")
Back to Journals » Advances in Medical Education and Practice » Volume 8
Creating physicians of the 21st century: assessment of the clinical years
Authors Vanderbilt AA, Perkins SQ, Muscaro MK, Papadimos TJ, Baugh RF
Received 10 March 2017
Accepted for publication 15 May 2017
Published 23 June 2017 Volume 2017:8 Pages 395—398
DOI https://doi.org/10.2147/AMEP.S136664
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Allison A Vanderbilt,1 Sara Q Perkins,2 Moriah K Muscaro,2 Thomas J Papadimos,3 Reginald F Baugh4
1Department of Family Medicine, 2College of Medicine and Life Sciences, University of Toledo, 3Department of Anesthesiology, 4Department of Surgery, College of Medicine and Life Sciences, University of Toledo, Toledo, OH, USA
Abstract: Medical education has been under a constant state of revision for the past several years. The overarching theme of the curriculum revisions for medical schools across the USA has been creating better physicians for the 21st century, with the same end result: graduating medical students at the optimal performance level when entering residency. We propose a robust, thorough assessment process that will address the needs of clerkships, residents, students, and, most importantly, medical schools to best measure and improve clinical reasoning skills that are required for the learning outcomes of our future physicians. The Accreditation Council for Graduate Medical Education (ACGME) evaluates and accredits medical school graduates based on competency-based outcomes and the assessment of specialty-specific milestones; however, there is some evidence that medical school graduates do not consistently meet the Level 1 milestones prior to entering/beginning residency, thus starting their internship year underprepared and overwhelmed. Medical schools should take on the responsibility to provide competency-based assessments for their students during the clinical years. These assessments should be geared toward preparing them with the cognitive competencies and skills needed to successfully transition to residency. Then, medical schools can produce students who will ultimately be prepared for transition to their residency programs to provide quality care.
Keywords: ACGME Core Competencies, milestones, clerkships, medical education, evaluation
Creating physicians of the 21st century: assessment of the clinical years
Medical education has been under a constant state of revision for the past several years. Innovation is the newest word when it comes to medical education, as medical schools charge forward to reconfigure their curriculum. The novel vernacular is experiential learning,1 integrated approaches, and a variety of early clinical experiences.2 The overarching theme of integrated curriculum that medical schools across the USA have deployed is to create better physicians for the 21st century, with the same end result: graduating medical students at the optimal performance level when entering residency. With all the brilliant minds in medicine and medical education, the question still remains – why are the clinical years lagging in performance measures and outcomes, thus leading to medical students falling behind? The answer is rather simple: the assessment of students’ performance during the clinical years of medical school is not standardized, nor is it up to par to best prepare students for residency. The assessments do not compare with the depth, specificity, or actionable content compared to basic science years. The National Board of Medical Examiners’ subject-specific exams are not sufficient on their own, as they primarily measures content knowledge and not clinical reasoning or the students’ ability to synthesize the information, particularly novel information. We propose a robust, thorough assessment process that will address the needs of clerkships, residents, students, and, most importantly, medical schools to best measure and improve clinical reasoning skills that are required for the learning outcomes of our future physicians.
ACGME Core Competencies
In the USA, assessment for medical students and residents is increasingly based on the model developed by the Accreditation Council for Graduate Medical Education (ACGME).3 The ACGME model focuses on six core interrelated competencies: medical knowledge; patient care; professionalism; interpersonal and communication skills; practice-based learning and improvement; and systems-based practice.4 The ACGME moved on to competency-based outcomes and the assessment of specialty-specific milestones; however, there is some evidence that medical school graduates do not consistently meet the Level 1 milestones prior to entering/beginning residency,5 thus starting their internship year underprepared and overwhelmed. The enormity of the problem begins within the medical education community for not clearly defining or documenting clinical competency during clerkship rotations. Furthermore, there is no clear definition or documentation of competency during the matriculation from medical school into residency. Although the medical education community (both undergraduate and graduate medical education) has not clarified where the responsibility for ensuring Level 1 competency of graduates falls,6 it does not detract from the need to do so. The assessment of competencies should provide insight into the actual performance and capacity to adapt to change, to find and generate new knowledge, and to improve overall performance7 as medical students matriculate through the clinical years and into residency. To best prepare our medical students for residency, medical schools should take responsibility for providing residency programs with accurate, competency-based assessments of their graduates8 and develop competency-based instruments to assess medical students as they progress through medical school toward internship.9
As medical educators and physicians, we know that medical knowledge and competence is developmental; however, habits of the mind – behavior and practical – and wisdom are achieved through deliberate practice10 that can be achieved throughout medical school and with further refinement of medical skills during the clinical years via robust, clinically meaningful assessments and feedback. The ultimate goal of medical education is for students to be able to competently practice medicine independently by the end of their medical training.11 Therefore, it is essential that medical schools begin to properly and systematically evaluate medical students early in their clinical years with assessments that will best prepare and train them for their transition to residency. This can be achieved with a focus on early assessment of cognition in an environment of uncertainty to identify students with clinical cognitive difficulties. The traditional transition from basic science to clinical years represented a change in the demands on medical students by going from certainty (the answers are on the page somewhere) to operating in the environment of clinicians, where degrees of clinical uncertainty are always present. Many otherwise-strong students in basic sciences struggle to achieve clinical reasoning competence. Therefore, through the application of the ACGME Core Competency: Patient Care (Clinical Reasoning), Table 1 represents how medical schools can begin to evaluate medical students during clinical rotations to determine how a student is matriculating through the clerkship toward the intended competency.
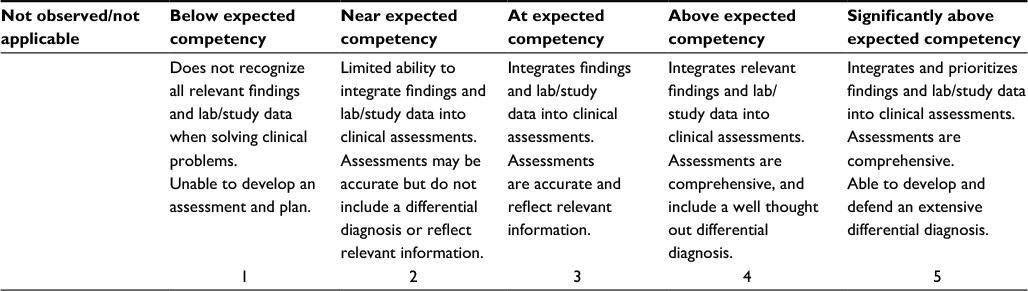 | Table 1 Patient care – clinical reasoning |
All the classification systems of clinical reasoning are different, but there is fairly uniform agreement that the majority of the academic difficulties of medical students are cognitive in nature and that these cognitive problems are the source of difficulties in clinical reasoning as well.12 Identifying learners who may have difficulty early in the clinical curriculum, informing the students, and providing them with appropriate training and mediation measures as indicated.13 For the training and remediation to be successful, understanding the specific student’s difficulties and specific needs is necessary. The assessment must be student specific and the recommendations generated able to be supported by the clinical faculty/department. The clinical faculty must be able to identify the problem and have the skills and pedagogical framework in which to construct training and remediation as necessary. Otherwise, the faculty would teach as they were taught in medical school and as undergraduates relying upon dispensing information, just as they were taught previously.14
The focus of early clinical diagnosis courses should be the teaching of clinical reasoning. Decades of experience have shown that acquisition of clinical skills, although often a strong desire of medical students, should be a secondary goal. Students must receive specific feedback on their clinical reasoning skills so that they engage in deliberate practice to improve their skills.9 Timely feedback, not just feedback, following summative evaluations such as semester evaluations is warranted for optimal student learning. Mid-year and formal formative evaluations will be necessary to identify those learners who are beginning to lag behind and who need extra help to remain with their classmates.
As we move to more active learning in medical education, we should recall the fundamental premise of constructivism – learners construct knowledge based on previously held beliefs and experiences. The interaction is dynamic between the learner and the experiences. Only by carefully crafting the appropriate experience can the learner learn as knowledge is constructed by the individual and is not passively acquired. Active participation, critical inquiry, self-regulation, and self-assessment are needed, combined with deliberate practice and appropriate feedback, for the active learner to learn.
Faculty members require basic training in educational theory and need to acquire new teaching skills to teach effectively. Unfortunately, most faculty training programs are workshops or short weekend courses, which offer the participants satisfaction as an outcome but little else. There is a growing consensus that longer-term interventions are required to produce a sustainable change in learning, behavior, and organizational culture. Interventions must navigate the competition among patient care, research, and teaching demands on clinical faculty, and in such cases teaching routinely draws the short straw.
Conclusion
In order to best prepare graduating medical students for critical thinking and ensure that they have achieved the ACGME Core Competencies, a comprehensive and thorough assessment and evaluation process of clinical education is necessary. Medical schools should take on the responsibility to provide competency-based assessments for their students during the clinical years. These assessments should be geared toward preparing them with the cognitive competencies and skills needed to successfully transition to residency. The competency-based assessments could provide a baseline for each individual student’s clinical skills, as well as give insight to students who are lagging behind and need remediation. In order to accomplish this task, physician-educators need longer-term interventions directed at improving their abilities and capabilities in providing this new educational curriculum. The proposed intervention would help physician-educators have a pedagogical framework to then personalize to their specialty and teaching style. The educators could then adapt the skills acquired to help them construct training, engage in creating an active learning environment, and give timely feedback. Although a big task, graduating medical school students will ultimately be prepared for transition to their residency programs to provide quality care.
Acknowledgment
The authors thank Miss Margaret A Hoogland, Clinical Medical Librarian, College of Medicine and Life Science, University of Toledo, for her assistance in acquiring pertinent literature related to this article.
Disclosure
The authors report no conflicts of interest in this work.
References
Cooke M, Irby DB, O’Brien BC. Educating Physicians: A Call for Reform of Medical School and Residency. San Francisco, CA: Jossey-Bass; 2010. | ||
Chen HC, McNamara M, Teherania A, Cate OT, O’Sullivan P. Developing entrustable professional activities for entry into clerkship. Acad Med. 2016;96:247–255. | ||
Epstein RM. Assessment in medical education. N Engl J Med. 2007;356:387–396. | ||
Santen SA, Rademacher N, Heron SL, Khandelwal S, Hauff S, Hopson L. How competent are emergency medicine interns for level 1 milestones: who is responsible? Acad Emerg Med. 2013;20:736–739. | ||
Batalden P, Leach D, Swing S, Drefus H, Drefus S. General competencies and accreditation in graduate medical education. Health Aff. 2002;21;103–111. | ||
Santen SA, Peterson WJ, Khandelwal S, House JB, Manthey DE, Sozener CB. Medical student milestones in emergency medicine. Acad Emerg Med. 2014;21:905–911. | ||
Fraser SW, Greenhalgh T. Coping with complexity: educating for capability. BMJ. 2001;323:799–803. | ||
Sozener CB, Lypson ML, House JB, et al. Reporting achievement of medical student milestones to residency program directors: an educational handover. Acad Med. 2016;91:676–684. | ||
Ericsson KA. Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Acad Med. 2004;79(Suppl 10):S70–S81. | ||
ten Cate O, Snell L, Carraccio C. Medical competence: the interplay between individual ability and the health care environment. Med Teach. 2010;32:669–675. | ||
The Accreditation Council for Graduate Medical Education. Available from: http://www.acgme.org. Accessed December 5, 2016. | ||
Audétat MC, Lubarsky S, Blais JG, Charlin B. Clinical reasoning: where do we stand on identifying and remediating difficulties? CreaEdu. 2013;4(6):42–48. | ||
Evans DE, Alstead EM, Brown J. Applying your clinical skills to students and trainees in academic difficulty. Clin Teach. 2010;7(4):230–235. | ||
Hurst JW. The overlecturing and underteaching of clinical medicine. Arch Inter Med. 2004;164(15):1605–1608. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.