")
Back to Journals » Nature and Science of Sleep » Volume 13
COVID-19 Vaccine Could Trigger the Relapse of Secondary Hypersomnia
Authors Wu M, Li SX , Xue P, Zhou J, Tang X
Received 22 October 2021
Accepted for publication 15 December 2021
Published 29 December 2021 Volume 2021:13 Pages 2267—2271
DOI https://doi.org/10.2147/NSS.S345801
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ahmed BaHammam
Min Wu,1,2 Shirley Xin Li,3,4 Pei Xue,5 Junying Zhou,5 Xiangdong Tang5
1West China School of Nursing, Sichuan University/Sleep Medicine Center, West China Hospital, Sichuan University, Chengdu, Sichuan Province, People’s Republic of China; 2Shihezi University School of Medicine, Shihezi University, Shihezi, Xinjiang Province, People’s Republic of China; 3Department of Psychology, The University of Hong Kong, Pokfulam, Hong Kong Special Administrative Region, People’s Republic of China; 4The State Key Laboratory of Brain and Cognitive Sciences, The University of Hong Kong, Pokfulam, Hong Kong Special Administrative Region, People’s Republic of China; 5Sleep Medicine Center, West China Hospital, Sichuan University, Chengdu, Sichuan Province, People’s Republic of China
Correspondence: Junying Zhou; Xiangdong Tang
Sleep Medicine Center, West China Hospital, Sichuan University, 28 Dian Xin Nan Jie, Chengdu, Sichuan Province, 610041, People’s Republic of China
Tel +86 189 8060 6836; +86 28 8542 2733
Fax +86 28 8542 2632
Email [email protected]; [email protected]
Abstract: The coronavirus disease (COVID-19) has brought significant social and economic disruptions and devastating impacts on public health, and vaccines are being developed to combat the disease. Timely vaccination may prevent complications and morbidity but may also potentially result in unforeseen outcomes in some special clinical populations. We report on a case of hypersomnia relapse after the COVID-19 vaccination, with the aim of informing the development of the guideline on vaccination in specific groups. A 19-year old female presented with persistent daytime sleepiness after receiving the COVID-19 vaccine. She had a known history of hypersomnia secondary to infectious mononucleosis but has fully recovered for 8 months. A series of examinations were performed on this patient. Neurologic and psychiatric examinations were unremarkable. Despite normal nocturnal subjective sleep quality (Pittsburgh Sleep Quality Index score = 5, Insomnia Severity Index score = 7), her Epworth sleepiness scale score (15) suggested an abnormal level of subjective sleepiness. Consistent with the subjective report, the objective assessment by Multiple Sleep Latency Test found mean sleep latency was 1.3 min with no sleep onset rapid-eye-movement (REM) period. We speculate that COVID-19 vaccine may potentially trigger the relapse of hypersomnia. The immune memory could be an explanation for the increased response to vaccine in patients with secondary hypersomnia. Caution should be warranted when administering COVID-19 vaccine in patients with hypersomnia secondary to infections.
Keywords: SARS-CoV-2, COVID-19 vaccine, pandemic, excessive daytime sleepiness, hypersomnia
Introduction
The outbreak of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has resulted in substantial morbidity and mortality worldwide. This pandemic may also result in significant adverse psychosocial impacts, including increasing the incidence of mental health problems and the risk for sleep problems.1–4 Recently, two systematic reviews showed a high prevalence of sleep problems both in the general populations and the patients with COVID-19.5,6 Remarkably, 33.01% of the patients with SARS-CoV-2 infection presented with daytime sleepiness.7 In addition, two cases of Kleine-Levin Syndrome were reported to have relapsed due to SARS-CoV-2.8,9
Nowadays, there is a pressing need to receive COVID-19 vaccine, which is an essential tool to overcome the pandemic.10 A multinational randomized controlled trial has confirmed that a two-dose regimen of BNT162b2 mRNA could result in 95% protection against COVID-19 in individuals aged 16 years or above.11 However, as for anything biologically active, the vaccine may carry potential risks of causing adverse effects in vulnerable individuals.12 For example, a sudden increase in the incidence of narcolepsy was reported in several European countries following the pandemic influenza A (H1N1) vaccination campaign with Pandemrix.13 It is worth noting that previous studies have reported that sleepiness was one of the most common adverse events, with up to 62.5% cases complaining of sleepiness after the administration of COVID-19 vaccines.14–16 Therefore, the potential risks related to the administration of the vaccines in those vulnerable individuals need to be carefully considered. We herein report a novel case of hypersomnia relapse, possibly due to COVID-19 vaccination. The findings may have implications for informing guidelines development and clinical decision-making with regard to administering COVID-19 vaccine in patients with secondary hypersomnia.
Case Report
A 19-year old female was admitted into our sleep medicine center with a complaint of excessive daytime sleepiness (EDS) lasting for 10 days. It was clear that the patient received the first dose of COVID-19 vaccine (CoronaVac, an inactivated whole-virion SARS-CoV-2 vaccine developed by Sinovac Life Sciences (Beijing, China)) one day prior to the occurrence of EDS. In addition, the patient presented with red and itchy bumps on her skin after one week of EDS.
Notably, the patient had a known history of hypersomnia secondary to infectious mononucleosis (IM) caused by Epstein - Barr virus (EBV) infection verified by serologic testing for mononucleosis from age 13. At the worst time, her total sleep time was 16 hours per day and 18 hours during menstruation. The persistent EDS had resulted in her significant difficulty in staying alert at school, and she had to suspend her study and stay home for two years. She was initially presented to our sleep medicine center in November 2018 (at age 16). We conducted a series of examinations including blood test, brain MRI, nocturnal polysomnography (PSG) and Multiple Sleep Latency Test (MSLT). The results of her blood tests (eg TNF-α, CRP, IL-6, IL-10, IL-1β) and MRI were normal. Remarkably, she presented with a significant subjective EDS as reflected by Epworth sleepiness scale (ESS) score of 23 (cutoff score = 10). In addition, MSLT results showed mean sleep latency (SL) was 5 minutes with no sleep onset REM period (SOREMP). The patient was subsequently diagnosed with hypersomnia secondary to IM and received regular treatment for hypersomnia using Methylphenidate and Sertraline in December 2018. When she was followed up in August 2020 (at age 18), the symptom of EDS was found to be significantly improved. By October 2020, the patient no longer reported any daytime sleepiness (eg ESS score = 6) even after stopping drug treatment for 2 months. The subjective sleep assessments also showed that she had a reasonably good nocturnal sleep (Pittsburgh Sleep Quality Index (PSQI) score = 1, Insomnia Severity Index (ISI) score = 1). The total sleep time decreased to 9 hours per day even during the menstruation. Moreover, she was able to actively participate in school life and social activities.
When the patient was presented to our center again in June 2021, she reported EDS and the total sleep time was approximately 13 hours per day. She could not get up at the usual rise time and reported feeling excessive sleepiness throughout the day. A series of reexaminations except blood test (rejected by the patient) were conducted. Neurologic and psychiatric examinations were unremarkable. MSLT showed that mean SL was 1.3 minutes with no SOREMP. Her ESS score (15) was suggestive of an abnormal level of sleepiness, while she had a fair nocturnal sleep quality (ISI score = 7; PSQI score = 5). The patient was subsequently given the same prescription (Methylphenidate and Sertraline) and was followed up regularly in our clinic. However, she continued to complain about EDS until October 2021. A timeline of the events is shown in Figure 1.
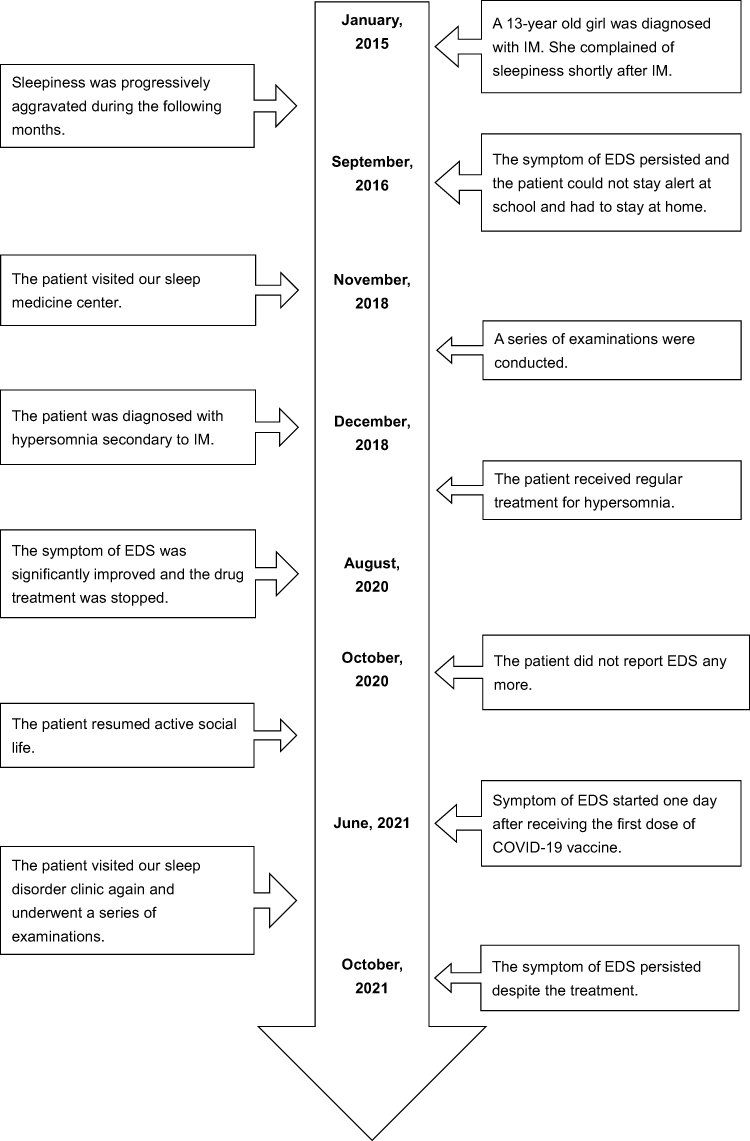 |
Figure 1 Timeline of events. Abbreviations: IM, infectious mononucleosis; EDS, excessive daytime sleepiness. |
Discussion
The ICSD-3 classifies eight different central disorders of hypersomnolence, in which hypersomnia due to a medical disorder is a common condition.17 In the current case, the patient progressively developed hypersomnia after IM caused by EBV infection. She was definitely a case of infection-induced hypersomnia and recovered after a few years of treatment. Unfortunately, hypersomnia recurred shortly after she received the vaccine for COVID-19. We speculated that EDS was induced by the COVID-19 vaccine based on the clinical history and a lack of other precipitating factors.
EBV is a human herpesvirus, which infects essentially all human beings across the life span and is carried out as a lifelong asymptomatic infection in the B lymphoid system.18 When the virus–host balance is disturbed, a range of virus-associated diseases may then ensue, such as IM and certain autoimmune conditions.19 A study conducted in the college students infected by IM reported that the diurnal somnolence was more prominent, as compared to other infections in convalescent phases.20 Two other retrospective studies also reported hypersomnia secondary to the IM infection.21,22 In particular, Sforza et al proposed that autoinflammatory processes and immune dysregulation mechanism might result in hypersomnia in patients with IM.21
The COVID-19 pandemic has negatively affected sleep health in the general population.23 Furthermore, sleep impairment was the most frequent symptom in patients with SARS-CoV-2.7 Sleep quality was found to be significantly decreased even after recovery of COVID-19 in those infected individuals.24 It was also documented that preexisting EDS was significantly associated with the risk of mortality and hospitalization in patients infected by COVID-19.25 Thus, there could be a close link between COVID-19 and EDS, albeit that the underlying mechanism remained unclear.
Vaccines are well known as one of the most effective ways to prevent diseases and their complications. The development of effective COVID-19 vaccines may change the course of the current pandemic.15 However, the immune response activated by a vaccine could be good or bad depending on individual reactions, especially for some specific cases with autoimmune diseases.12 When a specific area of the central nervous system (CNS), which generates and modulates sleep, is disrupted in response to the abnormal immune reaction, the patients may experience EDS.26 Lippert et al found an association of activated T-cells in the CNS with increased EDS, which provided further evidence suggesting T-cell-mediated neuronal damage and autoimmunity in hypersomnia.27 Furthermore, previous studies indicated that influenza H1N1 infection and some influenza vaccines might lead to selective immune-mediated destruction of orexin-producing neurons, which triggered the development of narcolepsy.28 In addition, it has been suggested that an acute infection or a vaccine could alter the immune system thereby resulting in an increased but non-specific response against reinfection, which is named “immune memory”.29 Interestingly, sleep duration at the time of vaccination was found to potentially affect the immune response and boost the virus-specific adaptive cellular immunity.30 Therefore, we hypothesized that the autoimmune process elicited by increased response to vaccine could possibly play a potential role in the pathogenesis of hypersomnia secondary to COVID-19 vaccination, but we were unable to confirm the underlying cause because the patient refused to take part in further examinations on immune function.
Based on the available evidence, it remained unclear whether the benefits of COVID-19 vaccine far outweigh the risks in patients with a history of hypersomnia secondary to infections. Given the urgency of achieving an effective control over COVID-19 pandemic globally, we strongly advocate planning carefully when administering vaccines in certain special populations. It is necessary to update and review the newly available evidence of COVID-19 vaccine and make timely clinical recommendations so as to facilitate the clinicians and patients to make their informed decision. To date, some guidance statements were made based on the consensus to provide the directions on the use of the COVID-19 vaccine in the individuals with certain autoimmune and inflammatory diseases.10 We strongly suggest the administrative departments to review the existing evidence and establish specific guidelines on the administration of COVID-19 vaccine in the patients with hypersomnia secondary to infections.
Several limitations should be noted in this study. First, we were unable to verify our hypothesis due to a lack of blood tests for examining the amount of antibodies and the level of inflammation after the COVID-19 vaccination in this case. Second, this is a clinical case report in which the findings may not be generalizable to the general population. Prophylactic COVID-19 vaccines are still urgently needed to control the ongoing pandemic and reduce the devastating medical, economic and social impacts associated with COVID-19.11 Nonetheless, for patients with hypersomnia secondary to infections, it is critical to weigh up the pros and cons of getting COVID-19 vaccines due to the risk of developing EDS.
Conclusion
The current study presented an unusual case where a patient with a history of hypersomnia due to IM infection had a relapse of EDS shortly after receiving the COVID-19 vaccine. The potential pathogenesis of the hypersomnia relapse may be associated with an autoimmune mechanism. Our finding emphasized the need for carefully planning and establishing a guideline on the administration of COVID-19 vaccines in vulnerable individuals. More attention should be directed to the unexpected outcomes following COVID-19 vaccination in the patients with hypersomnia secondary to infections.
Ethical Standard Statement
This study was approved by the ethics committees of West China Hospital of Sichuan University. Written informed consent for publication of their details was obtained from the patient.
Acknowledgments
We thank the patient and her family for their cooperation.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval for the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Project of Sichuan Science and Technology Agency (grant no. 2020YJ0279).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhou J, Liu L, Xue P, Yang X, Tang X. Mental health response to the COVID-19 outbreak in China. Am J Psychiatry. 2020;77(5):574–575. doi:10.1176/appi.ajp.2020.20030304
2. Wu M, Ren J, Li SX, Xue P, Su C, Zhou J. Management of narcolepsy during COVID-19: a challenge or an opportunity? Sleep. 2021;44(2):zsaa273. doi:10.1093/sleep/zsaa273
3. Nigam M, Hippolyte A, Dodet P, et al. Sleeping through a pandemic: impact of COVID-19 related restrictions on narcolepsy and idiopathic hypersomnia. J Clin Sleep Med. 2021:1–18. doi:10.5664/jcsm.8990
4. Ainge-Allen HW, Yee BJ, Ip MSM. Contemporary concise review 2020: sleep. Respirology. 2021;26(7):700–706. doi:10.1111/resp.14084
5. Lin YN, Liu ZR, Li SQ, et al. Burden of sleep disturbance during COVID-19 pandemic: a systematic review. Nat Sci Sleep. 2021;13:933–966. doi:10.2147/NSS.S312037
6. Jahrami H, BaHammam AS, Bragazzi NL, Saif Z, Faris M, Vitiello MV. Sleep problems during the COVID-19 pandemic by population: a systematic review and meta-analysis. J Clin Sleep Med. 2021;17(2):299–313. doi:10.5664/jcsm.8930
7. Liguori C, Pierantozzi M, Spanetta M, et al. Subjective neurological symptoms frequently occur in patients with SARS-CoV2 infection. Brain Behav Immun. 2020;88:11–16. doi:10.1016/j.bbi.2020.05.037
8. Marčić M, Marčić L, Marčić B. SARS-CoV-2 infection causes relapse of Kleine-Levin syndrome: case report and review of literature. Neurol Int. 2021;13(3):328–334. doi:10.3390/neurolint13030033
9. Nasrullah A, Javed A, Ashraf O, Malik K. Possible role of COVID-19 in the relapse of Klein-Levin syndrome. Respir Med Case Rep. 2021;33:101445. doi:10.1016/j.rmcr.2021.101445
10. Curtis JR, Johnson SR, Anthony DD, et al. American college of rheumatology guidance for COVID-19 vaccination in patients with rheumatic and musculoskeletal diseases: version 1. Arthritis Rheumatol. 2021;73(7):1093–1107. doi:10.1002/art.41734
11. Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA covid-19 vaccine. N Engl J Med. 2020;383(27):2603–2615. doi:10.1056/NEJMoa2034577
12. Mignot E, Black S. Narcolepsy risk and COVID-19. J Clin Sleep Med. 2020;16(10):1831–1833. doi:10.5664/jcsm.8668
13. Hallberg P, Smedje H, Eriksson N, et al. Pandemrix-induced narcolepsy is associated with genes related to immunity and neuronal survival. EBioMedicine. 2019;40:595–604. doi:10.1016/j.ebiom.2019.01.041
14. Sakinah EN, Nugraha MY, Qodar TS, Mulyono BW, Tohari AI. COVID-19 vaccines programs: adverse events following immunization (AEFI) among medical clerkship student in Jember, Indonesia. BMC Pharmacol Toxicol. 2021;22(1):58–64. doi:10.1186/s40360-021-00528-4
15. Kaya F, Pirincci E. Determining the frequency of serious adverse reactions of inactive SARS-COV-2 vaccine. Work. 2021;69(3):735–739. doi:10.3233/WOR-210473
16. Tran VN, Nguyen HA, Le TTA, Truong TT, Nguyen PT, Nguyen TTH. Factors influencing adverse events following immunization with AZD1222 in Vietnamese adults during first half of 2021. Vaccine. 2021;39(44):6485–6491. doi:10.1016/j.vaccine.2021.09.060
17. American Academy of Sleep Medicine. International Classification of Sleep Disorders.
18. Houen G, Trier NH. Epstein-Barr virus and systemic autoimmune diseases. Front Immunol. 2021;11:587380. doi:10.3389/fimmu.2020.587380
19. Taylor GS, Long HM, Brooks JM, Rickinson AB, Hislop AD. The immunology of Epstein-Barr virus-induced disease. Annu Rev Immunol. 2015;33:787–821. doi:10.1146/annurev-immunol-032414-112326
20. Lambore S, McSherry J, Kraus AS. Acute and chronic symptoms of mononucleosis. J Fam Pract. 1991;33(1):33–37.
21. Sforza E, Hupin D, Roche F. Mononucleosis: a possible cause of idiopathic hypersomnia. Front Neurol. 2018;9:922–925. doi:10.3389/fneur.2018.00922
22. Guilleminault C, Mondini S. Mononucleosis and chronic daytime sleepiness. A long-term follow-up study. Arch Intern Med. 1986;146(7):1333–1335. doi:10.1001/archinte.1986.00360190107014
23. Simonelli G, Petit D, Delage JP, et al. Sleep in times of crises: a scoping review in the early days of the COVID-19 crisis. Sleep Med Rev. 2021;60:101545. doi:10.1016/j.smrv.2021.101545
24. Bozan Ö, Atiş Ş, Çekmen B, Şentürk M, Kalkan A. Healthcare workers’ sleep quality after COVID-19 infection: a cross-sectional study. Int J Clin Pract. 2021;75(11):e14772. doi:10.1111/ijcp.14772
25. Li P, Zheng X, Ulsa MC, et al. Poor sleep behavior burden and risk of COVID-19 mortality and hospitalization. Sleep. 2021;44(8):zsab138.
26. Iranzo A. Sleep and neurological autoimmune diseases. Neuropsychopharmacology. 2020;45(1):129–140. doi:10.1038/s41386-019-0463-z
27. Lippert J, Young P, Gross C, et al. Specific T-cell activation in peripheral blood and cerebrospinal fluid in central disorders of hypersomnolence. Sleep. 2019;42(2):1–9. doi:10.1093/sleep/zsy223
28. Bassetti CLA, Adamantidis A, Burdakov D, et al. Narcolepsy - clinical spectrum, aetiopathophysiology, diagnosis and treatment. Nat Rev Neurol. 2019;15(9):519–539. doi:10.1038/s41582-019-0226-9
29. Netea MG, Schlitzer A, Placek K, Joosten LAB, Schultze JL. Innate and adaptive immune memory: an evolutionary continuum in the host’s response to pathogens. Cell Host Microbe. 2019;25(1):13–26. doi:10.1016/j.chom.2018.12.006
30. Benedict C, Cedernaes J. Could a good night’s sleep improve COVID-19 vaccine efficacy? Lancet Respir Med. 2021;9(5):447–448. doi:10.1016/S2213-2600(21)00126-0
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.