")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Deciding to Enrol in a Cancer Trial: A Systematic Review of Qualitative Studies
Authors Viljoen B, Chambers SK, Dunn J, Ralph N , March S
Received 5 June 2020
Accepted for publication 1 September 2020
Published 27 October 2020 Volume 2020:13 Pages 1257—1281
DOI https://doi.org/10.2147/JMDH.S266281
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Bianca Viljoen,1– 3 Suzanne K Chambers,1,2,4– 7 Jeff Dunn,1,2,4,5 Nicholas Ralph,1,3– 5 Sonja March1,8
1Centre for Health Research, Institute for Resilient Regions, University of Southern Queensland, Springfield, Brisbane, Australia; 2Cancer Council Queensland, Brisbane, Australia; 3School of Nursing & Midwifery, University of Southern Queensland, Toowoomba, Australia; 4Faculty of Health, University of Technology Sydney, Sydney, Australia; 5Australian and New Zealand Urogenital and Prostate Cancer (ANZUP) Trials Group, Sydney, NSW, Australia; 6Prostate Cancer Foundation of Australia, Sydney, NSW, Australia; 7Exercise Medicine Research Institute, Edith Cowan University, Perth, WA, Australia; 8School of Psychology and Counselling, University of Southern Queensland, Springfield, Brisbane, Australia
Correspondence: Nicholas Ralph
Institute for Resilient Regions, University of Southern Queensland, Springfield, Brisbane, QLD 4350, Australia
Email [email protected]
Background: Clinical trials are essential for the advancement of cancer treatments; however, participation by patients is suboptimal. Currently, there is a lack of synthesized qualitative review evidence on the patient experience of trial entry from which to further develop decision support. The aim of this review is to synthesise literature reporting experiences of participants when deciding to enrol in a cancer clinical trial in order to inform practice.
Methods: A systematic review and meta-synthesis of qualitative studies were conducted to describe the experiences of adult cancer patients who decided to enrol in a clinical trial of an anti-cancer treatment.
Results: Forty studies met eligibility criteria for inclusion. Three themes were identified representing the overarching domains of experience when deciding to enrol in a cancer trial: 1) need for trial information; (2) trepidation towards participation; and (3) justifying the decision. The process of deciding to enrol in a clinical trial is one marked by uncertainty, emotional distress and driven by the search for a cure.
Conclusion: Findings from this review show that decision support modelled by shared decision-making and the quality of a shared decision needs to be accompanied by tailored or personalised psychosocial and supportive care. Although the decision process bears similarities to theoretical processes outlined in decision-making frameworks, there are a lack of supportive interventions for cancer patients that are adapted to the clinical trial context. Theory-based interventions are urgently required to support the specific needs of patients deciding whether to participate in cancer trials.
Keywords: advanced cancer, qualitative, guideline development, consolidated framework for implementation research
Introduction
Clinical trials play a central role in the advancement of medical care, ensuring effectiveness and safety in new health-care interventions and treatments.1 In oncology, cancer treatments are evaluated on a pathway of development, testing and implementation, relying on results from clinical trials to substantiate their therapeutic efficacy.2 Despite more than 2300 clinical trials initiated across the globe in 2016 alone,3 consistent estimates suggest fewer than one in twenty adults with cancer enrol in a trial.2 Although as many as 70% of individuals diagnosed with cancer are willing to participate in trials4 barriers to participation have persisted over the last twenty years.5 Hence, there appears to be a gap between the numbers of individuals willing to enrol in a clinical trial and the percentage of those who actually participate. Barriers to participant recruitment and retention in oncology trials are well reported and include, but are not limited to, treatment uncertainty;6 financial barriers;7 logistical concerns such as protocol stringency;8 and a lack of resources for patients and clinicians to support clinical trial enrolment and retention.7 Findings from a systematic review of barriers to participant recruitment report similar challenges persisting in studies published from 1995 to 2012.9
One approach to addressing these barriers has been the development and application of decisions aids in the clinical trial setting. A Cochrane review of decision aids in this context outlined the application of informational-based decisional tools targeting outcomes such as decisional regret, knowledge, conflict, anxiety, trial participation and attrition.10 The review found only low-level evidence for effectiveness of these decision aids, and further noted that process outcomes, such as decisional involvement, values and risk expectations, were not considered. In addition, a deeper consideration of more patient-centred outcomes for such studies was proposed. In this regard, the decision to enrol in a clinical trial of a cancer treatment is influenced by a range of extrinsic and intrinsic factors with the process both complex, personal and potentially significant given it can have life-altering consequences.11 Studies report that for individuals with cancer, these factors can include, but are not limited to, increased hope about disease prognosis;12,13 the chance to compare interventions;14 enhanced therapeutic relationships with specialist clinicians;12 relief from the financial burden of care in some cases;14 and improved overall survival.15 Additionally, making the decision to participate in a clinical trial is particularly difficult where proposed treatments are new or novel and information about their safety, efficacy or effectiveness is lacking when compared to conventional treatments.9
Despite the need to understand the context in which trial participation is made and how to support individuals with cancer, there is a lack of synthesized review evidence on both the patient experience of deciding to enrol in a clinical trial and how best to support them. To date, a review by Gregerson et al16 on clinical trial decision making in advanced cancer with a focus on end of life decisions is the only review that examines experiences of patients in this area. To our knowledge, there is no review-based evidence reporting the experiences and subsequent supportive care and decision needs of cancer patients deciding to enrol in a clinical trial. Accordingly, we undertook a systematic review of qualitative studies describing the experiences of adult cancer patients deciding to enrol in a clinical trial of an anti-cancer treatment.
Methods
The aim of this review was to synthesise literature reporting experiences of participants deciding to enrol in a clinical trial of anti-cancer treatment. For the purposes of this study, active cancer treatment includes the provision of anti-cancer therapy to patients with active cancer. For example, chemotherapy, immunotherapy, radiotherapy and surgery. This study will systematically review all aspects of participant enrolment in active anti-cancer treatment trials. The study proposes to develop and exhaustive qualitative understanding of the experience leading up to consenting to a clinical trial in order to identify the individual factors, barriers and enablers that may influence the decision to enrol in a clinical trial of an anti-cancer treatment.
Search Strategy
A comprehensive search strategy sought all eligible qualitative studies from the following electronic databases: PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, Scopus and ProQuest Theses & Dissertations. No date restriction was applied. The search strategy for each database or platform consists of both Medical Subject Headings (MeSH) and free-text words (as appropriate) (see Table 1).
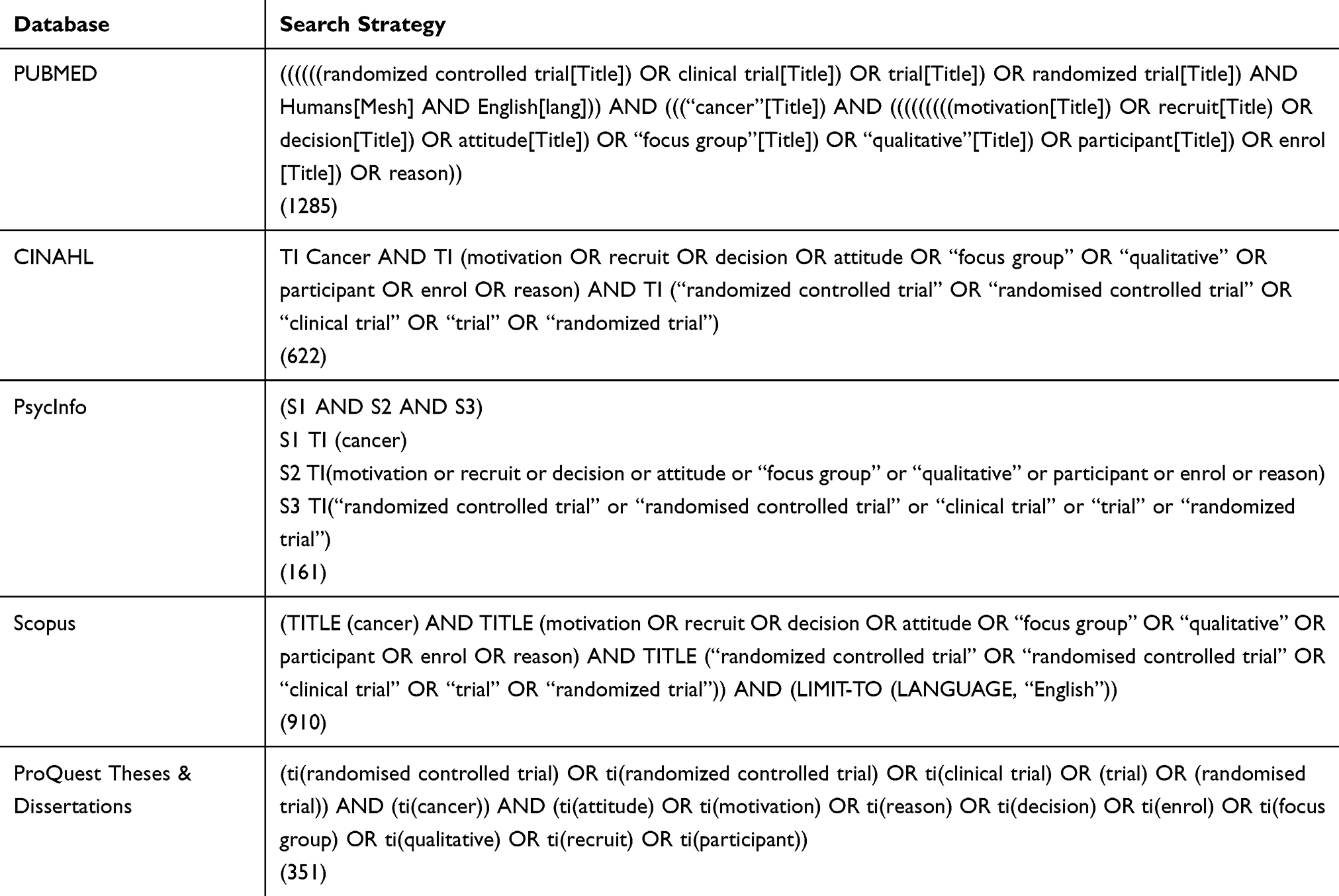 |
Table 1 Search Strategy |
Eligibility Criteria
We included studies that reported the experiences of patients deciding to enrol in clinical trial of anti-cancer treatment. For this reason, qualitative studies on the experiences of this cohort were included. Studies were included if they were peer-reviewed, published in English and included adult human patients only. Dissertations and theses were also included; however none were identified. Full-text articles were also included. Studies were excluded if they were nested and reported quantitative data only. We also excluded nested studies within cancer-related interventions that were not for anti-cancer treatment. Grey literature was not included in the review (eg, government or professional organisation documents) (see Table 2 for the inclusion and exclusion criteria).
 |
Table 2 Study Inclusion and Exclusion Criteria |
Study Selection
Succeeding the search, all identified citations were gathered and uploaded into EndNote database (EndNote X8.1) and duplicate records removed. Titles and abstracts were then screened by two independent reviewers (BV, NR) for assessment against the inclusion criteria. These two reviewers independently screened 100% each of the articles. A list of potential studies for inclusion was circulated between BV and NR. Disagreements on study eligibility were resolved through discussion.
The full text of selected studies was retrieved following the initial screening and assessed in detail. Authors were contacted in cases of incomplete data or irretrievable articles. If the article was irretrievable (ie, not accessible from any source or from the authors), the study was excluded. The full text of each selected article was screened by the two independent authors (NR [100%], BV [100%]) to determine eligibility against the inclusion and exclusion criteria.
To ensure that all relevant studies were included, a manual search of citations and references of eligible studies was also conducted. Resulting references were exported separately and provided to the two reviewers (BV, NR) for independent review. Where necessary, study authors were contacted for missing information. To ensure impartiality the inclusion and exclusion criteria was constantly referred to (see Table 2). The results of the search are reported according to the PRISMA guidelines for systematic reviews, detailing the number of papers identified by the search strategy and the number of papers that were included and excluded are stated. Any disagreements that arose between the reviewers were resolved through discussion. A PRISMA flow diagram of the study selection is outlined in Figure 1.17
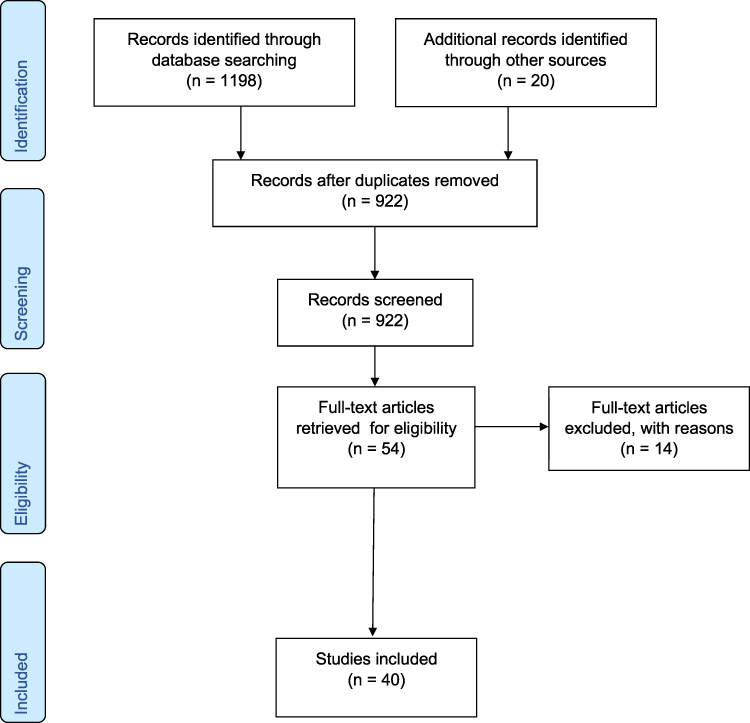 |
Figure 1 PRISMA flow diagram. |
Data Analysis and Synthesis
Data were extracted by two independent authors (BV, NR) for a random 10% (selected by simple random sampling) of the included studies. For the remaining studies, one author (BV) extracted the data and checked by a second author (NR). Any disagreements were resolved through discussion. The PDF files (or equivalent) of manuscripts were download and imported into NVivo and data extracted.
Data were synthesised by utilising a thematic analysis approach, which enables extraction of concepts and hypotheses from multiple qualitative studies.18 Data were coded using NVivo and identified themes were categorised and presented as a narrative. All aspects of the thematic analysis were reviewed against the data. This involved several readings of each paper. The analysis and its explanations were repeatedly discussed among the researchers until consensus was reached.19 The findings from the systematic review are described using meta-synthesis. Qualitative meta-synthesis aims to synthesise qualitative data to further develop identified themes and provide a more extensive interpretation of the findings.20 In this qualitative review, quotations were included (see Table 3) to allow readers to assess the validity of the domains.
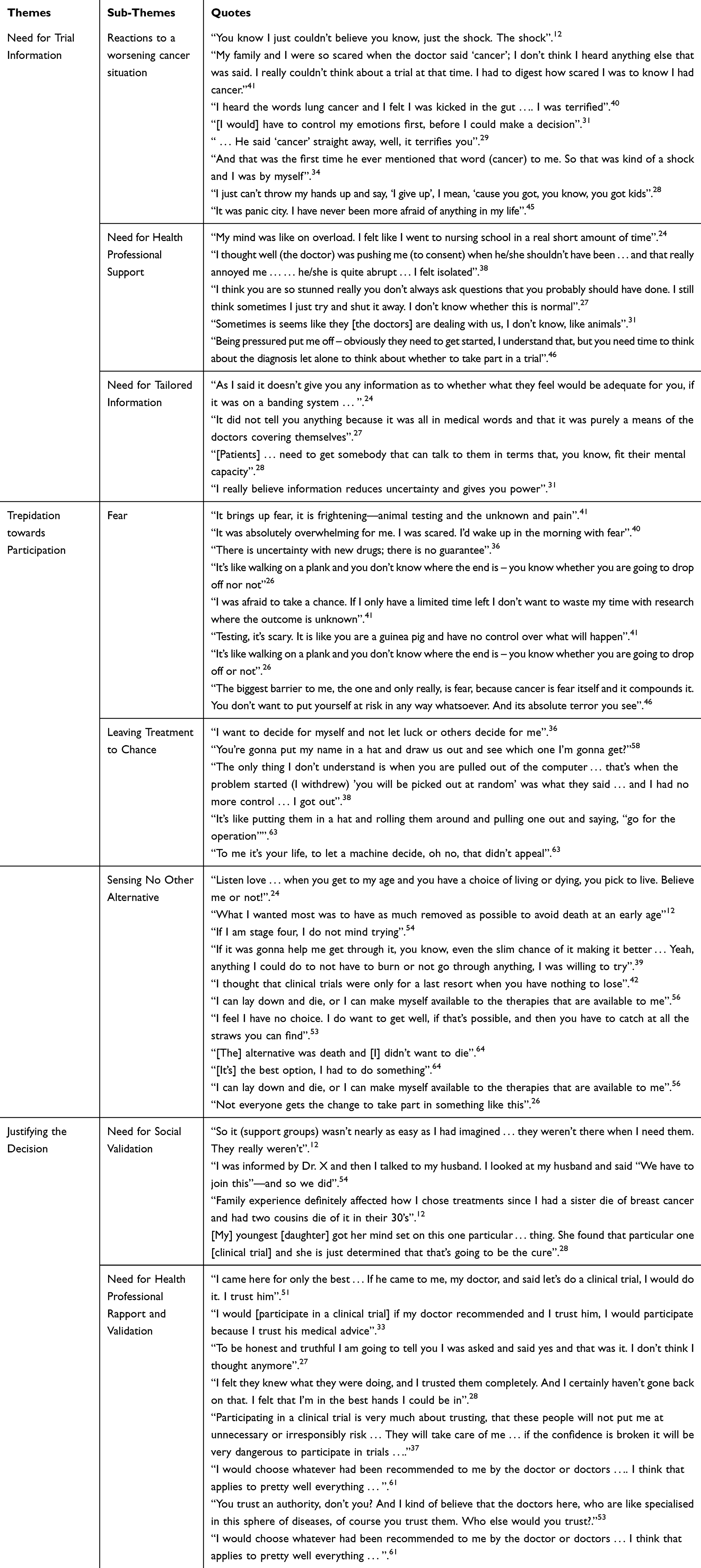 |
Table 3 Themes and Quotations |
Patient and Public Involvement
No patients from the included studies were involved in this review.
Quality Assessment
Two independent reviewers (BV, NR) performed quality assessment. Each included study was critically appraised using a quality assessment tool drawn from the Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields21 with the additional of: a statement of human research ethics committee approval. To assess the reliability and validity of included studies, studies had to meet the criteria provided in Table 4.21 Studies were independently screened and scored (0–22) by two reviewers (BV, NR). The two reviewers also referred to the Consolidated Criteria for Reporting Quality Research (COREQ)22 guidelines to discuss study quality and appraise the standard of evidence. Each paper could achieve a maximum score of 22. On each criterion two points were awarded for yes, one for partial and zero for no. All studies were judged to be either of high quality (scores of 17–20 points), adequate (scores of 11–16 points) or weak (scores of 0–10 points). High-quality studies were subsequently included in the final analysis (Table 5). Discrepant scores were resolved through discussion and consensus. The main methodological issues included inadequate explanation of the researcher-participant relationship, how this may have influenced conclusions and inadequate explanation of analytical rigour.
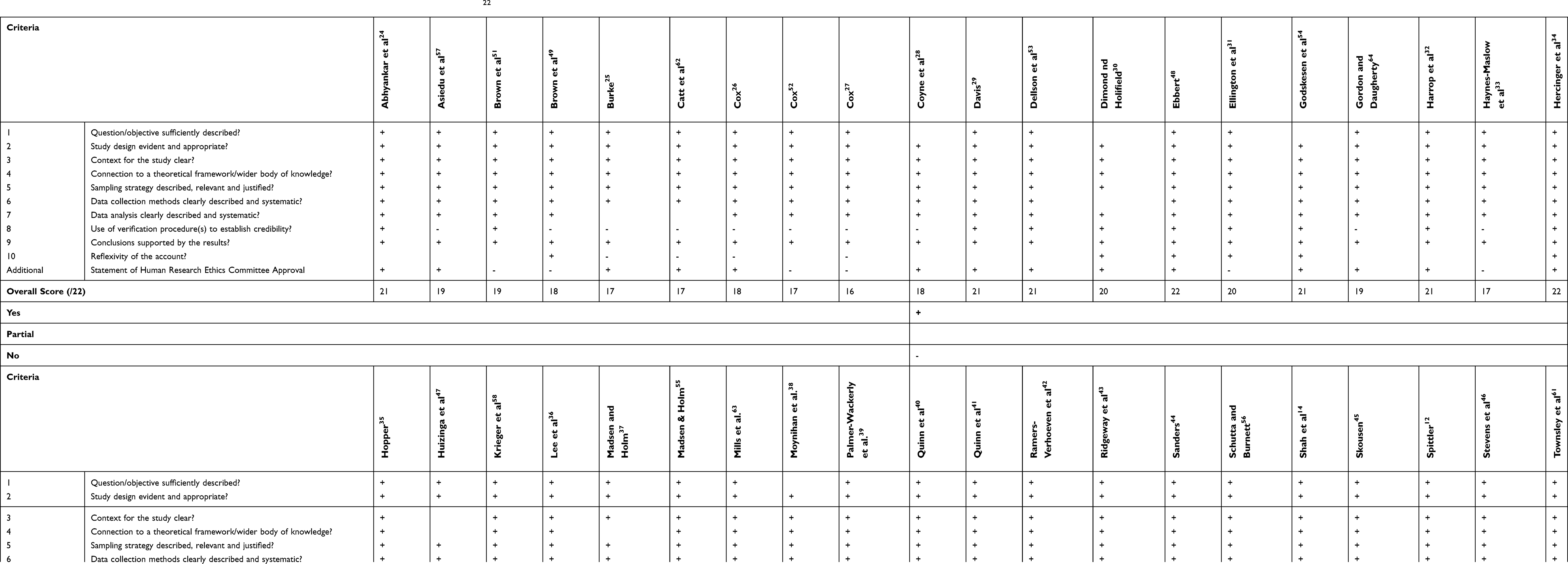 |
Table 4 Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields22 |
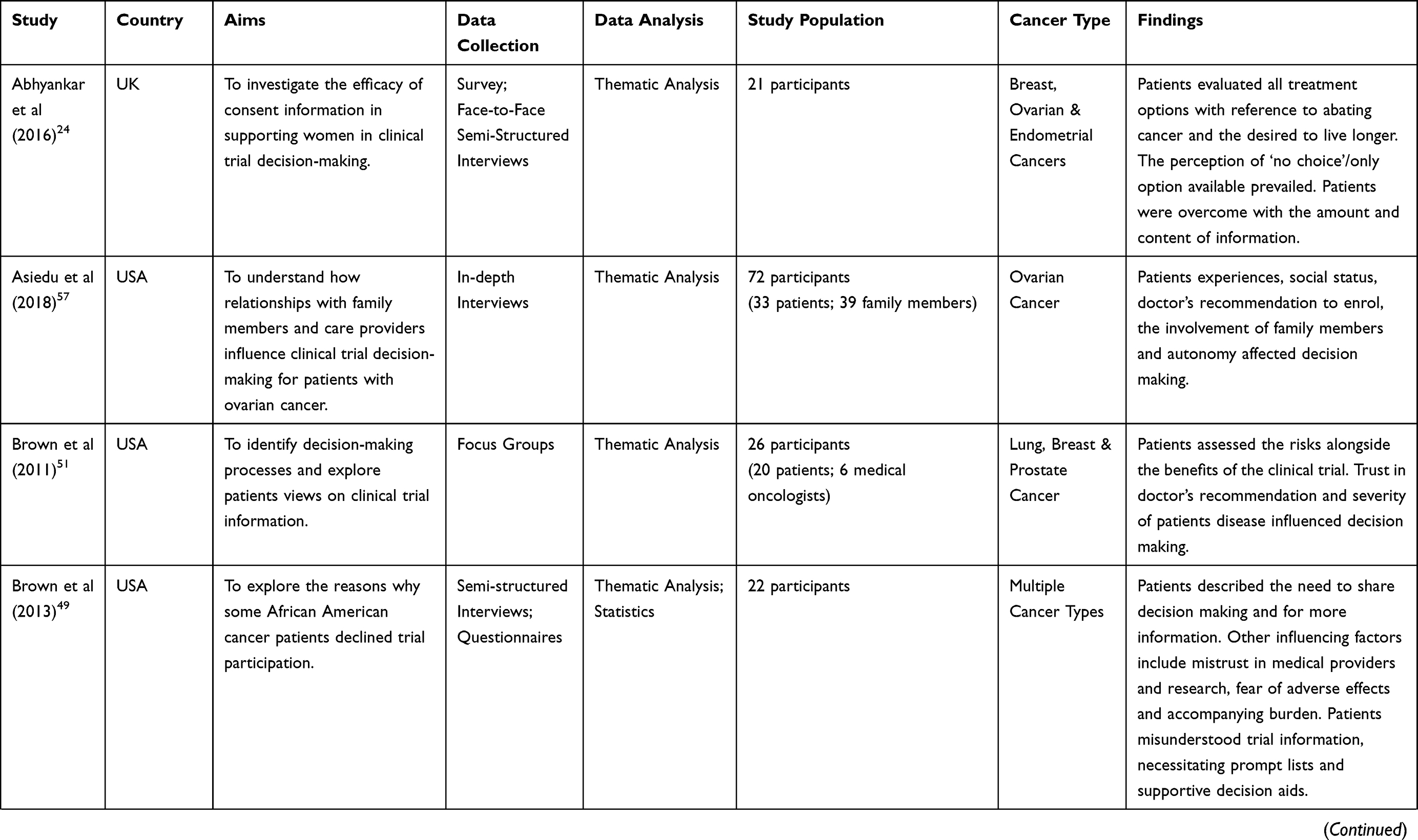 | 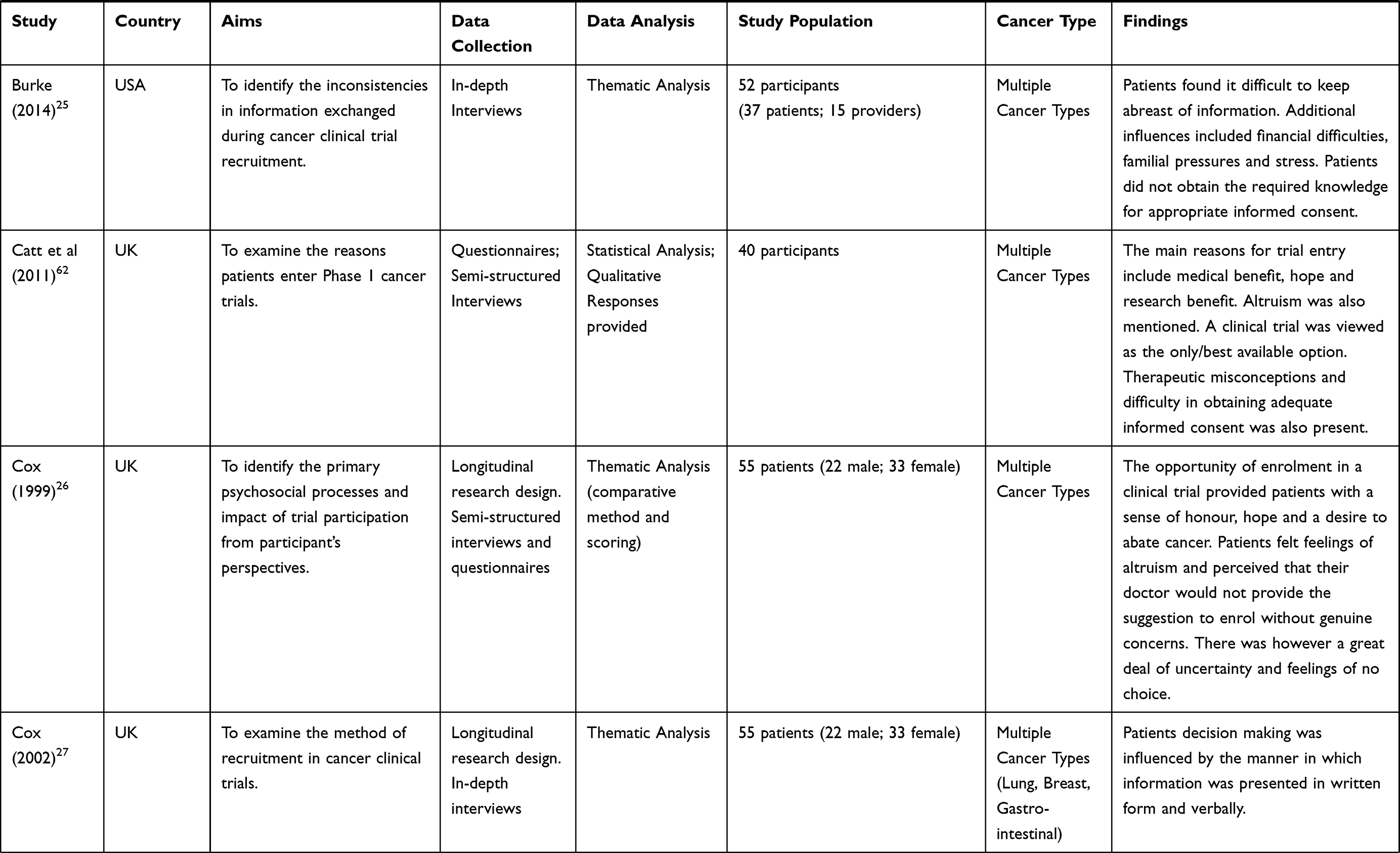 | 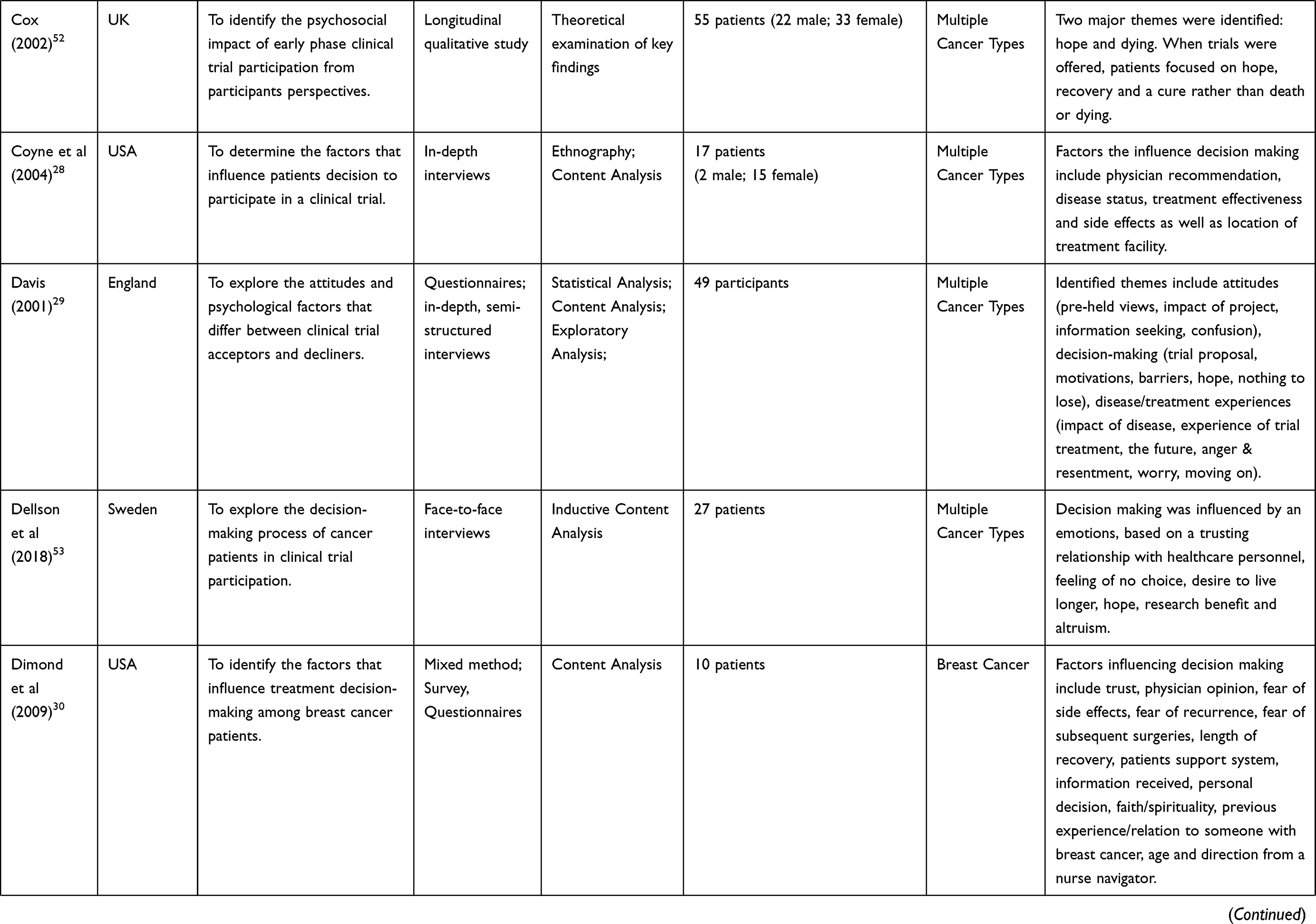 | 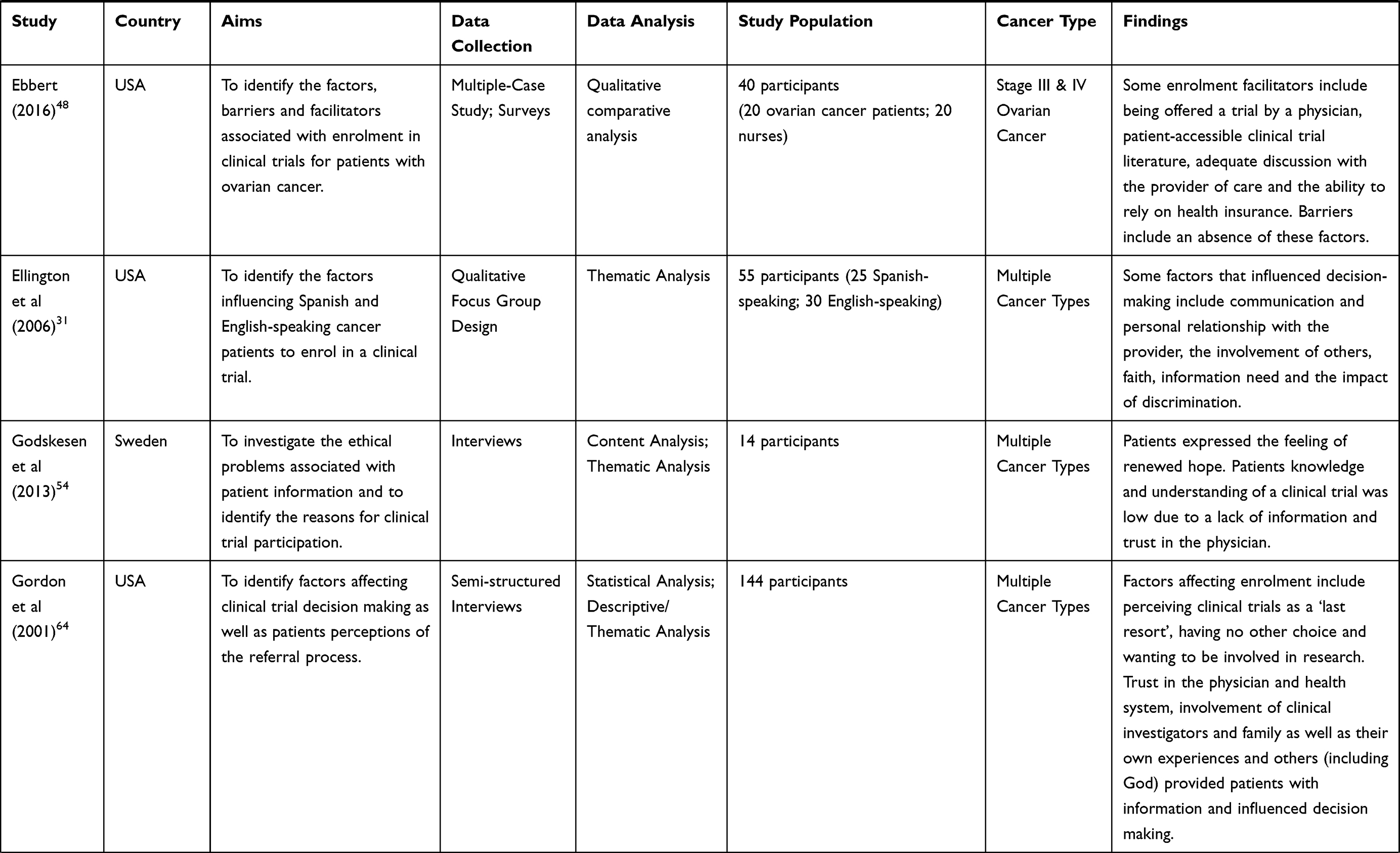 | 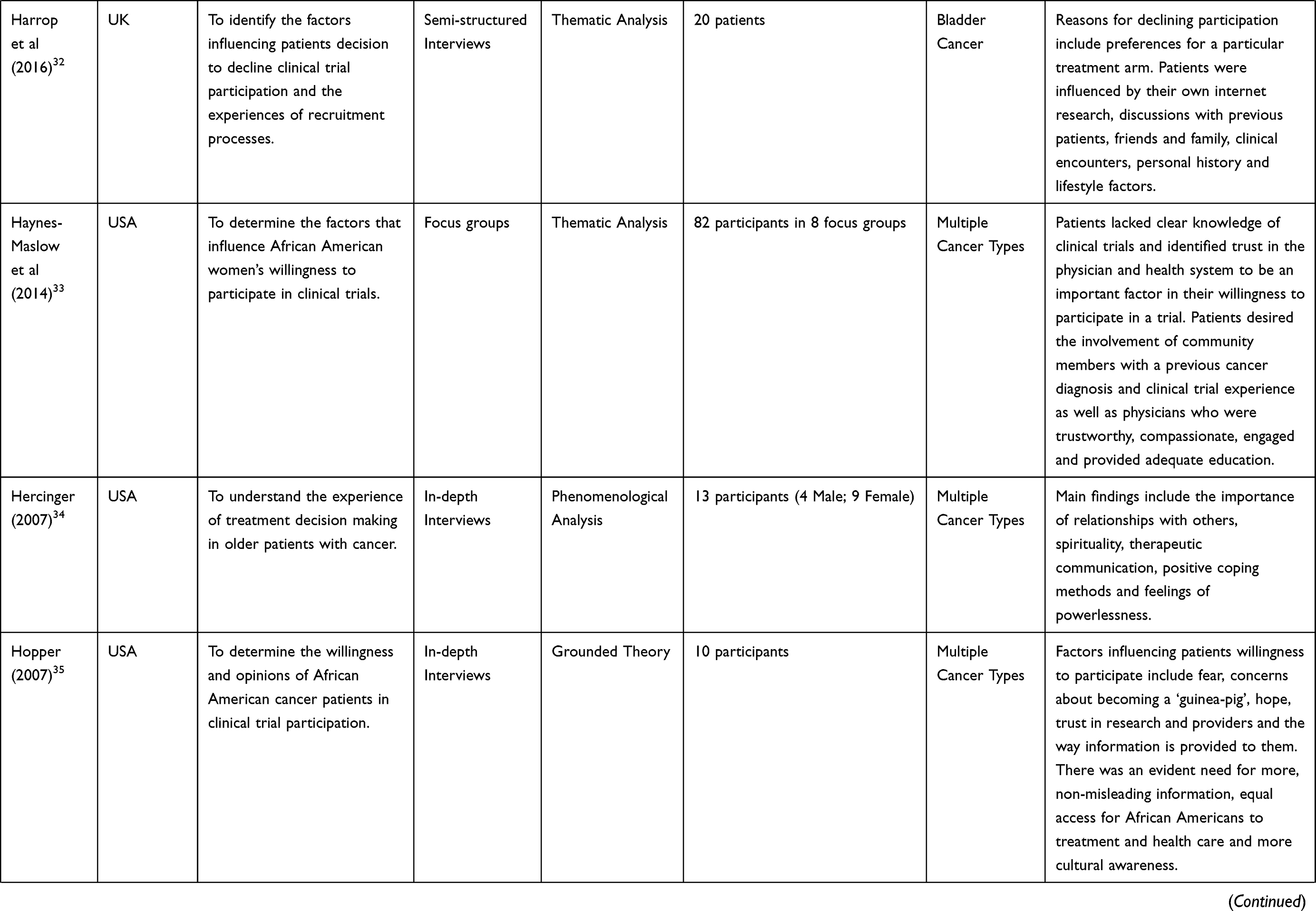 | 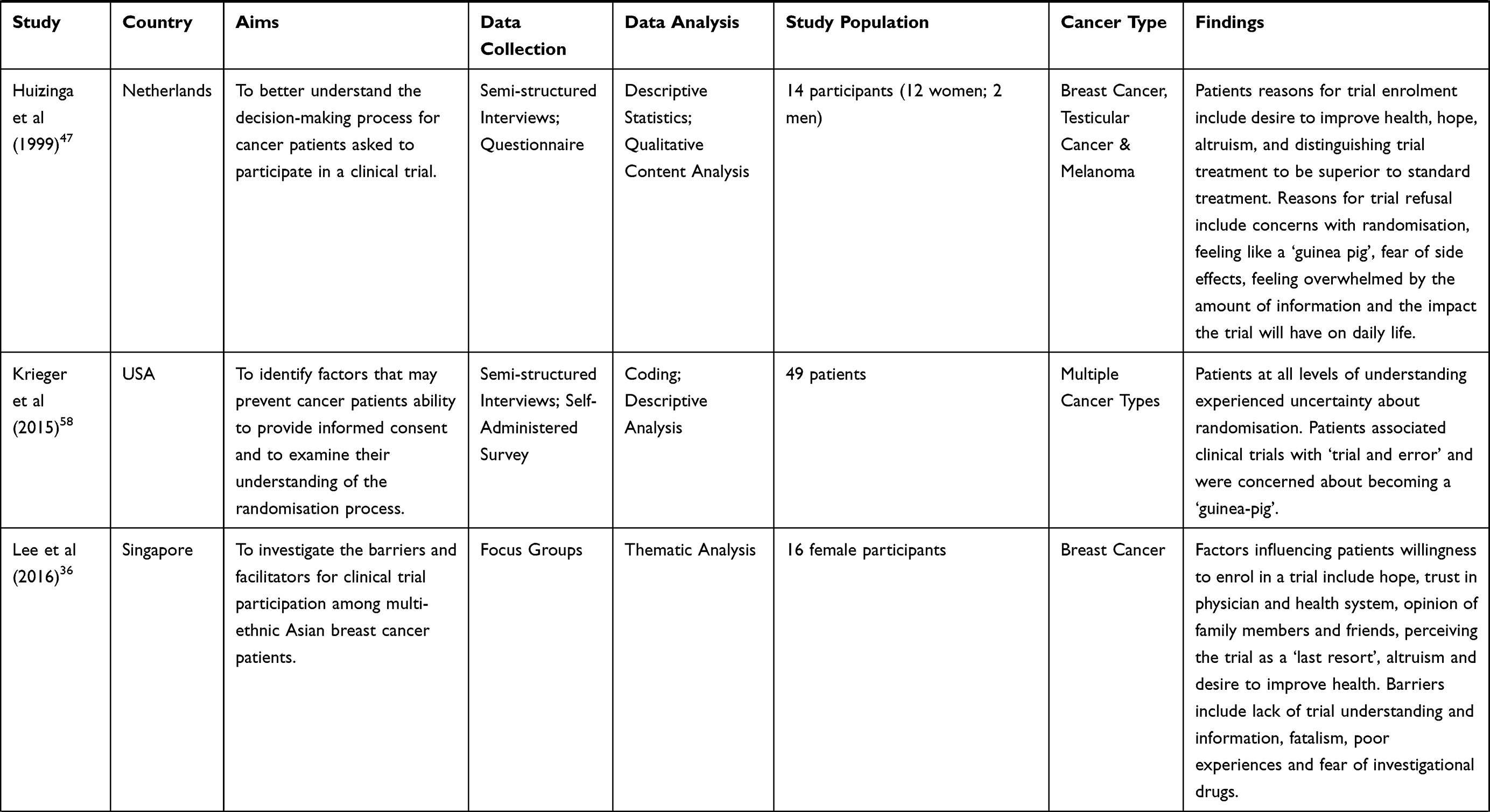 | 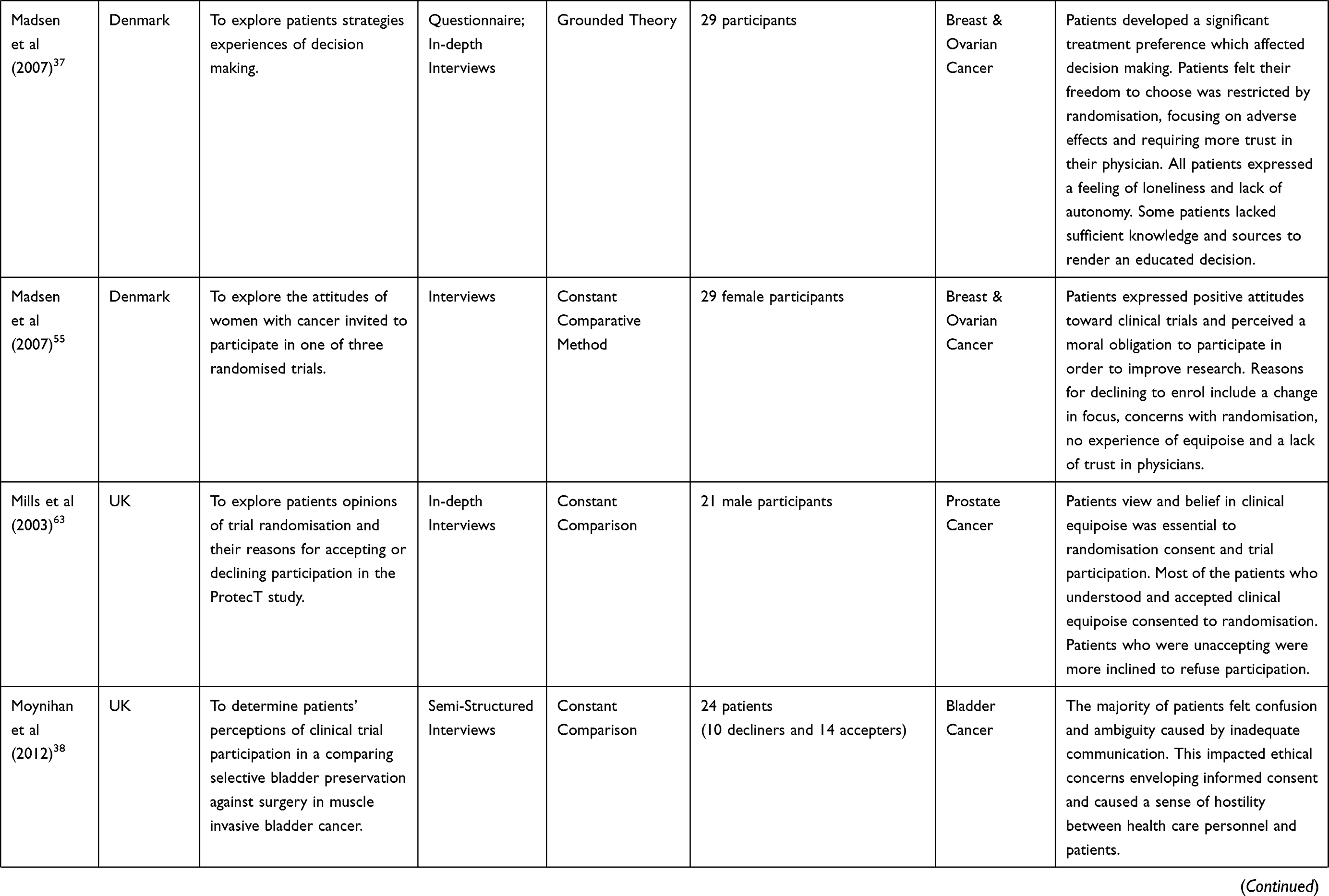 | 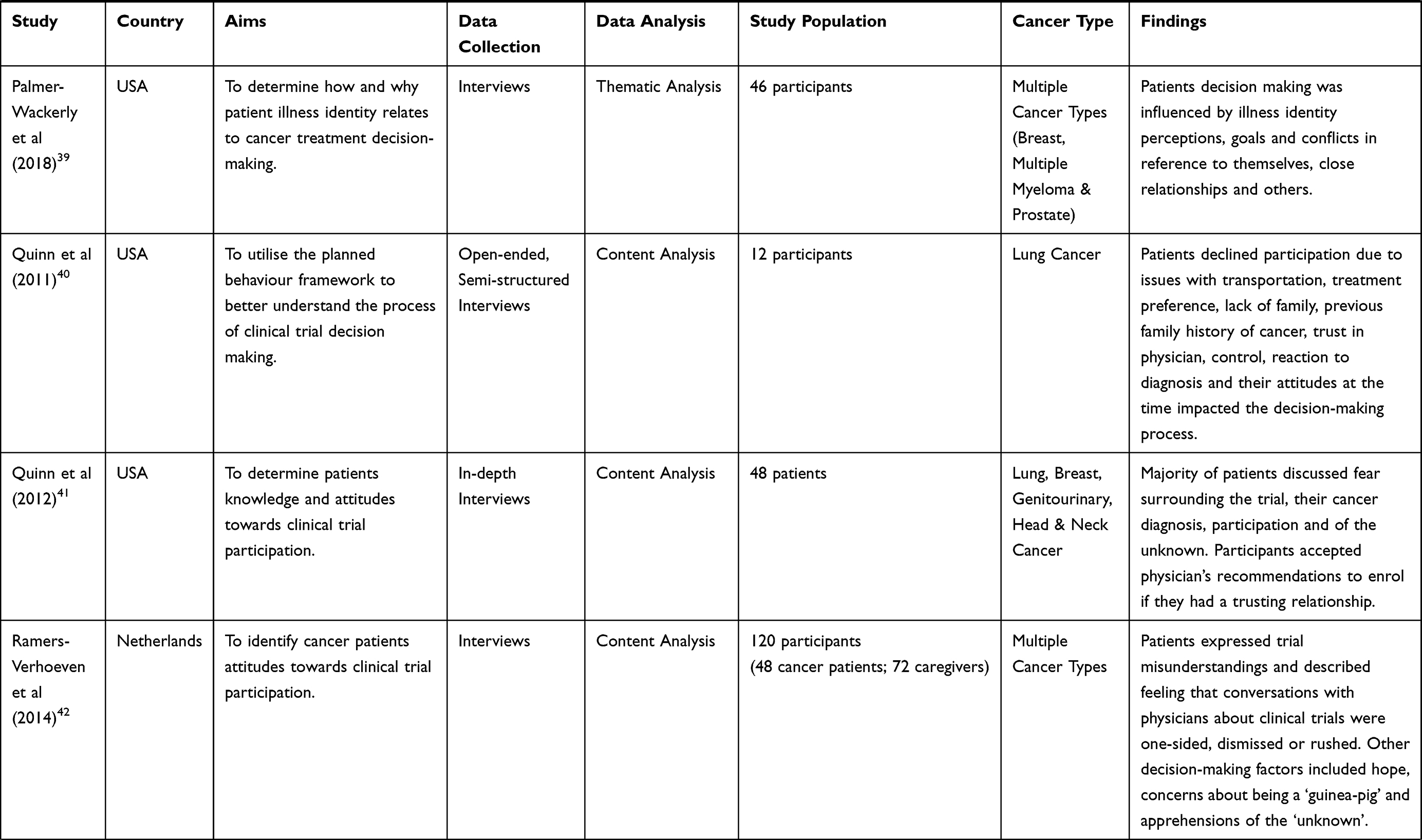 |  | 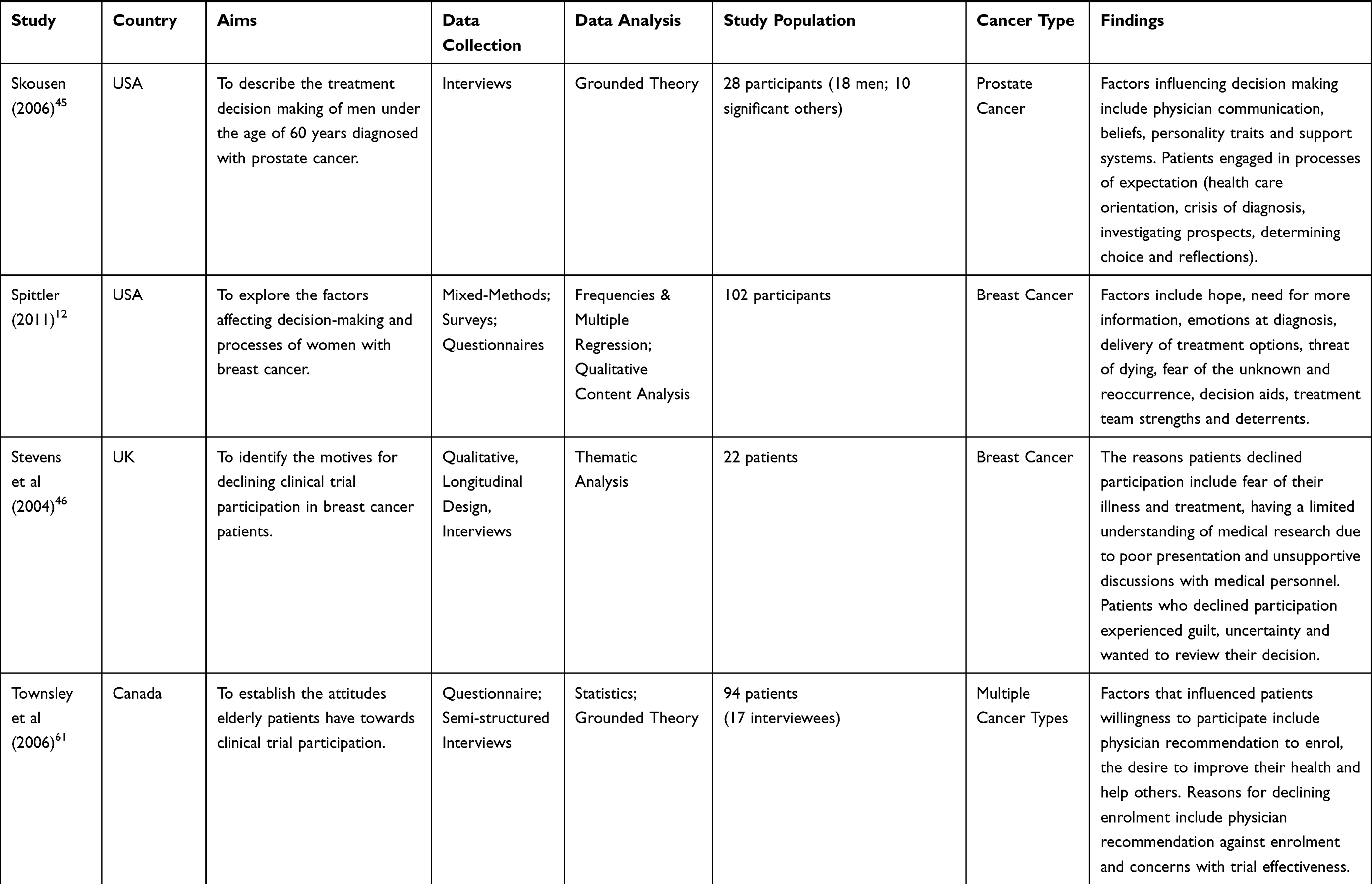 |
Table 5 Characteristics of the Included Studies |
Results
Of the 40 studies reviewed, 11 were of local and 3 of advanced cancers; 19 included mixed cancer types and 7 did not specify. The phase of the trial was reported inconsistently throughout studies with 4 Phase I and 6 Phase III; 11 studies reported patients across a number of trials at different phases and 19 were not specified. All studies were conducted in countries with highly developed health-care systems such as USA (21), UK (10), Sweden (2), Netherlands (2), Denmark (2), England (1), Canada (1) and Singapore (1). Following meta-synthesis, three themes were identified representing the overarching domains of experience in deciding to participate in a cancer trial: (1) need for trial information; (2) trepidation towards participation; and (3) justifying the decision. Selected quotations reported in primary studies are included in Table 3 to demonstrate the correlation between the identified themes and patients’ perspectives on treatment decision making. A summary of the included studies is provided in Table 5.
Need for Trial Information
Consideration of trial participation was reported in most studies (25/40) to stem from “reactions to a worsening cancer situation”.12,23–46 This situation could be described as a rapid change in health status or prognosis. Throughout the context of distress, confusion, uncertainty and illness, patients desperately attempt to identify and understand all of the appropriate treatment options available to them.41
Reactions to a Worsening Cancer Situation
Once cancer patients were informed their cancer was worsening, they experienced feelings of shock, fear and disbelief.27,28,33,44,45 “You know I just couldn’t believe it you know, just the shock. The shock”12 (see Table 3). As patients tried to comprehend this change in health status, treatment options were introduced, including the invitation to take part in a clinical trial.12,47 Due to the overwhelming emotions at this stage of their cancer trajectory, patients expressed a desire for their physician to consider their emotional concerns and offer support before providing them with trial information.30 The patients’ distressed state affected the amount of information they absorbed and impeded their ability to make health-related decisions.23,40,45,48 Making the decision to enrol in a clinical trial of an active anti-cancer treatment is complex and personal for all cancer patients. Being confronted with trial information and not receiving enough emotional support during this time, led to decisional conflict.49
Need for Health Professional Support
The interaction and information exchange between physician and patient was reported as a significant issue in most of the included studies (31/40).12,23–28,30–37,39–46,48,50–55 Patients experienced one-sided, dismissed or rushed conversations with physicians, resulting in feelings of alienation, pressure, coercion and an absence in autonomy.37,41,45
(…) I thought well (the doctor) was pushing me (to consent) when he/she shouldn’t have been … and that really annoyed me … … he/she is quite abrupt … () I felt isolated37
This hindered most patients’ desire and ability to make treatment-related decisions (see Table 3).37 In some cases, patient autonomy and ethical practice were not upheld, often due to a perceived lack of time to consider information about the trial.37,56 Patients clearly stated that if physicians acknowledged their concerns, offered reassurance and took the time to listen, they felt they could then trust that the physicians recommendation on clinical trial participation.30 Patients also reinforced the importance of having enough time to comprehend a cancer prognosis and filter through treatment information before making decisions.12,45,47
Being pressured put me off – obviously they need to get started, I understand that, but you need time to think about the diagnosis let alone to think about whether to take part in a trial.45
Need for Tailored Information
The treatment information patients received was mostly described as confusing (25/40).23,24,26–34,36,37,41–48,52,53,57,58 Written information was reported as lacking in detail23 and difficult to read in terms of sentence length and word complexity.26,43 “It did not tell you anything because it was all in medical words and that it was purely a means of the doctors covering themselves”26 (see Table 3). Most participants used internet-based sources to better understand the material they received or to obtain information described in more layman’s terms.30,31,33,44,56 Even with this initiative, confusion was still evident and the level of knowledge about trial basics was considerably low amongst most cancer patients.26,27,37,53,59,60 “[Patients] … need to get somebody that can talk to them in terms that, you know, fit their mental capacity”.27 This lack of trial understanding demonstrated a clear disconnect between trialists and their patients, to the extent that not all patients understood their position in the consent process. Some even believed that withdrawal from a trial was impossible, affecting treatment decision-making.37
(Once randomised) you couldn’t volunteer for the other (treatment) because you only got that if you went into the trial and got away with it through randomisation.37
Trepidation Towards Participation
A substantial finding across reported studies (29/40) was patients experience of trepidation, most commonly expressed as “fear”.12,14,25,27–29,31–33, 35–46,48,50,51,54,57,60–62 This was frequently associated with cancer diagnosis, prognosis and treatment options.29,40 Trepidation towards participation was associated with fear of cancer diagnosis, prognosis and treatment options.29,40 Common reasons for trepidation included cancer fatalism,35 the lack of time to decide on treatment,40 concern about the “unknown”47 and the possibility of a negative response to the trial.47 Patients with a history of cancer, not only expressed uncertainty but the fear of cancer reoccurrence as well.12,27,40 These factors formed a mental barrier and delayed the decision to enrol in a clinical trial.12,27,35,47
Participants described not wanting to lose control, feel isolated, alienated or powerless during decision-making.33,37 Common statements associated with the idea of participating in a clinical trial included “I am scared”,29 “I am nervous” about joining a trial,47 concerns about feeling like a “guinea pig”, or an “experiment”, “trial and error”,32 “feeling alone” and “having no say”34,37,45,46,48,57,61 (see Table 3). Another primary influence in considering treatment options was patients’ fear of potential adverse side effects associated with clinical trial participation27,29,33,43,44,46. This included both the known and unknown risks intrinsic in clinical trial medicines.27,35 There was a clear need for patients to consider the potential side effects and its impact on future quality of life (QOL) against the therapeutic advantages of the trial.48 Patients desired and suggested that their health-care providers offer detailed discussions and deliver general and specific information about clinical trials in order to improve their understanding of the risk-to-benefit ratio in clinical trial enrolment.35,40,54
Leaving Treatment to Chance
Before enrolling in a clinical trial, most participants expressed concerns about the process of randomisation and wanted to know the treatment group in which they would be placed.14,48,54,62 As depicted in Table 3, the idea of randomisation made most patients feel uncomfortable or stressed46 and made some unwilling to join a clinical trial.35 Patients wanted to make an informed choice and felt “unpleasant” leaving treatment decisions to chance.31,35 There was a general lack of knowledge about the concept of random assignment and the need for comparing two different treatments.32,46,57 Patients struggled to make sense of their involvement in the trial process while questioning scientific principles.37
Sensing No Other Alternative
Evident in 30 out of the 40 included studies, was patients tendency to simplify their treatment options by evaluating them in terms of life versus death, regardless of fear or randomisation.12,23,25,27–30,32–36,38–44,46,48,50–54,60,61,63 There was a predisposition to perceive the active pursuit of treatment as the only option available and there was “no real choice” to make.23,25,28,30,43,52,63 The use of the term “last resort” was used by many patients offered Phase III clinical trials.32,35,42,50,63 As validated in Table 3, the majority of participants suggested that treatment options presented were considered with reference to the goal of living longer and hopefully abating cancer.43,44,46,60 This goal seemed to influence the way in which the options were comprehended, evaluated and experienced within decision making.12 For most, the offer to participate in a clinical trial provided some form of hope.25,26,28,33,43,46,51–53,61 Hope was viewed as complex, affected by spirituality and faith, interpersonal relationships, trust, positivity and vital to the coping process.29,48,51,53 When patients sensed they had no other alternative they tended to make the treatment decision quickly. Patients frequently described, “having already made their mind up”, “seeing trial as just a natural thing to do”, “going with their gut feelings” and even suggesting “it never entered my mind to say no”.23,25,28,47,52,53
Justifying the Decision
Patient decision-making processes are influenced by the knowledge and support received from their family, friends and physician. This is viewed as important in order to justify their decision about clinical trial participation.56 Many participants further expressed a moral obligation to participate in a clinical trial for altruistic purposes14,23,25,28,30,35,46,52,55,61 and the desire to assist in furthering clinical research.23,52,54,63,64
Need for Social Validation
Twenty-nine out of the forty studies suggest that patients’ approach to decision making is influenced by their sociodemographic, social and cultural backgrounds, their experiences with health-care services and their relationships with their health-care providers.14,23,25–29,31,33,34,36–44,48,51–56,60,61,63 The opinion and knowledge of patients’ physician, family and friends were predominantly noted as important in decision-making and facilitators for clinical trial enrolment.35 Brown (2013) states that patients actively want to share decisions.48 The support of family, peers and health professionals was fundamental in being able to comprehend their diagnosis, treatment options and treatment experience.12
With the established difficulty in decision-making and processing treatment information, many patients wished to seek the opinion of others and/or hear from previous trial participants’ experiences of clinical trial treatment.23,27 Patients stated they would try and contact previous clinical trial participants to enquire about “what they tried and what they used”56 to assist them in understanding the actuality of trial participation and inform decision-making.27,31,42,56 Patients also wanted to be aware of support groups before enrolment.12 Participants who heard about successful trials emphasised that hearing stories allowed them to feel more enthusiastic about the research, some even went online and/or approached clinical providers about trials42 as indicated in Table 3. Speaking with previous survivors was verbalised as decision aids, helping participants know they were not alone, providing an additional viewpoint and gave them a sense of feeling valued.12,23
Participants sought some form of family involvement in the clinical trial decision-making process. This was identified as a significant finding across the included studies (23/40).26–31,33–36,38–40,42–44,46,48,52,53,56,61,63 The involvement of family was either to assist patients in their search for more information about the trial, help them stay informed about the clinical trial process and/or support their final decision about treatment. The opinions of friends and family was viewed as an important facilitator if the opinions were positive and seen as a barrier if the opinions were negative.35 To manage this, patients selectively involved family members in their decision making, engaging with those they shared a strong and close relationship or when they had scientific or medical training.47,56 Patients also determined when and how to share particular types of information. Some reasons for excluding family members from discussions about trial participation included a desire to avoid creating perceived emotional and psychological burdens for family members.56
Patients who witnessed friends or family members who had experienced cancer, positive and negative results with treatment and any long-term outcomes impacted their treatment considerations and decision-making.12,29,44 As demonstrated in Table 3, some patients stressed the importance of making decisions in partnership with family members, as portrayed in the use of plural pronouns such as “we” and “our” in talking about the final decision.56 These relationships were essential; family members attended appointments, participated in discussions around clinical trial enrolment, showed concern, provided physical and emotional support, shared expert knowledge and therefore influenced the treatment decisions that were made.56
Need for Health Professional Rapport and Validation
Trust in a physician’s recommendation or opinion concerning enrolment in a clinical trial was reported as vital in majority of included studies (31/40).14,25–37,39–44,47,50,52–56,60,61,63,65 A commonly-held belief in one study was that the doctor would not offer trial participation if it was not in the patients’ best interest.26 Patients indicated that, if they held a long-standing relationship and developed trust in their doctors’ medical judgment, they would most likely adhere to their doctors’ guidance.30,39,50 Being content with decision-making appeared to be influenced by the trust, respect and relationships patients had with health-care providers and health-care personnel26,28,31,33,36,37,40,42,43,52,55,63 (see Table 3). Enabling trust and building rapport over time were identified as an important basis to facilitate good communication, willingness to participate in a trial and ultimately affected decision-making.14,25,43,55 Participants wanted their physician to be honest with them, providing reassurance and clarity through quality consultations and discussions.24,37,41,43,50 Trust in the doctor, specialists and medical team were crucial in considering the available treatment options.14,27 This trust, as well as trust in local governance, drug development processes and government legislation were all viewed as facilitators to clinical trial enrolment.35 Patients yearn for the knowledge that clinical trials are conducted in an ethical manner and cited confidence that adequate care is given during trial procedure as facilitators for clinical trial enrolment.35
Discussion
To our knowledge, this is the only review that comprehensively synthesises evidence from qualitative studies reporting the experience of patients deciding whether to enrol in a clinical trial. Our findings show that after a cancer diagnosis and being invited to enrol in a clinical trial, deciding to enrol revolves around the “need for trial information”; “trepidation towards participation”; and “justifying the decision”. Our data highlights several points among which is an overarching need to better address informational and decision-support needs in individuals deciding to enrol in a cancer trial.
Firstly, there is a need to improve the way patients are informed about clinical trials and supported to make a decision that is right for them. Moreover, given the broad array of needs voiced by patients across most included studies as well as the role of health professionals in meeting them, finding effective decision-support interventions should be a priority for health systems and clinical trialists everywhere.
Secondly, understanding decision-making in the context of a clinical trial and individuals’ associated needs for decision-support should be prioritised. Our findings bear similarity to the domains of Charles’ Shared Decision-Making Framework66 in which patients make decisions in the context of (1) “information exchange”; after (2) “deliberation” happens; and towards (3) “deciding on treatment to implement”. Given the broad applicability of Charles’ framework66 to health contexts, our thematically similar results suggest the decision process of enrolling in a clinical trial may not be dissimilar to other health-related decisions experienced by cancer patients. Instead, where the decision-process may differ is context; clinical trials present as uncertain and unfamiliar to many participants and health professionals lack the interventions that comprehensively address informational, psychological and decision support needs. For instance, a Cochrane review reported inconclusive results on whether individuals who were provided with a decision aid experienced changes in comprehension and/or uncertainty during decision making.10 Recently, decision aids adaptable to the clinical trial context have become available via the International Patient Decision Aids Standards (IPDAS) Collaboration however their effectiveness in the trial context remains unknown thus far.67–69
Thirdly, across every theme, participants reported a desire for personalised support from the clinician inviting them to participate in a trial. The communication style of the clinician plays an important role in patients understanding of information and willingness to join a trial.70 Poor communication techniques used by a physician can lead to insufficient patient understanding.71 Information provision should therefore be tailored to address patients’ needs, questions and concerns.70 For trialists and patients, addressing prospective participants’ emotional needs, actively listening and promoting opportunities to converse with, inform, question and interact with each other may provide the best mechanism for addressing negative aspects of the decision-making experience. It is important for clinicians to implement a variety of communication strategies to enhance participants understanding of clinical trial information.71 Efficacious communication ensures participants receive relevant information customised to their individual learning requirements and encourages informed decision-making.72
A focus for decision support may therefore be on improving communication skills using a shared decision-making framework to structure any proposed intervention. According to the IPDAS Collaboration how information is presented can have a significant impact on the knowledge patients acquire, by affecting patient ability to understand and integrate the information.68 These points are supported by Nishimura’s 2013 review of interventions for improving informed consent in trials insofar as conversational opportunities may lead to enhanced understanding of the study among participants, a greater sense of partnering in the research process, and heightened rapport between trialists and participants.73 The evaluation criteria for assessing the quality of patient decision aids as part of the IPDAS Collaboration, identified coaching/guidance in deliberation and communication as one of twelve broad dimensions in the field of patient design and development.74 Patients and physicians may therefore profit from receiving coaching and guidance in order to cultivate high-quality and productive two-way communication.74
Fourth, we would argue that the experiences synthesised from the data of 40 included studies show a need for interventions that address all facets of the decision-making process described herein. Supporting people to learn about trials in their preferred way and in view of their own circumstances is crucial for any decision support intervention. Participants should also be given the opportunity to express their emotions and be provided with the space to deliberate about the best course to take for their circumstances. Two-way communication that is accompanied by a strong-patient provider relationships, that recognises individual preferences and values and incorporates and evaluates the use of effective evidence-based information, leads to greater treatment satisfaction and positive health outcomes.74 Interventions therefore should be multimodal to reflect diverse learning styles in the broader community while space to make a decision should be better incorporated into the informed consent process.75 Nevertheless, with many failed interventions for supporting the decision to enrol in a clinical trial,10 more work is needed to build on the process identified in our review and identify ways to measure outcomes of decision support and design effective interventions for cancer survivors deciding whether to enrol in a clinical trial.
Strengths and Limitations
We used a carefully designed and systematic search strategy, rigorous inclusion criteria, and a validated quality assessment process to determine the merits of our review findings. Moreover, several experienced researchers reviewed the protocol and were involved in the key phases of the review. Additionally, we used a popular and robust approach to synthesising qualitative data for systematic reviews.18 Our review was limited by being unable to access raw qualitative transcripts from any authors identified for inclusion in the study due to either a lack of ethical approval, failure to reply or unavailability of transcripts mostly due to the elapsed time of some studies. All of the studies were conducted in the health systems of highly developed economies. Therefore, there is a limitation that these results may not apply to low-and-middle-income counties. Additionally, we have included studies that have focused on the experiences of patients involved in enrolling in a clinical trial however, of note is that six of these studies also included interviews of patients who subsequently declined clinical trial participation. While it was not possible to identify those who declined within the data from included studies, we believe the experiences of individuals declining to participate in a clinical trial is a gap in the literature and should be a topic for further research.
Conclusion
Our review findings indicate that the decision to participate in a clinical trial is an experience marked by complex informational, emotional and psychological needs. With a lack of evidence on effective interventions, further work is needed to design strategies for individuals considering whether to enrol in a trial which pair quality decision support with effective psychosocial and supportive care.
Acknowledgments
This project is supported by the NHMRC Centre for Research Excellence in Prostate Cancer Survivorship APP1098042.
Disclosure
Dr. Nicholas Ralph reports grants from Australian and New Zealand Urogenital and Prostate Cancer Trials Group, during the conduct of the study; fees from 3M Healthcare, outside the submitted work. The authors have declared no other potential conflicts of interest for this work.
References
1. World Health Organisation. Clinical trials. 2020; Available from: https://www.who.int/topics/clinical_trials/en/.
2. Unger JM, Cook E, Tai E, et al. The role of clinical trial participation in cancer research: barriers, evidence, and strategies. Am Soc Clin Oncol Educ Book. 2016;35(36):185–198. doi:10.1200/EDBK_156686
3. Grand MM, O’Brien PC. Obstacles to participation in randomised cancer clinical trials: a systematic review of the literature. J Med Imaging Radiat Oncol. 2012;56(1):31–39. doi:10.1111/j.1754-9485.2011.02337.x
4. Comis RL, Miller JD, Aldigé CR, et al. Public attitudes toward participation in cancer clinical trials. J Clin Oncol. 2003;21(5):830–835. doi:10.1200/JCO.2003.02.105
5. Gerido LH, He Z. Improving patient participation in cancer clinical trials: a qualitative analysis of HSRProj & RePORTER. Stud Health Technol Inform. 2019;264:1925–1926.
6. Ford JG, Howerton MW, Lai GY, et al. Barriers to recruiting underrepresented populations to cancer clinical trials: a systematic review. Cancer. 2008;112(2):228–242. doi:10.1002/cncr.23157
7. Nipp RD, Hong K, Paskett ED. Overcoming barriers to clinical trial enrollment. Am Soc Clin Oncol Educ Book. 2019;39(39):105–114. doi:10.1200/EDBK_243729
8. Mills EJ, Seely D, Rachlis B, et al. Barriers to participation in clinical trials of cancer: a meta-analysis and systematic review of patient-reported factors. Lancet Oncol. 2006;7(2):141–148. doi:10.1016/S1470-2045(06)70576-9
9. Bell JAH, Balneaves LG. Cancer patient decision making related to clinical trial participation: an integrative review with implications for patients’ relational autonomy. Support Care Cancer. 2015;23(4):1169–1196.
10. Gillies K, Cotton SC, Brehaut JC, Politi MC, Skea Z. Decision aids for people considering taking part in clinical trials. Cochrane Database Syst Rev. 2015;11.
11. Biedrzycki. Research Participation: Decision Making and Outcomes in Cancer Clinical Trials. Johns Hopkins University; 2010:216.
12. Spittler CA. Exploration of How Women Make Treatment Decisions After a Breast Cancer Diagnosis. Ann Arbor: University of Kansas; 2011:172.
13. Truong TH, Weeks JC, Cook EF, et al. Altruism among participants in cancer clinical trials. Clin Trials. 2011;8(5):616–623. doi:10.1177/1740774511414444
14. Shah A, Efstathiou JA, Paly JJ, et al. Prospective preference assessment of patients‘ willingness to participate in a randomized controlled trial of intensity-modulated radiotherapy versus proton therapy for localized prostate cancer. Int J Radiat Oncol Biol Phys. 2012;83(1):e13–e19. doi:10.1016/j.ijrobp.2011.11.072
15. Chow CJ, Habermann EB, Abraham A, et al. Does enrollment in cancer trials improve survival? J Am Coll Surg. 2013;216(4):774. doi:10.1016/j.jamcollsurg.2012.12.036
16. Gregersen TA, Birkelund R, Wolderslund M, et al. What matters in clinical trial decision-making: a systematic review of interviews exploring cancer patients’ experiences. Scand J Caring Sci. 2019;33(2):266–278. doi:10.1111/scs.12637
17. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339(jul21 1):b2535. doi:10.1136/bmj.b2535
18. Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8(1):45. doi:10.1186/1471-2288-8-45
19. Lachal J, Revah-Levy A, Orri M, et al. Metasynthesis: an original method to synthesize qualitative literature in psychiatry. Front Psychiatry. 2017;8:269. doi:10.3389/fpsyt.2017.00269
20. Hossain LN, Fernandez-Llimos F, Luckett T, et al. Qualitative meta-synthesis of barriers and facilitators that influence the implementation of community pharmacy services: perspectives of patients, nurses and general medical practitioners. BMJ Open. 2017;7(9):e015471. doi:10.1136/bmjopen-2016-015471
21. Kmet LM, Cook LS, Lee RC. Standard quality assessment criteria for evaluating primary research papers from a variety of fieldsAHFMRHTA Initiative20040213. 2004;2.
22. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
23. Abhyankar P, Velikova G, Summers B, et al. Identifying components in consent information needed to support informed decision making about trial participation: an interview study with women managing cancer. Soc Sci Med. 2016;161:83–91. doi:10.1016/j.socscimed.2016.05.040
24. Burke NJ. Rethinking the therapeutic misconception: social justice, patient advocacy, and cancer clinical trial recruitment in the US safety net. BMC Med Ethics. 2014;15(1):68. doi:10.1186/1472-6939-15-68
25. Cox K. Researching research: patients‘ experiences of participation in phase I and II anti-cancer drug trials. Eur J Oncol Nurs. 1999;3(3):143–152. doi:10.1016/S1462-3889(99)80705-4
26. Cox K. Informed consent and decision-making: patients’ experiences of the process of recruitment to phases I and II anti-cancer drug trials. Patient Educ Couns. 2002;46(1):31–38. doi:10.1016/S0738-3991(01)00147-1
27. Coyne CA, Demian-Popescu C, Brown P. Rural cancer patients’ perspectives on clinical trials: a qualitative study. J Cancer Educ. 2004;19(3):165–169. doi:10.1207/s15430154jce1903_11
28. Davis CJ. Psychological Factors That Influence Patient Participation in Cancer Clinical Trials. (BL: DXN053473). Ann Arbor: University of Hull (United Kingdom); 2001:1.
29. Dimond DL, Holifield EA. Factors That Affect the Surgical Decision-Making Process Among Women with Breast Cancer. Ann Arbor: University of Michigan-Flint; 2009:64.
30. Ellington L, Wahab S, Sahami Martin S, et al. Factors that influence Spanish- and English-speaking participants’ decision to enroll in cancer randomized clinical trials. Psychooncology. 2006;15(4):273–284. doi:10.1002/pon.943
31. Harrop E, Kelly J, Griffiths G, et al. Why do patients decline surgical trials? Findings from a qualitative interview study embedded in the cancer research UK BOLERO trial (bladder cancer: open versus lapararoscopic or RObotic cystectomy). Trials. 2016;17(1):35. doi:10.1186/s13063-016-1173-z
32. Haynes-Maslow L, Godley P, Dimartino L, et al. African American women’s perceptions of cancer clinical trials. Cancer Med. 2014;3(5):1430–1439. doi:10.1002/cam4.284
33. Hercinger MM. Treatment Decision-Making in Older Adults with Cancer. Ann Arbor: The University of Nebraska - Lincoln; 2007:200.
34. Hopper TM. The Lack of African-American Participation in Cancer Clinical Trials: Mistrust of Medical Researchers. Ann Arbor: Capella University; 2007:141.
35. Lee GE, Ow M, Lie D, et al. Barriers and facilitators for clinical trial participation among diverse Asian patients with breast cancer: a qualitative study. BMC Womens Health. 2016;16(1):43. doi:10.1186/s12905-016-0319-1
36. Madsen SM, Holm S, Riis P. Participating in a cancer clinical trial? The balancing of options in the loneliness of autonomy: a grounded theory interview study. Acta Oncol. 2007;46(1):49–59. doi:10.1080/02841860600911164
37. Moynihan C, Lewis R, Hall E, et al. The patient deficit model overturned: a qualitative study of patients‘ perceptions of invitation to participate in a randomized controlled trial comparing selective bladder preservation against surgery in muscle invasive bladder cancer (SPARE, CRUK/07/011). Trials. 2012;13(1):228. doi:10.1186/1745-6215-13-228
38. Palmer-Wackerly AL, Dailey PM, Krok-Schoen JL, et al. Patient perceptions of illness identity in cancer clinical trial decision-making. Health Commun. 2018;33(8):1045–1054. doi:10.1080/10410236.2017.1331189
39. Quinn GP, Pratt CL, Bryant-George K, et al. Lung cancer patients’ decisions about clinical trials and the theory of planned behavior. J Cancer Educ. 2011;26(4):641–648. doi:10.1007/s13187-010-0169-8
40. Quinn GP, Koskan A, Wells KJ, et al. Cancer patients‘ fears related to clinical trial participation: a Qualitative Study. J Cancer Educ. 2012;27(2):257–262. doi:10.1007/s13187-012-0310-y
41. Ramers-Verhoeven CW, Perrone F, Oliver K. Exploratory research into cancer patients’ attitudes to clinical trials. ecancermedicalscience. 2014;8:1.
42. Ridgeway JL, Asiedu GB, Carroll K, et al. Patient and family member perspectives on searching for cancer clinical trials: a qualitative interview study. Patient Educ Couns. 2017;100(2):349–354. doi:10.1016/j.pec.2016.08.020
43. Sanders T. Factors Influencing Treatment Decisions for Patients with Colorectal Cancer. Ann Arbor: University of Bath (United Kingdom); 2000:348.
44. Skousen T. Decision Making in a Health-Care Crisis: Men Under 60 Diagnosed with Prostate Cancer. Ann Arbor: The University of Utah; 2006:240.
45. Stevens T, Ahmedzai SH. Why do breast cancer patients decline entry into randomised trials and how do they feel about their decision later: a prospective, longitudinal, in-depth interview study. Patient Educ Couns. 2004;52(3):341–348. doi:10.1016/S0738-3991(03)00041-7
46. Huizinga GA, Sleijfer DT, van de Wiel HBM, et al. Decision-making process in patients before entering phase III cancer clinical trials: a pilot study. Cancer Nurs. 1999;22(2):119–125. doi:10.1097/00002820-199904000-00003
47. Ebbert JA. Multiple Case Study of Factors Associated with Enrollment of Women with Persistent or Recurrent Ovarian Cancer in Clinical Trials in Central Florida. Ann Arbor: University of South Florida; 2016:219.
48. Brown RF, Cadet DL, Houlihan RH, et al. Perceptions of participation in a Phase I, II, or III clinical trial among African American patients with cancer: what do refusers say? J Oncol Pract. 2013;9(6):287–293. doi:10.1200/JOP.2013.001039
49. Godskesen T, Hansson MG, Nygren P, et al. Hope for a cure and altruism are the main motives behind participation in Phase 3 clinical cancer trials. Eur J Cancer Care (Engl). 2015;24(1):133–141. doi:10.1111/ecc.12184
50. Brown RF, Shuk E, Leighl N, et al. Enhancing decision making about participation in cancer clinical trials: development of a question prompt list. Support Care Cancer. 2011;19(8):1227–1238. doi:10.1007/s00520-010-0942-6
51. Cox K. The hopes of the dying: examining patients’ experience of participation in early phase cancer clinical trials … including commentary by Copp G. NT Res. 2002;7(1):60–74. doi:10.1177/136140960200700110
52. Dellson P, Nilsson K, Jernström H, et al. Patients’ reasoning regarding the decision to participate in clinical cancer trials: an interview study. Trials. 2018;19(1):528. doi:10.1186/s13063-018-2916-9
53. Godskesen T, Nygren P, Nordin K, et al. Phase 1 clinical trials in end-stage cancer: patient understanding of trial premises and motives for participation. Support Care Cancer. 2013;21(11):3137–3142. doi:10.1007/s00520-013-1891-7
54. Madsen S, Holm S, Riis P. Attitudes towards clinical research among cancer trial participants and non-participants: an interview study using a grounded theory approach. J Med Ethics. 2007;33(4):234–240. doi:10.1136/jme.2005.015255
55. Schutta KM, Burnett CB. Factors that influence a patient’s decision to participate in a phase I cancer clinical trial. Oncol Nurs Forum. 2000;27(9):1435–1438.
56. Asiedu GB, Ridgeway JL, Carroll K, Jatoi A, Radecki Breitkopf C. Ultimately, mom has the call”: viewing clinical trial decision making among patients with ovarian cancer through the lens of relational autonomy. Health Expect. 2018;21(6):981–9.
57. Krieger J, Palmer-Wackerly A, Dailey PM, et al. Comprehension of randomization and uncertainty in cancer clinical trials decision making among rural, appalachian patients. J Cancer Educ. 2015;30(4):743–748. doi:10.1007/s13187-015-0789-0
58. Lee GE. Factors associated with willingness to participate in clinical trials among diverse Asian patients with breast cancer. Eur J Cancer. 2016;60:e7. doi:10.1016/j.ejca.2016.03.030
59. Wallington SF, Luta G, Noone AM, et al. Assessing the awareness of and willingness to participate in cancer clinical trials among immigrant Latinos. J Community Health. 2012;83(1):e13–e19. doi:10.1007/s10900-011-9450-y
60. Townsley CA, Chan KK, Pond GR, et al. Understanding the attitudes of the elderly towards enrolment into cancer clinical trials. BMC Cancer. 2006;6(1):34. doi:10.1186/1471-2407-6-34
61. Catt S, Langridge C, Fallowfield L, et al. Reasons given by patients for participating, or not, in Phase 1 cancer trials. Eur J Cancer. 2011;47(10):1490–1497. doi:10.1016/j.ejca.2011.02.020
62. Mills N, Donovan JL, Smith M, Jacoby A, Neal DE, Hamdy FC. Perceptions of equipoise are crucial to trial participation: a qualitative study of men in the ProtecT study. Control Clin Trials. 2008;8(1):272–282. doi:10.1016/S0197-2456(03)00020-5
63. Gordon EJ, Daugherty CK. Referral and decision making among advanced cancer patients participating in phase I trials at a single institution. J Clin Ethics. 2001;12(1):31–38.
64. Harrop JP, Dean JA, Paskett ED. Cancer survivorship research: a review of the literature and summary of current NCI-designated cancer center projects. Cancer Epidemiol Biomarkers Prev. 2011;20(10):2042–2047. doi:10.1158/1055-9965.EPI-11-0673
65. Cox K. A Means to an End?: a Study of Patients’ Experiences of Participation in Phase I and Ii Anti-Cancer Drug Trials. Ann Arbor: The University of Nottingham (United Kingdom); 1999:1.
66. Charles C, Gafni A, Whelan T. Decision-making in the physician-patient encounter: revisiting the shared treatment decision-making model. Soc Sci Med. 1999;49:651–661.
67. Brehaut JC, Fergusson DA, Kimmelman J, et al. Using decision aids may improve informed consent for research. Contemp Clin Trials. 2010;31(3):218–220. doi:10.1016/j.cct.2010.02.002
68. Feldman-Stewart D, O’Brien MA, Clayman ML, et al. Providing information about options in patient decision aids. BMC Med Inform Decis Mak. 2013;13(S2):S4. doi:10.1186/1472-6947-13-S2-S4
69. Brehaut JC, Lott A, Fergusson DA, et al. Can patient decision aids help people make good decisions about participating in clinical trials? A study protocol. Implement Sci. 2008;3(1):38. doi:10.1186/1748-5908-3-38
70. Elliott D, Husbands S, Hamdy FC, et al. Understanding and improving recruitment to randomised controlled trials: qualitative research approaches. Eur Urol. 2017;72(5):789–798. doi:10.1016/j.eururo.2017.04.036
71. Kadam RA. Informed consent process: A step further towards making it meaningful! Perspect Clin Res. 2017;8(3):107–112.
72. Elmore JG, Ganschow PS, Geller BM. Communication between patients and providers and informed decision making. J Natl Cancer Inst Monogr. 2010;2010(41):204–209. doi:10.1093/jncimonographs/lgq038
73. Nishimura A, Carey J, Erwin PJ, et al. Improving understanding in the research informed consent process: a systematic review of 54 interventions tested in randomized control trials. BMC Med Ethics. 2013;14(1):28. doi:10.1186/1472-6939-14-28
74. Stacey CD. Development and Evaluation of a Breast Cancer Prevention Decision Aid to Address the Needs of Women Aged 50 and Older at High Risk for Breast Cancer. Ann Arbor: University of Ottawa (Canada); 2000:227.
75. Klein PD. Rethinking the multiplicity of cognitive resources and curricular representations: alternatives to ‘learning styles‘ and ‘multiple intelligences’. J Curric Stud. 2003;35(1):45–81. doi:10.1080/00220270210141891
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.