")
Back to Journals » International Medical Case Reports Journal » Volume 16
COVID-19 Infection as an Exacerbated Factor of Oral Candidiasis in HIV/AIDS Patient
Received 17 February 2023
Accepted for publication 27 April 2023
Published 18 May 2023 Volume 2023:16 Pages 303—310
DOI https://doi.org/10.2147/IMCRJ.S407597
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
M Hasan Hapid, Tenny Setiani Dewi
Oral Medicine Department, Faculty of Dentistry, Universitas Padjadjaran, Bandung, Indonesia
Correspondence: M Hasan Hapid, Oral Medicine Residency Program, Department of Oral Medicine, Faculty of Dentistry, Universitas Padjadjaran, Jl. Sekeloa Selatan I, Bandung, 40132, Indonesia, Tel +62 878 2296 2270, Email [email protected]
Introduction: Oral candidiasis is an oral mucosal infection caused by Candida sp. This infection can appear in patients with HIV/AIDS associated with immunodeficiency. Another factor that can aggravate the occurrence of oral candidiasis is the COVID-19 infection caused by the SARS-CoV-2 virus as a current pandemic condition. This case report aims to explain the mechanism of COVID-19 infection as a factor that can aggravate the condition of oral candidiasis in HIV/AIDS patients.
Case: A 56-year-old male patient was consulted from the COVID-19 isolation unit to the Department of Oral Medicine with complaints of sore and uncomfortable mouth related to white plaque covering the surface of the tongue. The patient was diagnosed with HIV/AIDS and had a COVID-19 infection. The management instructions were to maintain oral hygiene, administration of antifungal drugs such as nystatin oral suspension and fluconazole, chlorhexidine gluconate 0.2% mouthwash, and vaseline album.
Discussion: Generally, HIV/AIDS patient has dysregulation of the immune system which can suppress host immunity to fight pathogens, making it easy for opportunistic infections such as oral candidiasis. The COVID-19 infection can cause lymphopenia conditions that further reduce the host’s ability to fight pathogens. The SARS-CoV-2 virus can also directly attack various tissues in the oral mucosa which can contribute to exacerbating the severity of oral candidiasis in HIV/AIDS patients.
Conclusion: The COVID-19 infection is a factor that can exacerbate the condition of oral candidiasis in HIV/AIDS patients by further decreasing the host’s immunity and damaging various tissues in the oral mucosa.
Keywords: COVID-19 infection, HIV/AIDS, oral candidiasis
Introduction
Oral candidiasis is one of the most common oral white lesions. This lesion is caused by the fungus Candida sp and Candida albicans is the most common infecting fungal species. Usually, this fungus is a commensal microorganism in the oral cavity but can become a pathogen under certain conditions.1,2 The appearance of oral candidiasis is white to yellowish plaques that can be scrapped and leave an erythematous region, with a slightly higher in margin on the surface of the mucosa. Oral candidiasis can occur on all surfaces of the oral cavity, such as the labial mucosa, buccal mucosa, hard palate, and soft palate, and also spread to the oropharynx.1–3 Oral candidiasis can be caused by various factors, namely local and systemic factors, including poor oral hygiene, chronic local irritation, long-term corticosteroid use, xerostomia, severe blood dyscrasias, head and neck area radiation, systemic disorders such as iron deficiency anemia, diabetes mellitus, impairment of primary immune, leukemic, usage of broad-spectrum antibiotics, endocrine disease, and HIV/AIDS condition.1–3
HIV/AIDS is a disease that causes immunosuppression and is characterized by a decrease in the number of CD4+ cells. This condition can impair the host’s ability to defend against bacterial, fungal, parasitic, and viral infections. This causes a reduction in the patient’s quality of life. The most common oral manifestation in the HIV patient is oral candidiasis, the prevalence can reach up to 95%.4,5 The condition of oral candidiasis in HIV patient can be exacerbated by other factors such as COVID-19 infection.6,7
COVID-19 is a disease caused by SARS-CoV-2 virus. This virus infects the respiratory system and causes various symptoms, from mild to severe, such as coughing, runny nose, fever, sore throat, shortness of breath, and respiratory failure. Currently, covid-19 is causing a pandemic situation in the world.8,9 It has a significant impact and exacerbates a condition of opportunistic infections such as oral candidiasis in HIV/AIDS patients and is associated with immune suppression.6,7
In this case report, the authors would like to describe the mechanism of COVID-19 infection as a factor that exacerbates the condition of oral candidiasis in HIV patients.
Case Presentation
A 56-year-old male patient diagnosed with COVID-19 was referred to the Oral Medicine Department with the chief complaint of an uncomfortable burning sensation in the mouth along with whitish plaque covering the tongue. The complaint appeared a year ago, at first it was just a thin spot, which sometimes arise and disappear. For the last three months, the condition was getting worse parallel to the hospitalization of the patient because infected by COVID-19. Furthermore, in the last five months, he experienced a massive weight loss of 25 kg.
The patient was diagnosed with HIV for the last six years and stopped taking ARV medication during the mid-COVID-19 pandemic. In addition, the patient was diagnosed positive for COVID-19, for 8 months since this examination was carried out and had not come back negative. The symptoms that patient got during COVID-19 infection are coughing, fever, and shortness of breath. The symptoms are getting worse from month to month.
On the first visit when the examination was carried out, the general condition of the patient was compos mentis but looked weak and suffered. The patient was wearing nasal cannula oxygen with a saturation of 94%. The intraoral examination is inadequate, but there was visible a white plaque that covers almost the entire surface of the tongue and intraoral mucosa (Figure 1).
 |
Figure 1 Whole of the intraoral mucosa and tongue surface covered by white plaque. |
The patient underwent various supporting examinations including complete blood count, examination of CD4+ count, and HIV viral load, which can be seen in Table 1 and Table 2. Based on the results of the investigations carried out, the patient has anemia, lymphopenia, also HIV positive with high viral load results, and COVID-19 infection for 8 months. In conclusion, based on the history, clinical examination, and supporting examinations, it was found that the patient was diagnosed with HIV stage IV with wasting syndrome, confirmed COVID-19 severe case, and intraoral diagnosis as pseudomembranous oral candidiasis.
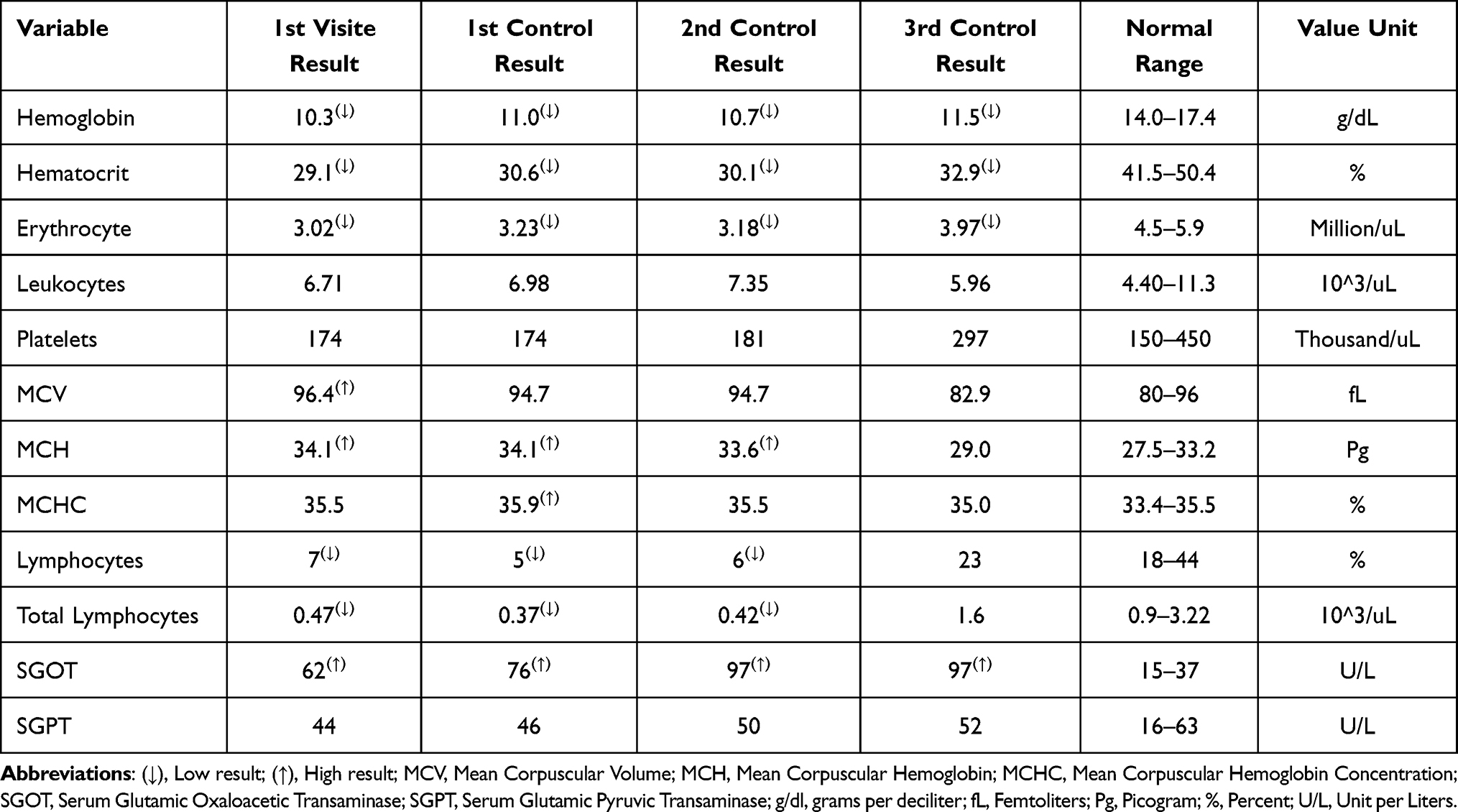 |
Table 1 Blood Laboratory Examination Results |
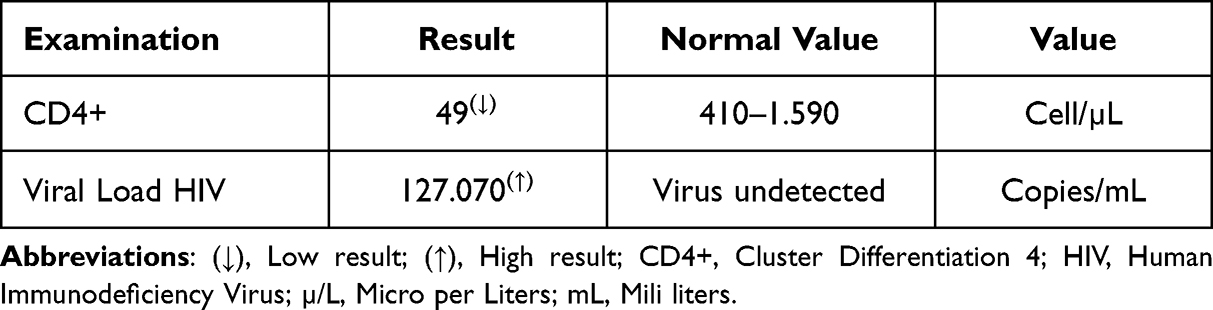 |
Table 2 CD4+ Test Results and HIV Viral Load |
The management for this case from Department of Internal Medicine were given Co-Trimoxazole (Trimetropin/Sulfamethoxazole), Efavirenz/Emtricitabine, Tenofovir, Lovenox, Enoxaparin Sodium, Anticoagulant, Remdesivir, and Vitamin D 5000 IU. While the management provided by the Department of Oral Medicine were in form of education and oral hygiene instruction, including brushing the teeth and tongue at least two times a day and administering nystatin oral suspension 4 times 2 mL per day by swishing for a minute before spit.
At the first medical control, showing that the general condition of the patient still looked breathless, with thick white plaques that covered almost the entire intra-oral mucosa conditions still showed in the mouth even worse, oral candidiasis conditions spread to the oropharynx. The patient still had difficulty following the instructions given, such as brushing his teeth and tongue regularly because of the general condition of the patient. The results of the intraoral examination can be seen in Figure 2.
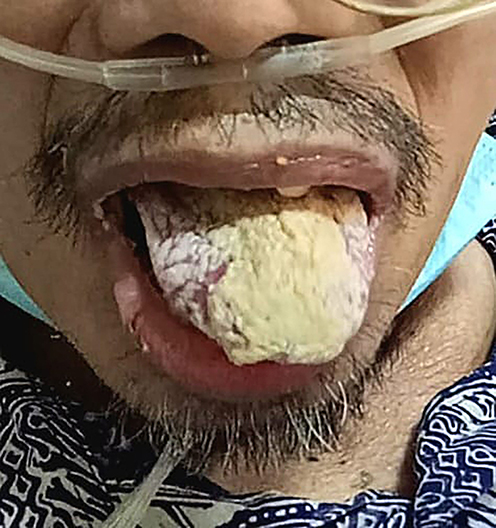 |
Figure 2 First control - thick plaques still covering of intraoral mucosa and tongue surface of the patient. |
The patient was instructed to continue maintaining oral hygiene, discontinue the usage of nystatin oral suspension, and replaced it with systemic antifungal administration of fluconazole. Because the patient is struggling in cleaning his teeth and tongue mechanically, we administered chlorhexidine gluconate mouthwash 0.2% of 10 mL swish and spit three times a day to prevent secondary infection.
During the second medical control, the patient’s general condition improved, less shortness of breath was visible and the patient was able to follow the instructions from the previous visit. In the intraoral examination, it was found that the white plaque on the surface of the tongue had thinned. An overview of the intraoral examination can be seen in Figure 3.
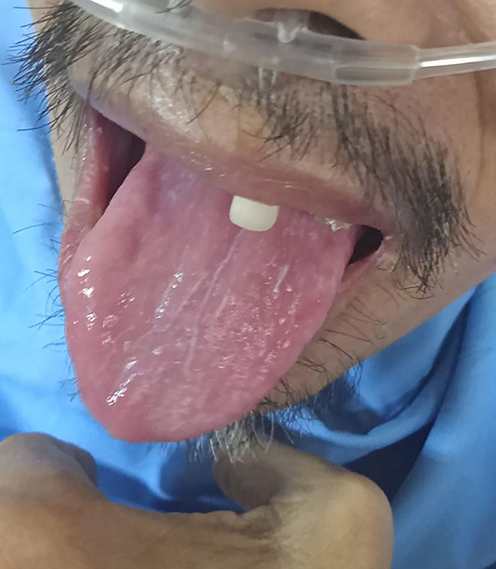 |
Figure 3 White plaque covering the intraoral mucosa and the surface of the tongue is getting thinner. |
The patient was instructed to maintain the cleanliness of his oral cavity by brushing his teeth and tongue twice a day, continue to use chlorhexidine gluconate three times a day and additional therapy was given to apply a thin layer of Vaseline album on the upper and lower lips, because chapped lips were visible.
During the third medical control, the general condition of the patient was getting better compared to the previous visit, without any shortness of breath, but the patient’s lip was still dry and exfoliation was visible. While the white plaque covering the tongue disappeared completely (Figure 4). The instructions given to the patient are still the same as the previous visit.
 |
Figure 4 The disappearance of white plaque covering intraoral mucosa and the surface of the tongue patient. |
Treatment and monitoring that is carried out periodically give the expected results. Chief complaints of pain and discomfort experienced by the patient and the white plaque that covers the patient’s tongue were resolved completely. The good general condition of the patient makes the patient cooperative and supports the patient in carrying out the instructions given.
Discussion
Oral candidiasis is an opportunistic infection of the oral cavity caused by Candida sp, especially Candida albicans.2,10 This fungus is a dimorphic organism which in a non-pathogenic condition is part of the normal microflora of oral cavity.11,12 The prevalence of Candida species in oral cavity of healthy humans is around 40–60%.11 When there is a change in the environment of oral cavity, the fungus will transform from commensal to pathogenic fungus, and cause the formation of hyphae.11,12 The clinical features of candida infection that often appear are (1) pseudomembranous candidiasis, (2) hyperplastic candidiasis, (3) erythematous candidiasis, and (4) angular cheilitis.2,10
Oral candidiasis often occurs in patients with immunocompromised conditions such as those with HIV/AIDS. Candidiasis pseudomembranous is the most frequent type of Candida infection that occur along this condition. It appears not only in the oral cavity but can spread to the oropharynx region, known as oropharyngeal candidiasis. This condition usually affects most people who infected with severe condition HIV (stage 4 HIV) or AIDS conditions. Oral candidiasis can be used as a marker in development of HIV infection before another severe condition occurs and it can occur from months to years.2,10
In HIV/AIDS patients, there is a decrease the number of CD4+ T cells which can impair immune function. It also reduces the protection of the oral mucosa against infections, including Candida sp. So that it can be concluded that the predisposing factor for oral candidiasis in HIV/AIDS patients is immune dysfunction. In one study, HIV/AIDS patients with a decrease in the number of CD4+ T cells by 25% could influence the development of oral candidiasis and the prevalence of oral candidiasis in HIV/AIDS sufferers reached 62–93%.9–11,13
In this case, the patient was diagnosed with HIV/AIDS and experienced oral candidiasis which was exacerbated by COVID-19 infection. The current COVID-19 infection is a pandemic problem worldwide. COVID-19 infection is caused by the SARS-CoV-2 virus which can attack the upper respiratory system and can even reach the lower respiratory tract. As a defensive mechanism of the body’s innate immunity, virus-infected cells are phagocytosed by antigen-presenting cells (APC) such as dendritic cells (DC) or macrophages then undergo apoptosis. These APC cells migrate to the lymph nodes to present viral antigens to T cells as an acquired immune response. CD4+ T cells and CD8+ T cells have a major role in fighting the SARS-CoV-2 virus. CD4+ T cells activate B cells to promote the production of virus-specific antibodies, while CD8+ T cells can directly kill virus-infected cells.10
During the initial infection with mild symptoms of COVID-19, the number of lymphocytes were normal, whereas in severe COVID-19 infection, there was a decrease in the number of lymphocytes. in this case, a drastic reduction in T helper (CD4+) and cytotoxic (CD8+) cells.9,14 COVID-19 patients who are hospitalized usually have severe symptoms. The severity of the disease is related to the decreased number of blood lymphocytes and indicates impaired immune function.14 The lymphopenic condition also inhibits viral clearance and stimulates macrophages to release inflammatory mediators as a cytokine storm that can cause organ dysfunction. In this condition, CD4+ are important in mediating protective humoral immunity by stimulating B cells to produce virus-specific antibodies. On the other hand, CD8+ is responsible for eliminating infected cells, mainly through the production of perforin and granzymes, and has a major role in controlling various types of viruses through the secretion of cytokines.9 In this case report, the patient experienced severe clinical symptoms and decrease in the number of lymphocyte cells and CD4+ count which can be seen in the results of laboratory tests.2
All CD4+ cells such as T helper cells, macrophages, dendritic cells, and astrocytes are susceptible to the HIV virus.10 CD4+ T cells have an important role in against viral infections. Interrelation between the patients with HIV/AIDS and COVID-19 infection can be seen in the clinical feature, such as lymphopenia and a drastic decrease in the number of CD4+ T cells.9
The low level of CD4+ cells causes the antigen-specific immune response impaired for controlling the virus.9 It can exacerbate the development of COVID-19 infection and experience more severe complications in HIV/AIDS patients due to the synergistic effect of the two viruses.14 In this case report, the patient had a COVID-19 infection that lasted for 8 months and had not been resolved until the time this examination was carried out, marked by antigen and PCR tests which always showed positive results for being infected with COVID-19, and there was an increase in viral loads up to 127,070 copies/mL. In line with previous case reports, a patient infected with SARS-CoV-2 and HIV with a low CD4+ cell count exhibited a much slower SARS-CoV-2-specific IgG and IgM response and a prolonged course of the disease.14
Apart from function in the dysregulation of the body’s immunity which can exacerbate oral candidiasis, COVID-19 infection can also affect various conditions in the oral cavity. Angiotensin-converting enzyme 2 (ACE 2) is a receptor for SARS-CoV-2 virus. It expressed in the lungs, heart, ileum, kidneys, and bladder, and also found in various oral mucosal tissues. The SAR-Cov 2 virus can attack the ACE 2 receptors in the salivary glands. It causes salivary gland dysfunction and insufficient saliva secretion (xerostomia). The hypofunction of the salivary glands can change the oral microbiota and increase the risk of candidiasis. There was a significant negative correlation between decreased salivary flow rate and higher Candida colony formation in patients with xerostomia. This condition also results in increased morbidity.2,10,15
Besides the ability of invading directly various tissues in the oral mucosa, the SARS-CoV-2 virus can enter the central nervous system (CNS) via intranasal and peripheral nerves that express ACE2 receptors. The virus enters the peripheral nerves then spreads to the CNS affecting sensory and autonomic innervation of the parotid glands also parasympathetic innervation of the submandibular glands. This can exacerbate xerostomia, thereby increasing the risk of Candida infection.2,15
The initial management for oral candidiasis is by administering topical antifungal, such as nystatin oral suspension. This is a first-line drug for oral candidiasis. The administration of this antifungal is focused on suppressing the reproduction of Candida species.3 This medication disturbs the colonies of Candida sp that adhere to the oral mucosa’s epithelial cells, altered the formation of germ tube sheaths, and relative cell surface hydrophobicity. Therefore, the absorption of this medication into the mucosal epithelium may benefit the host to withstand yeast or hyphal formation.16 The use of nystatin oral suspension by swallowing could impair the liver’s normal function, which is marked by increased SGOT levels. In order to avoid this condition, we suggest the patient in this case to only swish and spit the drugs, because the patient already has a history of elevated liver enzymes.
Patients with severe HIV/AIDS conditions usually suffer Candida infections that affect the oral cavity and spread to the oropharynx and esophagus, therefore longer and higher doses of antifungals are required. The administration of nystatin oral suspension is usually given for mild to moderate condition when it comes to severe cases, the administration of fluconazole tablets may be more effective. About 95% of oral candidiasis can be resolve completely within 7–14 days.2,16
The administration of 0.2% chlorhexidine gluconate mouthwash was used in this case for antiseptic effect which has broad-spectrum antibacterial properties and at the same time has an antifungal effect to control Candida colonies. These topical bactericidal properties also prevent secondary infection which is objective in healing oral lesion.16,17 For the cheilitis exfoliative condition, a Vaseline album was administered to prevent more extensive chapped and wider peel of the lips. Instructions for maintaining oral health are also important because the normal flora is always in homeostasis condition with a clean oral cavity.Considering one of the factors that cause oral candidiasis is poor oral health.3,18 He also gave informed consent to the publication of this case report’s data and images. The institution has already approved to publish this case report.
Conclusion
HIV is an immunocompromised condition. Opportunistic infections such as oral candidiasis may occur. COVID-19 infection can cause lymphopenia resulting in an inadequate immune response. In addition, the SARS-Cov-2 virus can also damage various tissues in the oral mucosa, resulting in a higher risk of infection and more severe symptoms of oral candidiasis.
Acknowledgments
The authors would like to thank the patient who participated kindly in this case report. This study was approved by Oral Medicine Department, Faculty of Dentistry, Padjadjaran University.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Pérez-Gracia MT, Fernandez C, Cebriab BM. Chronic Hyperplastic Candidiasis of the oral mucosa: case report. HSOA J Clin Stud Med Case Rep. 2014;1(1):1–3. doi:10.24966/CSMC-8801/100001
2. Shetti A, Gupta I, Charantimath SM. Oral candidiasis: aiding in the diagnosis of HIV—a case report. Hindawi Publishing Corporation Case Reports in Dentistry. 2011;2011:1–4. doi:10.1155/2011/929616
3. Keser G, Öztürk M, Namdar Pekiner F. Assessment of Awareness and Knowlwdge of Oral Cancer Among Tobacco Using Dental Patients. Clin Exp Health Sci. 2021;11:279–284. doi:10.33808/clinexphealthsci.862928
4. Danwang C, Noubiap JJ, Robert A, Yombi JC. Outcomes of patients with HIV and COVID-19 co-infection: a systematic review and meta-analysis. AIDS Res Ther. 2022;19(1):1–12. doi:10.1186/s12981-021-00427-y
5. Shah N, Ray JG, Kundu S, Sardana D. Surgical management of chronic hyperplastic candidiasis refractory to systemic antifungal treatment. J Lab Physicians. 2017;9(02):136–139. doi:10.4103/0974-2727.199622
6. Nathania E, Widjaja JT. Candidiasis as secondary infection in post COVID-19: a new problem? J Respirasi. 2021;7(3):127. doi:10.20473/jr.v7-I.3.2021.127-133
7. Nanteza M, Tusiime JB, Kalyango J, Kasangaki A. Association between oral candidiasis and low CD4+ count among HIV positive patients in Hoima regional referral hospital. BMC Oral Health. 2014;14(143):1–6. doi:10.1186/1472-6831-14-143
8. Wu YC, Chen CS, Chan YJ. The outbreak of COVID-19: an overview. J Chin Med Assoc. 2020 doi:;83:217–220. doi:10.1097/JCMA.0000000000000270
9. Peng X, Ouyang J, Isnard S, et al. Sharing CD4+ T cell loss: when COVID-19 and HIV collide on immune system. Front Immunol. 2020;11(December):1–11. doi:10.3389/fimmu.2020.596631
10. Gatechompol S, Avihingsanon A, Putcharoen O, Ruxrungtham K, Kuritzkes DR. COVID-19 and HIV infection co-pandemics and their impact: a review of the literature. AIDS Res Ther. 2021;18(1):1–9. doi:10.1186/s12981-021-00335-1
11. Putranti A, Asmarawati TP, Rachman BE, Nasronudin HU. Oral candidiasis as clinical manifestation of HIV/AIDS infection in Airlangga University hospital patients. IOP Conf Ser Earth Environ Sci. 2018;125(1):012063. doi:10.1088/1755-1315/125/1/012063
12. Suryana K, Suharsono H, Antara IGPJ. Factors associated with oral candidiasis in people living with HIV/AIDS: a case control study. HIV/AIDS Res Palliat Care. 2020;12:33–39. doi:10.2147/HIV.S236304
13. Riou C, du Bruyn E, Stek C, et al. Relationship of SARS-CoV-2–specific CD4 response to COVID-19 severity and impact of HIV-1 and tuberculosis coinfection. J Clin Invest. 2021;131(12):1–15. doi:10.1172/JCI149125
14. Yang Y, Iwasaki A. Impact of Chronic HIV Infection on SARS-Cov-2 Infection, COVID-19 Disease and Vaccines [Internet]. The Global Epidemic; 2021:5–16. doi:10.1007/s11904-021-00590-x
15. Piliang A, Zakiawati D, Nur’aeny N. Xerostomia as a potential condition in patients COVID-19 with tetanus: a case report. Makassar Dent J. 2022;11(1):21–24. doi:10.35856/mdj.v11i1.501
16. Lyu X, Zhao C, Yan ZM, Hua H. Efficacy of nystatin for the treatment of oral candidiasis: a systematic review and meta-analysis. Drug Des Devel Ther. 2016;16(10):1161–1171. doi:10.2147/DDDT.S100795
17. Brookes ZLS, Bescos R, Belfield LA, Ali K, Roberts A. Current uses of chlorhexidine for management of oral disease: a narrative review. J Dent. 2020;103:103497. doi:10.1016/j.jdent.2020.103497
18. Garcia-Cuesta C, Sarrion-Pérez MG, Bagán JV. Current treatment of oral candidiasis: a literature review. J Clin Exp Dent. 2014;6(5):e576–e582. doi:10.4317/jced.51798
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.