")
Back to Journals » International Journal of Women's Health » Volume 14
COVID-19 Vaccine Acceptance in Pregnant and Lactating Women and Mothers of Young Children in Poland
Authors Kuciel N, Mazurek J, Hap K , Marciniak D, Biernat K, Sutkowska E
Received 16 November 2021
Accepted for publication 23 February 2022
Published 28 March 2022 Volume 2022:14 Pages 415—424
DOI https://doi.org/10.2147/IJWH.S348652
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Natalia Kuciel,1 Justyna Mazurek,1 Katarzyna Hap,1 Dominik Marciniak,2 Karolina Biernat,1 Edyta Sutkowska1
1University Centre of Rehabilitation, Wroclaw Medical University, Wroclaw, Poland; 2Department of Drugs Form Technology, Wroclaw Medical University, Wroclaw, Poland
Correspondence: Katarzyna Hap, University Centre of Rehabilitation, Wroclaw Medical University, Borowska St. 213, Wroclaw, Poland, Tel +48/717343220, Email [email protected]
Purpose: The World Health Organization indicated vaccine hesitancy as one of the top 10 threats to global health. The success of a vaccine depends not only on its efficacy but also on its acceptance. Our study aims to define COVID-19 vaccine acceptance in a sample of pregnant and lactating women in Poland. Since mothers are often key decision-makers for whether their children will receive vaccination, it is vital to measure vaccine confidence among this group.
Patients and Methods: An anonymous online survey was distributed to assess the level of acceptance of COVID-19 vaccination among pregnant and lactating women for themselves and their children in Poland.
Results: The trust of pregnant and breastfeeding women and women who have offspring in government, in healthcare professionals, in scientific authorities, and sound scientific data is strongly associated with vaccine acceptance and may influence an individual’s decision to perceive recommended actions as beneficial to the society as a whole.
Conclusion: Acceptance and confidence in receiving the COVID-19 vaccination among pregnant and lactating women and mothers with young children is strongly associated with feelings of trust in government, health professionals, scientific authorities, and sound scientific data. The dissemination of professional and reliable information regarding the safety and efficacy of COVID-19 vaccine uptake by qualified health care personnel can significantly increase the level of trust and public awareness regarding the safety and efficacy of COVID-19 vaccine uptake in pregnancy, while breastfeeding, and mothers with young children.
Keywords: COVID-19, vaccination, breastfeeding, pregnancy, acceptance of vaccination
Introduction
By the end of 2021, the total number of COVID-19 cases will reach more than 234 million worldwide, and the number of deaths from SARS-CoV-2 related causes will hit 4.8 million.1 Pregnant women are at high risk of severe illness, intensive care unit admission (3 times more likely), and invasive ventilation (1.5 times more likely) when compared with non-pregnant women of the same age.2 Children appear to have a lower risk for symptomatic SARS-CoV-2 but similar rates of infection. It makes children the potential transmitters of SARS-CoV-2.3
Vaccine for SARS-CoV-2 is the most promising mean of controlling the spread of the COVID-19 pandemic.4 On the one hand, the Joint Committee on Vaccination and Immunisation (in line with recommendations from the USA and the WHO) advises that pregnant women should be offered COVID-19 vaccines at the same time as people of the same age or risk group and recommends that the vaccines can be received while breastfeeding.5 On the other hand, unfortunately, the COVID-19 vaccine trials generated minimal data on safety and efficacy for pregnant and lactating women and children.6 This is because pregnant and lactating women are excluded from all clinical trials on COVID-19 vaccines. It means that we still have scant available data on vaccine safety and efficacy in pregnant and lactating women. For example, in the United States, according to the data from Vaccine Safety Datalink, only 16.3% of pregnant women received one or more doses of a COVID-19 vaccine during pregnancy (data from May 2021).7
The success of a vaccine depends not only on its efficacy but also on its acceptance. Even the most successful vaccines cannot combat the epidemic without widespread acceptance. Unfortunately, despite considerable progress in vaccine development and administration, the current acceptance level remains inadequate to meet the requirements for developing so-called herd immunity – the community immunity level needs to reach at least 75% to stop the SARS-CoV-2 pandemic.8 In addition, the World Health Organization indicated vaccine hesitancy as one of the top 10 threats to global health. This information predates the SARS-CoV-2 pandemic.9,10 Because of that, it is imperative to understand and indicate the reason for vaccine hesitancy and the level of vaccine acceptance.
While millions of women have become pregnant, given birth, and initiated breastfeeding during the SARS-CoV-2 pandemic, it is important to understand patient perception and barriers to vaccine acceptance as a crucial key factor in helping to end the pandemic. To our best knowledge, there have been no data on vaccine acceptance for pregnant and lactating women and those having young children in Poland. Therefore, we hypothesized that pregnant and lactating women would avoid the COVID-19 vaccine because of the available data inconsistency. Our study aims to define COVID-19 vaccine acceptance in a sample of pregnant and lactating women in Poland. Since mothers are often key decision-makers for whether their children will receive vaccination, it is vital to measure vaccine confidence among this group.
Materials and Methods
Study Design
An anonymous online survey (Appendix) was distributed between July 1, 2021, and August 30, 2021, to assess the level of acceptance of COVID-19 vaccination among pregnant and lactating women for themselves and their children in Poland. The survey included women aged 18 and older who were pregnant, breastfeeding, and/or had children under 18. Predictors assessed included sociodemographic data (pregnancy, breastfeeding, having children and number of children, age, marital status, education).
Further questions concerned general vaccine attitude, level of trust in healthcare in Poland, assessment of fear of COVID-19, confidence in safety and effectiveness of COVID-19 vaccination, and trust in government institutions and science. Question 13 (As the COVID-19 vaccination has been found 90% safe and effective and is available, do you want to get vaccinated?) applied only to pregnant and non-pregnant and breastfeeding women. Question 14 (As the COVID-19 vaccination has been found 90% safe and effective and is available, do you want to vaccinate your child?) only addressed the level of acceptance toward vaccinating their children.
A Likert scale (strongly disagree/disagree/neither agree nor disagree/agree/strongly agree and not at all/no/rather not/neither yes nor no/rather yes/yes/very much) was used to determine the degree of acceptance. All study participants were informed about the purpose of the work and the standards for archiving and anonymizing data. The survey was hosted on a social media platform on parenting and breastfeeding forums. Interested people clicked on the link, and a questionnaire was opened, ready to be filled in.
Ethics
The study was approved by the Bioethics Committee of the Medical University in Wroclaw, No. KB-761/2021.
Statistical Methods
For statistical evaluation, the results of the Likert scale questionnaire were integrated into three responses: agree/neither agree nor disagree/disagree and yes/neither yes nor no/no).
The data analyzed in this study, including survey results and demographic data collected from study participants (N = 118), were nominal variables, including dichotomous variables. Therefore, the choice of statistical tests performed was dictated by the nature of the variables obtained.
For all variables, count tables containing absolute raw counts and each category’s percentage and cumulative contribution to the nominal variable were determined. The main statistical inference was based on the results of two different computational procedures suitable for analyzing dependent variables based on nominal scales: non-parametric analysis using Pearson’s Chi-square statistic calculated for multivariate tables and univariate and multivariate logistic regression. When the expected values calculated based on Person’s Chi-square statistic were smaller than 10, the Yates correction for small numbers was considered when assessing the statistical significance of differences between the compared subgroups.
For dichotomous dependent variables, univariate and multivariate logistic regression was performed. Based on its results, an odds ratio (OR), statistical significance (p), and 95% confidence interval were determined for the obtained estimator value.
General relationships between all statistically evaluated variables were analyzed and then visualized using multivariate analyses based on dimension reduction utilizing the procedure of decomposition of the matrix of results according to singular values: principal component analysis (PCA) and correspondence analysis. The constructed PCA models were estimated using the NIPALS iterative algorithm, with the convergence criterion set at 0.00001 and the maximum number of iterations corresponding to 100. The number of principal components was determined by determining the maximum predictive ability of Q2 using the V-fold cross-validation method, setting the maximum number of them at Vmax = 7.
PCA allowed us to pre-select the variables that have the most significant influence on the built model and select the most significant relationships among them. Thus, selected variables were then subjected to further statistical evaluation.
In all statistical analyses performed, the assumed significance level was α = 0.05. Statistical analyses were carried out using STATISTICA PL ® version 13.
Results
Sociodemographic Data
Out of 118 respondents, 28 (23.73%) women were pregnant, 60 (50.84%) were breastfeeding, and 109 (92.37%) had children. Furthermore, 51 (44.07%) had one child, 50 (42.37%) had two children, and 7 women (5.91%) had 3 and 4 children. The largest group, ie, 55 individuals, constituted women aged 30–35 (46.61%); moreover, 106 (89.83%) had higher education, and 102 (86.44%) were married.
Correlation Analysis Between Sociodemographic Data and Survey Questions
Statistically significant results for pregnant women indicated that they have confidence in government health institutions as opposed to non-pregnant women (p=0.002). Pregnant women are 4 times more likely to trust government health information than non-pregnant women (OR = 4.150; p = 0.009).
Breastfeeding women declared that they vaccinate their children as opposed to non-breastfeeding women (p=0.001). Moreover, breastfeeding women expressed trust in health services (p=0.039). They had confidence in COVID-19 vaccination with regard to its safety and effectiveness (p=0.023; p=0.010). Therefore, they were determined to get vaccinated themselves (p=0.006) and have their children vaccinated against COVID-19 (p=0.000). They agreed with the statement that vaccines are safe and do not cause serious side effects (p=0.007).
Breastfeeding women are 53 times more likely than non-breastfeeding women to vaccinate their children (OR = 53.302; p = 0.002), while they are 5 times more likely than non-breastfeeding women to want to vaccinate their children against COVID-19 (OR = 5.129; p = 0.004).
Surveyed women with children declared a lack of trust in government health information. Women who had one or two children were more likely to vaccinate them than those with more children (p=0.000). Participants with one child declared confidence in the safety and effectiveness of childhood vaccinations in preventing infectious diseases in contrast to women who have more children (p=0.000).
Women aged 30–35 believed that vaccinations were safe and effective in preventing infectious diseases in children as opposed to women aged 35–40. Younger women tended not to have an opinion (p=0.031). The distribution of responses was different in terms of willingness to vaccinate their children against COVID-19. Women in the 35–40 group were more likely to declare their willingness to vaccinate their children for this disease than younger women (p=0.018).
There is a significant correlation between the level of education and trust in healthcare and vaccination. Women with higher education declared confidence in health services in Poland (p=0.007); they vaccinate their children (p=0.005) and think that vaccinating children is safe and effective in preventing infectious diseases (p=0.055). Responses regarding the effectiveness of COVID-19 vaccination suggest that some of this group of respondents agreed with the statement, and some did not (p=0.001). Those with higher education were more afraid of the virus (p=0.041) and declared confidence in science as opposed to those with lower education (p=0.000). Moreover, their trust in science increased during the pandemic (p=0.035). Regarding vaccination against COVID-19, some women with higher education were willing to vaccinate themselves, and some were against vaccinating themselves against COVID-19, while in the group of women with secondary education, a large number of respondents did not have an opinion on this issue (p=0.001). Respondents with higher education declared the willingness to vaccinate their children against COVID-19 (p=0.002).
The correlations discussed along with the level of statistical significance are described Table 1
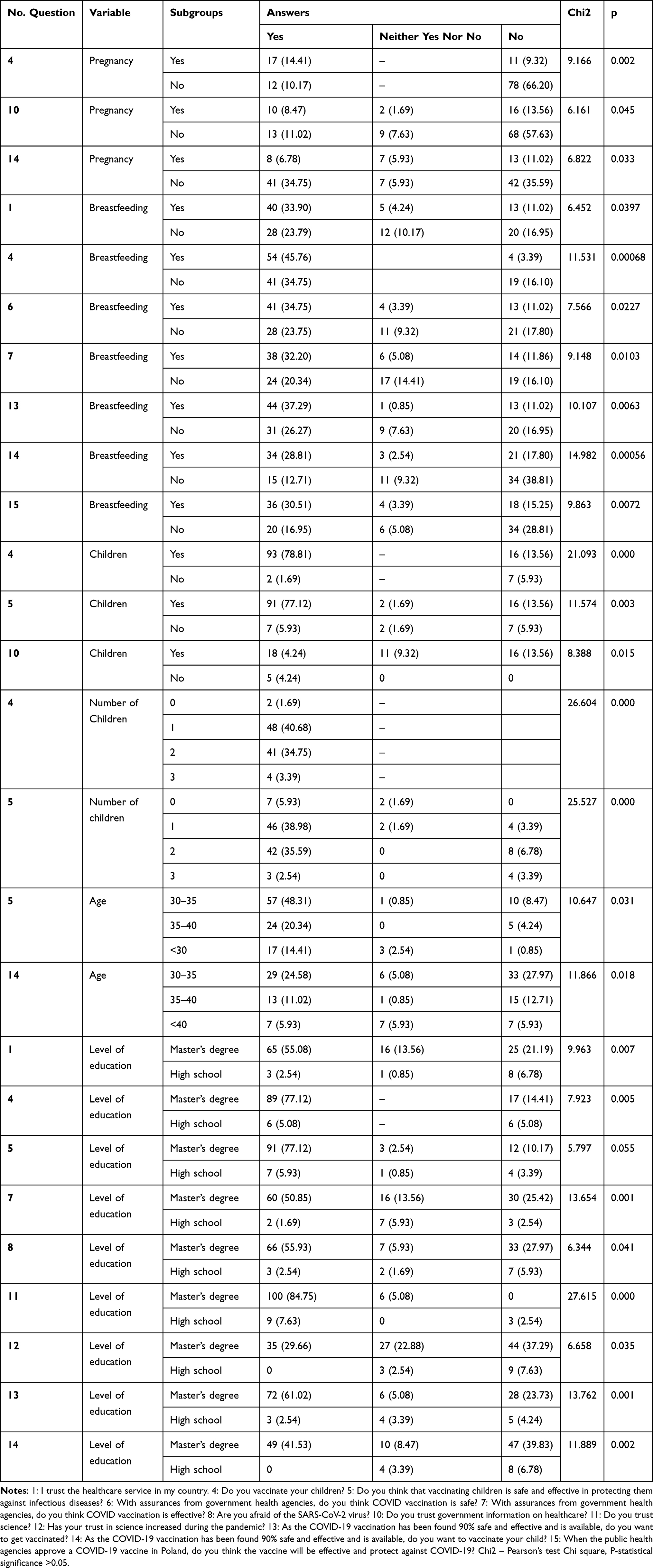 |
Table 1 Correlation Analysis Between Socio Demographic Data and Survey Questions |
In addition, all effects and correlations are presented graphically in PCA in Figure 1 Principal component analysis (PCA) evaluating corresponding variables.
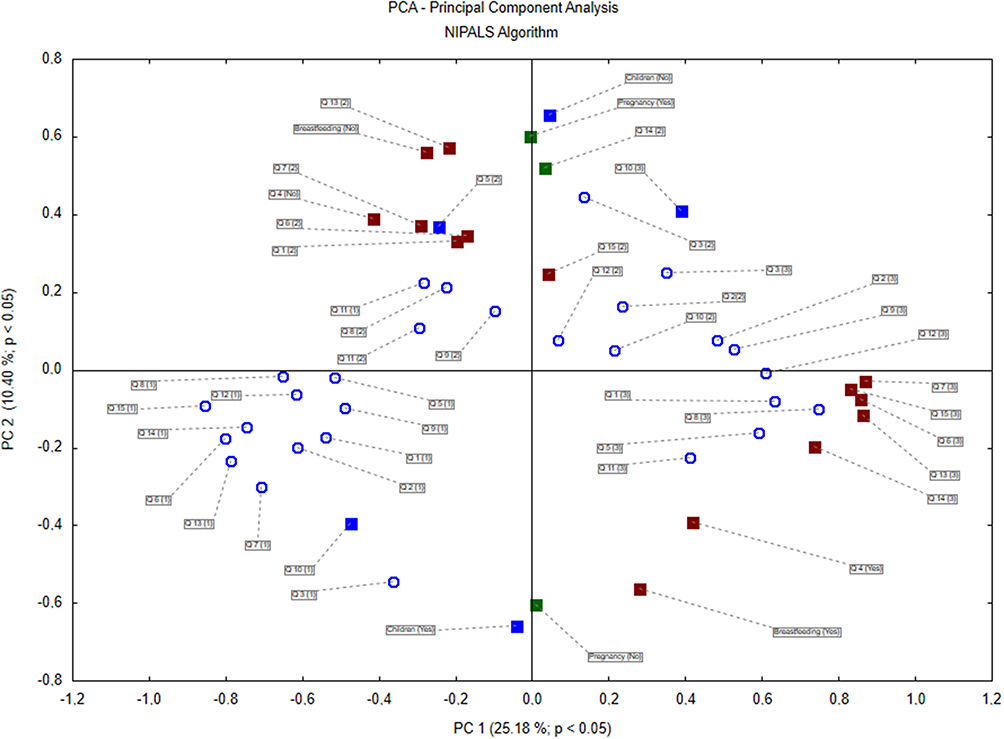 |
Figure 1 Principal component analysis (PCA) evaluating corresponding variables. Notes: Q1: I trust the healthcare service in my country. Q2: During the pandemic, my confidence in my country’s healthcare increased. Q3: I am satisfied with the performance of the government and professionals in my country in controlling the pandemic. Q4: Do you vaccinate your children? Q5: Do you think that vaccinating children is safe and effective in protecting them against infectious diseases? Q6: With assurances from government health agencies, do you think COVID vaccination is safe? Q7: With assurances from government health agencies, do you think COVID vaccination is effective? Q8: Are you afraid of the SARS-CoV-2 virus? Q9: Do you monitor pandemic information at least once a day? Q10: Do you trust government information on healthcare? Q11: Do you trust science? Q12: Has your trust in science increased during the pandemic? Q12: As the COVID-19 vaccination has been found 90% safe and effective and is available, do you want to get vaccinated? Q14: As the COVID-19 vaccination has been found 90% safe and effective and is available, do you want to vaccinate your child? Q15: When the public health agencies approve a COVID-19 vaccine in Poland, do you think the vaccine will be effective and protect against COVID-19? {1} – Disagree; {2} – Neither agree nor disagree; {3} – Agree. |
Correlation Analysis Between COVID-19 Vaccination Acceptance Questions and Other Survey Questions
Correlation analysis between selected questions of the questionnaire showed that women who want to vaccinate themselves and their children against COVID-19 and who believe that this vaccination does not have serious side effects (questions 13,14,15) also have confidence in health services (Q 1), their confidence increased during the pandemic (Q 2), they are satisfied with the actions of the government in controlling the pandemic (Q 3), and believe that vaccination against COVID-19 is safe (Q 6) and effective (Q 7).
The correlations are shown in Table 2
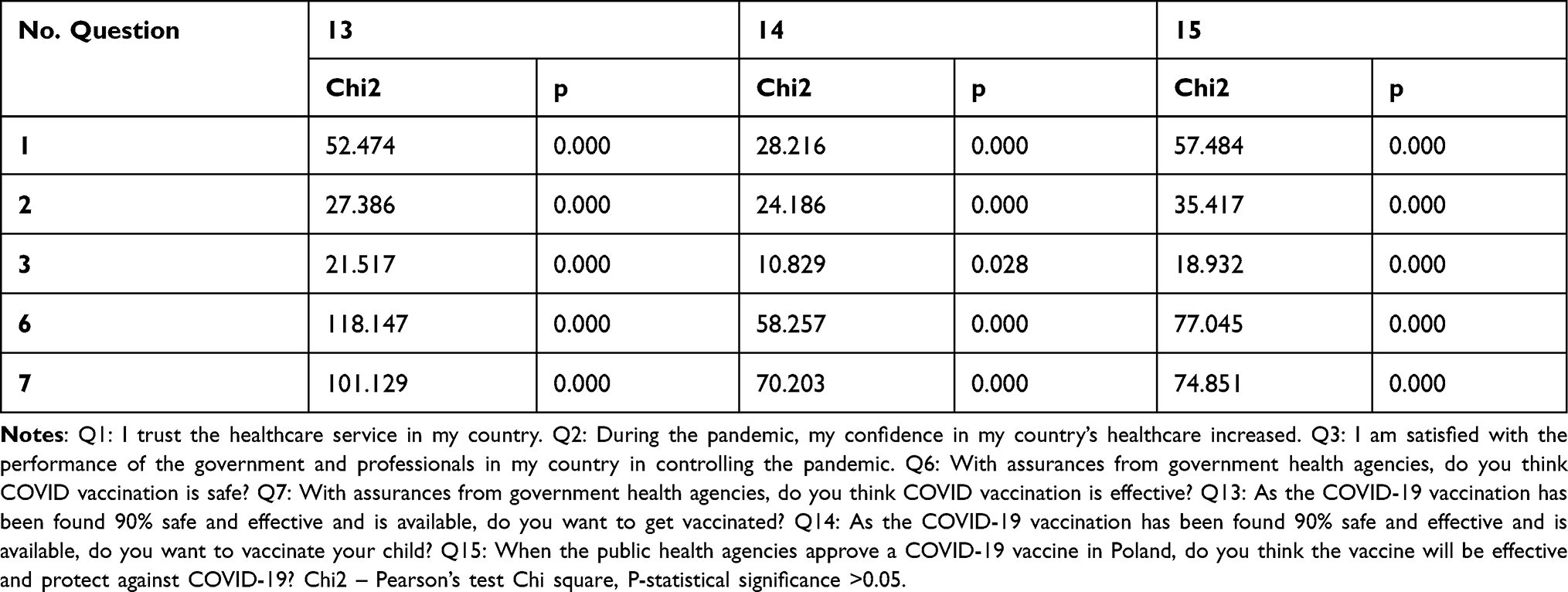 |
Table 2 Correlation Analysis Between COVID-19 Vaccination Acceptance Questions and Other Survey Questions |
Discussion
There is an ongoing concern in Polish society about the safety of receiving COVID-19 vaccinations. According to a report dated October 12, 2021, 46% of Poland’s population has been fully vaccinated.11 However, according to alarming data from the NHS (National Health Service) in the UK, nearly one-fifth of the most critically ill COVID-19 patients are unvaccinated pregnant women.20
The present study was designed to assess the attitudes of three categories of women: pregnant, breastfeeding, and having children toward receiving COVID-19 vaccination. According to our research, the profile of a woman who accepts COVID-19 vaccination is the one who is breastfeeding, has 1 or 2 children, with higher education, in age between 30 and 35 years old. Participants, who did not declare breastfeeding, have more than 2 children, and with a high school education, did not trust in COVID-19 vaccination and their vaccine acceptance level was lower. The analysis may prove helpful in further work on vaccine campaigns against the SARS-CoV-2 virus, as the success of a vaccine depends not only on its efficacy but also on its acceptance. Despite limited data on the effects of COVID-19 vaccination on pregnancy, there is no biological evidence to pose maternal and child safety risks associated with receiving COVID-19 vaccination.12,13 However, it has been documented abundantly that SARS-CoV-2 virus infection during pregnancy is associated with severe disease course and adverse obstetric outcomes.14–16
Overcoming public fears and relying on sound and factual knowledge can help women make informed decisions, achieve high vaccination rates, and stop the pandemic.
Our study showed high acceptance of the COVID-19 vaccine among pregnant and breastfeeding women. In addition, pregnant and breastfeeding women have been shown to have high trust in government health institutions as opposed to women who are not pregnant. The above results may be influenced by frequent contacts of pregnant and breastfeeding women with health care professionals (check-ups during pregnancy, patronage visits as part of the newborn’s primary healthcare). Involving health professionals in providing information focused on the safety of vaccine uptake and its effectiveness may be a useful way to counter women’s hesitancy to receive vaccinations.
During the pandemic, the expert panel of the Polish Society of Gynecologists and Obstetricians (PTGiP) agreed with the positions of the American College of Obstetricians and Gynecologists (ACOG), Royal College of Obstetricians and Gynaecologists (RCOG), Centers for Disease Control and Prevention (CDC), and the Society for Maternal-Fetal Medicine (SMFM), emphasizing that COVID-19 vaccination should be offered to pregnant and breastfeeding women.17 The ever-increasing body of scientific evidence related to the safety of vaccine uptake during pregnancy and lactation may influence wider acceptance of COVID-19 vaccination in this population.
Different results were found by Ayhan et al, who measured the acceptance of COVID-19 vaccination in a group of pregnant women in Turkey. The authors showed low acceptance of COVID-19 vaccination among pregnant women. Lack of confidence in vaccination was one of the most common reasons for vaccination refusal.9 On the other hand, in a study conducted in the Czech Republic, high level of education was found to be a significant predictor of Covid-19 vaccine uptake among pregnant and lactating women.20 The authors of the above study also emphasize the relationship between acceptance of COVID-19 vaccine and trimester of pregnancy. The study showed that women who were in the third trimester of pregnancy declared the highest level of acceptance of the vaccine.20 This observation may be related to the fact that a number of vaccinations, including influenza (H1N1) vaccines, are recommended and widely accepted in the third trimester of pregnancy. The first and second trimester of pregnancy is presented as a critical period for organogenesis. During this period, women avoid taking medications during pregnancy.20 In observation reported by Sutton et al18 where attitudes and beliefs regarding the acceptance of COVID-19 vaccination were examined in pregnant, lactating, and non-pregnant women. Pregnant as well as breastfeeding women were less likely to receive the vaccination compared to non-pregnant women. They argued their stance on the lack of sufficient research on vaccination.18
Very often, mothers are the key decision-makers in matters concerning their children. In our study, we set out to measure the level of acceptance and attitudes toward COVID-19 vaccination among mothers of children under 18. Surveyed women with children declared a lack of trust in government health information. Mothers with one or two children and breastfeeding women accept COVID-19 vaccination, want to be vaccinated, and want to vaccinate their children as opposed to non-breastfeeding women and women with more than two offspring. COVID-19 vaccine acceptance and prognostic factors among women vary worldwide. The meta-analysis by Skjefte et al6 presented results from 16 countries where COVID-19 vaccination acceptance rates were measured among pregnant women and mothers of children under 18. Significant geographical variation in the acceptance of vaccination among pregnant women and young mothers has been demonstrated. Vaccine acceptance was generally highest in India, the Philippines, and all sampled countries in Latin America; it was lowest in Russia, the United States, and Australia.6 Women in Russia and the US consistently expressed lower acceptance and confidence in the safety/efficacy of the COVID-19 vaccine and reported lower confidence in public health agencies.6 The decision to vaccinate against COVID-19 is a multi-faceted event. SARS-CoV-2 virus disease perceptions and public trust play a key role in shaping vaccine acceptance. COVID-19 vaccination campaigns for women, lactating women, and mothers should be unique to each country in order to achieve the highest possible level of acceptance and trust of a given population in vaccination.
We investigated women’s level of education and determined its effect on confidence and acceptance of COVID-19 vaccination. Women with higher education declared confidence in science and the healthcare system in Poland. They expressed willingness to get vaccinated themselves and have their children vaccinated against COVID-19 as opposed to those with lower education. In Poland, the predominant group of unvaccinated persons includes those with primary education.11 Doubt about SARS-CoV-2 virus disease, skepticism about the vaccine, distrust of the health care system, and pre-formed beliefs about vaccination may contribute to the reluctance we observed among the women interviewed. Differences in education were also significant in other countries. For example, the study by Lazarus et al19 proved that people with high education in Ecuador, France, Germany, India, and the United States reported vaccine acceptance; however, individuals with higher levels of education in Canada, Spain, and the United Kingdom demonstrated lower vaccine acceptance.19 Thus, there is considerable heterogeneity in terms of demographic factors in respondents’ propensity to receive the vaccine recommended by the World Health Organization. Clear and consistent communication from government officials is critical to building public confidence in immunization programs.
A limitation of this study was that respondents’ reported intentions to vaccinate against COVID-19 may not always translate into vaccine uptake, as vaccination decisions are multifactorial and may change over time.
Conclusion
In conclusion, acceptance and confidence in receiving the COVID-19 vaccine is an integral and modifiable part of the efficacy against the SARS-CoV-2 virus. Our results indicate that the trust of pregnant and breastfeeding women and women who have offspring in government, in healthcare professionals, in scientific authorities, and sound scientific data is strongly associated with vaccine acceptance and may influence an individual’s decision to perceive recommended actions as beneficial to the society as a whole. Therefore, it is critical to expand scientific evidence regarding the safety and efficacy of COVID-19 vaccines in pregnancy and during breastfeeding.
Building trust and public awareness is a multifactorial aspect that must start at the global, national, and sub-national levels. Vaccination campaigns for pregnant and lactating women and mothers should be specific to each country to achieve the greatest impact on still undecided women.
Abbreviations
NHS, National Health Service; PTGiP, Polish Society of Gynecologists and Obstetricians; ACOG, American College of Obstetricians and Gynecologists; RCOG, Royal College of Obstetricians and Gynaecologists; CDC, Centers for Disease Control and Prevention; SMFM, Society for Maternal-Fetal Medicine (SMFM); Q, question.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Bioethics Committee of the Medical University in Wroclaw, No. KB-761/2021.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. World Health Organization. COVID-19 weekly epidemiological update edition60. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19—5-october-2021.
2. Martinez-Portilla RJ, Sotiriadis A, Chatzakis C, et al. Pregnant women with SARS-CoV-2 infection are at higher risk of death and pneumonia: propensity score matched analysis of a nationwide prospective cohort (COV19Mx). Ultrasound Obstet Gynecol. 2021;57(2):224–231. doi:10.1002/uog.23575
3. Li X, Xu W, Dozier M, et al. The role of children in transmission of SARS-CoV-2: a rapid review. J Glob Health. 2020;10(1):011101. doi:10.7189/jogh.10.011101
4. Garg I, Shekhar R, Sheikh AB, et al. COVID-19 vaccine in pregnant and lactating women: a review of existing evidence and practice guidelines. Infect Dis Rep. 2021;13(3):685–699. doi:10.3390/idr13030064
5. Press release. JCVI issues new advice on COVID-19 vaccination for pregnant women. Available from: https://www.gov.uk/government/news/jcvi-issues-new-advice-on-covid-19-vaccination-for-pregnant-women.
6. Skjefte M, Ngirbabul M, Akeju O, et al. COVID-19 vaccine acceptance among pregnant women and mothers of young children: results of a survey in 16 countries. Eur J Epidemiol. 2021;36(2):197–211. doi:10.1007/s10654-021-00728-6
7. Razzaghi H, Meghani M, Pingali C, et al. COVID-19 vaccination coverage among pregnant women during pregnancy - Eight Integrated Health Care Organizations, United States, December 14, 2020–May 8, 2021. MMWR Morb Mortal Wkly Rep. 2021;70(24):895–899. PMID: 34138834; PMCID: PMC8220952. doi:10.15585/mmwr.mm7024e2
8. Jaffe E, Goldfarb IT, Lyerly AD. The costs of contradictory messages about live vaccines in pregnancy. Am J Public Health. 2021;111(3):498–503. doi:10.2105/AJPH.2020.306045
9. Ayhan GS, Oluklu D, Atalay A, et al. COVID-19 vaccine acceptance in pregnant women. Int J Gynaecol Obstet. 2021;154(2):291–296. doi:10.1002/ijgo.13713
10. Report of the Sage Working Group on Vaccine Hesitancy. Available from: https://www.thecompassforsbc.org/sbcc-tools/report-sage-working-group-vaccine-hesitancy.
11. Kto i dlaczego nie chce się szczepić́ na COVID-19? Available from: https://bp.wum.edu.pl/sites/bp.wum.edu.pl/files/2021_09_01_wum_arc_rynek_opinia.pdf.
12. Zauche L, Wallace B, Smoots AN, et al. Receipt of mRNA COVID-19 vaccines preconception and during pregnancy and risk of self-reported spontaneous abortions, CDC v-safe COVID-19 Vaccine Pregnancy Registry. Res Sq. 2021:
13. Shimabukuro TT, Kim SY, Myers TR, et al. Preliminary findings of mRNA Covid-19 vaccine safety in pregnant persons. N Engl J Med. 2021;384:2273–2282. doi:10.1056/NEJMoa2104983
14. Zambrano LD, Ellington S, Strid P, et al. Update: characteristics of symptomatic women of reproductive age with laboratory-con rmed SARS-CoV-2 Infection by pregnancy status — United States, January 22–October 3, 2020. MMWR. 2020;69:1641–1647. doi:10.15585/mmwr.mm6944e3
15. Wei SQ, Bilodeau-Bertrand M, Liu S, et al. The impact of COVID-19 on pregnancy outcomes: a systematic review and meta-analysis. CMAJ. 2021;193(16):E540–E548. doi:10.1503/cmaj.202604
16. John Allotey J, Stallings E, Bonet M, et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. BMJ. 2020;370:m3320. doi:10.1136/bmj.m3320
17. Stanowisko PTGiP dotyczące szczepień kobiet ciężarnych przeciwko COVID19. Available from: http://www.ptgin.pl/stanowisko-ptgip-dotyczace-szczepien-kobiet-ciezarnych-przeciwko-covid19.
18. Sutton D, D’Alton M, Zhang Y, et al. COVID-19 vaccine acceptance among pregnant, breast- feeding, and nonpregnant reproductive-aged women. Am J Obstet Gynecol. 2021;3:100403. doi:10.1016/j.ajogmf.2021.100403
19. Lazarus VJ, Wyka K, Rauh L, et al. Hesitant or not? The association of age, gender, and education with potential acceptance of a COVID-19 vaccine: a country-level analysis. J Health Commun. 2020;25(10):799–807. doi:10.1080/10810730.2020.1868630
20. Riad A, Jouzova A, Ustun B, et al. COVID-19 vaccine acceptance of pregnant and lactating women (PLW) in Czechia: an analytical cross-sectional study. Int J Environ Res Public Health. 2021;18:13373. doi:10.3390/ijerph182413373
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.