")
Back to Journals » Patient Preference and Adherence » Volume 17
Current Status and Influencing Factors of Readiness for Discharge of Elderly Patients with Chronic Obstructive Pulmonary Disease
Authors Wu DL, Luo CL, Du X, Li PP, Jiang M, Liu T, Sun Y
Received 1 March 2023
Accepted for publication 3 May 2023
Published 25 May 2023 Volume 2023:17 Pages 1323—1333
DOI https://doi.org/10.2147/PPA.S410725
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Dao-Lin Wu,1,2,* Chun-Li Luo,3,* Xu Du,1 Pei-Pei Li,1 Min Jiang,1 Tao Liu,2,4 Yun Sun1,2
1School of Nursing, Chengdu Medical College, Chengdu, Sichuan, People’s Republic of China; 2Clinical Medical College and the First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, People’s Republic of China; 3School of Nursing, Chongqing Medical University, Chongqing, People’s Republic of China; 4Department of Oncology, Clinical Medical College and the First Affiliated Hospital of Chengdu Medical College, Key Clinical Specialty of Sichuan, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yun Sun, No. 783, Xindu Avenue, Xindu District, Chengdu, Sichuan, People’s Republic of China, Email [email protected] Tao Liu, No. 783, Xindu Avenue, Xindu District, Chengdu, Sichuan, People’s Republic of China, Email [email protected]
Objective: Readiness for hospital discharge is an important indicator of patients’ transition from illness to health and can predict rehabilitation and prognosis. Identifying factors that influence readiness for discharge is crucial for developing effective nursing interventions. Therefore, this study aims to investigate the current status of discharge readiness and its influencing factors in elderly patients with chronic obstructive pulmonary disease (COPD).
Methods: A total of 311 elderly inpatients diagnosed with COPD were enrolled in this investigation at a tertiary hospital in Chengdu between December 2021 and June 2022. Questionnaires were designed to collect general information, disease-related information, and responses to the Readiness for Hospital Discharge Scale (RHDS) and the Quality of Discharge Teaching Scale (QDTS). Univariate and multivariate linear regression analyses were employed to further analyze factors related to discharge readiness and the correlation between discharge readiness and the quality of discharge guidance.
Results: The total score of discharge readiness of elderly COPD patients was 77.72 ± 11.86 with a mean score of 6.48 ± 0.19 for each item. The quality of discharge instructions was 110.54 ± 15.66, with a mean score of 6.12 ± 0.15 for each item. Discharge preparation was positively correlated with the quality of discharge guidance. Multivariate analysis showed that marital status, admission mode, length of stay in hospital, Classification of Severity of Airflow Limitation, mMRC classification, number of medications taken with discharge, presence of inhalers in medication orders, mode of home oxygen therapy, and quality of discharge guidance were independent factors of discharge readiness in elderly COPD patients (P < 0.05).
Conclusion: Both discharge readiness and the quality of discharge guidance for elderly COPD patients in China are currently suboptimal and need further improvement. The survey findings provide valuable insights that can guide future management practices and interventions aimed at improving discharge readiness.
Keywords: chronic obstructive pulmonary disease, discharge readiness, quality of discharge guidance, nursing care
Introduction
Chronic obstructive pulmonary disease (COPD), also referred to as slow obstructive pulmonary disease, is one of the common chronic diseases of the respiratory system. It is the third leading cause of death worldwide, accounting for 6% of the total number of deaths worldwide each year.1,2 In China, the prevalence and mortality rates of COPD remain high, with 24% of new COPD cases being diagnosed and one-third of deaths worldwide attributed to COPD in 2019. The mortality rate and disease burden of COPD in China are much higher than the global average, and advanced age (≥60 years) has been identified as the most important factor contributing to the prevalence of COPD.3,4 Therefore, elderly COPD patients have become the main population for chronic disease prevention and treatment in China. Furthermore, with the implementation of the new healthcare reform policy in China, there has been a growing trend of elderly patients with COPD transitioning from hospital-based care to self-management at home.5 In light of this, there is an urgent to study the current status of discharge readiness and its influencing factors, further improving management models and efficiency.
Discharge readiness was introduced by Fenwick6 in 1979 as a comprehensive assessment of the patient’s physical, psychological and social status, and refers to the perceived readiness of the patient and his/her caregivers for discharge. Readiness for discharge can be used to predict the recovery ability after leaving a healthcare facility, to determine whether a patient can safely transition to a home or community-based nursing facility, and to predict the risk of readmission and death.7–10 Readiness for discharge in COPD patients is strongly associated with mean length of stay and readmission rates.11 Studies on discharge care outcomes in COPD patients have shown that patients are poorly prepared for perceived health and psychosocial well-being upon discharge. This impedes their rehabilitation and self-management of the disease after discharge.12 Due to inadequate nursing knowledge and skills among healthcare providers, COPD patients may be discharged with insufficient preparation, resulting in unplanned readmissions.13 A study of readmissions in adult patients also noted that one of the most common reasons for readmission was acute exacerbation of COPD, and that up to one-third of readmissions could have been avoided via enhancing the readiness of patients and their family caregivers for discharge prior to discharge.14 Therefore, it is important to reasonably determine discharge preparation, ensure the safety of patients discharged from the hospital, and assess the ability of patients to self-management outside of the hospital so as to reduce the readmission and mortality rates of COPD in the elderly. However, there is still a lack of systematic surveys related to the readiness of elderly COPD patients for hospital discharge in China.
Herein, based on the above background, we explored the current status of discharge readiness of elderly patients with COPD and its impacts, with the aim of informing the development of tailored interventions and policies aimed at improving the quality of care and outcomes for elderly COPD patients in China.
Materials and Methods
Participants
Convenience sampling method was used to recruit 311 elderly COPD patients from December 2021 to June 2022 at the Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Chengdu Medical College. Inclusion criteria: 1) Patients meeting the diagnostic criteria for COPD in the 2021 Global Initiative for Chronic Obstructive Lung Disease (GOLD); 2) Age ≥ 60 years; 3) length of stay in hospital ≥ 3 days and discharged against medical advice; 4) Patients had no significant cognitive and language dysfunction and had ability to complete the questionnaire independently or with the help of the investigator; 5) Voluntary participation in this study, and all patients signed an informed consent. The study conforms to the World Medical Association Declaration of Helsinki and has been approved by the Ethics Committee of The First Affiliated Hospital of Chengdu Medical College.
Measurement
Questionnaire of Patients’ General and Clinical Data
Data collection included general and clinical characteristics, including gender, age, education level, marital status, payment method of medical costs, family per capita monthly income, residence status, disease course, whether first hospitalization, admission mode, comorbidities, Classification of Severity of Airflow Limitation, modified Medical Research Council dyspnea scale (mMRC) classification, presence or absence of ventilator, length of stay in hospital, reason for discharge, number of medications taken with discharge, presence of inhalers in medication orders, and long-term home oxygen therapy.
Readiness for Hospital Discharge Scale (RHDS)
We used the Chinese version of the RHDS, which was developed by Weiss et al,15 revised by Lin et al.16 The scale contains 3 dimensions, which are divided into personal status (3 items), adaptive capacity (5 items), and expected support (4 items).17 The Cronbach's alpha coefficient of the scale was 0.91, and the Cronbach's alpha of the three dimensions ranged from 0.84–0.89. Each item was scored 0–10, resulting in a total score of 0–120, with higher scores indicating better readiness for hospital discharge. The level of discharge readiness was determined by adding item scores and dividing by the number of items, resulting in the RHDS score as the mean of item scores. (low level: item mean score <7; moderate level: 7–7.9; high level: 8–8.9; extremely high level ≥9).18
Quality of Discharge Teaching Scale (QDTS)
The Chinese version of QDTS was derived from the version developed by Weiss et al,19 and was translated and adjusted by Wang et al.20 The scale contains 3 dimensions: content needed before discharge (6 items), teaching content actually obtained (6 items), and teaching skills and effectiveness (12 items), for a total of 24 entries.17 The effectiveness of the guidance quality was judged by the total score (180 points) of the two dimensions of “actual content obtained” and “teaching skills and effectiveness”. The higher the total score on QDTS, the higher the patients’ recognition of the quality of discharge guidance. We used the mean of the items to increase the interpretability of the results (sum of items divided by the number of items). The scale ranges from 0 to 10 (low level: item mean score <7; moderate level: 7–7.9; high level: 8–8.9; extremely high level ≥9).
Data Collection
The study was a cross-sectional survey study. Within 4 hours after the discharge order was given, specially trained investigators used uniform instructional language to explain the purpose and content of the survey, as well as the requirements for completing out the questionnaire, to the patients. After obtaining the patients’ consent, the questionnaire was distributed, and the patients completed it anonymously according to their own conditions to ensure authenticity and validity. For patients with dyslexia who could not fill out the questionnaire independently, the researcher provided explanations and then assisted them in completing it. All the data were checked and collected on the spot after completion.
Statistical Methods
All data were entered into Microsoft Excel, and statistical analysis was performed using SPSS 26.0 software. Qualitative data were expressed as the number of cases or percentage (%) and analyzed using Chi-Square Test. Quantitative data were expressed as mean ±standard deviation (SD) and analyzed between two groups using Student’s t-test or among multiple groups using one-way analysis of variance (ANOVA). Using multiple linear regression analysis, we conducted a multivariate analysis by including statistically significant factors obtained from the univariate analysis as independent variables. The discharge readiness score was considered the dependent variable. Additionally, we examined the correlation between discharge readiness and the quality of discharge instructions using Pearson correlation analysis. The test level α was set at 0.05, unless otherwise stated.
Results
Demographic Data of Participants
A total of 311 questionnaires were distributed, and 302 valid questionnaires were obtained, resulting in an effective return rate of 97.1%. Of the total number of patients, 205 were male (67.9%) and 97 were female (32.1%). The survey subjects’ average age ranged from 60 to 95 years old, with a mean age of 74.43±7.84 years old. The overall education level of the survey subjects was low, with 245 patients having only an elementary school education level or below, accounting for 81.10% of the total number of patients, and only 1% of patients had a college education level or above. The majority of elderly COPD patients included in the study were married, as indicated by 227 cases accounting for 75.2% of the total patient sample. Additional general patient information pertaining to discharge readiness scores is provided in Table 1.
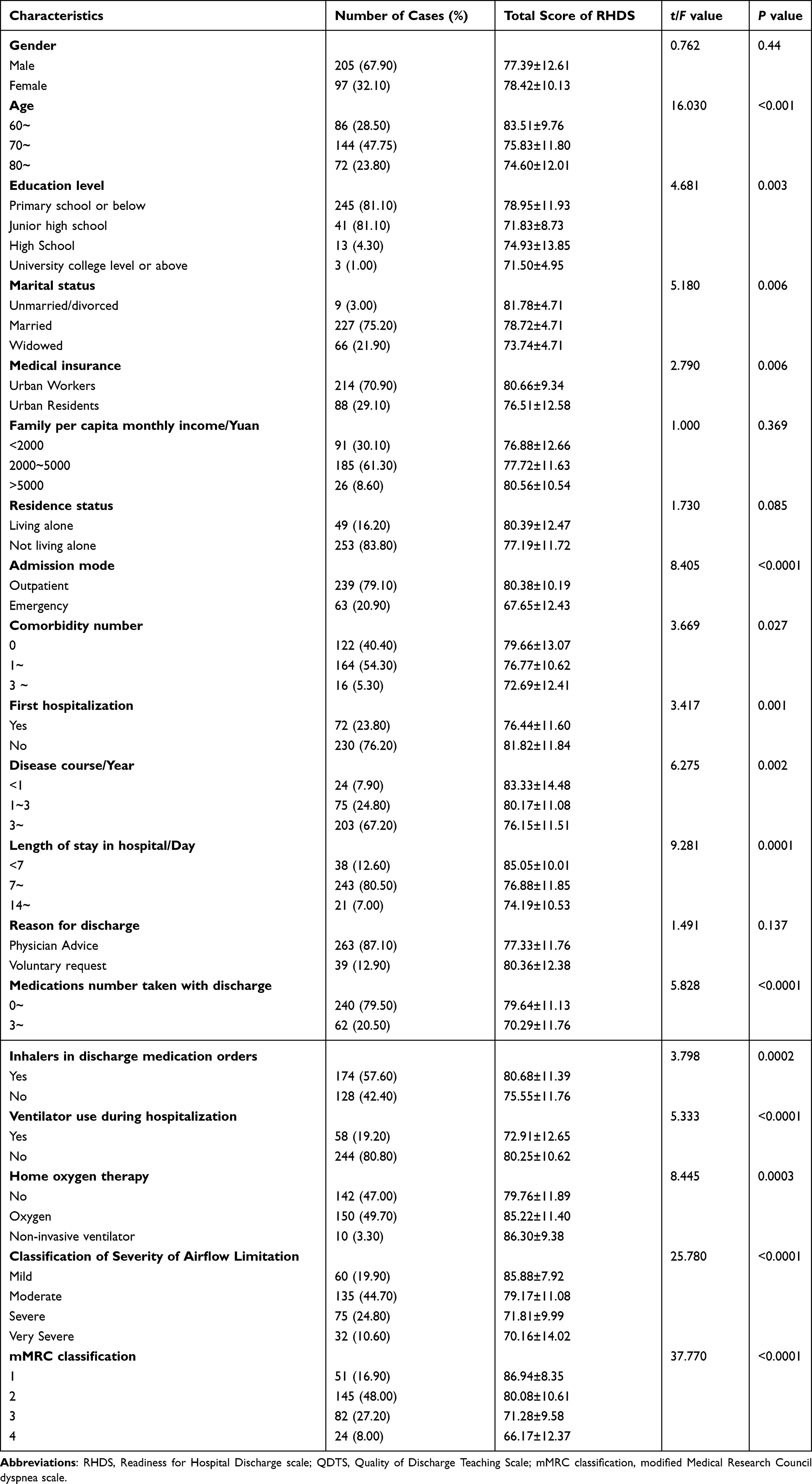 |
Table 1 Demographic Characteristics and Different Range of Discharge Readiness Scores |
Evaluation of Discharge Readiness and Quality of Discharge Guidance
The RHDS total score ranged from 36 to 96, with a mean score of 77.72±11.86 (Table 2). The scores for the three-dimensions were 21.05±3.60 for personal status, 31.11±6.26 for adaptive capacity, and 25.57±4.00 for expected support, respectively. The mean item score was 6.48±0.19. The distribution of total RHDS scores in elderly COPD patients is shown in Figure 1A and B, indicating that the majority of patients are at low levels of discharge readiness. The QDTS total score ranged from 26 to 143, with a mean score of 110.54±15.66 (Table 3). The mean item score was 6.12±0.15. The scores for the three dimensions were 49.48±6.13 for needed content, 29.40±6.35 for actually obtained content, and 81.14±11 for instructional skills and effectiveness, respectively, suggesting poor quality of discharge guidance in elderly COPD patients (Figure 1C and D).
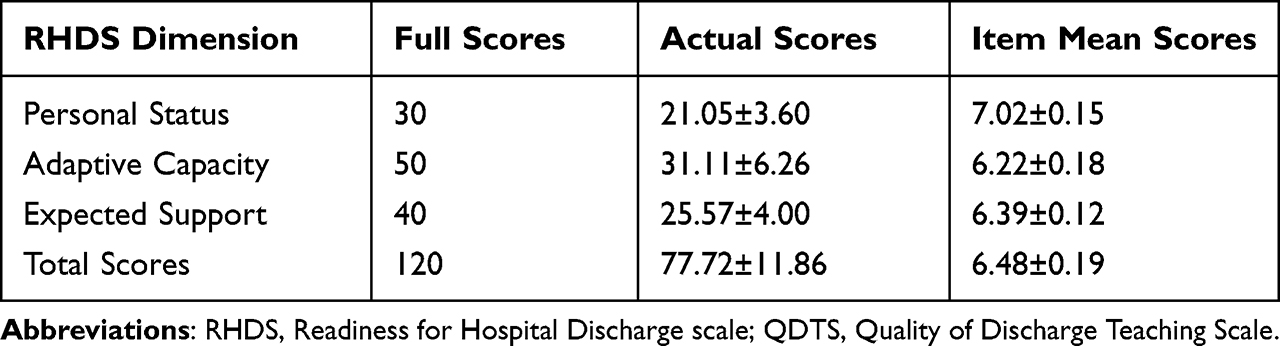 |
Table 2 Total Scores of Discharge Readiness and Different Range of Scores for Each Dimension in Elderly COPD Patients (Points, n=302) |
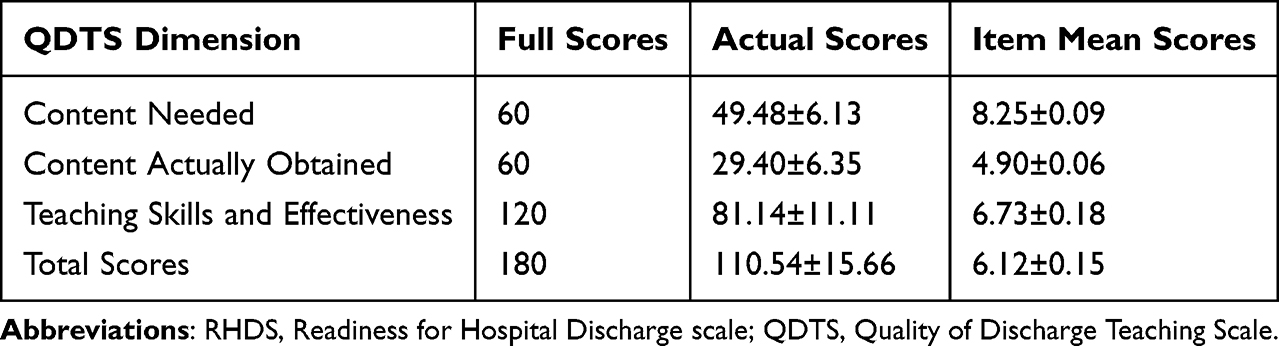 |
Table 3 Total Scores of Quality of Discharge Guidance and Different Range of Scores for Each Dimension in Elderly COPD Patients (Points, n=302) |
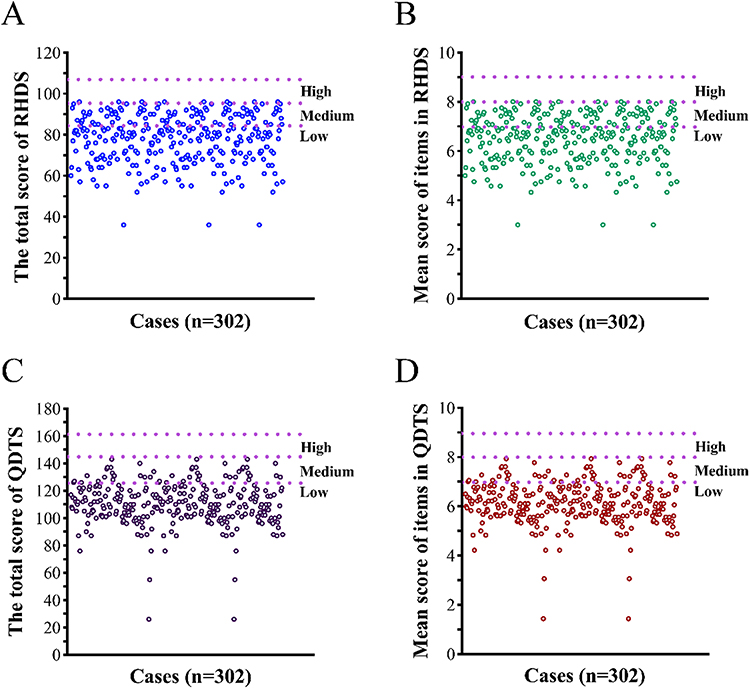 |
Figure 1 Distribution of total and entry mean scores of discharge readiness and quality of discharge guidance for 302 elderly COPD patients. Abbreviations: RHDS, Readiness for Hospital Discharge scale; QDTS, Quality of Discharge Teaching Scale. Notes: (A) Distribution of total score of RHDS; (B) Distribution of mean item score of QDTS; (C) Distribution of total score of RHDS; (D) Distribution of mean item score of QDTS. |
Influencing Factors of Readiness for Discharge in Elderly COPD Patients
As shown in Table 1, many factors were found to influence readiness for discharge in elderly COPD patients. Age, education level, marital status, medical payment method, disease course, whether first hospitalized, admission mode, comorbidity, Classification of Severity of Airflow Limitation, mMRC classification, ventilator use during hospitalization, length of stay in hospital, medications number taken with discharge, inhalers in discharge medication orders, and home oxygen therapy (P < 0.05). In addition, a multiple linear regression analysis was performed to identify independent factors related to discharge readiness, which found out 9 independent variables including marital status, admission mode, length of stay in hospital, Classification of Severity of Airflow Limitation, mMRC classification, medications number taken with discharge, presence or absence of inhalers in the medical discharge orders, home oxygen therapy and quality of discharge instruction (Table 4).
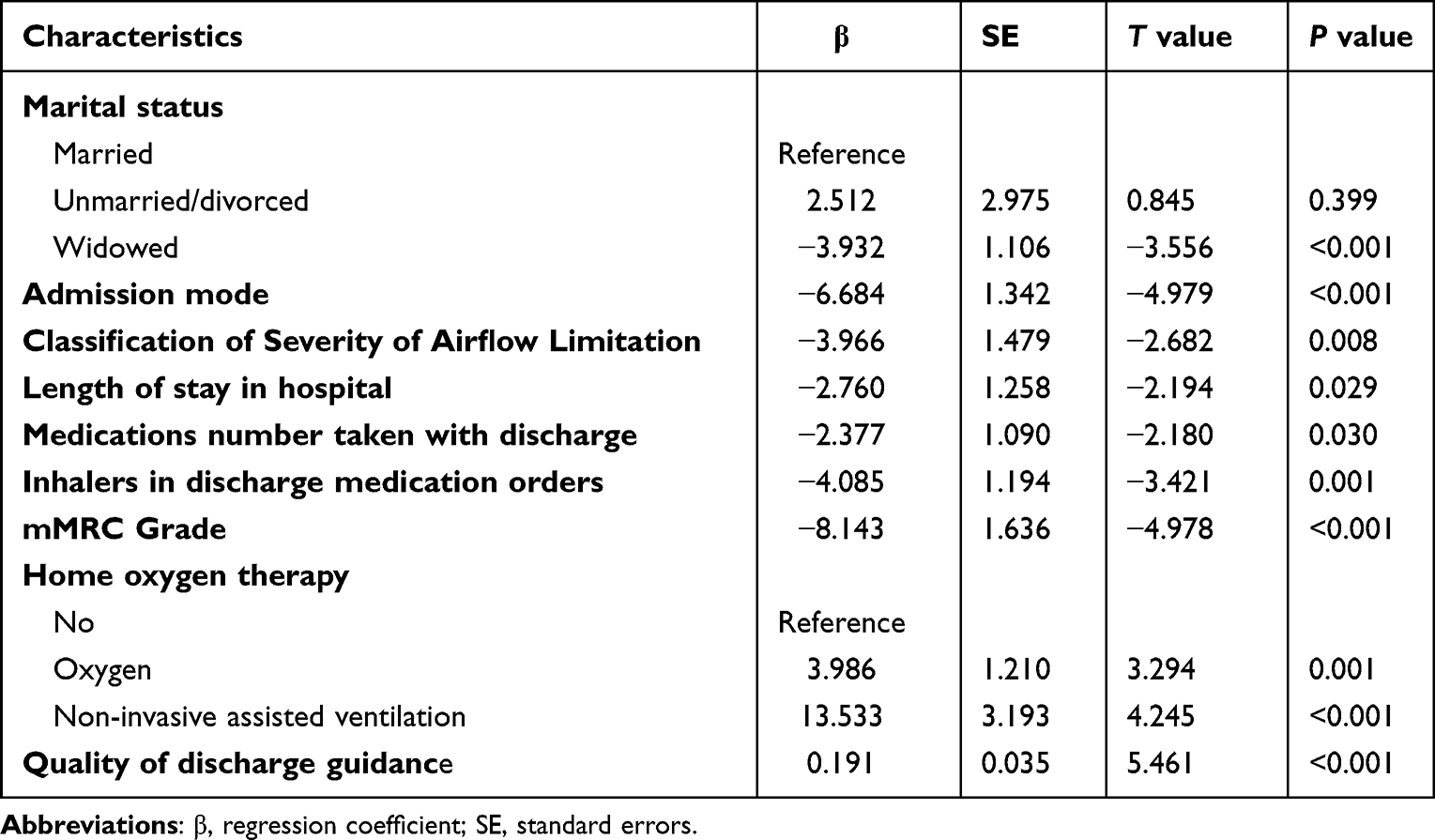 |
Table 4 Multiple Linear Regression Analysis for Factors Affecting Discharge Readiness in Elderly COPD Patients |
Correlations Between Discharge Readiness and Quality of Discharge Guidance in Elderly COPD Patients
The study conducted a Pearson correlation analysis to examine the relationships between several variables. It indicated that the total score of QDTS was positively correlated with the total score of RHDS (r=0.46, P<0.001). In addition, “teaching content actually obtained” (r=0.368) and “teaching skills and effectiveness” (r=0.439) of QDTS were also found to be positively correlated with the total score of RHDS (P<0.001, Table 5). The findings suggest significant linear associations between the total discharge quality score and the total discharge readiness score (Figure 2).
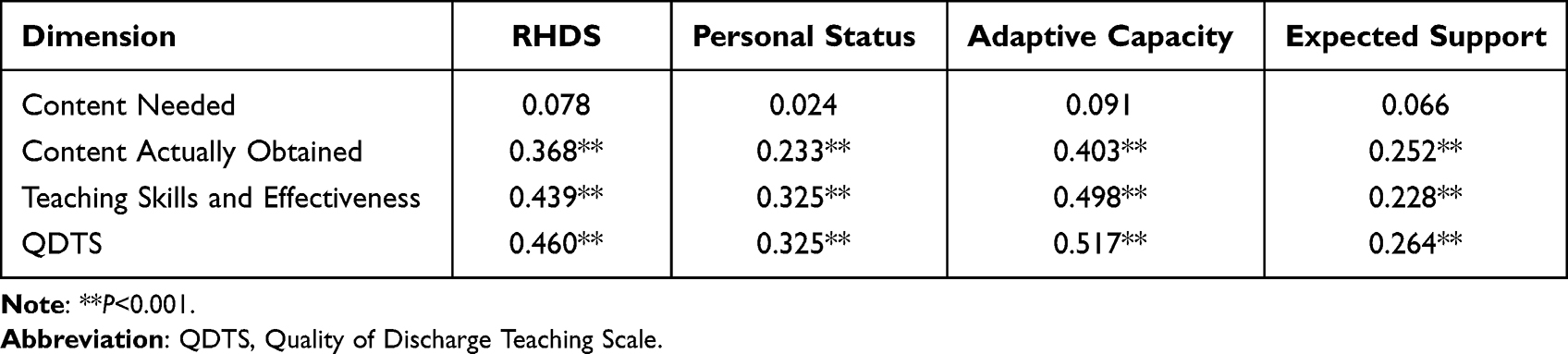 |
Table 5 Correlations Between Discharge Readiness and Quality of Discharge Guidance in Elderly COPD Patients |
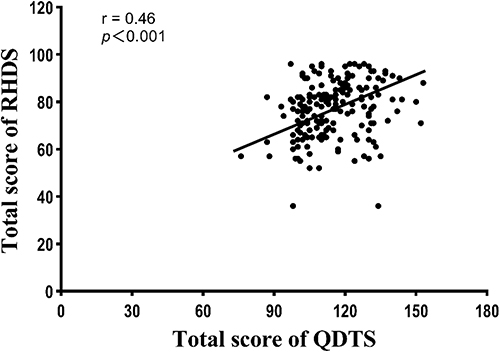 |
Figure 2 Discharge guidance quality and discharge readiness were significant for a linear relation. |
Discussion
COPD is a progressive chronic disease marked by recurrent hospitalizations due to constant symptom onset and a high readmission rate for acutely exacerbated COPD.13 Age is an important physiological factor affecting patients’ readiness for hospital discharge,21 and with the increasing aging problem in China, the health issues of elderly COPD patients are of great concern. In this study, we found that the 6-month rehospitalization rate of elderly COPD patients in this study was up to 76.2%. Out-of-hospital transition preparation has a significant impact on readmission of COPD patients.22 Discharge readiness assessment is an important indicator to ensure the safety of out-of-hospital transition period and to determine the ability to self-management.7 In this study, we observed that elderly COPD patients had a total discharge readiness score of 77.72±11.86 and a mean score of 6.48±0.19 for each term, which is lower than the standardized score,18 suggesting that indeed elderly COPD patients are at a low level of discharge readiness, which increases rehospitalization rate, and that readiness for discharge needs to be improved. Specifically, these patients also need long-term follow-up after discharge, combined with nutritional support and pulmonary rehabilitation training to improve exercise tolerance and tissue oxygenation, as well as autonomous dynamic monitoring of their physical status and proper identification of acute exacerbation episodes.23 Ma et al also suggested that patients readmitted with COPD had a greater need for self-management medical knowledge and skills, family care needs, professional guidance, and information on health care referral services.24 Taken together, discharge readiness plays a non-negligible role in rehospitalization management, and need to be improved.
There is a clear correlation between discharge readiness and marital status, admission mode, length of stay in hospital, Classification of Severity of Airflow Limitation, mMRC classification, number of medications taken with discharge, inhalers in discharge medication orders, mode of home oxygen therapy, as well as quality of discharge guidance. Firstly, this study found that elderly widowed COPD patients were less willing to be discharged. The reason for this may be due to the lack of attentive care, or even companionship for widowed patients, suggesting that spousal support facilitates patient discharge preparation. In addition, the low level of discharge readiness of elderly COPD patients with emergency admissions may be due to lack of home health monitoring and recognition of acute exacerbation symptoms of COPD, weak awareness of disease health monitoring, demonstrate poor self-management.25 This also could be due to the fact that patients with a history of emergency admissions are generally more debilitated and sicker compared to other patient groups.26 Furthermore, these patients may have had experiences of repeated painful symptoms of diseases before, which may lead to medical staff showing greater concern and providing additional protection during hospitalization. Therefore, these patients have a greater reliance on the hospital and medical personnel. And Classification of Severity of Airflow Limitation and mMRC score also influenced the readiness of patients. The higher the patient’s impaired lung function, the lower the patient’s readiness for discharge; the higher the patient’s mMRC score, the lower the patient’s readiness for discharge. This could be related to the fact that COPD is a chronic progressive disease, which means that patients with impaired lung function will gradually worsen and will become more dyspnea. Patients suffering from severe illness often experience symptoms of dyspnea, which can affect their abilities to perform basic tasks such as dressing, eating, and using the bathroom. In severe cases, dyspnea can even occur at rest. As mMRC score grades increase, patients’ quality of life significantly decreases.27 In addition, the effect of drug treatment is limited and some patients choose to give up treatment. This suggests that in our clinical work, we should pay attention to the pulmonary function and mMRC classification of elderly COPD patients, assess the needs of such patients as early as possible, and provide tailored interventions to improve dyspnea symptoms and enhance patients’ readiness for discharge. In addition, discharge readiness of elderly COPD patients is influenced by length of stay in hospital and home oxygen therapy modality. This study observed that elderly COPD patients who could be discharged within one week had higher readiness for discharge than those who were hospitalized for more than one week. The reason arises from two aspects: 1) these patients had relatively stable disease; 2) patients are more receptive to the advice of medical works during hospitalization and are able to follow the medical workers to learn self-care skills. It was also found that the level of readiness for discharge was higher in elderly COPD patients who were able to have long-term home oxygen therapy than those who are not. One study showed that up to 60% of COPD patients were found to remain severely hypoxemic and required continued home supplemental oxygen at a 3-month follow-up after discharge.28 Evidence supports that noninvasive ventilator-assisted ventilation may also improve survival and quality of life in patients with chronic hypercapnia who are stable after discharge.29 Alice et al30 also stated that long-term oxygen therapy improves survival in COPD patients with severe chronic resting hypoxemia. Thus, oxygen therapy modalities are necessary to facilitate the perception of readiness for discharge in elderly patients with COPD.
This study also found that the higher the number of medications brought to the hospital, the lower the readiness to discharge, which is consistent with the results of a chronic single-disease studies in China.31 Patients with inhalants in their discharge medication orders also had lower readiness for discharge. The higher number of medications brought to the hospital for discharge means that patients need to master more drug-related knowledge, and the use of inhalants is far different from that of common medications. If medical personnel do not provide sufficient guidance or patients fail to accurately grasp how to take the medications, it may lead to adverse drug reactions or missed or incorrect doses.32,33 Counseling instructions to provide patients with medications and inhalation devices during discharge are essential in the prevention and management of exacerbations in COPD patients. It has been pointed out that COPD patients have low medication compliance, especially not adhering to inhaled therapy.12,34 Therefore, for elderly COPD patients who are discharged with ≥3 medications or discharged with inhalants, medical workers should strengthen medication instruction and preferably have patients accurately describe and record the precautions for taking medications.
In this study, we also showed that the quality of discharge guidance for elderly COPD patients was at a low level, suggesting that medical workers should pay attention to the quality of discharge guidance. Previous study has shown that the quality of discharge guidance is an important predictor of readiness for discharge.35 The quality of discharge guidance, as an important part of overall care, plays a significant role in patients’ home rehabilitation and compliance behavior. Weiss et al36 pointed out that discharge readiness was positively correlated with discharge skills, and the scores of the discharge instruction skills dimension in this study were also low, suggesting that we should improve the discharge instruction skills in the process of discharge guidance. We should compare the difference between what patients need and what they actually get so that we can provide targeted support and avoid generalized guidance to improve the quality of discharge guidance and thus improve the level of patient readiness for discharge.
As a study limited to a single hospital in Chengdu, Sichuan Province, its population may not be representative of the entire Chinese population. In addition, the present study was a questionnaire study with a small sample size. Therefore, a multicenter study with a larger-sample population needs to be further conducted in the future. Nevertheless, the findings of our study still have noteworthy implications for the development of individualized clinical discharge interventions.
In summary, discharge readiness plays an important role in the recovery and safety of patients during the out-of-hospital transition period. However, there is still room for improvement in the discharge readiness of elderly COPD patients in China. Specifically, the study identified key factors that can be targeted for improvement, such as the quality of discharge guidance and the presence of inhalers in medication orders. These insights can inform the development of tailored interventions and policies to improve the quality of care and outcomes for elderly COPD patients in China. Further research and monitoring will be necessary to evaluate the impact of these interventions on actual practice and outcomes.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki. The studies involving human participants were reviewed and approved by Ethics Committee of The First Affiliated Hospital of Chengdu Medical College. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Department of Sichuan Province (21YYJC0003).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/S0140-6736(22)00470-6
2. Andreas S, Rover C, Heinz J, Taube C, Friede T. COPD mortality and exacerbations in the placebo group of clinical trials over two decades: a systematic review and meta-regression. ERJ Open Res. 2022;8(1):00261–2021. doi:10.1183/23120541.00261-2021
3. Yin P, Wu J, Wang L, et al. The burden of COPD in China and its provinces: findings from the global burden of disease study 2019. Front Public Health. 2022;10:859499. doi:10.3389/fpubh.2022.859499
4. Wang N, Cong S, Fan J, et al. Geographical disparity and associated factors of COPD prevalence in China: a spatial analysis of national cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2020;15:367–377. doi:10.2147/COPD.S234042
5. Gledhill K, Hanna L, Nicks R, Lannin NA. Defining discharge-readiness from subacute care from all stakeholders’ perspectives: a systematic review. Disabil Rehabil. 2021;43(22):3127–3134. doi:10.1080/09638288.2020.1733107
6. Fenwick AM. An interdisciplinary tool for assessing patients’ readiness for discharge in the rehabilitation setting. J Adv Nurs. 1979;4(1):9–21. doi:10.1111/j.1365-2648.1979.tb02984.x
7. Steele NF, Sterling YM. Application of the case study design: nursing interventions for discharge readiness. Clin Nurse Spec. 1992;6(2):79–84. doi:10.1097/00002800-199200620-00008
8. Titler MG, Pettit DM. Discharge readiness assessment. J Cardiovasc Nurs. 1995;9(4):64–74. doi:10.1097/00005082-199507000-00007
9. Mixon AS, Goggins K, Bell SP, et al. Preparedness for hospital discharge and prediction of readmission. J Hosp Med. 2016;11(9):603–609. doi:10.1002/jhm.2572
10. Kaya S, Sain Guven G, Aydan S, et al. Patients’ readiness for discharge: predictors and effects on unplanned readmissions, emergency department visits and death. J Nurs Manag. 2018;26(6):707–716. doi:10.1111/jonm.12605
11. Cope K, Fowler L, Pogson Z. Developing a specialist-nurse-led ‘COPD in-reach service’. Br J Nurs. 2015;24(8):441–445. doi:10.12968/bjon.2015.24.8.441
12. Chai YH, Yang H, Huang GP, Wu T, Dong Y. Nursing Outcomes and Risk Factors of Patients with Chronic Obstructive Pulmonary Disease After Discharge. Int J Chron Obstruct Pulmon Dis. 2021;16:2911–2916. doi:10.2147/COPD.S321375
13. Ruan H, Zhang H, Wang J, Zhao H, Han W, Li J. Readmission rate for acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Respir Med. 2023;206:107090. doi:10.1016/j.rmed.2022.107090
14. Kirk E, Prasad MK, Abdelhafiz AH. Hospital readmissions: patient, carer and clinician views. Acute Med. 2006;5(3):104–107. doi:10.52964/AMJA.0142
15. Weiss ME, Piacentine LB. Psychometric properties of the readiness for hospital discharge scale. J Nurs Meas. 2006;14(3):163–180. doi:10.1891/jnm-v14i3a002
16. Lin YH, Kao CC, Huang AM, Chi MT, Chou FH. 中文版醫院出院準備度量表之信效度檢定 [Psychometric testing of the Chinese version of the readiness for hospital discharge scale]. Hu Li Za Zhi. 2014;61(4):56–65. Chinese. doi:10.6224/JN.61.4.56
17. Marquette University. Hospital Discharge Scales - General Information [webpage on the Internet]. https://www.marquette.edu/nursing/hospital-discharge-scales-general.php.
18. Weiss M, Yakusheva O, Bobay K. Nurse and patient perceptions of discharge readiness in relation to postdischarge utilization. Med Care. 2010;48(5):482–486. doi:10.1097/MLR.0b013e3181d5feae
19. Weiss ME, Lokken L. Predictors and outcomes of postpartum mothers’ perceptions of readiness for discharge after birth. J Obstet Gynecol Neonatal Nurs. 2009;38(4):406–417. doi:10.1111/j.1552-6909.2009.01040.x
20. Wang BH, Wang H, Yang CZ. Reliability and validity of the Chinese version of the quality of discharge teaching scale. Chin J Nurs. 2016;51:752–755.
21. Baksi A, Arda Surucu H, Gülsah IN. Postcraniotomy Patients’ Readiness for Discharge and Predictors of Their Readiness for Discharge. J Neurosci Nurs. 2020;52(6):295–299. doi:10.1097/JNN.0000000000000554
22. Ridwan ES, Hadi H, Wu YL, Tsai PS. Effects of transitional care on hospital readmission and mortality rate in subjects with COPD: a systematic review and meta-analysis. Respir Care. 2019;64(9):1146–1156. doi:10.4187/respcare.06959
23. Bouza E, Alvar A, Almagro P, et al. Chronic obstructive pulmonary disease (COPD) in Spain and the different aspects of its social impact: a multidisciplinary opinion document. Rev Esp Quimioter. 2020;33(1):49–67. doi:10.37201/req/2064.2019
24. Ma Jiachu SL, Shuhua L, Lirong Y. Discharge readiness service needs of readmission patients with COPD: a qualitative study. Chin J Nurs. 2021;35(17):3144–3148. in Chinese.
25. Bringsvor HB, Langeland E, Oftedal BF, Skaug K, Assmus J, Bentsen SB. Effects of a COPD self-management support intervention: a randomized controlled trial. Int J Chron Obstruct Pulmon Dis. 2018;13:3677–3688. doi:10.2147/COPD.S181005
26. Phillips TM, Moloney C, Sneath E, et al. Associated factors, assessment, management, and outcomes of patients who present to the emergency department for acute exacerbation of chronic obstructive pulmonary disease: a scoping review. Respir Med. 2022;193:106747. doi:10.1016/j.rmed.2022.106747
27. Ouaalaya EH, Falque L, Dupis JM, et al. The determinants of dyspnoea evaluated by the mMRC scale: the French Palomb cohort. Respir Med Res. 2021;79:100803. doi:10.1016/j.resmer.2020.100803
28. Soumagne T, Maltais F, Corbeil F, et al. Short-term oxygen therapy outcomes in COPD. Int J Chron Obstruct Pulmon Dis. 2022;17:1685–1693. doi:10.2147/COPD.S366795
29. Owens RL, Derom E, Ambrosino N. Supplemental oxygen and noninvasive ventilation. Eur Respir Rev. 2023;32(167). doi:10.1183/16000617.0159-2022
30. Coffey A, McCarthy GM. Older people’s perception of their readiness for discharge and postdischarge use of community support and services. Int J Older People Nurs. 2013;8(2):104–115. doi:10.1111/j.1748-3743.2012.00316.x
31. Zuo Danni ZH, Fanglei X. Correlations between hospital discharge readiness and discharge instruction quality in chronic disease patients. Chin J Mod Nurs. 2019;25(34):4431–4435. in Chinese.
32. Bourbeau J, Bartlett SJ. Patient adherence in COPD. Thorax. 2008;63(9):831–838. doi:10.1136/thx.2007.086041
33. Sulaiman I, Cushen B, Greene G, et al. Objective assessment of adherence to inhalers by patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;195(10):1333–1343. doi:10.1164/rccm.201604-0733OC
34. Ingebrigtsen TS, Marott JL, Nordestgaard BG, et al. Low use and adherence to maintenance medication in chronic obstructive pulmonary disease in the general population. J Gen Intern Med. 2015;30(1):51–59. doi:10.1007/s11606-014-3029-0
35. Balvardi S, Pecorelli N, Castelino T, et al. Measuring in-hospital recovery after colorectal surgery within a well-established enhanced recovery pathway: a comparison between hospital length of stay and time to readiness for discharge. Dis Colon Rectum. 2018;61(7):854–860. doi:10.1097/DCR.0000000000001061
36. Weiss ME, Sawin KJ, Gralton K, et al. Discharge teaching, readiness for discharge, and post-discharge outcomes in parents of hospitalized children. J Pediatr Nurs. 2017;34:58–64. doi:10.1016/j.pedn.2016.12.021
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.