")
Back to Journals » Infection and Drug Resistance » Volume 13
Current Status of Laboratory Diagnosis for COVID-19: A Narrative Review
Authors Russo A , Minichini C, Starace M, Astorri R, Calò F, Coppola N
Received 22 May 2020
Accepted for publication 5 July 2020
Published 3 August 2020 Volume 2020:13 Pages 2657—2665
DOI https://doi.org/10.2147/IDR.S264020
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Antonio Russo, Carmine Minichini, Mario Starace, Roberta Astorri, Federica Calò, Nicola Coppola On behalf of the Vanvitelli COVID-19 group
Department of Mental Health and Public Medicine, Infectious Diseases Unit, University of Campania Luigi Vanvitelli, Naples, Italy
Correspondence: Nicola Coppola
Department of Mental Health and Public Medicine, Infectious Diseases Unit, University of Campania Luigi Vanvitelli, Via: L. Armanni 5, Naples 80131, Italy
Tel +39 0815666719
Fax +39 0815666013
Email [email protected]
Abstract: The outbreak of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and the related disease (COVID-19) has spread rapidly to pandemic proportions, increasing the demands on healthcare systems for the containment and management of COVID-19. One of the critical issues to be addressed is the improvement in laboratory diagnosis and screening of large portions of the population to stop the virus spreading. Currently, the laboratory diagnosis of SARS-CoV-2 infection and the related disease is based on the research of viral RNA with rt-PCR methods in upper and lower respiratory airways. Serological tests to detect SARS-CoV-2 antibodies could help physicians and healthcare workers to support COVID-19 diagnosis and follow-up and perform population screening. Our review, using MEDLINE and EMBASE, summarizes the current knowledge of direct and serological tests performed to research RNA, antigens, or antibodies for SARS-CoV-2, evaluating the advantages and drawbacks for specific tests.
Keywords: COVID-19, SARS-CoV-2, laboratory diagnosis, serological test, PCR
Introduction
In late December 2019, an outbreak of a respiratory disease of uncertain etiology occurred in Wuhan, the capital of Hubei region, China.1,2 On January 10, 2020, the first genome of the new virus was deposited by Zhang et al,3 on GenBank (MN908947) and other platforms. The Coronavirus Study Group of the International Committee on Taxonomy of Viruses (ICTV) renamed the virus, previously 2019-nCoV, as severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2).4 Despite increasingly rigorous restrictions, China and most of the primarily involved countries failed to contain COVID-19's global spread, as of May 10, 2020, the WHO Situation Report-111 declared 3,917,366 confirmed cases worldwide (1,707,946 in Europe, 218,268 in Italy), with 274,61 deaths (155,552 in Europe, 30,395 in Italy).5
COVID-19 infection has a broad spectrum of severity ranging from an asymptomatic form to a severe acute respiratory syndrome that requires mechanical ventilation; typical symptoms of infected patients by SARS-CoV-2 are fever, fatigue, and dry cough.6
To date there is uncertainty about the mode of transmission of SARS-CoV-2, but it is likely similar to SARS, which is spread by contact, droplets, aerosol, and contaminated environments;6,7 studies have highlighted the higher risk of transmission from patients with respiratory symptoms,8,39 but it is also possible from asymptomatic patients.9 Nowadays, to identify the asymptomatic carriers of SARS-CoV-2 and patients with COVID-19 is the diagnostic gold standard and seems to be important point in the strategies to fight the spread of the epidemic; on the other hand to identify the subjects with previous contact with the virus seems to also be important in the strategies of epidemiological knowledge.
Virology
SARS-CoV-2 (Order Nidovirales, Family Coronaviridae, Sub-family Orthocoronavirinae, Genus Betacoronavirus) is an enveloped positive-sense single-stranded RNA (+ssRNA) virus.4 The Orthocoronavirinae sub-family comprises four distinct clades: alpha- (α-CoV), beta- (β-CoV), gamma- (γ-CoV), and delta-coronavirus (δ-CoV),10 among which only the first two can also infect mammals and encompass human pathogens. In contrast with the endemic relatively mild α-CoVs, β-CoVs include highly virulent zoonotic epidemic viruses, already known for the massive outbreaks of SARS (2002) and Middle East respiratory syndrome (2012): SARS-CoV and MERS-CoV, respectively.11,12 According to genomic and phylogenetic analyses, SARS-CoV-2 is included in the Sarbecovirus subgenus (B-lineage of β-CoV genus) comprising SARS-CoV and several bat viruses.13,14 Surprisingly, SARS-CoV-2 genome is closer to the RaTG13 bat CoV (̴ 96.2% identity)15 than to SARS-CoV (̴ 79%) and MERS-CoV (̴ 50%).14
The virion presents an almost spherical pleomorphic structure (60–140 nm in diameter) characterized by a peculiar external “crown” of S protein spikes (8–12 nm in length), under transmission electron microscopy.1 The SARS-CoV-2 genome (̴ 30 Kb) encodes 16 non-structural proteins (nsp 1–16),16 including the RNA-dependent RNA-polymerase (RdRp, nsp12)17 and the helicase (nsp13), and four structural proteins: the spike (S), the membrane (M), and the nucleocapsid (N) glycoproteins, and the envelope (E) protein.13,17–19 The viral envelope comprises the S, E, and M proteins, enclosing the N protein and the RNA genome.19,21 The S glycoprotein, a class I fusion protein,22,23 is pivotal for the endocytosis-mediated viral entry22,24 and consists of two subunits (S1, S2);25 the S1 harbors the receptor-binding domain (RBD),14,26 which directly binds human angiotensin-converting enzyme 2 (hACE2).26,28 Crucially, while the M glycoprotein is the most abundant SARS-CoV-2 protein, the S glycoprotein is the main inducer of neutralizing antibodies29,30 and the most diverging protein, with a high mutation rate,17,32,34 possibly modifying glycosylation sites and consequently altering hACE2 binding, CTL epitopes,32,35 and accessibility to proteases and neutralizing antibodies.22
Aim of the Narrative Review
The aim of this narrative review was to evaluate the tools for the etiological diagnosis of SARS-CoV-2 infection and their use in different clinical settings. The article is addressed particularly to physicians providing care to COVID-19 patients and to Healthcare authorities designing screening programs for the general population.
Methods
We conducted a comprehensive computerized literature research to identify studies analyzing diagnostic tests for COVID-19 using MEDLINE and EMBASE from January 2020 up to April 2020, involving both medical subject heading (MeSH) terminology and relevant keywords for search strings to locate articles that analyzed the diagnostic test for COVID-19. The following items were used to search for the studies: “diagnosis”, “laboratory test”, “COVID-19,” and “SARS-CoV-2”. We performed this research to summarize the latest and future perspectives on the laboratory diagnosis for SARS-CoV-2 infection and the related disease.
Etiological Diagnosis
As for all viral infections, the diagnosis of SARS-CoV-2 infection is based on the direct identification of viral RNA or antigens or the indirect identification of specific antibody responses. A direct diagnosis is the gold standard for an active infection, while the detection of specific anti-SARS-CoV-2 antibodies is the cornerstone for the identification of previous contact with the virus, both for diagnostic and epidemiological aims.36
Direct Diagnosis of SARS-CoV-2 Infection
The direct diagnosis of SARS-CoV-2 infection is based on the detection of SARS-CoV-2 RNA on nasopharyngeal swabs or on lower respiratory tract specimens.36
In clinical practice, the most widely used is the former, while tests on lower respiratory tract specimens are performed in some defined cases.36 In patients with a good outcome, viral RNA is detected for 20 days or longer after the onset of symptoms, and a rebound of the viral load, after undetectable with PCR, is possible.31
In addition, rt-PCR positivity for SARS-CoV-2 RNA peaked in upper respiratory tract specimens at 7–10 days after the onset of symptoms and then steadily declined; conversely, rt-PCR RNA detection in lower respiratory tract specimens remained stable for 3 weeks after symptom onset/clinical presentation.31
The characteristics for optimal testing for a direct diagnosis of SARS-CoV-2 infection include a short turnaround time, high throughput, minimum batching, low infrastructural requirements, elevated accuracy, low cost to allow access to testing, also considering testing priorities to diagnose vulnerable populations, and to reduce viral spread, especially in nosocomial, family, and closed community settings.40,47 Nucleic acid testing (real-time rt-qPCR) on respiratory tract specimens have several of these characteristics, thus representing the current gold standard in the diagnosis of SARS-CoV-2 infection.41 However, various factors, either procedural or virus-related, may impair its reliability,42 for example a single-time point,38 and an unmet need for procedural standardization43 (from sample collection, including swab types, to processing) remains complicated by shortages of personnel and materials.38,44 For these reasons, new rapid tests (either based on antigens or antibodies),38,45 point-of-care (POC) assays,38,46 and digital technologies47 would support infection detection and containment, also in low- and middle-income settings, but require careful evaluation.
Tables 1 and 2 show the characteristics and the advantages and disadvantages of different direct tests for SARS-CoV-2, respectively.
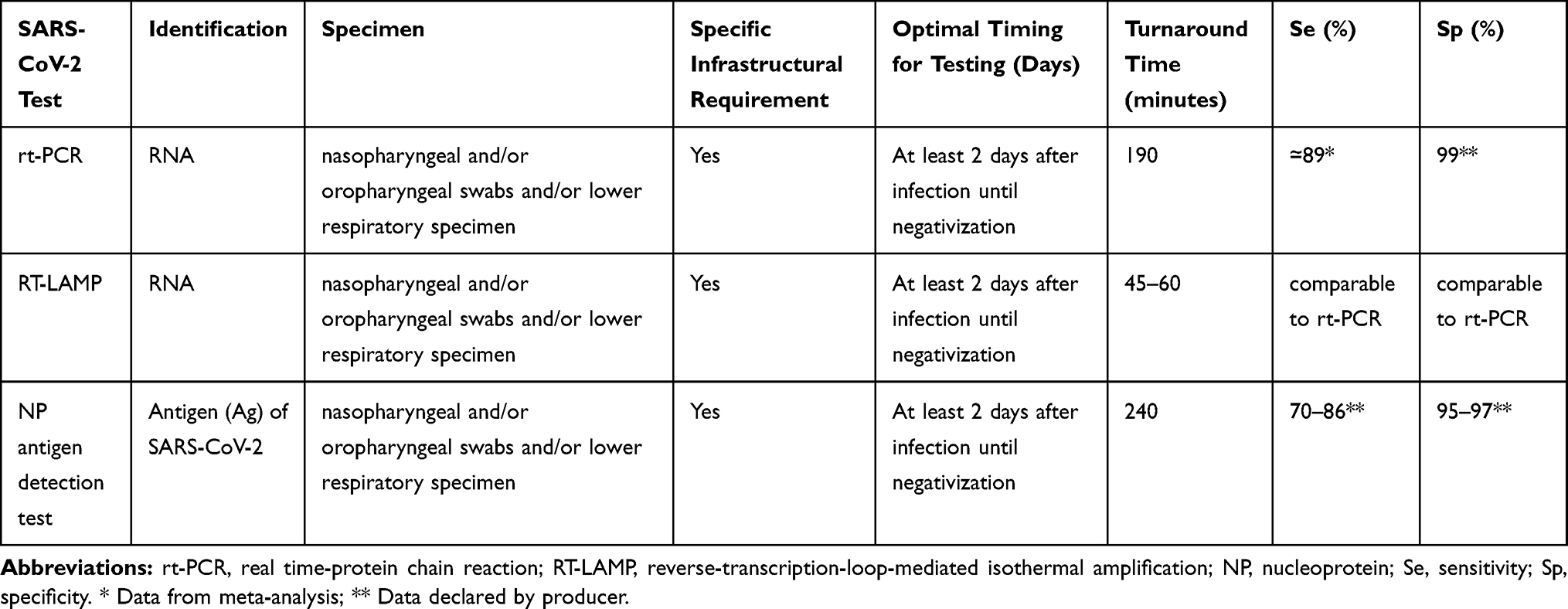 |
Table 1 Characteristics of Different Direct Tests for SARS-CoV-2 |
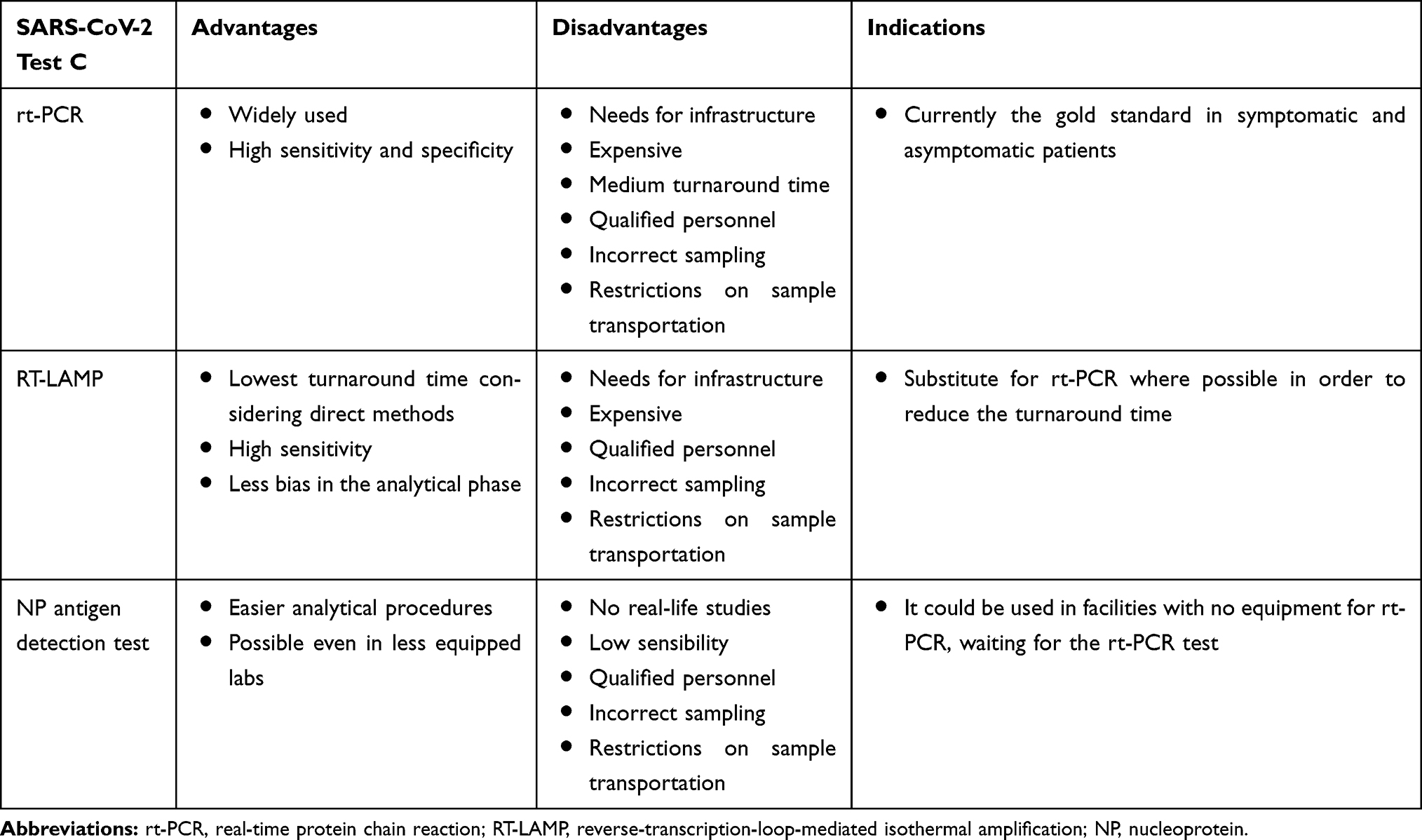 |
Table 2 Advantages, Disadvantages, and Possible Indications of Different Direct Tests for SARS-CoV-2 |
Real-Time PCR Tests
Real-time rt-PCR technology is the most used SARS-CoV-2 RNA detection.36 In several real-time PCR tests, the primers were designed against the envelope (E) and RNA-dependent RNA polymerase (RdRp) regions:48 the E-region was used for first-line screening, while the RdRp region was employed for confirmatory testing. Other researchers developed one-step rt-PCR assays to detect open reading frame (ORF) 1b and N regions of SARS-CoV-2:49 the N region assay was used for screening, while ORF1b testing served as a confirmatory test. However, since ORF1b and N regions are highly conserved in Sarbecoviruses, the specific primers could also bind other coronaviruses and closely related viruses. As regards the rt-PCR performances, a recent meta-analysis performed by Kim et al50 considering 19 studies identified a pooled sensitivity of 89% (95% CI=81–94%; I2=90%), while the positive predictive value (PPV) ranged from 47.3–98.3% and the negative predictive value (NPV) ranged from 93.4–99.9%. In fact, false negative results may not only derive from poor sensitivity, but they can also be due to low amounts of sample, inadequate conservation, or the presence of amplification inhibitors or of mutations in the target regions of the specific primer used.51,52 For example, Li et al53 observed that, of the 610 patients enrolled, 384 (63.0%) had a negative nasopharyngeal specimen at baseline: of these 384, 48 patients were positive at the second swab test and 12 at the third. Comparably, Xiao et al,51, considering 70 patients with COVID-19, in 15 (21.4%) observed a positive rt-PCR result after two negative specimens. Thus, a negative result does not exclude SARS-CoV-2 infection and should not be used alone for clinical management.
As for the identification of an optimal specimen type, the nasopharyngeal swab remains the gold standard for the detection of SARS-CoV-2 RNA. Azzi et al54 highlighted the possibility of performing rt-PCR also on saliva samples; all 25 patients with a positive rt-PCR on nasopharyngeal swabs were positive also on saliva samples, more easily collected. Of relevance, the collection of sequential upper respiratory specimens or a single lower respiratory specimen may be necessary to detect the virus in symptomatic subjects with initial negative rt-PCR testing. In fact, Guo et al55 Pshowed that rt-PCR performed on throat washing samples was more accurate for COVID-19 diagnosis than nasopharyngeal swab samples (P<0.031).
Reverse-Transcription-Loop-Mediated Isothermal Amplification (RT-LAMP)
In recent years, the loop-mediated isothermal amplification (LAMP) method, which includes an exponential amplification of specific nucleic acid sequences at a constant temperature, has been widely utilized for the rapid detection of virus-specific genes, with a specificity and sensitivity comparable to that reported for rt-PCR assays. The LAMP technique eludes some PCR limitations, such as the need for high-purity samples, trained personnel, and expensive laboratory instruments.56
A combination of LAMP with reverse transcription (rt-LAMP) allows the direct detection of RNA, including SARS-CoV-2 RNA. In a small study, Wui et al57 validated the RT-LAMP method employing 16 clinical samples, eight positive and eight negative for SARS-CoV-2 by rt-PCR: the testing results were consistent with the conventional rt-PCR.
Antigen-Based Tests
Direct methods for COVID-19 diagnosis also encompass a double antibody sandwich enzyme-linked immunoassay identifying the SARS-CoV-2 nucleoprotein (NP) by a microplate pre-coated with specific antibodies against SARS-CoV-2 NP and the use of a horseradish peroxidase (HRP)-labeled secondary antibody against the same protein. This direct method is simple, rapid, and does not require trained personnel and expensive laboratory instruments. However, in a meta-analysis by Castro et al58 the sensitivity of this test ranged from 70–86%, while the specificity ranged from 95–97%, and thus a single negative test result cannot rule out SARS-CoV-2 infection.59
Indirect Diagnosis of SARS-CoV-2 Infection
The indirect diagnosis of SARS-CoV-2 infection is based on the detection of specific IgG and/or IgM antibodies. Importantly, the WHO underlines a strong need for serological IgM and IgG testing and a rapid design of easy and inexpensive point-of-care (POC) tests.38,46,60
The dynamics of antibody responses were studied by several authors. To et al31 evaluated the viral load and antibody kinetics on deep-throat saliva specimens (posterior nasopharyngeal samples), suggesting that serological testing may be complementary with rt-PCR testing; they observed that IgG and IgM responses against the internal viral NP and the S protein receptor-binding domain (RBD) occurred mostly within 10 days after symptom onset and positively correlated with neutralizing antibody titres; antibodies against RBD showed an earlier rise, when compared to those against NP, and a rise of IgG prior to IgM was noticed. In addition, they showed a more prolonged rt-PCR positivity in patients who formed early antibodies and in those with a poor prognosis.61,62 Analysing 173 patients with SARS-CoV-2 infection, Zhao et al63 observed seroconversion in less than 40% of the patients within 1-week from the onset of symptoms and in all patients (94.3% for IgM and 79.8% for IgG) within day 15 after clinical presentation.
In April 2020, Long et al64 evaluated the antibody dynamics in a Chinese cohort of 285 COVID-19 patients, using a magnetic chemiluminescence immunoassay (MCLIA). All patients had virus-specific IgG approximately at day 17–19 after the onset of symptoms, while 94.1% had virus-specific IgM at day 20–22. Moreover, higher IgG titers were observed in patients with a severe course of illness compared to those without (P=0.001).64 Of the 285 patients enrolled, a serological course was observed in 26 who were initially seronegative with three different dynamics: synchronous IgG/IgM seroconversion (9 patients), IgM seroconversion earlier than that of IgG (7 patients), and IgM seroconversion later than that of IgG (10 patients).64
Several serological immunoassays have been developed for the detection of SARS-CoV-2 viral proteins and antibodies in serum or plasma samples. The most widely used commercial tests are based on rapid lateral flow immunoassay (LFIA), automated chemiluminescence immunoassay (CLIA), and enzyme-linked immune assay (ELISA).65
Tables 3 and 4 show the characteristics and the advantages and disadvantages of different indirect tests for SARS-CoV-2, respectively.
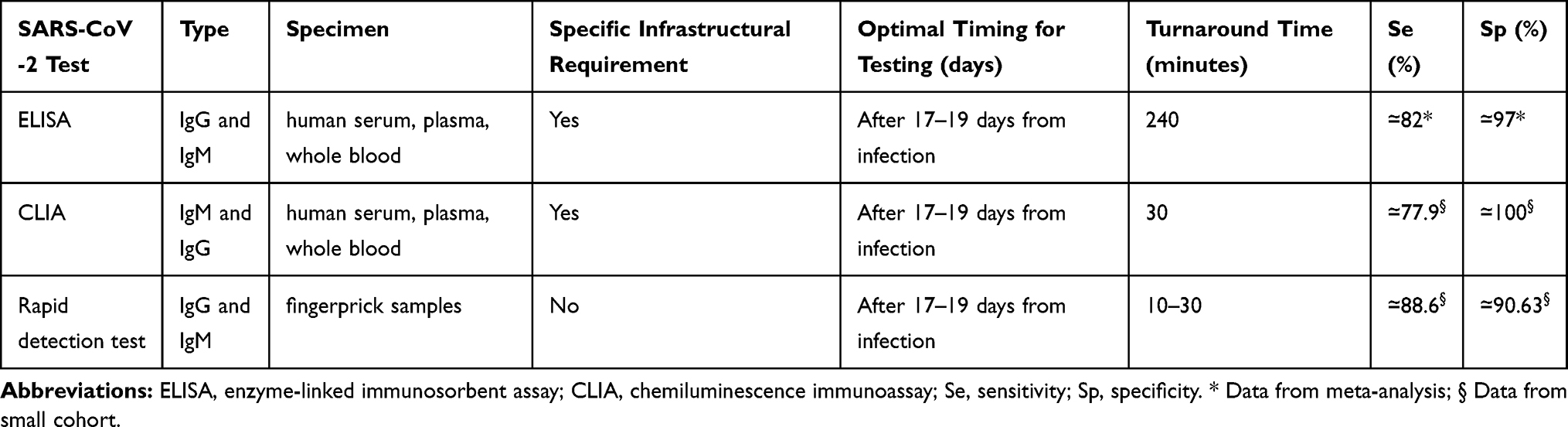 |
Table 3 Characteristics of Different Indirect Test for SARS-CoV-2 |
 |
Table 4 Advantages, Disadvantages, and Possible Indications of Different Indirect Tests for SARS-CoV-2 |
Enzyme-Linked Immune Assay (ELISA)
Enzyme-linked immune assay (ELISA) is a method to detect anti-SARS-CoV-2 IgG and IgM responses by identifying antibodies against the NP and spike proteins, but the absence of defined standards represents a limitation. In a recent meta-analysis whose aim was to analyze the accuracy of available tests to detect SARS-CoV-2 infection in Brazil, the pooled diagnostic measures of ELISA tests were: for IgM antibodies, sensitivity of 82% [95% CI=76–87], specificity of 97% [95% CI=96–98]; for IgG antibodies, sensitivity of 97% [95% CI=90–99], specificity of 98% [95% CI=97–99].58
Chemiluminescent Immunoassay (CLIA)
CLIA offers significant advantages over traditional assay detection methods, especially in the quantification of antibodies. Light-producing chemical reactions (a substrate reacts with the Avidin-Horseradish Peroxidase resulting in light development) allowed estimating the titers of IgG and IgM by the amount of the emitted luminous signal. Padoan et al66 analyzed the kinetics of anti-SARS-CoV-2 IgG and IgM antibodies by CLIA, showing a rapid increase in IgM and IgG after 6–7 days from symptom onset. In particular from day 1 to day 5 after symptom onset, no patient had detectable IgM and IgG; of the six patients observed between day 6 and 7, three (50%) were positive for IgM and four (66.6%) for IgG; of the nine patients observed between day 12 and 13, seven (77.8%) were positive for IgM and all (100%) for IgG.
Rapid Serological Tests
Many rapid IgM/IgG tests have been developed by several companies, mainly based on immunoassay technology67 providing results in 10–15 minutes. These devices contain colloidal gold-labeled SARS-CoV-2 recombinant protein and murine anti-human IgG antibodies immobilized in the G area, murine anti-human IgM antibodies immobilized in the M area, and the corresponding antibody in quality control area C.
However, the clinical accuracy of rapid tests needs to be stringently evaluated before they are authorized for mass screening of COVID-19. The manufacturers declare a relative specificity of 100%, a relative sensitivity of 81% in subjects observed between day 4 and 10 after the onset of symptoms, and a relative sensitivity of 97% between day 11 and 24. Cassaniti et al68 compared the results of rapid serological tests with those of nasopharyngeal swab in 30 healthy subjects, 30 rt-PCR-SARS-CoV-2-positive subjects, and 50 subjects admitted to the emergency department with fever and respiratory syndrome: all 30 healthy subjects were negative by rapid IgM/IgG testing; of the 30 positive subjects, 19 (63.3%) showed clear positivity for both IgM and IgG antibodies, five (16.7%) weak positivity for both, one (3.3%) an isolated IgM positivity, and five (16.7%) negativity for both IgG and IgM antibodies. Interestingly, among the 50 patients admitted to the emergency department, 38 tested COVID-19-positive by rt-PCR; of these 38, only seven patients showed a positive rapid test with a sensitivity of 18.4% and a specificity of 91.7%, NPV 26.2%, PPV 87.5%. Based on current data, the WHO does not recommend the use of antibody-detecting rapid diagnostic tests for patient care, but encourages the continuation of the present work to establish their usefulness in disease surveillance and epidemiological research.36
Conclusions
The COVID-19 pandemic poses a major global challenge, with a massive yet possibly underestimated burden and several unknowns. With a subtle clinical presentation and asymptomatic carriage, and in the absence of specific treatment and vaccines, it is clear that an early and accurate diagnosis is crucial for the control of the disease.69,71 Although rt-PCR represents a cornerstone for SARS-CoV-2 laboratory diagnosis, several limitations have been observed. Therefore, a combined approach harmonizing laboratory methods (ie, rt-PCR and serology) with imaging features and clinical findings is essential to guide patient management and infection control.
Acknowledgments
The Vanvitelli COVID-19 group included the following: Nicola Coppola, Caterina Sagnelli, Stefania De Pascalis, Maria Stanzione, Gianfranca Stornaiuolo, Angela Cascone, Salvatore Martini, Margherita Macera, Caterina Monari, Federica Calò, Andrea Bianco, Antonio Russo, Valeria Gentile, Clarissa Camaioni, Giulia De Angelis, Giulia Marino, Roberta Astorri, Ilario De Sio, Marco Niosi, Serena Borrelli, Vincenzo Carfora, Benito Celia, Maria Ceparano, Salvatore Cirillo, Maria De Luca, Marco Di Mauro, Grazia Mazzeo, Marco Migliaccio, Filiberto Fausto Mottola, Giorgio Paoli, Riccardo Ricciolino, Giorgio Spiniello, and Nicoletta Verde.
Author Contributions
NC and AR were involved in the review concept and design and critical revision for important intellectual content. MS, CM, RA, FC, and AR performed the literature search and drafting of the manuscript. RA, CM, and MS were involved in the critical revision of the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no funding and no conflicts of interest for this work.
References
1. Zhu N, Zhang D, Wang W, et al. A Novel Coronavirus from patients with Pneumonia in China, 2019. N Engl J Med. 2020;382(8):
2. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China [published correction appears in Lancet. 2020 Jan 30;:]. Lancet. 2020;395(10223):
3. Loeffelholz MJ, Tang YW. Laboratory diagnosis of emerging human coronavirus infections - the state of the art. Emerg Microbes Infect. 2020;9(1):
4. WHO situation report-111. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200510covid-19-sitrep-111.pdf?sfvrsn=1896976f_2.
5. World Health Organization Press Conference. The World Health Organization (WHO) has officially named the disease caused by the Novel Coronavirus as COVID-19. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
6. Guo G, Ye L, Pan K, et al. New insights of emerging SARS-CoV-2: epidemiology, etiology, clinical features, clinical treatment, and prevention. Front Cell Dev Biol. 2020;8:410. doi:10.3389/fcell.2020.00410
7. Yu IT, Li Y, Wong TW, et al. Evidence of airborne transmission of the severe acute respiratory syndrome virus. N Engl J Med. 2004;350(17):1731–1739. doi:10.1056/NEJMoa032867
8. Yang R, Gui X, Xiong Y. Patients with respiratory symptoms are at greater risk of COVID-19 transmission. Respir Med. 2020;165:105935. doi:10.1016/j.rmed.2020.105935
9. Han Y, Yang H. The transmission and diagnosis of 2019 novel coronavirus infection disease (COVID-19): A Chinese perspective. J Med Virol. 2020;92(6):639–644. doi:10.1002/jmv.25749
10. Li F. Structure, function, and evolution of coronavirus spike proteins. Annu Rev Virol. 2016;3(1):
11. de Wit E, van Doremalen N, Falzarano D, Munster VJ. SARS and MERS: recent insights into emerging coronaviruses. Nat Rev Microbiol. 2016;14(8):
12. Cui J, Li F, Shi ZL. Origin and evolution of pathogenic coronaviruses. Nat Rev Microbiol. 2019;17(3):
13. Zhou P, Yang XL, Wang XG, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579(7798):
14. Lu R, Zhao X, Li J, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395(10224):
15. Paraskevis D, Kostaki EG, Magiorkinis G, Panayiotakopoulos G, Sourvinos G, Tsiodras S. Full-genome evolutionary analysis of the novel corona virus (2019-nCoV) rejects the hypothesis of emergence as a result of a recent recombination event. Infect Genet Evol. 2020;79:104212. doi:10.1016/j.meegid.2020.104212
16. Kang S, Peng W, Zhu Y, et al. Recent progress in understanding 2019 novel coronavirus (SARS-CoV-2) associated with human respiratory disease: detection, mechanisms and treatment [published online ahead of print, 2020 Mar 29]. Int J Antimicrob Agents. 2020;55:105950. doi:10.1016/j.ijantimicag.2020.105950
17. Gao Y, Yan L, Huang Y, et al. Structure of the RNA-dependent RNA polymerase from COVID-19 virus [published online ahead of print, 2020 Apr 10]. Science. 2020:eabb7498. 10.1126/science.abb7498.
18. Wu A, Peng Y, Huang B, et al. Genome composition and divergence of the Novel Coronavirus (2019-nCoV) originating in China. Cell Host Microbe. 2020;27(3):
19. Yang P, Wang X. COVID-19: a new challenge for human beings. Cell Mol Immunol. 2020;17(5):
20. Khailany RA, Safdar M, Ozaslan M. Genomic characterization of a novel SARS-CoV-2 [published online ahead of print, 2020 Apr 16]. Gene Rep. 2020;19:100682. doi:10.1016/j.genrep.2020.100682
21. Mousavizadeh L, Ghasemi S. Genotype and phenotype of COVID-19: their roles in pathogenesis [published online ahead of print, 2020 Mar 31]. J Microbiol Immunol Infect. 2020. doi:10.1016/j.jmii.2020.03.022
22. Kirchdoerfer RN, Cottrell CA, Wang N, et al. Pre-fusion structure of a human coronavirus spike protein. Nature. 2016;531(7592):
23. Ou X, Liu Y, Lei X, et al. Characterization of spike glycoprotein of SARS-CoV-2 on virus entry and its immune cross-reactivity with SARS-CoV. Nat Commun. 2020;11(1):1620. doi:10.1038/s41467-020-15562-9
24. Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, function, and antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell. 2020;181(2):
25. Yuan Y, Cao D, Zhang Y, et al. Cryo-EM structures of MERS-CoV and SARS-CoV spike glycoproteins reveal the dynamic receptor binding domains. Nat Commun. 2017;8:15092. doi:10.1038/ncomms15092
26. Yan R, Zhang Y, Li Y, Xia L, Guo Y, Zhou Q. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science. 2020;367(6485):
27. Wrapp D, Wang N, Corbett KS, et al. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science. 2020;367(6483):
28. Wang Q, Zhang Y, Wu L, et al. Structural and functional basis of SARS-CoV-2 entry by using human ACE2 [published online ahead of print, 2020 Apr 7]. Cell. 2020;S00928674(20):30338X. doi:10.1016/j.cell.2020.03.045
29. de Haan CA, Kuo L, Masters PS, Vennema H, Rottier PJ. Coronavirus particle assembly: primary structure requirements of the membrane protein. J Virol. 1998;72(8):
30. Che XY, Qiu LW, Liao ZY, et al. Antigenic cross-reactivity between severe acute respiratory syndrome-associated coronavirus and human coronaviruses 229E and OC43. J Infect Dis. 2005;191(12):
31. To KK, Tsang OT, Leung WS, et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. Lancet Infect Dis. 2020;20(5):
32. Kumar S, Maurya VK, Prasad AK, Bhatt MLB, Saxena SK. Structural, glycosylation and antigenic variation between 2019 novel coronavirus (2019-nCoV) and SARS coronavirus (SARS-CoV). Virusdisease. 2020;31(1):
33. Petherick A. Developing antibody tests for SARS-CoV-2. Lancet. 2020;395(10230):
34. Xu X, Chen P, Wang J, et al. Evolution of the novel coronavirus from the ongoing Wuhan outbreak and modeling of its spike protein for risk of human transmission. Sci China Life Sci. 2020;63(3):
35. Lan J, Ge J, Yu J, et al. Structure of the SARS-CoV-2 spike receptor-binding domain bound to the ACE2 receptor [published online ahead of print, 2020 Mar 30]. Nature. 2020. doi:10.1038/s41586-020-2180-5
36. Laboratory testing for coronavirus disease (COVID-19) in suspected human cases. WHO; [Cited march 19, 2020]. Available from: https://www.who.int/publications-detail/laboratory-testing-for-2019-novel-coronavirus-in-suspected-human-cases-20200117.
37. Evaluating and testing persons for Coronavirus Disease 2019 (COVID-19). Available from: www.cdc.gov/coronavirus/2019-nCoV/hcp/clinical-criteria.html.
38. Cheng MP, Papenburg J, Desjardins M, et al. Diagnostic testing for severe acute respiratory syndrome-related Coronavirus-2: a narrative review [published online ahead of print, 2020 Apr 13]. Ann Intern Med. 2020:M201301. 10.7326/M20-1301.
39. Chan JF, Yuan S, Kok KH, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. 2020;395(10223):
40. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China [published online ahead of print, 2020 Feb 7]. JAMA. 2020;323(11):
41. WHO Coronavirus disease (COVID-19) technical guidance: laboratory testing for 2019-nCoV in humans. Available from: https://www.who.int/emergencies/diseases/novelcoronavirus-2019/technical-guidance/laboratory-guidance. Accessed April 17, 2020.
42. Lippi G, Simundic AM, Plebani M. Potential preanalytical and analytical vulnerabilities in the laboratory diagnosis of coronavirus disease 2019 (COVID-19) [published online ahead of print, 2020 Mar 16]. Clin Chem Lab Med. 2020. 10.1515/cclm-2020-0285
43. Liu Y, Yan LM, Wan L, et al. Viral dynamics in mild and severe cases of COVID-19 [published online ahead of print, 2020 Mar 19]. Lancet Infect Dis. 2020;S14733099(20):230232. doi:10.1016/S1473-3099(20)30232-2
44. Vermeiren C, Marchand-Senécal X, Sheldrake E, et al. Comparison of Copan Eswab and FLOQswab for COVID-19 PCR diagnosis: working around a supply shortage [published online ahead of print, 2020 Apr 15]. J Clin Microbiol. 2020:
45. European Centre for Disease Prevention and Control. An overview of the rapid test situation for COVID-19 diagnosis in the EU/EEA. Stockholm: ECDC; [Cited April 1, 2020]. Available from: https://www.ecdc.europa.eu/en/novelcoronavirus/laboratory-support.
46. Yang T, Wang YC, Shen CF, Cheng CM. Point-of-Care RNA-based diagnostic device for COVID-19. Diagnostics. 2020;10(3:165. doi:10.3390/diagnostics10030165.
47. Mahmood S, Hasan K, Colder Carras M, Labrique A. Global preparedness against COVID-19: we must leverage the power of digital health. JMIR Public Health Surveill. 2020;6(2:e18980. doi:10.2196/18980.
48. Corman VM, Landt O, Kaiser M, et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020;25(3):2000045. doi:10.2807/1560-7917.ES.2020.25.3.2000045
49. Chu DKW, Pan Y, Cheng SMS, et al. Molecular diagnosis of a Novel Coronavirus (2019-nCoV) causing an outbreak of Pneumonia. Clin Chem. 2020;66(4):
50. Kim H, Hong H, Yoon SH. Diagnostic Performance of CT and reverse transcriptase-polymerase chain reaction for Coronavirus Disease 2019: a meta-analysis [published online ahead of print, 2020 Apr 17]. Radiology. 2020;201343. doi:10.1148/radiol.2020201343
51. Xiao AT, Tong YX, Zhang S. False-negative of RT-PCR and prolonged nucleic acid conversion in COVID-19: rather than recurrence. J Med Virol. 2020. doi:10.1002/jmv.25855
52. Wang X, Yao H, Xu X, et al. Limits of detection of six approved RT-PCR Kits for the Novel SARS-coronavirus-2 (SARS-CoV-2) [published online ahead of print, 2020 Apr 13]. Clin Chem. 2020:hvaa099. doi:10.1093/clinchem/hvaa099.
53. Li Y, Yao L, Li J, et al. Stability issues of RT-PCR testing of SARS-CoV-2 for hospitalized patients clinically diagnosed with COVID-19 [published online ahead of print, 2020 Mar 26]. J Med Virol. 2020. doi:10.1002/jmv.25786
54. Azzi L, Carcano G, Gianfagna F, et al. Saliva is a reliable tool to detect SARS-CoV-2 [published online ahead of print, 2020 Apr 14]. J Infect. 2020;S01634453(20):30213–30219. doi:10.1016/j.jinf.2020.04.005
55. Guo WL, Jiang Q, Ye F, et al. Effect of throat washings on detection of 2019 novel coronavirus [published online ahead of print, 2020 Apr 9]. Clin Infect Dis. 2020:ciaa416. doi:10.1093/cid/ciaa416.
56. Baek YH, Um J, Antigua KJC, et al. Development of a reverse transcription-loop-mediated isothermal amplification as a rapid early-detection method for novel SARS-CoV-2 [published online ahead of print, 2020 Apr 20]. Emerg Microbes Infect. 2020:
57. Huang WE, Lim B, Hsu CC, et al. RT-LAMP for rapid diagnosis of coronavirus SARS-CoV-2 [published online ahead of print, 2020 Apr 25]. Microb Biotechnol. 2020. doi:10.1111/1751-7915.13586
58. Castro R, Luz PM, Wakimoto MD, Veloso VG, Grinsztejn B, Perazzo H. COVID-19: a meta-analysis of diagnostic test accuracy of commercial assays registered in Brazil [published online ahead of print, 2020 Apr 18]. Braz J Infect Dis. 2020;S14138670(20):530029. doi:10.1016/j.bjid.2020.04.003
59. SARS-COV-2 DIAGNOSTIC PIPELINE. Available from: https://www.finddx.org/covid-19/pipeline/?section=show-all#diag_tab.
60. Report of the WHO-china joint mission on Coronavirus Disease 2019 (COVID-19). Geneva, Switzerland:WHO;2020. Available from: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf.
61. Zhang L, Zhang F, Yu W, et al. Antibody responses against SARS coronavirus are correlated with disease outcome of infected individuals. J Med Virol. 2006;78(1):
62. Liu L, Wei Q, Lin Q, et al. Anti-spike IgG causes severe acute lung injury by skewing macrophage responses during acute SARS-CoV infection. JCI Insight. 2019;4(4):e123158. doi:10.1172/jci.insight.123158
63. Zhao J, Yuan Q, Wang H, et al. Antibody responses to SARS-CoV-2 in patients of novel coronavirus disease 2019 [published online ahead of print, 2020 Mar 28]. Clin Infect Dis. 2020:ciaa344. doi:10.1093/cid/ciaa344.
64. Long QX, Liu BZ, Deng HJ, et al. Antibody responses to SARS-CoV-2 in patients with COVID-19 [published online ahead of print, 2020 Apr 29]. Nat Med. 2020. doi:10.1038/s41591-020-0897-1
65. Vashist SK. In vitro diagnostic assays for COVID-19: recent advances and emerging trends. Diagnostics. 2020;10(4:E202. doi:10.3390/diagnostics10040202.
66. Padoan A, Cosma C, Sciacovelli L, Faggian D, Plebani M. Analytical performances of a chemiluminescence immunoassay for SARS-CoV-2 IgM/IgG and antibody kinetics [published online ahead of print, 2020 Apr 16]. Clin Chem Lab Med. 2020. doi:10.1515/cclm-2020-0443
67. Li Z, Yi Y, Luo X, et al. Development and clinical application of a rapid IgM-IgG combined antibody test for SARS-CoV-2 infection diagnosis [published online ahead of print, 2020 Feb 27]. J Med Virol. 2020. doi:10.1002/jmv.25727
68. Cassaniti I, Novazzi F, Giardina F, et al. Performance of VivaDiag COVID-19 IgM/IgG rapid test is inadequate for diagnosis of COVID-19 in acute patients referring to emergency room department [published online ahead of print, 2020 Mar 30]. J Med Virol. 2020. doi:10.1002/jmv.25800
69. Sardu C, D’Onofrio N, Balestrieri ML, et al. Outcomes in patients with hyperglycemia affected by COVID-19: can we do more on glycemic control? Diabetes Care. 2020;43(7):1408–1415. doi:10.2337/dc20-0723
70. Marfella R, Paolisso P, Sardu C, et al. Negative impact of hyperglycaemia on tocilizumab therapy in Covid-19 patients. Diab Metab. 2020;S12623636(20):30082–30083. doi:10.1016/j.diabet.2020.05.005
71. Sagnelli C, Gentile V, Tirri R, et al. Chronic conventional disease-modifying anti-rheumatic drugs masking severe SARS-CoV-2 manifestations in an elderly rheumatic patient. J Infect. 2020;S01634453(20):30322–30324. doi:10.1016/j.jinf.2020.05.043
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.