")
Back to Journals » Patient Preference and Adherence » Volume 13
Cross-cultural adaptation and validation of the Jefferson Scale of Patient’s Perceptions of Physician Empathy (JSPPPE) for the Portuguese population
Authors Domingues AC, Santiago LM , Rodrigues AR, Pires B , Velho D , Ferreira PL
Received 10 April 2019
Accepted for publication 14 May 2019
Published 15 July 2019 Volume 2019:13 Pages 1145—1152
DOI https://doi.org/10.2147/PPA.S211764
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ana Catarina Domingues,1 Luiz Miguel Santiago,2–4 Ana Rita Rodrigues,5 Beatriz Pires,2 Denise Velho,6 Pedro L Ferreira4,7
1General Practice and Family Medicine Resident, Family Health Unit Topázio, Health Centers Group of Baixo Mondego, Coimbra, Portugal; 2Faculty of Medicine, University of Coimbra, Coimbra, Portugal; 3Faculty of Medicine, University Clinic of General Practice and Family Medicine, Coimbra, Portugal; 4Centre for Health Studies and Research, University of Coimbra, Coimbra, Portugal; 5Faculty of Health Sciences, University of Beira Interior, Covilha, Portugal; 6Faculty of Health Sciences, University of Beira Interior, Covilha, Portugal; 7Faculty of Economy, University of Coimbra, Coimbra, Portugal
Objectives: To translate the Jefferson Scale of Patient Perceptions of Physician Empathy (JSPPPE) to the European Portuguese spoken language and to verify its reliability and validity.
Methods: Cultural adaptation and linguistic translation from English to European Portuguese, revision of translations, semantics equivalence, and grammar correction of the Portuguese wording were made. Readability of the Portuguese version was verified and the analysis of internal consistency and correlation with the subscale “physician–patient relationship” of the Portuguese version of European Task Force on Patient Evaluation of General Practice Care Scale (EuroPEP) were made. Reliability was tested by intertemporal stability and internal consistency. Validity of criteria and construction was also verified.
Results: The Portuguese translation was adapted to the 8th or 9th grade level, easy to understand. There was the need to change the visual appearance of the scale, answers below sentences. Interclass correlation coefficient for reliability varied between 0.737 and 1.000 and Cronbach’s α between 0.806 and 0.877. Validity was verified by comparing values of socio-demographic variables for JSPPPE index and for EuroPEP with no differences. Correlation values between the total score and its five items varied from 0.806 to 0.934. Criterion validity against EuroPEP had a correlation of 0.831.
Conclusion: This study fulfilled the necessary steps to translate, verify the validity and the reliability of the Portuguese version of the JSPPPE, with minimum layout alteration. All five items were maintained. The authors recommend the use of the JSPPPE in research and clinical practice.
Keywords: empathy, physician-patient relationship, patient centered medicine
Background
Empathic communication is essential when speaking of physician–patient relationship.1 This multidimensional concept was defined by Hojat as a predominantly cognitive attribute (more than emotional), involving understanding (more than feeling) the patient’s experiences, concerns, and perspectives, in combination with the ability to communicate that understanding.2,3 It contrasts with the concept of sympathy, for with empathy the doctor must retain his abilities of technical analysis and judgment to take action.2
When analyzing empathy we must always take into account the patient’s participation in the decision-making process which, in the case of General Practice and Family Medicine, falls under the biopsychosocial approach. McWhinney and Moira Stewart developed methodologies for person-centered consultation.4
A good physician–patient relationship with empathic involvement is associated with better adherence to treatment, higher levels of satisfaction with the doctor and the health system, better memory and understanding of the information given by the doctor and to a better quality of life and psychological, physical, and social well-being.5
Hojat and collaborators validated the original version of the Jefferson Scale of Patients Perceptions of Physician Empathy (JSPPPE), a five-item measurement instrument, to be answered by patients on a Lickert scale from 1 (strongly disagree) to 7 (strongly agree), aggregated in a single component.6 The corrected item-total scores ranged from 0.88 to 0.94 as well as showing strong correlations with scores of patient satisfaction. In the original version, Cronbach’s α coefficient varied between 0.97 and 0.99 for the total sample and for patients in different gender and age groups. This scale measures (i) understanding patients’ perspectives, (ii) inquiring about daily life, (iii) showing concern for the patient and their family, (iv) understanding patients’ emotions, feelings, and concerns, and (v) patient understanding by the doctor.6 The global score is obtained by the mean score of all five items.
The same authors have also developed the Jefferson Scale of Empathy (JSE) to measure doctors and student´s empathy a student´s version recently used to verify the change in beliefs in students recently admitted to Medicine.7
Several studies have shown positive associations between medical empathy, patient satisfaction and empowerment, patients becoming more able to withstand their problems, and the scale reaching good levels of internal consistency and reliability.8–11 In 2011, it was demonstrated that the perceived medical empathy, as measured by JSPPPE, is associated with better clinical outcomes in diabetic patients, as well as in patients with trauma.12,13
According to our research, there are no published papers in Portugal about empathy as perceived by the patient, using the JSPPPE scale. Taking this and the importance of empathy to effective physician–patient communication14 into consideration, it is pertinent to measure it by answering the question “How do patients value empathy in their relationship with their doctor?”.
The goal of this study was to translate the JSPPPE scale to Portuguese spoken in Portugal and verify its reliability and validity.
Methods
After the original author’s authorization, the process of translating the questionnaire into Portuguese followed the sequential approach.15,16 The English version was first independently translated into Portuguese by two professional language translators, both native Portuguese speakers. The two translations were revised and reconciled in a meeting by a team consisting of one psychologist, one sociologist, one nurse, and three physicians, thus creating the first Portuguese version of the JSPPPE.
The English translation was then made by two General Practitioners (GPs) working in England. In order to ensure semantic equivalence,17 two experts, Portuguese specialists in Family Medicine, reviewed technical aspects of the translation in terms of understandability and use of medical jargon, to make it more readable for the general public. Finally, a Portuguese linguist guaranteed the grammatical correction of the text.
Readability of the Portuguese version was estimated with the Flesch index on a 100-point scale, with cut-off points at 30, 50, 60, 70, 80, and 90, where the range [90–100] corresponds to a very easy to read text and the interval [0–30] to a text which is very difficult to read.18,19 This index also allows an estimate of the number of years of education required for an adequate understanding of the text.
This observational study involved the collection of two samples at different times. The purpose of the first one was to evaluate the reliability of the measure and was carried out during the month of July 2015, with interviews of patients from two practices, one Family Health Unit from Baixo Mondego Health Centre Group and one Traditional Health Center from the Pinhal Litoral Health Centre Group. Only those patients who had given written informed consent and attended the interview at the stipulated time were included, according to the ethics committee protocol. Interviews took place immediately after each patient’s appointment with their family doctor and consisted of an initial self-fulfillment followed by 15 mins later one with marked answers by the interviewer. Doctors were not aware of the interviews that were made in a non-visible place to doctors according to the study protocol approved by the ethics committee and the board of the health units.”
The second data collection was carried out in 2017 at several Family Medicine practices, also on randomly selected days. The questionnaire was self-administered, except for those unable to read or write, in which case the researcher interviewed them. As before, participants had previously given informed consent and were given the questionnaire immediately after an appointment with their family doctor, to be filled in a quiet place of the health unit. The study had been approved by all participating Health units, but unbeknownst to the Family Doctors.
This study was approved by the Ethics committee of the Centre Regional Health Authority.
Collected data were stored in computer records, without any identification of the participants. This data were analyzed and some hypotheses were tested in order to demonstrate the reliability and validity of the Portuguese version of the JSPPPE.
A three-part data collection instrument was used: (1) brief collection of socio-demographic data, (2) the previously obtained Portuguese version of the JSPPPE; and (3) “physician–patient relationship” sub-dimension from the Portuguese version of the European Task Force on Patient Evaluation of General Practice Care Scale (EuroPEP).
- Socio-demographic information collected in this study comprised patient age, gender, literacy, and employment status.
Age was organized into three categories, up to 35, from 36 to 65, and over 65 years old. The level of literacy was classified into four categories, ‘only knows how to read and write’, completed 9th grade (or 4th grade for older people), completed 12th grade (or 7th grade for older people), higher education degree. Participants were also questioned on their main occupation and/or source of income. Activities in agriculture, commerce, industry or services, as well as home keeping were classified as active, whereas pensioners, students, and unemployed were classified as inactive.
- The Portuguese version of the JSPPPE consists of five items, each being measured on a seven category concordance scale. The resulting index was obtained by calculating the mean of answers.
- The EuroPEP also allows us to measure relational and satisfaction aspects, often understood as synonyms of empathy. The conceptual model of the Portuguese version of this questionnaire, tested and validated in Portugal and developed by the “Centre for Health Studies and Research of the University of Coimbra”, includes the dimensions “medical care”, “non-medical care”, “organization of services”, and ‘quality of premises.20,21‘ The eight items used in this study constitute the sub-dimension “physician–patient relationship” of the “medical care” dimension. The score for this sub-dimension was obtained by the mean of the answers to its various items, ignoring “not applicable” answers.
In order to address reliability, we tested intertemporal stability and internal consistency. Intertemporal stability was tested using the interclass correlation coefficient (ICC) in a test–retest design with 15 mins interval between writing (first moment) and an interview (second moment). A score of less than 0.5 is considered weak, between 0.5 and 0.75 moderate, between 0.75 and 0.9 good, and above 0.9 excellent.22
Internal consistency, representing the homogeneity of the items, was tested using Cronbach’s α, with desirable values between 0.7 and 0.9.23
For the validity tests of the Portuguese version of the JSPPPE, this study considered the three known forms of content, construction, and criterion validity.23 Content validity was tested in a pre-test after the cultural and linguistic adaptation, to verify and guarantee the adequacy of the measurable characteristics while simultaneously evaluating the questionnaire filling-out time and difficulties in perception, item clarity, interpretation of the Portuguese language, and visual agreeability of the questionnaire.
Initially, the hypothesis that these socio-demographic variables had no impact on the empathy index felt by the patients was considered.
For construct validity, hypotheses were tested in known groups, taking into account socio-demographic variables and the following research hypothesis:
H1: The JSPPPE scores are sensitive to socio-demographic variables
For normally distributed numerical variables, we used Student’s t-test and for non-normally distributed as well as for ordinal variables, the Mann–Whitney U and Kruskal–Wallis H tests were used as well as the χ2 test.
Additionally, to find the underlying factorial structure of the JSPPPE, a factorial analysis with varimax rotation and Kaiser criterion was performed, after confirmation with KMO and Bartlett’s test.24
In order to test criterion validity, we used bivariate statistical analysis (Pearson’s correlation coefficient) between the JSPPPE index and the values of the sub-dimension “physician–patient relationship” of the EuroPEP scale. The following research hypothesis was formulated:
H2: The JSPPPE scores are related to the EuroPEP “physician–patient ratio”
Considering the specificity of both measures, it is expected that there will be strong and significant correlations between the JSPPPE index and each of the items of the sub-dimension “physician–patient relationship” of the EuroPEP scale.
Results
Cultural and linguistic adaptation
Throughout this study, great effort was made to ensure that the translated Portuguese version of JSPPPE was in the agreement with the original English text, both in spirit and semantically.
The process of translating the questionnaire into Portuguese and back-translating into English resulted in a set of sentences that, when analyzed in the light of Flesch’s Reading Ease Test, revealed an average of 2 syllables per word and 11.2 words per sentence, thus obtaining a final result of 68.63, corresponding to an intermediate 8th–9th grade level, publishable and easy to understand.
This was confirmed in the pre-test with the users. However, they showed a desire for changes in the graphical layout, so that the response scale would be placed below the sentence to be classified, rather than being placed at the beginning of the sentence. There was also a need to highlight “ … phrases about your doctor … ” in the text, to make it clear that the questionnaire concerned their opinion about the doctor and not the last consultation.
Sample and reliability
Table 1 shows the characteristics of the two samples used in this study.
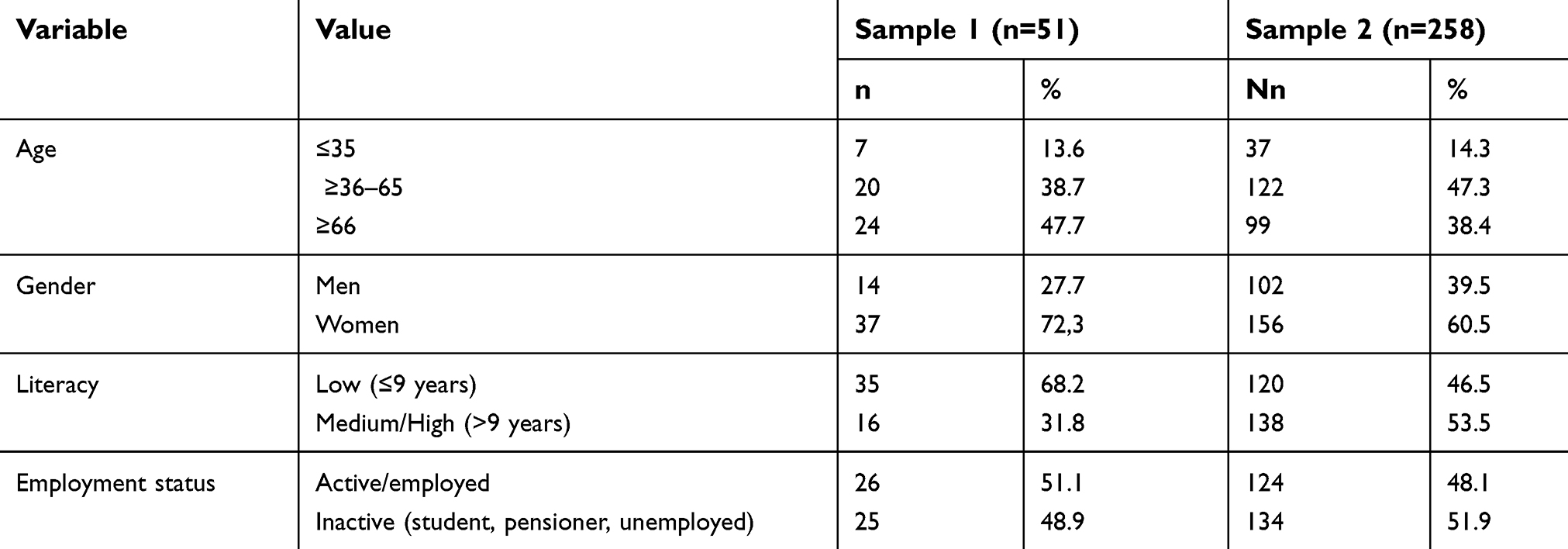 |
Table 1 Descriptive samples’ socio-demographic characteristics |
In the first sample, 51.1% were active, 13.6% were under 35 years and 47.7% were over 65 years old, 27.7% were men, and 68.2% had low academic education. The second sample had socio-demographic characteristics similar to the first one (p>0.05), with the exception of literacy in which the percentage of participants with medium or high literacy was higher (χ2=8,3; p<0,005).
The Kolmogorov–Smirnov test showed that the mean values of the JSPPPE and EuroPEP scales were normally distributed. Thus, Table 2 presents the descriptive statistics of the JSPPPE empathy scale and the sub-dimension “physician–patient relationship” of EuroPEP. The corresponding Kolmogorov–Smirnov normality test results are also presented.
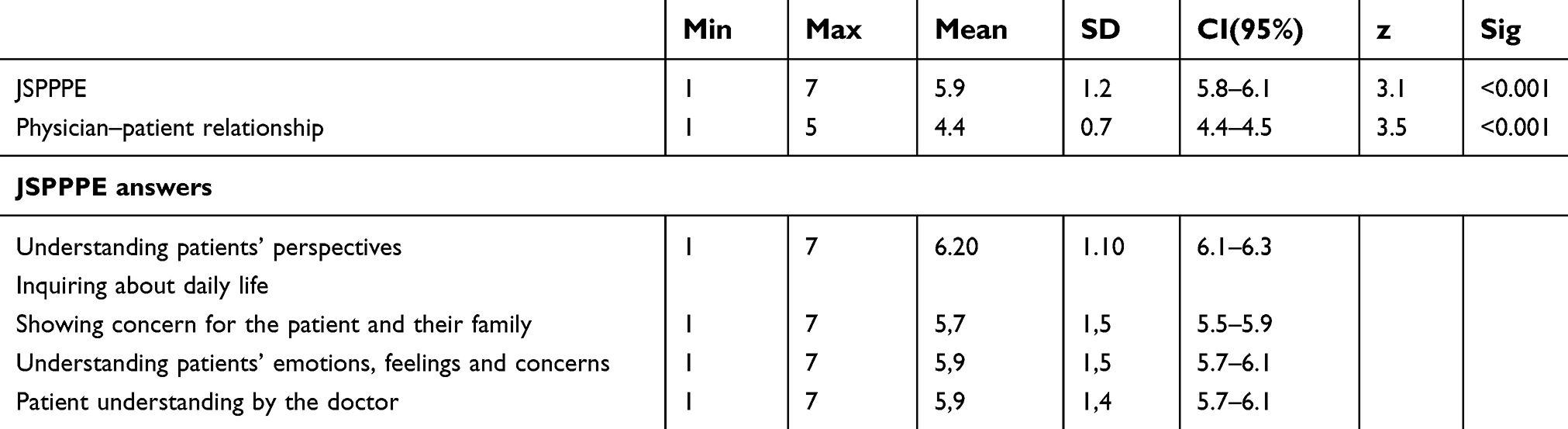 |
Table 2 JSPPPE and “physician-patient” relationship score distribution (n=258) |
Table 3 contains the excellent reliability values obtained in this study.
 |
Table 3 Reliability values by test–retest, internal consistency, item-total correlation, mean±SD, and 95% confidence interval |
The ICC test–retest reliability ranged from 0.737 to 1.000 and Cronbach’s α varied between 0.806 and 0.877. On the other hand, the correlation values between the whole scale and its five items ranged from 0.806 to 0.934.
To test the H1 hypothesis, the values of the JSPPPE index were compared for each of the socio-demographic variables collected. Table 4 presents the results.
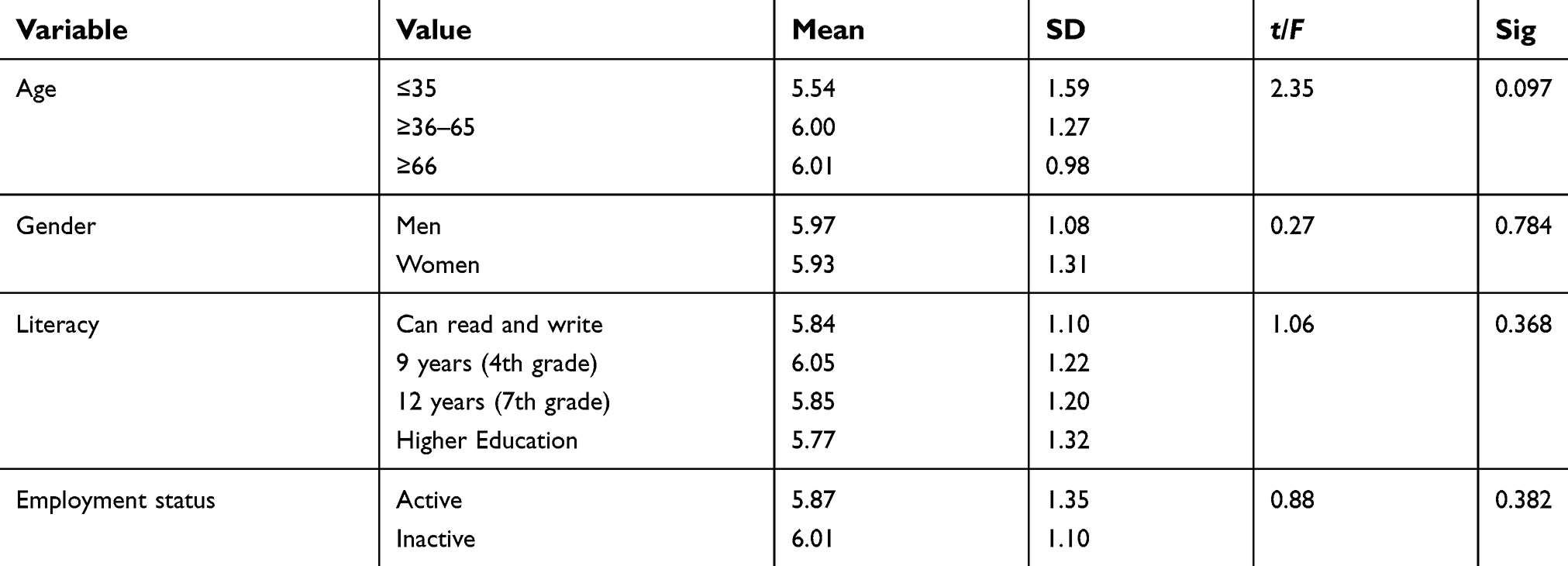 |
Table 4 Reliability values by age, gender, literacy, and employment status |
As we had anticipated, the socio-demographic variables do not have a discriminatory role in the JSPPPE index.
This index was confirmed in the Portuguese version through a factor analysis with varimax rotation and after verification of KMO (0.873) and Bartlett’s test of sphericity (p<0.001). In fact, the Kaiser criterion produced a single index explaining almost 80% of the variance. Table 5 presents the results of this analysis.
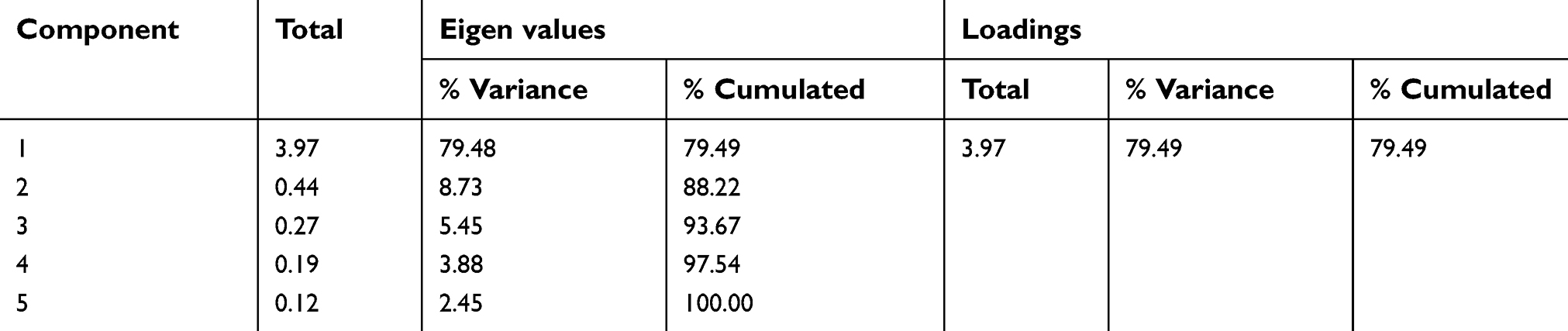 |
Table 5 Reliability values for extracted component of JSPPPE |
To test the hypothesis H2, we calculated the correlation coefficients between the JSPPPE scale index and the EuroPEP sub-dimension “physician–patient relationship”. Table 6 presents the results of these correlations.
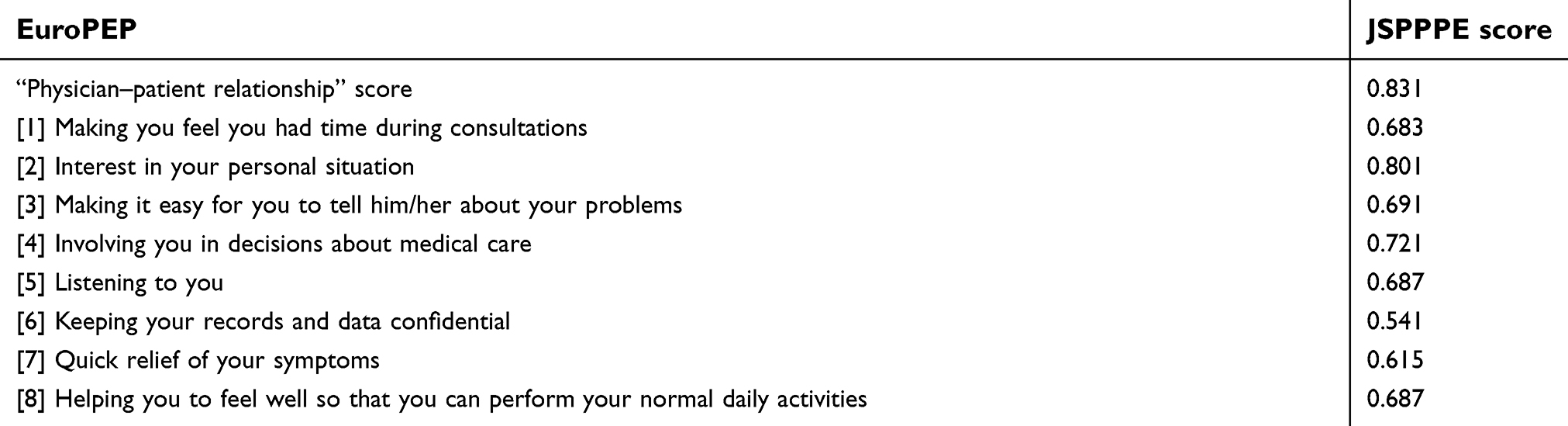 |
Table 6 Criterion validity between JSPPPE and “physician–patient relationship” (n=258) |
As can be seen, both scores had a correlation of 0.831. Among the items of the sub-dimension “physician–patient relationship”, the interest shown in their personal situation (item 2) had the highest correlation whereas confidentiality of clinical records (item 6) had the lowest correlation. When we tried to explain the JSPPPE index through the eight items of the sub-dimension “physician–patient relationship”, items 2 and 8 were most significant. Therefore, based on both measures and data from this study it seems that the concept of empathy is perceived by patients as interest displayed in their personal situation and helping them to perform their daily activities.
Discussion
The physician–patient relationship goes beyond the situational meeting between them. It is more than asking questions, examining the patient, prescribing medication, and giving recommendations. Several studies suggest that this relationship combines technical and personal abilities as well as empathic attitudes.25,26
The increasing use of complementary diagnostic tests, the permanent development of technologies and the pressure to reduce costs and consultation times may distance the doctor from the patient; therefore we need to go back to the principles of the therapeutic relationship.27
With this study, the JSPPPE was translated to Portuguese, its internal consistency and reliability was verified, and it was validated according to a sub-dimension of EuroPEP, an instrument widely used and with papers published in Portugal.2,3,21
The translation of the JSPPPE questionnaire and further proceedings allowed the authors to fulfill all the needed steps to validate the linguistic translation of this instrument for European Portuguese language which can be different from the Brazilian Portuguese one.28
We found no difficulties in the comprehension of the five statements of the JSPPPE questionnaire. However, it was necessary to add a scale from 1 to 7 below each statement in alternative to the formulation of the initial JSPPPE. This was the only change to the original questionnaire. The average time needed to complete the questionnaire was approximately 3 mins, with individuals with higher levels of education tasking less time.
The observation of a significant strong positive correlation between the average score on the JSPPPE and the average score of the physician–patient relationship indicator means that it is possible to measure how the patient perceives empathy with a short five question scale.
The instrument now validated will undoubtedly be of huge value in clinical practice. The application of the JSPPPE in population studies will allow doctors and students to ascertain if this measure can be a marker of adequate consequences of the consultation and be used not only to assess a contact but the experience of the contact eventually prolonged between doctor and patient.
There is still the need to study the association between the value of the perceived doctor’s empathy with indicators of clinical activity such as accessibility, financial and morbidity management indicators, as well as with the impact on doctor’s life and patient’s perception of the quality of life.
Conclusions
The Portuguese version of the JSPPPE preserved the dimensions used in the construction of the original scale testifying its construct validity.
The application of the JSPPPE will allow the observation of patient’s perception of doctor’s empathy and its use where necessary in national and international studies.
Abbreviation List
JSPPPE, Jefferson Scale of Patients Perceptions of Physician Empathy; JSE, Jefferson Scale of Empathy; GP, General Practitioner; EuroPEP, European Task Force on Patient Evaluation of General Practice Care scale.
Data sharing statement
All data are available for researchers upon request.
Ethics approval
This study was approved by the Ethics committee of the Centre Regional Health Authority and the Ethics Committee of the Adiministração Regional de Saúde do Centro de Portugal.
Acknowledgments
To José Gabriel, MD, and Bruno Heleno, MD, PhD for the Portuguese-English translation. To the experts who, anonymously, helped to translate the scale to Portuguese. There was no specific funding received for this work.
Author contributions
Ana Catarina Domingues, Ana Rita Rodrigues, and Beatriz Pires were leading field authors, collecting data. They read the paper and gave their informed scientific consent. Luiz Miguel Santiago and Pedro Ferreira wrote the paper, and made the statistical work. Denise Velho made scientific inputs and made the English writing. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McWhinney IR. A Textbook of Family Medicine. Oxford, UK: Oxford University Press; 1989;13:27.
2. Hojat M. Empathy in Patient Care : Antecedents, Development, Measurement, and Outcomes. New York: Springer; 2007.
3. Hojat M, Mangione S, Nasca TJ, et al. The Jefferson scale of physician empathy: development and preliminary psychometric data. Educ Psychol Meas. 2001;61(2):349–365. doi:10.1177/00131640121971158
4. Gusso G, Lopes JMC, editors. Tratado De Medicina De Família E Comunidade: Princípios, Formação E Prática. Artmed Editora; 2012;113–123.
5. Ogle J, Bushnell JA, Caputi P. Empathy is related to clinical competence in medical care. Med Educ. 2013;47(8):824–831. doi:10.1111/medu.12232
6. Hojat M, Louis DZ, Maxwell K, Markham F, Wender R, Gonnella JS. Patient perceptions of physician empathy, satisfaction with physician, interpersonal trust, and compliance. Int J Med Educ. 2010;14(1):83–87. doi:10.5116/ijme.4d00.b701
7. Loureiro J, Gonçalves-Pereira M, Trancas B, Caldas-de-Almeida JM, Castro-Caldas A. Empathy in the physician-patient relationship as viewed by first-year medical students: data on validity and sensibility to change of the Jefferson measure in Portugal. Acta Med Port. 2011;24(S2):431–442.
8. Jani BD, Blane DN, Mercer SW. The role of empathy in therapy and the physician-patient relationship. Forschende Komplementärmedizin/Res Complement Med. 2012;19(5):252–257. doi:10.1159/000342998
9. Neumann M, Wirtz M, Bollschweiler E, et al. Determinants and patient-reported long-term outcomes of physician empathy in oncology: a structural equation modelling approach. Patient Educ Couns. 2007;69(1–3):63–75. doi:10.1016/j.pec.2007.07.003
10. Mercer SW, Neumann M, Wirtz M, Fitzpatrick B, Vojt G. General practitioner empathy, patient enablement, and patient-reported outcomes in primary care in an area of high socio-economic deprivation in Scotland—a pilot prospective study using structural equation modeling. Patient Educ Couns. 2008;73(2):240–245. doi:10.1016/j.pec.2008.07.046
11. Rakel D, Barrett B, Zhang Z, et al. Perception of empathy in the therapeutic encounter: effects on the common cold. Patient Educ Couns. 2011;85(3):390–397. doi:10.1016/j.pec.2011.01.009
12. Hojat M, Louis DZ, Markham FW, Wender R, Rabinowitz C, Gonnella JS. Physiciansʼ empathy and clinical outcomes for diabetic patients. Acad Med. 2011;86(3):359–364. doi:10.1097/ACM.0b013e3182086fe1
13. Steinhausen S, Ommen O, Thüm S, et al. Physician empathy and subjective evaluation of medical treatment outcome in trauma surgery patients. Patient Educ Couns. 2014;95(1):53–60. doi:10.1016/j.pec.2013.12.013
14. Derksen F, Bensing J, Lagro-Janssen A. Effectiveness of empathy in general practice: a systematic review. Br J Gen Pract. 2013;63(606):e76–84. doi:10.3399/bjgp13X660814
15. Acquadro C, Conway K, Hareendran A, Aaronson N. European regulatory issues and quality of life assessment (ERIQA) Group. Literature review of methods to translate health-related quality of life questionnaires for use in multinational clinical trials. Value Heal. 2008;11(3):509–521. doi:10.1111/j.1524-4733.2007.00292.x
16. Eremenco SL, Cella D, Arnold BJ. A comprehensive method for the translation and cross-cultural validation of health status questionnaires. Eval Health Prof. 2005;28(2):212–232. doi:10.1177/0163278705275342
17. Herdman M, Fox-Rushby J, Badia X. A model of equivalence in the cultural adaptation of HRQoL instruments: the universalist approach. Qual Life Res. 1998;7(4):323–335. doi:10.1023/A:1008846618880
18. Flesch R. A new readability yardstick. J Appl Psychol. 1948;32(3):221–233. doi:10.1037/h0057532
19. Scarton C, Aluísio S. Análise da Inteligibilidade de textos via ferramentas de Processamento de Língua Natural: adaptando as métricas do Coh-Metrix para o Português. Linguamática. 2010;2(1):45–61.
20. Ferreira PL. A voz dos doentes: satisfação com a medicina geral e familiar. In: Instrumentos Para a Melhoria Contínua Da Qualidade. Lisboa: Direcção Geral da Saúde; 1999:1–57. Available from: http://www2.acss.min-saude.pt/Portals/0/2015.08.24-Relat%C3%B3rio%20Final-VF.pdf. Accessed May 14, 2018.
21. Ferreira PL, Antunes P, Portugal S. O Valor Dos Cuidados Primários: Perspectiva Dos Utilizadores Das USF. Lisboa: Ministério da Saúde; 2010.
22. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi:10.1016/j.jcm.2016.02.012
23. Terwee CB, Bot SDM, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42. doi:10.1016/j.jclinepi.2006.03.012
24. Lisboa JV, Augusto MG, Ferreira PL. Estatística Aplicada À Gestão. Porto: Vida Económica; 2012.
25. Costa FDD, Azevedo RCSD. Empatia, relação médico-paciente e formação em medicina: um olhar qualitativo. Rev Bras Educ Med. 2010;34(2):261–269. doi:10.1590/S0100-55022010000200010
26. Rakel RE, Rakel DP. Textbook of Family Medicine. Philadelphia, PA: Elsevier Saunders; 2016.
27. Baptista S. A empatia na intersubjectividade da relação clínica. Rev Port Med Geral Fam. 2012;28(3):224–226.
28. Bernardo MO, Cecílio-Fernandes D, Costa P, Quince TA, Costa MJ, Carvalho-Filho MA. Physicians’ self assessed empathy levels do not correlate with patients’ assessments. PLoS One. 2018:13(5):e0198488. eCollection 2018. doi:10.1371/journal.pone.0198488.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.