")
Back to Journals » Open Access Journal of Contraception » Volume 11
Decision-Making Power of Married Women on Family Planning Use and Associated Factors in Dinsho Woreda, South East Ethiopia
Authors Dadi D , Bogale D, Minda Z , Megersa S
Received 30 July 2019
Accepted for publication 12 January 2020
Published 7 February 2020 Volume 2020:11 Pages 15—23
DOI https://doi.org/10.2147/OAJC.S225331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Dinku Dadi,1 Daniel Bogale,2 Zenebe Minda,2 Sintayehu Megersa3
1Madda Walabu University, Bale-Robe, Ethiopia; 2Department of Public Health, School of Health Sciences, Madda Walabu University Goba Referral Hospital, Bale-Goba, Ethiopia; 3Bale Zone Health Department, Bale-Robe, Ethiopia
Correspondence: Dinku Dadi P.O. Box, 243, Bale-Robe, Ethiopia
Tel +251911771873
Email [email protected]
Background: Women’s decisions on family planning use have multiple benefits to the family and community at large. In developing countries like Ethiopia, the choice of women to use a contraceptive is challenged by social and environmental factors that mitigate their ability to decide independently and freely. This study therefore determined the level of women’s decision-making power on family planning use and associated factors among married women in the study area.
Methods: A community-based cross-sectional study was conducted in Dinsho woreda from March to April 2017. A simple random sampling technique was used to select 373 married women. A structured and pre-tested questionnaire was used to collect data by trained data collectors under continuous supervision. Multivariable logistic regression was performed to identify factors associated with women’s decision-making power on family planning use. Crude and adjusted odds ratios with 95% confidence interval were used and p-value of < 0.05 was considered as statistical significance.
Results: A total of 344 (92.2%) women participated in the study. Of the total respondents, 179 (52%) of women had good decision-making power on modern family planning use. Multivariable analysis showed that younger age (adjusted odds ratio [AOR] =8.59 [1.61, 45.80]), good participation in household decision-making (AOR =2.65 [1.46, 4.79]), positive attitude towards family planning (AOR =2.34 [1.31, 4.19]), and better knowledge towards family planning (AOR =3.04 [1.49, 6.22]) were factors statistically significantly associated with married women’s decision-making power on family planning use.
Conclusion and Recommendation: Women’s knowledge and attitudes toward family planning and their participation in household decision-making increased the likelihood of women’s decision-making power for modern family planning use. There is a need to adopt a more comprehensive approach to reach men and women on modern family planning, to help women to decide freely without any restriction.
Keywords: family planning, participation in household decision-making, knowledge, attitude
Introduction
Worldwide, in 2015, 64% of married or in-union women of reproductive age were using some form of contraception. Family planning allows women to reduce unintended pregnancies and it also reduces the need for unsafe abortion.1 Likewise, it is an important component of reproductive health because it helps people to have the desired number of children, which directly improves the health of mothers.2,3 Women have been playing a key role, not only in the improvement of family wellbeing but also in the development of the economic, political, social and ecological environments.4
An estimated 225 million people in developing countries would like to delay or stop childbearing but are not using any method of contraception. In the least developed countries, contraceptive use was much lower (40%) and was particularly low in Africa (33%).1 Family planning use in developing countries is challenged by social and environmental factors that mitigate their ability to decide independently and freely.5,6 In Ethiopia, men are dominant decision-makers in most family matters, including reproductive health issues.7,8 Lack of women decision-making on the use of family planning leads to an unplanned pregnancy and unsafe abortion that will affect maternal health and their children health.9
According to the Ethiopian demographic and health survey (EDHS) 2016 report, maternal mortality ratio was 412 deaths per 100,000 live births and the infant mortality rate was 28 per 1,000 live births. However, the total fertility rate (TFR) was 4.6 and only 36% of currently married women are using a method of family planning.10 Women’s decision on modern family planning use has multiple benefits to the family and community at large. Decision-making power of women in family planning defined as a woman ability to freely decide individually or discuss with their partners about family planning needs and choices.8 Therefore, efforts need to be made for women involvement in family planning either to use the contraceptives or to support each other on when to start and stop the contraceptive and thereby regulate their fertility.8,11
There are limited studies that documented on assessing factors associated with married women’s decision-making power on family planning in the study area. Identifying the level of women’s decision-making power in family planning use at the household level and identifying associated factors has paramount importance for designing a targeted program in the study area. Besides, it could also be used as input for policymakers and programmer managers of the study area in the field of contraceptive uses and women decision-making. Therefore, the result of this study determined the level of women’s decision-making power in family planning use and associated factors among married women in Southeast Ethiopia.
Materials and Methods
Study Setting
Dinsho Woreda is found at the Southeast of the country at 400 km from Addis Ababa. Bale mountain national park is also found in this woreda with different animals some of them are only found in this park. Currently, there are three health centers and eleven health posts in this wereda. The woreda has ten kebeles (the lowest administrative unit) and one rural town.
Study Design and Population
The study was conducted from March to April 2017. A community-based cross-sectional study was employed. All married women of reproductive age group (15–49 years) who are residing in the study area were the source population. The study populations were all married women of reproductive age group (15–49 years) in the selected kebeles.
Inclusion and Exclusion Criteria
Married women who live in the study area who are fecund at a time of data collection were included. Women who are incapable of responding to the questions due to serious health problems were excluded.
Sample Size Determination and Sampling Techniques
The sample size is determined using single population proportion formula by considering 95% confidence interval, 5% tolerated sampling error and taking the level of decision-making power on contraceptive use from a study done in Mizan-Aman which is 67.2%.12 The final sample size after adding a 10% non-response rate was 373.
A simple random sampling technique was employed to select participants. From a total of eleven kebele found in the woreda four kebeles (36%) were selected by using simple random sampling technique. Then after, the total sample size (373) was proportionally allocated to each selected kebele based on the number of households it has. Data on the population of married women in reproductive age in each kebele were obtained from the health post family folder. Therefore, simple random sampling method was used to select sample population that was included in the study from the sampling frame.
Data Collection Instruments and Technique
The questionnaire was developed from EDHS 2011, women empowerment scale and from related literatures.13,14 It was modified according to the local context by the investigators. Data were collected face to face by four trained diploma female clinical nurses and midwifery nurses who work in another area (other than study area) and speak both Amharic and Afan Oromo. The reason for selecting female data collector was for ease of communication during data collection since the study participants were female who may easily communicate with female health workers. Two recruited supervisors who speak Afan Oromo language and degree holder conducted supervision during the entire data collection period.
Study Variables
Dependent Variable
Married women's decision-making power on family planning use.
Independent Variables
Socio-economic and demographic factors – age of women, family monthly income, education and occupation status of the women and the husband, exposure to media, and total family size.
Women’s participation in household decision-making – related to decision-making on husband’s earnings are used, major household purchases, visits to family, friends, or relatives, women’s healthcare, children’s healthcare, visiting a health facility.
Reproductive history: number of pregnancies, age at first pregnancy, number of live births and stillbirth, abortion history, total no. of children ever born and need for more children.
Attitude towards family planning use and Knowledge towards family planning use.
Operational Definition
Married women's decision-making power on family planning use: measured in relation to women's ability to freely decide individually or decide jointly with their partners about family planning needs and choices using six questions. A score of 1 was given if women decided independently or together and a score of zero (0) was scored by partners who decided independently, or decision was made by others. A woman who scored below the mean was considered as having no decision-making power, and those who scored greater or equal to the mean were considered as having good decision-making power.12
Women’s participation in household decision-making is assumed to be reflective of couple’s ideologies regarding gender roles in the family affairs. A score of 1 was given if women decided independently or together and a score of zero (0) was scored by partners who decided independently or decision was made by others. A woman who scored below the mean was considered as having no participation in household decision-making, and those who scored greater or equal to the mean was considered as having good participation in household decision-making.9,15
Knowledge on family planning: Knowledge of contraceptive method was measured by using ten questions, all are related to contraceptive methods, and having correct answers for at least 70% were considered as better knowledge on family planning otherwise not better knowledge.15
Attitudes on family planning: Three Likert scale items were used to measure attitude to a contraceptive method with a possible response of (agree, disagree or neutral). A score above 70% was considered as having a positive attitude otherwise considered as negative attitude.8
Data Quality Assurance
The data collection tool was first prepared in English and translated to local language (Afan Oromo) and then translated back to English to check its consistency. The process of translation was done by language experts. A pretest was done on 5% of the sample size in Sinana woreda after giving training for data collector and necessary corrections were made accordingly. Cronbach's alpha was calculated and found out to be 0.85, which grantee the reliability of the instruments.
Method of Data Analysis
Raw data were coded, entered, cleaned and analyzed using SPSS statistical software package version 20. Descriptive statistics such mean, percentage and frequency table were computed to summarize data. Bivariate and multivariable analysis were done to identify independent factors associated with women's decision-making power on family planning use. Crude and adjusted Odds ratios with 95% confidence intervals (CIs) were used to determine significance association and p-value < 0.05 were considered as a statistical significance.
Ethical Consideration
Before data collection ethical clearance was obtained from Madda Walabu University Goba referral hospital public health department. A formal letter of permission was obtained from the administrative bodies of the Woreda and kebele. Participation in the study was on voluntary bases and they were informed about the right not to participate or withdraw at any time. Confidentiality was assured for the information provided and finally, informed verbal consent was obtained from every study participant takes part in the study during data collection time after explaining the general outcome and results of the study.
Results
A total of 344 women responded to the questionnaire, yielding a response rate of 92.2%.
Socio-Economic and Demographic Characteristics of Respondents
The total family size of the respondents ranges from 1 to 13 with mean 6.3 and standard deviation ±2.99. The mean age of the respondents was 31.44 with standard deviation ±7.783. Most of the respondents were in the age group of 25–34 years with an age range from 18 to 49 years. Ninety-two percent of the respondents were Oromo in ethnicity and 262 (76%) were followers of the Muslim religion. Regarding the educational status of the spouses, 131 (38.1%) of women and 118 (34.3%) of husbands have not attended formal education. From total respondents, 233 (68%) and 243 (71%) had television and radio, respectively. From those who had television, 143 (61%) of them watch daily and from those who have a radio, 139(40%) of them listen daily.
Women’s Participation in Household Decision-Making
Half of the participants decide on their husband earning and on household purchases jointly. The study revealed that 16% of participants made decision related to visiting family, friend or relatives jointly with their husband. Surprisingly, one-third of the husbands decide on women's health independently, and 210 (61%) of the women decide on their children health with their husbands. Again, half of the respondents reported to decide visiting health facility jointly. Overall, 193 (56%) of married women in the study area have good participation in household decision-making (Table 1).
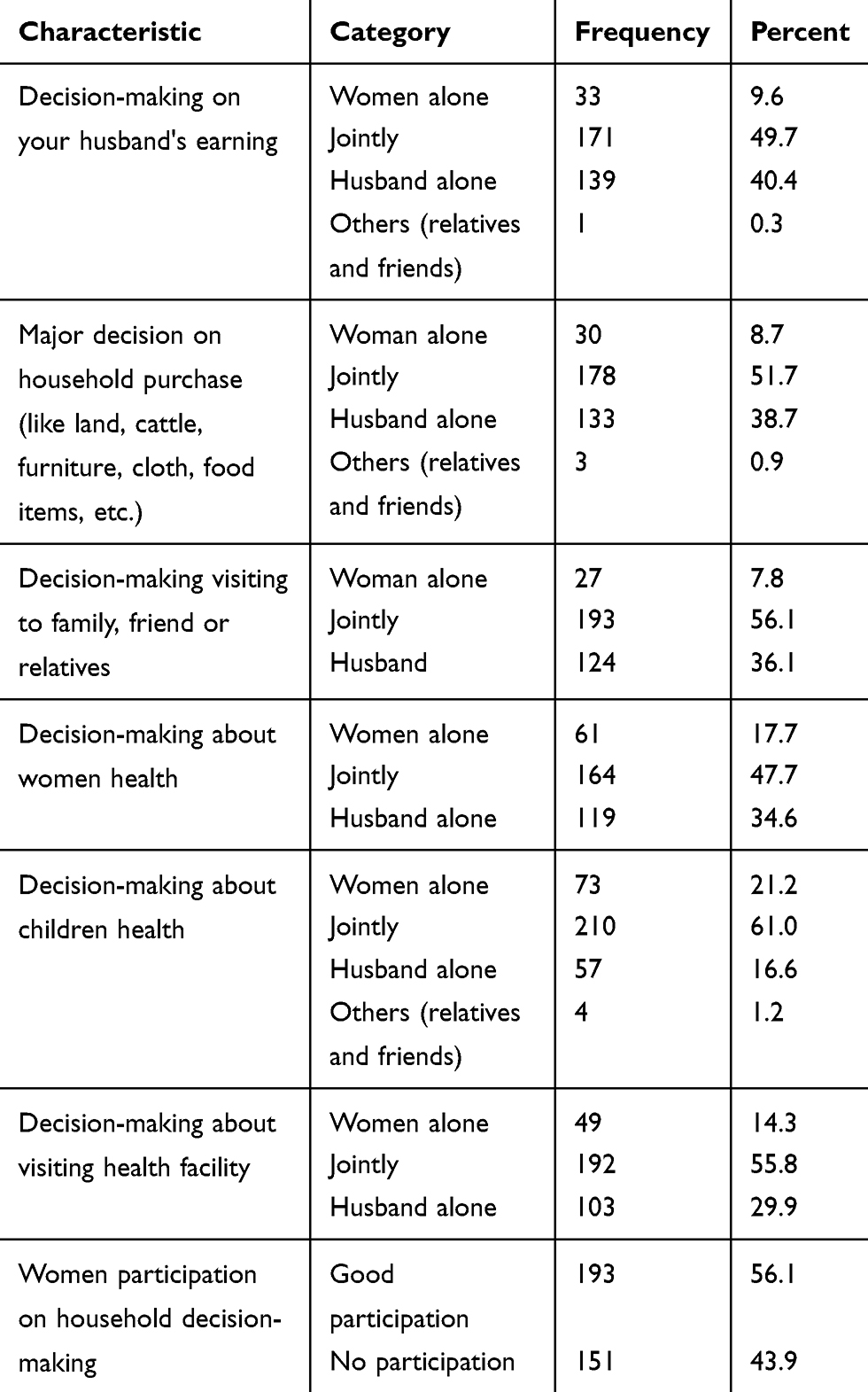 |
Table 1 Women’s Participation in Household Decision-Making in Dinsho Woreda, 2017 |
Reproductive History
In this study, 169(49%) and 247(72%) of the married women have been current and ever modern contraceptive users, respectively. From those who stop using contraceptive 41 (16.6%) reasoned that they stop using because of their husband dominance. From those married women who have had pregnancy 35 (10%) experience abortion and 8 (2.4%) where have stillbirth only once in their life. Two-third (210) of respondents reported that they have desire to have children.
Attitude and Knowledge Related to Family Planning
In this study, 310 (90%) of respondents agree on children will have a better opportunity, if the parent use contraceptive and 306 (89%) of them agree that family planning will help to improve one's standard of life. One-third of women disagree with the idea “if a woman who has many children looks tired and wear out”. More than half of the participant 191 (55.5%) agree that family planning cause loss of confidence between wife and husband and almost half percent of the respondents agree with the idea “wife’s who use family planning abandoned by her husband”. Again, most of the respondents 302 (88%) of married women agree that a woman needs her husband’s permission to use family planning. Generally, 134 (39%) of married women in the study area had a positive attitude towards contraceptive use (Table 2).
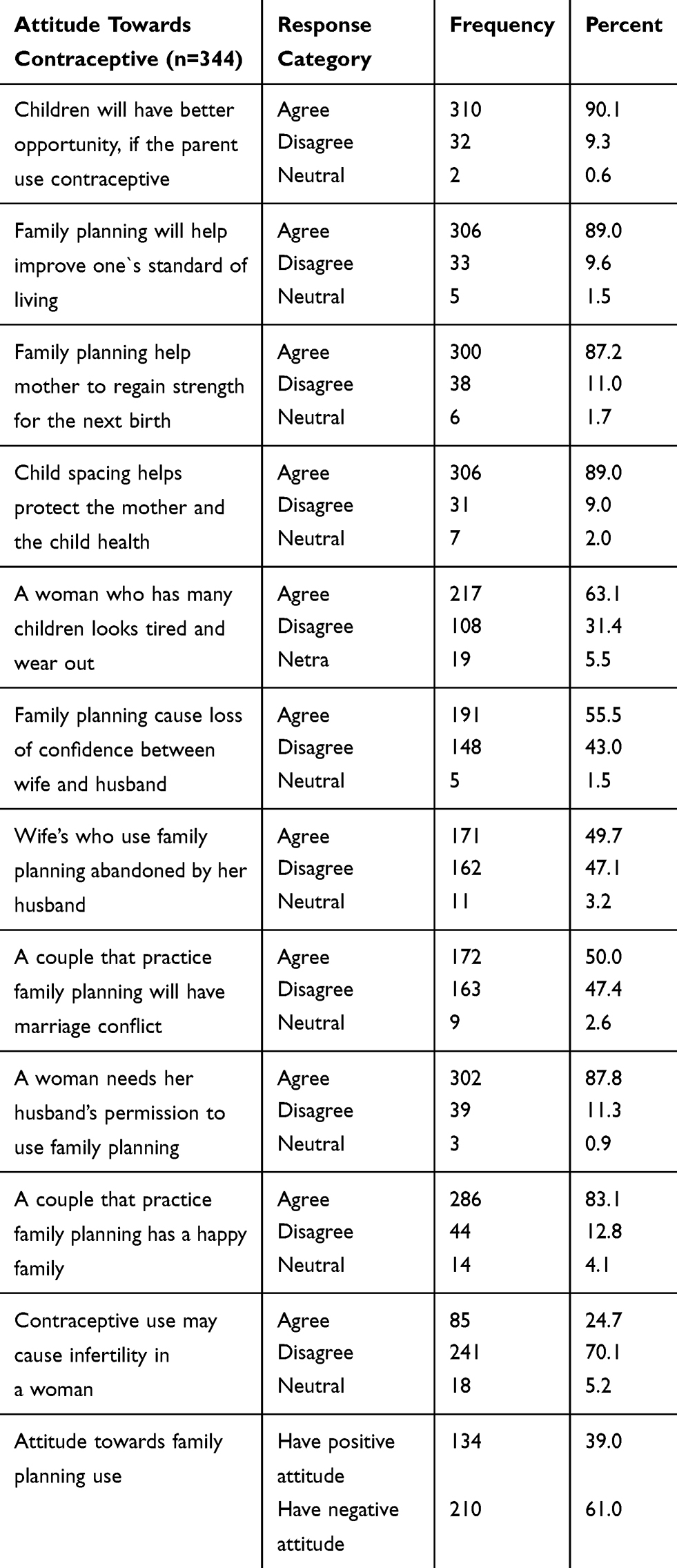 |
Table 2 Married Women Attitude Towards Family Planning Use Dinsho Woreda, 2017 |
Regarding knowledge of the study participants, 310 (90%) of them heard of modern contraceptives. Three hundred seventeen (92.2%) of study participants know about the importance of family planning. Regarding the side effect of using a modern contraceptive, 243 (70.6%) of women know the side effect of using a modern contraceptive. The most mentioned side effect is a headache 161(66.3%) next to irregular menstruation 173 (71%). Two hundred sixty (63%) of women discuss family planning with their husband and only 132 (38.4%) of study participants ever heard about emergency contraception. Generally, from total respondents, 187 (57.3%) of women have better knowledge regarding family planning (Table 3).
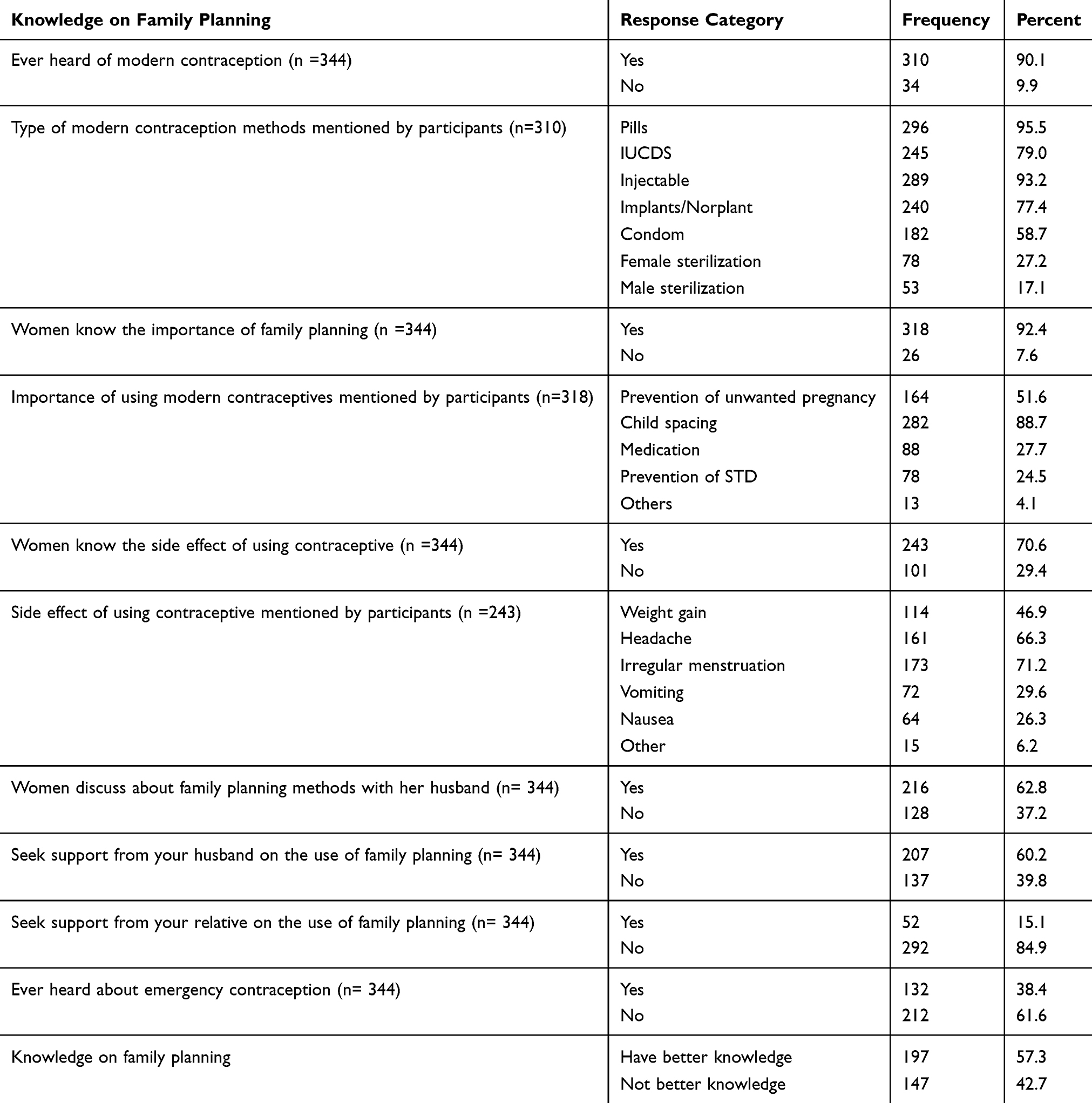 |
Table 3 Knowledge on Family Planning of Married Women in Dinsho Woreda, 2017 |
Women Decision-Making Power on Family Planning
The findings of this study showed that half of the study participants decide jointly on the number of children the family could have, and one-third woman could decide on the choice of family planning independently. Regarding decision on when to give births and where to get family planning service 160 (46.5%) and 128 (37.2%) decision is made jointly by women and husband, respectively. Regarding decisions related to seeking reproductive health services, the majority is made by husband 136 (39.5%) whereas 134 (39%) of married women decide jointly with their husband on continuation or stopping using/intending family planning. Generally, 179 (52%) of married women have good decision-making power on family planning in the study area (Table 4).
 |
Table 4 Married Women Decision-Making Power on Family Planning Use in Dinsho Woreda, 2017 |
Multivariable Analysis of Factors Associated with Married Women Decision-Making Power on Family Planning Use
Variables in the bivariate analysis of socio-economic, reproductive history of women, attitude and knowledge towards contraceptive as well as women participation in household decision-making with respect to women decision-making power on family planning; which were found at p-value ≤ 0.2 were further considered into multivariate analysis.12 Finally, in the multivariate logistic regression age of women, women participation in household decision-making, attitude towards family planning, knowledge towards family planning remained significantly associated with women’s decision-making power in family planning use.
Women age 18–20 years of age were 8.6 times more likely to have decision-making power on family planning use when compared to women age 35 and above; adjusted odds ratio (AOR) =8.59 (95% CI: 1.61, 45.80). The odds of decision-making power of women on family planning use were 2.6 times higher among women who have good participation in household decision-making when compared to their counterparts; AOR= 2.65 (95% CI: 1.46, 4.79). Women who have better knowledge on family planning were 3 times more likely to have decision-making power on family planning use than women who didn't have knowledge on family planning; AOR =3.04 (95% CI: 1.49, 6.22). In addition, women who have a positive attitude on family planning were 2.3 times more likely to have decision-making power on family planning than women who have negative attitude towards family planning as shown in Table 3; AOR =2.34 (95% CI: 1.31, 4.19) (Table 5).
 |
Table 5 Multivariable Logistic Regression on Women Decision-Making Power on Family Planning Use in Dinsho Woreda, 2017 |
However, variables that were having significant association with the dependent variable in the bivariate analysis like monthly income, current family planning users and family who have television were not showed statistically significant association when all possible confounders were controlled.
Discussion
The level of women’s decision-making power on family planning use in this study was 52%. This result was lower than the study done in southern Ethiopia 64% and 67%.12,14 This might be due to the difference in socioeconomic and demographic status of the married women and the nature of the study area since this study is conducted among rural women. Women participation in household decision-making in the study area was 56%, which is in line with the study done in southern Ethiopia where domestic decision-making in the rural area was 55%.15
In this study, only 39% of women have a positive attitude on family planning, which was much lower than the study done in Gedeo Zone.8 This might be due to the different socioeconomic factors, exposure to media and poor utilization of health promotion and education service from health care providers in the study area. However, women's knowledge on family planning (57%) was in line with the result of the study done in Gedeo and quite higher than the study done in Dawro, Southern Ethiopia.8,15
Age of women, women participation in household decision-making, attitude towards family planning and knowledge on family planning were significantly associated with women’s decision-making power on family planning use. In this study, younger women have a higher decision-making power on family planning as compared to older age women. In contrary to this, a study done in Mizan-Aman, South Ethiopia showed that women of age 30–44 were having higher decision-making power on family planning use when compared to younger age women.12 This discrepancy could be due to the current government and other stakeholder efforts to increase women's empowerment in decision-making related to reproductive health.
The effect of poor women participation in household decision-making on decision-making power on family planning was in line with the study done in Dawro zone, Southern Ethiopia.15 This might be because women who are able to participate in household decision-making were also able to participate in decision related to family planning use. Since both participation in household decision-making and decision-making power on family planning were more related to the women's autonomy to decide freely or jointly with their husband on family health issues.
The odds of decision-making power on family planning use were higher in those women who have better knowledge of family planning and this result was supported by the study done in southern Ethiopia Dawaro zone.15 This might result from a woman who has better knowledge regarding contraceptives will develop autonomy to use family planning or discuss with her partner on the use of family planning. In contrary to this, a study conducted in Gedeo Zone revealed that women who were knowledgeable about contraceptive methods were less likely to have a joint decision on contraceptive use.8 This might be due to women in the study area might be influenced by the decision-making of husbands even if they have the knowledge of family planning.
Moreover, the result of this study showed that women who have a positive attitude towards family planning were two times to decide on family planning use than women who have negative attitude towards family planning. The result is more similar to the study done in southern Ethiopia in Gedeo and in Dawro zone.8,15
Conclusion
The findings indicate that the level of women’s decision-making power on family planning use was lower than other study conducted before in Ethiopia. The difference is observed between the studies clearly indicates that the husband is the individual that influence the wife to use family planning in this study area. The study also concludes that younger age women and women who have good participation in household decision have good decision-making power on family planning use. Moreover, women who have good knowledge and a positive attitude towards family planning have good decision-making power on family planning use.
Recommendation
Increasing women's participation in household decision-making should be strengthened in the study area. We recommend increasing women's knowledge and attitude towards family planning through health education and promotion through the health extension program. Moreover, there is a need to adopt a more comprehensive approach to reach men and women on modern family planning which helps women to decide freely without any restriction.
Acknowledgment
We thank study participants and all individuals involved in the undertakings of this study.
Disclosure
The authors report no funding and no conflicts of interest in this work.
References
1. World Health Organization. WHO| family planning/contraception: fact sheet No 351; 2015.
2. Kesetebirhan A. National Guideline for Family Planning Services in Ethiopia. Federal Democratic Republic of Ethiopia: Ministry of Health; Oct 2011.
3. United Nations, Department of Economic and Social Affairs, Population Division. Trends in contraceptive use worldwide; 2015.
4. Rezapour Z, Ansari H. Studying the factors associated with women’s participation in family decision-making (Case study: northern Khorasan, Iran). Euro J Exp Bio. 2014;4(1):553–556.
5. Jan M, Akhtar S. An analysis of decision-making power among married and unmarried women. Stud Home Community Sci. 2008;2(1):43–50. doi:10.1080/09737189.2008.11885251
6. Woldemicael G. Do women with higher autonomy seek more maternal health care? Evidence from Eritrea and Ethiopia. Health Care Women Int. 2010;31(7):599–620. doi:10.1080/07399331003599555
7. Alemayehu M, Hailesellasie K, Biruh G, et al. Married women’s autonomy and associated factors on modern contraceptive use in Adwa Town, Northern Ethiopia. Science. 2014;2(4):297–304.
8. Eshete A, Adissu Y. Women’s joint decision on contraceptive use in Gedeo zone, Southern Ethiopia: a community based comparative cross-sectional study. Int J Family Med. 2017;2017:9
9. Tadesse M, Teklie H, Yazew G, Gebreselassie T. Women’s empowerment as a determinant of contraceptive use in Ethiopia further analysis of the 2011 Ethiopia demographic and health survey. DHS Further Analysis Reports; 2013;82.
10. Central Statistical Agency (CSA) [Ethiopia], Demographic IE. Health Survey 2016: Key Indicators Report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA; 2016.
11. Alemu MN, Worku AG, Beyera GK. Status of men involvement in family planning: an application of trans-theoretical model, Northwestern Ethiopia. Public Health Frontier. 2014;3(2):35–42.
12. Belay AD, Mengesha ZB, Woldegebriel MK, Gelaw YA. Married women’s decision-making power on family planning use and associated factors in Mizan-Aman, South Ethiopia: a cross sectional study. BMC Women’s Health. 2016;16(1):12. doi:10.1186/s12905-016-0290-x
13. Nanda G. Compendium of Gender Scales. Washington, DC: FHI; 2011:360.
14. Central Statistical Agency (CSA) [Ethiopia] and ICF International. Ethiopia Demographic and Health Survey 2011. Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistical Agency and ICF International; 2012:430.
15. Bogale B, Wondafrash M, Tilahun T, Girma E. Married women’s decision-making power on modern contraceptive use in urban and rural southern Ethiopia. BMC Public Health. 2011;11(1):342. doi:10.1186/1471-2458-11-342
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.