")
Back to Journals » Veterinary Medicine: Research and Reports » Volume 14
Cytokine Adsorption as an Adjunctive Treatment for Patients with Immune-Mediated Hemolytic Anemia Receiving Therapeutic Plasma Exchange: A Case Series of 3 Dogs
Authors Meagher J, Hendricks J, Eatroff A
Received 22 February 2023
Accepted for publication 19 May 2023
Published 1 June 2023 Volume 2023:14 Pages 103—110
DOI https://doi.org/10.2147/VMRR.S407139
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Young Lyoo
John Meagher, Jeanette Hendricks, Adam Eatroff
Advanced Critical Care Emergency and Specialty Services, Culver City, CA, USA
Correspondence: John Meagher, Advanced Critical Care Emergency and Specialty Services, 9599 Jefferson Blvd, Culver City, CA, 90232, USA, Tel + 1 310 558 6100, Fax + 1 310 558 6199, Email [email protected]
Abstract: The use of cytokine adsorption is an emerging treatment for inflammatory diseases in human medicine. There are few reports of this treatment modality in veterinary medicine and no reports of the use of a cytokine adsorbent for immune-mediated hemolytic anemia (IMHA). These case reports illustrate the use of a cytokine adsorbent as an adjunctive treatment during therapeutic plasma exchange (TPE). All dogs were unresponsive to conventional treatment or were severely affected by rapid hemolysis of red blood cells. The aim was to treat all dogs with three sequential TPE sessions; however, one dog died before completion of three sessions and one dog required additional sessions. Preliminary evidence indicates that the use of a cytokine adsorption is well tolerated and can be considered as an adjunct in the management of IMHA that is severe or refractory to traditional treatment.
Keywords: IMHA, TPE, IL-6, VetResQ, CytoSorb
Introduction
Immune-mediated hemolytic anemia (IMHA) is a potentially life-threatening disease in which red blood cells (RBCs) are destroyed by antierythrocyte antibody production.1 In addition to immunoglobulins (Ig), multiple cytokines have been implicated in the pathogenesis of IMHA. High levels of interleukin (IL)-10 have been shown to be a common feature in several different types of IMHA in humans.2 Elevated levels of IL-6 have also been associated with multiple autoimmune diseases in humans.3 Similar to humans, dogs with IMHA have an imbalance or pro- and anti-inflammatory cytokines.4–6 The cytokine profile of dogs with IMHA and sepsis are remarkably similar.4 Prognostically in dogs, IL-18 has been found to be higher in non-survivors with IMHA.6
Conventional treatment for IMHA involves suppression of the immune system to halt destruction of RBCs with glucocorticoids being the mainstay of treatment.7 Other immunosuppressive medications are often used as secondary agents.7 Despite these interventions, survival associated with IMHA ranges from 44% to 73%.8,9 A more recent multicenter study showed a survival rate of 67%10 for the first month. While this demonstrates improved survival compared to other studies, a subset of patients remains refractory to traditional medical treatment and warrants alternative treatments.
In humans, therapeutic plasma exchange (TPE) is accepted as a second-line treatment for IMHA.11 TPE is an extracorporeal technique performed in an apheresis device in which the patient’s plasma is separated from other blood components and removed, while the patient’s other blood components and a replacement solution are returned to the circulation.12 The successful use of TPE for the treatment of IMHA in dogs has been described.13–16 In veterinary medicine, this modality has been reserved for patients refractory to standard immunosuppressant medications, allowing patients with more severe disease to have similar outcomes to those less severely affected.14
In humans, a cytokine adsorbent (CytoSorb®; CytoSorbents Inc., Princeton, NJ) has been used in conjunction with other blood purification and oxygenation systems to treat a variety of diseases by bulk removal of cytokines. Cytokine adsorption has been used to improve outcomes in patients with highly inflammatory diseases.17–19
VetResQTM (CytoSorbents Inc, Princeton, NJ) is a veterinary-specific cytokine adsorber that can be used in conjunction with TPE. Like CytoSorb in human medicine, VetResQ is an in-line blood purification cartridge composed of multiple, porous, polymer beads. Given that cytokines are implicated in the pathogenesis, maintenance, and malignant sequelae of IMHA, their removal is an attractive therapeutic option. The addition of a cytokine adsorbent to an apheresis circuit has not been previously described in veterinary medicine. This case series is the first to describe the use of a cytokine adsorption with TPE in the treatment of autoimmune disease in dogs. In the cases described, the owners consented to therapeutic plasma exchange and the use of a cytokine adsorbent. This course of treatment was recommended as best practice given the severity of the disease for these patients.
Cases
Case 1
Patient 1 is a 7-year Female Spayed Golden Retriever that was presented for acute onset of lethargy and anorexia. CBC showed a regenerative anemia (hematocrit 14.0% [37.3–61.7]; reticulocytes 130 k/mcl [10.0–110.0]) and a mild leukocytosis (white blood cell = 18.1k/mcl [5.05–16.76]). Initial chemistry showed mild elevation in blood urea nitrogen (blood urea nitrogen = 28mg/dl [7–27]) and hyperbilirubinemia (3.6mg/dl [0–0.9]) (Table 1) Initial testing in house did not reveal obvious agglutination, however CBC submitted to an outside laboratory revealed mild spherocytosis and persistent autoagglutination despite saline dilution. The degree of dilution performed by the outside laboratory was not specified. Urinalysis revealed pigmenturia. Based on these findings, a presumptive diagnosis of IMHA was made.
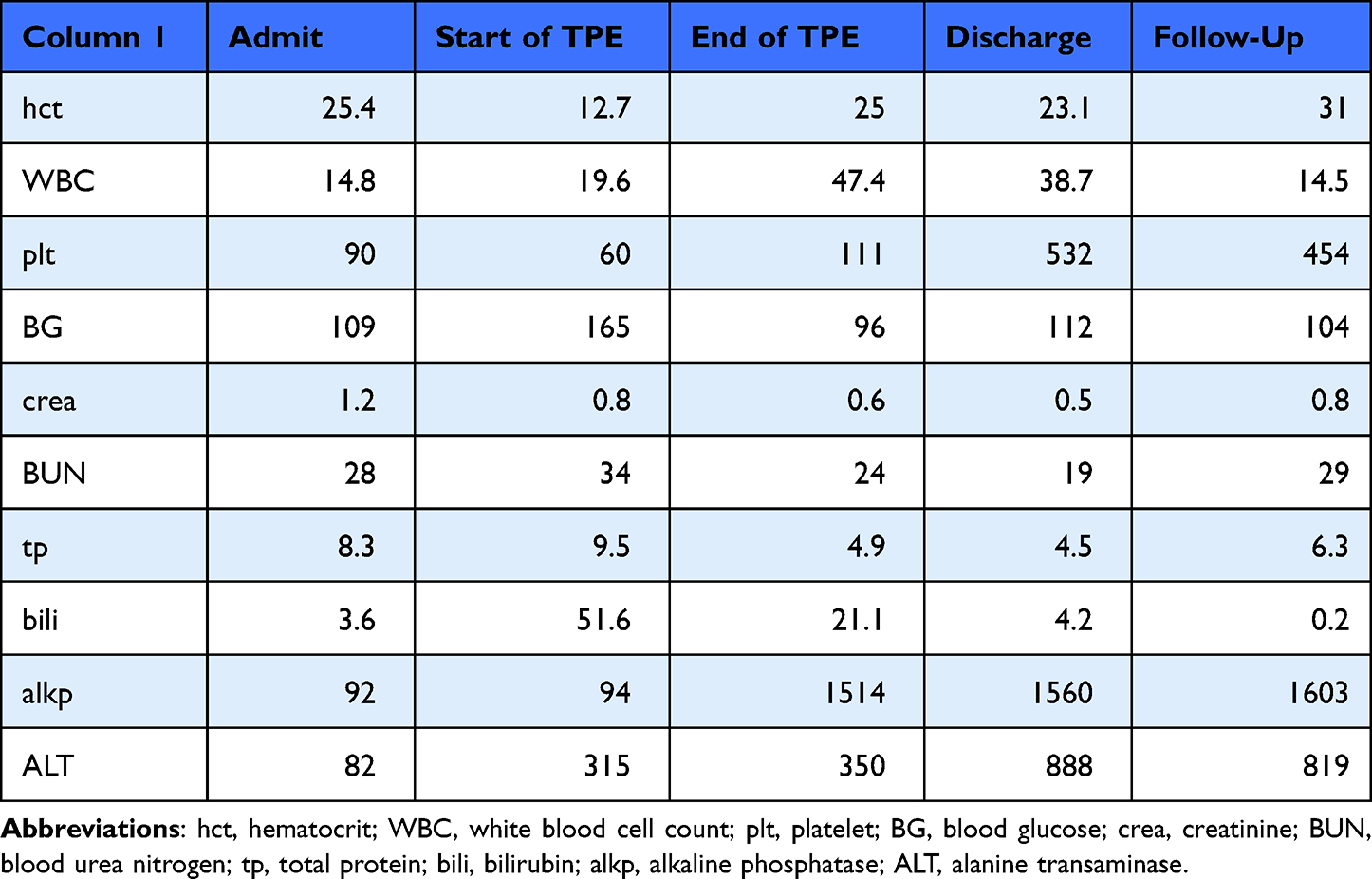 |
Table 1 Pertinent Bloodwork Parameters of Patient 1 at Different Times During Hospitalization and Follow-Up |
Initial treatment consisted of dexamethasone sodium phosphate 0.2mg/kg IV q24h, mycophenolate 8.3mg/kg PO q12h, clopidogrel 2.8mg/kg PO q24h, rivaroxaban 0.74mg/kg PO q24h, and doxycycline 9.3 mg/kg IV q24h. Over the course of 48 hours, this patient required three transfusions of packed red blood cells (pRBCs) which totaled 26.7mL/kg. In addition to requiring multiple transfusions, the patient was also becoming progressively icteric and was exhibiting a deteriorating mental status. Based on these developments, the patient was deemed a candidate for TPE.
Before her first TPE treatment, she was obtunded, markedly icteric, and had pelvic limb extensor rigidity without cranial nerve deficits. Petechiation was noted on the ventral abdomen. Recheck bloodwork showed marked hyperbilirubinemia (total bilirubin = 51.6mg/dL) and an elevated C-reactive protein (CRP) (IDEXX Catalyst CRP Test, Westbrook, ME) at 7.8mg/dl [0–1.0]. A recheck CBC revealed a platelet estimate of approximately 50k cells/mcL, which could explain the petechiation.
A dialysis catheter was placed using a modified Seldinger technique. The dialysis catheter was used to perform TPE treatments with a total of three planned treatments. A TPE 2000 filter (Baxter, Deerfield, Illinois) was used plus VetResQ 150mL cartridge in a pre-filter configuration. The patient was given a bolus of unfractionated heparin 2500 units (83 units/kg). The priming fluid used was NaCl 0.9% with unfractionated heparin 2000 U/L. Accounting for the patient’s low hematocrit, the patient’s plasma volume was calculated to be 1400mL and 1.5x the patient’s plasma volume was calculated as 2100mL. During the session, 2200mL were exchanged. Runtime was 256 minutes with an approximate flow rate of blood of 170mL/min. For the replacement solution, the patient was given 1700mL of 3% Vetstarch (Zoetis, Parsippany-Troy Hills, NJ) diluted with Normosol-R (ICU Medical, San Clemente, CA) + KCl 5mEq/L. The patient was also given fresh frozen plasma 500mL as part of the replacement fluid. During the session anticoagulation was achieved with a heparin continuous rate infusion run at 2500 units/hour for the first hour and then 2000 units/hour for the rest of the session. During the patient’s second TPE treatment, she had a grand mal seizure that responded to a single dose of diazepam and then she was started on levetiracetam.
This patient was hospitalized for a total of 14 days. During that time, the petechiation resolved, the severe hyperbilirubinemia markedly improved, elevation in CRP resolved, and her mentation markedly improved. Comprehensive testing for vector-borne diseases was negative. She was sent home on prednisone 0.77mg/kg PO q12h, doxycycline 10mg/kg PO q24h, and clopidogrel 2.8mg/kg PO q24h.
Following hospitalization, she was eventually weaned off all immunosuppressive drugs over a period of 6 months. She regained the ability to walk with only mild ataxia noted. At one-year follow-up, the patient continued to do well off all immunosuppressive medications.
Case 2
Patient 2 is an 8-year, female spayed Pit Bull that was presented to a local emergency and specialty hospital for a three-day history of lethargy and anorexia. Her bloodwork at presentation showed that her hematocrit was 20% and her bilirubin was 1.1mg/dl (Table 2). Saline agglutination test (4 drops saline:1 drop blood) revealed macroagglutination. Early treatment consisted of dexamethasone sodium phosphate 0.2mg/kg IV q24h, mycophenolate 8.3mg/kg PO q12h, clopidogrel 1.1mg/kg PO q24h, and doxycycline 6.7mg/kg PO q12h. An initial 8.3mL/kg pRBC transfusion was administered to this patient at presentation. The patient required two additional pRBC transfusions and continued to rapidly hemolyze her transfusions. On day 3 of hospitalization, her PCV was 14%, prompting referral for TPE.
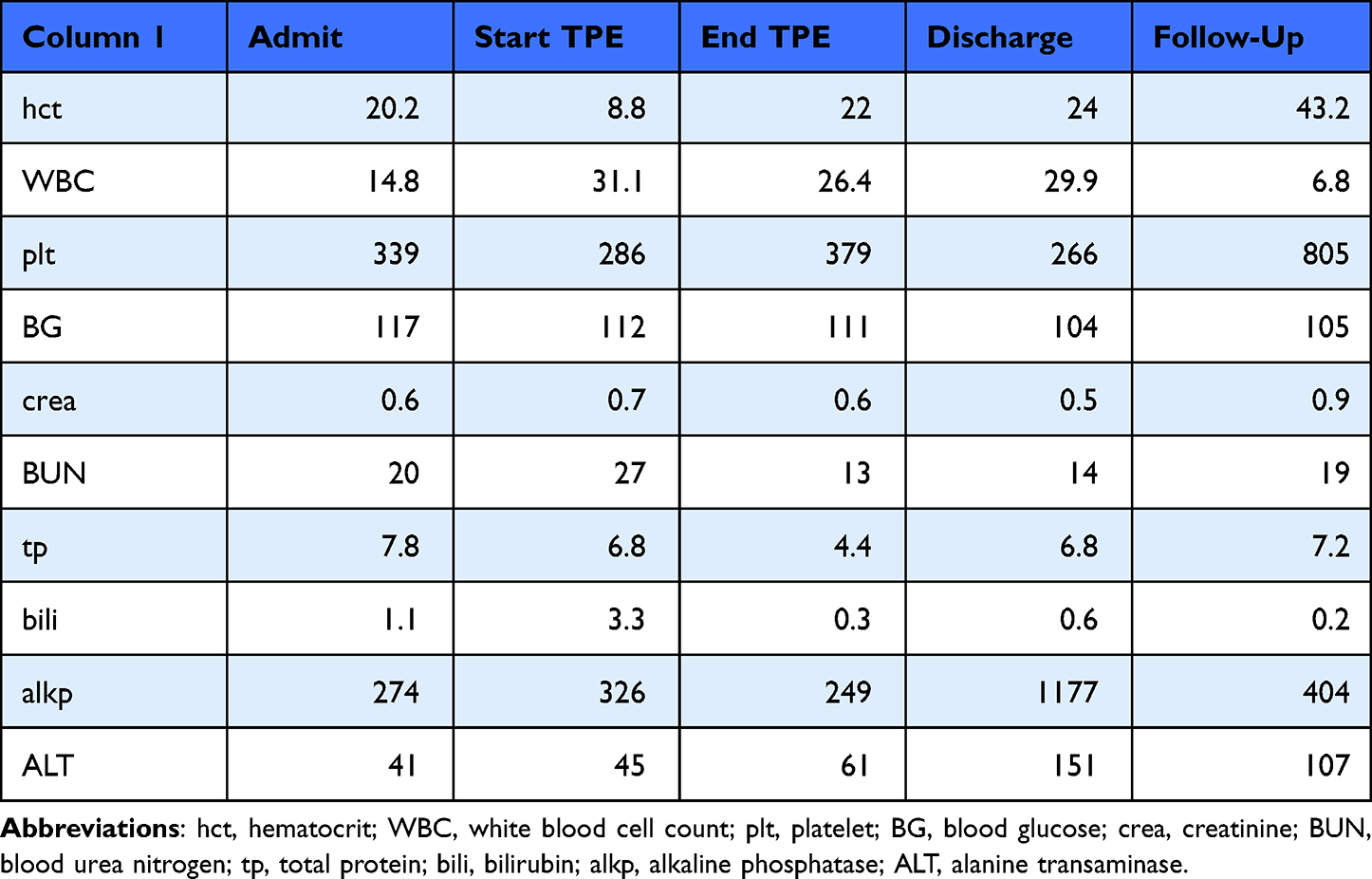 |
Table 2 Pertinent Bloodwork Parameters of Patient 2 at Different Times During Hospitalization and Follow-Up |
On presentation to our hospital, the patient had a severe, strongly regenerative anemia (hematocrit = 8.8%, reticulocytes = 264k/mcl). Her bilirubin was elevated at 3.3mg/dL, and she had a markedly elevated CRP at 26.1mg/dL.
The patient received TPE on day 3, 4, and 6 of hospitalization at any hospital. The filters used during treatment were TPE 2000 and VetResQ 150mL. Dialysis catheter placement, plasma volume calculations, anticoagulant targets, and the replacement solution were similar to Patient 1. She required a pRBC transfusion during her first TPE session. After the first TPE session, the patient was started on Xarelto 0.67mg/kg PO q24h.
Despite undergoing three TPE treatments, the patient started to hemolyze again. She required another two pRBC transfusions 8.3mL/kg each on days 10 and 11 of hospitalization. Given her ongoing hemolysis, the decision was made to perform two additional TPE treatments. Even though her infectious testing was negative, given her lack of sustained response and her breed, she was started on aggressive treatment for Babesiosis. Her doxycycline was discontinued, and she was started on atovaquone 15mg/kg PO q8h and azithromycin 10mg/kg PO q24h. Her glucocorticoids were decreased to a physiologic dose (prednisolone 0.17mg/kg PO q24h). The patient was hospitalized for a total of 19 days. She was sent home on previously mentioned atovaquone, azithromycin, and prednisolone.
The patient did well long term. Within 40 days of presentation to the initial hospital, she was off all medications. Subsequent examinations over the next year did not show recurrence of anemia.
Case 3
Patient 3, a 10-year female spayed terrier mix, was initially presented to a local emergency and specialty hospital for lethargy and pale gums. Initial bloodwork revealed anemia (hematocrit = 24.4%) and mild elevations of alanine transaminase (229 U/L [10–125]), alkaline phosphatase (207 [23–212U/L]), and bilirubin (1.3 mg/dL). Saline agglutination utilizing a dilution of 4 drops saline to 1 drop blood test was macroscopically positive. The cells were not washed prior to the saline agglutination test. Early treatment consisted of dexamethasone sodium phosphate, mycophenolate, clopidogrel, rivaroxaban, and doxycycline.
On Day 2 of hospitalization, her anemia progressed (PCV = 15%) warranting a 13.7mL/kg pRBC transfusion. After the transfusion, her packed cell volume increased to 20%. The patient became progressively anemic on day 3 of hospitalization and required another pRBC transfusion. The patient also became mildly azotemic (creatinine = 1.7 mg/dl [0.5–1.5]) and markedly hyperbilirubinemic (17.7 mg/dL). Considering the degree of hyperbilirubinemia and requirement for repeated transfusions, the patient was referred for TPE.
On presentation to our hospital, a chemistry panel revealed progressive hyperbilirubinemia (bilirubin = 96.5mg/dL) and azotemia (creatinine = 2.4mg/dL). CBC showed a marked inflammatory leukogram (white blood cells = 42.4k/mcl), thrombocytopenia (80k/mcl), and a regenerative anemia (hematocrit = 19.9%, reticulocytes = 166k/mcl). Clotting times were moderately elevated prior to the administration of any heparin.
Placement of the dialysis catheter and the TPE + VetResQ session was similar to those described above.
That evening, the patient became stuporous and bruising was noted on all four limbs and at the site of insertion of the dialysis catheter. On Day 4, the patient experienced cardiopulmonary arrest. The patient achieved return of spontaneous circulation with cardiopulmonary resuscitation. Due to the patient’s poor prognosis, the owners elected euthanasia.
Discussion
This case series describes the first veterinary use of a cytokine adsorbent in a TPE circuit for patients treated for IMHA. The cytokine adsorber did not lead to any apparent adverse reactions directly attributable to VetResQ. While complications were noted in the patients in this series, these are consistent with complications previously encountered with TPE and with severe IMHA.
Based on serial neurologic exams and her underlying disease process, Patient 1 is presumed to have had a cerebrovascular accident. The eventual improvement in neurologic status also supports the presumptive diagnosis of an ischemic stroke. However, given the patient’s presence of petechiation and thrombocytopenia, a brain bleed due can also not be ruled out. Another possibility for this patient’s neurologic deficits would be kernicterus.
The hypercoagulable state may be lessened by the usage of TPE and VetResQ, possibly preventing a second, potentially life-ending thromboembolic event. Removal of cytokines and free heme can reduce the hypercoagulable state.20 Since TPE and VetResQ may decrease the exuberant hemolytic process, TPE and VetResQ may help the patient recover neurologic function secondary to kernicterus. Cytokine adsorbers can also remove bilirubin.21
Patient 2 required multiple treatments with TPE. The use of TPE with VetResQ is postulated to have kept the patient alive long enough for the correct treatment to be implemented. In this case, aggressive treatment for Babesiosis resulted in remission of IMHA. Although the patient tested negative for Babesiosis, treatment for this disease process resulted in remission of the hemolytic process and therefore likely had a false negative test.
Patient 3 had the highest bilirubin of the three patients, and elevated bilirubin has been associated with mortality in a multicenter study.10 Given the high risk of thrombosis in IMHA patients,22 this patient most likely died due to a life-threatening thromboembolic event such as a cerebrovascular infarct or massive pulmonary thromboembolism. Although no fibrinogen or D-dimer levels were available, the degree of thrombocytopenia and elevated prothrombin time and partial thromboplastin time are suspicious for disseminated intravascular coagulation.23 Other potential causes of death in patients with IMHA would be complications from systemic inflammatory reaction syndrome. Sequelae of SIRS include hypotension, cardiac arrhythmias, and end-organ failure.24,25 Given that a life-threatening inflammatory disease likely played a role in this patient’s death, earlier use of TPE may have been beneficial.
Initial treatment of IMHA in dogs and cats involves administration of immunosuppressive medications. No concurrent consensus exists for when to initiate TPE in canine patients. In humans, the American Society for Apheresis recommends the use of TPE for patients who are unresponsive to pRBC transfusions and/or steroid therapy26 and similar criteria have been applied to veterinary patient. In the future, more definitive criteria on when to initiate TPE may be useful. Criteria may be based on total transfusion requirement, length of time between transfusion needs, length of time in which a patient is unresponsive to standard therapy, or serum bilirubin concentrations.
There are currently no recommended guidelines for the number of TPE treatments needed to effectively treat IMHA in dogs. Serial treatment may decrease the overall immunoglobulin burden as IgG and IgM rapidly redistribute to the intravascular space after removal of the plasma portion.27 An exchange of 1–1.5 patient plasma volume removes 60–70% of any substances contained within the intravascular space.28 Bulk removal of immunoglobulins is TPE’s proposed mechanism of action, but there may also be beneficial immunomodulatory effects.29
When TPE is deemed appropriate for a patient with autoimmune disease, VetResQ can easily be used as an adjunctive treatment. VetResQ is a hemoadsorption device that is designed to remove small substances, such as cytokines, from patients. The device can be used in series with a dialysis filter in patients already receiving hemodialysis treatment and can easily be integrated in any extracorporeal circuit used in the hospitals such as renal replacement therapy, TPE and a hemoperfusion circuit.
In these patients, CRP is used as a cage-side biomarker for inflammation. CRP has been shown to be increased in patients with IMHA.30 IL-6 induces formation of CRP by hepatocytes.31 CRP itself then induces release of IL-1, IL-6, and TNF-α.32 Both survivors in this series had a demonstrable reduction in CRP levels after treatment with TPE and VetResQ (Figure 1). This reduction could be from bulk removal of CRP or from removal of cytokines which stimulate CRP production. Cytosorb, and likely VetResQ adsorb IL-6.33 Since IL-6 has a direct stimulatory effect on CRP production, removal of IL-6 should decrease CRP levels.
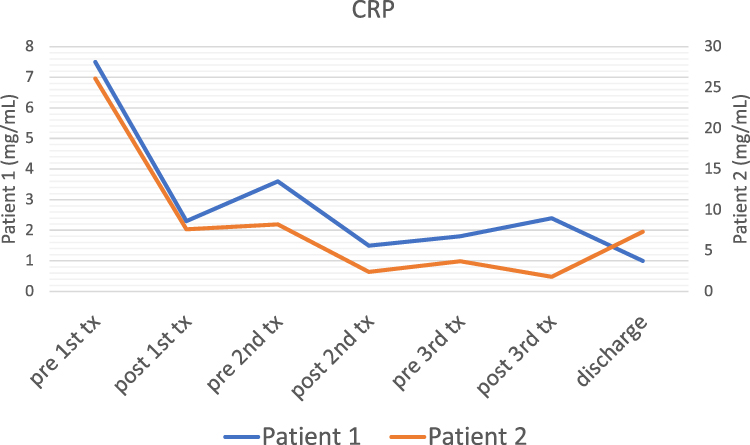 |
Figure 1 Changes in patients’ CRP before and after each treatment (tx.). |
Other than removing cytokines, VetResQ and TPE are also capable of removing high levels of bilirubin21,34 and toxic,free hemoglobin,35 which are produced from RBC destruction and tissue breakdown of RBC hemoglobin. While solely receiving conventional treatment, both patient 1 and 2 showed an increase in bilirubin. Once TPE was instituted, both patients that survived showed an overall reduction in bilirubin (Figure 2) which may be due to the combination of TPE, use of cytokine adsorption, and remission of the hemolytic crisis.
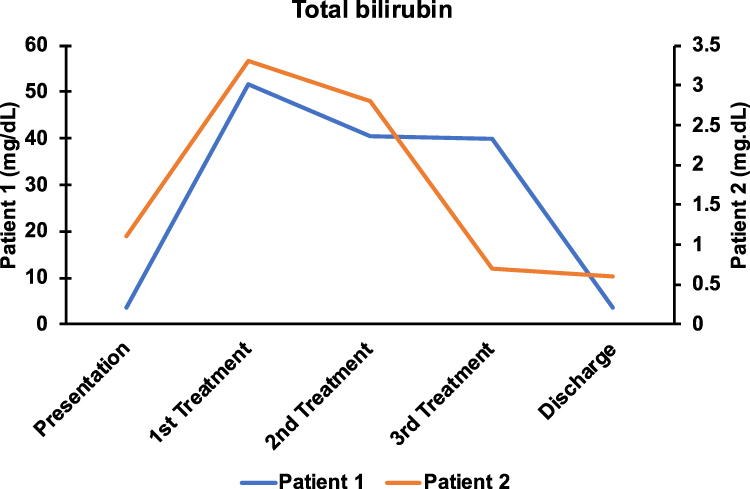 |
Figure 2 Change in the patients’ total bilirubin over time. |
As TPE becomes more widespread in the treatment of refractory autoimmune diseases, the concurrent use of cytokine adsorbents may also become widespread. TPE has been previously described in the treatment of IMHA, myasthenia gravis, and immune mediated thrombocytopenia.16,36,37 In these patients whose disease process depends on the production of autoantibodies and cytokines, the dual removal of both, theoretically, could provide better outcomes and quicker remission times.
Case series are limited in nature. Inability to measure cytokines before and after treatments was also a limitation of this case series. Although there are theoretical benefits to the use of a cytokine adsorbent in autoimmune diseases, large trials are needed to see if these theoretical benefits result in a true benefit in patients. TPE is a costly treatment modality, and future studies are likely to be based on small sample sizes. As cytokine adsorbents are an emerging treatment modality in veterinary and human medicine, a translation approach based on future human studies may prove to be useful in our patients.
Disclosure
Due to clinical interest in the product, VetResQ cartridges were supplied to Advanced Critical Care Emergency and Specialty Services free of charge. The authors report no other conflicts of interest in this work.
References
1. Frank MM; NIH conference. Pathophysiology of immune hemolytic anemia. Ann Intern Med. 1977;87(2):210–222. doi:10.7326/0003-4819-87-2-210
2. Toriani-Terenzi C, Fagiolo E. IL-10 and the cytokine network in the pathogenesis of human autoimmune hemolytic anemia. Ann N Y Acad Sci. 2005;1051:29–44. doi:10.1196/annals.1361.044
3. Kaur S, Bansal Y, Kumar R, et al. A panoramic review of IL-6: structure, pathophysiological roles and inhibitors. Bioorg Med Chem. 2020;28(5):115327. doi:10.1016/j.bmc.2020.115327
4. Johnson V, Burgess B, Morley P, et al. Comparison of cytokine responses between dogs with sepsis and dogs with immune-mediated hemolytic anemia. Vet Immunol Immunopathol. 2016;1(180):15–20. doi:10.1016/j.vetimm.2016.08.010
5. Swann JW, Woods K, Wu Y, et al. Characterisation of the immunophenotype of dogs with primary immune-mediated haemolytic anaemia. PLoS One. 2016;11(12):e0168296. doi:10.1371/journal.pone.0168296
6. Kjelgaard-Hansen M, Goggs R, Wiinberg B, et al. Use of serum concentrations of interleukin-18 and monocyte chemoattractant protein-1 as prognostic indicators in primary immune-mediated hemolytic anemia in dogs. J Vet Intern Med. 2011;25(1):76–82. doi:10.1111/j.1939-1676.2010.0642.x
7. Swann JW, Garden OA, Fellman CL, et al. ACVIM consensus statement on the treatment of immune-mediated hemolytic anemia in dogs. J Vet Intern Med. 2019;33(3):1141–1172. doi:10.1111/jvim.15463
8. Piek CJ, Junius G, Dekker A, et al. Idiopathic immune-mediated hemolytic anemia: treatment outcome and prognostic factors in 149 dogs. J Vet Intern Med. 2008;22(2):366–373. doi:10.1111/j.1939-1676.2008.0060.x
9. Weinkle TK, Center SA, Randolph JF, et al. Evaluation of prognostic factors, survival rates, and treatment protocols for immune-mediated hemolytic anemia in dogs: 151 cases (1993–2002). J Am Vet Med Assoc. 2005;226(11):1869–1880. doi:10.2460/javma.2005.226.1869
10. Walker S, Warman S, Di Bella A, et al. Predicting outcome in dogs with primary immune-mediated hemolytic anemia: results of a multicenter case registry. J Vet Intern Med. 2015;29(6):1603–1610. doi:10.1111/jvim.13642
11. Zanatta E, Cozzi M, Marson P, et al. The role of plasma exchange in the management of autoimmune disorders. Br J Haematol. 2019;186(2):207–219. doi:10.1111/bjh.15903
12. Fernández-Zarzoso M, Gómez-Seguí I, de la Rubia J. Therapeutic plasma exchange: review of current indications. Transfus Apher Sci. 2019;58(3):247–253. doi:10.1016/j.transci.2019.04.007
13. Scagnelli AM, Walton SA, Liu CC, et al. Effects of therapeutic plasma exchange on serum immunoglobulin concentrations in a dog with refractory immune-mediated hemolytic anemia. J Am Vet Med Assoc. 2018;252(9):1108–1112. doi:10.2460/javma.252.9.1108
14. Francey T, Etter M, Schweighauser A. Evaluation of membrane-based therapeutic plasma exchange as adjunctive treatment for immune-mediated hematologic disorders in dogs. J Vet Intern Med. 2021;35(2):925–935. doi:10.1111/jvim.16049
15. Culler CA, Vigani A, Ripoll AZ, et al. Centrifugal therapeutic plasma exchange in dogs with immune-mediated hemolytic anemia (2016–2018): 7 cases. J Vet Emerg Crit Care. 2022;32(5):645–652.
16. Crump KL, Seshadri R. Use of therapeutic plasmapheresis in a case of canine immune‐mediated hemolytic anemia. J Vet Emerg Crit Care. 2009;19:
17. Akil A, Ziegeler S, Reichelt J, et al. Combined use of CytoSorb and ECMO in patients with severe pneumogenic sepsis. Thorac Cardiovasc Surg. 2021;69(3):246–251. doi:10.1055/s-0040-1708479
18. Alharthy A, Faqihi F, Memish ZA, et al. Continuous renal replacement therapy with the addition of CytoSorb cartridge in critically ill patients with COVID-19 plus acute kidney injury: a case-series. Artif Organs. 2021;45(5):E101–E112. doi:10.1111/aor.13864
19. Ruiz-Rodríguez JC, Molnar Z, Deliargyris EN, et al. The use of CytoSorb therapy in critically Ill COVID-19 patients: review of the rationale and current clinical experiences. Crit Care Res Pract. 2021;17(2021):7769516.
20. Nyakundi BB, Tóth A, Balogh E, et al. Oxidized hemoglobin forms contribute to NLRP3 inflammasome-driven IL-1β production upon intravascular hemolysis. Biochim Biophys. Acta Mol Basis Dis. 2019;1865(2):464–475. doi:10.1016/j.bbadis.2018.10.030
21. Gemelli C, Cuoghi A, Magnani S, et al. Removal of bilirubin with a new adsorbent system: in vitro kinetics. Blood Purif. 2019;47(1–3):10–15. doi:10.1159/000492378
22. deLaforcade A, Bacek L, Blais MC, et al. Consensus on the rational use of antithrombotics in veterinary critical care (CURATIVE): domain 1-defining populations at risk. J Vet Emerg Crit Care. 2019;29(1):37–48. doi:10.1111/vec.12797
23. Goggs R, Mastrocco A, Brooks MB. Retrospective evaluation of 4 methods for outcome prediction in overt disseminated intravascular coagulation in dogs (2009–2014): 804 cases. J Vet Emerg Crit Care. 2018;28(6):541–550.
24. Silverstein DC, Hopper K. Chapter 6: systemic inflammatory response syndrome. In: Small Animal Critical Care Medicine.
25. Silverstein DC, Hopper K. Chapter 7: multiple organ dysfunction syndrome. In: Small Animal Critical Care Medicine.
26. Padmanabhan A, Connelly-Smith L, Aqui N, et al. Guidelines on the use of therapeutic apheresis in clinical practice - evidence-based approach from the writing committee of the American Society for apheresis: the eighth special issue. J Clin Apher. 2019;34(3):171–354. doi:10.1002/jca.21705
27. Williams ME, Balogun RA. Principles of separation: indications and therapeutic targets for plasma exchange. Clin J Am Soc Nephrol. 2014;9(1):181–190. doi:10.2215/CJN.04680513
28. Pham HP, Staley EM, Schwartz J. Therapeutic plasma exchange - A brief review of indications, urgency, schedule, and technical aspects. Transfus Apher Sci. 2019;58(3):237–246. doi:10.1016/j.transci.2019.04.006
29. Winters JL. Plasma exchange: concepts, mechanisms, and an overview of the American Society for Apheresis guidelines. Hematology Am Soc Hematol Educ Program. 2012;2012:7–12. doi:10.1182/asheducation.V2012.1.7.3797920
30. Griebsch C, Arndt G, Raila J, et al. C-reactive protein concentration in dogs with primary immune-mediated hemolytic anemia. Vet Clin Pathol. 2009;38(4):421–425. doi:10.1111/j.1939-165X.2009.00146.x
31. Ohsugi Y. Recent advances in immunopathophysiology of interleukin-6: an innovative therapeutic drug, tocilizumab (recombinant humanized anti-human interleukin-6 receptor antibody), unveils the mysterious etiology of immune-mediated inflammatory diseases. Biol Pharm Bull. 2007;30(11):2001–2006. doi:10.1248/bpb.30.2001
32. Black S, Kushner I, Samols D. C-reactive protein. J Biol Chem. 2004;279(47):48487–48490. doi:10.1074/jbc.R400025200
33. Pieri M, Fominskiy E, Nardelli P, et al. CytoSorb purification in critically ill SARS-CoV-2 patients. Int J Artif Organs. 2022;45(2):216–220. doi:10.1177/03913988211052572
34. Heffner GG, Cavanagh A, Nolan B. Successful management of acute bilirubin encephalopathy in a dog with immune-mediated hemolytic anemia using therapeutic plasma exchange. J Vet Emerg Crit Care. 2019;29(5):549–557. doi:10.1111/vec.12876
35. Gleason TG, Argenziano M, Bavaria JE, et al. Hemoadsorption to reduce plasma-free hemoglobin during cardiac surgery: results of REFRESH I pilot study. Semin Thorac Cardiovasc Surg. 2019;31(4):783–793. doi:10.1053/j.semtcvs.2019.05.006
36. Palm CA, Cowgill LD, Dickinson PJ, et al. Therapeutic apheresis: a novel treatment for myasthenia gravis in dogs. J Vet Intern Med. 2011;25:
37. Kopecny L, Palm CA, Naylor S, Kirby J, Cowgill LD. Application of therapeutic plasma exchange in dogs with immune-mediated thrombocytopenia. J Vet Intern Med. 2020;34(4):1576–1581. doi:10.1111/jvim.15836
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.