")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Current Perspectives on the Impact of the National Diabetes Prevention Program: Building on Successes and Overcoming Challenges
Authors Ritchie ND , Baucom KJW, Sauder KA
Received 2 June 2020
Accepted for publication 8 July 2020
Published 19 August 2020 Volume 2020:13 Pages 2949—2957
DOI https://doi.org/10.2147/DMSO.S218334
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Natalie D Ritchie,1– 3 Katherine JW Baucom,4 Katherine A Sauder5,6
1Ambulatory Care Services, Denver Health and Hospital Authority, Denver, CO, USA; 2Department of Psychiatry, University of Colorado School of Medicine, Aurora, CO, USA; 3University of Colorado College of Nursing, Aurora, CO, USA; 4Department of Psychology, University of Utah, Salt Lake City, UT, USA; 5Department of Pediatrics, University of Colorado School of Medicine, Aurora, CO, USA; 6Lifecourse Epidemiology of Adiposity and Diabetes (LEAD) Center, University of Colorado, Aurora, CO, USA
Correspondence: Natalie D Ritchie
Denver Health and Hospital Authority Email [email protected]
Abstract: To address the public health and economic burden of type 2 diabetes, the Centers for Disease Control and Prevention (CDC) began dissemination of the National Diabetes Prevention Program (NDPP) in the United States in 2010. Based on the intensive lifestyle intervention from a large efficacy trial, the NDPP aims to reduce incidence through lifestyle change and weight loss. This narrative review summarizes evidence on reach, effectiveness, and sustainability of the NDPP, while highlighting opportunities to overcome challenges in these areas. Major successes include reaching hundreds of thousands of at-risk individuals across the nation, with notable effectiveness upon full participation and widespread insurance coverage. Yet, more work is needed to ensure greater public health impact, particularly among priority populations at heightened risk who also experience disparities in program outcomes. Preliminary evidence suggests a number of strategies may improve reach and effectiveness of the NDPP, often with more rigorous study needed prior to widespread uptake. Updating the NDPP to better match the current evidence-base may also be important, such as directly targeting glycemia with a patient-centered approach and promoting metformin as an adjunct or second-line treatment. Finally, revisiting pay-for-performance reimbursement models may be critical to sustainability by ensuring adequate availability of suppliers and ultimately reducing diabetes prevalence.
Keywords: obesity, type 2 diabetes mellitus, prediabetes, lifestyle modification, prevention
Introduction
Diabetes affects 13% of adults in the US,1 imposing major public health and economic burdens. Another 34.5% of US adults are estimated to have prediabetes,1 or elevated blood glucose that may progress to type 2 diabetes without intervention. The National Diabetes Prevention Program (NDPP) is an evidence-based intervention to prevent diabetes in at-risk populations in the US that has been disseminated nationwide since 2010 under Centers for Disease Control and Prevention (CDC) leadership,2 with the first participants served in 2012.3 The NDPP is a translation of the intensive lifestyle intervention from the Diabetes Prevention Program (DPP) trial, which demonstrated a 58% reduction in incidence over 3 years,4 with benefits persisting up to 15 years.5,6 Using a lower-cost scalable model, the NDPP promotes ≥5% weight loss over one year via in-person classes, distance learning, online programming, or a combination of modalities. Participants may include overweight/obese adults with prediabetes or other risk factors such as past gestational diabetes. This narrative review examines the current impact of NDPP dissemination in the US based on recent literature and reports, including successes as well as opportunities to overcome challenges regarding reach, effectiveness, and sustainability.
Reach
Successes with Reach
The NDPP has achieved impressive scaling with over 1,500 sites as of 2020, per the CDC’s registry of organizations participating in their Diabetes Prevention and Recognition Program (DPRP) that monitors fidelity and quality.7,8 This reflects an exceptional degree of adoption for a prevention program that transitioned from a clinical trial to translation into communities.9 There are currently NDPP sites in all 50 US states, the District of Columbia, and most US territories.7 Sites include community-based organizations, healthcare clinics and systems, pharmacies, health plans, public health and other governmental institutions, universities, and private wellness companies,7 uniquely providing a variety of settings in which to access the program. In turn, population reach has been fast increasing from about 35,000 eligible participants served as of 20163 to over 324,000 by early 2019.10 Whereas the inherently limited capacity of in-person sites might cap potential growth, online and distance learning models have also been approved by the CDC since 2015 and 2018, respectively,10 with more limitless potential to expand reach. Indeed, despite fewer online than in-person NDPP suppliers7 and later approval for dissemination, online delivery exceeds the reach of in-person programs.10 Such virtual delivery can also ensure wide geographic reach to fill the many gaps where in-person sites are unavailable.11,12
Overcoming Challenges with Reach
Increasing Awareness of Diabetes Risks
As 88 million US adults are estimated to have prediabetes,1 reach to hundreds of thousands of at-risk persons with the NDPP is highly commendable, but not yet scaled for population health impact. An upstream issue is that few adults with prediabetes are aware of their condition (15.3%),1 although it is encouraging that risk awareness has been increasing over time. Self-reports of perceived risk for diabetes due to a variety of factors increased from 30% in 2011 to 45% in 2016.13 Moreover, when individuals become aware of having prediabetes, they are likely to take preventative action as 71% report efforts to reduce the likelihood of diabetes onset.13 Media campaigns are a common approach to increase widespread risk awareness and promote the NDPP (i.e., 90.2% of NDPP sites reported use of mass media as a recruitment strategy),14 yet resulting uptake appears limited,15 and cost-effectiveness is unclear. Increasing awareness and reach of the NDPP through systematic screening and referrals has arisen as a more promising scalable strategy.
Increasing Provider Referrals to the NDPP
A large study led by the American Medical Association found 56% enrollment upon point-of-care referrals to the NDPP and 11% enrollment using a retrospective, algorithm-based approach to referrals.16 These results are fully consistent with the first known study of NDPP uptake with provider referrals.17 Despite the comparably low rate of engagement upon algorithmic referrals, the potential to automate this approach is important for scalability, as well as reducing provider burden to meet US Preventive Services Task Force recommendations to refer at-risk individuals to intensive lifestyle interventions.18,19 Relatively few point-of-care referrals to the NDPP are made currently.16 First, many providers are unaware of the NDPP as a resource for their patients. A 2016 survey of over 1,200 primary care providers found that only 38% were aware of the NDPP, and fewer (23%) had referred patients to the program.20 To address this issue, NDPP sites can proactively seek to establish referral networks with providers. Indeed, the majority of NDPP sites participating in a recent CDC-led evaluation (70.1%) were found to use provider referrals for recruitment,14 and there are ongoing on efforts to support systematic linkages between clinical providers and community-based NDPPs (e.g., a study funded by the Agency for Healthcare Research and Quality; R18HS026172).
Addressing Disparities in Reach
A challenge is that men and younger individuals are under-represented in the NDPP, and additional participation gaps exist for priority populations. In a 2019 CDC report, only 24.7% of NDPP participants were men,10 despite their higher prevalence of prediabetes compared to women (37.4% vs. 29.2%).1 There may also be a missed opportunity for lifelong diabetes prevention among the 28.7 million US adults under age 45 with prediabetes,1 as the average age of participants is 55.1.3 Another challenge is high initial “no shows” among enrollees overall (25–60%),21–23 which appear higher yet for racial/ethnic minority, low-income, and younger participants. Specifically, Latino enrollees were half as likely to initially attend as compared to non-Hispanic white enrollees,21 and women <40 years were about a quarter as likely to attend as their older counterparts (men were not included in this study).22 Other data suggest lower show rates for Medicaid beneficiaries (69.6%) versus enrollees with other types of insurance (77.7%; no p-value reported).23 Low intervention uptake in these groups is likely related to previously identified factors including social support, transportation/costs, beliefs about illness and lifestyle change,24 as well as social and economic disadvantages.25 To increase reach, encouraging enrollment alongside a partner or family member may be beneficial, as likelihood of initial attendance was three-fold greater than with individual enrollment, which especially benefited men and Latinos (indicating potential to address their reach gaps).26 Qualitative studies have further suggested strategies including more education and motivational interventions at referral and/or enrollment, providing childcare and transportation, offering classes solely for similar target populations, and using a more flexible and interactive class format.27,28 In turn, more empirical work is needed to fully demonstrate the potential benefits of these and other strategies.
Effectiveness
Successes with Effective Implementation
The NDPP was closely based on successes demonstrated with the lifestyle arm of the DPP clinical trial, in which participants achieved 4.9% mean weight loss by the end of intervention through low-fat diet and increased physical activity.29 The NDPP similarly promotes ≥5% weight loss through lifestyle change to reduce risk.30 Reports show a promising 4.2% mean weight loss for in-person NDPP classes3 and 4.3% weight loss for virtual programs.31 These are impressive outcomes given delivery to the general population of adults with diabetes risks, in contrast to extensive eligibility criteria in the original DPP trial, including completion of a 3-week run-in to ensure compliance.32 Although incident type 2 diabetes has not yet been systematically examined as a program outcome, it is nonetheless encouraging that each kilogram of weight loss was associated with 16% decreased incidence among lifestyle intervention participants in the DPP trial,33 suggesting considerable benefit is likely.
Additional successes with NDPP implementation include evidence that adults age 65 and older have remarkable weight loss (e.g., 6.4% median weight loss after ≥6 months in the program3), consistent with the exceptional benefit observed for seniors in the DPP’s lifestyle arm,4 and important given high age-related risks.1 Further, while the DPP trial required elevated blood glucose at enrollment,32 individuals who qualify for the NDPP based on broader definitions of risk appear to have positive outcomes. Specifically, no significant differences in weight loss were observed for participating women with and without a history of gestational diabetes,34 or for participants who qualified based on a risk survey versus confirmed prediabetes and/or prior gestational diabetes.3 Moreover, the original DPP trial largely excluded women in their childbearing years,32 yet early evidence suggests that participating women who become pregnant appear to have favorable obstetric and neonatal outcomes.35 Together, these findings suggest that the NDPP’s broad eligibility criteria enable many individuals to benefit from intervention, and might even be leveraged to break the transgenerational disease cycle.36
Overcoming Challenges with Effective Implementation
Improving Outcomes for All
Nearly three-quarters of participants (71.7%) do not achieve the ≥5% weight loss goal according to a CDC report.10 Of further concern, disparately low weight loss is observed for women, younger adults, and racial/ethnic minority and low-income participants, who lose about half as much weight as their counterparts.3,21,37 Improving retention appears key overall to ensuring beneficial weight loss outcomes (e.g., each session attended is associated with 0.3% more weight loss).3 Yet median attendance is only 134 days, such that most participants complete less than half of the yearlong program.38 In many cases, greater attendance mitigates, or at least attenuates, weight loss disparities.10,21,22 Improved retention has been observed with a variety of implementation strategies, including delivering a motivational session before the NDPP begins (+100 days for “pre-session” attendees), attending with a partner (+35 days), provider referrals (+34 days), special population tailoring (e.g., culture- and gender-specific adaptions; +30 days), and non-monetary incentives (e.g., gym memberships; +28 days).14,26 Evidence for monetary incentives is mixed with no greater retention observed in a report comparing site-level strategies,14 while increased attendance was found specifically among Medicaid beneficiaries in another study, but without greater weight loss.39 Overall, it remains important to consider feasibility, cost, and utility of these strategies for specific settings and populations.
In addition to increasing reach, virtually-delivered programming also has potential to address barriers to retention given findings that 61% of enrollees anticipated challenges attending in-person classes due to other responsibilities (e.g., work, school, dependent care) and 30% anticipated challenges with transportation.40 Yet, despite high rates of early engagement in online NDPPs, only 19% of participants attended for ≥9 months, and patterns of disparate weight loss outcomes among subgroups remained a concern.41 Thus, online delivery alone does not appear to resolve effectiveness challenges. Low retention rates in both in-person and online NDPPs likely affect reported outcomes, as data are typically examined for only those who attend a minimum number of sessions or have a minimum number of recorded weights, which often varies from one report to another (particularly as CDC standards for evaluating NDPP outcomes have been revised over time).3,10 Supplementing online interventions with in-person coaching was shown to improve weight loss (mean = 4.6%).31 A less resource-intensive approach of supplemental text message support did not improve retention or weight loss in the in-person NDPP.42 Reducing the intervention to delivery via short text messages demonstrated high retention but also was insufficiently effective.43 Overall, further research appears needed, including to examine what specific virtual components are beneficial, and to what extent additional in-person or other “real” interaction with a lifestyle coach may yield optimal results. As of 2019, less than 1% of participants receive combined in-person and virtual delivery approaches,10 which may be an important area for future growth.
Opportunities to Modernize the NDPP
While achieving all lifestyle goals was associated with the greatest risk reduction in the DPP, few (17%) were able to do so.33 Evidence continues to confirm the majority of participants are unable to achieve the recommended lifestyle goals of the NDPP.10 Thus, an opportunity for improvement is updating the NDPP to ensure generalizability, while incorporating more current evidence. Otherwise, there is tremendous risk of many participants being “set up to fail,” which may contribute to learned helplessness44 and dissuade future behavior change attempts. Dietary guidance merits reconsideration as achieving ≤25% of calories from fat appeared to be the least protective DPP goal. For example, achieving the low-fat dietary goal, on top of physical activity and weight loss goals, appeared to add minimal or even reduced benefit in terms of resulting diabetes incidence.33 Although the newest CDC-published curriculum (Prevent T2)45 relaxes the dietary goal to ≤30% of calories from fat without required dietary monitoring, the NDPP continues to promote a low-fat diet that nutrition science has generally evolved away from.46 Newer evidence suggests that various eating plans reduce risk and individualization is needed.47 An inflexible physical activity goal may also inadvertently deter retention, as NDPP participants were 25% less likely to return after not meeting the current goal of ≥150 weekly minutes in a prior session.48 Weight loss was the most protective goal in the DPP lifestyle intervention,33 but regain begins even during intervention,49 and much is regained over time,5,6 which is likely problematic. Moreover, despite aiming to prevent diabetes, glycemia is minimally addressed in CDC-published NDPP curricula.45
Incorporating a Health at Every Size (HAES) approach50 may allow a more flexible focus on long-term risk reduction (i.e., lowered glycemia) over temporary weight loss, with guidance on intuitive eating (i.e., eating in response to internal cues without a prescribed diet) and reframing physical activity as a tool for well-being. HAES-aligned interventions have shown better retention than traditional weight loss interventions,51 which may have important implications for the NDPP. This approach would also likely benefit participants with binge eating behavior,52 reported by nearly 10% of the DPP sample.53 Adding quarterly monitoring of glycated hemoglobin (A1C) using point-of-care instruments54 could enable sites to meaningfully incorporate glycemia testing into their NDPP delivery, or participants could seek laboratory testing. At least annual testing is recommended to detect diabetes onset among individuals with prediabetes,55 which would help evaluate the NDPP, although more frequent testing could be used for biofeedback during the yearlong program. Continuous glucose monitoring could also be considered as a newer technology to inform risk reduction behavior, but is relatively costly,56 and not likely covered by insurance for this purpose. Additionally, there is substantial evidence for metformin to reduce risk, including as an adjunct treatment to lifestyle intervention, yet it is infrequently adopted in real-world practice to prevent diabetes57 and unaddressed in the current NDPP curricula.45 Participants could be advised to discuss metformin with their providers upon joining the NDPP, which may be especially important to ensure continued treatment for the many individuals unable to complete the program. Overall, encouraging participants to adopt a range of preferred behaviors and treatment strategies that lower glycemia on an individual basis may be more beneficial, patient-centered, and better align with precision medicine initiatives58 than a one-size-fits-all approach.
Sustainability
Successes with Payer Coverage
Long-term sustainability of the NDPP is likely dependent on payer coverage as initial dissemination appears largely supported by time-limited grant funding. Payer coverage was established as an early priority and has required a remarkable collaboration of government, academic, community, healthcare, and payer sectors.9 For example, United Health Group was collaborating by 2009 to demonstrate payer involvement with an early translation of the NDPP in community settings of the Young Men’s Christian Association.59 Subsequently, nearly 50 insurers began to cover NDPP services by 2016.14 Notably, Medicare coverage began in April 2018,60 offering unprecedented opportunity to prevent diabetes among the estimated 46.6% of seniors with prediabetes.1 The adapted Medicare-covered model, the Medicare Diabetes Prevention Program (MDPP), is near-identical to the in-person NDPP. Additionally, the MDPP provides a second year of services beyond the one-year NDPP model disseminated by the CDC, offering an enhanced opportunity to support weight loss maintenance.60,61 In turn, Medicare coverage has tremendous potential to further bolster private payer coverage by setting industry standards, and ensure expanded Medicaid coverage that has become available for 11 states as of January 2020).62 A common feature of these coverage models is requiring adherence to CDC-established standards for NDPP delivery.60,62
Ensuring payer coverage is facilitated by strong return on investment (ROI) findings. Early projections suggested that providing the NDPP could yield 5.7 billion USD in savings over 25 years.63 More current estimates of future healthcare cost savings have continued to demonstrate that the NDPP is a high-value service.64–66 For a commercially-insured population, 3-year ROI was up to 42% based on maximum net savings of 35,037 USD.66 For Medicare beneficiaries, a 2017 report calculated an average reduction in Medicare Part A and B expenditures of 278 USD per quarter, or 1112 USD per member per year, over the 3 years following NDPP enrollment relative to a comparison group of beneficiaries. Cost-effectiveness has also been demonstrated in a Medicaid beneficiary population, particularly if considering a time horizon greater than 10 years.67
Overcoming Challenges with Payer Coverage
Addressing Low Payment Rates
Pay-for-performance reimbursement rates appear insufficient relative to reported costs, limiting sustainability. For a private payer example, cost of delivering an early version of the in-person NDPP appeared to range from 275–425 USD per participant68 with average reimbursement of 212 USD,59 leaving a gap of 63–213 USD. With Medicare, reported delivery costs (for first-year, in-person services) were 553–800 USD with average reimbursement of only 108–190 per participant,69,70 resulting in a gap of 363–792 USD. Medicaid reimbursement rates tend to be comparably low, producing an especially wide gap. For example, costs for in-person NDPP delivery to Minnesota Medicaid beneficiaries was 767–915 USD per participant,67 with estimated average reimbursement of 163 USD (based on 13.62 USD reimbursed per session71 and 12 sessions attended on average),67 producing a large gap of 604–752 USD to suppliers for each beneficiary they serve. How or why low payment rates came to be established is unclear, especially given compelling evidence for ROI, yet they are likely detrimental to achieving a sufficient number of suppliers relative to the need. Although low reimbursement rates benefit third-party payers in the short-term,72 they are likely to miss opportunity for substantial long-term savings from reduced diabetes prevalence. More evidence also appears needed to assess the sustainability of virtual NDPP delivery. Costs for online programming are generally not reported (possibly for proprietary protections in for-profit business models), but were found to be about one-third of in-person delivery costs in one evaluation yet still produced an unsustainable gap after reimbursement of 206 USD per participant.73
Addressing Limited Suppliers
Insufficient reimbursement relative to costs may be a deterrent to maintaining and growing NDPP access. Half of suppliers who previously offered the NDPP appear to have since extinguished their services. Over 3000 organizations provided the NDPP between 2012–2019,10 whereas only half remain in 2020.7 Regarding Medicare suppliers, a report found relatively few locations where beneficiaries could receive services over a year after coverage began, with only 1 site per 100,000 beneficiaries on average.74 Specifically, 75% of US states/territories had no MDPP sites, <1 site per 100,000 beneficiaries, and/or availability limited to a single municipality. Another concern is that suppliers may be dissuaded from entering markets with especially high-risk populations who are less likely to achieve performance payment milestones.69,75 In fact, severe shortages of MDPP sites were observed in states/territories with largest populations of racial/ethnic minority beneficiaries,74 continuing patterns observed with NDPP availability.11 While it is encouraging that MDPP suppliers since appear to be increasing,76 the overall downward trend in NDPP sites may be further problematic. Although value-based care is important, increased rates and risk-adjusted payment models appear needed to attract more suppliers. Expanded coverage of virtually-delivered programs may also help.
Conclusion
Over the past decade, the CDC has successfully led the translation of an efficacious lifestyle intervention into a nationwide program reaching hundreds of thousands of individuals at risk for type 2 diabetes, with notable effectiveness upon full participation and widespread insurance coverage. Nonetheless, working to overcome challenges in reach, effectiveness, and sustainability of the NDPP appears needed to achieve substantial public health impact, as summarized in Table 1. These challenges will likely demand continued collaboration of cross-sector stakeholders that enabled successes to date,9 which can be difficult given differing priorities at times.72 There is particular urgency to capitalize on the incredible growth of NDPP dissemination before critical momentum is lost. For example, Medicare coverage of the NDPP remains under the umbrella of the Centers for Medicare and Medicaid Services Innovation Center, and coverage may be discontinued if the model is unsuccessful. Resolving low reimbursement rates may be an especially critical factor, such that market forces can in turn drive improved reach and effectiveness. The NDPP must be withstanding in the years to come, as having enormous resources again dedicated to scaling the next promising intervention in the US is otherwise unlikely, such that NDPP is a must-succeed effort both to prevent diabetes and forge a path for future public health initiatives.
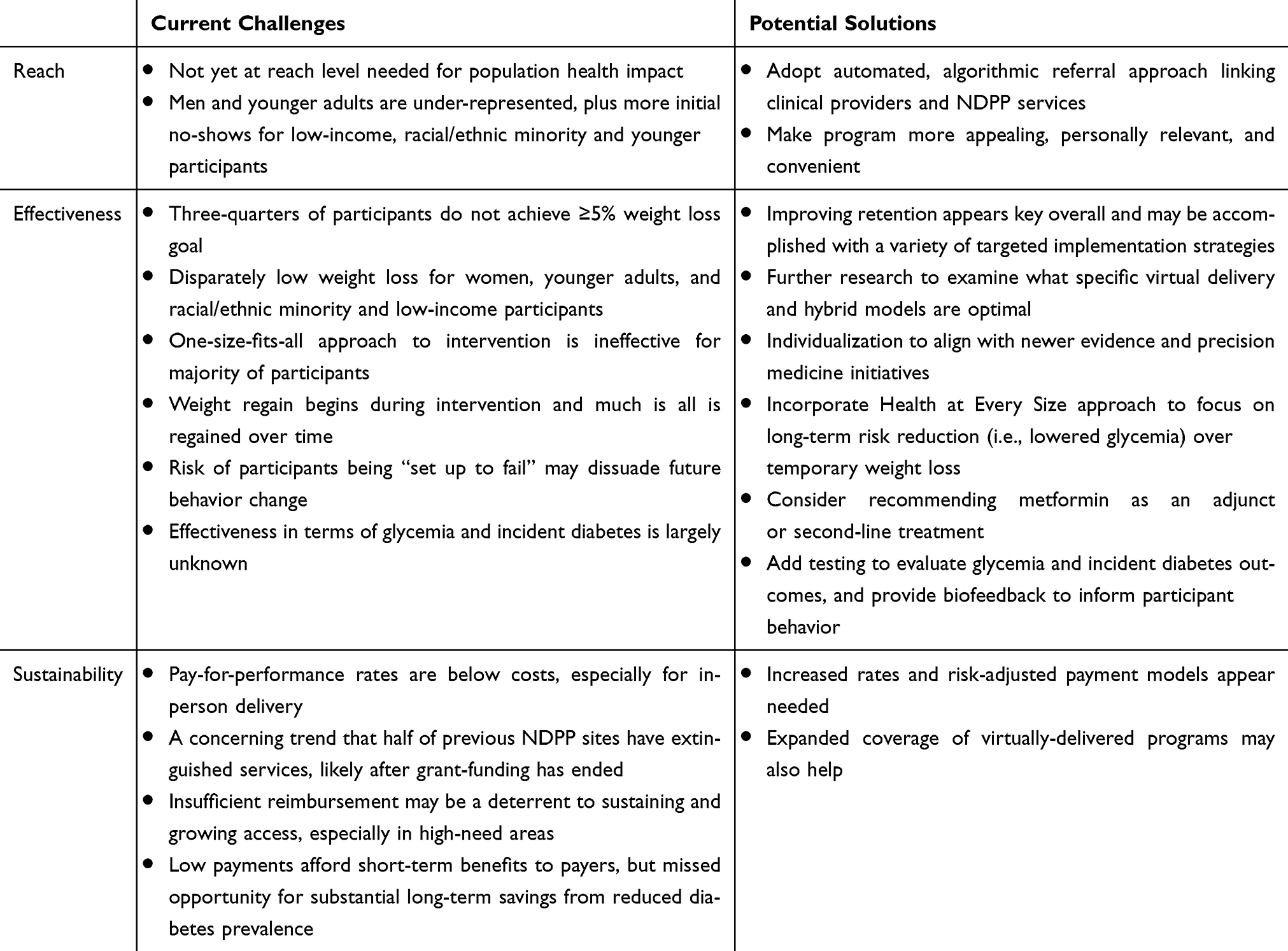 |
Table 1 Overview of Suggested Strategies to Build on Successes and Overcome Challenges to Impact of the National Diabetes Prevention Program |
Disclosure
NDR has received past and present grant support from the Centers for Disease Control and Prevention for work related to the National Diabetes Prevention Program, and grants from National Institutes of Health, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. CDC. National Diabetes Statistics Report, 2020: Estimates of Diabetes and Its Burden in the United States. Atlanta:GA: US Department of Health and Human Services; 2020.
2. Albright AL, Gregg EW. Preventing type 2 diabetes in communities across the U.S.: the national diabetes prevention program. Am J Prev Med. 2013;44(4 Suppl 4):S346–351. doi:10.1016/j.amepre.2012.12.009
3. Ely EK, Gruss SM, Luman ET, et al. A national effort to prevent type 2 diabetes: participant-level evaluation of CDC’s national diabetes prevention program. Diab Care. 2017;40:1331–1341. doi:10.2337/dc16-2099
4. Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6):393–403.
5. Knowler WC, Fowler SE, Hamman RF, et al. 10-year follow-up of diabetes incidence and weight loss in the diabetes prevention program outcomes study. Lancet. 2009;374(9702):1677–1686.
6. Diabetes Prevention Program Research Group. Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: the diabetes prevention program outcomes study. Lancet Diab Endocrinol. 2015;3(11):866–875. doi:10.1016/S2213-8587(15)00291-0
7. CDC. Diabetes prevention recognition program registry of recognized organizations. Available from: https://nccd.cdc.gov/DDT_DPRP/Registry.aspx.
8. CDC. Diabetes prevention recognition program: standards and operating procedures; 2018. Available from: https://www.cdc.gov/diabetes/prevention/pdf/dprp-standards.pdf.
9. Burd C, Gruss S, Albright A, Zina A, Schumacher P, Alley D. Translating knowledge into action to prevent type 2 diabetes: medicare expansion of the national diabetes prevention program lifestyle intervention. Milbank Q. 2020;98(1):172–196. doi:10.1111/1468-0009.12443
10. Gruss SM, Nhim K, Gregg E, Bell M, Luman E, Albright A. Public health approaches to type 2 diabetes prevention: the US national diabetes prevention program and beyond. Curr Diab Rep. 2019;19(9):78. doi:10.1007/s11892-019-1200-z
11. Jayapaul-Philip B, Dai S, Kirtland K, Haslam A, Nhim K. Availability of the national diabetes prevention program in united states counties, March 2017. Prev Chronic Dis. 2018;15:E109. doi:10.5888/pcd15.180063
12. Ariel-Donges AH, Gordon EL, Dixon BN, et al. Rural/urban disparities in access to the national diabetes prevention program. Transl Behav Med. 2019. doi:10.1093/tbm/ibz098
13. Kirkman MS, Tuncer D, Brown CE. Findings from a national diabetes survey: highlighting progress and opportunities for diabetes prevention and care. Diabetes Spectr. 2019;32(3):277–283. doi:10.2337/ds18-0086
14. Nhim K, Gruss SM, Porterfield DS, et al. Using a RE-AIM framework to identify promising practices in national diabetes prevention program implementation. Impl Sci. 2019;14(1):81. doi:10.1186/s13012-019-0928-9
15. Sinclair-White B, Nett B, Ilagan L, et al. Insights in public health: development, implementation, and evaluation of the prevent diabetes, Hawai’i Campaign. Hawaii J Health Soc Welf. 2020;79(3):86–90.
16. Holliday CS, Williams J, Salcedo V, Kandula NR. Clinical identification and referral of adults with prediabetes to a diabetes prevention program. Prev Chronic Dis. 2019;16:E82. doi:10.5888/pcd16.180540
17. Ritchie N, Swigert T. Establishing an effective primary care provider referral network for the national diabetes prevention program. AADE Practice. 2016;4(4):20–25. doi:10.1177/2325160316647707
18. Siu A, on behalf of the U.S. Preventive Services Task Force. Screening for abnormal blood glucose and type 2 diabetes mellitus: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2015; doi:10.7326/M15-2345.
19. Bowen ME, Schmittdiel JA, Kullgren JT, Ackermann RT, O’Brien MJ. Building toward a population-based approach to diabetes screening and prevention for US adults. Curr Diab Rep. 2018;18(11):104. doi:10.1007/s11892-018-1090-5
20. Nhim K, Khan T, Gruss SM, et al. Primary care providers’ prediabetes screening, testing, and referral behaviors. Am J Prev Med. 2018;55(2):e39e47. doi:10.1016/j.amepre.2018.04.017
21. Ritchie ND, Christoe-Frazier L, McFann KK, Havranek EP, Pereira RI. Effect of the national diabetes prevention program on weight loss for english- and spanish-speaking latinos. Am J Health Promot. 2018;32(3):812–815. doi:10.1177/0890117117698623
22. Ritchie ND, Sauder KA, Fabbri S. Reach and effectiveness of the national diabetes prevention program for young women. Am J Prev Med. 2017;53(5):714–718. doi:10.1016/j.amepre.2017.06.013
23. Chambers EC, Gonzalez JS, Marquez ME, Parsons A, Rehm CD. The reach of an urban hospital system-based diabetes prevention program: patient engagement and weight loss characteristics. Diabetes Educ. 2019;45(6):616–628. doi:10.1177/0145721719880503
24. Murray J, Craigs CL, Hill KM, Honey S, House A. A systematic review of patient reported factors associated with uptake and completion of cardiovascular lifestyle behaviour change. BMC Cardiovasc Disord. 2012;12:120. doi:10.1186/1471-2261-12-120
25. Braveman P. What are health disparities and health equity? We need to be clear. Public Health Rep. 2014;129(Suppl 2):5–8. doi:10.1177/00333549141291S203
26. Ritchie ND, Baucom KJW, Sauder KA. Benefits of participating with a partner in the national diabetes prevention program. Diab Care. 2020;43(2):e20e21. doi:10.2337/dc19-1489
27. Harrison CR, Phimphasone-Brady P, DiOrio B,et al. Barriers and Facilitators of National Diabetes Prevention Program Engagement Among Women of Childbearing Age: A Qualitative Study. Diabetes Educ. 2020;46(3):279-88. doi:10.1177/0145721720920252
28. Realmuto L, Kamler A, Weiss L, et al. Power up for health-participants’ perspectives on an adaptation of the national diabetes prevention program to engage men. Am J Mens Health. 2018;12(4):981–988. doi:10.1177/1557988318758786
29. Wing RR, Hamman RF, Bray GA, et al. Achieving weight and activity goals among diabetes prevention program lifestyle participants. Obes Res. 2004;12(9):1426–1434.
30. Centers for Disease Control and Prevention. CDC diabetes prevention recognition program standards and operating procedures; 2018. Available from: https://www.cdc.gov/diabetes/prevention/pdf/dprp-standards.pdf.
31. Joiner KL, Nam S, Whittemore R. Lifestyle interventions based on the diabetes prevention program delivered via eHealth: a systematic review and meta-analysis. Prev Med. 2017;100:194–207. doi:10.1016/j.ypmed.2017.04.033
32. The Diabetes Prevention Program. Design and methods for a clinical trial in the prevention of type 2 diabetes. Diab Care. 1999;22(4):623–634. doi:10.2337/diacare.22.4.623
33. Hamman RF, Wing RR, Edelstein SL, et al. Effect of weight loss with lifestyle intervention on risk of diabetes. Diab Care. 2006;29(9):2102–2107. doi:10.2337/dc06-0560
34. Brokaw SM, Carpenedo D, Campbell P, et al. Does a history of gestational diabetes mellitus affect key outcomes in women participating in a diabetes prevention program? Matern Child Health J. 2018;22(4):529–537. doi:10.1007/s10995-017-2420-y
35. Ritchie ND, Fabbri S, Sauder KA. Case reports on diabetes-related outcomes for pregnant women in the national diabetes prevention program. Clin Diab. 2019;37(4):395–397. doi:10.2337/cd18-0104
36. Dabelea D, Crume T. Maternal environment and the transgenerational cycle of obesity and diabetes. Diabetes. 2011;60(7):1849–1855. doi:10.2337/db11-0400
37. Ritchie ND, Sauder KA, Phimphasone-Brady P, Amura CR. Rethinking the national diabetes prevention program for low-income whites. Diab Care. 2018;41(4):e56e57. doi:10.2337/dc17-2230
38. Easterbrook PJ, Berlin JA, Gopalan R, Matthews DR. Publication bias in clinical research. Lancet. 1991;337(8746):867–872. doi:10.1016/0140-6736(91)90201-Y
39. VanEpps EM, Troxel AB, Villamil E, et al. Effect of process- and outcome-based financial incentives on weight loss among prediabetic new york medicaid patients: a randomized clinical trial. Am j Health Promotion. 2019;33(3):372–380. doi:10.1177/0890117118783594
40. Ritchie ND, Phimphasone-Brady P, Sauder KA, Amura CR. Perceived barriers and potential solutions to engagement in the National Diabetes Prevention Program ADCES in Practice. In press.
41. Sauder KA, Ritchie ND, Crowe B, Cox E, Hudson M, Wadhwa S. Participation and weight loss in online national diabetes prevention programs: a comparison of age and gender subgroups. Transl Behav Med. 2020. doi:10.1093/tbm/ibaa048
42. Ritchie ND, Raghunath SG, Durfee MJ, Fischer H. Supplemental Text Message Support with the National Diabetes Prevention Program: A Pragmatic Comparative Effectiveness Trial. JMIR mHealth & uHealth. 2020 8(6):e15478. doi:10.2196/15478.
43. Fischer HH, Durfee MJ, Raghunath SG, Ritchie ND. Short message service text message support for weight loss in patients with prediabetes: pragmatic trial. JMIR Diab. 2019;4(2):e12985. doi:10.2196/12985
44. Seligman ME. Learned helplessness. Annu Rev Med. 1972;23:407–412. doi:10.1146/annurev.me.23.020172.002203
45. CDC. National diabetes prevention program. Available from: https://www.cdc.gov/diabetes/prevention/lifestyle-program/curriculum.html.
46. Mozaffarian D. Foods, nutrients, and health: when will our policies catch up with nutrition science? Lancet Diab Endocrinol. 2017;5(2):85–88. doi:10.1016/S2213-8587(16)30265-0
47. Evert AB, Dennison M, Gardner CD, et al. Nutrition therapy for adults with diabetes or prediabetes: a consensus report. Diab Care. 2019;42(5):731–754. doi:10.2337/dci19-0014
48. Ritchie ND, Carroll JK, Holtrop JS, Havranek EP. Effects of physical activity goal attainment on engagement and outcomes in the national diabetes prevention program. Transl Behav Med. 2018. doi:10.1093/tbm/ibx021
49. Sauder KA, Ritchie ND, Crowe B, Cox E, Hudson M, Wadhwa S. Participation and weight loss in online National Diabetes Prevention Programs: a comparison of age and gender subgroups. Trans Beh Med. 2020;ibaa048. doi:10.1093/tbm/ibaa048.
50. Bacon L, Stern JS, Van Loan MD, Keim NL. Size acceptance and intuitive eating improve health for obese, female chronic dieters. J Am Diet Assoc. 2005;105(6):929–936. doi:10.1016/j.jada.2005.03.011
51. Schaefer JT, Magnuson AB. A review of interventions that promote eating by internal cues. J Acad Nutr Diet. 2014;114(5):734–760. doi:10.1016/j.jand.2013.12.024
52. Alpizar J, Ritchie N. Addressing binge eating behavior in the national diabetes prevention program: practical strategies for lifestyle coaches. ADCES in Practice. In press.
53. Delahanty LM, Meigs JB, Hayden D, Williamson DA, Nathan DM. Diabetes Prevenion Program Research G. Psychological and behavioral correlates of baseline BMI in the diabetes prevention program (DPP). Diab Care. 2002;25(11):1992–1998. doi:10.2337/diacare.25.11.1992
54. Whitley HP, Yong EV, Rasinen C. Selecting an A1C point-of-care instrument. Diabetes Spectr. 2015;28(3):201–208. doi:10.2337/diaspect.28.3.201
55. American Diabetes A. 3. prevention or delay of type 2 diabetes: standards of medical care in diabetes-2020. Diab Care. 2020;43(Suppl 1):S32S36.
56. Fonda SJ, Graham C, Munakata J, Powers JM, Price D, Vigersky RA. The cost-effectiveness of real-time continuous glucose monitoring (RT-CGM) in type 2 diabetes. J Diabetes Sci Technol. 2016;10(4):898–904. doi:10.1177/1932296816628547
57. Moin T, Schmittdiel JA, Flory JH, et al. Review of metformin use for type 2 diabetes prevention. Am J Prev Med. 2018;55(4):565–574. doi:10.1016/j.amepre.2018.04.038
58. Collins FS, Varmus H. A new initiative on precision medicine. N Engl J Med. 2015;372(9):793–795. doi:10.1056/NEJMp1500523
59. Ackermann RT, Kang R, Cooper AJ, et al. Effect on health care expenditures during nationwide implementation of the diabetes prevention program as a health insurance benefit. Diab Care. 2019;42(9):1776–1783. doi:10.2337/dc18-2071
60. Centers for Medicare & Medicaid Services (CMS) HHS. Medicare program; revisions to payment policies under the physician fee schedule and other revisions to part b for cy 2018; medicare shared savings program requirements; and medicare diabetes prevention program. final rule. Fed Regist. 2017;82(219):52976–53371.
61. CMS. Medicare program; revisions to payment policies under the physician fee schedule and other revisions to part b for cy 2018; medicare shared savings program requirements; and medicare diabetes prevention program; 2017. Available from: https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-07-07.html.
62. National diabetes prevention program coverage toolkit participating payers; 2017. Available from: https://coveragetoolkit.org/participating-payers.
63. Zhuo X, Zhang P, Gregg EW, et al. A nationwide community-based lifestyle program could delay or prevent type 2 diabetes cases and save $5.7 billion in 25 years. Health Affairs. 2012;31(1):50–60. doi:10.1377/hlthaff.2011.1115
64. Alva ML, Hoerger TJ, Jeyaraman R, Amico P, Rojas-Smith L. Impact of the ymca of the usa diabetes prevention program on medicare spending and utilization. Health Affairs. 2017;36(3):417–424. doi:10.1377/hlthaff.2016.1307
65. Alva ML. How much does attendance impact weight loss and health care spending in a diabetes prevention program serving older adults? Am j Health Promotion. 2019;33(7):1067–1072. doi:10.1177/0890117119848985
66. Khan T, Tsipas S, Wozniak G. Medical care expenditures for individuals with prediabetes: the potential cost savings in reducing the risk of developing diabetes. Popul Health Manag. 2017;20(5):389–396. doi:10.1089/pop.2016.0134
67. Gilmer T, O’Connor PJ, Schiff JS, et al. Cost-effectiveness of a community-based diabetes prevention program with participation incentives for medicaid beneficiaries. Health Serv Res. 2018;53(6):4704–4724. doi:10.1111/1475-6773.12973
68. Ackermann RT, Marrero DG. Adapting the diabetes prevention program lifestyle intervention for delivery in the community: the YMCA model. Diabetes Educ. 2007;33(1):
69. Ritchie ND, Gritz RM. New medicare diabetes prevention coverage may limit beneficiary access and widen health disparities. Med Care. 2018;56(11):908–911. doi:10.1097/MLR.0000000000000981
70. Parsons AS, Raman V, Starr B, Zezza M, Rehm CD. Medicare underpayment for diabetes prevention Program: implications for DPP suppliers. Am J Manag Care. 2018;24(10):475–478.
71. National diabetes prevention program coverage toolkit - reimbursement models for medicaid agencies and mcos; 2020. Available from: https://coveragetoolkit.org/medicaid-mco-reimbursement/.
72. Ackermann RT, O’Brien MJ. Evidence and challenges for translation and population impact of the diabetes prevention program. Curr Diab Rep. 2020;20(3):9. doi:10.1007/s11892-020-1293-4
73. RTI I Evaluation of the medicaid coverage for the national diabetes prevention program demonstration project final report [executive summary]; 2018. Available from: https://cdn.ymaws.com/www.chronicdisease.org/resource/resmgr/diabetes_dpp_materials/medicaid_demonstration_proje.pdf.
74. Ritchie ND, Sauder KA, Gritz RM. Medicare Diabetes Prevention Program: Where are the Suppliers? Am J Man Care. 2020; 26(6):294-e297.doi:10.37765/ajmc.2020.43496.
75. Ritchie ND, Havranek EP, Moore SL, Pereira RI. Proposed medicare coverage for diabetes prevention: strengths, limitations, and recommendations for improvement. Am J Prev Med. 2017;53(2):260–263. doi:10.1016/j.amepre.2017.02.005
76. CMS. Medicare diabetes prevention program. Available from: https://data.cms.gov/Special-Programs-Initiatives/Medicare-Diabetes-Prevention-Program/vwz3-d6x2/data.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.