")
Back to Journals » Journal of Pain Research » Volume 9
D2-like receptors in the descending dopaminergic pathway are not involved in the decreased postoperative nociceptive threshold induced by plantar incision in adult rats
Received 23 August 2016
Accepted for publication 28 September 2016
Published 21 October 2016 Volume 2016:9 Pages 865—869
DOI https://doi.org/10.2147/JPR.S120470
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael Schatman
Norimasa Ohtani, Eiji Masaki
Division of Dento-oral Anesthesiology, Tohoku University Graduate School of Dentistry, Sendai, Miyagi, Japan
Background: Approximately half of all patients who undergo surgery develop postoperative pain, the mechanisms of which are not well understood by anesthesiologists. D2-like receptors in the descending dopaminergic pathway play an important role in regulation of pain transmission in the spinal cord. Impairment of inhibitory neurons in the spinal cord is suggested as part of the mechanism for neuropathic pain, which is one component of postoperative pain. The purpose of this study was to investigate whether impairment of D2-like receptors in the descending dopaminergic pathway in the spinal cord is involved in the decreased postoperative nociceptive threshold in rats.
Methods: Male Sprague-Dawley rats (250–300 g) were anesthetized with sevoflurane and an intrathecal (IT) catheter was implanted. Six days later, a plantar incision was made. On the following day, saline, a D2-like receptor agonist (quinpirole), or a D2-like receptor antagonist (sulpiride) was administered intrathecally. Thermal and mechanical nociceptive responses were assessed by exposure to infrared radiant heat and the von Frey filament test before and after plantar incision.
Results: Plantar incision decreased both thermal latency and the mechanical nociceptive threshold. IT administration of quinpirole inhibited the nociceptive responses induced by plantar incision, but sulpiride had no effect.
Conclusion: A D2-like receptor agonist had antinociceptive effects on the hypersensitivity response triggered by a surgical incision, but a D2-like receptor antagonist had no effect on this response. These results suggest that impairment and/or modification of D2-like receptors in the descending dopaminergic pathway in the spinal cord is not involved in the postoperative decrease in nociceptive threshold.
Keywords: postoperative pain, descending pathway, dopamine, D2-like receptor, quinpirole, sulpiride
Introduction
Postoperative pain is very difficult to treat because it comprises different types of pain, including pain with a neuropathic component. The mechanisms of neuropathic pain are still not well understood, so treatment for this type of pain remains difficult. Chemical modulators of pain are released in the spinal cord after surgical incision or nerve injury1 and cause aberrant nociceptive signaling.2,3 Impairment of inhibitory neurons induced by such chemical modulators is one of the possible mechanisms of neuropathic pain.4
Among the descending spinal pathways, relatively little is known about the role of the dopaminergic pathway, but recent evidence indicates that D1-like receptors mediate pronociceptive signals whereas D2-like receptors are involved in antinociception. It has also been reported that activation of the spinal D1-like receptor exacerbates N-methyl-d-aspartate receptor-induced hyperexcitability5 and the intrathecal (IT) administration of a D2-like receptor agonist has an antinociceptive effect in rats.6 Further, there is some evidence that the neuroplasticity contributing to the development of pathological pain states may be mediated by a D1/D5 mechanism in the spinal cord.7 However, it is not known whether impairment of D2-like receptors is involved in pathological pain states, including early postoperative pain.
The aim of this study was to investigate the contribution of D2-like receptors in the descending dopaminergic pathway to the decrease in nociceptive threshold seen during the early postoperative period. Our hypothesis was that a D2-like agonist would have a pronociceptive effect and a D2-like antagonist would have an antinociceptive effect if D2-like receptors in the descending pathways are impaired or modulated after surgery. To examine this hypothesis, we investigated the effect of IT administration of a D2-like agonist and antagonist on mechanical allodynia and heat hypersensitivity after surgical incision in a rat model of postoperative pain.
Materials and methods
Ethics statement
This study was approved by the Animal Care Committee of Tohoku University (permit number 2015DnA-030) and all animal procedures were conducted in concordance with the Guiding Principles for the Care and Use of Animals in the Field of Physiological Science published by the Physiological Society of Japan.
Animals
Male Sprague-Dawley rats (250−300 g) were housed individually in standard animal cages under a 12-hour light/dark cycle with controlled temperature (22°C), humidity (40%–50%), and had free access to water and food. In total, 156 rats were used in this study. The animals were acclimated to these conditions for 6 days before experimentation.
IT catheterization
An IT catheter for administration of saline or drugs was implanted in each rat under sevoflurane anesthesia (3.0%) in oxygen following the method described by Yaksh and Rudy8 with minor modifications. Each rat was secured in a stereotaxic frame with the head flexed forward. After shaving and sterilizing the skin with povidone iodine, midline skin and fascia incisions were made and the atlanto-occipital membrane was exposed. The membrane was carefully punctured using a 22-gauge needle, and a single-lumen polyethylene-5 catheter (outer diameter 0.36 mm) connected by application of heat to a polyethylene-10 catheter (outer diameter 0.61 mm) was passed into the IT space at the L4–L5 spinal segment. The rats were monitored for any neurologic deficit after catheterization, and any showing signs of a neurologic deficit were removed from the study.
Plantar incision
Six days after IT catheterization, a single 1 cm longitudinal incision was made through the skin and fascia on the plantar aspect of the left hind limb starting 0.5 cm from the end of the heel according to the method described by Brennan et al9 under sevoflurane anesthesia (3.0%) in oxygen. The underlying muscle was exposed, and the skin was then closed with two 5-0 nylon mattress sutures.
Drugs
Quinpirole hydrochloride (a D2-like agonist; Sigma-Aldrich, Tokyo, Japan) and sulpiride (a D2-like antagonist; Sigma-Aldrich) were dissolved in 0.9% normal saline without and with 0.1% dimethyl sulfoxide, respectively, and administered through the IT catheter at a volume of 10 µL followed by a 10 µL flush of normal saline. The dose of each drug was selected based on previous studies.10,11
Investigation of pain
The 156 rats were divided into four groups (control: 16 rats [anesthesia only for IT catheterization, no incision], saline: 20 rats, quinpirole: 60 rats, and sulpiride: 60 rats) for observation of the time course of changes in the behavioral response to pain after plantar incision. We also tested the pain response of the hind paw on the non-incision side in the quinpirole and sulpiride groups. The investigator assessing the behavioral tests was blinded to group allocation.
The rats were tested for thermal hypersensitivity and mechanical allodynia of the hind paw before plantar incision, on the day following the incision (before IT administration of quinpirole or sulpiride) and 5, 10, 15, 60, and 120 min after administration of quinpirole or sulpiride. Thermal hypersensitivity was evaluated using a plantar test apparatus (model 37370; Ugo Basile, Comerio, Italy). An infrared radiant heat source was focused on the midpoint of the incision on the hind paw, and time taken for paw withdrawal was measured automatically. To avoid thermal injury, the cutoff duration of exposure was set at 20 s. The withdrawal latencies for three trials performed at 5 min intervals were averaged.
Mechanical nociceptive thresholds were evaluated using an automated von Frey-type dynamic plantar esthesiometer (model 37450; Ugo Basile). Each rat was placed in a plastic cage with a wire mesh floor. The tip of a von Frey filament was applied to the middle of the plantar surface of the hind paw with increasing force until the paw was withdrawn or a cutoff force of 50 g was reached. The force required to elicit a reflex withdrawal of the hind paw was automatically recorded. The lowest force required in three trials performed at 5 min intervals was considered to be the withdrawal threshold.
Statistical analysis
Using G*power (version 3.0.10.; Heinrich Heine University, Düsseldorf, Germany), we calculated that a sample size of ten rats in each group would be needed to have at least 80% power with an α-value of 0.05 for detecting mean (±standard deviation) differences in withdrawal threshold of 20.0±10.0, 25.0±10.0, 35.0±10.0, and 35.0±10.0 g in saline and quinpirole 10, 30, and 50 nmol, respectively. These values were selected from our preliminary experiment. All data are expressed as means ± standard deviation. The between-group statistical comparisons were performed using one-way analysis of variance (ANOVA) followed by Bonferroni’s post hoc test. Statistical significance was set at P<0.05.
Results
In this postoperative pain model, a plantar incision decreased the nociceptive threshold, which was expressed as reduced hind paw withdrawal latency to infrared radiant heat and a reduced withdrawal threshold for mechanical stimulation on the day after plantar surgery (Figures 1 and 2).
There was no change in the withdrawal latency or mechanical nociceptive thresholds in the control group (anesthesia only for IT catheterization, no incision), indicating no thermal hyperalgesia or mechanical allodynia (data not shown).
IT administration of quinpirole (30 nmol per rat), but not sulpiride (30 nmol per rat), significantly increased the mean thermal withdrawal latency when compared with saline at both 5 min (3.5±1.6, 8.4±2.1, and 4.0±1.5 s in the saline, quinpirole, and sulpiride groups, respectively; P<0.0001 [ANOVA] F2,27=22.0) and 15 min (4.2±1.3, 8.6±2.5, and 3.4±1.4 s; P<0.0001 [ANOVA] F2,27=21.9; Figure 1A). The mechanical withdrawal threshold was also significantly increased by quinpirole at 5 min (22.9±6.1, 39.7±8.2, and 29.6±13.2 g in the saline, quinpirole, and sulpiride groups, respectively; P=0.0037 [ANOVA] F2,27=6.96) and at 15 min (20.6±5.1, 38.5±7.2, and 27.3±13.7 g, respectively; P=0.0017 [ANOVA] F2,27=8.12; Figure 1B). However, this antinociceptive effect was not found at 30 min or at any subsequent assessment points. The increased nociceptive thresholds were significant at quinpirole doses of 30 and 50 nmol, but not at doses of 10 nmol. The decreased postoperative nociceptive thresholds were not altered by any sulpiride dose (Figure 2). IT administration of quinpirole or sulpiride had no effect on the nociceptive threshold in the control rats with no plantar incision (data not shown).
 | Figure 1 Effects of IT administration of quinpirole and sulpiride on the response to noxious heat (A) and mechanical stimuli (B). Notes: The plantar incision markedly reduced both the heat withdrawal latency (A) and the mechanical withdrawal threshold (B), indicating successful establishment of a decreased postoperative nociceptive threshold. (a) Before plantar incision and (b) IT administration. Between-group statistical comparisons were performed using one-way analysis of variance followed by Bonferroni’s post hoc test. Data are expressed as the means ± standard deviation (n=10, *P<0.05 vs saline, #P<0.05 vs sulpiride). Abbreviation: IT, intrathecal; min, minutes, s, seconds. |
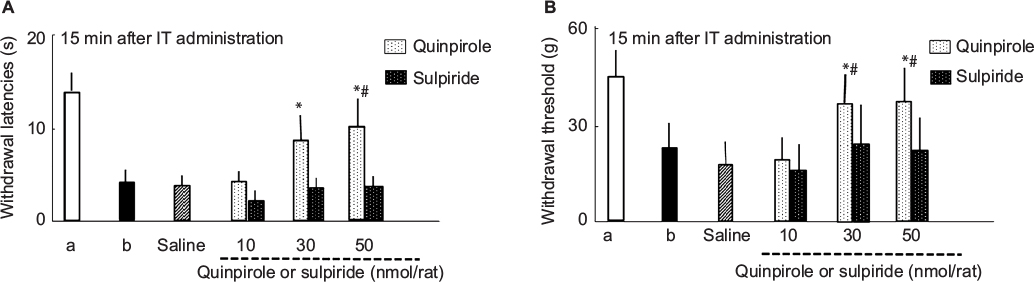 | Figure 2 Dose-related responses to noxious heat (A) and mechanical stimuli (B) at 15 min after IT administration of quinpirole and sulpiride. Notes: (a) Before plantar incision and (b) IT administration in the saline group. Between-group statistical comparisons were performed using one-way analysis of variance followed by Bonferroni’s post hoc test. Data are expressed as means ± standard deviation (n=10, *P<0.05 vs saline, #P<0.05 vs sulpiride). Abbreviation: IT, intrathecal; min, minutes; s, seconds. |
Discussion
The main findings of this study are that IT administration of a D2-like agonist inhibited the decreased nociceptive thresholds induced by plantar incision and that these thresholds were not affected by IT administration of a D2-like antagonist. These results suggest that the incision did not impair or modulate D2-like receptors in the descending dopaminergic pathway. Therefore, this mechanism is unlikely to be involved in the decreased postoperative nociceptive threshold observed after a surgical incision.
The mechanisms of the decrease in nociceptive threshold induced surgery are not well understood because this pathological pain state comprises different types of pain, including pain with a neuropathic component. After peripheral nerve injury, numerous modulators are produced1 and promote a range of changes in the sensory components of the central and peripheral nervous systems, including inhibitory pain transduction systems such as gamma aminobutyric acid (GABA) interneurons and descending pathways, leading to complex neuropathic pain. The present study investigated the involvement of D2-like receptors in the descending dopaminergic pathway in the development of a pathological pain state after a surgical incision. As mentioned above, many chemical modulators are produced after nerve injury and initiate abnormal sensory responses. One of these modulators, brain-derived neurotrophic factor (BDNF), has been suggested to be a molecular substrate for neuropathic pain.12 Following peripheral nerve injury, release of BDNF contributes to an impaired inhibition of GABAergic neurons in the spinal cord.4 Therefore, we hypothesized that a surgical incision would cause release of BDNF that would impair or modulate D2-like receptors, such as inhibitory GABAergic neurons, which is a known pain inhibitory system in the descending dopaminergic pathway. If D2-like receptors in this pathway are impaired or modulated, the effect of a D2-like agonist and D2-like antagonist (ie, pronociceptive and antinociceptive, respectively) on the decreased nociceptive threshold induced by a plantar incision should be atypical. However, this was not the case. The D2-like agonist inhibited the decreased nociceptive threshold and the D2-like antagonist had no effect, suggesting that the decrease in postoperative nociceptive threshold after surgical incision was not due to impairment or modulation of D2-like receptors in the descending dopaminergic pathway.
A recent study by Almanza et al has demonstrated that small doses of a D2-like receptor agonist have an antinociceptive effect in treatment-naive rats.6 The results of their study are not consistent with our findings in terms of the requirement for high doses of quinpirole to exert analgesic effects in the postoperative pain model. The exact reasons for this discrepancy are not clear, but Almanza et al suggested the possibility that a D2-like receptor agonist may have a nonspecific action when administered at high doses.6 Further studies are needed to clarify this matter. A nonspecific action of quinpirole cannot be ruled out because we did not use specific D2, D3, and D4 receptor antagonists in our study.
There are several limitations to this study. First, the direct effects of the D2-like agonist on the pain signal transduction pathway in the spinal cord were not investigated. Therefore, we could not rule out impairment and/or modulation of the descending dopaminergic pathway via the D2-like receptor. After plantar incision and subsequent release of numerous chemical modulators, there may be changes in the characteristics of various types of pain transduction13,14 and regulation systems.15 These changes might mask the impairment and/or modulation of D2-like receptors in the descending dopaminergic pathway and the resulting antinociceptive effects of a D2-like agonist on the decreased nociceptive threshold observed after plantar incision. Second, we did not coadminister a D2-like agonist and antagonist in this study. Useful information on the specific antinociceptive effect of quinpirole could be elucidated by coadministration of an agonist and antagonist, especially with regard to the postoperative pain state.
Conclusion
IT administration of a D2-like agonist had an antinociceptive effect on the decreased nociceptive threshold induced by a surgical incision in a mouse model of neurological pain, while a D2-like antagonist had no such effect. These results suggest that impairment and/or modulation of D2-like receptors in the descending dopaminergic pathway did not occur in response to the surgical incision. Therefore, this pathway is unlikely to be involved in development of the decreased nociceptive threshold observed after a surgical incision.
Acknowledgments
The authors thank Dr. Kido for his kind preparation of the manuscript.
Disclosure
This study was supported in part by a grant-in-aid for scientific research from the Ministry of Education, Culture, Sports, Science, and Technology of Japan to NO (No. 2493046) and EM (No. 26463056). The authors report no conflicts of interest in this work.
References
Hefti FF, Rosenthal A, Waliche PA, Wyatt S, Vergara G, Shelton DL, Davies AM. Novel class of pain drug based on antagonism of NGF. Trends Pharmacol Sci. 2006;27(2):85–91. | ||
Masaki E, Mizuta K, Ohtani N, Kido K. Early postoperative nociceptive threshold and production of brain-derived neurotrophic factor induced by plantar incision are not influenced with minocycline in a rat: role of spinal microglia. Neurosignals. 2016;24(1):15–24. | ||
Li CQ, Xu JM, Liu D, Zhang JY, Dai RP. Brain derived neurotrophic factor (BDNF) contributes to the pain hypersensitivity following surgical incision in the rats. Mol Pain. 2008;4:27. | ||
Coull JA, Beggs S, Boudreau D, et al. BDNF from microglia causes the shift in neuronal anion gradient underlying neuropathic pain. Nature. 2005;438(7070):1017–1021. | ||
Aira Z, Barrenetxea T, Buesa I, Martínez E, Azkue JJ. Spinal D1-like dopamine receptors modulate NMDA receptor-induced hyperexcitability and NR1 subunit phosphorylation at serine 889. Neurosci Lett. 2016;618:152–158. | ||
Almanza A, Simón-Arceo K, Coffeen U, Fuentes-García R, Contreras B, Pellicer F, Mercado F. A D2-like receptor family agonist produces analgesia in mechanonociception but not in thermonociception at the spinal cord level in rats. Pharmacol Biochem Behav. 2015;137:119–125. | ||
Kim JY, Tillu DV, Quinn TL, et al. Spinal dopaminergic projections control the transition to pathological pain plasticity via a D1/D5-mediated mechanism. J Neurosci. 2015;35(16):6307–6017. | ||
Yaksh TL, Rudy TA. Chronic catheterization of the spinal subarachnoid space. Physiol Behav. 1976;17(6):1031–1036. | ||
Brennan TJ, Vandermeulen EP, Gebhart GF. Characterization of a rat model of incisional pain. Pain. 1996;64(3):493–501. | ||
Tamae A, Nakatsuka T, Koga K, Kato G, Furue H, Katafuchi T, Yoshimura M. Direct inhibition of substantia gelatinosa neurones in the rat spinal cord by activation of dopamine D2-like receptors. J Physiol. 2005;568:243–253. | ||
Taniguchi W, Nakatsuka T, Miyazaki N, et al. In vivo patch-clamp analysis of dopaminergic antinociceptive actions on substantia gelatinosa neurons in the spinal cord. Pain. 2011:152(1):95–105. | ||
Trang T, Beggs S, Salter MW. Brain-derived neurotrophic factor from microglia: a molecular substrate for neuropathic pain. Neuron Glia Biol. 2011;7(1):99–108. | ||
Oliveira SM, Drewes CC, Silva CR, et al. Involvement of mast cells in a mouse model of postoperative pain. Eur J Pharmacol. 2011;672(1–3):88–95. | ||
Jang JH, Liang D, Kido K, Sun Y, Clark DJ, Brennan TJ. Increased local concentration of complement C5a contributes to incisional pain in mice. J Neuroinflammation. 2011;8:80. | ||
Yalamuri SM, Brennan TJ, Spofford CM. Neuropeptide Y is analgesic in rats after plantar incision. Eur J Pharmacol. 2013;698(1–3):206–212. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.