")
Back to Journals » Advances in Medical Education and Practice » Volume 9
CPR in medical TV shows: non-health care student perspective
Authors Alismail A , Meyer NC , Almutairi W, Daher NS
Received 12 July 2017
Accepted for publication 8 December 2017
Published 7 February 2018 Volume 2018:9 Pages 85—91
DOI https://doi.org/10.2147/AMEP.S146149
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Abdullah Alismail,1 Nicole C Meyer,2 Waleed Almutairi,1 Noha S Daher3
1Cardiopulmonary Sciences Department, School of Allied Health Professions, Loma Linda University, Loma Linda, CA, USA; 2Respiratory Care Department, Loma Linda University Children’s Hospital, Loma Linda, CA, USA; 3Department of Allied Health Studies, School of Allied Health Professions, Loma Linda University, Loma Linda, CA, USA
Introduction: There are over a dozen medical shows airing on television, many of which are during prime time. Researchers have recently become more interested in the role of these shows, and the awareness on cardiopulmonary resuscitation. Several cases have been reported where a lay person resuscitated a family member using medical TV shows as a reference. The purpose of this study is to examine and evaluate college students’ perception on cardiopulmonary resuscitation and when to shock using an automated external defibrillator based on their experience of watching medical TV shows.
Methods: A total of 170 students (nonmedical major) were surveyed in four different colleges in the United States. The survey consisted of questions that reflect their perception and knowledge acquired from watching medical TV shows. A stepwise regression was used to determine the significant predictors of “How often do you watch medical drama TV shows” in addition to chi-square analysis for nominal variables.
Results: Regression model showed significant effect that TV shows did change students’ perception positively (p<0.001), and they would select shock on asystole as the frequency of watching increases (p=0.023).
Conclusion: The findings of this study show that high percentage of nonmedical college students are influenced significantly by medical shows. One particular influence is the false belief about when a shock using the automated external defibrillator (AED) is appropriate as it is portrayed falsely in most medical shows. This finding raises a concern about how these shows portray basic life support, especially when not following American Heart Association (AHA) guidelines. We recommend the medical advisors in these shows to use AHA guidelines and AHA to expand its expenditures to include medical shows to educate the public on the appropriate action to rescue an out-of-hospital cardiac arrest patient.
Keywords: medical shows, cardiopulmonary resuscitation, CPR, college student
Introduction
The introduction of a medical television shows was in 1951: City Hospital.1 Since then, medical shows range in content from drama and reality to comedy. Joseph Turow described how medical TV shows affect people’s perception of their physician in real life.2 He reflected on how physicians’ characters in these shows changed across time where it started to focus on the physicians’ personal life and relationship with staff vs patients’ life as it used to be since City Hospital was aired. Therefore, this can cause a negative perception to the audience when they visit their physicians. Other studies reported that lay rescuers with no medical background used medical shows to perform medical interventions on a victim. Eisenman et al3 reported two cardiac arrest resuscitations at their facility by a lay rescuer using medical knowledge acquired via medical shows. Hirt et al4 discussed medical drama on TV and whether it can be used as an educational tool. The authors suggested that a person can learn professionalism, mentorship, and procedures from the TV shows such as House; Scrubs, another prime time show, offers good teaching and learning styles, communication skills, and mentorship. Additionally, Grey’s Anatomy offers education on interpersonal conflict and the hospital environment. Hirt et al4 on the other hand, believe that these examples should be integrated into medical programs’ curriculum at various institutions. They view these medical shows as an engagement tool for learners.
In a Letter to the Editor of the journal of Resuscitation, Lederman explained how several medical TV shows ignore the victim’s family being present during resuscitation, where, in reality, they would be there.5 Diem et al discussed cardiopulmonary resuscitation (CPR) on TV after reviewing and watching several medical TV shows to record the number of cardiac arrests and their causes. They reported an increased level of survival rate of CPR cases compared with reality. Thus, these shows are creating a misperception of reality for patients and their families. The authors believe that the producers of these shows should recognize and have some civic responsibility to provide more accurate information given the huge influence of these TV shows.6
At the same time, according to the American Heart Association (AHA), four out of five cardiac arrests occur at home.7 This indicates that a bystander/lay rescuer most likely will have the first opportunity to attempt resuscitation in the majority of out-of-hospital cardiac arrest (OHCA) cases. In fact, there are reported cases where lay rescuers are asked what led them to attempt CPR without formal training or instructions; their responses were directed to information gained from medical TV show cardiac arrest scenes.8
In addition, various studies have evaluated the cardiac arrest scenes of medical TV shows. They concluded that these shows depict not only a higher than average patient survival rates but also inaccurate representations of CPR in contrast to CPR national guidelines and algorithms by AHA. An observed example is delivering a shock to a patient with an asystole heart rhythm.6,9–13
The AHA has turned its focus (38% of expenditure) to educating the public, or those without a medical background, in CPR.14 It was reported in 2013 that 40% of OHCA incidents were first resuscitated by a bystander with an overall 9.5% survival rate.7,15 AHA programs seek to find simple, stepwise methods for the lay person to focus on the critical, lifesaving steps of CPR while overcoming barriers that commonly impede bystanders from initiating CPR.31
With this in mind, brain research has shown that information presented on television is easily stored in our memory, especially when it involved emotions.16,17 This could explain why previous cases were able to help and resuscitate OHCA victims using knowledge acquired from medical shows. Therefore, with a plethora of medical TV shows being aired today, the purpose of this study was to examine the effect of medical TV shows on public/bystander perceptions, beliefs, and knowledge of medical concepts using theories and application from brain research as conceptual framework. This study hypothesized that as the viewer intensity or frequency of watching medical TV shows increases, their willingness to provide CPR increases. Another objective of this study was to investigate whether a bystander nonmedical person who is addicted to medical TV shows believes that a shock should be delivered when a patient is in asystole heart rhythm, due to watching medical TV shows.
Methods
Data collection
The survey was distributed electronically to the full student bodies of all participating institutions, after obtaining approval from each institution. The study was approved as exempt by Loma Linda University Institutional Review Board. Informed consent was provided at the beginning of the survey as the first question where they were able to view the consent and read it. Respondents had an option to either select “Yes-I would like to participate” or “No-I do not like to participate”. If “Yes” is selected, the survey starts automatically; if “No” is selected, the survey ends and they will be directed to a thank you page without seeing the survey questions. A total of 195 students were surveyed in this study. Among those, 25 did not complete the survey and, therefore, were excluded from the analysis. Thus, the data collection yielded a total of 170 usable surveys.
Questionnaire
The survey questions were grouped by themes (Table 1). The survey was reviewed by several AHA personnel for content validity. In one question, respondents were asked to observe three ECG rhythms (normal sinus, ventricular fibrillation, and asystole) and then answer based on their experience with medical TV shows.
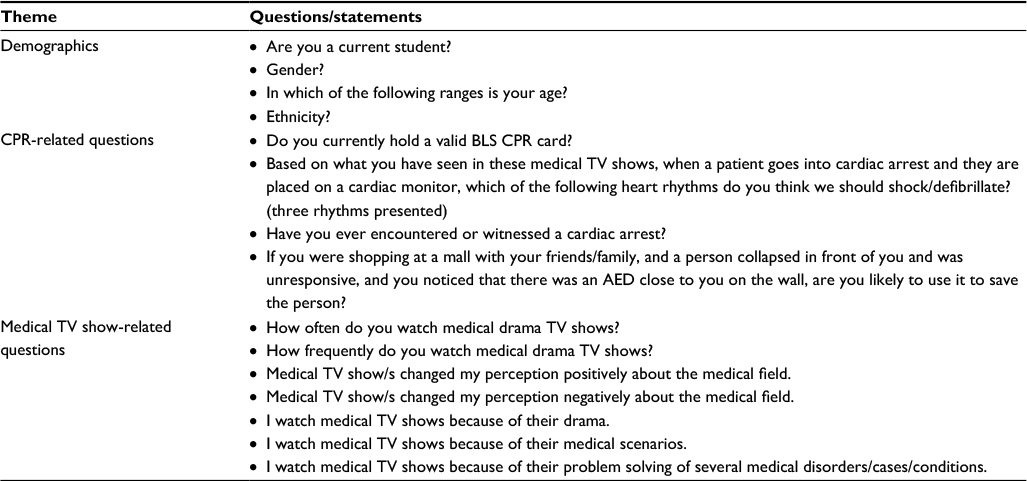 | Table 1 Key variables for the questionnaire included questions and themes concerning CPR and medical TV shows Note: The questions were grouped based on their content and were used in the analysis to test the presented hypothesis. Abbreviations: AED, automatic external defibrillator; BLS, basic life support; CPR, cardiopulmonary resuscitation. |
Data analysis
The data were analyzed using SPSS for Windows version 24.0 (IBM Corp., Armonk, NY, USA). A chi-square test was used to examine the relationships between watching medical TV shows, owning a CPR card, the frequency of watching medical TV shows, level of education, and witnessing a cardiac arrest. A stepwise regression analysis was conducted to determine the significant predictors of “How often do you watch medical drama TV shows?” The predictors examined were Gender, Age, “How frequently do you watch medical drama TV shows?”, “Medical TV show/s changed my perception positively about the medical field”, “Medical TV show/s changed my perception negatively about the medical field”, “I watch medical TV shows because of their drama”, “Based on what you have seen in these medical TV shows when a patient goes into cardiac arrest and they are placed on a cardiac monitor, which of the following heart rhythms do you think we should shock/defibrillate?”, “Have you encountered a cardiac arrest?”, “I watch medical TV shows because of their medical scenarios”, and “I watch medical TV shows because of their problem solving of several medical disorders/cases/conditions”. The level of significance was set at a p-value <0.05. Comments were also analyzed for qualitative analysis to examine emerging themes regarding medical shows.
Results
A total of 195 subjects started the survey, and 170 (87%) completed it. Graduate students accounted for 60% (n=103) of the completed survey respondents, and undergraduates accounted for 40% (n=67). With respect to gender, the participants included 21 males, 131 females, and one individual who declined to state his or her gender; the remainder did not respond to the question concerning gender. The majority of the respondents (47%) were between 18 and 24 years old (Table 2).
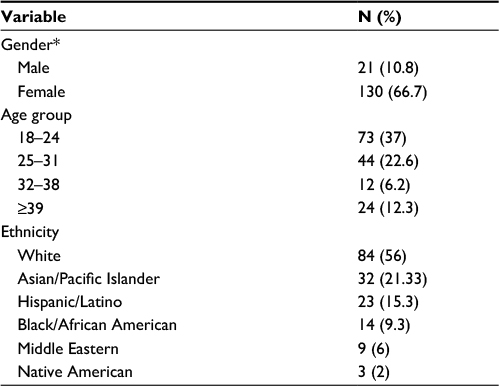 | Table 2 Frequency distribution of respondents’ demographic variables, N (%) Note: *Percentage do not adds up to 100 because of missing data. |
Of the respondents, only 18.8% (32) held a valid basic life support (i.e. CPR) card, and none of these had ever encountered or witnessed a cardiac arrest scene. Interestingly, 13 non-CPR card holders had encountered or witnessed a cardiac arrest scene. Of the CPR card holders, 18 reported having a card issued by the AHA. Of these, 88% (n=15) received the card after attending a formal AHA class.
Overall, 28% (n=42) of the respondents watched medical TV shows on a weekly basis. Of this group, 76% (n=32) believed that medical TV shows had positively changed their perceptions of the medical field, and 95% (n=40) of this same group denied having a negative perception of the field.
Overall, 62% (n=95) of the total respondents believed that medical TV shows had positively changed their perceptions about the medical field. In addition, 82% (n=125) denied that these shows had negatively changed their perceptions about the medical field. The respondents watched medical TV shows primarily because of their problem solving (75%), medical scenarios (40.79%), and drama (20%).
A chi-square test was performed to test the relationships between the nominal variables. There was a significant relationship between owning a CPR card and both witnessing a cardiac arrest (X2=5.92, p=0.015) and earning the card from an in-class session (X2(2)=31.0, p<0.001). In addition, a significant relationship was found between watching medical shows and both level of education (X2=17.7, p=0.001) and age range (X2=8.86, p=0.31). Specifically, younger individuals were more likely to watch medical TV shows.
A chi-square analysis was also performed to test the relationship between owning a CPR card and the frequency of watching medical TV shows. There was a significant association between having a CPR card and watching medical TV shows for their problem solving (p=0.033). There was also a significant association between holding a CPR card and being willing to rescue an OHCA victim (p<0.001).
The final regression model was ŷ=1.68+0.93 X1+0.38 X2+0.52 X3+0.28 X4+0.24 X5–0.28 X6.
The X values are defined as follows: X1= How frequent do you watch medical TV shows, X2= Medical shows changed perceptions positively, X3= Watching medical TV shows for drama, X4= Watching medical TV shows for medical scenarios, X5=Wave form selection, and X6= Medical shows changed perceptions negatively.
Results showed that 58% of the variability in the outcome is explained by these significant predictors (R2=57.7, F6,146=33.2, p<0.001). All of the coefficients in the above model were positive except for “TV shows have negative effect” which indicates that watching TV shows changed the perceptions positively (p<0.05). However, age, gender, watching shows for problem solving, and willingness to use an AED, and previously encountering cardiac arrest did not have a significant effect on the dependent variable (Table 3).
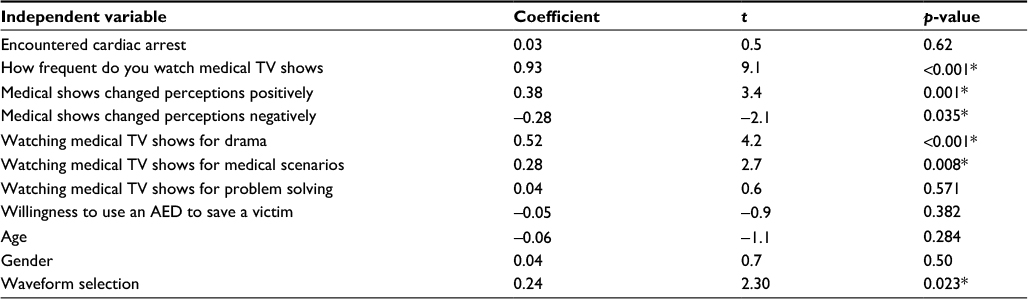 | Table 3 Results of the linear regression model examining the predictors of watching medical TV shows Note: *Significant at p<0.05. Abbreviation: AED, automatic external defibrillator. |
In addition to answering the described survey questions, the participants also reflected qualitatively about their overall experience of watching medical TV shows. Many students shared that one of the main reasons they watched these shows was because of the dramatic relationships these shows portray about the medical field. They believe that the primary focus of medical shows is the relationships among the medical staff members. For example, one subject shared, “I love ER, but the newer shows tend to stray away from the medical component and focus more on romance, which is not as interesting”. Other subjects similarly noted, “They tend to be more interested in the drama of the doctors and staff than medical accuracy”, “Too much drama, sleeping around. Not enough lifesaving messages”, and “Not really a fan of all the sexual relationships embedded in the story because they seem to be just for the sake of drawing in viewers that like to ‘ship’ characters”.
Many viewers also noted that they did not use medical shows as a source of learning. Most believed that whatever was portrayed in these shows was essentially unrealistic and could not be seen as medical learning experience. Examples of such comments were as follows: “Most are just for entertainment. They are not very realistic”, “It is a show, not for medical education”, and “They’re written for entertainment purposes. I certainly don’t take my medical advice from a TV show”.
On the other hand, other respondents explicitly referenced getting medical knowledge from medical TV shows, with some students stating that they watched medical shows for medical advice and/or knowledge. Some examples were as follows: “I’ve only ever watched House in terms of medical dramas, but I watched it religiously. Years later, I continue to amuse my friends with my faux medical knowledge, often throwing around terms like sarcoidosis”, and “They’re ridiculous. I only watch them for the drama. I also enjoy how they solve the medical problems because they’re always such strange treatments/diagnoses (I’m a biology student)”. These qualitative responses suggest that college students who watch medical TV shows do so for the problem solving and out of an interest in learning.
Discussion
To our knowledge, this is the first study to measure the student’s knowledge of and perceptions concerning the influence of medical TV shows. The results show that medical TV shows have a significant influence on college students, perhaps confirming why several medical TV shows are currently highly rated and aired during prime time.18
Most prior studies in this area have measured medical students’ or current medical staffs’ opinions and perceptions of medical TV shows. For example, Haboubi et al19 surveyed medical doctors of all grades to measure their reasons for and frequencies of watching medical TV shows. They discovered that a large portion of physicians watch such programs and that some even use them as a source of medical information.19 In their observational study, Lapostolle et al20 reported that the population (patients) and examinations (tests and procedures) in the TV show House M.D. were unrealistic. They noted that the discrepancies between the show’s portrayal of medicine and the reality might negatively impact patients’ understandings of how investigations and tests are performed.20 The results of the present study support Lapostolle et al’s20 findings by showing that there is a public misconception that confirms the ways in which tests and protocols that are performed in medical shows are unrealistic.
The findings of this study support the findings of Pfau et al21 and Chory-Assad and Tamborini,22 who showed that TV shows’ portrayals of medical staff may affect viewers’ perceptions of real medical professionals. In particular, the qualitative comments in the present study show that the portrayals of medical staff on medical TV shows imply that the medical field is about relationships and drama. This finding supports the conclusions drawn by Chory-Assad and Tamborini,22 who surveyed undergraduate students’ perceptions concerning the real roles of physicians in comparison to what was being portrayed on TV. They reported that higher exposure to medical TV shows results in a perception of physicians as unethical, tense, and inconsiderate. These results are consistent with our findings, which show that some students feel that characters in medical TV shows exhibit a high level of “drama”. This response may explain why many of the participants commented that they would not use the medical knowledge presented in a TV show as a source of information. This finding also suggests that organizations like the AHA should more closely monitor the resuscitation scenarios featured in medical shows. Furthermore, our results support Lee and Taylor’s1 findings that most viewers watch medical shows for their drama and problem-solving content and consider them solely as a source of entertainment. However, whereas Lee and Taylor’s study1 examined the reasons for viewers watching medical shows, this study investigated the possibility of a link between watching medical shows and being willing to deliver a shock via an AED to a person with a non-shockable heart rhythm.
In addition, the results of this study indicate a statistically significant relationship between watching medical TV shows and being willing to deliver a shock to help resuscitate a victim. This can be seen in the results of the regression model, which show that subjects who watch medical TV shows are more likely to attempt to resuscitate a victim and use an AED to deliver a shock. Furthermore, more than half of the participants identified the “asystole” heart rhythm as indicating a need to deliver a shock. Based on the presented theoretical framework, this finding suggests that the participants developed this misconception from medical TV shows.
Diem et al6 reported that medical TV shows depict an unrealistic cardiac arrest survival rate. Their finding supports the findings of this study, which show that cardiac arrest scenes are not regulated or monitored for accuracy in relation to AHA reports and guidelines. By itself, this finding is very concerning, given the dangers such perceptions can have for patients’ families in the clinical setting. Many hospitals have recently instituted policies to include family members in the resuscitation process.23–27 However, if a patient experiencing cardiac arrest exhibits an asystole heart rhythm, the presence of family members who are used to watching patients with asystole rhythms being shocked on medical TV shows may cause issues.
Moreover, the results of the regression model show that watching these medical shows contributes positively to the watchers’ perception, belief, and knowledge. For perception, the results showed that the more the person watches medical shows the more his/her perception changes positively (Coef= 0.38, p≤0.001). The findings of this variable were also consistent with the negative perception (Coef=−0.28, p=0.035). This basically means that they tended to move toward the positive since the coefficient is negative. Furthermore, the findings showed that the more the person watches medical shows, the more they will shock a patient in asystole. We believe that this finding is significant as it meets our main hypothesis and supports our theoretical framework. It appears that whatever is portrayed in these shows can be learned by the TV viewers and saved into their memory and belief. This finding does support the reported findings in science research where learning does occur while watching TV, even if it is for fun.28
Most medical shows retain medical advisors29; however, it seems that they do not implement AHA international guidelines in critical scenarios, such as cardiac arrest. We believe that our findings shed light on a critical opportunity to use medical shows as a platform for public education on OHCA scenarios. Therefore, it is recommended that organizations like the AHA regulate these platforms and use medical TV shows as channels for educating the public; especially, these shows already hiring medical advisors as a part of the team.
Limitations
The survey used in this study was distributed by key personnel (e.g., the Dean of Students) at each institution. These individuals emailed the survey link to their student bodies. Due to this distribution method, neither the author nor the distributors were able to identify the actual number of students who received the survey link. Furthermore, the total group of subjects included both current students and alumni, and the distributors were unable to differentiate among student classifications. This could represent a limitation to this study. As a result, our sample size was not that large. Furthermore, the surveyed respondents may not reflect the opinions of the general public. Expanding the study to other colleges and including more institutions could produce a better and clearer understanding of the wide variety of viewer perspectives on medical TV shows.
Future research
Future researchers should consider performing randomized observational studies, in which selected participants watch selected medical shows and then report their findings. It may also be helpful to collect both quantitative and qualitative baseline data from participants and then follow up with them for a minimum of 3 months. Such a study design could produce stronger and more controlled data concerning lay rescuers’ learning and ability to recall medical information. Research with qualitative outcomes should use gratification theory and mass communication as theoretical framework for explaining the complexity of viewers’ understanding of medical TV shows.30
Conclusion
The findings of this study indicate that there exists a relationship between watching medical shows and being willing to help others in emergency situations. This confirms that medical TV shows do have a positive effect on viewers. The high percentage of respondents believing that a shock should be delivered in the event of an asystole rhythm confirms our hypothesis that lay rescuers acquire misinformation from medical TV shows without the intent of acquiring them. Our qualitative analysis showed that most respondents watch these shows for nonmedical purposes. At the same time, they were able to recall what these shows portray when it comes to when to deliver a shock. We recommend that this finding needs to be tested further on a larger scale. Overall, the study findings indicate a need for health care individuals and organizations, such as medical technical advisors and the AHA, to engage in more comprehensive monitoring of medical TV shows. This way, they will ensure accurate information is being presented regarding CPR and AEDs on television. As a result, this will offer significant advantages in terms of educating the general public on how and what to do in an OHCA case.
Acknowledgments
We would like to thank the participating schools and students for their participation in this study. Special thanks to Dr. Evelyn Massey, Director of the AHA Life Support Education Center at Loma Linda University, for the time she took to review the survey for content validity. In addition, we would like to thank Mr. Louis Kelly for his time to review the manuscript as well.
Disclosure
The authors report no conflicts of interest in this work.
References
Lee TK, Taylor LD. The motives for and consequences of viewing television medical dramas. Health Commun. 2014;29(1):13–22. | ||
Turow J. Television entertainment and the US health-care debate. Lancet. 1996;347(9010):1240–1243. | ||
Eisenman A, Rusetski V, Zohar Z, Avital D, Stolero J. Can popular TV medical dramas save real life? Med Hypotheses. 2005;64(4):885–885. | ||
Hirt C, Wong K, Erichsen S, White JS. Medical dramas on television: a brief guide for educators. Med Teach. 2013;35(3):237–242. | ||
Lederman Z. Bioethics on TV – a case study. Resuscitation. 2012; 83(3):e91. | ||
Diem SJ, Lantos JD, Tulsky JA. Cardiopulmonary resuscitation on television. Miracles and misinformation. N Engl J Med. 1996;334(24):1578–1582. | ||
Association AH. CPR Statistics: CPR & Sudden Cardiac Arrest (SCA); 2011. Available from: http://www.heart.org/HEARTORG/CPRAndECC/WhatisCPR/CPRFactsandStats/CPR-Statistics_UCM_307542_Article.jsp. Accessed November, 2014. | ||
Eisenman A, Rutetski V, Zohar Z, Stolero J. Subconscious passive learning of CPR techniques through television medical drama. Australasian J Paramed. 2005;3(3). | ||
Baer NA. Cardiopulmonary resuscitation on television. Exaggerations and accusations. N Engl J Med. 1996;334(24):1604–1605. | ||
Hinkelbein J, Spelten O, Marks J, Hellmich M, Bottiger BW, Wetsch WA. An assessment of resuscitation quality in the television drama Emergency Room: guideline non-compliance and low-quality cardiopulmonary resuscitation lead to a favorable outcome? Resuscitation. 2014;85(8):1106–1110. | ||
Portanova J, Irvine K, Yi JY, Enguidanos S. It isn’t like this on TV: Revisiting CPR survival rates depicted on popular TV shows. Resuscitation. 2015;96:148–150. | ||
Van den Bulck JJ. The impact of television fiction on public expectations of survival following inhospital cardiopulmonary resuscitation by medical professionals. Eur J Emerg Med. 2002;9(4):325–329. | ||
Harris D, Willoughby H. Resuscitation on television: realistic or ridiculous? A quantitative observational analysis of the portrayal of cardiopulmonary resuscitation in television medical drama. Resuscitation. 2009;80(11):1275–1279. | ||
Association AH. History of the American Heart Association; 2015. Available from: http://www.heart.org/HEARTORG/General/History-of-the-American-Heart-Association_UCM_308120_Article.jsp -.VzCx9IQrKUk. Accessed May 05, 2016. | ||
Sasson C, Meischke H, Abella BS, et al. Increasing cardiopulmonary resuscitation provision in communities with low bystander cardiopulmonary resuscitation rates: a science advisory from the American Heart Association for healthcare providers, policymakers, public health departments, and community leaders. Circulation. 2013;127(12):1342–1350. | ||
Krugman HE. Processes underlying exposure to advertising. Am Psychol. 1968;23(4):245–253. | ||
Krugman HE, Hartley EL. Passive learning from television. Public Opin Quart. 1970;34(2):184190. | ||
Nielsen. Nielsen Twitter TV Ratings; 2016. Available from: http://www.nielsensocial.com/nielsentwittertvratings/weekly/. Accessed May 1, 2016. | ||
Haboubi HN, Morgan H, Aldalati O. Hospital doctors’ Opinions regarding educational Utility, public Sentiment and career Effects of Medical television Dramas: the HOUSE MD study. Med J Aust. 2015;203(11):462–466. | ||
Lapostolle F, Montois S, Alheritiere A, De Stefano C, Le Toumelin P, Adnet F. Dr House, TV, and reality. Am J Med. 2013;126(2):171–173. | ||
Pfau M, Mullen LJ, Garrow K. The Influence of television viewing on public perceptions of physicians. J Broadcast Electron. 1995;39(4):441–458. | ||
Chory-Assad RM, Tamborini R. Television exposure and the public’s perceptions of physicians. J Broadcast Electron. 2003;47(2):197–215. | ||
Goldberger ZD, Nallamothu BK, Nichol G, et al. Policies allowing family presence during resuscitation and patterns of care during in-hospital cardiac arrest. Circ Cardiovasc Qual Outcomes. 2015;8(3):226–234. | ||
Jabre P, Belpomme V, Azoulay E, et al. Family presence during cardiopulmonary resuscitation. N Engl J Med. 2013;368(11):1008–1018. | ||
Lederman Z, Wacht O. Family presence during resuscitation: attitudes of Yale-New Haven Hospital staff. Yale J Biol Med. 2014;87(1):63–72. | ||
Oczkowski SJ, Mazzetti I, Cupido C, Fox-Robichaud AE. The offering of family presence during resuscitation: a systematic review and meta-analysis. J Intensive Care. 2015;3:41. | ||
Oczkowski SJ, Mazzetti I, Cupido C, Fox-Robichaud AE; Canadian Critical Care S. Family presence during resuscitation: a Canadian Critical Care Society position paper. Can Respir J. 2015;22(4):201–205. | ||
Beste C, Dinse HR. Learning without training. Curr Biol. 2013;23(11): R489–R499. | ||
Chanchlani N. Medics in the media; 2011. Available from: http://careers.bmj.com/careers/advice/Medics_in_the_media. Accessed April 15, 2017. | ||
Rubin AM. An Examination of television viewing motivations. Commun Res. 1981;8(2):141–165. | ||
Abella BS, Aufderheide TP, Eigel B, et al. Reducing barriers for implementation of bystander-initiated cardiopulmonary resuscitation: a scientific statement from the American Heart Association for healthcare providers, policymakers, and community leaders regarding the effectiveness of cardiopulmonary resuscitation. Circulation. 2008;117(5):704–709. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.