")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
COVID-19 Prevention Practices and Associated Factors Among Farmers in Peri-Urban Areas of Northeastern Ethiopia
Authors Berhanu L , Berihun G , Walle Z , Teshome D , Gizeyatu A, Abebe M, Hassen S , Ademas A , Wagaye B , Adane M
Received 25 May 2021
Accepted for publication 11 June 2021
Published 12 July 2021 Volume 2021:14 Pages 1843—1852
DOI https://doi.org/10.2147/JMDH.S321456
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Leykun Berhanu,1 Gete Berihun,1 Zebader Walle,2 Daniel Teshome,3 Adinew Gizeyatu,1 Masresha Abebe,1 Seada Hassen,1 Ayechew Ademas,1 Birhanu Wagaye,4 Metadel Adane1
1Department of Environmental Health Science, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 2Department of Social and Public Health, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 3Department of Anatomy, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 4Department of Public Health Nutrition, School of Public Health, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
Correspondence: Leykun Berhanu Email [email protected]
Background: COVID-19 is a global health threat due to its rapid spread and ability to kill millions of people. The majority of pandemic-fighting approaches rely on prevention activities, which can be influenced by a variety of factors. Farmers are more vulnerable to COVID-19, so evaluating existing prevention practices and associated factors is critical to prevent the COVID-19 pandemic.
Objective: To assess COVID-19 prevention practices and associated factors among farmers in peri-urban areas of Northeastern Ethiopia.
Methods: A community-based cross-sectional study design was conducted among 409 selected farmers. Data were collected using face-to-face interviews and on-the-spot-observational checklist. Data were analyzed using bivariable logistic regression model at 95% CI (confidence interval). During the bivariable analysis (crude odds ratio [COR]), varibales having a p-value of less than 0.250 were included into the multivariable analysis (adjsuted odds ratio [AOR]). Factors associated with COVID-19 preventive practices were determined using a multivariable analysis at a p-value of 0.050.
Results: Of 409 participants, 206 (63.6%), 157 (38.4%), and 117 (28.6%) of them had satisfactory knowledge, positive attitude, and good prevention practices about COVID-19, respectively. Age of the farmers with greater than or equal to 45 years (AOR: 3.2; 95% CI: 1.7– 6.1), educational status of secondary school and above (AOR: 3.1; 95% CI: 1.4– 6.6), and income level of having greater than or equal to 2,001.00 Ethiopian birr (ETB) (AOR: 1.9; 95% CI: 1.1– 3.4) were all found to be significantly associated with the COVID-19 prevention practices.
Conclusion: Even though the majority of farmers had satisfactory knowledge, a considerable proportion of them had a negative attitude and poor COVID-19 prevention practices. Age, educational status, and income level are factors associated with COVID-19 prevention practices. Hence, health education should be given to improve the farmers’ knowledge, attitudes and prevention practices to minimize the risk of COVID-19 among farmers in semi-urban areas of northestern Ethiopia.
Keywords: COVID-19, Dawa Chefa District, Peri-urban Areas, Farmers, Northeast Ethiopia
Introduction
COVID-19 is a virus that originated in Wuhan, China, and is more infectious than the Coronavirus that causes Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS).1 Evidence indicate that the virus is carried by birds and mammals, with humans being particularly vulnerable to infection and transmission.2,3 COVID-19 is transferred largely by droplets from infected people coughing, sneezing, or speaking, as well as by touching a contaminated surface and then contacting the eyes, nose, or mouth without washing hands.4,5
COVID-19 manifests itself as cough, fever, malaise, weakness, and shortness of breath. The new virus has sparked widespread alarm around the world because of its great potential for quick spread and the fact that it can be deadly.6,7 COVID-19 in its later stage resulted in respiratory distress syndrome, septic shock, hemorrhage, and coagulation malfunction.8
Hand washing, wearing a face mask, maintaining a safe physical distance, keeping the space ventilated, avoiding crowded areas, covering the nose and mouth while coughing or sneezing, avoiding direct contact with animals and suspected areas of coronavirus infections, and avoiding the intake and handling of raw meat to prevent cross-contamination are among the COVID-19 prevention practices suggested by the World Health Organization (WHO).9
COVID-19 prevention efforts are said to be influenced by group awareness and mindset, according to researchers.10,11 For example, the SARS outbreak in China demonstrated how a lack of information and mindset can make disease prevention more difficult.12 People’s desire to support government attempts to combat the pandemic is also substantially influenced by their level of awareness, and having more knowledge is highly associated to a good attitude regarding COVID-19 prevention methods.13
Despite taking a number of prevention measures, numerous countries, including Ethiopia, are still unable to contain the pandemic. Many African continents, including Ethiopia, are seeing an increase in infection rates. As of March 23, 2021, the WHO reported that more than 120 million individuals had been infected and more than 2.7 million had perished. In Africa, more than 3 million people have been affected. Since March 23, 2021, when the first incidence of COVID-19 was discovered in Ethiopia on March 13, 2020, more than 190,000 people have been infected and over 2500 people have died.14
Effective infection prevention and control practices must be implemented at the global, national, and individual levels to combat the COVID-19 pandemic, which necessitates sufficient knowledge of the etiology, transmission, and various community responses to the pandemic, as well as a positive mindset, to correctly implement the prevention practices.13,15,16 The best example was during the Ebola pandemic, when research on awareness, attitude, and practice (KAP) helped to establish preventive techniques. The data support the theory that a lack of understanding about the diseases contributes to an increase in the number of cases. This means that community awareness, thinking, and prevention activities helps in containing the outbreak and minimizing its impact on public health, social, economic, and political issues.17
Several studies have focused on COVID-19 prevention practices in the general population, healthcare workers, and those with chronic illnesses. However, as per our knowledge, so far no research has been done to determine the prevention practices and related factors among vulnerable populations in peri-urban areas such as farmers, who are the backbone of society in low- and middle-income countries, including Ethiopia. Agriculture provides food through harvesting crops including wheat, sugar cane, rice, and a variety of other crops. Farmers are important for the establishment of a good crop with a fair yield, which they can only supply, thus none of this would be possible without them. The COVID-19 pandemic has had a profound impact on humanity’s lifestyle and activities, including agriculture. Food demand and hence food security are significantly impacted as a result of mobility restrictions, reduced purchasing power, and a disproportionate impact on the most vulnerable population groups. According to the Food and Agriculture Organization, COVID-19 has a substantial impact on agriculture in two areas: food supply and demand. These two factors are inextricably linked to food security.18
As a result, protecting farmer’s health from the COVID-19 pandemic entails enhancing the public’s health. Therefore, this study aimed to assess COVID-19 prevention practices and associated factors among farmers in peri-urban areas of Dawa Chefa District, Northeastern Ethiopia.
Methods
Study Area Description
The study was conducted in the peri-urban areas of Dawa Chefa District, which consists of four Kebeles (the smallest administrative unit in Ethiopia) of Oromia Special Zone in Amhara region, Northeastern Ethiopia. The district is 326 km far from Addis Ababa, the capital city of Ethiopia, to Northern Ethiopia. According to the Central Statistical Agency (CSA), the population projection of Dawa Chefa district was 150,165 populations composed of 74,687 (49.7%) male and the remaining 75,478 (50.3%) female.19 Dawa Chefa District is located at a latitude and longitude of 10°43′N and 39°52′E, respectively. The altitude of the area ranges from 1500 to 2300 meters above sea level. Based on the climatic classification, the area is classified under semiarid climatic conditions. The rainfall distribution of the study area has highly seasonal and temporal variations. The predominant production system in this area is mixed crop-livestock farming in which cattle are the most important livestock species.20
Study Design and Populations
A community-based cross-sectional study design was conducted from January 1 to February 15, 2021. The source populations were all farmers in the peri-urban areas of Dawa Chefa District whose age 18 years and above, whereas the study population was all farmers living in the selected peri-urban Kebeles of Dawa Chefa District.
Sample Size Determination and Sampling Procedure
The sample size was determined using a single population proportion formula.21
Using the assumptions of:
Zα/2 is the standard normal variable value at (1–α) % confidence level (α is 0.05 with 95% CI [confidence interval], Zα/2 = 1.96), p is an estimate of the expected prevention practices for COVID-19 in Dawa Chefa District taken as a good prevention practice of 50.0%. A proportion of 50.0% was considered since there had been no previous study conducted in the study area or other similar setting, and d margin of error (5.0%). Adjusting for a 10% non-response rate, the final sample size was determined to be 422. Of the total four peri-urban Kebeles, two Kebeles were selected randomly. Households with residents aged 18 years and above were selected from each Kebele and study participants were allocated proportionally. A sampling frame was made within households that had at least one resident aged 18 years and above. Households with study participants aged 18 years or above were selected using a systematic sampling technique. When there is more than one eligible participant with the selected household, a simple random sampling technique was used. From the selected household, if there was no eligible study participant during the first visit, another visit was done on the same day or the next day.
Dependent and Independent Variable Measurement
The dependent variable of this study was the prevention practices of COVID-19, measured as good or poor and the independent variables were socio-demographic characteristics, presence of training about COVID-19, source of information about COVID-19, knowledge about COVID-19 (satisfactory or unsatisfactory), and attitude towards COVID-19 (positive or negative). The outcome variable of good or poor prevention practices was measured using 11 close-ended questions having aresponse of “often, sometimes, and never” with ascore of 2, 1, and 0 points, respectively. The total score ranged from 0 to 22. Then, the respondents were classified as having good COVID-19 prevention practices if they had amean score of 80% and above, whereas poor preventive practice for amean score of below 80%.10,22 The independent variables of socio-demographic factors of the study participants and source of information, knowledge, and attitude about COVID-19 were measured by self-reporting of the study participants.
Knowledge about COVID-19
To examine knowledge about COVID-19: 18 close-ended questions were used which had a “Yes, No, and do not know” response. A score of “1” mark was assigned for a correct response and a value of “0” to an incorrect and do not know the response. The total score ranged from 0 to 18. If the respondents correctly answered 80% and above, they classified as having satisfactory knowledge otherwise they classified as having unsatisfactory knowledge.10,16
Attitude towards COVID-19
The attitude of the respondents was assessed using 17 close-ended questions, which had a response of “agree, undecided, and disagree” with a score of 2, 1, and 0, respectively. The total score ranged from 0 to 34. Then, participants were classified as having a positive attitude if they score 80% and above otherwise classified as having a negative attitude towards COVID-19.10,16,22
Data Collection and Data Quality Assurance
A structured close-ended questionnaire was prepared in English language, translated to the local language Amharic, and re-translated back to English. The questionnaire had four parts. Part I contains socio-demographic information of the respondents; Part II contains questions prepared to assess the knowledge about COVID-19. Part III comprises questions designed to assess the attitude towards COVID-19 and Part IV includes questions prepared to assess the prevention practices applied by households. Before the beginning of the actual data collection, the questionnaire was pre-tested on 5% of the sample size. Based on the finding obtained, the necessary correction such as the ordering of the questions, addition of the missed question, removing less important questions, and language editions were done accordingly. The primary investigator gave one-day training for both data collectors and supervisors about the objective of the study, data collection tool, ethical issues and other consideration that has to be clear before the beginning of the actual data collection. The data were collected by five environmental health professionals using face-to-face interviews and observational checklist. During data collection, three master holder public health professionals carried out daily supervision.
Data Processing and Analysis
The data were entered into EpiData version 4.6 and exported to SPSS version 25.0 software for data cleaning and analysis. Descriptive statistics such as frequency and percentage were calculated to examine the overall distribution of the variables. A binary logistic regression model was used to determine the association between the dependent and the independent variables. All the independent variables, which had a p-value of less than 0.250 from the bi-variable analysis, were entered for multivariable analysis. In the multivariable analysis, a p-value of < 0.05 and AOR (adjusted odds ratio) with 95% CI was used to measure associations, and variables with p-value < 0.05 were assumed statistically significant and associated factors of prevention practices against COVID-19 pandemic. The presence of multicollinearity among independent variables was checked using standard error at the cutoff value of 2 and we found that a maximum standard error of 0.380, which indicate no multicollinearity. Model fitness was checked using the Hosmer and Lemeshow test and we found a p-value of 0.485.
Results
Socio-Demographic Characteristics of the Respondents
The survey was completed by 409 of the 422 respondents, for a response rate of 96.9%. Around half 215 (52.6%) of the respondents were female, and more than one-third 135 (33.0%) of them could not read or write. Less than one-third 108 (26.4%) of the respondents, had a monthly income of more than or equal to 2,000.00 ETB (Average exchange rate of United States Dollars (USD) to Ethiopia birr was 39.6237 during the study period), and nearly half 194 (47.4%) of them had a family size of more than five (Table 1).
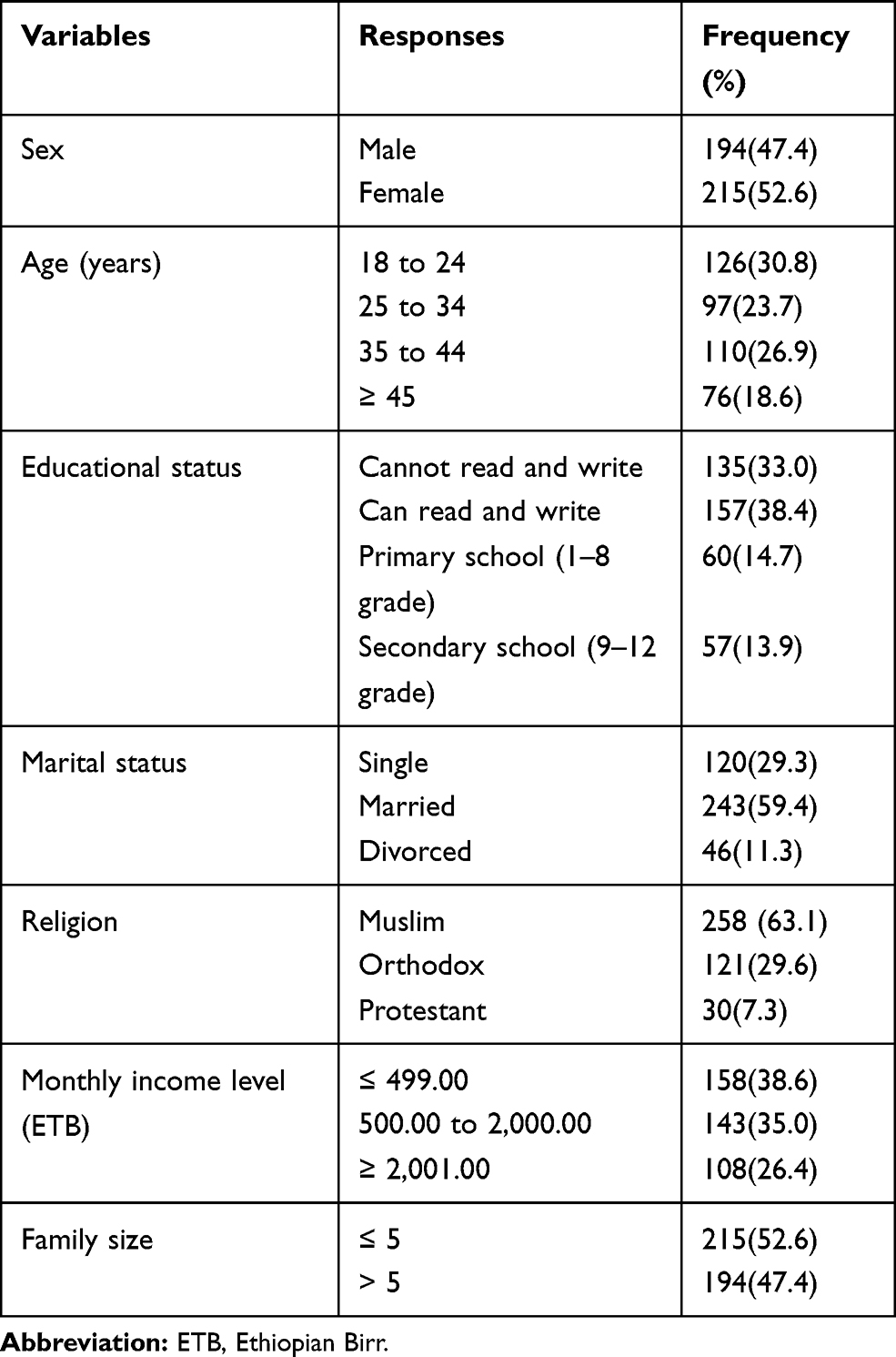 |
Table 1 Socio-Demographic Characteristics of Farmers in Peri-Urban Areas of Dawa Chefa District, Northeastern Ethiopia, January 1 to February 15, 2021 (N = 409) |
Presence of Training and Source of Information about COVID-19
Of 409 study participants, about half 228 (55.7%) of them received training about COVID-19. About half 199 (48.7%), 108 (26.4%), and 198 (48.4%) of the respondents received information about COVID-19 from their family or friends, social media, and radio or television outlets, respectively (Table 2).
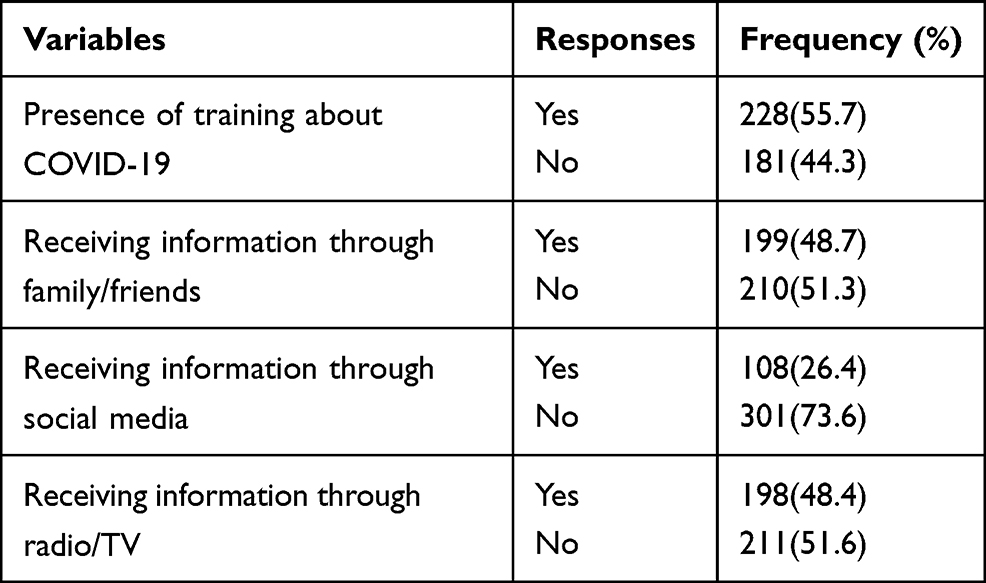 |
Table 2 Presence of Training and Source of Information About COVID-19 Among Farmers in Peri-Urban Areas of Dawa Chefa District, Northeastern Ethiopia, January 1 to February 15, 2021 (N = 409) |
Knowledge of the Respondents about COVID-19
The majority 338 (82.6) of respondents were aware of the cause of the COVID-19 pandemic. The majority 354 (86.6%) of respondents said there is no cure for COVID-19, but that supportive care might help them recover, and most 359 (87.8%) of them were aware of the presence of an effective vaccine. The respondents’ average knowledge score was 82.3±9.6%. According to the mean score value, 63.6% of the respondents had satisfactory knowledge about COVID-19 (Table 3).
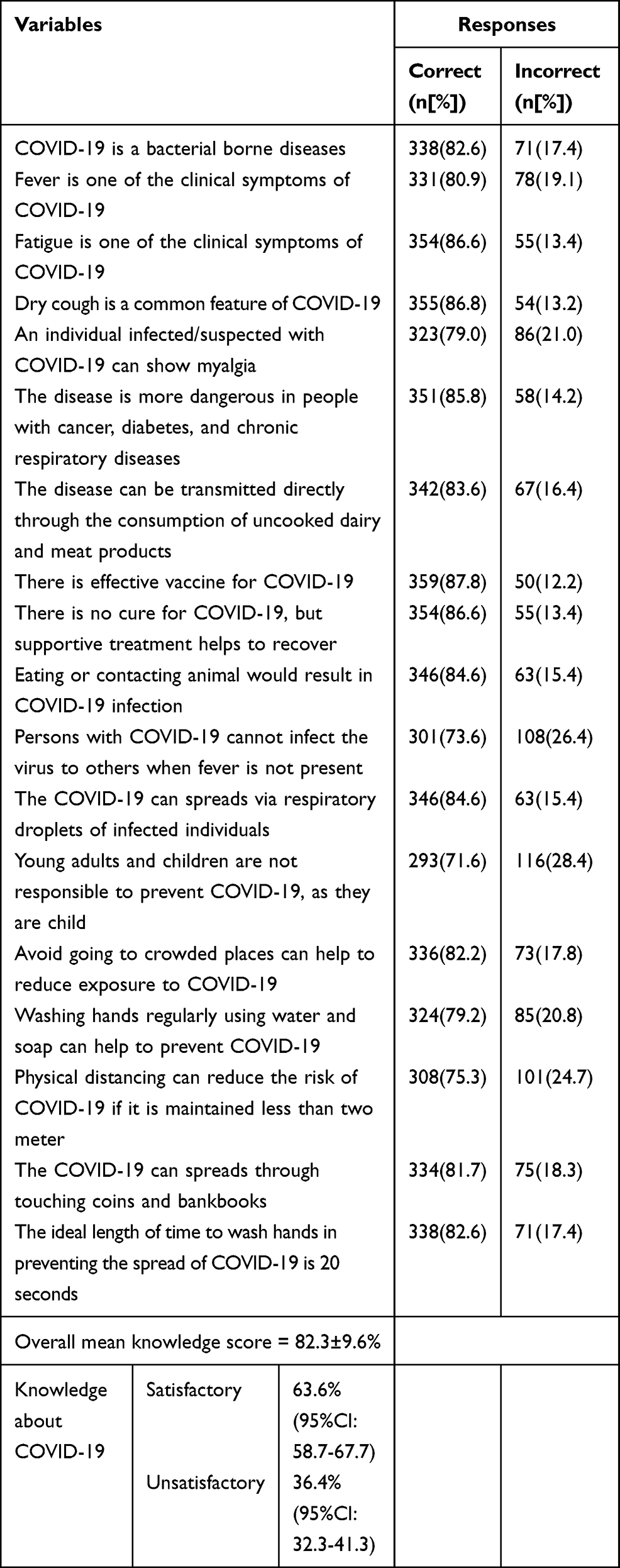 |
Table 3 Knowledge of farmers about COVID-19 in Peri-Urban Areas of Dawa Chefa District, Northeastern Ethiopia, January 1 to February 15, 2021 (N = 409) |
The Attitude of the Respondents towards COVID-19
About two-thirds 255 (62.3%) of the respondents agreed that avoiding touching the eyes, nose, and mouth would reduce the risk of exposure to COVID-19. Almost similar percentage 253 (61.9%) of them agreed that coughing and sneezing into the elbow or within the cloth is a good practice to prevent the spread of COVID-19. About three fourth 294 (71.9%) of them agreed that proper mask usage should include covering nose, mouth, and chin and almost similar proportion 291 (71.4%) of them agreed that staying at home play a significant role in preventing the spread of the pandemic. The overall mean attitude score of the respondents was 77.3±9.3%. Nearly two-fifth 38.4% of the respondents had a positive attitude towards COVID-19 (Table 4).
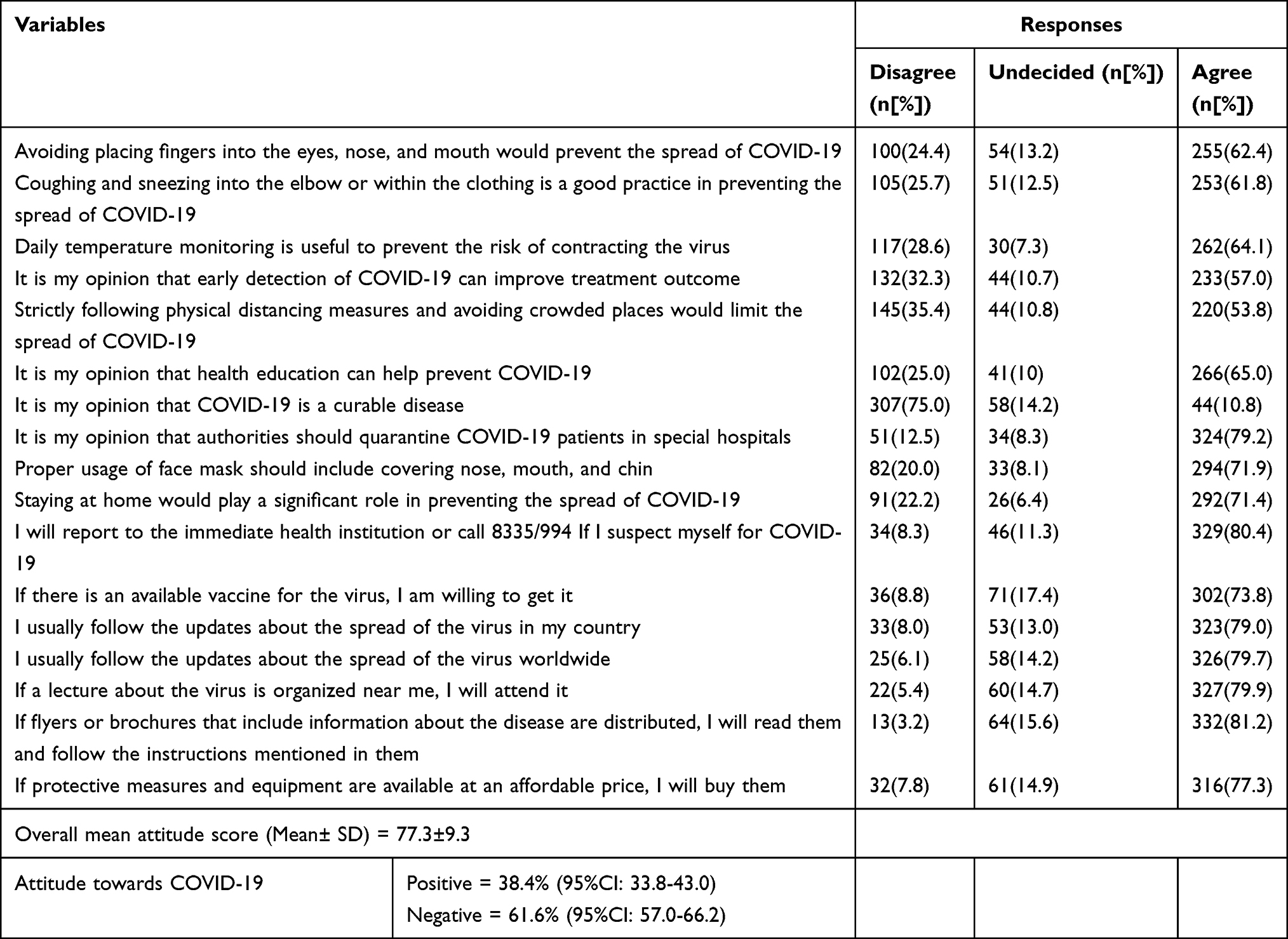 |
Table 4 Attitude of Farmers towards COVID-19 in Peri-Urban Areas of Dawa Chefa District Northeastern Ethiopia, January 1 to February 15, 2021 (N = 409) |
COVID-19 Prevention Practices of the Respondents
Nearly half 188 (46.0%) of the respondents often went to a crowded place. About two-thirds 253 (61.9%) of the respondents often wash their hands with soap for at least 20 seconds. Almost similar percentages of the respondents use a face mask and avoid kissing and contacting others. About half of them often go to the health institution if they get a fever, headache, and breathing problems. The overall mean practice score of the respondents was 70.6±13.2%. Less than one-third 117 (28.6%) of the respondents had good COVID-19 prevention practices (Table 5).
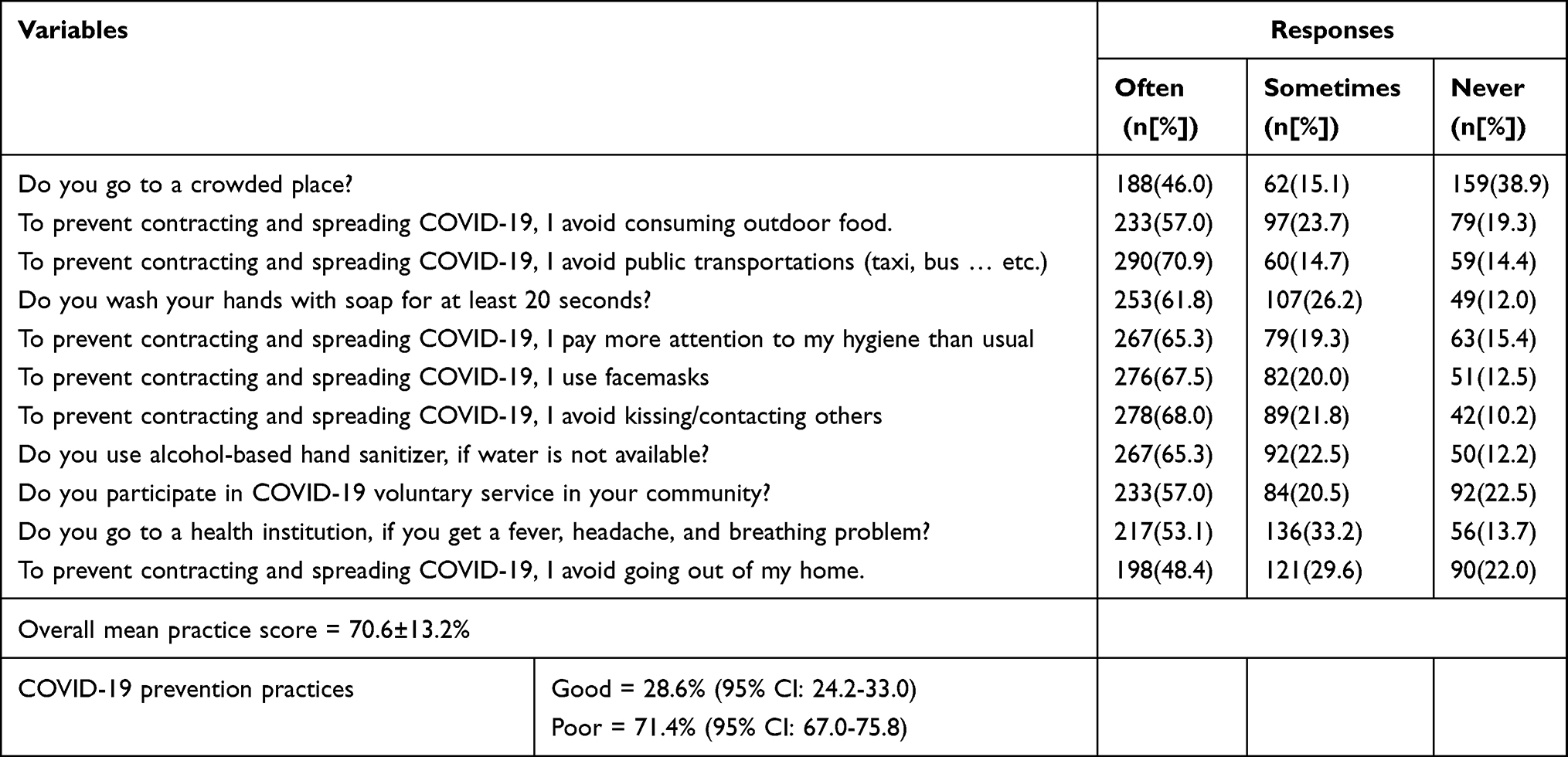 |
Table 5 COVID-19 Prevention Practices Among Farmers in Peri-Urban Areas of Dawa Chefa District Northeastern Ethiopia, January 1 to February 15, 2021 (N = 409) |
Factors Affecting COVID-19 Prevention Practices
From the bi-variable analysis, we found that age, educational status, income level, family size, receiving COVID-19 information from family or friends, receiving COVID-19 information from TV or radio, and receiving COVID-19 information from social media were the candidate variables for the multivariable logistic regression analysis. Multivariable logistic regression analysis revealed that respondents’ age, educational level, and monthly income were all significantly associated (p<0.05) with COVID-19 prevention practices. The analysis indicated that respondents aged greater than or equal to 45 years old were 3.2 times more likely to apply good COVID-19 prevention practices compared to those whose ages ranged from 18 to 24 years. Those who completed secondary school were 3.1 times more likely to have good COVID-19 prevention practices than those who cannot read and write. Respondents who had a monthly income greater than or equal to 2,001.00 ETB were 1.9 times more likely to apply better COVID-19 prevention practices than those who had less than or equal to 499.00 ETB (Table 6).
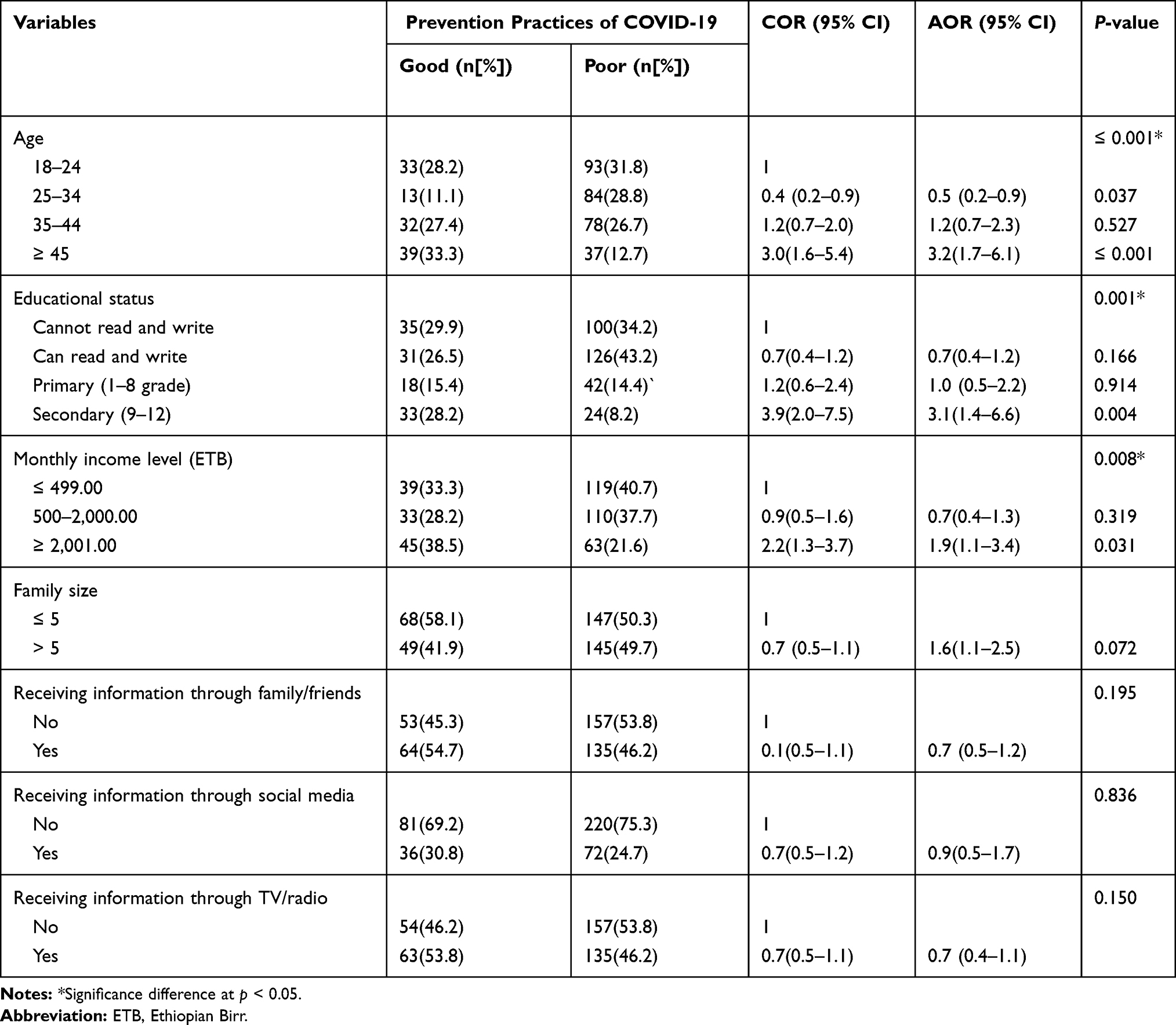 |
Table 6 Factors Affecting COVID-19 Prevention Practices Among Farmers in Peri-Urban Areas of Dawa Chefa District, Northeastern, Ethiopia, January 1 to February 15, 2021 (N = 409) |
Discussion
Despite repeated attempts to prevent and control COVID-19, the problem persists, harming the lives and economic progress of millions of people across worldwide, including Ethiopia. Lack of studies to identify the status of COVID-19 prevention practices and assoicated factors in peri-urban areas in northeastern Ethiopia hinders the efforts of the prevention programs towards COVID-19.3
Having sufficient knowledge of COVID-19 is beneficial in gaining a clear understanding of the disease burden, which allows a person to take appropriate prevention practices.22 The current study found that 63.6% (95% CI; 58.7–67.7) of the respondents had satisfactory knowledge, which is almost similar to a study conducted in Africa, which found that 61.6% of the study participants had a satisfactory knowledge.14 The majority of those who took part in this study were aware of the main COVID-19 transmission routes as well as the fact that there is no effective COVID-19 cure. The current figure, however, is lower than that of an Indian survey, which indicated that around 70% of respondents possessed satisfactory knowledge.23 This can be credited to India’s health ministry’s concerted attempts to inform the people about the pandemic’s scope and severity, as well as its transmission, prevention, and control techniques. In addition, the average mean knowledge score of the respondents was 82.3%, which is consistent with a survey conducted in Saudi Arabia,24, and Vietnam,3 where the mean knowledge score of the respondents was found to be 81.6% and 81.7%, respectively. Measures such as mass education and providing training programs for those who are in need should be taken to improve the level of knowledge among respondents. However, the higher result was reported in Pakistan and India where the mean knowledge score of the respondents was 90% and 88.9%, respectively.6,8 A slightly lower results was reported in China in which the overall mean knowledge score of the respondents was 80%.25
People’s attitude affect their decision to do or not do something, and having a positive attitude means that they are eager, capable, and committed to taking various prevention steps to avoid contracting COVID-19 infection. According to the findings, 38.4% (95% CI: 33.8–43.0) of the respondents had a positive attitude towards COVID-19, which was almost a half lower than the study done in Pakistan where 80–90% of the respondents had a positive attitude towards COVID-198 and consistent with the study done in China.11 In addition, the respondents’ overall mean attitude score was 77.3%, which is consistent with the study conducted in India,6 where the mean attitude score of the respondents was 73.3%. The higher result was reported in China25 and Saudi Arabia,24 where the mean attitude score of the respondents is reported to be 85.4% and 94.1% respectively. Without a positive mindset, learning about the transmission and mitigation methods is useless for any interventions aimed at reducing the pandemic’s health and economic effects. As a result, a strategy should be devised to shift the respondent’s thinking and prepare them to correctly implement the numerous prevention measures in order to protect themselves and their families from the risk of COVID-19 exposure.
Due to a shortage of effective treatment procedures and an enough budget to deliver vaccines for all people, especially in poor countries like Ethiopia; more effort is needed to focus on the holistic preventive strategy. In this survey, less than a third, 28.6% (95% CI: 24.2–33.0) of the respondents had a good COVID-19 prevention practice. This figure was lower than the study conducted in Pakistan, where nearly all participants perform the basic prevention practices.8 In Jordan, 87.5% of respondents had good COVID-19 prevention practices, which included hand washing with soap or alcohol, wearing personal protective equipment, and wearing a mask.1
Lower COVID-19 prevention practices found in this study may be attributed to a lack of sufficient public education, community carelessness in implementing various prevention practices, a negative attitude toward the pandemic, and most importantly, the absence of clear legal issues that suggest what to do and what not to do in terms of pandemic control. Furthermore, the respondents’ overall mean practice score was 70.6%, which is lower than a study done in Saudi Arabia, where the respondents’ mean practice score was 86.8%.24 A higher result was also reported in India,6 where the mean practice score of the respondents was 93.0%, and China in which about 90% of the study subjects had a good COVID-19 prevention practices.25 Appropriate preventive initiatives will help to save millions of people’s lives and reduce the cost of medicine and supportive care.
The current study also found that individuals aged 45 and up were 3.2 times more likely to apply good COVID-19 prevention practice than those aged 18 to 24 years (AOR: 3.2; 95% CI; 1.7–6.1). The current result is in line with the research conducted in Egypt, India, Jordan, Bangladesh, Gondar, and Dire Dawa City administration.5,6,9,10,13,26 Because the elderly have a larger chance of contracting and developing complications from the diseases, they used better preventative strategies.15
The survey also found that people with a secondary education or higher were 3.1 times more likely to apply good prevention practices than those who could not read or write (AOR: 3.1; 95% CI: 1.4–6.6). This finding is supported by the study done in Jordan5 and Bangladeshi,16 where higher education is associated with good COVID-19 prevention practices.
Moreover, the study found that respondents having a monthly income of greater than or equal to 2,001.00 ETB were 1.9 times more likely to employ better COVID-19 prevention practices than those who had a monthly income of less than or equal to 499 ETB (AOR: 1.9; 95% CI; 1.1–3.4). The present finding is consistent with the study done in Egypt10 and Bangladeshi,16 where poor income was associated with poor COVID-19 prevention practices. This suggests that a lack of sufficient income to carry out various prevention practices is an obstacle to lowering the risk of infection.15
Conclusion
Even though the majority of farmers had satisfactory knowledge, the survey found that a considerable proportion of them had a negative attitude and poor COVID-19 prevention practices. Age, educational status, and monthly income of the respondents were significantly associated (p<0.05) with COVID-19 prevention practices. As a result, steps should be taken to improve the attitudes, educational status, and income level of the farmers to minimize the risk of COVID-19 exposure. This can be achieved by informing the vulnerable population, which may be at risk of contracting COVID-19, about the pandemic’s seriousness and political, social, economic, and health consequences on a regular and timely basis. For those who cannot afford it, hand sanitizer and a face mask should be given. Vaccines should also be available for the elderly.
Ethical Consideration
All of the methods used in this study were done following the Helsinki declaration. As a result, ethical clearance was obtained from the ethical review board of Wollo University College of Medicine and Health Science. A formal letter of cooperation was also written to the town administration. Because not all of the study participants were educated, obtaining written consent from them was difficult. As a result, after receiving ethical review board permission, verbal consent was received from study participants. Before starting the interview, the data collector explained the purpose of the study for all the participants, and verbal consent was obtained from the study participants. During data collection, individuals with COVID-19 symptoms were linked to the surrounding health institution for screening and further treatment. All the information obtained from each study participant was kept confidential.
Acknowledgment
First, the authors wish to express their gratitude to Wollo University’s College of Medicine and Health Sciences for providing the funds necessary to duplicate the data collection tool. The authors would like to express their gratitude to the Dawa Chefa District Administration for providing the necessary information required to conduct the study. Finally, the authors would like to express their gratitude to the data collectors, supervisors, and participants in the research.
Author's Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Khader Y, Al Nsour M, Al-Batayneh OB, et al. Dentists’ awareness, perception, and attitude regarding COVID-19 and infection control: Cross-sectional study among Jordanian dentists. JMIR Public Health Surveill. 2020;6(2):1–7. doi:10.2196/18798
2. Schoeman D, Fielding BC. Coronavirus envelope protein: current knowledge. Virol J. 2019;16(69):1–22.
3. Giao H, Han NTN, Khanh TV, Ngan VK, Tam VV, Le An P. Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pac J Trop Med. 2020;13(6):260–265. doi:10.4103/1995-7645.280396
4. Adhikari SP, Meng S, Wu YJ, et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infect Dis Poverty. 2020;9(1):1–12. doi:10.1186/s40249-020-00646-x
5. Elayeh E, Aleidi SM, Ya’acoub R, Haddadin RN, Mallhi TH. Before and after case reporting: a comparison of the knowledge, attitude and practices of the Jordanian population towards COVID-19. PLoS One. 2020;15(10):1–17. doi:10.1371/journal.pone.0240780
6. Yousaf MA, Noreen M, Saleem T, Yousaf I. A cross-sectional survey of Knowledge, Attitude, and Practices (KAP) toward pandemic COVID-19 among the general population of Jammu and Kashmir, India. Soc Work Public Health. 2020;35(7):569–578. doi:10.1080/19371918.2020.1806983
7. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
8. Hussain I, Majeed A, Imran I, et al. Knowledge, attitude, and practices toward COVID-19 in primary healthcare providers: a Cross-Sectional Study from three tertiary care hospitals of Peshawar, Pakistan. J Community Health. 2020;0123456789.
9. Amsalu B, Guta A, Seyoum Z, et al. Practice of COVID-19 prevention measures and associated factors among residents of Dire Dawa City, Eastern Ethiopia: Community-Based Study. J Multidiscip Healthc. 2021;14:219–228. doi:10.2147/JMDH.S292409
10. Kasemy ZA, Bahbah WA, Zewain SK, et al. Knowledge, attitude and practice toward COVID-19 among Egyptians. J Epidemiol Glob Health. 2020;10(4):378–385. doi:10.2991/jegh.k.200909.001
11. Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
12. Hung L. The SARS epidemic in Hong Kong. What lessons have we learned? J R Soc Med. 2003;57(9):652–654.
13. Islam S, Emran GI, Rahman E, et al. Knowledge, attitudes and practices associated with the COVID-19 among slum dwellers resided in Dhaka City: a Bangladeshi interview-based survey. J Public Health. 2020;1–13.
14. Hager E, Odetokun IA, Bolarinwa O, et al. Knowledge, attitude, and perceptions towards the 2019 coronavirus pandemic: a bi-national survey in Africa. PLoS One. 2020;15(7):1–13. doi:10.1371/journal.pone.0236918
15. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E, Tu W-J. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):1–15. doi:10.1371/journal.pone.0233668
16. Ferdous Z, Islam S, Sikder T, Mosaddek AS, Zegarra-Valdivia JA, Gozal D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: an online-based cross-sectional study. PLoS One. 2020;15(10):1–17. doi:10.1371/journal.pone.0239254
17. Jalloh MF, Robinson SJ, Corker J, et al. Knowledge, attitudes, and practices related to ebola virus disease at the end of a national epidemic — guinea, August 2015. MMWR Morb Mortal Wkly Rep. 2017;66(41):1109–1115. doi:10.15585/mmwr.mm6641a4
18. Agropecuarias FC, Trujillo UN, Pablo AJ. What is the impact of COVID-19 disease on agriculture? Sci Agropecu. 2020;11(1):3–6. doi:10.17268/sci.agropecu.2020.01.00
19. Central Statistical Agency. Federal democratic Republic of Ethiopia central statistical agency population projection of Ethiopia for all regions at wereda level from 2014–2017. 2017. Available from: www.academia.edu›30252151›Federal_Democratic.
20. Amakelew S, Eshetu M, Animut G, Gebeyaw K. Microbial quality of cow milk in Dawa Chefa District, Amhara Region. Adv Dairy Res. 2015;3(2):1–4.
21. Ekpenyong B, Obinwanne CJ, Ovenseri-Ogbomo G, et al. Assessment of knowledge, practice and guidelines towards the novel COVID-19 among eye care practitioners in Nigeria–a Survey-Based Study. Int J Environ Res Public Health. 2020;17(14):1–12. doi:10.3390/ijerph17145141
22. Reuben RC, Danladi MMA, Saleh DA, Ejembi PE. Knowledge, attitudes, and practices towards COVID-19: an epidemiological survey in North-Central Nigeria. J Community Health. 2020;1–14. doi:10.1007/s10900-019-00710-0
23. Mbroh LA. Assessing knowledge, attitude, and practices of hand hygiene among university students. Public Health. 2019;232. Available from: https://cornerstone.lib.mnsu.edu/etdshttps://cornerstone.lib.mnsu.edu/etds/950. Accessed April, 2021
24. Al-Hanawi MK, Angawi K, Alshareef N, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a Cross-Sectional Study. Front Public Health. 2020;8(217):1–10. doi:10.3389/fpubh.2020.00217
25. Peng Y, Pei C, Zheng Y, et al. Knowledge, attitude and practice associated with COVID-19 among university students: a cross-sectional survey in China. BMC Public Health. 2020;20(1292):1–8. doi:10.1186/s12889-020-09392-z
26. Asmelash D, Fasil A, Tegegne Y, Akalu TY, Ferede HA, Aynalem GL. Knowledge, attitudes, and practices toward prevention and early detection of COVID-19 and associated factors among religious clerics and traditional healers in Gondar town, northwest Ethiopia: a community-based study. Risk Manag Healthc Policy. 2020;13:2239–2250. doi:10.2147/RMHP.S277846
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.