")
Back to Journals » Cancer Management and Research » Volume 11
Decentralized colorectal cancer care in Germany over the last decade is associated with high in-hospital morbidity and mortality
Authors Ghadban T , Reeh M , Bockhorn M, Grotelueschen R, Bachmann K, Grupp K, Uzunoglu FG, Izbicki JR, Perez DR
Received 12 December 2018
Accepted for publication 21 January 2019
Published 12 March 2019 Volume 2019:11 Pages 2101—2107
DOI https://doi.org/10.2147/CMAR.S197865
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Tarik Ghadban,* Matthias Reeh,* Maximilian Bockhorn, Rainer Grotelueschen, Kai Bachmann, Katharina Grupp, Faik G Uzunoglu, Jakob R Izbicki, Daniel R Perez
Department of General, Visceral and Thoracic Surgery, University Medical Center Hamburg-Eppendorf, 20246 Hamburg, Germany
*These authors contributed equally to this work
Purpose: Despite several national initiatives, centralization of cancer care in Germany remains insufficient for most malignancies. Currently, there is a plethora of centers, including 290 voluntary certified and audited colorectal cancer (CRC) centers by the end of 2017, in the nation with many patients still being treated outside of such centers. This study aimed to assess morbidity and mortality rates of surgical procedures for primary colorectal CRC in Germany over the last decade through a comprehensive unbiased analysis.
Patients and methods: We performed an analysis of the national diagnosis-related group inpatient statistics from 2005 to 2015 including all German hospitals. All patients who underwent surgeries for primary CRC during the study period were included.
Results: A total of 351,028 cases were analyzed (61.6% colonic and 38.4% rectal resections). The mortality rate of colonic resections remained high during the study period (4.9% in 2005 vs 4.5% in 2015; P=0.57). Reduced perioperative mortality after rectal surgery was observed only after 2012 compared to previous years (3.8% in 2005 vs 3.0% in 2015; P<0.001), with no further improvement. In-hospital morbidity such as anastomotic leak, wound infections, hemorrhage, pneumonia, deep vein thrombosis, and lung embolism did not improve for either rectal or for colonic surgery, but in contrast, most outcomes deteriorated over time.
Conclusion: The present study challenges the current national health policies aiming to improve outcomes of surgical patients. CRC care in Germany remains decentralized with high in-hospital morbidity and mortality rates. New national strategies focusing on the implementation of centralization and high-quality CRC care are urgently needed.
Keywords: outcome, centralization, CRC, surgery, certification, colorectal cancer
Introduction
In Germany, over 60,000 cases of colorectal cancer (CRC) are diagnosed each year. CRC is the third most common cancer in both men and women, and 25,000 patients die because of CRC each year.1
Traditionally, CRC surgery has been performed in most hospitals across Germany, with no legal restriction for hospitals to treat CRC patients, and even nowadays, the situation remains the same.
In 2015, ~30,000 surgical procedures for CRC were undertaken in Germany. The recently published German data suggest excellent outcomes, with low morbidity and mortality rates.2 However, these data were generated by single- or multicenter studies in high-volume centers, whereas smaller or less-experienced centers do not tend to publish their results. Given that a large proportion of patients do not undergo surgery in high-volume centers, the published data may thus lead to misinterpretations of the outcomes of surgery for CRC in Germany. A recent population-based study reported a mortality rate of 3.2% in Germany, which is higher than that reported in a randomized trial (1.1%).2,3
In the early 2000s, a European study suggested that despite enormous financial resources, the results regarding cancer survival in Germany were only moderate compared to the results obtained in other European countries.4 This led to several initiatives aimed at improving care for CRC patients, such as the development of clinical guidelines and a novel but voluntary auditing process by the German Cancer Society [Deutsche Krebsgesellschaft, DKG] at institutions treating CRC patients. Institutions complying with the requirements set by the DKG are certified as CRC centers.
Since 2004, the German hospital remuneration process for inpatient treatment has been regulated through the diagnosis-related group (DRG) system. Data relating to every inpatient hospital stay, including the diagnosis and procedure codes, are entered into the nationwide DRG database. Individuals’ hospitalization data are available for research purposes within the context of the regulations that surround confidentiality. Federal law allows the data to be used for scientific purposes without an ethical review. In the past, several important studies based on DRG data have been published.5–8 In 2005, the DRG database included 1,725 hospitals with a continuous decrease in the number of hospitals, which counted 1,514 in 2015.
This study aimed to evaluate trends in in-hospital morbidity and mortality associated with primary CRC patients undergoing operations in Germany over the last decade, through a comprehensive and unbiased analysis using DRG data.
Patients and methods
Data
A controlled remote analysis of the nationwide DRG database from 2005 to 2015 was undertaken to evaluate inpatient data provided by the Research Data Centers of the Federal Statistical Office and the Statistical Offices of the Länder. The German adaptation of the International Classification of Diseases (ICD) Tenth Revision and the procedure coding system [Operationen- und Prozedurenschlüssel, OPS] were used to identify diagnoses and procedures.
Case definitions, types of surgery, and principal diagnoses
Every inpatient case with a procedure code for an elective colorectal resection with CRC as the primary diagnosis was included. Laparoscopic, converted, and open colectomies (right-sided, transverse colon, left-sided, and sigmoid) and laparoscopic and open rectal resections (anterior, abdominoperineal, and abdominosacral) were included. Converted cases were classified as open surgery. Used ICD codes were C18, C19, and C20, and the procedure codes were 5-455.01-7, 5-455.51-7, 5-456.01-7, 5-457.01-7, 5-484.31-9, 5-484.51-9, 5-484.61-9, 5-485.01-2, and 5-485.21-2.
Mortality
For each case, DRG data include the dismissal reason with a specific code for in-hospital death. Therefore, our reported mortality represents in-hospital mortality.
Morbidities
Secondary diagnoses I26, T81.0, T81.1, T81.3, T81.4, I80.2, K65, J1, and K91.83 were used to identify patients’ morbidities.
Statistical analyses
Data were analyzed descriptively. Temporal trends were assessed by using weighted least squares based on the number of observations. P-value <5% was considered as statistically significant. IBM® SPSS® software for Windows, version 24.0 (IBM Corporation, Armonk, NY, USA) was used. The reference was the outcome in 2005 where no certified centers existed.
Results
Surgical procedures
A total of 351,028 elective procedures for CRC were identified, including 216,272 (61.6%) colonic and 134,756 (38.4%) rectal resections (Figure 1). The proportion of cases that underwent minimally invasive surgery increased continuously. For colonic resections, the rate increased from 5.9% in 2005 to 20.3% in 2015 (P<0.001); for rectal resections, the corresponding rates were 7.4% and 38.4%, respectively (P<0.001; Figure 2). A total of 35,857 colon cancer cases were scheduled to undergo minimally invasive surgery, and, of these, 4,527 (12.6%) cases were converted to open surgery.
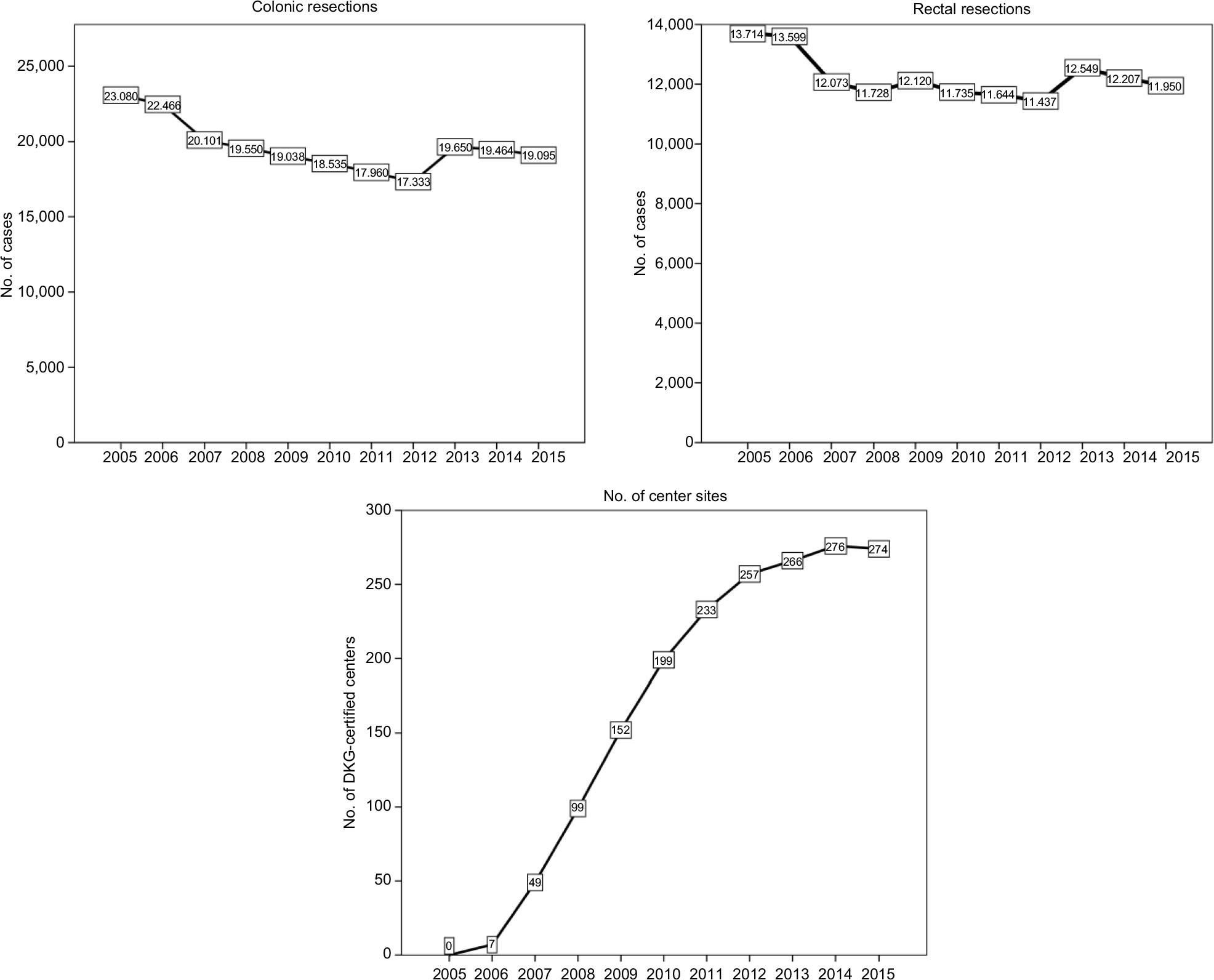 | Figure 1 Annual numbers of elective surgically treated CRC cases and development of certified center sites between 2005 and 2015. Abbreviations: CRC, colorectal cancer; DKG, German Cancer Society [Deutsche Krebsgesellschaft]. |
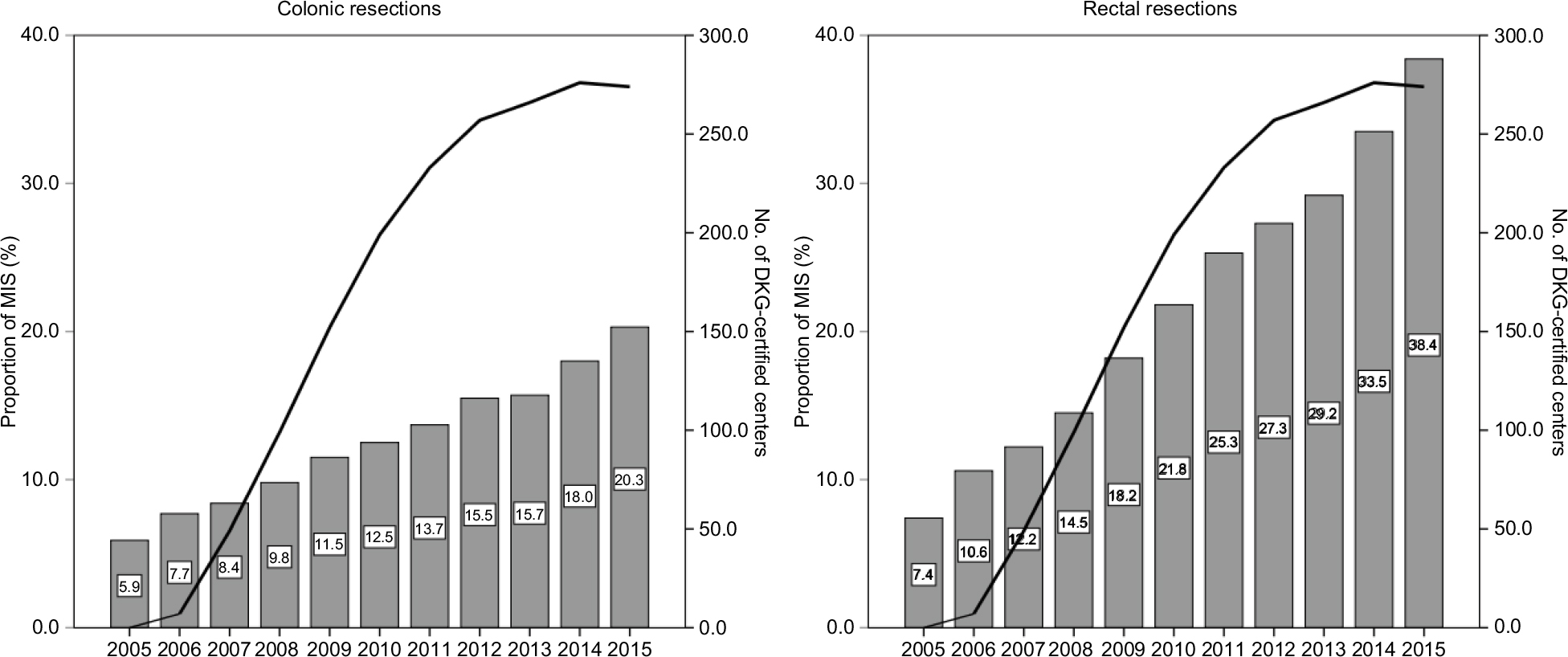 | Figure 2 Annual rates of MIS. Abbreviations: DKG, German Cancer Society [Deutsche Krebsgesellschaft]; MIS, minimally invasive surgery. |
Mortality
Over the 11-year period, no significant improvement in the mortality rate was observed for colonic resections (4.9% in 2005 vs 4.5% in 2015; P=0.57). For rectal resections, a significant improvement in the mortality rate was achieved since 2012 compared to 2005, with no further improvement found after 2012 (3.8% in 2005 vs 3.0% in 2015; P<0.001), as shown in Figure 3. The overall mortality rates for open and minimally invasive surgery were 4.7% and 1.8%, respectively (P<0.001).
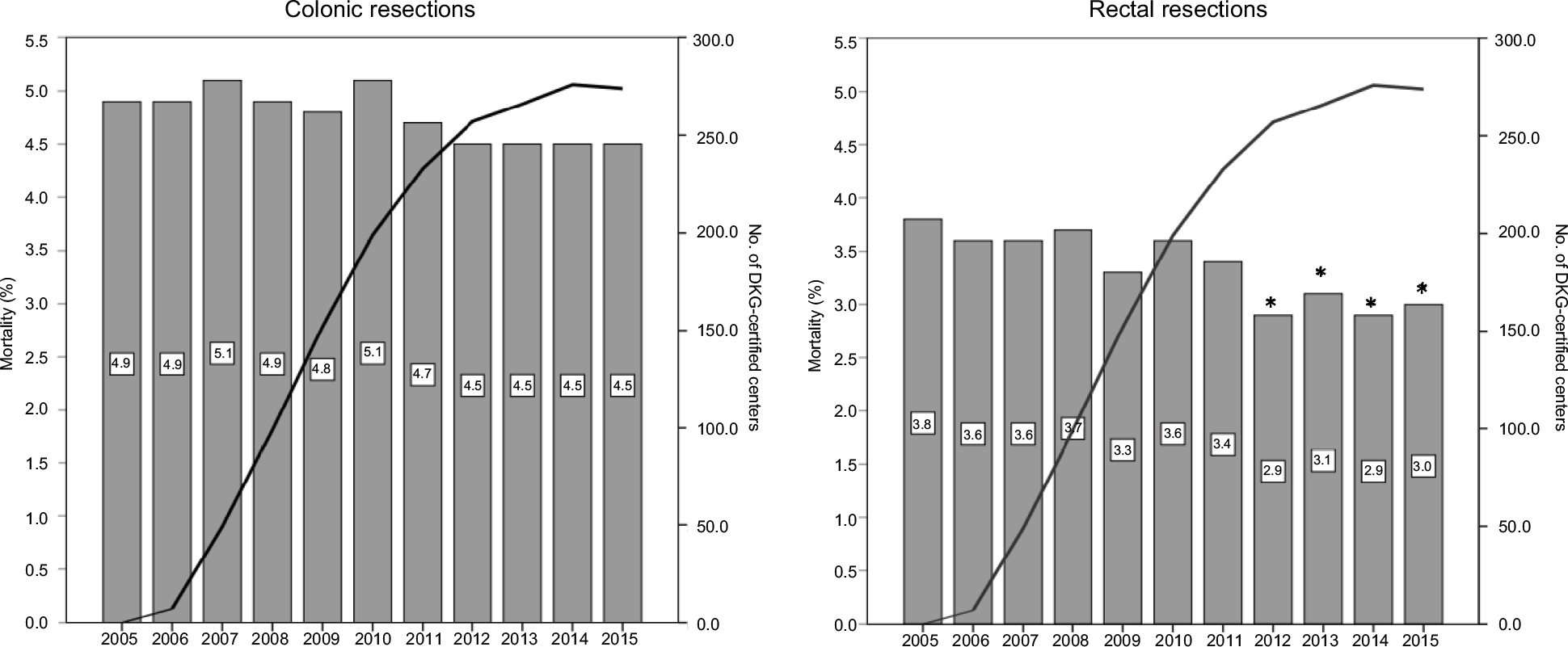 | Figure 3 Annual mortality rates of surgically treated CRC cases. Notes: *P<0.05 compared to 2005. Abbreviations: CRC, colorectal cancer; DKG, German Cancer Society [Deutsche Krebsgesellschaft]. |
Morbidity
We analyzed the rates of deep vein thrombosis, pulmonary embolism, wound and abdominal infections, postoperative hemorrhage, pneumonia, and anastomotic leaks. Between 2005 and 2015, no improvement in the morbidity rates was achieved for either rectal or colonic resections, whereas there was a trend of increasing morbidity rates, which in some cases reached statistical significance.
On comparing the morbidity rates in 2005 and 2015, the colon cancer cases showed an increased rate of anastomotic leaks from 3.9% to 5.9% (P<0.001), wound and abdominal infections from 4.9% to 7.0% (P<0.001), postoperative hemorrhage from 3.1% to 4.1% (P<0.001), pneumonia from 4.6% to 6.0% (P<0.001), and deep vein thrombosis and pulmonary embolism from 1.1% to 1.4% (P=0.018), as shown in Figure 4.
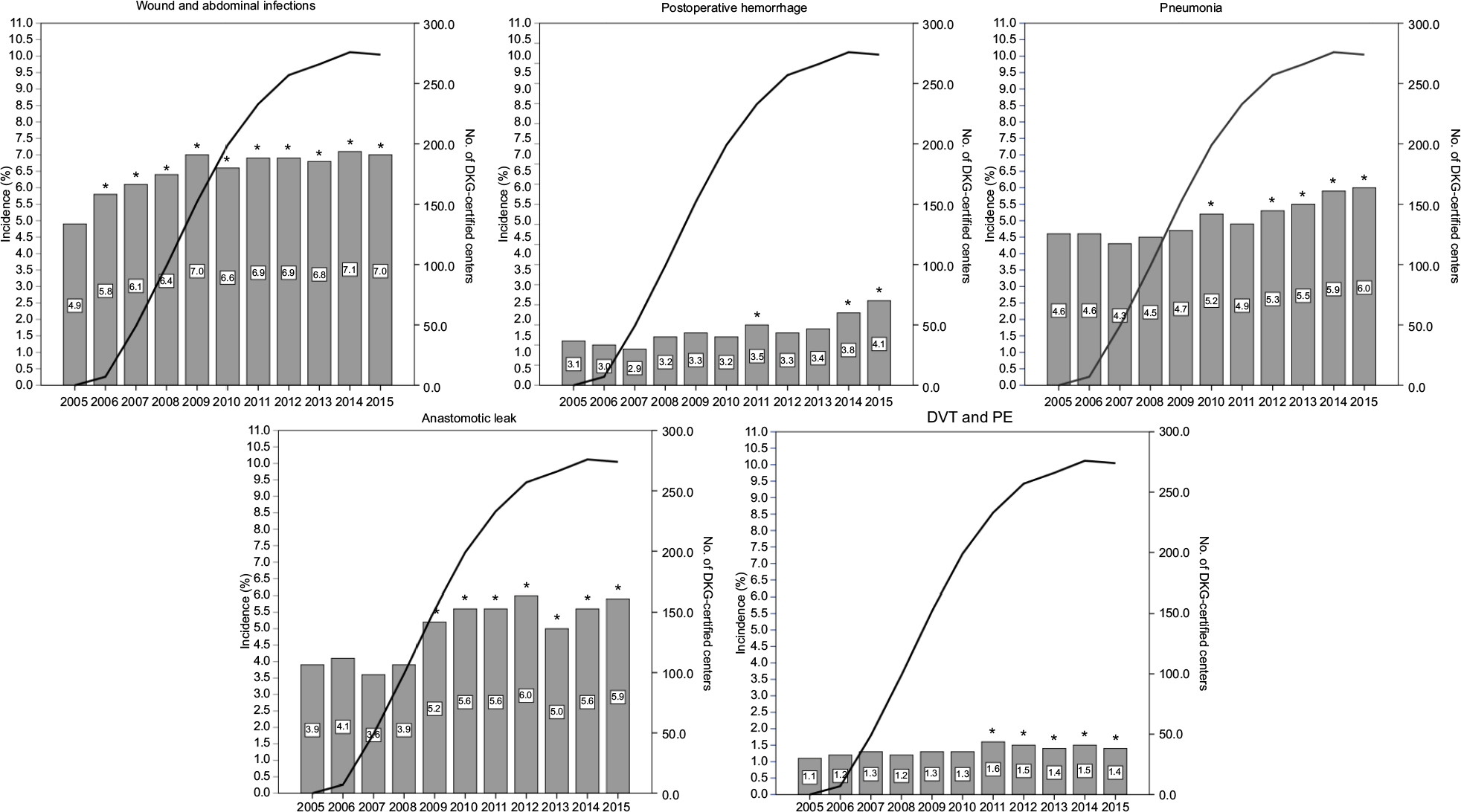 | Figure 4 Annual morbidity rates of surgically treated colonic cancer cases. Notes:*P<0.05 compared to 2005. Abbreviations: DKG, German Cancer Society [Deutsche Krebsgesellschaft]; DVT, deep vein thrombosis; PE, pulmonary embolism. |
For the rectal cancer cases, the rate of anastomotic leaks increased from 7.7% to 10.9% (P<0.001), wound and abdominal infections increased from 7.7% to 9.2% (P<0.001), postoperative hemorrhage tended to decrease from 4.8% to 4.6% (P=0.365), pneumonia increased from 4.2% to 4.9% (P=0.008), and deep vein thrombosis and pulmonary embolism tended to increase from 1.1% to 1.2% (P=0.751), as shown in Figure 5.
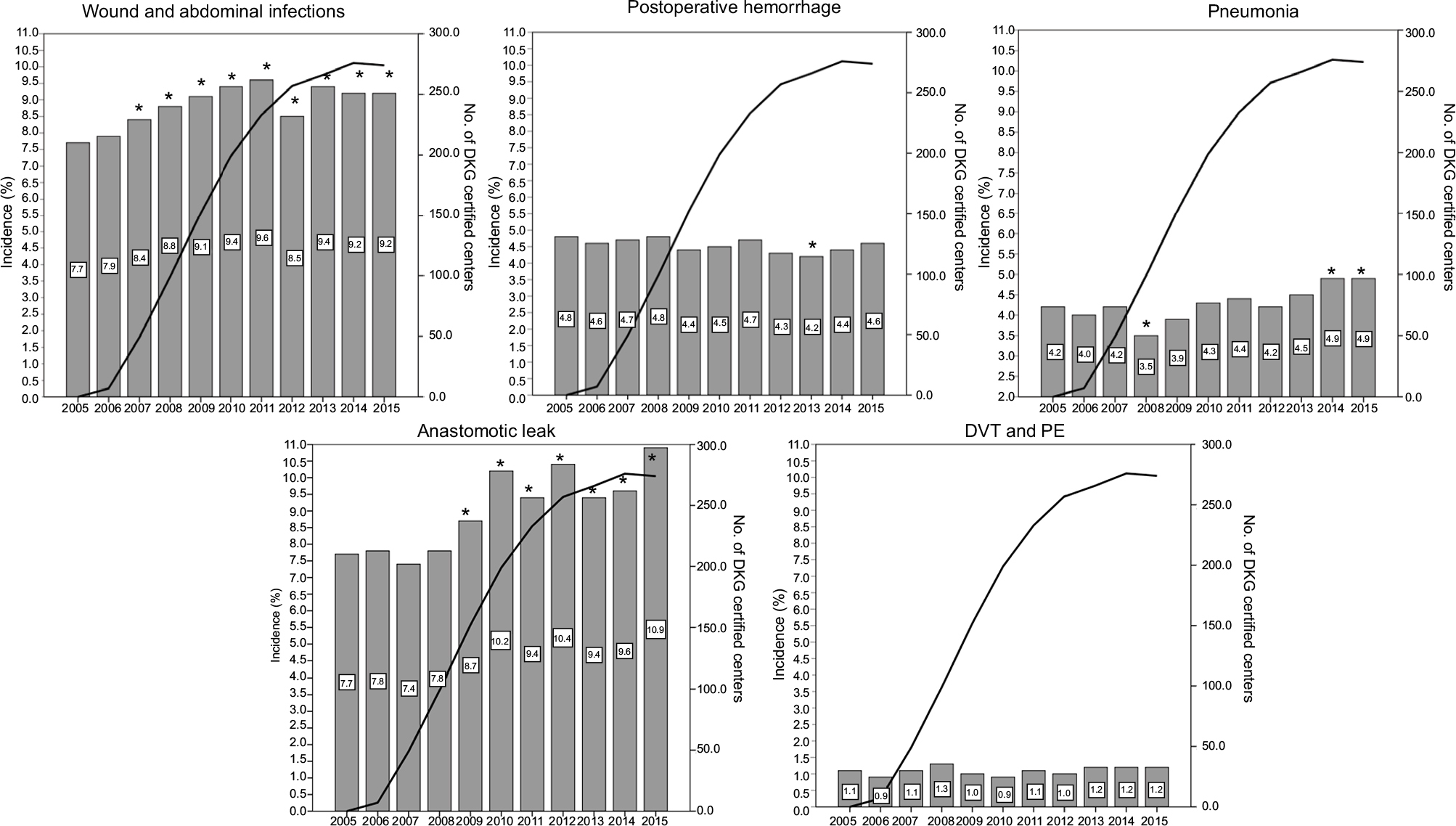 | Figure 5 Annual morbidity rates of surgically treated rectal cancer cases. Notes: *P<0.05 compared to 2005. Rectal extirpations were excluded in anastomotic leaks. Abbreviations: DKG, German Cancer Society [Deutsche Krebsgesellschaft]; DVT, deep vein thrombosis; PE, pulmonary embolism. |
Discussion
By the end of 2015, a total of 1,956 hospitals nationwide were providing acute care in Germany. Of these, 274 (14%) institutions were voluntarily undergoing an annual external auditing process to obtain certification as a CRC center. These centers deliver care for approximately two-thirds of all CRC patients. Currently, the requirements for certification by the German Cancer Society include a series of quality outcome measures (eg, anastomotic leak rate, reoperation rate), multidisciplinary institutional collaboration (eg, multidisciplinary tumor conference), psycho-oncological support, and a minimum number of annual primary operative cases for colon (n≥30) and rectal (n≥20) cancers. Despite the growing number of certified CRC centers over the last decade, the present study showed that the in-hospital patient outcomes are disappointing. Key outcome parameters such as the mortality and morbidity rates did not improve substantially between 2005 and 2015. In fact, except for the mortality rate of rectal cancer patients after the year 2012, most outcomes were worse by the end of the study period compared to those in 2005. The causes that might have led to increased short-term morbidity over the years are difficult to understand and can only be speculated (eg, demographic and/or epidemiologic changes or administrative changes such as “up-coding” of disease). After the implementation of the DRG system, the medical and administration staff learned to maximize the hospital’s revenue by including every possible diagnosis and procedure in the reimbursement process, and “up-coding” of diagnosis might hence have contributed to some results seen in this study; however, most outcome parameters are dichotomous (eg, mortality, deep vein thrombosis) and allow no room for interpretation.
In Germany, centralization of care is mainly driven by medical societies and by health care insurance providers. Legal regulations regarding centralization of patient care on a national level are absent. For some organ systems, there is more than one society offering certification pathways to be credentialed as a specialized center. This obviously contributes to the dispersion of expertise and caseload between the centers. Experiences in other countries which followed centralization and in-service training strategies could show a significant decrease of mortality rates. Results from Denmark showed a decrease from 7.3% in 2001–2002 to 2.8% in 2011.9 In the Netherlands, a decrease from 3.4% to 1.8% in colon cancer and from 2.3% to 1% in rectal cancer between 2009 and 2016 was reported.10
The development of minimally invasive surgery during the last two decades has led to a steady increase in the number of minimally invasive colorectal resections undertaken.11–13 The results from several randomized trials have demonstrated that the long-term oncologic outcomes associated with laparoscopic resections are comparable with those of open surgery, and that laparoscopic resection is superior regarding short-term outcomes.14–20 In Germany, the use of minimally invasive surgery for colon (20%) and rectal (38%) cancers constantly increased over the study period, but still remains far lower compared to the international benchmark. National training programs, such as the laparoscopic colorectal surgery national training program in the UK, help to develop surgical skills and promote acceptance of new techniques in the surgical community. At present, similar national programs have not been implemented in Germany.
A major strength of this study is the completeness of data. The analysis was based on all nationwide hospital-based visits and is, therefore, not affected by selection bias. The present data represent comprehensive results rather than a statistical sample, and the results are true values as opposed to estimates. Moreover, the data were unaffected by the hospitals’ self-reporting.
Although the study is likely to be representative of the state of CRC care in Germany, it does have some limitations. Especially, data were collected from administrative records in an anonymized fashion. The anonymization of the DRG data rules out any validation of the data that could be achieved by comparing the assigned codes with representative samples of the patients’ case notes. DRG validation studies at particular hospitals would not be of any benefit because they would not be representative of the population as a whole and routine documentation in hospitals cannot necessarily be considered the gold standard for validation. Furthermore, any comparative analysis at the hospital level or between certified and non-certified centers is missing.
Conclusion
The present study challenges the current national health policies aiming to improve outcomes of cancer patients. This population-based analysis of mortality and morbidity after CRC surgery in Germany from an independent data source revealed no substantial improvements over time despite implementation of certification with minimum volume standards with high in-hospital morbidity and mortality rates. New national strategies focusing on the implementation of centralization and quality improvement of CRC care are urgently needed.
Disclosure
The authors report no conflicts of interest in this work.
References
Cancer in Germany 2011/2012. 10th edition. Berlin, Germany: Robert Koch Institute (ed.) and the Association of Population-based Cancer Registries in Germany. 2016. | ||
Benz S, Barlag H, Gerken M, Fürst A, Klinkhammer-Schalke M. Laparoscopic surgery in patients with colon cancer: a population-based analysis. Surg Endosc. 2017;31(6):2586–2595. | ||
Schwenk W, Neudecker J, Haase O. [Current evidence for laparoscopic surgery of colonic cancer]. Chirurg. 2014;85(7):570–577. German. | ||
Sant M, Capocaccia R, Verdecchia A, et al. Survival of women with breast cancer in Europe: variation with age, year of diagnosis and country. The EUROCARE Working Group. Int J Cancer. 1998;77(5):679–683. | ||
Nimptsch U, Krautz C, Weber GF, Mansky T, Grützmann R. Nationwide in-hospital mortality following pancreatic surgery in Germany is higher than anticipated. Ann Surg. 2016;264(6):1082–1090. | ||
Stang A, Katalinic A, Dieckmann KP, et al. A novel approach to estimate the German-wide incidence of testicular cancer. Cancer Epidemiol. 2010;34(1):13–19. | ||
Stang A, Merrill RM, Kuss O. Hysterectomy in Germany: a DRG-based nationwide analysis, 2005–2006. Dtsch Arztebl Int. 2011;108(30):508–514. | ||
Stang A, Merrill RM, Kuss O. Nationwide rates of conversion from laparoscopic or vaginal hysterectomy to open abdominal hysterectomy in Germany. Eur J Epidemiol. 2011;26(2):125–133. | ||
Iversen LH, Ingeholm P, Gögenur I, Laurberg S. Major reduction in 30-day mortality after elective colorectal cancer surgery: a nationwide population-based study in Denmark 2001–2011. Ann Surg Oncol. 2014;21(7):2267–2273. | ||
de Neree Tot Babberich MPM, Detering R, Dekker JWT, et al; Dutch ColoRectal Audit Group. Achievements in colorectal cancer care during 8 years of auditing in the Netherlands. Eur J Surg Oncol. 2018;44(9):1361–1370. | ||
Alnasser M, Schneider EB, Gearhart SL, et al. National disparities in laparoscopic colorectal procedures for colon cancer. Surg Endosc. 2014;28(1):49–57. | ||
Yeo H, Niland J, Milne D, et al. Incidence of minimally invasive colorectal cancer surgery at national comprehensive cancer network centers. J Natl Cancer Inst. 2015;107(1):362. | ||
Lee MG, Chiu CC, Wang CC, et al. Trends and outcomes of surgical treatment for colorectal cancer between 2004 and 2012- an analysis using national inpatient database. Sci Rep. 2017;7:2006. | ||
Lacy AM, Delgado S, Castells A, et al. The long-term results of a randomized clinical trial of laparoscopy-assisted versus open surgery for colon cancer. Ann Surg. 2008;248(1):1–7. | ||
Clinical Outcomes of Surgical Therapy Study Group; Nelson H, Sargent DJ, Wieand HS, et al. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med. 2004;350(20):2050–2059. | ||
Colon Cancer Laparoscopic or Open Resection Study Group; Buunen M, Veldkamp R, Hop WC, et al. Survival after laparoscopic surgery versus open surgery for colon cancer: long-term outcome of a randomised clinical trial. Lancet Oncol. 2009;10(1):44–52. | ||
Fleshman J, Sargent DJ, Green E, et al. Laparoscopic colectomy for cancer is not inferior to open surgery based on 5-year data from the COST Study Group trial. Ann Surg. 2007;246(4):655–664. | ||
Jayne DG, Guillou PJ, Thorpe H, et al. Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC trial group. J Clin Oncol. 2007;25(21):3061–3068. | ||
Guillou PJ, Quirke P, Thorpe H, et al. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet. 2005;365(9472):1718–1726. | ||
Jayne DG, Thorpe HC, Copeland J, Quirke P, Brown JM, Guillou PJ. Five-year follow-up of the Medical Research Council CLASICC trial of laparoscopically assisted versus open surgery for colorectal cancer. Br J Surg. 2010;97(11):1638–1645. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.