")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 13
Current Knowledge of Vaccinations in Chronic Kidney Disease Patients
Authors Haddiya I
Received 16 September 2019
Accepted for publication 3 July 2020
Published 27 July 2020 Volume 2020:13 Pages 179—185
DOI https://doi.org/10.2147/IJNRD.S231142
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Intissar Haddiya
Department of Nephrology, Laboratory of Epidemiology, Clinical Research and Public Health, Faculty of Medicine and Pharmacy of Oujda, University Mohamed Premier, Oujda, Morocco
Correspondence: Intissar Haddiya Department of Nephrology
Laboratory of Epidemiology, Clinical Research and Public Health, Faculty of Medicine and Pharmacy of Oujda, University Mohamed Premier, 12, Avenue Al Ouafae, Hay AlHikma, Oujda 60050, Morocco
Tel +212 661 281400
Email [email protected]
Abstract: Chronic kidney disease (CKD) patients are at high risk for infectious complications. This is partly due to their dysfunctional immune system, especially in advanced CKD stages. Vaccination represents an important prevention strategy in these patients, as several studies have reported lower infection rates and significantly reduced morbidity and mortality in hospitals adopting vaccination protocols. However, vaccination rates are particularly low in these patients, and the diminished immune responsiveness remains the main issue of vaccination in CKD patients. Besides, there are various immunization protocols across the world in the absence of optimal vaccination policies. This paper aims to discuss the current knowledge of vaccination in this immunocompromised group of patients based on recent evidence and recommendations.
Keywords: immunizations, vaccines, immune system, chronic kidney disease, dialysis, kidney transplant
Introduction
Infections are recognized as the most common cause of hospitalization and mortality in end-stage renal disease (ESRD) patients, particularly in hemodialysis (HD) patients, after cardiovascular disease.1 In fact, the incidence of the common infections (urinary tract infections (UTIs), pneumonia, sepsis) is three times greater among CKD patients who have not yet initiated dialysis than in the general population, whereas, dialysis patients have higher annual mortality rates caused by sepsis compared with the general population.2 Yet, several publications have reported lesser infection rates and therefore decreased morbidity and mortality in hospitals adopting vaccination regimen in CKD and ESRD patients.1–3 But, these patients, regardless of their initial nephropathy or comorbidities, are less efficiently immunized than the general population.4 In fact, the particularly dysfunctional immune system of the late-stage chronic kidney disease (CKD) patients, with impaired innate and adaptative immunity, is partly responsible for an increased susceptibility to infection as well as low response to vaccines.3,4 On one hand, these data suggest that expanding vaccination strategies would diminish infections-related burden and probably improve patients' well-being and survival. However, vaccination practices in these patients are often hindered by the reduced efficacy of the established protocols, the frequent need of booster doses as well as safety issues in renal transplant recipients.5,6 Therefore, various guidelines were developed to improve the care and diminish morbidity and mortality in this high-risk group of patients. This paper aims to discuss the current knowledge of vaccination in these immunocompromised patients based on recent evidence and recommendations.
Impaired Immune Response in CKD Patients
The chronic decline of kidney function entails abnormalities in both innate and adaptive immunity. As a result, CKD patients are at high risk for infections and experience reduced vaccine effectiveness. In fact, B lymphocyte and CD4+ T lymphocyte are decreased in this population as well as the T-cell response to antigenic stimuli. Moreover, impaired monocyte functioning results in inadequate antigen presentation to the antigen-presenting cells, generating weakened memory cells and inadequate antibody production after vaccination. These disturbances are mostly noted in CKD stages 4 and 5. Additionally, CKD patients are known to have impaired function of neutrophils, with a lower capacity of phagocytosis and a greater rate of apoptosis although their number remains unchanged.7–12
In addition, the underlying mechanisms of the impaired immune system in CKD are multifactorial. Several studies have discussed the potential link between endothelial dysfunction and impaired immune function.13–15 CKD patients have higher levels of endothelial dysfunction markers compared to controls.16,17
Besides, uremic toxins, oxidative stress, endothelial dysfunction, low-grade inflammation as well as mineral and bone disorders are involved and may contribute to the impaired immune system in these patients.8
Vaccination in CKD: General Considerations
One of the difficulties in immunization of CKD patients is the lack of an optimal policy, as there are variations in immunization for CKD between countries, mainly due to epidemiological priorities.1,2
In fact, the Centers for Disease Control and Prevention (CDC) guidelines for vaccination in CKD summarized in the Recommendations of the Advisory Committee on Immunization Practices (ACIP) recommend for all adults the diphtheria/tetanus, the annual inactivated influenza vaccine, the measles/mumps/rubella (MMR), and the varicella vaccine if not contraindicated. In CKD and dialysis, it adds the hepatitis B vaccine in adapted dose as well as the pneumococcal vaccine.18
Besides, here are some fundamental considerations for vaccination practices:1–3,18–20
- Early-stage CKD patients can be safely vaccinated as they have mild immune impairment and ESRD patients should not be excluded from routine vaccination with Live-attenuated vaccines (LAV).
- The immune status of transplant candidates must be assessed, and complete appropriate vaccination must be performed in the pretransplant period at least 4 weeks prior to kidney transplantation. Noteworthy that LAVs are contraindicated in kidney transplant recipients.
Moreover, KDIGO recommend the following guidelines in CKD patients:20
- Annual influenza vaccination in adults with CKD, unless contraindicated.
- Vaccination with polyvalent pneumococcus vaccine every 5 years unless contraindicated in CKD stages 4 and 5 and patients at high risk of pneumococcal infection (nephrotic syndrome, diabetes, or those undergoing immunosuppression).
Immunization against hepatitis B in adults with a progressive CKD and have GFR <30 mL/min/1.73 m2. The response should be evaluated by an appropriate serological testing.
Furthermore, American guidelines of vaccination in adult solid organ transplantation updated by the American Society of Transplantation (AST) and the Infectious Disease Society of America in 2013 recommend that vaccination status should be documented during pre-transplant workup and necessary immunizations must be administered as soon as possible afterwards.3,18-20
Recommended Vaccines for Adult CKD Patients
The recommended vaccines for adult CKD patients are summarized in Table 1.
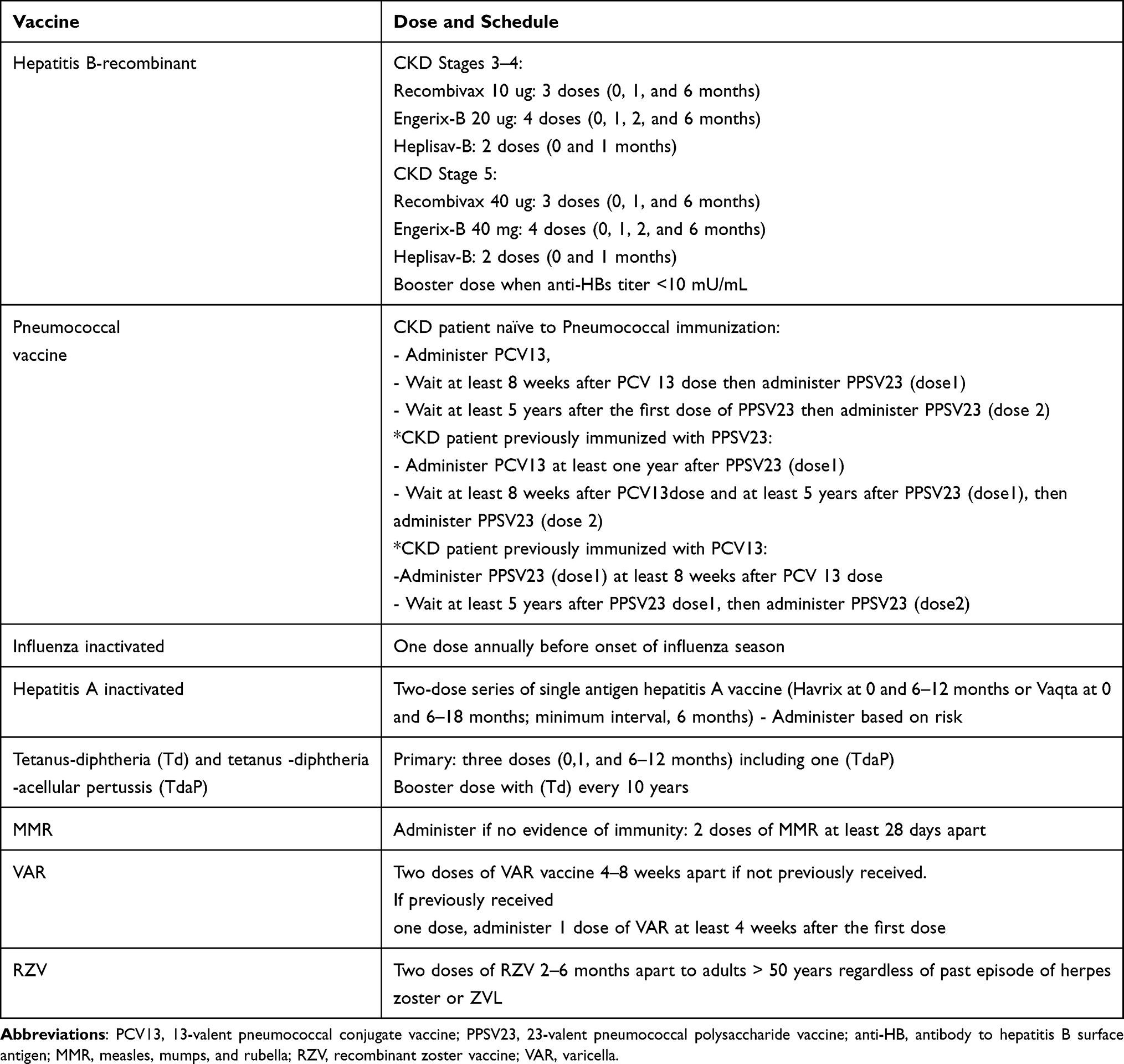 |
Table 1 Recommended Vaccines for Adults with CKD |
Hepatitis B
Hemodialysis patients have an elevated risk of Hepatitis B (HBV) transmission (percutaneous or blood/mucosal exposure) via contaminated surfaces and objects. HBV is very contaminant and persists on environmental surfaces for at least 7 days. Besides, patients with chronic HBV infection are at high risk for cirrhosis and liver cancer.1–21
Due to their dysfunctional immune system, infected dialysis patients are likely to become chronic carriers.1–20,22 Therefore, increasing transmission risk in dialysis units.22 During the last years, the incidence of HBV infection in HD patients has diminished since the introduction of erythropoiesis-stimulating agents (ESA), the improvement in controls of the blood products for the HBV, the introduction of hepatitis B vaccination programs, additional adherence to rigorous universal precautions to control infection, and regular screening for hepatitis B in dialysis units.1,3,23
As early vaccination is correlated with better seroconversion rates, HBV vaccination is recommended as early in the course of their CKD as possible.24 In fact, Stage 5 CKD patients present lower seroconversion rates and HBV-antibody responses are less effective and less lasting.23
However, there is heterogeneity in practices for the prevention of HBV infection across the world. Firstly, the adequacy of the immune response to hepatitis B vaccination measured by the titer of antibody to hepatitis B surface antigen (anti-HBs) after 3 doses of vaccine at 0-, 1-, and 6-month intervals differs between North America (>10 U/L) and Europe (>100 U/L) according to a Cochrane review.3,25,26
As first-generation plasma-derived hepatitis B vaccines were generally ineffective, recombinant yeast-derived second-generation vaccines have progressively replaced them, in order to improve seroconversion rates.3 Currently, commonly used commercial brands are Recombivax and Engerix-B.1
Several studies have compared the intradermal (ID) route to the intramuscular (IM) one. A meta-analysis demonstrated that the ID route was more efficient, and revealed a significantly higher percentage of patients achieving seroconversion in the ID group versus the IM group.15,27,28
ESRD patients as well as those undergoing HD require higher vaccine doses to increase seroresponsiveness.26–29 Currently, recommendations for adults on dialysis are either 40 mg of Recombivax administered at 0.1 and 6 months or Engerix-B administered at 0, 1, 2 and 6 months.1,3,25-30
HBV-antibody titer should be assessed 1 to 2 months after the final dose.30,31 If the latter is <10 mIU/mL, repeating the entire dosing series is suggested with an evaluation of the antibody response in 1 to 4 months. For patients on HD, the need for booster doses should be guided by annual testing of the anti-HB levels.31–34 A European Consensus group on hepatitis B immunity recommends for immunocompromised patients a regular testing for anti- HBs, and a single booster dose when the titer is inferior to 10 mIU/mL.3,30-34
Influenza and Pneumococcal Vaccines
Influenza Vaccine
Over the years, epidemics of influenza have caused thousands of deaths, and ESRD patients are likely to present complicated forms of influenza due to their disturbed immune system. Nonetheless, vaccinations have clear benefits in this vulnerable group.35
In fact, annual vaccination with the seasonal influenza vaccine for all patients with chronic medical conditions including the dialysis patients is highly recommended as vaccinated ESRD patients had significantly lower infection-related hospitalization and mortality rates. Ideally, vaccination should occur throughout the influenza season prior to the outbreak of the influenza activity.33,35-38
Quadrivalent influenza vaccine may be coadministered with pneumococcal vaccines. Besides, in patients aged > 65 years, a high-dose trivalent vaccine may be used.33,36 Optimal Influenza vaccine schedules in ESRD patients lack because of the nonavailability of large, prospective randomized studies.33,37,38 Whereas, in practice, seasonal inactivated influenza vaccine is strongly recommended on an annual basis, and the CDC recommends a 0.5 mL dose of inactivated influenza vaccination for all patients with kidney dysfunction and close contacts including, physicians, nurses, and personnel in the hospital.1,3,37,38,39
All types of influenza vaccines have a significantly reduced effect 7 months after the vaccination. A booster dose of the vaccine is not recommended as it is ineffective and thus unnecessary according to a number of studies.40,41
Noteworthy, that live-attenuated influenza vaccine is contraindicated in high-risk conditions such as kidney transplant recipients and has not been tested in CKD, ESRD, or in organ transplantation.3,33,36–38
Pneumococcal Vaccine
Due to their weak immune protection, CKD patients, especially children with nephrotic syndrome and elderly on dialysis, are remarkably vulnerable to severe pneumococcal infection.3 In fact, dialysis patients have a high incidence of respiratory infections with mortality rates up to 16-fold higher compared to the general population. Moreover, community-acquired pneumonia in both dialysis patients and kidney transplant recipients is mainly caused by Streptococcus pneumonia.42
Currently, there are 2 different anti-pneumococcal vaccines:3
The 13-valent pneumococcal conjugate vaccine (PCV-13: Prevnar 13)
The 23-valent (PPV-23: Pneumovax 23)
The use of both pneumococcal vaccines might provide broader protection. Thus, PCV13 in combination with the PPSV23 vaccine has been included in the vaccination recommendations of immunocompromised individuals including CKD patients.43
From 2013 to 2014, according to American, Spanish and French guidelines, PCV-13 followed by a PPV-23, 6–12 months later is recommended for all adults ≥65 years old, and in congenital or acquired immune-deficient adults of ≥19 years with a booster dose of PPV-23 at least 5 years later. In PPV-23-vaccinated persons, PCV-13 should be administered at least 1 year after the PPV-23 dose. Additionally, coadministration with the inactivated influenza vaccine may have synergistic positive effects.44–47.
In practice, based on the current knowledge, IM vaccination is recommended in all ESRD patients with the PCV 13 vaccine and the PPSV23 at least 8 weeks later, then A booster dose of the PPSV23 is administered every 5 years.3
Tetanus-Diphtheria (Td) and Tetanus-Diphtheria-Acellular Pertussis Vaccines (TdaP)
An Iranian study on a group of HD patients found that only 16% and 24% of them were immune to diphtheria and tetanus, respectively, demonstrating therefore the particularly low seroprotection in these patients.48 Additionally, survey data report under vaccination against tetanus and diphtheria in adults48,49, whereas Maintaining seroprotection against these diseases through adherence to the ACIP-recommended vaccination schedule is important for adults of all ages.49
Regarding Pertussis, although vaccines induced protection declines over time, vaccination remains the best protection available against this disease.1
Therefore, three doses of the vaccine are recommended at (0,1, and 6–12 months) including One dose of TdaP (vaccine against Tetanus, Diphtheria and Pertussis) should be administered to adults who previously did not receive a dose as an adult or child, followed by a dose of tetanus and diphtheria toxoids (Td) booster every 10 years.1,48-50 In dialysis patients with open wounds, a tetanus toxoid booster should be administered if in doubt regarding the seroresponsiveness.2
Hepatitis A
Vaccination to hepatitis A virus (HAV) is not universally recommended,51 and infection with HAV usually provides lifelong immunity in most healthy adults while vaccination offers about 99% seroconversion.52
CKD and ESRD patients who should be considered for vaccination are those who travel or live in endemic areas, patients with chronic liver disease, hepatitis C or HIV, homosexual men, and intravenous drug users. These patients are particularly at high risk of HAV associated morbidity and mortality.52–54 Consequently, vaccination with 2 doses IM at 0 and 6–12 months is recommended in these patients.53
The Food and Drug Administration has licensed 2 inactivated vaccines, Harvix (GlaxoSmithKline) and Vaqta (Merck) offered in a 2-dose series.54 Studies on the safety and efficacy of HAV vaccine in patients with CKD are mitigated. The subcutaneous (SC) route is as effective as the IM route.52–55
Herpes Zoster Vaccine
Herpes zoster vaccine has been reported to decrease shingles and post-herpetic neuralgia.1 In many countries, ZLV, a live-attenuated vaccine, is still the only available vaccine for Herpes zoster, but, recently, a new Recombinant Zoster Vaccine (RZV), an adjuvant Herpes Zoster (HZ) vaccine, was approved for the prevention of HZ.2
Two doses of recombinant zoster vaccine 2 to 6 months apart are recommended in adults aged 50 years or older regardless of past episode of herpes zoster or receipt of zoster vaccine live.56
Indeed, given its better efficacy, RZV will certainly replace ZLV and therefore reduce the risk of HZ in vulnerable patients, including, those who are immunosuppressed.57
Measles, Mumps, and Rubella Vaccine (MMR) and Varicella Vaccine (VAR)
In fact, MMR and varicella serology should be assessed prior to transplantation and transplant candidates should be immunized. One or 2 doses of MMR and varicella should be done.58,59 If seroconversion does not occur, the dose can be repeated once, if time permits prior to transplantation.58 Additionally, two live vaccines, MMR and varicella for instance, can be both given on the same day; otherwise, the second live vaccine should be given > 28 days later.58
Conclusion
Currently, given the lack of large randomized trials, no optimal vaccination policy in CKD patients is available. In addition, there are differences in vaccination practices across the world, depending on the local epidemiological priorities. Besides, various strategies are used to enhance the vaccine-induced seroconversion rate in advanced CKD patients. Additional research is needed to improve rates of seroresponsiveness, as well as the morbidity and mortality due to infections. Yet, adherence to the available immunization recommendations is highly required in this group of immunocompromised patients.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Snigdha R, Chandrika C, Jerry Y. Vaccination in Chronic Kidney Disease. Adv Chronic Kidney Dis. 2019;26(1):72–78. doi:10.1053/j.ackd.2018.10.002
2. Naqvi SB, Collins AJ. Infectious complications in Chronic Kidney Disease. Adv Chronic Kidney Dis. 2006;13(3):199–204. doi:10.1053/j.ackd.2006.04.004
3. Kosmadakis G, Albaret J. Enrique Da Costa Correia, Frederic Somda, Didier Aguilera. Vaccination practices in dialysis patients: A narrative review. Semin Dial. 2018;1–12.
4. Lee Ventola C. Immunization in the United States: recommendations, barriers, and measures to improve compliance. part 2: adult vaccinations. Pharm Ther. 2016;41(8):
5. Annunziata K, Rak A, Del Buono H, et al. Vaccination rates among the general adult popula- tion and high-risk groups in the United States. PLoS One. 2012;7(11):e50553. doi:10.1371/journal.pone.0050553
6. Bitsori M, Galanakis E. Vaccine-preventable infection morbidity of patients with chronic kidney disease and cocoon cination strategies, expert review of vaccines. Expert Rev Vaccines. 2015;14(10):1385–1395. doi:10.1586/14760584.2015.1075397
7. Kato S, Chmielewski M, Honda H, et al. Aspects of immune dysfunction in end-stage renal disease. Clin J Am Soc Nephrol. 2008;3(5):1526–1533. doi:10.2215/CJN.00950208
8. Ishigami J, Matsushita K. Clinical epidemiology of infectious disease among patients with chronic kidney disease. Clin Exp Nephrol. 2019;23(4):437–447. doi:10.1007/s10157-018-1641-8
9. Litjens NH, van Druningen CJ, Betjes MG. Progressive loss of renal function is associated with activation and depletion of naive T lymphocytes. Clin Immunol. 2006;118(1):83–91. doi:10.1016/j.clim.2005.09.007
10. Meier P, Dayer E, Blanc E, Wauters JP. Early T cell activation correlates with expression of apoptosis markers in patients with end-stage renal disease. J Am Soc Nephrol. 2002;13(1):204–212.
11. Anding K, Gross P, Rost JM. The influence of uraemia and haemodialysis on neutrophil phagocytosis and antimicrobial killing. Nephrol Dial Transplant. 2003;18(10):2067–2073. doi:10.1093/ndt/gfg330
12. Gollapudi P, Yoon JW, Gollapudi S. Leukocyte toll-like receptor expression in end-stage kidney disease. Am J Nephrol. 2010;31(3):247–254. doi:10.1159/000276764
13. sela S, Shurtz-Swirski R, Cohen-Mazor M, et al. Primed peripheral polymorphonuclear leukocyte: a culprit underlying chronic low-grade inflammation and systemic oxidative stress in chronic kidney disease. J Am Soc Nephrol. 2005;16(8):2431–2438. doi:10.1681/ASN.2004110929
14. Maverakis E, Kim K, Shimoda M, et al. Glycans in the immune system and the altered gly- can theory of autoimmunity: a critical review. J Autoimmun. 2015;57:1–13. doi:10.1016/j.jaut.2014.12.002
15. Schmidt EP, Yang Y, Janssen WJ, et al. The pulmonary endothelial glycocalyx regulates neutrophil adhesion and lung injury during experimental sepsis. Nat Med. 2012;18(8):1217–1223. doi:10.1038/nm.2843
16. Bazzoni G, Dejana E. Endothelial cell-to-cell junctions: molecu- lar organization and role in vascular homeostasis. Physiol Rev. 2004;84(3):869–901. doi:10.1152/physrev.00035.2003
17. Landray MJ, Wheeler DC, Lip GY, et al. Inflammation, endothelial dysfunction, and platelet activation in patients with chronic kidney disease: the chronic renal impairment in Birmingham (CRIB) study. Am J Kidney Dis. 2004;43(2):244–253. doi:10.1053/j.ajkd.2003.10.037
18. Guidelines for vaccinating kidney dialysis patients and patients with chronic kidney disease summarized from recommendations of the Advisory Committee on Immunization Practices (ACIP); 2012. Available from: https://www.cdc.gov/vaccines/pubs/dialysis-guide-2012.pdf.
19. Danziger-Isakov L, Kumar D. AST Infectious diseases community of practice. Vaccination in solid organ transplantation. Am J Transplant. 2013;13(Suppl 4):311–317. doi:10.1111/ajt.12122
20. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2012;2013(Suppl 3):1–150.
21. Preboth M. PHS guidelines for management of occupational expo- sure to HBV, HCV and HIV: management of occupational blood exposures. Am Fam Physician. 2001;64(12):2012–2014.
22. Edey M, Barraclough K, Johnson DW. Review article: hepatitis B and dialysis. Nephrology. 2010;15(2):137–145. doi:10.1111/j.1440-1797.2009.01268.x
23. Mast EE, Margolis HS, Fiore AE, et al. A comprehensive immuniza- tion strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) part 1: immunization of infants, children, and adolescents. MMWR Recommend Rep. 2005;54(RR16):1–31.
24. DaRoza G, Loewen A, Djurdjev O, et al. Stage of chronic kidney disease predicts seroconversion after hepatitis B immunization: earlier is better. Am J Kidney Dis. 2003;42:1184–1192. doi:10.1053/j.ajkd.2003.08.019
25. Burdick RA, Bragg-Gresham JL, Woods JD, et al. Patterns of hepatitis B prevalence and seroconversion in hemodialysis units from three continents: the DOPPS. Kidney Int. 2003;63:2222–2229. doi:10.1046/j.1523-1755.2003.00017.x
26. A two-dose hepatitis B vaccine for adults (Heplisav-B). JAMA. 2018;319(8):822–823. doi:10.1001/jama.2018.1097
27. Barraclough KA, Wiggins KJ, Hawley CM, et al. Intradermal versus intramuscular hepatitis B vaccination in hemodialysis patients: a prospective open-label randomized controlled trial in nonresponders to primary vaccination. Am J Kidney Dis. 2009;54:95–103. doi:10.1053/j.ajkd.2009.03.010
28. Micozkadioglu H, Zumrutdal A, Torun D, Sezer S, Ozdemir FN, Haberal M. Low dose intradermal vaccination is superior to high dose intramuscular vaccination for hepatitis B in unresponsive hemodialysis patients. Ren Fail. 2007;29:285–288. doi:10.1080/08860220601166263
29. Rubin LG, Levin MJ, Ljungman P, et al. Infectious Diseases Society of America. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin Infect Dis. 2014;58:e44100.
30. Fabrizi F, Martin P, Messa P. Novel perspectives on the hepatitis B virus vaccine in the chronic kidney disease population. Int J Artif Organs. 2015;38:625–631. doi:10.5301/ijao.5000458
31. Mulley WR, Le ST, Ives KE. Primary seroresponses to double-dose compared with standard-dose hepatitis B vaccination in patients with chronic kidney disease: a systematic review and meta-analysis. Nephrol Dial Transplant. 2017;32:136–143. doi:10.1093/ndt/gfv443
32. Ong KY, Wong HY, Khee GY. What is the hepatitis B vaccination regimen in chronic kidney disease? Cleve Clin J Med. 2018;85(1):32–34. doi:10.3949/ccjm.85a.17017
33. Kim DK, Riley LE, Hunter P. on behalf of the Advisory Committee on Immunization Practices. recommended immunization schedule for adults aged 19 years or older, united states, 2018. Ann Intern Med. 2018;168(3):210–220. doi:10.7326/M17-3439
34. European Consensus Group on Hepatitis B Immunity: are booster immunizations needed for lifelong hepatitis B immunity? Lancet. 2000;355:561–565. doi:10.1016/S0140-6736(99)07239-6
35. Wang IK, Lin CL, Lin PC, et al. Effectiveness of influenza vaccination in patients with end-stage renal disease receiving hemodialysis: a population-based study. PLoS One. 2013;8(3):e58317. doi:10.1371/journal.pone.0058317
36. Bosaeed M, Kumar D. Seasonal influenza vaccine in immunocompromised persons. Hum Vaccin Immunother. 2018;14(6):1311–1322. doi:10.1080/21645515.2018.1445446
37. Gilbertson DT, Unruh M, McBean AM, et al. Influenza vaccine delivery and effectiveness in end- stage renal disease. Kidney Int. 2003;63(2):738–743. doi:10.1046/j.1523-1755.2003.00787.x
38. Kumar D, Blumberg EA, Danziger-Isakov L, et al. Influenza vaccination in the organ transplant recipient: review and summary recom- mendations. Am J Transplant. 2011;11(10):2020–2030. doi:10.1111/j.1600-6143.2011.03753.x
39. Grohskopf LA, Sokolow LZ, Broder KR, et al. Prevention and control of seasonal influenza with vaccines: recommendations of the advisory committee on immunization practices United States, 2017–18 Influenza Season. MMWR Recomm Rep. 2017;66:1–20. doi:10.15585/mmwr.rr6602a1
40. Remschmidt C, Wichmann O, Harder T. Methodological quality of systematic reviews on influenza vaccination. Vaccine. 2014;32:1678–1684. doi:10.1016/j.vaccine.2014.01.060
41. Song JY, Cheong HJ, Ha SH, Kee SY, Jeong HW, Kim WJ. Active influenza immunization in hemodialysis patients: comparison between single-dose and booster vaccination. Am J Nephrol. 2006;26:206–211. doi:10.1159/000093306
42. Sarnak MJ, Jaber BL. Pulmonary infectious mortality among patients with end-stage renal disease. Chest. 2001;120:1883–1887. doi:10.1378/chest.120.6.1883
43. Vandecasteele SJ, Ombelet S, Blumental S, Peetermans WE. The ABC of pneumococcal infections and vaccination in patients with chronic kidney disease. Clin Kidney J. 2015;8(3):318–324. doi:10.1093/ckj/sfv030
44. Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine for adults with immunocom- promising conditions: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morbidity Mortality Weekly Rep. 2012;61(40):816–819.
45. Tomczyk S, Bennett NM, Stoecker C, et al. Use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine among adults aged >/=65 years: recommendations of the advisory committee on immunization practices (ACIP). MMWR Morb Mortal Wkly Rep. 2014;63:822–825.
46. Portoles-Perez J, Marques-Vidas M, Picazo JJ, et al. Recommendations for vaccination against pneumococcus in kidney patients in Spain. Nefrologia. 2014;34:545–551. doi:10.3265/Nefrologia.pre2014.May.12534
47. Haut Conseil de la Santé publique, France. Avis relatif aux recommandations Vaccinales contre les infections a pneumocoque pour les adultes. Haut Conseil de la Santé Publique:France;1–13.
48. Sagheb MM, Sajjadi S, Sajjady G. A study on the protection of hemodialysis patients against diphtheria and tetanus. Ren Fail. 2009;31:904–909. doi:10.3109/08860220903268353
49. Mathew R, Mason D, Kennedy JS. Vaccination issues in patients with chronic kidney disease. Expert Rev Vaccin. 2014;13(2):285–298. doi:10.1586/14760584.2014.874950
50. Ventola CL. Immunization in the United States: recommendations, barriers, and measures to improve compliance. Part 2: adult vaccinations. P T. 2016;41(8):492–506.
51. Lin KY, Chen GJ, Lee YL, et al. Hepatitis A virus infection and hepatitis A vaccination in human immunodeficiency virus-positive patients: A review. World J Gastroenterol. 2017;23(20):3589–3606. doi:10.3748/wjg.v23.i20.3589
52. Craig AS, Watson B, Zink TK, et al. Hepatitis A outbreak activity in the United States: responding to a vaccine-preventable disease. Am J Med Sci. 2007;334(3):180–183. doi:10.1097/MAJ.0b013e3181425411
53. Gunawansa N, Rathore R, Sharma A, Halawa A. Vaccination practices in end stage renal failure and renal transplantation; review of current guidelines and recommendations. World J Transpl. 2018;8(3):68–74. doi:10.5500/wjt.v8.i3.68
54. DeVault KR, Wallace MB, Aqel BA, Keith D. Practical Gastroenterology and Hepatology Board Review Toolkit. Lindor John Wiley & Sons; 2016 sept 26:680
55. Fleischmann EH, Kruppenbacher J, Bock HL, et al. Active immunization against hepatitis A in dialysis patients. Nephrol Dial Transplant. 2002;17:1825–1828. doi:10.1093/ndt/17.10.1825
56. Dooling KL, Guo A, Patel M, et al. Recommendations of the advisory committee on immunization practices for use of herpes zoster vaccines. MMWR Morb Mortal Wkly Rep. 2018;67:103–108. doi:10.15585/mmwr.mm6703a5
57. Gabutti G, Bolognesi N, Sandri F, Florescu C, Stefanati A. Varicella zoster virus vaccines: an update. Immunotargets Ther. 2019;8:15–28. doi:10.2147/ITT.S176383
58. McLean HQ, Fiebelkorn AP, Temte JL, Wallace GS. Prevention of measles, rubella, congenital rubella syndrome, and mumps, 2013: summary recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2013;62(RR04):1–34.
59. Kim YJ, Kim SI. Vaccination strategies in patients with solid organ transplant: evidences and future perspectives. Clin Exp Vaccine Res. 2016;5(2):125–131. doi:10.7774/cevr.2016.5.2.125
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.