")
Back to Journals » Journal of Asthma and Allergy » Volume 13
Current Perspectives on the Management of Infantile Atopic Dermatitis
Authors Davari DR , Nieman EL , McShane DB, Morrell DS
Received 6 September 2020
Accepted for publication 13 October 2020
Published 5 November 2020 Volume 2020:13 Pages 563—573
DOI https://doi.org/10.2147/JAA.S246175
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Luis Garcia-Marcos
Danielle R Davari, Elizabeth L Nieman, Diana B McShane, Dean S Morrell
Department of Dermatology, University of North Carolina School of Medicine, Chapel Hill, NC, USA
Correspondence: Dean S Morrell
Department of Dermatology, University of North Carolina School of Medicine, 410 Market Street Suite 400, Chapel Hill, NC 27516, USA
Tel +1 984 974 3900
Fax +1 984 974 3692
Email [email protected]
Abstract: Atopic dermatitis (AD) is a common disease of childhood, and infantile AD may manifest from birth to 2 years. Guidelines for the management of infantile AD are lacking, and our aim is to provide a comprehensive review of best practices and possible interventions. We will focus on topical therapy, since the use of systemic immunomodulating agents in infantile AD is rarely advised. Topical agents include emollients, topical corticosteroids (TCS), topical calcineurin inhibitors (TCIs), and phosphodiesterase 4 (PDE-4) inhibitors. We will also provide a brief overview of promising emerging therapies currently under investigation in the pediatric population.
Keywords: eczema, pediatric, infants, treatment
Introduction
Atopic dermatitis (AD) is an inflammatory skin disorder affecting 5% to 20% of children worldwide.1,2 The estimated annual cost of AD in the United States in 2004 was $4.228 billion, which is the equivalent of approximately $5.9 billion in 2020.3,4 The current lack of uniform diagnostic criteria and availability of an objective test to confirm diagnosis impacts prevalence estimates; however, the burden of AD seems to be increasing, especially among younger children in developing nations.2,5,6 Numerous sets of diagnostic criteria for AD have been proposed, with the Hanifin and Rajka criteria being the most widely used followed by the United Kingdom Working Party criteria.7–9 Common clinical features of AD include pruritus, xerosis, lichenification, flexural involvement, disease course influenced by emotional and/or environmental factors, and early onset of disease.10 Various methods have been established to measure disease severity, such as the Severity Scoring of Atopic Dermatitis index (SCORAD) and the Eczema Area and Severity Index (EASI), which are recommended to estimate objective disease severity.11 AD is often more severe in African American than white children, and structural racism is an important risk factor that contributes to this disparity.12
The three phases of AD are infantile, childhood, and adult. The focus of this review article will be on the infantile phase, which may manifest from birth to 2 years. AD is part of the ‘atopic march’, which is a progression of allergic conditions that develop during infancy and childhood. While not all atopic individuals progress through all features, the atopic march classically begins with AD, followed by IgE-mediated food allergies, asthma and allergic rhinitis. The atopic march is believed to be initiated by allergen exposure through inflamed skin, which may trigger an immunologic response.13 Infantile AD typically begins with erythematous papules and vesicles arising on the cheeks, forehead, and/or scalp, which are intensely pruritic and exudative. These lesions may remain localized or extend to the trunk and extremities, particularly the extensor surfaces. The affected areas are edematous, leading to serous oozing and crusting. Generalized xerosis is also characteristic.14 AD is common in infancy, and almost half the children with infantile AD are in remission by age 3 years.15,16 Significant predictors of a poor prognosis of infantile AD are severity of disease, atopic sensitization, early wheeze, and a strong family history of atopy.16 Quality of life is significantly impacted by infantile AD, with patients suffering from intense pruritus and sleep disturbances, and parents affected by poor sleep quality, cost, emotional stressors and time off work to care for the child.17,18
Pathogenesis
The pathogenesis of AD includes genetic risk factors, environmental triggers and dysregulation of innate and adaptive immunity.19 Epidermal barrier dysfunction is a common precursor of AD in some, and filaggrin gene mutations are a major genetic predisposing factor due to impaired integrity of the stratum corneum.20 Environmental factors that may adversely impact the skin barrier include mechanical damage, such as from repetitive scratching, and certain climate conditions.19,21 The immune response in AD is skewed towards TH2 cell-mediated pathways, with activated TH2 cells releasing IL-4 and IL-13, and systemic IgE-mediated sensitization.22 The skin microbiome is abnormal in patients with AD, which leads to increased Staphylococcus aureus colonization and susceptibility to cutaneous infections.23 The goal of AD management is to control inflammation, improve symptoms and achieve long-term disease control. Guidelines for the management of infantile AD are lacking, and our aim is to provide a comprehensive review of possible interventions. We will evaluate topical and systemic treatment options indicated for infantile AD, as well as off-label therapies.
Literature Search
A systematic search of the PubMed database was performed to identify contributions associated with treatment of infantile AD. Searches were limited to publications in the English language. MeSH terms used in various combinations in the literature search included: atopic dermatitis, eczema, infants, pediatric, children, treatment, topical therapy, emollient, bleach baths, wet wrap therapy, topical corticosteroid, topical calcineurin inhibitor, tacrolimus, pimecrolimus, crisaborole, phototherapy, systemic therapy, dupilumab, and emerging therapy.
Topical Therapy
Topical therapy for AD includes emollients, topical corticosteroids (TCS), topical calcineurin inhibitors (TCIs), and phosphodiesterase 4 (PDE-4) inhibitors. Topical agents provide the foundation of therapy in the management of patients with AD and are often used concomitantly with systemic or phototherapy in more severe cases. TCS are most effective in treating and controlling moderate to severe flares of AD compared to TCIs and PDE-4 inhibitors. We will not discuss topical antimicrobials or antihistamines, since these are generally not recommended in infants.24
Emollients, Bathing Practices and Wet Wrap Therapy
One of the most common clinical features of AD is xerosis resulting from a dysfunctional epidermal barrier, caused by primary epidermal defects or secondary to cutaneous inflammation. Topical emollients should be used to improve skin hydration in patients with AD, and have been shown to prolong the time to flare, decrease the number of flares, and reduce the amounts of topical corticosteroids required to control AD.25 Furthermore, topical anti-inflammatory treatment for AD is more effective when used in combination with emollients.25 There is little evidence that certain emollients perform better than others, and the ideal moisturizing product should be safe, effective, inexpensive, and free of sensitizing agents including additives, fragrances, and perfumes.24,25 Emollient usage seemed promising for primary prevention of AD in high-risk infants; however, a population-based, randomized clinical trial showed that development of AD by age 12 months was not prevented by regular use of emollient bath additives and emollient facial cream beginning at age 2 weeks.26
There is no standard for the frequency or duration of bathing for patients with AD; however, once daily bathing is generally recommended and moisturizer should be applied soon after, especially in the setting of xerotic skin.24 Non-soap cleansers that are neutral to low pH, hypoallergenic, and fragrance-free may be used sparingly.24 A systematic review found that dilute bleach baths do not appear to be more effective than water baths in decreasing AD severity, and there were no differences in S. aureus density in patients treated with dilute bleach baths compared to water baths.27 The utility of dilute bleach baths in the management of AD remains controversial, and any benefits derived are likely due to direct anti-inflammatory activity on the skin rather than the inhibition of S. aureus.28 Wet wrap therapy involves the application of a topical agent under a wet inner layer and dry outer layer of cotton bandages or cotton pajamas. While time intensive and tedious to perform at home, wet wraps may be recommended for patients with moderate to severe AD to decrease disease severity and water loss during flares.24 However, a systematic review found low-quality evidence supporting that wet wrap therapy is more effective than conventional treatment with topical corticosteroids.29
Topical Corticosteroids (TCS)
TCS are used as first-line therapy in the management of patients with AD for both acute flares and maintenance when lesions fail to respond to emollients alone. TCS were introduced in the 1950s for the treatment of inflammatory skin diseases and are classified into 7 groups based on potency.30 Potency levels are measured with a vasoconstrictor assay, in which skin blanching is evaluated after topical application.31 TCS approved for infants 3 months of age and older include hydrocortisone butyrate cream 0.1%, desonide gel/foam 0.05%, fluticasone propionate cream/lotion 0.05%, and fluocinolone acetonide oil 0.01%.32–37 TCS approved for infants 1 year of age and older include prednicarbate emollient cream 0.1% and alclometasone dipropionate cream/ointment 0.05% (Table 1).38,39 For long-term management, the least potent corticosteroid that is effective should be used, however, during acute flares, the use of higher potency TCS may be appropriate and more effective to achieve symptom control. Caution regarding TCS potency and chronicity is required when treating areas such as the face, neck, axillae, perineum, and intertriginous surfaces since these are thin skin sites at higher risk for potential atrophy. TCS are generally applied twice daily until the lesions are significantly improved. Previously, when symptom improvement was achieved TCS usage was discontinued, however, recent studies have shown that a proactive approach may help prevent relapses.40,41
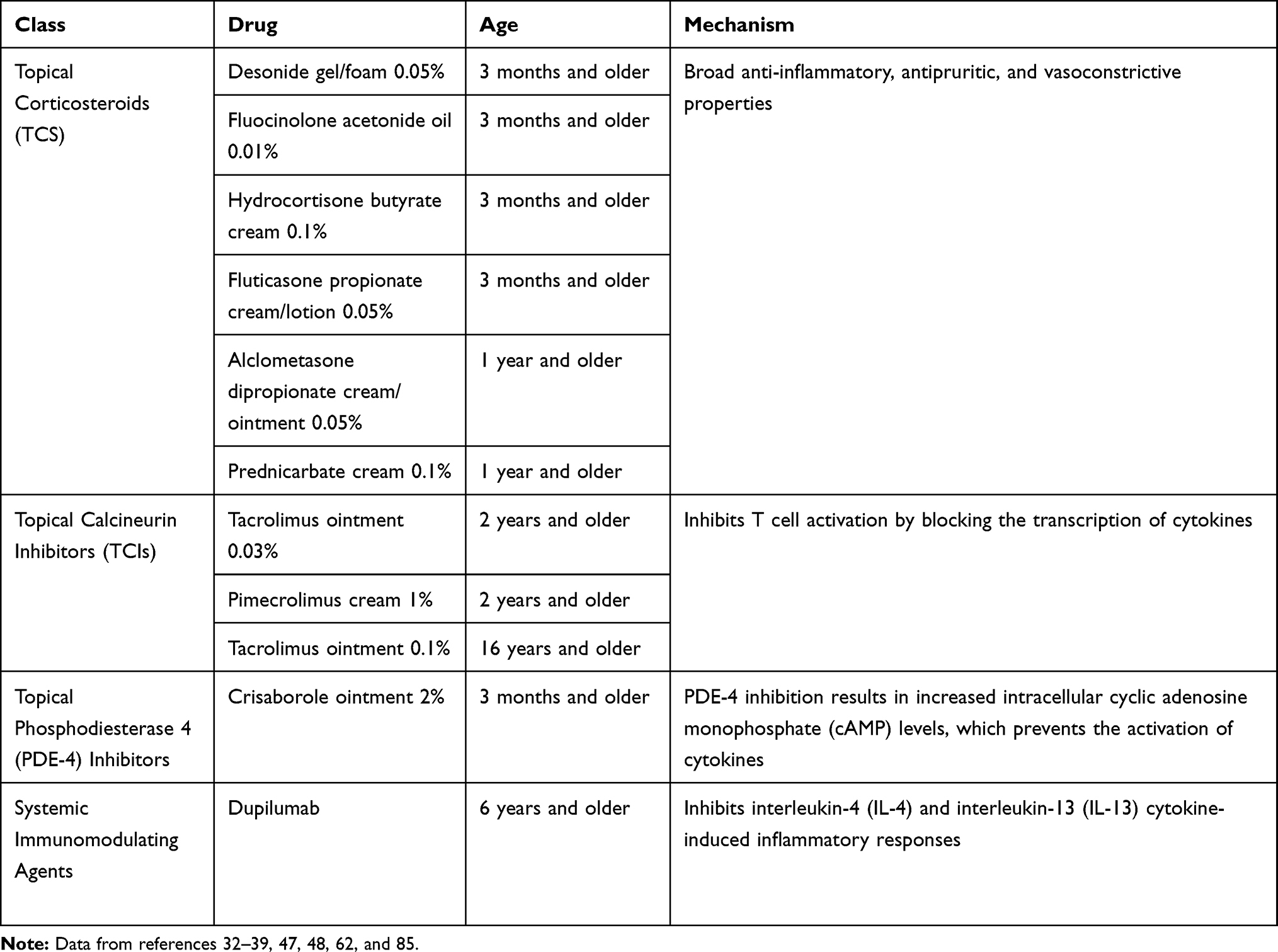 |
Table 1 Therapies Approved for Infantile and Childhood Atopic Dermatitis |
Adverse effects of TCS may be local as well as systemic, however, local effects are more common. These include skin atrophy, striae, rosacea, perioral dermatitis, acne, purpura, hypertrichosis, pigmentation alterations, delayed wound healing, and exacerbations of skin infections. Systemic reactions include hyperglycemia, glaucoma, and adrenal insufficiency.42 Children are more at risk for developing systemic reactions to TCS because of their higher ratio of total body surface area to body weight. The quantities of TCS to apply to children with AD have been described based on patient age and anatomical region beginning at age 3 months.43,44 If TCS usage is discontinued upon the resolution of acute inflammation and the ensuing return of normal-appearing skin, it is very unlikely for patients to experience local or systemic adverse effects. A meta-analysis of 12 clinical trials determined that the incidence of adrenal insufficiency in children (including those younger than age 3 years) using TCS is low, and thus, routine testing of the HPA axis following up to 4 weeks of TCS usage is not recommended unless symptoms of adrenal insufficiency arise.45 Regardless of TCS application frequency and potency, no detrimental growth parameter effects were demonstrated in a study comparing age versus predicted parental heights.46
Topical Calcineurin Inhibitors (TCIs)
TCIs are used as second-line therapy in the management of non-immunocompromised patients with mild to moderate AD for short-term and non-continuous chronic treatment when lesions fail to respond to other topical prescriptions or when those treatments are not advisable.47,48 Introduced in the early 2000s, TCIs are immunosuppressants that inhibit T cell activation by blocking cytokine transcription.47,48 Pimecrolimus cream treats mild to moderate AD and tacrolimus ointment treats moderate to severe AD. Tacrolimus ointment 0.03% and pimecrolimus cream 1% are approved for individuals age 2 years and older, while tacrolimus ointment 0.1% is approved for those age 16 years and older (Table 1).47,48 While not very effective for moderate to severe flares, twice daily application of TCIs during AD exacerbations is recommended to achieve greater symptomatic improvement compared to once daily application.49,50 In addition to treating acute flares, a proactive approach of applying TCIs to recurrent sites of disease two to three times weekly may help reduce relapses.51–53
The most common adverse effects of TCIs are localized site reactions, including burning, stinging, and pruritus.54 Unlike TCS, TCIs do not cause skin atrophy and can be used in areas with thinner skin such as the face and flexor surfaces. Although TCIs are not FDA-approved to treat infantile dermatitis, systematic reviews and meta-analyses of clinical trials support the safe and effective use of TCIs in infants less than 2 years of age.55–57 TCIs are used off-label to treat these infants, and Lugar et al argue that the labeling restrictions should be reconsidered.58 In 2006, the FDA issued a black box warning based on a theoretical risk of malignancy with TCI use. Since then, there is little evidence that a causal relationship exists between TCI use and lymphoma risk based on several epidemiological and clinical studies.59 A multicenter database cohort study that included 19,948 children and 66,127 adults initiating topical tacrolimus, and 23,840 children and 37,417 adults initiating topical pimecrolimus concluded that the use of topical tacrolimus and pimecrolimus was associated with a small excess risk of lymphoma for individual patients, and that results may have been confounded by the severity of atopic dermatitis.60 An observational prospective cohort study of 7954 children with AD treated with topical tacrolimus before 16 years of age for greater than 6 weeks found no evidence of increased long-term cancer risk.61
Crisaborole
Crisaborole ointment 2% is a PDE-4 inhibitor indicated for topical treatment of mild to moderate AD in adults and pediatric patients age 3 months and older (Table 1).62 The inhibition of PDE-4 results in increased intracellular cyclic adenosine monophosphate (cAMP), which prevents the activation of proinflammatory cytokines.62 In December 2016, the FDA approved crisaborole ointment to treat mild to moderate AD in patients age 2 years and older, and in March 2020, this indication was expanded to include patients as young 3 months of age.62 Crisaborole has been shown to be an efficacious and safe option for the treatment of mild to moderate AD in multiple clinical trials.6,63–68,70 A phase IV study of 137 infants aged 3 to less than 24 months with mild to moderate AD demonstrated that twice daily application of crisaborole for 28 days was well tolerated, and 47.3% of patients achieved an Investigator’s Static Global Assessment (ISGA) of clear or almost clear by day 29.70 A network meta-analysis showed that crisaborole was superior to vehicle and pimecrolimus, and comparable to tacrolimus 0.1% or 0.03% in achieving an ISGA of clear or almost clear in patients aged 2 years and older with mild to moderate AD.71
The most commonly reported adverse effect of crisaborole is application site burning or stinging.62 In the clinical study of crisaborole in infants aged less than 24 months, crisaborole was well tolerated and the most frequently reported side effects were similar to those associated with childhood illnesses, including pyrexia, upper respiratory tract infection, diarrhea, and cough. Application site pain and application site discomfort were reported at similar rates to those seen in crisaborole studies in patients aged 2 years and older.70 Importantly, crisaborole is FDA-approved to treat infantile AD, albeit less effective, while most TCS and TCIs are used off-label in this population. However, medication cost may limit its clinical use, and head-to-head trials over longer periods of time are needed to compare crisaborole to other topical therapies.
Phototherapy
Phototherapy is used in the management of patients with AD when lesions fail to respond to topical treatments. Phototherapy delivers ultraviolet (UV) radiation to patients and exerts a variety of immunomodulatory effects, including the suppression of T cell pathways.72,73 Due to complications with administration in infants, this modality is rarely utilized in this age group. Multiple forms of light therapy are available, with narrowband (NB) UVB being the preferred modality based on its low risk profile, relative efficacy, availability, and provider comfort level.74 Retrospective and prospective studies have shown that phototherapy is an effective and generally well tolerated treatment for childhood AD; however, none of these trials included infants less than 2 years of age.75–80
Short-term adverse effects of UVB phototherapy include erythema, blistering, xerosis, pruritus, photosensitive eruptions, and recurrent herpes simplex virus infections. Long-term risks include photo-aging and cutaneous carcinogenesis.81 Further investigations are needed to assess long-term adverse effects, including the true carcinogenic risk of NB-UVB. Certain challenges may arise when using phototherapy in children, including poor compliance with wearing eyewear, difficulty holding still for treatment, and anxiety when entering the light box alone.82 Due to long-term safety risks and treatment challenges, phototherapy may be best utilized as a potential adjunctive treatment in older children, especially those with chronic, lichenified AD.83
Systemic Therapy
Systemic therapy is recommended when the signs and symptoms of AD are not adequately controlled with optimized topical regimens, or when the patient’s medical, physical, or psychological state is negatively impacted.74 Systemic immunomodulating agents include cyclosporine A (CsA), azathioprine (AZA), methotrexate (MTX), mycophenolate mofetil (MMF), interferon gamma (IFN-γ), and biologics, such as dupilumab. The use of systemic agents in childhood and infantile AD is rare and typically off-label, with the only FDA-approved treatment being dupilumab in patients aged 6 years and older. There is a lack of randomized trials in this younger population, especially in infants less than 2 years of age. Insufficient data exist to firmly recommend optimal dosing or duration of therapy for the systemic immunomodulating medications, but all agents should be adjusted to the minimal effective dose once an adequate response is attained.74 Of the off-label agents, CsA, AZA, and MTX are recommended for the treatment of refractory AD, while MMF and IFN- γ may be considered as alternative therapies.74
The TREatment of severe Atopic dermatitis in children Taskforce (TREAT), a project of the Pediatric Dermatology Research Alliance (PeDRA), developed a survey to gather information on systemic agent prescribing practices for severe childhood AD among clinicians in the US and Canada. The survey was completed by 122 members of the Society for Pediatric Dermatology and showed that the most commonly chosen first-line agents were CsA and MTX, second-line agents were MTX and MMF, and third-line agents were AZA and MMF.84
The choice of systemic therapy should be based on each individual patient’s needs, taking into account efficacy and safety, as well as convenience and cost. Most systemic immunomodulating medications require baseline and follow-up laboratory monitoring, with the exception of dupilumab, and some may be cost prohibitive. Detailed mechanisms of action, efficacy, adverse effects, laboratory monitoring, and off-label pediatric dosing for CsA, AZA, MTX, MMF, and IFN- γ may be found elsewhere, as these are not typically appropriate for infantile AD.83 Systemic corticosteroids are not recommended, and their use should be reserved for acute, severe exacerbations as a short-term bridge to another systemic, steroid-sparing agent.74 Adverse effects include rebound flares and increased disease severity upon discontinuation of treatment, as well as decreased linear growth in children.74 The use of systemic antibiotics is recommended in patients with bacterial infections and systemic antiviral agents are recommended in patients with eczema herpeticum.74
Dupilumab
Dupilumab is a human monoclonal IgG4 antibody indicated for the treatment of moderate to severe AD in patients aged 6 years and older whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable (Table 1).85 Dupilumab inhibits IL-4 and IL-13 cytokine-induced inflammatory responses.85 In March 2017 the FDA approved dupilumab to treat adults with moderate to severe AD, and in May 2020 this indication was expanded to include children aged 6 years and older, making it the only biologic approved to treat AD for this patient population.85 It is administered by subcutaneous injection, and the recommended dose in pediatric patients is specified by body weight.85 Dupilumab has been shown to be an efficacious and safe option for the treatment of moderate to severe AD in multiple clinical trials.86–88 A phase III study of 367 children aged 6 to 11 years with severe AD demonstrated that patients treated with dupilumab plus TCS for 16 weeks had a significant improvement in Investigator’s Global Assessment (IGA) compared to those treated with placebo plus TCS.89
The most common adverse reactions of dupilumab are injection site reactions, conjunctivitis, blepharitis, oral herpes, keratitis, eye pruritus, other herpes complex virus infections, and dry eye.85 In the clinical study of dupilumab in children aged 6 to 11 years, dupilumab was well tolerated and the most frequently reported side effects were upper respiratory tract infections, nasopharyngitis, headache, vomiting, injection site erythema and conjunctivitis.89 While dupilumab is not approved to treat infantile AD, a phase II/III study investigating the pharmacokinetics, safety, and efficacy of dupilumab in patients aged greater than 6 months to less than 6 years with moderate to severe AD is currently recruiting.90 It should be noted that access to dupilumab may be restricted due to cost, especially when used off-label in children less than 6 years of age, since patient age may be used to justify denial of insurance coverage.
Emerging Therapies
Emerging topical therapies for AD include janus kinase (JAK) inhibitors, PDE-4 inhibitors, and aryl hydrocarbon receptor modulators. Topical JAK inhibitors currently in clinical trials include ruxolitinib and delgocitinib. Ongoing phase III studies are assessing the efficacy and safety of ruxolitinib cream in patients aged 12 years and older with AD.91,92 An ongoing phase I study is evaluating the safety and pharmacokinetics of delgocitinib cream in pediatric patients aged 2 to 17 years and adults with AD.93 Roflumilast cream is a topical PDE-4 inhibitor and a phase I study is currently recruiting to evaluate its pharmacokinetics, safety and efficacy in pediatric patients aged 2 to 17 years with mild to moderate AD.94 Tapinarof cream is a therapeutic aryl hydrocarbon receptor (AhR) modulating agent shown to be efficacious and well tolerated in 247 patients aged 12 years and older with AD in a phase II study.95
Emerging systemic therapies for AD include biologics and oral JAK inhibitors. Tralokinumab and lebrikizumab are monoclonal antibodies that target IL-13, and nemolizumab is a monoclonal antibody that targets IL-31. An ongoing phase III study is evaluating the efficacy of tralokinumab compared with placebo in treating adolescents aged 12 to 17 years with moderate to severe AD.96 Several phase III trials are recruiting to assess the efficacy and safety of lebrikizumab in patients aged 12 years and older with moderate to severe AD.97–101 An ongoing phase II study is assessing the pharmacokinetics and safety of nemolizumab in adolescents aged 12 to 17 years with moderate to severe AD.102 Phase III studies are recruiting and enrolling by invitation to evaluate the safety and efficacy of nemolizumab in patients aged 12 years and older with moderate to severe AD.103–105 Oral JAK inhibitors currently in clinical trials include baricitinib, upadacitinib, and abrocitinib. A phase III trial is recruiting to assess the efficacy and safety of baricitinib in pediatric patients aged 2 to 17 years with moderate to severe AD.106 Phase III trials are recruiting and ongoing to assess the efficacy and safety of upadacitinib in patients aged 12 years and older with moderate to severe AD.107–110 A phase I study is recruiting to evaluate the safety, pharmacokinetics and tolerability of upadacitinib in pediatric patients aged 6 months to 12 years with severe AD.111 A phase III study is enrolling by invitation to evaluate the efficacy and safety of abrocitinib in patients aged 12 years and older with moderate to severe AD.112 Ultimately, few clinical trials evaluating emerging therapies for AD have been completed in the pediatric population; however, it is promising that several of these studies are ongoing.
Conclusion
The goal of infantile AD management is to control inflammation, improve symptoms and achieve long-term disease control. Once daily bathing is generally recommended, and topical emollients should be applied soon after to improve skin hydration. The pharmacologic treatment of infantile AD is mainly comprised of topical therapy, as systemic therapy is rarely utilized in this population due to long-term safety concerns. TCS are superior to other topical agents for acute flares and maintenance of moderate to severe AD. While TCS may be prescribed off-label, several are approved for infants as young as 3 months of age. Systemic corticosteroids are not recommended, while the use of systemic antibiotics and antiviral agents may be appropriate for patients suffering from superimposed infections. Currently, the only approved systemic treatment for childhood AD is dupilumab in patients aged 6 years and older. However, clinical trials investigating the efficacy and safety of novel topical and systemic therapies for infantile and childhood AD are ongoing. Ultimately, the choice of therapy should be individualized to each patient’s needs and family education is advised to improve treatment adherence.
Disclosure
Dr. Nieman was a principal investigator in an AbbVie trial for upadacitinib (M16-049 trial) and a sub-investigator in a Pfizer trial for a JAK inhibitor (JADE 1036 trial). Dr. McShane was a sub-investigator in a now closed Regeneron investigational study for dupilumab. The authors report no other potential conflicts of interest for this work.
References
1. Williams H, Robertson C, Stewart A, et al. Worldwide variations in the prevalence of symptoms of atopic eczema in the international study of asthma and allergies in childhood. J Allergy Clin Immunol. 1999;103(1 Pt 1):125–138. doi:doi:10.1016/s0091-6749(99)70536-1
2. Odhiambo JA, Williams HC, Clayton TO, Robertson CF, Asher MI, ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J Allergy Clin Immunol. 2009;124(6):1251–8.e23. doi:doi:10.1016/j.jaci.2009.10.009
3. Bickers DR, Lim HW, Margolis D, et al. The burden of skin diseases: 2004 a joint project of the American Academy of dermatology association and the society for investigative dermatology. J Am Acad Dermatol. 2006;55(3):490–500. doi:doi:10.1016/j.jaad.2006.05.048
4. CPI Inflation Calculator. U.S. Bureau of labor statistics. Available from: https://www.bls.gov/data/inflation_calculator.htm.
5. Asher MI, Montefort S, Björkstén B, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys [published correction appears in Lancet. 2007 Sep 29;370(9593):1128]. Lancet. 2006;368(9537):733–743. doi:doi:10.1016/S0140-6736(06)69283-0
6. Williams H, Stewart A, von Mutius E, Cookson W, Anderson HR. International Study of Asthma and Allergies in Childhood (ISAAC) phase one and three study groups. Is eczema really on the increase worldwide? J Allergy Clin Immunol. 2008;121(4):947–54.e15. doi:doi:10.1016/j.jaci.2007.11.004
7. Hanifin J, Rajka G. Diagnostic features of atopic-dermatitis. Acta Derm Venereol. 1980;92:44–47.
8. Williams HC, Burney PG, Hay RJ, et al. The U.K. working party’s diagnostic criteria for atopic dermatitis. i. derivation of a minimum set of discriminators for atopic dermatitis. Br J Dermatol. 1994;131(3):383–396. doi:doi:10.1111/j.1365-2133.1994.tb08530.x
9. Vakharia PP, Chopra R, Silverberg JI. Systematic review of diagnostic criteria used in atopic dermatitis randomized controlled trials. Am J Clin Dermatol. 2018;19(1):15–22. doi:doi:10.1007/s40257-017-0299-4
10. Yew YW, Thyssen JP, Silverberg JI. A systematic review and meta-analysis of the regional and age-related differences in atopic dermatitis clinical characteristics. J Am Acad Dermatol. 2019;80(2):390–401. doi:doi:10.1016/j.jaad.2018.09.035
11. Schmitt J, Langan S, Williams HC. European dermato-epidemiology network. What are the best outcome measurements for atopic eczema? A systematic review. J Allergy Clin Immunol. 2007;120(6):1389–1398. doi:doi:10.1016/j.jaci.2007.08.011
12. Tackett KJ, Jenkins F, Morrell DS, McShane DB, Burkhart CN. Structural racism and its influence on the severity of atopic dermatitis in African American children. Pediatr Dermatol. 2020;37(1):142–146. doi:doi:10.1111/pde.14058
13. Hill DA, Spergel JM. The atopic march: critical evidence and clinical relevance [published correction appears in Ann Allergy Asthma Immunol. 2018 Mar 9]. Ann Allergy Asthma Immunol. 2018;120(2):131–137. doi:doi:10.1016/j.anai.2017.10.037
14. Spergel JM, Paller AS. Atopic dermatitis and the atopic march. J Allergy Clin Immunol. 2003;112(6 Suppl):S118–S127. doi:doi:10.1016/j.jaci.2003.09.033
15. Kay J, Gawkrodger DJ, Mortimer MJ, Jaron AG. The prevalence of childhood atopic eczema in a general population. J Am Acad Dermatol. 1994;30(1):35–39. doi:doi:10.1016/s0190-9622(94)70004-4
16. Illi S, von Mutius E, Lau S, et al. The natural course of atopic dermatitis from birth to age 7 years and the association with asthma. J Allergy Clin Immunol. 2004;113(5):925–931. doi:doi:10.1016/j.jaci.2004.01.778
17. Vakili V, Mollazade Z, Ahanchian H, Kiafar B, Pedram A. The impact of infantile atopic dermatitis on patients’ and their families’ quality of life. International j Pediatrics. 2019;7(6):9517–9524. doi:doi:10.22038/ijp.2019.37437.3256
18. Su JC, Kemp AS, Varigos GA, Nolan TM. Atopic eczema: its impact on the family and financial cost. Arch Dis Child. 1997;76(2):159–162. doi:doi:10.1136/adc.76.2.159
19. Tsakok T, Woolf R, Smith CH, Weidinger S, Flohr C. Atopic dermatitis: the skin barrier and beyond. Br J Dermatol. 2019;180(3):464–474. doi:doi:10.1111/bjd.16934
20. Palmer CN, Irvine AD, Terron-Kwiatkowski A, et al. Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nat Genet. 2006;38(4):441–446. doi:doi:10.1038/ng1767
21. Silverberg JI, Hanifin J, Simpson EL. Climatic factors are associated with childhood eczema prevalence in the United States. J Invest Dermatol. 2013;133(7):1752–1759. doi:doi:10.1038/jid.2013.19
22. Weidinger S, Beck LA, Bieber T, Kabashima K, Irvine AD. Atopic dermatitis. Nat Rev Dis Primers. 2018;4(1):1. doi:doi:10.1038/s41572-018-0001-z
23. Powers CE, McShane DB, Gilligan PH, Burkhart CN, Morrell DS. Microbiome and pediatric atopic dermatitis. J Dermatol. 2015;42(12):1137–1142. doi:doi:10.1111/1346-8138.13072
24. Eichenfield LF, Tom WL, Berger TG, et al. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. J Am Acad Dermatol. 2014;71(1):116–132. doi:doi:10.1016/j.jaad.2014.03.023
25. van Zuuren EJ, Fedorowicz Z, Arents BWM. Emollients and moisturizers for eczema: abridged Cochrane systematic review including GRADE assessments. Br J Dermatol. 2017;177(5):1256–1271. doi:doi:10.1111/bjd.15602
26. Skjerven HO, Rehbinder EM, Vettukattil R, et al. Skin emollient and early complementary feeding to prevent infant atopic dermatitis (PreventADALL): a factorial, multicentre, cluster-randomised trial [published correction appears in Lancet. 2020 Mar 21;395(10228):e53]. Lancet. 2020;395(10228):951–961. doi:doi:10.1016/S0140-6736(19)32983-6
27. Chopra R, Vakharia PP, Sacotte R, Silverberg JI. Efficacy of bleach baths in reducing severity of atopic dermatitis: A systematic review and meta-analysis. Ann Allergy Asthma Immunol. 2017;119(5):435–440. doi:doi:10.1016/j.anai.2017.08.289
28. Sawada Y, Tong Y, Barangi M, et al. Dilute bleach baths used for treatment of atopic dermatitis are not antimicrobial in vitro [published correction appears in J Allergy Clin Immunol. 2019 Nov;144(5):1456]. J Allergy Clin Immunol. 2019;143(5):1946–1948. doi:doi:10.1016/j.jaci.2019.01.009
29. González-López G, Ceballos-Rodríguez RM, González-López JJ, Feito Rodríguez M, Herranz-Pinto P. Efficacy and safety of wet wrap therapy for patients with atopic dermatitis: a systematic review and meta-analysis. Br J Dermatol. 2017;177(3):688–695. doi:doi:10.1111/bjd.15165
30. Del Rosso J, Friedlander SF. Corticosteroids: options in the era of steroid-sparing therapy. J Am Acad Dermatol. 2005;53(1 Suppl 1):S50–S58. doi:doi:10.1016/j.jaad.2005.04.030
31. McKenzie AW, Stoughton R. Method for comparing percutaneous absorption of steroids. Arch Dermatol. 1962;86(5):608. doi:doi:10.1001/archderm.1962.01590110044005.
32. Hydrocortisone Butyrate Cream 0.1% (Lipophilic) [Prescribing Information]. Mahwah: Glenmark Generics Inc; 2013.
33. Desonate® (Desonide) Gel 0.05% [Prescribing Information]. Whippany: Bayer HealthCare Pharmaceuticals Inc; 2014.
34. Verdeso® (Desonide) Foam 0.05% [Prescribing Information]. Research Triangle Park: Stiefel Laboratories, Inc; 2011.
35. Cutivate® (Fluticasone Propionate) Cream 0.05% [Prescribing Information]. Melville: Nycomed US Inc; 2010.
36. Cutivate® (Fluticasone Propionate) Lotion 0.05% [Prescribing Information]. Melville: Fougera Pharmaceuticals Inc; 2015.
37. Derma-Smoothe/FS® (Fluocinolone Acetonide) Topical Oil 0.01% [Prescribing Information]. Sanford: Hill Dermaceuticals, Inc; 2007.
38. Dermatop® (Prednicarbate) Emollient Cream 0.1% [Prescribing Information]. Bridgewater: Sanofi-aventis U.S. LLC; 2010.
39. Aclovate® (Alclometasone Dipropionate) Cream 0.05% and Ointment 0.05% [Prescribing Information]. Melville: Nycomed US Inc; 2010.
40. Schmitt J, von Kobyletzki L, Svensson A, Apfelbacher C. Efficacy and tolerability of proactive treatment with topical corticosteroids and calcineurin inhibitors for atopic eczema: systematic review and meta-analysis of randomized controlled trials. Br J Dermatol. 2011;164(2):415–428. doi:doi:10.1111/j.1365-2133.2010.10030.x
41. Glazenburg EJ, Wolkerstorfer A, Gerretsen AL, Mulder PG, Oranje AP. Efficacy and safety of fluticasone propionate 0.005% ointment in the long-term maintenance treatment of children with atopic dermatitis: differences between boys and girls? Pediatr Allergy Immunol. 2009;20(1):59–66. doi:doi:10.1111/j.1399-3038.2008.00735.x
42. Hengge UR, Ruzicka T, Schwartz RA, Cork MJ. Adverse effects of topical glucocorticosteroids. J Am Acad Dermatol. 2006;54(1):1–18. doi:doi:10.1016/j.jaad.2005.01.010
43. Long CC, Mills CM, Finlay AY. A practical guide to topical therapy in children. Br J Dermatol. 1998;138(2):293–296. doi:doi:10.1046/j.1365-2133.1998.02077.x
44. Nelson AA, Miller AD, Fleischer AB, Balkrishnan R, Feldman SR. How much of a topical agent should be prescribed for children of different sizes? J Dermatolog Treat. 2006;17(4):224–228. doi:doi:10.1080/09546630600894998
45. Wood Heickman LK, Davallow Ghajar L, Conaway M, Rogol AD. Evaluation of hypothalamic-pituitary-adrenal axis suppression following cutaneous use of topical corticosteroids in children: a meta-analysis. Horm Res Paediatr. 2018;89(6):389–396. doi:doi:10.1159/000489125
46. Thomas MW, Panter AT, Morrell DS. Corticosteroids’ effect on the height of atopic dermatitis patients: a controlled questionnaire study. Pediatr Dermatol. 2009;26(5):524–528. doi:doi:10.1111/j.1525-1470.2009.00865.x
47. Protopic® (Tacrolimus) Ointment 0.03% and Ointment 0.1% [Prescribing Information]. Deerfield: Fujisawa Healthcare, Inc; 2000.
48. Elidel® (Pimecrolimus) Cream 1% [Prescribing Information]. East Hanover: Novartis Pharmaceuticals Corporation; 2010.
49. Reitamo S, Harper J, Bos JD, et al. 0.03% Tacrolimus ointment applied once or twice daily is more efficacious than 1% hydrocortisone acetate in children with moderate to severe atopic dermatitis: results of a randomized double-blind controlled trial. Br J Dermatol. 2004;150(3):554–562. doi:doi:10.1046/j.1365-2133.2004.05782.x
50. Ruer-Mulard M, Aberer W, Gunstone A, et al. Twice-daily versus once-daily applications of pimecrolimus cream 1% for the prevention of disease relapse in pediatric patients with atopic dermatitis. Pediatr Dermatol. 2009;26(5):551–558. doi:doi:10.1111/j.1525-1470.2009.00981.x
51. Breneman D, Fleischer AB
52. Paller AS, Eichenfield LF, Kirsner RS, et al. Three times weekly tacrolimus ointment reduces relapse in stabilized atopic dermatitis: a new paradigm for use. Pediatrics. 2008;122(6):e1210–e1218. doi:doi:10.1542/peds.2008-1343
53. Thaci D, Chambers C, Sidhu M, Dorsch B, Ehlken B, Fuchs S. Twice-weekly treatment with tacrolimus 0.03% ointment in children with atopic dermatitis: clinical efficacy and economic impact over 12 months. J Eur Acad Dermatol Venereol. 2010;24(9):1040–1046. doi:doi:10.1111/j.1468-3083.2010.03577.x
54. Eichenfield LF, Ahluwalia J, Waldman A, Borok J, Udkoff J, Boguniewicz M. Current guidelines for the evaluation and management of atopic dermatitis: A comparison of the joint task force practice parameter and american academy of dermatology guidelines. J Allergy Clin Immunol. 2017;139(4S):S49–S57. doi:doi:10.1016/j.jaci.2017.01.009
55. El-Batawy MM, Bosseila MA, Mashaly HM, Hafez VS. Topical calcineurin inhibitors in atopic dermatitis: a systematic review and meta-analysis. J Dermatol Sci. 2009;54(2):76–87. doi:doi:10.1016/j.jdermsci.2009.02.002
56. Huang X, Efficacy XB. Safety of Tacrolimus versus Pimecrolimus for the Treatment of Atopic Dermatitis in Children: A Network Meta-Analysis. Dermatology. 2015;231(1):41–49. doi:doi:10.1159/000381948
57. Siegfried EC, Jaworski JC, Kaiser JD, Hebert AA. Systematic review of published trials: long-term safety of topical corticosteroids and topical calcineurin inhibitors in pediatric patients with atopic dermatitis. BMC Pediatr. 2016;16:75. doi:doi:10.1186/s12887-016-0607-9
58. Luger T, Boguniewicz M, Carr W, et al. Pimecrolimus in atopic dermatitis: consensus on safety and the need to allow use in infants. Pediatr Allergy Immunol. 2015;26(4):306–315. doi:doi:10.1111/pai.12331
59. Siegfried EC, Jaworski JC, Hebert AA. Topical calcineurin inhibitors and lymphoma risk: evidence update with implications for daily practice. Am J Clin Dermatol. 2013;14(3):163–178. doi:doi:10.1007/s40257-013-0020-1
60. Castellsague J, Kuiper JG, Pottegård A, et al. A cohort study on the risk of lymphoma and skin cancer in users of topical tacrolimus, pimecrolimus, and corticosteroids (Joint European Longitudinal Lymphoma and Skin Cancer Evaluation - JOELLE study). Clin Epidemiol. 2018;10:299–310. doi:doi:10.2147/CLEP.S146442
61. Paller AS, Fölster-Holst R, Chen SC, et al. No evidence of increased cancer incidence in children using topical tacrolimus for atopic dermatitis. J Am Acad Dermatol. 2020;83(2):375–381. doi:doi:10.1016/j.jaad.2020.03.075
62. Eucrisa® (Crisaborole) Ointment 2% [Prescribing Information]. New York: Pfizer Inc; 2020.
63. Zane LT, Kircik L, Call R, et al. Crisaborole topical ointment, 2% in patients ages 2 to 17 years with atopic dermatitis: a phase 1b, open-label, maximal-use systemic exposure study. Pediatr Dermatol. 2016;33(4):380–387. doi:doi:10.1111/pde.12872
64. Tom WL, Van Syoc M, Chanda S, Zane LT. Pharmacokinetic Profile, Safety, and Tolerability of Crisaborole Topical Ointment, 2% in Adolescents with Atopic Dermatitis: an Open-Label Phase 2a Study. Pediatr Dermatol. 2016;33(2):150–159. doi:doi:10.1111/pde.12780
65. Zane LT, Hughes MH, Shakib S. Tolerability of crisaborole ointment for application on sensitive skin areas: a randomized, double-blind, vehicle-controlled study in healthy volunteers. Am J Clin Dermatol. 2016;17(5):519–526. doi:doi:10.1007/s40257-016-0204-6
66. Stein Gold LF, Spelman L, Spellman MC, Hughes MH, Zane LT. A phase 2, randomized, controlled, dose-ranging study evaluating crisaborole topical ointment, 0.5% and 2% in adolescents with mild to moderate atopic dermatitis. J Drugs Dermatol. 2015;14(12):1394–1399.
67. Murrell DF, Gebauer K, Spelman L, Zane LT. Crisaborole topical ointment, 2% in adults with atopic dermatitis: a phase 2a, vehicle-controlled, proof-of-concept study. J Drugs Dermatol. 2015;14(10):1108–1112.
68. Paller AS, Tom WL, Lebwohl MG, et al. Efficacy and safety of crisaborole ointment, a novel, nonsteroidal phosphodiesterase 4 (PDE4) inhibitor for the topical treatment of atopic dermatitis (AD) in children and adults [published correction appears in J Am Acad Dermatol. 2017 Apr;76(4):777]. J Am Acad Dermatol. 2016;75(3):494–503.e6. doi:doi:10.1016/j.jaad.2016.05.046
69. Eichenfield LF, Call RS, Forsha DW, et al. Long-term safety of crisaborole ointment 2% in children and adults with mild to moderate atopic dermatitis. J Am Acad Dermatol. 2017;77(4):641–649.e5. doi:doi:10.1016/j.jaad.2017.06.010
70. Schlessinger J, Shepard JS, Gower R, et al. Safety, effectiveness, and pharmacokinetics of crisaborole in infants aged 3 to < 24 months with mild-to-moderate atopic dermatitis: a phase iv open-label study (crisade care 1). Am J Clin Dermatol. 2020;21(2):275–284. doi:doi:10.1007/s40257-020-00510-6
71. Fahrbach K, Tarpey J, Washington EB, et al. Crisaborole ointment, 2%, for treatment of patients with mild-to-moderate atopic dermatitis: systematic literature review and network meta-analysis [published online ahead of print, 2020 may 20]. Dermatol Ther (Heidelb). 2020. doi:doi:10.1007/s13555-020-00389-5
72. Krutmann J, Morita A. Mechanisms of ultraviolet (UV) B and UVA phototherapy. J Investig Dermatol Symp Proc. 1999;4(1):70–72. doi:10.1038/sj.jidsp.5640185
73. Tintle S, Shemer A, Suárez-Fariñas M, et al. Reversal of atopic dermatitis with narrow-band UVB phototherapy and biomarkers for therapeutic response. J Allergy Clin Immunol. 2011;128(3):583–93.e934. doi:10.1016/j.jaci.2011.05.042
74. Sidbury R, Davis DM, Cohen DE, et al. Guidelines of care for the management of atopic dermatitis: section 3. Management and treatment with phototherapy and systemic agents. J Am Acad Dermatol. 2014;71(2):327–349. doi:10.1016/j.jaad.2014.03.030
75. Collins P, Ferguson J. Narrowband (TL-01) UVB air-conditioned phototherapy for atopic eczema in children. Br J Dermatol. 1995;133(4):653–655. doi:10.1111/j.1365-2133.1995.tb02725.x
76. Clayton TH, Clark SM, Turner D, Goulden V. The treatment of severe atopic dermatitis in childhood with narrowband ultraviolet B phototherapy. Clin Exp Dermatol. 2007;32(1):28–33. doi:10.1111/j.1365-2230.2006.02292.x
77. Pavlovsky M, Baum S, Shpiro D, Pavlovsky L, Pavlotsky F. Narrow band UVB: is it effective and safe for paediatric psoriasis and atopic dermatitis? J Eur Acad Dermatol Venereol. 2011;25(6):727–729. doi:10.1111/j.1468-3083.2010.03832.x
78. Darné S, Leech SN, Taylor AE. Narrowband ultraviolet B phototherapy in children with moderate-to-severe eczema: a comparative cohort study. Br J Dermatol. 2014;170(1):150–156. doi:10.1111/bjd.12580
79. Dayal S, Pathak K, Sahu P, Jain VK. Narrowband UV-B phototherapy in childhood atopic dermatitis: efficacy and safety. An Bras Dermatol. 2017;92(6):801–806. doi:10.1590/abd1806-4841.20175958
80. Eustace K, Dolman S, Alsharqi A, Sharpe G, Parslew R. Use of Phototherapy in Children. Pediatr Dermatol. 2017;34(2):150–155. doi:10.1111/pde.13072
81. Crall CS, Rork JF, Delano S, Huang JT. Phototherapy in children: considerations and indications. Clin Dermatol. 2016;34(5):633–639. doi:10.1016/j.clindermatol.2016.05.018
82. Juarez MC, Grossberg AL. Phototherapy in the Pediatric Population. Dermatol Clin. 2020;38(1):91–108. doi:10.1016/j.det.2019.08.012
83. Slater NA, Morrell DS. Systemic therapy of childhood atopic dermatitis. Clin Dermatol. 2015;33(3):289–299. doi:10.1016/j.clindermatol.2014.12.005
84. Totri CR, Eichenfield LF, Logan K, et al. Prescribing practices for systemic agents in the treatment of severe pediatric atopic dermatitis in the US and Canada: the PeDRA TREAT survey. J Am Acad Dermatol. 2017;76(2):281–285. doi:10.1016/j.jaad.2016.09.021
85. Dupixent® (Dupilumab) Injection [Prescribing Information]. Tarrytown: Regeneron Pharmaceuticals, Inc; 2020.
86. Blauvelt A, de Bruin-weller M, Gooderham M, et al. Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): a 1-year, randomised, double-blinded, placebo-controlled, Phase 3 trial. Lancet. 2017;389(10086):2287–2303. doi:10.1016/S0140-6736(17)31191-1
87. Simpson EL, Bieber T, Guttman-Yassky E, et al. Two Phase 3 Trials of Dupilumab versus Placebo in Atopic Dermatitis. N Engl J Med. 2016;375(24):2335–2348. doi:10.1056/NEJMoa1610020
88. Simpson EL, Paller AS, Siegfried EC, et al. Efficacy and safety of dupilumab in adolescents with uncontrolled moderate to severe atopic dermatitis: a phase 3 randomized clinical trial [published online ahead of print, 2019 Nov 6]. JAMA Dermatol. 2019;156(1):44–56. doi:10.1001/jamadermatol.2019.3336
89. Regeneron Pharmaceuticals. Study to investigate the efficacy and safety of dupilumab administered with topical corticosteroids (TCS) in participants ≥6 to <12 years with severe atopic dermatitis (AD). Available from: https://clinicaltrials.gov/ct2/show/NCT03345914?term=NCT03345914&draw=2&rank=1. NLM identifier: NCT03345914.
90. Regeneron Pharmaceuticals. Safety, pharmacokinetics and efficacy of dupilumab in patients ≥6 months to <6 years with moderate-to-severe atopic dermatitis (liberty AD PRESCHOOL) (Liberty AD). Available from: https://clinicaltrials.gov/ct2/show/NCT03346434?term=NCT03346434&draw=2&rank=1. NLM identifier: NCT03346434.
91. Incyte Corporation. TRuE AD1 - an efficacy and safety study of ruxolitinib cream in adolescents and adults with atopic dermatitis. Available from: https://www.clinicaltrials.gov/ct2/show/NCT03745638?term=NCT03745638&draw=2&rank=1. NLM identifier: NCT03745638.
92. Incyte Corporation. TRuE AD2 - an efficacy and safety study of ruxolitinib cream in adolescents and adults with atopic dermatitis. Available from: https://www.clinicaltrials.gov/ct2/show/NCT03745651?term=NCT03745651&draw=2&rank=1. NLM identifier: NCT03745651.
93. Pharma LEO. Delgocitinib cream for the treatment of moderate to severe atopic dermatitis during 8 weeks in adults, adolescents, and children. Available from: https://www.clinicaltrials.gov/ct2/show/NCT03826901?term=NCT03826901&draw=2&rank=1. NLM identifier: NCT03826901.
94. Arcutis Biotherapeutics, Inc. Pharmacokinetics, safety, and efficacy of ARQ-151 once a day in adolescents and children with mild to moderate eczema. Available from: https://www.clinicaltrials.gov/ct2/show/NCT04156191?term=NCT04156191&draw=2&rank=1. NLM identifier: NCT04156191.
95. Peppers J, Paller AS, Maeda-Chubachi T, et al. A phase 2, randomized dose-finding study of tapinarof (GSK2894512 cream) for the treatment of atopic dermatitis. J Am Acad Dermatol. 2019;80(1):89–98.e3. doi:10.1016/j.jaad.2018.06.047
96. Pharma LEO. Tralokinumab monotherapy for adolescent subjects with moderate to severe atopic dermatitis - ECZTRA 6 (ECZema TRAlokinumab Trial no. 6). Available from: https://www.clinicaltrials.gov/ct2/show/NCT03526861?term=NCT03526861&draw=2&rank=1. NLM identifier: NCT03526861.
97. Eli Lilly and Company. Long-term safety and efficacy study of lebrikizumab (ly3650150) in participants with moderate-to-severe atopic dermatitis. Available from: https://www.clinicaltrials.gov/ct2/show/NCT04392154?term=NCT04392154&draw=2&rank=1. NLM identifier: NCT04392154.
98. Eli Lilly and Company. Study to assess the safety and efficacy of lebrikizumab (ly3650150) in adolescent patients with moderate-to-severe atopic dermatitis (ADore). Available from: https://www.clinicaltrials.gov/ct2/show/NCT04250350?term=NCT04250350&draw=2&rank=1. NLM identifier: NCT04250350.
99. Eli Lilly and Company. Evaluation of the efficacy and safety of lebrikizumab (ly3650150) in moderate to severe atopic dermatitis (advocate2). Available from: https://www.clinicaltrials.gov/ct2/show/NCT04178967?term=NCT04178967&draw=2&rank=1. NLM identifier: NCT04178967.
100. Eli Lilly and Company. Evaluation of the efficacy and safety of lebrikizumab (ly3650150) in moderate to severe atopic dermatitis (advocate1). Available from: https://www.clinicaltrials.gov/ct2/show/NCT04146363?term=NCT04146363&draw=2&rank=1. NLM identifier: NCT04146363.
101. Eli Lilly and Company. Safety and efficacy of lebrikizumab (ly3650150) in combination with topical corticosteroid in moderate to severe atopic dermatitis. (adhere). Available from: https://www.clinicaltrials.gov/ct2/show/NCT04250337?term=NCT04250337&draw=2&rank=1. NLM identifier: NCT04250337.
102. Galderma R&D. A pharmacokinetics and safety study of nemolizumab in adolescent subjects with atopic dermatitis (AD). Available from: https://www.clinicaltrials.gov/ct2/show/NCT03921411?term=NCT03921411&draw=1&rank=1. NLM identifier: NCT03921411.
103. Galderma R&D. Long-term safety and efficacy of nemolizumab with moderate-to-severe atopic dermatitis. Available from: https://www.clinicaltrials.gov/ct2/show/NCT03989206?term=NCT03989206&draw=2&rank=1. NLM identifier: NCT03989206.
104. Galderma R&D. Efficacy and safety of nemolizumab in subjects with moderate-to-severe atopic dermatitis. Available from: https://www.clinicaltrials.gov/ct2/show/NCT03985943?term=NCT03985943&draw=2&rank=1. NLM identifier: NCT03985943.
105. Galderma R&D. Efficacy & safety of nemolizumab in subjects with moderate-to-severe atopic dermatitis. Available from: https://www.clinicaltrials.gov/ct2/show/NCT03989349?term=NCT03989349&draw=2&rank=1. NLM identifier: NCT03989349.
106. Eli Lilly and Company. A study of baricitinib (ly3009104) in children and adolescents with atopic dermatitis (BREEZE-AD-PEDS), Available from: https://www.clinicaltrials.gov/ct2/show/NCT03952559?term=NCT03952559&draw=2&rank=1. NLM identifier: NCT03952559.
107. AbbVie. Evaluation of upadacitinib in adolescent and adult patients with moderate to severe atopic dermatitis (eczema) (measure up 1). Available from: https://www.clinicaltrials.gov/ct2/show/NCT03569293?term=NCT03569293&draw=2&rank=1. NLM identifier: NCT03569293.
108. AbbVie. A study to evaluate upadacitinib in combination with topical corticosteroids in adolescent and adult participants with moderate to severe atopic dermatitis (AD Up). Available from: https://www.clinicaltrials.gov/ct2/show/NCT03568318?term=NCT03568318&draw=2&rank=1. NLM identifier: NCT03568318.
109. AbbVie. A study to evaluate safety of upadacitinib in combination with topical corticosteroids in adolescent and adult participants with moderate to severe atopic dermatitis. Available from: https://www.clinicaltrials.gov/ct2/show/NCT03661138?term=NCT03661138&draw=2&rank=1. NLM identifier: NCT03661138.
110. AbbVie. A study to evaluate upadacitinib in adolescent and adult subjects with moderate to severe atopic dermatitis (measure up 2). Available from: https://www.clinicaltrials.gov/ct2/show/NCT03607422?term=NCT03607422&draw=2&rank=1. NLM identifier: NCT03607422.
111. AbbVie. A study to evaluate the pharmacokinetics, safety and tolerability of upadacitinib in pediatric participants with severe atopic dermatitis. Available from: https://www.clinicaltrials.gov/ct2/show/NCT03646604?term=NCT03646604&draw=2&rank=1. NLM identifier: NCT03646604.
112. Pfizer. Study to evaluate efficacy and safety of pf-04965842 with or without topical medications in subjects aged 12 years and older with moderate to severe atopic dermatitis (JADE EXTEND). Available from: https://www.clinicaltrials.gov/ct2/show/NCT03422822?term=NCT03422822&draw=2&rank=1. NLM identifier: NCT03422822.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.