")
Back to Journals » International Medical Case Reports Journal » Volume 15
COVID-19 Induced Acute Pancreatitis in a Malagasy Woman Patient: Case Report and Literature Review
Authors Razafindrazoto CI , Hasina Laingonirina DH , Ralaizanaka BM , Randriamifidy NH , Rakotomaharo M , Randrianiaina AF, Rakotoniaina H , Maherison S, Rakotomalala JA , Rasolonjatovo AS, Rakotozafindrabe ALR , Rabenjanahary TH , Razafimahefa SH, Ramanampamonjy RM
Received 22 December 2021
Accepted for publication 24 March 2022
Published 29 March 2022 Volume 2022:15 Pages 125—134
DOI https://doi.org/10.2147/IMCRJ.S355276
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Chantelli Iamblaudiot Razafindrazoto,1 Domoina Harivonjy Hasina Laingonirina,1 Behoavy Mahafaly Ralaizanaka,2 Nitah Harivony Randriamifidy,1 Mialitiana Rakotomaharo,1 Antsa Fihobiana Randrianiaina,1 Henintsoa Rakotoniaina,1 Sonny Maherison,1 Jolivet Auguste Rakotomalala,3 Anjaramalala Sitraka Rasolonjatovo,1 Andry Lalaina Rinà Rakotozafindrabe,1 Tovo Harimanana Rabenjanahary,1 Soloniaina Hélio Razafimahefa,2 Rado Manitrala Ramanampamonjy1
1Unity of Gastroenterology, University Hospital Joseph Raseta Befelatanana, Antananarivo, Madagascar; 2Unity of Hepato-Gastroenterology, University Hospital Andrainjato, Fianarantsoa, Madagascar; 3Unity Hepato-Gastroenterology, University Hospital Mahavoky Atsimo, Mahajanga, Madagascar
Correspondence: Chantelli Iamblaudiot Razafindrazoto, Unity of Gastroenterology, University Hospital Joseph Raseta Befelatanana, Antananarivo, Madagascar, Tel +261342315887, Email [email protected]
Background: SARS-CoV-2 has been described as a respiratory tropic virus since its emergence in December 2019. During the course of the disease, other extra-pulmonary manifestations have been reported in the literature including pancreatic involvement such as acute pancreatitis. This phenomenon linking COVID-19 and acute pancreatitis has been reported by several case reports and cohort studies. No cases had been reported in sub-Saharan Africa and Madagascar. We report one more case Of COVID-19 induced acute pancreatitis in a Malagasy woman patient without risk factors, further consolidating the existing evidence.
Case Presentation: A 44-year-old woman was diagnosed with severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection and had a favorable course under home isolation and drug treatments. One week later, the patient was admitted to hospital with severe acute abdominal pain. Acute pancreatitis was considered according to the revised Atlanta criteria with the presence of the three criteria. Other etiologies of acute pancreatitis (lithiasis, alcohol, hypercalcemia, hypertriglyceridemia, tumor, trauma, surgery) were excluded. Ultimately, a COVID-19 induced acute pancreatitis was retained. The outcome was favorable under symptomatic medical treatment (fluid resuscitation, bowel rest, management of pain and vomiting, and early oral feeding). The patient was discharged after one week of hospitalization.
Conclusion: COVID-19 is a possible etiology of acute pancreatitis. Acute pancreatitis should be routinely ruled out in a patient with COVID-19 infection with acute abdominal pain.
Keywords: acute pancreatitis, COVID-19, Madagascar
Background
The current coronavirus disease 2019 (COVID-19) originated in Wuhan, China in December 2019. COVID-19 disease causes severe acute respiratory syndrome.1 In November 2021, more than 250 million people have been infected worldwide and more than 5 million deaths have occurred.2 Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) is a respiratory-tropic virus with manifestations such as cough, dyspnea and fever.3 Over time, atypical presentations of the disease including cardiac, hepatic, renal, musculoskeletal, gastrointestinal and neurological manifestations have been identified.1 However, gastrointestinal (GI) manifestations of COVID-19 are currently drawn significant attention. GI manifestations are reported in 11.4–61.1% of individuals with COVID-19, with variable onset and severity.3 The majority of COVID-19 associated GI symptoms are mild and self-limiting and include anorexia, diarrhea, nausea, vomiting and abdominal pain.3–5 Abdominal pain is less common than the other symptoms. However, a minority of patients with acute abdominal pain had a real abdominal cause; such as acute pancreatitis (AP), acute appendicitis, intestinal obstruction, bowel ischemia, hemoperitoneum, etc.3,6 COVID-19 has been reported by a number of authors as a possible etiology of AP.1,7–36 Although viral AP has been described in other infections, evidence of pancreatic involvement induced by SARS-CoV-2 infection remains limited. Clinicians involved in the management of AP should be aware of its existence in the context of COVID-19.10 Moreover, no cases have been reported in Madagascar or even in sub-Saharan Africa. We report one more case of SARS-CoV-2 infection induced AP in a Malagasy woman patient without risk factors, further consolidating the existing evidence.
Case Presentation
A 44-year-old woman was admitted to hospital during the 2nd wave of the COVID-19 pandemic in Madagascar (April 2021), for severe epigastric pain. She was neither an alcoholic nor a smoker. The patient did not report a history of trauma or recent surgery. The patient presented a week earlier with asthenia, myalgia, dry cough, a few episodes of difficulty breathing and fever. The Chest computed tomography scan showed bilateral ground glass opacities (Figure 1). COVID-19 reverse transcription polymerase chain reaction (RT-PCR) of nasopharyngeal swabs was positive. A moderate COVID-19 was retained. The patient had a favorable evolution with home isolation and drug management (paracetamol, aspirin, atorvastatin, amoxicillin-clavulanic acid, enoxaparin preventive dose). One week later, severe epigastric pain (visual analog scale 9/10), associated with nausea and vomiting (3–4 times) suddenly appeared, leading to hospitalization. General examination reported a Body mass index of 28.5 kg/m2, a blood pressure of 100/70 mmHg, a heart rate of 64 bpm, a respiratory rate of 26/min and an oxygen saturation of 94%. Physical examination on admission showed epigastric tenderness and abdominal bloating. Laboratory tests reported a serum lipase level at 301 U/L (> 3 X Upper limit of normal), C-reactive protein at 25 mg/L, serum calcium level at 2.2 mmol/L, serum triglyceride level at 2.1 g/L, D-dimer at 805 ng/mL. The other laboratory tests are reported in Table 1. Abdominal ultrasound showed no extrahepatic or intrahepatic lithiasis. The Abdominal computed tomography scan showed a benign edematous pancreatitis with no evidence of gallstones (Figure 2). The outcome was favorable under symptomatic medical treatment associating fluid resuscitation, bowel rest, management of pain and vomiting, preventive dose of enoxaparin and early oral feeding upon pain resolution. The patient was discharged after one week of hospitalization. We ultimately retained the diagnosis of SARS-CoV-2 infection induced AP in a woman patient without risk factors.
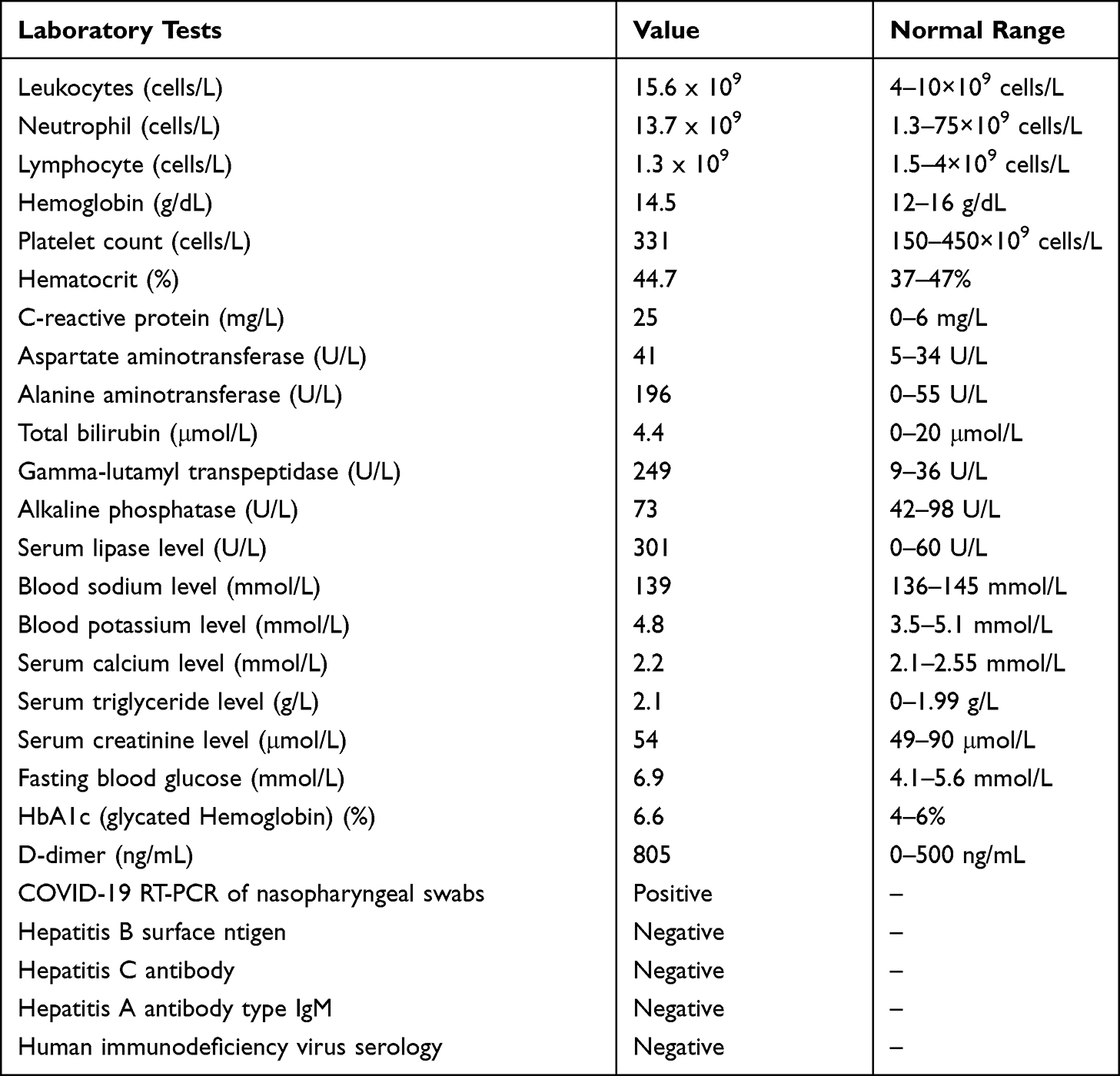 |
Table 1 Laboratory Results |
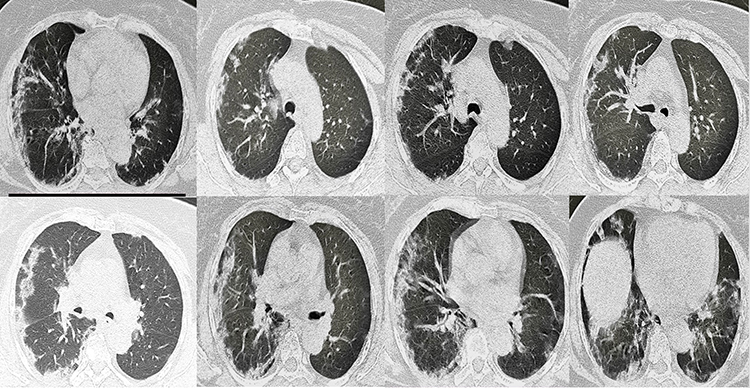 |
Figure 1 Chest computed tomography in a 44-year-old woman showing bilateral ground glass opacities. |
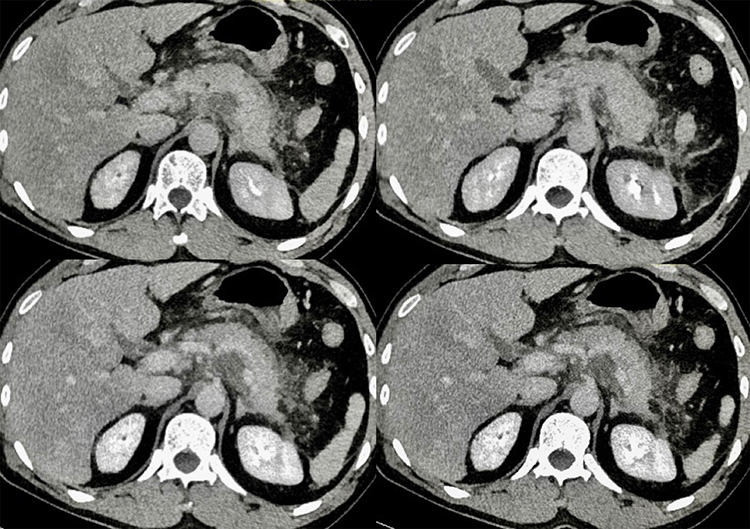 |
Figure 2 Abdominal computed tomography in a 44-year-old woman showing interstitial edema of the pancreas with the homogeneous enhancement of the pancreatic suggesting benign edematous pancreatitis with no evidence of gallstones. |
Discussion and Conclusions
AP appears to be an uncommon complication or association of COVID-19.37 A retrospective American study had objectified a point prevalence of AP of 0.27% (32 patients) out of 11,883 hospitalized COVID-19 patients.38 We report this first case in sub-Saharan Africa of SARS-CoV-2 infection induced AP, to show the possibility of this association in the black African population. The association between COVID-19 and AP had already been reported by many North African authors (2 cases in Egypt, 4 cases in Morocco, 6 cases in Algeria).7,8,27,34,39
The revised Atlanta criteria defines AP if at least 2 of the following 3 criteria are met: (1) severe abdominal pain; (2) serum lipase level (or amylase) more than 3 times the upper limit of normal (ULN); (3) radiological features compatible with AP.40 Our case fulfilled all 3 criteria, allowing us to definitely retain the diagnosis of AP.
The causes of AP are dominated by lithiasis and alcoholic causes (>80%).40,41 But, about 10% of AP cases are directly caused by infectious microorganisms such as parasites, bacteria, and viruses.41 Viral AP has been widely reported in the medical literature. The main viruses reported were cytomegalovirus, Epstein Barr virus, mumps, hepatitis A, B and E viruses, herpes simplex virus, varicella zona virus, coxsackie viruses, echo viruses and human immunodeficiency virus (HIV).7,9,12,14 Recently, COVID-19 has been identified as a possible viral cause of AP. The mechanism of the relationship between pancreatitis and COVID-19 infection remains unknown and multifactorial. Pancreatic injury could be explained by the expression of angiotensin-converting enzyme-2 (ACE-2) receptors on the pancreas, with subsequent injury to the islet of the pancreas with an elevation of serum amylase and lipase enzymes and risk of development of acute diabetes, as in our case.42 Several case reports on SARS-CoV-2 infection induced AP have been reported by numerous authors confirming this relationship between COVID-19 and AP.1,7–36 The description of these numerous case reports of COVID-19 induced AP is reported in Table 2.
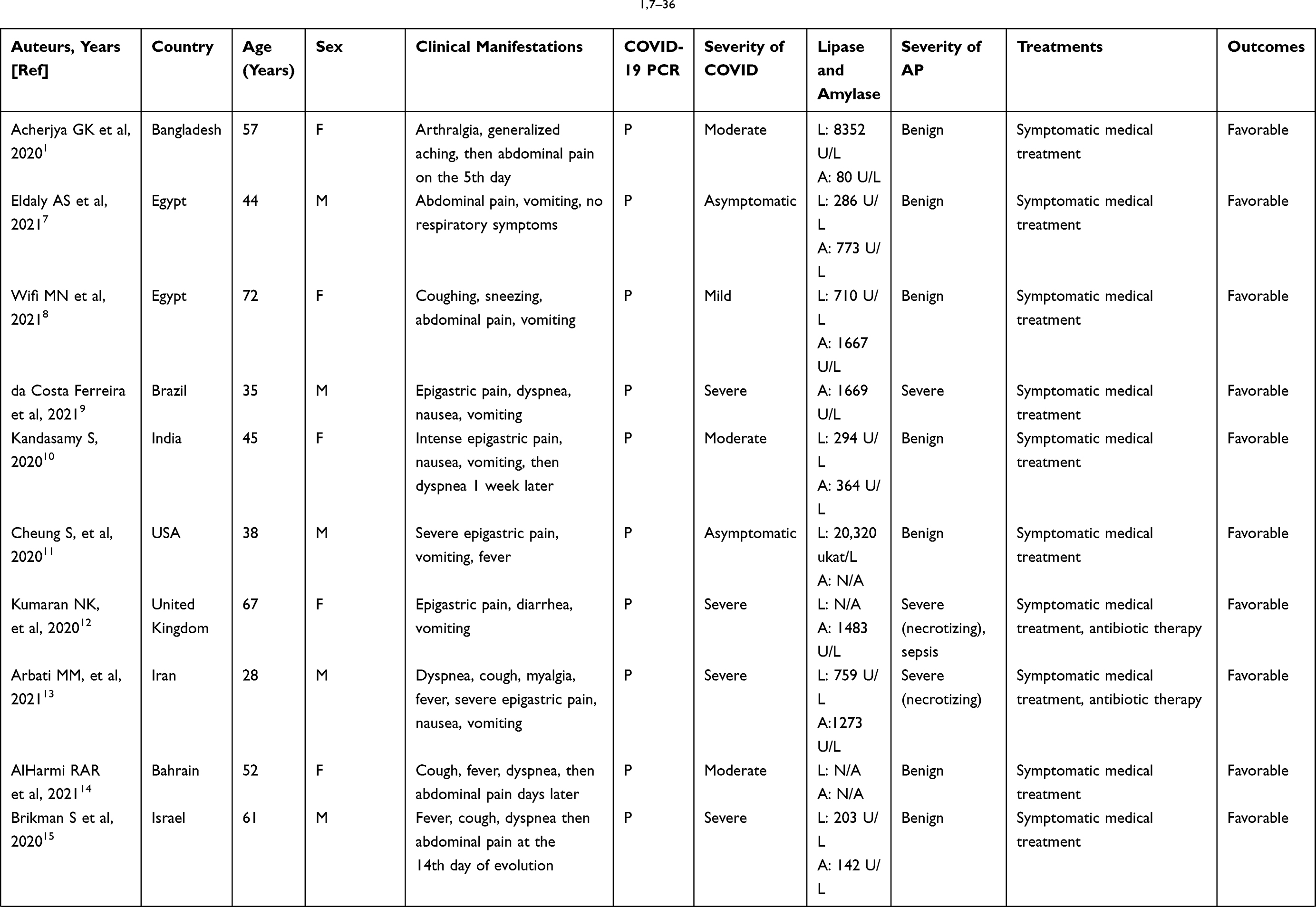 | 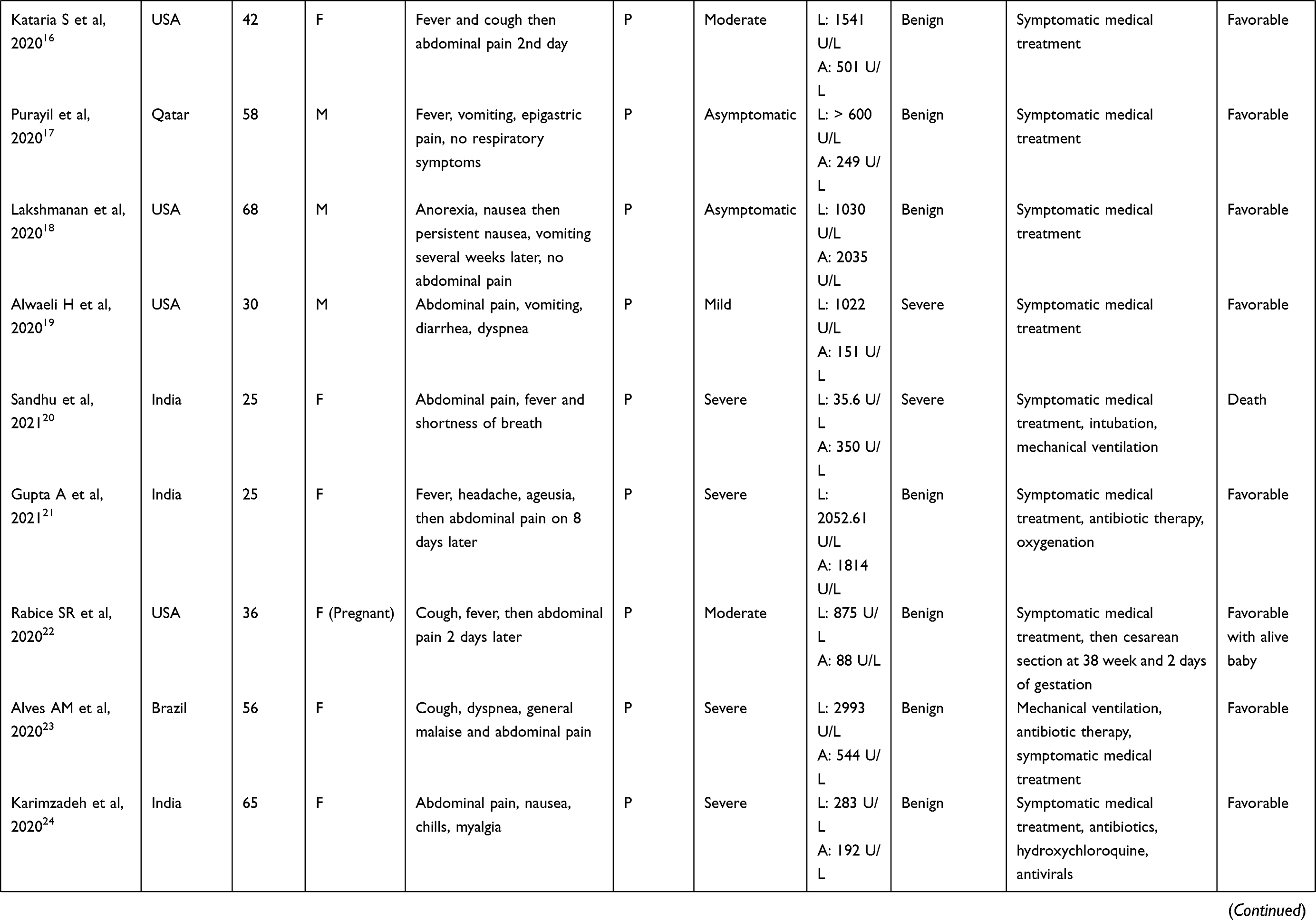 | 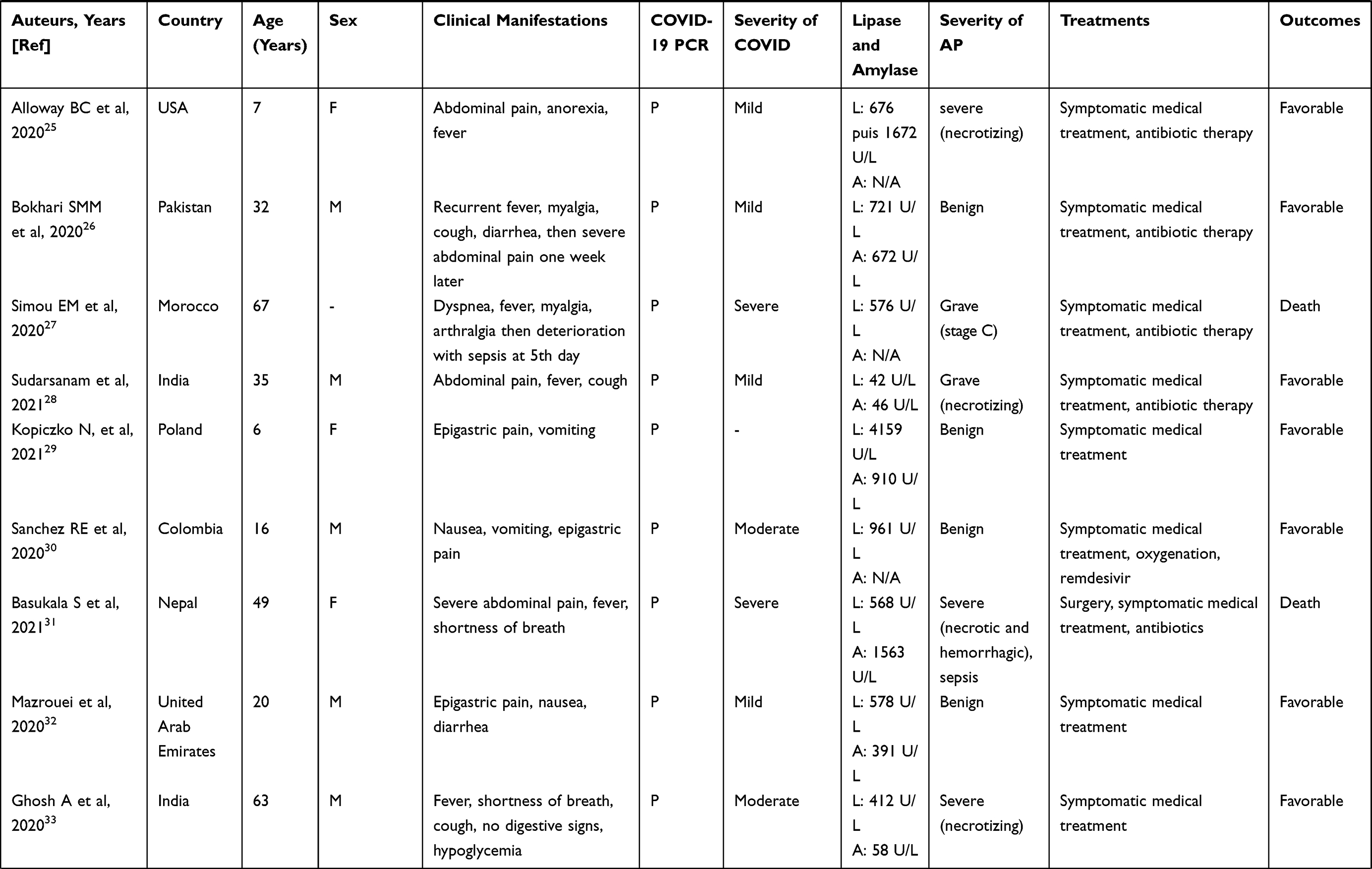 | 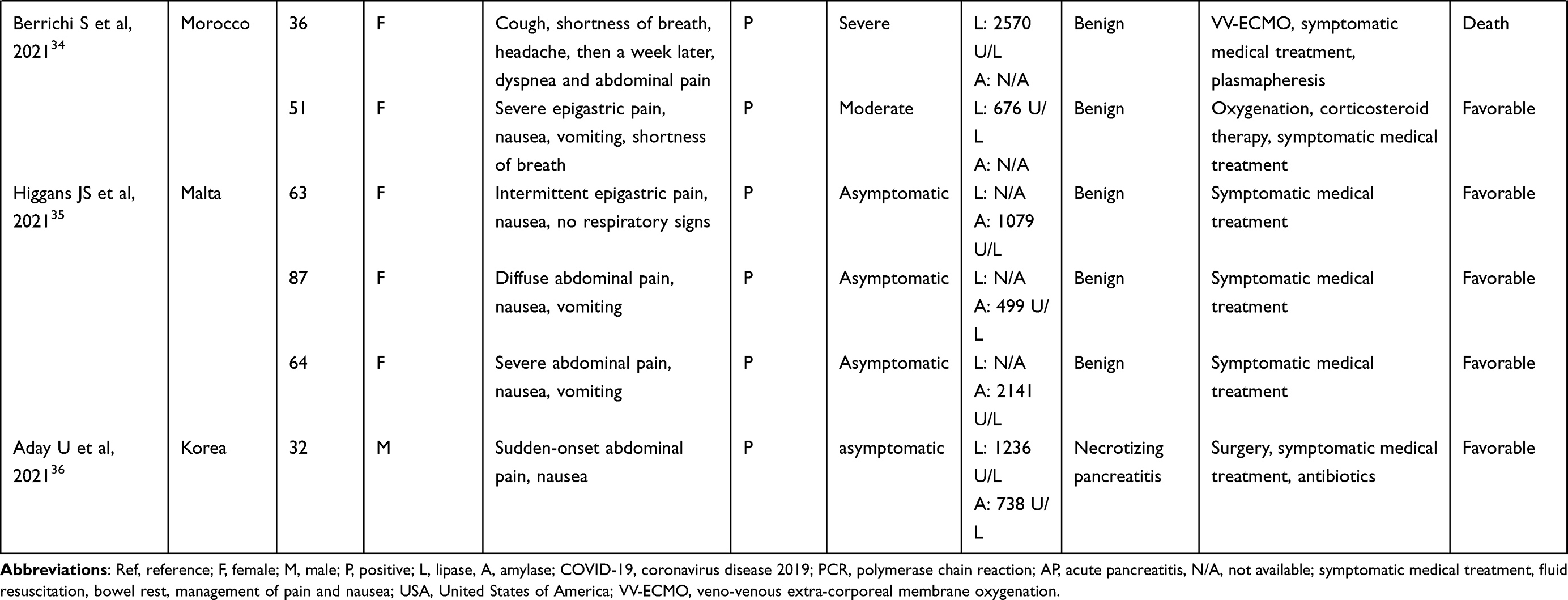 |
Table 2 A Few Reported Cases of COVID-19 Induced Acute Pancreatitis (2020–2021)1,7–36 |
However, in our clinical practice, further investigations should be conducted to exclude other causes in order to establish a correlation between the virus and AP, to avoid misdiagnosis and subsequent mismanagement of the disease. In addition, a retrospective cohort study conducted in 6 US centers had shown that approximately 48% of patients with lipase elevation above 3 x ULN were due to non-pancreatic etiologies.43 Hence the importance of a radiological features in favor of AP and the elimination of all other possible causes of AP. In our case, the other causes of AP (gallstones, alcohol, hypercalcemia, hypertriglyceridemia, trauma, surgery, drugs, comorbidities) were ruled out, in order to retain COVID-19 as a possible origin of AP.
Abdominal pain is a classic gastrointestinal symptom of COVID-19, which may not alert clinicians to a possible AP.3–6 However, all reported cases of COVID-19-induced AP have reported the almost constant presence of abdominal pain, either concomitant or remote from the acute respiratory episode.1,7–36 Hence, the importance of routine pancreatic enzyme testing (Serum lipase and/or amylase level) in COVID-19 patients with abdominal pain.
The management of viral AP is no different from the treatment of AP due to other causes. Because COVID-19 AP is moderate in 70% of reported cases (23/33 of the cases described in Table 2, symptomatic medical treatment (fluid resuscitation, bowel rest, management of pain and vomiting, and early oral feeding) combined with adequate COVID-19 management was usually sufficient, such as our case.1,7–36
The prognosis of COVID-19-related AP was favorable in the majority of reported cases, including our patient.1,7–36 Of the 33 case reports described in Table 2, we had listed 4 deaths, which were concomitantly related to the severity of the AP and the respiratory involvement of COVID-19.1,7–36
In conclusion, SARS-CoV-2 infection is a possible etiology of AP. AP should be routinely ruled out in the presence of concomitant or delayed onset of acute abdominal pain in COVID-19 patients. The prognosis of COVID-19-induced AP remains favorable in the majority of cases.
Ethical Approval and Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images. The publication of this case has been approved by the University Hospital Joseph Raseta Befelatanana Antananarivo Ethics Committee.
Acknowledgments
The authors would like to thank the members of the Department of Gastroenterology of the Joseph Raseta Befelatanana University Hospital.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Acherjya GK, Rahman MM, Islam MT, et al. Acute pancreatitis in a COVID-19 patient: an unusual presentation. Clin Case Rep. 2020;8:3399–3406.
2. COVID-19 coronavirus a pandemic. Available from: https://www.worldometers.info/coronavirus/.
3. Kariyawasam JC, Jayarajah U, Riza R, Abeysuriya V, Seneviratne SL. Gastrointestinal manifestations in COVID-19. Trans R Soc Trop Med Hyg. 2021;115:1–27.
4. Han C, Duan C, Zhang S, et al. Digestive symptoms in COVID-19 patients with mild disease severity: clinical presentation, stool viral RNA testing, and outcomes. Am J Gastroenterol. 2020;115(6):916–923.
5. Pan L, Mu M, Yang P, et al. Clinical characteristics of COVID-19 patients with digestive symptoms in Hubei, China: a descriptive, cross-sectional, multicenter study. Am J Gastroenterol. 2020;115(5):766–773.
6. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069.
7. Eldaly AS, Fath AR, Mashaly SM, Elhadi M. Acute pancreatitis associated with severe acute respiratory syndrome coronavirus-2 infection: a case report and review of literature. J Med Case Rep. 2021;15:461.
8. Wifi MN, Nabil A, Awad A, Eltatawy R. COVID-induced pancreatitis: case report. Egyptian J Int Med. 2021;33:10.
9. da Costa Ferreira CP, Marques KR, de Mattos GHF, de Campos T. Acute pancreatitis in a COVID-19 patient in Brazil: a case report. J Med Case Rep. 2021;15:541.
10. Kandasamy S. An unusual presentation of COVID-19: acute pancreatitis. Ann Hepatobiliary Pancreat Surg. 2020;24(4):539–541. doi:10.14701/ahbps.2020.24.4.539
11. Cheung S, Fuentes AD, Fettterman AD. Recurrent acute pancreatitis in a patients with COVID-19 infection. Am J Case Rep. 2020;21:e927076. doi:10.12659/AJCR.927076
12. Kumaran NK, Karmakar BK, Taylor OM. Coronavirus disease-19 (COVID- 19) associated with acute necrotising pancreatitis (ANP). BMJ Case Rep. 2020;13(9):e237903. doi:10.1136/bcr-2020-237903
13. Arbati MM, Molseghi MH. COVID-19 presenting as acute necrotizing pancreatitis. J Invest Med High Imp Case Rep. 2021;9:1–3.
14. AlHarmi RAR, Fateel T, Sayed Adnan J, AlAwadhi K. Acute pancreatitis in a patient with COVID-19. BMJ Case Rep. 2021;14(2):e239656. doi:10.1136/bcr-2020-239656
15. Brikman S, Denysova V, Menzal H, Dori G. Acute pancreatitis in a 61-years-old man with COVID-19. CMAJ. 2020;192(30):E858–859. doi:10.1503/cmaj.201029
16. Kataria S, Sharif A, Ur Rehman A, Ahmed Z, Hanan A. COVID-19 induced acute pancreatitis: a case report and literature review. Cureus. 2020;12(7):e9169. doi:10.7759/cureus.9169
17. Purayil N, Sirajudeen J, Va N, Mathew J. COVID-19 presenting as acute abdominal pain: a case report. Cureus. 2020;12(8):e9659. doi:10.7759/cureus.9659
18. Lakshmanan S, Malik A. Acute pancreatitis in mild COVID-19 infection. Cureus. 2020;12(8):e9886. doi:10.7759/cureus.9886
19. Alwaeli H, Shabbir M, Khamissi Sobi M, Alwaeli K. A case of severe acute pancreatitis secondary to COVID-19 infection in a 30-year-old male patient. Cureus. 2020;12(11):e11718. doi:10.7759/cureus.11718
20. Sandhu H, Mallik D, Lokavarapu M, Huda F, Basu S. Acute recurrent pancreatitis and COVID-19 infection: a case report with literature review. Cureus. 2021;13(2):e13490. doi:10.7759/cureus.13490
21. Gupta A, Bansal DP, Rijhwani P, Singh V. A case report on acute pancreatitis in a patient with Coronavirus disease 2019 (COVID-19) pneumonia. Cureus. 2021;13(4):e14628. doi:10.7759/cureus.14628
22. Rabice SR, Altshuler PC, Bovet C, Sullivan C, Gagnon AJ. COVID-19 infection presenting as pancreatitis in a pregnant woman: a case report. Case Rep Womens Health. 2020;27:e00228.
23. Alves AM, Yvamoto EY, Marzinotto MAN, Teixeira ACS, Carrilho FJ. SARS-CoV-2 leading to acute pancreatitis: an unusual presentation. Braz J Infect Dis. 2020;24(6):561–564. doi:10.1016/j.bjid.2020.08.011
24. Karimzadeh S, Manzuri A, Ebrahimi M, Tien Huy N. COVID-19 presenting as acute pancreatitis: lessons from a patient in Iran. Pancreatology. 2020;20(5):1024–1025. doi:10.1016/j.pan.2020.06.003
25. Alloway BC, Yaeger SK, Mazzaccaro RJ, Villalobos T, Hardy SG. Suspected case of COVID-19-associated pancreatitis in a child. Radiol Case Rep. 2020;15(8):1309–1312.
26. Bokhari SMM, Mahmood F. Case report: novel Coronavirus-A potential cause of acute pancreatitis? Am J Trop Med Hyg. 2020;103(3):1154–1155.
27. Simou EM, Louardi M, Khaoury I, et al. Coronavirus disease-19 (COVID-19) associated with acute pancreatitis: case report. Pan Afr Med J. 2020;37:150.
28. Sudarsnam H, Ethiraj D, Govarthanan NK, Kalyanasundaram S, Chitra SA, Mohan S. Pancreatitis with normal serum amylase and lipase levels: report of an unusual findings. Oman Med J. 2020;36(5):e304.
29. Kopiczko N, Kwiatek-Sredzinska K, Uscinowicz M, Kowalczuk-Kryston M, Lebensztejn DM. SARS-CoV-2 infection as a cause of acute pancreatitis in a child – a case report. Pediatr Rep. 2021;13:552–557.
30. Sanchez RE, Flahive CB, Mezoff EA, Gariepy C, Hunt G, Vaz KKH. Case report: acute abdominal pain as presentation of pneumonia and acute pancreatitis in a pediatric patient with COVID-19. JPGN Rep. 2020;2(1):e011.
31. Basukala S, Shah KB, Karki B, et al. Acute hemorrhagic necrotizing in patients with COVID-19: a case report and review of literature. J Surg Case Rep. 2021;9:1–4.
32. Al Mazrouei SS, Saeed GA, Al Helali AA. COVID-19-associated acute pancreatitis: a rare cause of acute abdomen. Rad Case Rep. 2020;15:1601–1603.
33. Ghosh A, Gupta V, Misra A. COVID 19 induced acute pancreatitis and pancreatic necrosis in a patient with type 2 diabetes. Diabetes Metab Syndr. 2020;14:2097–2098.
34. Berrichi S, Bouayed Z, Jebar K, et al. Acute pancreatitis as an atypical manifestation of COVID-19: a report of 2 cases. Ann Med Surg. 2021;68:102693.
35. Higgans JS, Bowman S, Abela JE. COVID-19 associated pancreatitis: a mini case-series. Int J Surg Case Rep. 2021;87:106429.
36. Aday U, Gedik E, Kafadar MT, Özbek E. Acute necrotizing pancreatitis coronavirus disease-2019 (COVID-19). Korean J Gastroenterol. 2021;78:353–358.
37. McNabb-Baltar J, Jin DX, Grover AS, et al. Lipase elevation in patients with COVID-19. Am J Gastroenterol. 2020;115:1286–1288.
38. Inamdar S, Benias PC, Liu Y, et al. prevalence, risk factors, and outcomes of hospitalized patients with coronavirus disease 2019 presenting as acute pancreatitis. Gastroenterology. 2020;159(6):2226–2228.
39. Remouche H, Benssetti Houari AK, Kadjam O, et al. COVID-19 et la pancréatite aiguë. J Chir Visc. 2021;158(4):S66.
40. Foster BR, Jensen KK, Bakis G, Shaaban AM, Coakley FV. Revised Atlanta classification for acute pancreatitis: a pictorial essay. RadioGraphics. 2016;36:675–687.
41. Forsmark CE, Swaroop Vege S, Wilcox CM. Acute pancreatitis. N Engl J Med. 2016;375:1972–1981.
42. Liu F, Long X, Zhang W, Chen X, Zhang Z. ACE2 expression in pancreas may cause pancreatic damage after SRAS-Cov-2 infection. Clin Gastroenterol Hepatol. 2020;18(9):2128–2130.
43. Jin DX, Yang AL, Suleiman SL, McNabb-Baltar J, Banks PA. Marked serum lipase elevations are associated with longer hospitalizations in patients with non-pancreatic hyperlipasemia. Gastroenterology. 2019;156(6):
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.