HCV subtyping method was used to identify HCV subtype and mixed infections (infection with more than one subtype at the same time).7 The HCV NS3, NS5A and NS5B regions, which are targeted by DAAs, were amplified by RT-PCR-Nested using G4a-specific primers (Table 1).8 Reverse transcription and the first round of PCR amplification were performed with the Transcriptor One-Step RT-PCR Kit (Roche Diagnostics, Mannheim, Germany), using an annealing temperature of 55 ºC and 40 seconds of elongation during 35 cycles. The KAPA HiFi HotStart PCR Kit (KAPA Biosystems, Wilmington, Massachusetts, USA) was used for nested amplification, applying an annealing temperature of 55 ºC and elongation time of 15 seconds for a total of 30 cycles. The KAPA Library Preparation Kit for Illumina Platforms (KAPA Biosystems, Wilmington, Massachusetts, USA) was used to prepare the DNA library, and the SeqCap Adapter Kit A/B (Nimblegen, Roche, Mannheim, Germany) to label each patient’s amplified product. KAPA Pure Beads (KAPA Biosystems, Wilmington, Massachusetts, USA) were used at a 0.8:1 ratio for the purification steps. Deep sequencing on the MiSeq (Illumina) platform was performed using the MiSeq Reagent Kit v3 for 600 cycles (Illumina, San Diego, California, USA).
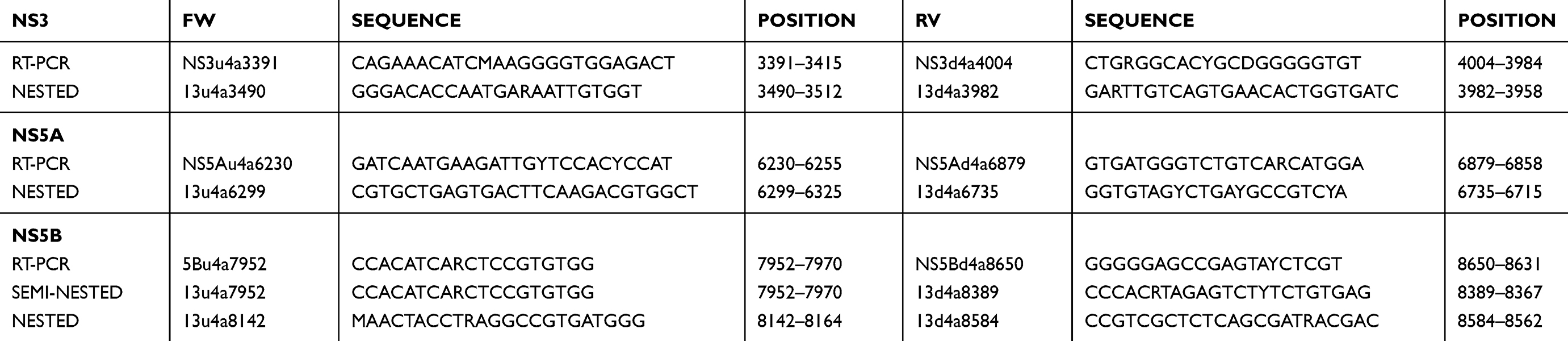 |
Table 1 Specific primers for G4a RT-nested-PCR amplifications of DAA-targeted regions NS3, NS5A and NS5B |
An in-house R script was used to obtain RAS reports from raw data after running the MiSeq in 2×300 mode.9 Additional details related to the RT-PCR-Nested amplification and deep-sequencing methodology can be found in a previous study.7
A bioinformatics haplotype-centric procedure was developed to filter and exclude reads with lower quality than a minimum requirement. The FLASH software program was used to overlap paired-end reads, establishing a minimum overlap between R1 and R2 of 20 bp, with a maximum of 10% differences. A detailed description of these steps can be found in the study by Soria et al.8
Because of the considerable intra-subtype diversity of HCV, 1068 sequences were retrieved from the Los Alamos databank to generate a consensus sequence (defined by the most frequent amino acid at each position) for subtypes G1a, G1b, G2c, G2i, G2j, G3a, G4a, and G4d to designate amino acid changes. All the reported amino acid changes were included in a final report, highlighting those changes that have been described as resistance associated substitutions compared to the G4a consensus sequence, but also including all other changes found in this study (Figure 1 and Table 2).
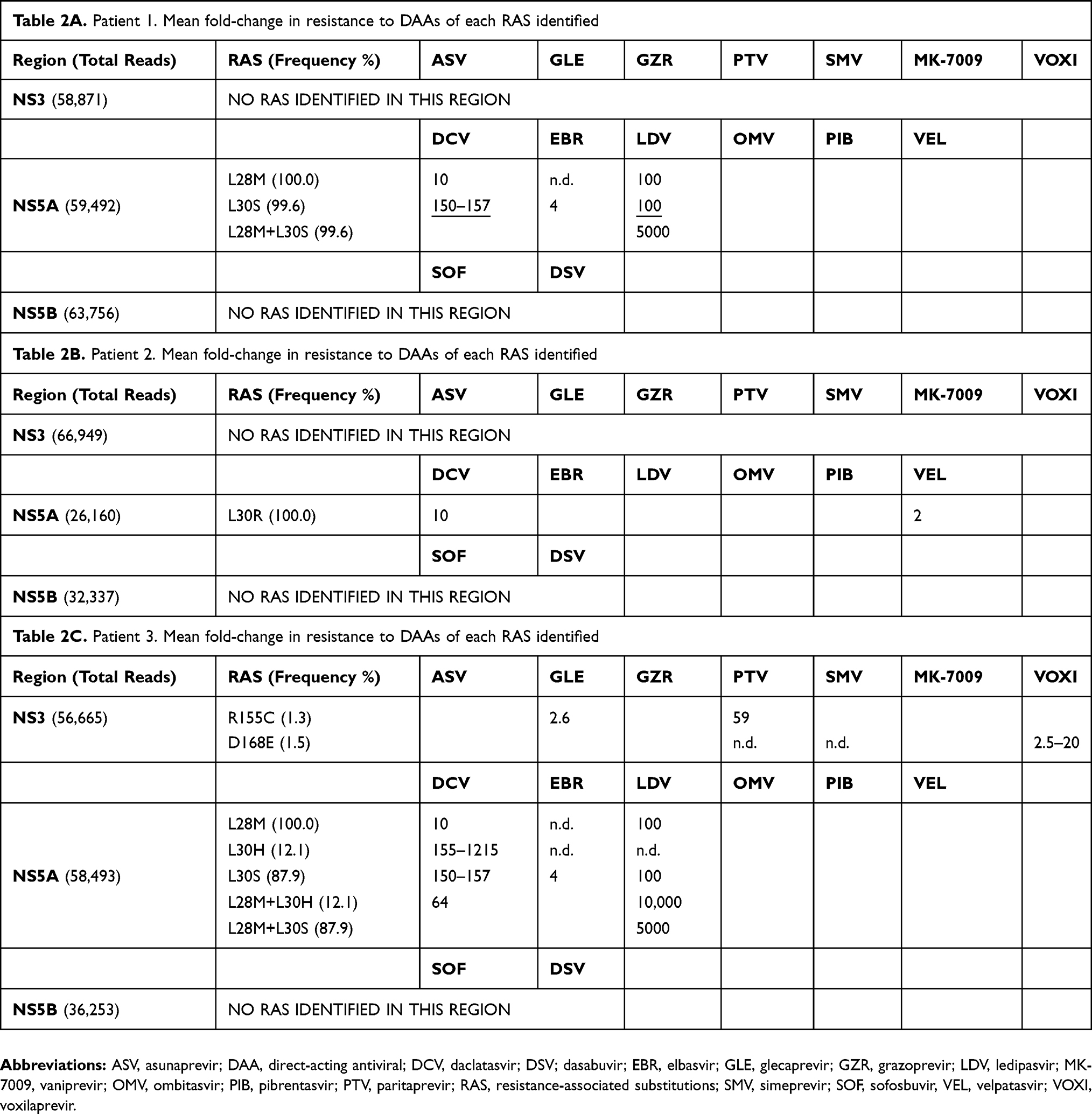 |
Table 2 Individual RAS and RAS combinations found in samples from patient 1 (Table 2A), patient 2 (Table 2B), and patient 3 (Table 2C). The tables show the frequency at which each substitution was observed (after passing the filter) in the total number of reads obtained for each region, and the mean fold-change in resistance compared to the wild type. Underlined values indicate the reported mean fold-change in resistance for the substitution independently of the wild-type amino acid |
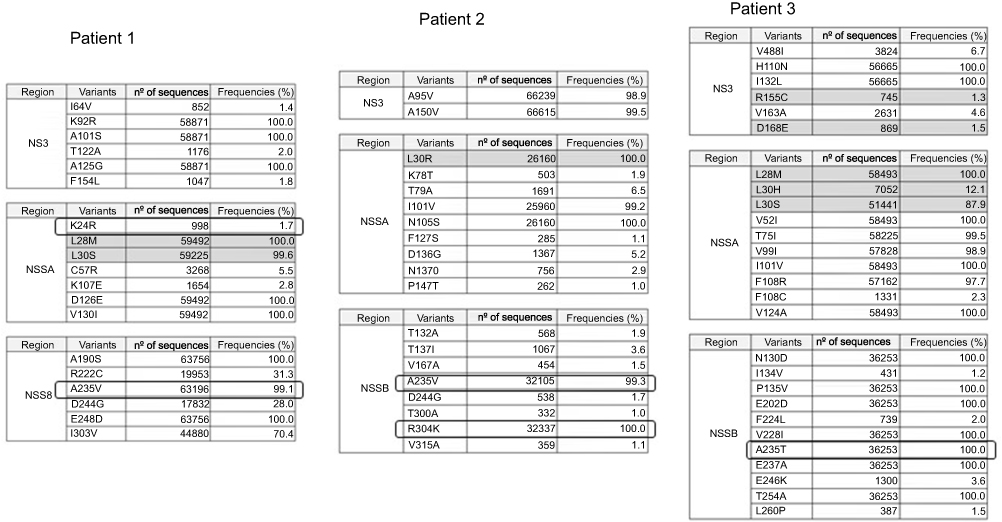 |
Figure 1 Amino acid substitutions found in samples from patients 1, 2, and 3 in the three HCV antiviral target regions, NS3, NS5A, and NS5B, compared to a subtype 4a consensus sequence retrieved from Los Alamos databank. For each patient and region we report (in columns) the region, the amino acid change, the number of reads (sequences) obtained, and the frequency of each substitution in the total reads obtained. Total reads: Patient 1, NS3 (58,871 reads), NS5A (59,492), and NS5B (63,756); Patient 2, NS3 (66,949); NS5A (26,160), and NS5B (32,337); Patient 3, NS3 (56,665), NS5A (58,493), and NS5B (36,253).Abbreviation: HCV, Hepatitis C virus. |
Results
The NS3, NS5A and NS5B sequences from the three patients have been deposited in the GenBank database with accession number “PRJNA554981”.
At 4 weeks of DAA-based treatment, patients 1 and 3 showed an early positive antiviral response, whereas patient 2 had a viral load of 132 IU/mL and continued treatment for 24 weeks.
Patient 1 tested HCV RNA-positive at EOT (12 W), with a value of 393 IU/mL, suggesting viral breakthrough. At 12 WFU, viral load had increased to 707,999 IU/mL. In the case of patient 2, HCV-RNA was undetectable at 12 W and 16 W during treatment, and at 24 W EOT. At 12 WFU, viral load was 865,000 IU/mL, reflecting viral relapse. Patient 3 had undetectable HCV-RNA at 12 W EOT, but 24 weeks later HCV relapsed to 402,020 IU/mL. All 3 patients were infected by G4a. No other subtypes were observed (no mixed infections).
The first and third patients failed DCV+SOF treatment. The second patient failed combination therapy with these two agents plus RBV. Deep-sequencing analysis was performed on the NS3, NS5A, and NS5B regions. Coverage (number of reads sequenced per amplicon) was between 26,160 and 66,949 reads per region per patient (Table 2).
RAS appeared in the NS5A region at residues 30 and/or 28 in all patients (Table 2). In 2 patients (patients 1 and 3), all viral genomes carried the L28M substitution, and in most genomes, this substitution was combined with L30S (Table 2A and C). Additionally, in patient 3, 12.1% of reads showed the L28M+L30H combination (Table 2C). RAS in residues 28 and 30 cause resistance to DCV, elbasvir, and ledipasvir. Moreover, RAS combination patterns in the same viral particle cause dramatically increased resistance to the inhibitor used in the failed treatment and in other inhibitors of the same family. For example, L28M+L30H cause a mean-fold resistance of 10,000 to ledipasvir (Table 2C). In patient 2, who had received RBV, the L30R RAS was observed alone (Table 2B), conferring resistance to DCV and velpatasvir.
Interestingly, deep-sequencing study showed two RAS (R155C and D168E) at very low frequencies (1.3% and 1.5%, respectively) in the non-targeted NS3 region in patient 3. R155C causes resistance to glecaprevir and paritaprevir, whereas D168E is associated with resistance to voxilaprevir, simeprevir, and paritaprevir (Table 2C). We also observed the minority substitution K24R (1.9%), which confers ledipasvir resistance in HCV G1a,10,11 but has an unknown RAS effect in G4a.
No RAS were observed in the NS5B region in any patient. However, alignment of the patients’ sequences with the consensus G4a sequence, composed of isolates downloaded from the Los Alamos database, identified two NS5B amino acid substitutions (A235V/T, R304K) with an unknown RAS effect. Specifically, all three patients were carrying the A235V substitution in almost all reads (99.3–100%), whereas R304K, reported at baseline in Portuguese G4a patients,12 was prevalent in patient 3.
Amino acid substitutions in patients 1, 2, and 3 in the three HCV antiviral target regions (NS3, NS5A, NS5B) compared to a subtype 4a consensus sequence retrieved from the Los Alamos databank are shown in Figure 1. For each patient and region we report (in columns) the region, the amino acid change, the number of reads (sequences) obtained, and the frequency of each substitution among the total reads obtained: patient 1, NS3 (58,871 reads in total), NS5A (59,492), and NS5B (63,756); patient 2, NS3 (66,949), NS5A (26,160), and NS5B (32,337); and patient 3, NS3 (56,665), NS5A (58,493), and NS5B (36,253).
Discussion
The recent introduction of DAA therapy has revolutionized the treatment of chronic HCV infection in several countries worldwide, including Egypt, with very high SVR rates in clinical trials and slightly lower rates in real-life cohorts.13 The emergence of HCV resistance variants (ie, RAS), is the main reason for this difference, but little information on resistance in G4a patients has been reported, as most studies include only a small number of patients with this subtype, and very few have been done using deep-sequencing.10,11,14,15 In this study, we report the RAS profile determined by this technique in Egyptian patients failing DAA-based treatments.
All samples were analyzed for RAS in the NS3, NS5A and NS5B proteins by deep-sequencing using the MiSeq (Illumina) platform. The rationale to study all three DAA-targeted regions was that extra-target mutations and hitchhiking mutations can be selected at failure and negatively impact salvage treatments. In this sense, two minority RAS (R155C and D168E) in the non-targeted NS3 region were observed in patient 3 at very low frequencies (1.3% and 1.5%, respectively) (Table 2C). Neither of these minority RAS would have been detected using population (Sanger) sequencing, and both of them could have reduced retreatment options.14,16 R155C causes resistance to glecaprevir and paritaprevir, whereas D168E confers resistance to voxilaprevir, simeprevir, and paritaprevir.10,11
The level of resistance to an inhibitor depends on several conditions: the genetic barrier to resistance of the HCV region, the drug used, the type of RAS, the frequency at which RAS are present in the viral isolate, and the presence of RAS combinations in the same viral particle, all of which can significantly increase resistance to some DAA treatments. RAS combinations in the same genome have been shown to cause a dramatic increase in resistance to the inhibitor used in the failed treatment and to other inhibitors of the same family.17 For example, L28M+L30H causes a mean-fold resistance of 10,000 to ledipasvir (Table 2C).
Our results show that L30R appeared alone in a patient who had received RBV, whereas other L30 substitutions seem to require combination with L28 mutations.16 This observation should be confirmed in additional patients to know whether it is an occasional finding or the rule. A deep-sequencing study in a large cohort of patients treated with and without RBV has just been completed, and this molecule did not have an influence on the type or number of RAS at HCV treatment failure (data not shown, paper in preparation).
Coinciding with the results of a previous study16 the L28M and L30 substitutions were the main RAS in G4a. However, in contrast to that same study18 in which L30R was the majority substitution, L30S was the most prevalent in our patients. The RAS pattern in G4a was completely different from that of G4d, the most prevalent G4 subtype in Spain, in which the most common RAS was T58P (data not shown, paper in preparation). Moreover, NS5A polymorphisms at Y93 (Y93H/S/T) were not identified in the 3 patients failing therapy, in agreement with previous studies.11,18 Additional studies are needed to demonstrate whether or not A235V/T and R304K in the NS5B protein and K24R in NS5A are resistant to the inhibitors. Other highly prevalent substitutions observed in our study, such as A150V in NS3,19 V52I, T75I, V99I, I101V,20 N105S, F108R/C, V124A, D126E,21 and V130I,20 in NS5A, and N130D, P135V, A190S, E202D,20 V228I, E237A, E248D, and T254A in NS5B should still be considered simple polymorphic substitutions without resistance implications, requiring further study. As there are few studies on RAS emerging in patients failing DAA treatment, more work is needed to determine whether any newly described substitutions can be classified as RAS, as adaptive mutations, or as random occurrences.
To our knowledge, this is the first study investigating resistance-associated substitutions using next-generation sequencing in Egyptian HCV-infected patients failing DAA treatment. Deep sequencing-based studies of the three antiviral targeted regions facilitate identification of major and minor substitutions, the frequency at which they are present in the viral isolate, and whether or not they are combined with others in the same viral genome. This information is useful for designing successful retreatment strategies, and is of particular importance in the absence of next-generation HCV treatments incorporating pangentotypic22 DAAs that will be effective in Egypt and other parts of the world having a high GT4 burden. Until future pangenotypic DAAs become affordable, accessible, and easily provided, a scenario that may not materialize for several years, precise identification of RAS leading to treatment failure is of value for better patient management, offering the possibility of improved quality of life.
In view of lack of facilities or very high cost of RAS testing in Egyptian laboratories together with the huge number of patients treated daily, the NCCVH recommends empirical retreatment of patients who fail NS5A inhibitor-based therapy with a combination of HCV multitargeted drugs. Quadruple therapy with sofosbuvir, daclatasvir, and simeprevir plus ribavirin (SOF/DCV/SMV/RBV) or sofosbuvir, ombitasvir, paritaprevir, and ritonavir plus ribavirin (SOF/OBV/PTV/r/RBV) for 12 weeks is recommended for these patients, provided they have neither decompensated liver function nor an estimated glomerular filtration rate (eGFR) below 30 mL/min/1.73 m2 body surface area.23 The efficacy and safety of SOF/OBV/PTV/r/RBV quadruple therapy has been assessed in chronic HCV GT4 patients failing DAA-based regimens in Egypt. SVR was achieved in 97% (109/113) of patients with good tolerability and safety of the drug combination.23 The same group of researchers conducted another study using SOF/DCV/SMV/RBV in a similar cohort of Egyptian patients, and reported similar efficacy (SVR 97%) and safety results.24 However, the studies from Egypt are limited and include relatively small patient samples. Efficacy and safety analyses of data from the Egyptian NCCVT in patients using these DAA combinations are needed. In July 2017 the Food and Drug Administration (FDA) approved a regimen consisting of a fixed-dose combination of sofosbuvir, velpatasvir and a second-generation HCV-protease inhibitor, voxilaprevir, for retreatment of HCV GT 1–6 after failure with sofosbuvir or other NS5A inhibitors without RAS testing.25 Again, clinical trials are needed to assess the efficacy and safety of these new generations of DAAs in Egyptian patients. Until these pangenotypic DAAs become affordable, accessible, and easily provided in Egypt’s market based on clinical proof of better safety and efficacy, a scenario that may not materialize for several years, precise identification of RAS leading to treatment failure is of value for better patient management, providing the possibility of improved quality of life.
Consent for publication
Written informed consent was obtained from the cases included in the study
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
Acknowledgments
This study was supported by the Spanish Ministry of Health, Consumer Affairs, and Social Welfare, grant name: Plan Estratégico Nacional contra la Hepatitis C. This study was also funded by Instituto de Salud Carlos III, PI15/00856 and PI16/00337, cofinanced by CIBERehd (Consorcio Centro de Investigación en Red de Enfermedades Hepaticas y Digestivas), which is funded by Instituto de Salud Carlos III and Centro para el Desarrollo Tecnológico Industrial (CDTI) from the Spanish Ministry of Economy and Business, grant number, IDI-20151125. The authors thank Celine Cavallo for English language support and helpful editing suggestions.
Disclosure
The funder, Roche Diagnostics S.L., provided support in the form of salaries for one author (Josep Gregori), but the company did not have any additional role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors report no other conflicts of interest in this work.
References
1. Health M. Population/Egypt, El-Zanaty, Associates/Egypt, ICF International. Egypt Health Issues Survey 2015 Cairo. Egypt: Ministry of Health and Population/Egypt and ICF International; 2015.
2. Amer FA. Large-scale hepatitis C combating campaigns in Egypt and Georgia: past, current and future challenges. J Infect Dev Countries. 2018;12:404–414. doi:10.3855/jidc.9784
3. Kouyoumjian SP, Chemaitelly H, bu-Raddad LJ. Characterizing hepatitis C virus epidemiology in Egypt: systematic reviews, meta-analyses, and meta-regressions. Sci Rep. 2018;8:1661. doi:10.1038/s41598-017-17936-4
4. Amer FAGM, Gohar M. Epidemiology of hepatitis C virus infection in Egypt. Int J Trop Dis. 2015;7:119–131. doi:10.9734/IJTDH
5. El-Akel W, El-Sayed MH, El Kassas M. National treatment programme of hepatitis C in Egypt: Hepatitis C virus model of care. J.Viral Hepat. 2017;24:262–267.
6. Kwok S, Higuchi R. Avoiding false positives with PCR. Nature. 1989;339:237–238. doi:10.1038/339237a0
7. Quer J, Gregori J, Rodriguez-Frias F, et al. High-resolution hepatitis C virus subtyping using NS5B deep sequencing and phylogeny, an alternative to current methods. J Clin Microbiol. 2015;53:219–226. doi:10.1128/JCM.02093-14
8. Soria ME, Gregori J, Chen Q, et al. Pipeline for specific subtype amplification and drug resistance detection in hepatitis C virus. BMC Infect Dis. 2018;18:446. doi:10.1186/s12879-018-3109-6
9. Team RC. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2016.
10. Lontok E, Harrington P, Howe A, et al. Hepatitis C virus drug resistance-associated substitutions: state of the art summary. Hepatology. 2015;62:1623–1632. doi:10.1002/hep.27934
11. Sorbo MC, Cento V, Di MV, et al. Hepatitis C virus drug resistance associated substitutions and their clinical relevance: update 2018. Drug Resist Update. 2018;37:17–39. doi:10.1016/j.drup.2018.01.004
12. Palladino C, Ezeonwumelu IJ, Marcelino R, et al. Epidemic history of hepatitis C virus genotypes and subtypes in Portugal. Sci Rep. 2018;8:12266. doi:10.1038/s41598-018-30528-0
13. Kanda T, Matsuoka S, Moriyama M. Hepatitis C virus genotype 4-infection and interferon-free treatment in Egypt. Hepatol Int. 2018;12:291–293. doi:10.1007/s12072-018-9883-9
14. Easl. EASL recommendations on treatment of hepatitis C 2018. J Hepatol. 2018;69:461–511. doi:10.1016/j.jhep.2018.03.026
15. Sarrazin C. The importance of resistance to direct antiviral drugs in HCV infection in clinical practice. J Hepatol. 2016;64:486–504. doi:10.1016/j.jhep.2015.09.011
16. Perales C, Chen Q, Soria ME, et al. Baseline hepatitis C virus resistance-associated substituions present at frequencies lower than 15% may be clinically significant. Infect Drug Resist. 2018;11:2207–2210. doi:10.2147/IDR.S172226
17. Hezode C, Hirschfield GM, Ghesquiere W, et al. Daclatasvir plus peginterferon alfa and ribavirin for treatment-naive chronic hepatitis C genotype 1 or 4 infection: a randomised study. Gut. 2015;64:948–956. doi:10.1136/gutjnl-2014-307498
18. Zhou N, Hernandez D, Ueland J, et al. NS5A sequence heterogeneity and mechanisms of daclatasvir resistance in hepatitis C virus genotype 4 infection. J Infect Dis. 2016;213:206–215. doi:10.1093/infdis/jiv379
19. Svarovskaia ES, Dvory-Sobol H, Parkin N, et al. Infrequent development of resistance in genotype 1–6 hepatitis C virus-infected subjects treated with sofosbuvir in phase 2 and 3 clinical trials. Clin Infect Dis. 2014;59:1666–1674. doi:10.1093/cid/ciu697
20. Minosse C, Selleri M, Giombini E, et al. Clinical and virological properties of hepatitis C virus genotype 4 infection in patients treated with different direct-acting antiviral agents. Infect Drug Resist. 2018;11:2117–2127. doi:10.2147/IDR.S179158
21. Marascio NPGGF, Salvo S, Reale M, et al. Real-word efficacy of HCV subtype 4d treatments: clinical cases. In: 46̊ Congresso Nazionale Della Societa Italiana Di Microbiologia. Palermo: Fondazione Sant’Elia. 26–29 September 2018. Societa Italiana Di Microbiologia.
22. Vermehren J, Park JS, Jacobson IM, Zeuzem S. Challenges and perspectives of direct antivirals for the treatment of hepatitis C virus infection. J Hepatol. 2018;69:1178–1187. doi:10.1016/j.jhep.2018.07.002
23. Abdel-Moneim A, Aboud A, bdel-Gabbar M, Zanaty M, Ramadan M. Retreatment efficacy of sofosbuvir/ombitasvir/paritaprevir/ritonavir + ribavirin for hepatitis C virus genotype 4 patients. Dig Dis Sci. 2018;63:1341–1347. doi:10.1007/s10620-018-5005-8
24. Abdel-Moneim A, Aboud A, bdel-Gabbar M, Zanaty MI, Ramadan M. A sofosbuvir-based quadruple regimen is highly effective in HCV type 4-infected Egyptian patients with DAA treatment failure. J Hepatol. 2018;68:1313–1315. doi:10.1016/j.jhep.2018.03.010
25. (FDA) USFaDA. FDA approves Vosevi for Hepatitis C; March 28, 2018. Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-vosevi-hepatitis-c. Accessed August 30, 2019.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.