")
Back to Journals » Cancer Management and Research » Volume 12
Cost-Effectiveness of Ribociclib for Hormone Receptor-Positive HER2-Negative Advanced Breast Cancer
Authors Yang J, Han J, Tian M, Tian K, Liao W, Yan X
Received 1 October 2020
Accepted for publication 25 November 2020
Published 15 December 2020 Volume 2020:12 Pages 12905—12913
DOI https://doi.org/10.2147/CMAR.S284556
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Jiangping Yang,1,* Jiaqi Han,1,* Maolang Tian,1 Kun Tian,2 Wenjun Liao,1 Xi Yan3,4
1Department of Head and Neck Oncology and Department of Radiation Oncology, Cancer Center and State Key Laboratory of Biotherapy, West China Hospital, Sichuan University, Chengdu, Sichuan 610041, People’s Republic of China; 2Department of Urology, Institute of Urology, West China Hospital, Sichuan University, Chengdu 610041, People’s Republic of China; 3Department of Head, Neck and Mammary Gland Oncology, Cancer Center, West China Hospital, Sichuan University, Chengdu, Sichuan 610041, People’s Republic of China; 4Laboratory of Molecular Diagnosis of Cancer, Clinical Research Center for Breast, West China Hospital, Sichuan University, Chengdu, Sichuan 610041, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xi Yan
Department of Head, Neck and Mammary Gland Oncology, Cancer Center, West China Hospital, Sichuan University, Chengdu, Sichuan 610041, People’s Republic of China
Tel +86 189 8060 1777
Email [email protected]
Purpose: Ribociclib has provided significant improvements in progression-free survival (PFS) and overall survival (OS) of postmenopausal patients with hormone receptor (HR)-positive and human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer (ABC). However, given the high cost of ribociclib, its value must be evaluated based on cost-effectiveness. Thus, we aimed to explore the cost-effectiveness of ribociclib for postmenopausal patients with HR-positive and HER2-negative ABC.
Methods: A comprehensive Markov model was developed to estimate the cost-effectiveness of ribociclib plus fulvestrant versus placebo plus fulvestrant as first-line treatment for HR-positive, HER2-negative ABC. Variables were estimated based on data from the randomized Phase III MONALEESA-3 trial. Ten-year values were estimated for quality-adjusted life years (QALYs), costs, and incremental cost-effectiveness ratios (ICERs). Direct treatment costs were estimated from the perspective of a United States payer. One-way and probabilistic sensitivity analyses were conducted to confirm the model’s robustness.
Results: Ribociclib plus fulvestrant increased the treatment cost by $382,172 and provided 0.47 QALYs, relative to fulvestrant alone, which corresponded to an ICER of $813,132 per QALY. Sensitivity analyses revealed that ribociclib was unlikely to be cost-effective even under the most favorable assumptions. When the cost of ribociclib was <$1,384, there was a > 50% chance of cost-effectiveness at a willingness-to-pay threshold of $150,000/QALY. Subgroup analyses also confirmed that ribociclib was not cost-effective.
Conclusion: At current drug prices in the United States, ribociclib is unlikely to be cost-effective for treating postmenopausal patients with HR-positive HER2-negative ABC. Despite the clinical benefits of ribociclib, its cost would need to decrease to provide more favorable economic outcomes.
Keywords: cost-effectiveness, ribociclib, fulvestrant, breast cancer, hormone receptor positive
Introduction
Breast cancer is the most common cancer affecting women worldwide, with an estimated 276,480 new cases and 42,170 breast cancer-related deaths in 2020.1 Approximately 70% of breast cancers are positive for hormone receptor (HR) and negative for human epidermal growth factor receptor 2 (HER2).2,3 Endocrine therapy is recommended as the standard treatment for patients with HR-positive, HER2-negative advanced breast cancer (ABC).4 Although endocrine therapy is effective and well-tolerated, primary or secondary endocrine resistance eventually occurs in most patients and leads to disease progression.5 The potential mechanisms underlying endocrine therapy resistance involve increased activity of cyclin-dependent kinases 4 and 6 (CDK 4/6), upregulation of the PI3K/AKT/mTOR signaling pathways, and loss of estrogen receptor expression.6–8
Ribociclib is a novel selective small-molecule inhibitor of CDK4/6 and has been approved in combination with an endocrine-based therapy as a first- or second-line therapy for HR-positive, HER2-negative advanced or metastatic breast cancer.9–12 The randomized phase III MONALEESA-3 trial evaluated ribociclib plus fulvestrant in postmenopausal patients with HR-positive, HER2-negative ABC who have received ≤1 previous endocrine treatment for advanced disease.10 The primary analysis,13 which was published in 2018, revealed that ribociclib plus fulvestrant provided a significant improvement in progression-free survival (PFS) relative to placebo plus fulvestrant (20.5 months vs. 12.8 months; hazard ratio: 0.59, 95% confidence interval [CI]: 0.48–0.73). Furthermore, updated overall survival (OS) data from the MONALEESA-3 trial was published in 2020,10 which revealed that ribociclib plus fulvestrant had a better 42-month OS rate (57.8% vs. 45.9%; hazard ratio: 0.72, 95% CI: 0.57–0.92), with consistent OS benefits across various patient subgroups. However, patients treated with ribociclib experienced more frequent serious adverse events (AEs), including neutropenia, leucopenia, and hepatobiliary toxic effects.10
Although ribociclib provides substantial clinical benefits, its use may increase drug-related costs and overall healthcare costs. Furthermore, the high cost of CDK4/6 inhibitors has made it unclear whether the cost of treatment using ribociclib plus fulvestrant is balanced by the treatment success and increased quality of life, relative to treatment using fulvestrant alone. Therefore, we developed a Markov model to investigate the cost-effectiveness of ribociclib plus fulvestrant, relative to placebo plus fulvestrant, for postmenopausal patients with HR-positive HER2-negative ABC from the perspective of a United States payer.
Materials and Methods
Model Overview
TreeAge Pro 2018 software (TreeAge, Williamstown, Massachusetts) was used to create a comprehensive Markov model for analyzing the health and economic outcomes of treating postmenopausal female patients with HR-positive, HER2-negative ABC with ribociclib plus fulvestrant (Figure 1). The model consisted of four mutually exclusive health states: PFS (entry stage), first progressive disease (1st PD), second progressive disease (2nd PD), and death. Each Markov model cycle length was 4 weeks based on the treatment schedules for the MONALEESA-3 trial.14 The time horizon was 10 years.
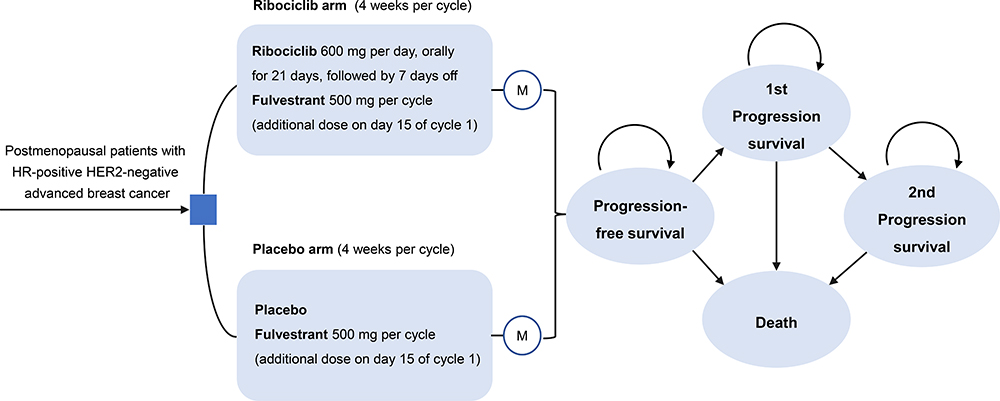 |
Figure 1 Schematics of the decision tree and the Markov state transition model. Abbreviation: M, Markov node. Notes: A network of four health states linked by transitional variables. During each 4-weeks cycle, patients either remained in their assigned health state or progressed to a new health state. It was assumed that the patients could not go back to previous health states. |
We created a hypothetical cohort of patients with baseline demographic and clinical characteristics that were similar to those of the patients included in the MONALEESA-3 trial (Supplementary Table 1). Two treatment groups were considered: (1) ribociclib group, treated with ribociclib (600 mg/day orally on days 1–21 of a 28-day cycle) plus fulvestrant (500 mg intramuscularly on day 1 of each 28-day cycle, with an additional dose on day 15 of cycle 1) and (2) placebo group, treated with placebo plus fulvestrant. We assumed that all patients received their assigned treatment in the PFS state until disease progression, unacceptable toxicity or death. All patients could also continue to receive treatment after progression and until death. At the first progression, subsequent therapy consisted of chemotherapy, hormone therapy, and/or targeted therapy alone (Supplementary Table 2). Subsequent therapy was provided to 81.5% of the ribociclib group (295/362) and 84.7% of patients in the placebo group (177/209), based on the MONALEESA-3 trial. After the second progression, we assumed that both groups received the best supportive care until death.15
The primary outcomes were the estimated values for total costs, life years (LYs), quality-adjusted life years (QALYs), and incremental cost-effectiveness ratios (ICERs). We applied half-cycle corrections to cost and effectiveness values in the model. Costs were based on 2020 US dollars, and costs and survival outcomes were discounted at a 3% annual rate to account for inflation. The ICERs were compared between the two groups based on a previously reported willingness-to-pay (WTP) threshold of $150,000/QALY.16,17
Model Transitions and Survival Estimates
Patients transitioned between health states based on transition probabilities that were calculated using the Kaplan-Meier survival curves for OS, PFS, and PFS2 from the MONALEESA-3 trial.10 First, we extract the data points from the curves using GetData Graph Digitizer (version 2.26), then the data points were applied to fit parametric survival models and survival distributions were tested for goodness-of-fit.18,19 The goodness-of-fit, which was evaluated using the R2 statistic, was used to guide the Weibull survival function for fitting each survival curve to estimate the transition probabilities for each 4-week cycle. A detailed description of the Weibull survival model for comparing the groups is provided in Table 1 and Supplementary Figure 1. The Weibull parameters were applied to estimate the time-dependent transition probabilities from PFS to death, PD to death, or PFS to PD according to the following formula: tp (tu) = 1 - exp {λ (t - u) γ – λtγ} (λ > 0; γ > 0). In that formula, λ represents the distribution scale, γ represents the distribution shape, and u represents the Markov cycle.20 The data analysis was performed using R software (version 3.3.1; http://www.r-project.org).
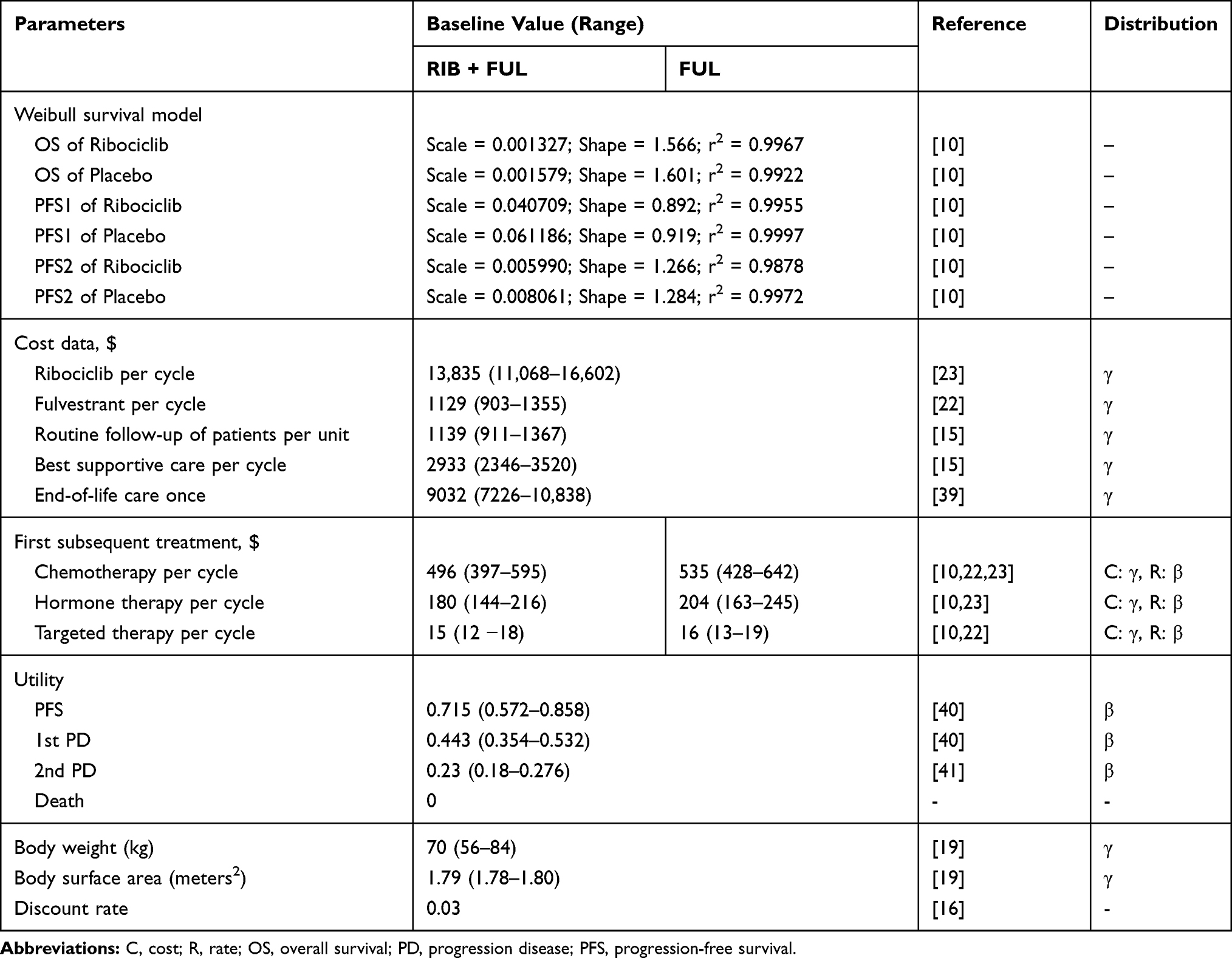 |
Table 1 Model Parameters: Baseline Values, Ranges, and Distributions for Sensitivity Analysis |
Cost and Utility Estimates
The costs associated with cancer treatment included drug acquisition, treatment of serious AEs, (grades 3–4), routine follow-up, best supportive care, and end-of-life care (Tables 1 and 2). The mean values were 70 kg for body weight and 1.79 m2 for body surface area.19,21 Drug doses and dosing schedule for each cycle were extracted from the National Comprehensive Cancer Network guidelines.11 Drug costs per unit were estimated using the April 2020 average sale price from the Centers for Medicare & Medicaid Services.22,23 Additional details on drug doses and unit price can be found in Supplementary Table 2 and Supplementary References.4,9,10,13,22–36
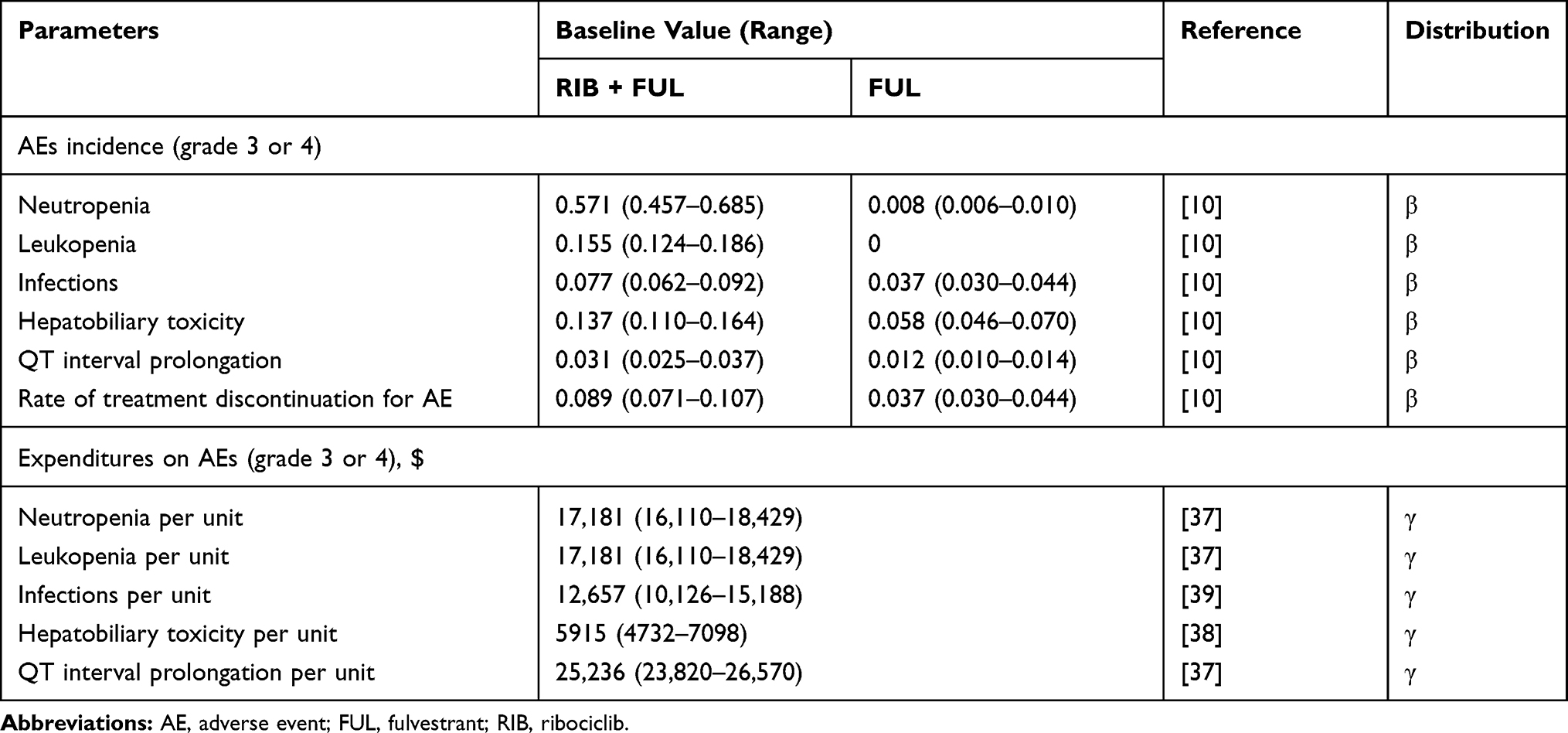 |
Table 2 Incidence and Expenditures on Grade 3 or 4 AEs |
During the MONALEESA-3 trial, patients underwent follow-up laboratory testing (hematology parameters, prothrombin time, and international normalized ratio), standard 12-lead electrocardiography within 15 days after the last dose, radiological assessments (computed tomography or magnetic resonance MR imaging) every 8 weeks during the first 18 months and every 12 weeks thereafter until disease progression, as well as evaluation of left ventricular ejection fraction as clinically indicated.10,13 We only considered the costs of grade 3–4 AEs with significantly different inter-group rates based on the MONALEESA-3 trial, which were neutropenia, leukopenia, infection, hepatobiliary toxicity, and QT interval prolongation (Table 2). The costs for managing each AE episode were derived from previous reports.37–39 Additionally, we estimated the cost of each serious AE by multiplying its unit cost by the probability of it occurring during the treatment.
Baseline utility values were adopted from previous reports regarding health utilities for ABC,40,41 which were assumed to be 0.715 for all patients in the PFS stage, 0.443 for patients receiving subsequent treatment during the 1st PD stage, and 0.230 for patients who progressed to the 2nd PD stage (Table 1).
Sensitivity Analysis
Sensitivity analyses were conducted to evaluate the robustness of the model. One-way sensitivity analyses were performed by varying the value of one parameter at a time over its defined range to examine its effects on the ICER. All parameters in the one-way sensitivity analyses were derived from the MONALEESA-3 trial and the published literature; when reported data were not available, the variance was defined as 20% of the base-case value.17,19 The results of the one-way sensitivity analyses were presented in a tornado diagram. The probabilistic sensitivity analysis involved 10,000 Monte Carlo simulations, with each simulation randomly sampling from the distributions for all parameters. Gamma distribution was assigned to the costs and beta distributions were assigned to clinical probabilities, utility scores and the transition probability. Subgroup analyses were also conducted to explore the probability of ribociclib being cost-effective for patients with different clinical characteristics (Supplementary Table 3). The results were presented as scatter plots and cost-effectiveness acceptability curves to predict the probability of cost-effectiveness for each treatment strategy under the different WTP thresholds. Our study followed the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement.42 Additional details can be found in Supplementary Table 4.
Results
Base Case Results
The results of the basic cost-effectiveness analysis are presented in Table 3. Over a 10-year time horizon, ribociclib plus fulvestrant resulted in a significantly higher incremental cost of $382,172 relative to placebo plus fulvestrant ($500,523 vs. $118,351). Ribociclib plus fulvestrant provided 2.17 QALYs (4.21 LYs) and placebo plus fulvestrant provided 1.70 QALYs (3.56 LYs), which indicated that patients treated using ribociclib plus fulvestrant lived 7.8 months longer than patients treated using fulvestrant alone. This corresponded to an ICER of $813,132/QALY ($587,956/LY) at a WTP threshold of $150,000/QALY. The ICERs for ribociclib over placebo were $876,870 in the PFS state and $19,640 in the 1st PD state. However, the ICER for placebo over ribociclib was $211,600 in the 2nd PD state, with a mean incremental cost of $4,232 and 0.02 QALYs.
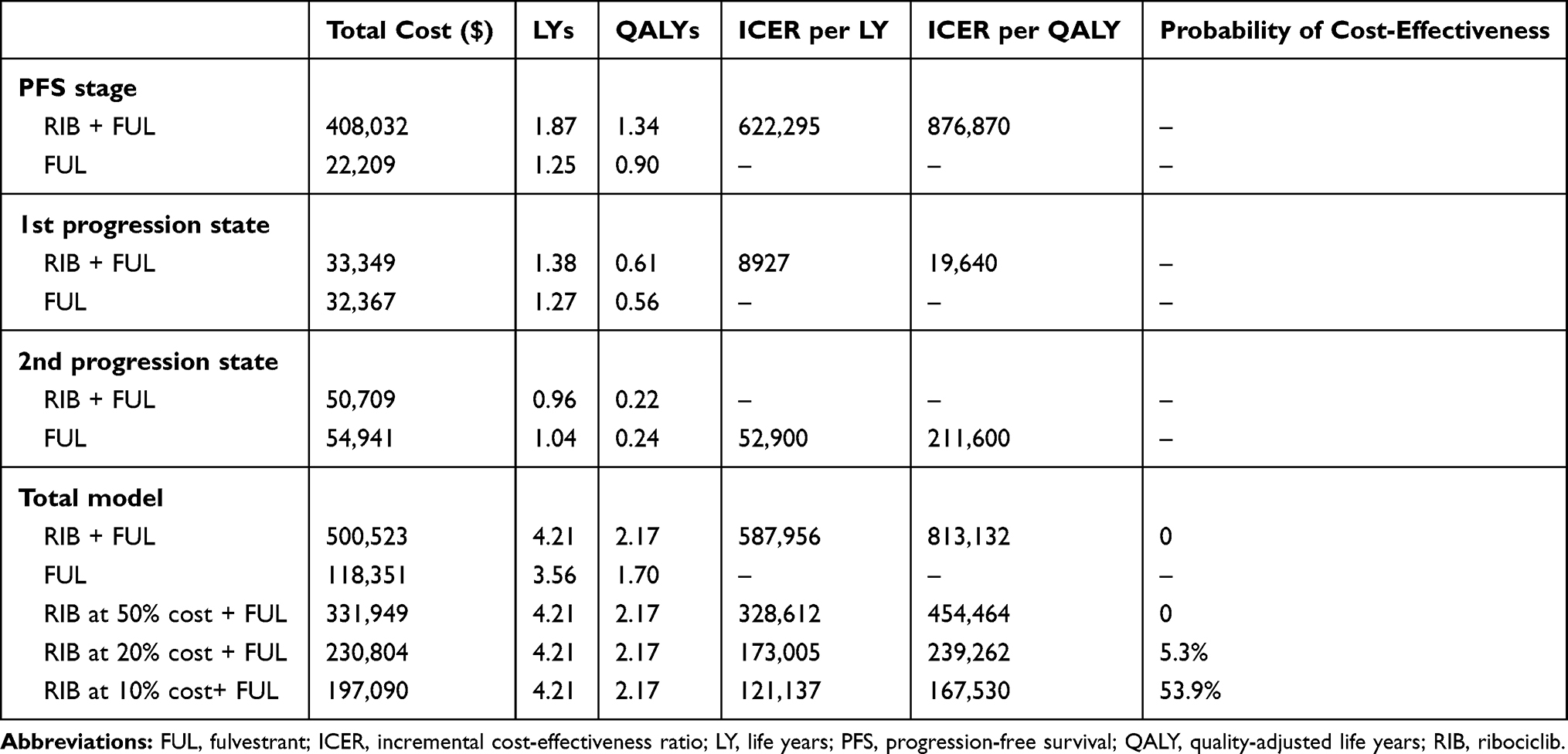 |
Table 3 Base Case Results |
The subgroup analyses revealed that the ICER for ribociclib plus fulvestrant varied from $512,190/QALY for patients with bone metastasis only to $634,849/QALY for patients with liver or lung metastasis (Supplementary Table 3).
Sensitivity Analysis
One-way sensitivity analyses (Figure 2) suggested that the greatest influence on ICER was determined by the utility of PFS (ranging from 0.57 to 0.86, with ICERs ranging from $676,990/QALY to $987,844/QALY) followed by the cost of ribociclib every 4 weeks. The minimum ICER ($661,646/QALY) was observed if the cost of ribociclib was $11,068/cycle. Other influential variables, including health state utilities, cost of fulvestrant per cycle, and the incidence of neutropenia in the ribociclib group, had minimal effects on the model outcomes. None of the ICERs in the model significantly changed when the parameters were altered within the estimated ranges.
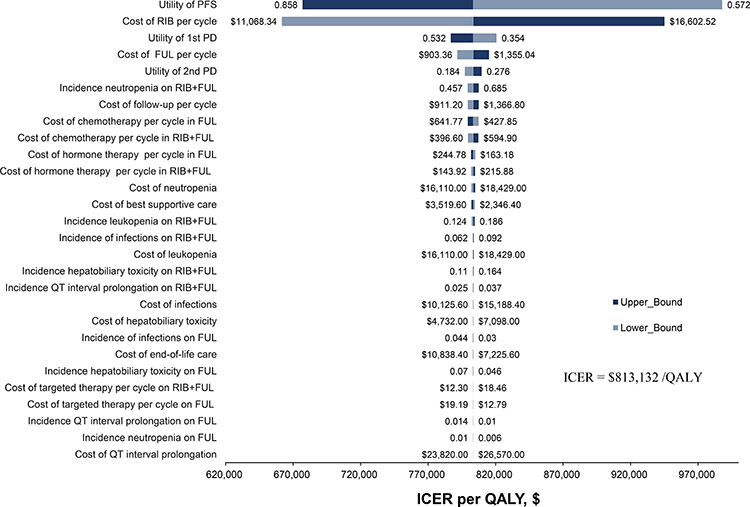 |
Figure 2 Tornado diagram for the one-way sensitivity analysis. Abbreviations: FUL, fulvestrant; ICER, incremental cost-effectiveness ratio; PD, progression disease; PFS, progression-free survival; RIB, ribociclib; QALY, quality-adjusted life year. Notes: The dark blue bar represents the upper bounds and the light blue bar represents the lower bounds for each variable. |
Probabilistic sensitivity analyses revealed cost-effectiveness probabilities of 0% for ribociclib plus fulvestrant and 100% for placebo plus fulvestrant at a WTP threshold of $150,000 in the United States (Figure 3). The ICERs were $454,464/QALY, $239,262/QALY, and $167,530/QALY at 50%, 20%, and 10% of the cost of ribociclib, respectively. Figure 3A shows the acceptability curves for the cost-effective probabilities according to each treatment strategy and the different WTP thresholds. Ribociclib plus fulvestrant was preferred in 5.3% and 53.9% of the simulations at 20% and 10% of the current cost of ribociclib, respectively (Table 3).
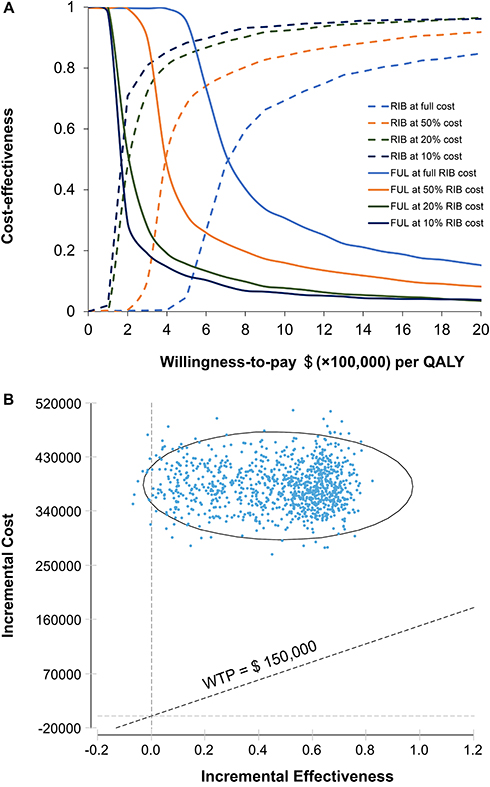 |
Figure 3 Probabilistic sensitivity analysis. Abbreviations: FUL, fulvestrant; RIB, ribociclib; QALY, quality-adjusted life year; WTP, willingness-to-pay. Notes: (A) Cost-effectiveness acceptability curves revealed the effects of cost on the probability of being cost-effective; (B) Incremental cost-effectiveness scatterplot for 10,000 Monte Carlo simulations revealed a low probability of cost effectiveness. |
Discussion
The MONALEESA-3 trial was a large randomized phase III trial that recently revealed significant improvements in PFS and OS after first-line treatment using ribociclib for postmenopausal women with HR-positive, HER2-negative ABC.10,13 Nevertheless, these benefits must be considered in the context of substantially increased costs, which generated an ICER of $813,132/QALY, and this result suggests that ribociclib is not cost-effective at current drug prices in the United States. Furthermore, there was a 100% probability that the ICER exceeded the WTP threshold of $150,000/QALY.
Our findings are consistent with existing evidence regarding CDK 4/6 inhibitor treatment for patients with HR-positive HER2-negative ABC. Mamiya et al evaluated data from the PALOMA3 trial and found that palbociclib plus fulvestrant was unlikely to be cost-effective with an ICER of $918,166/QALY, relative to fulvestrant alone.41 Another cost-effectiveness study evaluated CDK 4/6 inhibitors plus letrozole versus letrozole monotherapy and concluded that palbociclib and ribociclib were not cost-effective in the United States based on ICERs of $634,000/QALY for palbociclib plus letrozole and $440,000/QALY for ribociclib plus letrozole.43 Using clinical data of MONALEESA-7 trial, an analysis indicated that adding ribociclib to endocrine therapy was not cost-effective as first-line treatment for premenopausal women from the Singapore healthcare system perspective.44 Conversely, Mistry et al reported that ribociclib plus letrozole was a cost-saving choice as first-line treatment option for postmenopausal women in the US.45 Based on MONALEESA-2 trial, an analysis by the manufacturer for the National Institute for Health and Care Excellence of the United Kingdom reported an ICER below the WTP threshold of £30,000/QALY and recommended ribociclib as the first-line treatment of HR-positive, HER2- negative breast cancer.3,46 Likewise, from a Chinese perspective, ribociclib plus letrozole was estimated nearly 90% likelihood of being cost-effective at a threshold of $24,360/QALY, when the cost of ribociclib less than $721 per 4 weeks in China.47 These studies were conducted for markedly different health care systems with different costs and WTP thresholds. In addition, as the immaturity of OS data in the studies of CDK4/6 inhibitor, the published cost-effectiveness analyses were either based on immature OS data or other clinical trials which could have a significant impact on the final results.
To the best of our knowledge, this is the first Markov model-based study to investigated the cost-effectiveness of ribociclib plus fulvestrant versus placebo plus fulvestrant for postmenopausal female patients with HR-positive, HER2-negative ABC. Our model considered three lines of treatments and eight subpopulations to provide a comprehensive assessment of costs and benefits to help guide clinical decision-making. The results revealed that prolonging PFS and OS in an incurable setting was associated with substantially increased costs, and the cost of ribociclib ($13,835/4-week cycle) already exceeded $150,000/year before considering the costs of ancillary care and less-than-perfect health state utilities. Furthermore, patients who received ribociclib had increased risks of serious AEs, especially neutropenia and leukopenia, which were associated with lengthy hospitalizations, prolonged treatment, and increased monitoring costs. These factors may might explain why ribociclib is not cost-effective even with the most favorable assumptions. Nevertheless, the ICER approached the WTP threshold when the price of ribociclib was $1,384/cycle (10% of the current price), and the probability of cost-effectiveness at that threshold was >50% in the United States. Therefore, a substantial reduction in the cost of ribociclib might help improved its cost-effectiveness.
One-way sensitivity analysis revealed that the utility of PFS had the greatest effects on our findings. The health utility values in our model were derived from previous reports, which limits the accuracy of our results. When the utility of PFS was adjusted to the lower and upper values, the estimated ICER for ribociclib plus fulvestrant versus fulvestrant alone was still >$600,000/QALY, which suggests that the effects of the PFS utility scores on the long-term results were modest between the two groups. The subgroup analyses revealed that greatest decrease in ICER was in patients with only bone metastasis, followed by patients without liver or lung involvement and ≤2 metastatic sites. However, the decreased ICERs were still well above the WTP threshold of $150,000/QALY, which suggests that ribociclib plus fulvestrant was not cost-effective relative to placebo plus fulvestrant across the patient subgroups.
This study has several limitations that should be considered. First, the cost-effectiveness model was used to evaluate simulated data from a highly selected group of patients who were included in a randomized clinical trial, which suggests that external validation is required. In addition, real-world data are needed to evaluate cost-effectiveness based on the entire treatment sequences. Second, we extrapolated the long-term survival outcomes using short-term PFS and OS data from the MONALEESA-3 trial, which is subject to uncertainty. Although we considered three lines of treatment to account for normal clinical scenarios, long-term follow-up data are needed to validate our findings. Third, we did not consider the costs of grade 1–2 AEs, which suggests some underestimation in the overall treatment costs. However, the sensitivity analysis revealed that AEs had only modest effects across the two treatment strategies. Finally, the hypothetical cohorts of patients in our model were based on the characteristics of patients included in the MONALEESA-3 trial, which only enrolled postmenopausal patients. Therefore, further studies are needed to investigate the cost-effectiveness of ribociclib in premenopausal patients.
Conclusion
From the perspective of United States payers, ribociclib plus fulvestrant may not be cost-effective for treating postmenopausal female patients with HR-positive HER2-negative ABC, relative to placebo plus fulvestrant, at current drug prices. However, further discussions and negotiations regarding to the price of ribociclib are warranted, given the significant PFS and OS benefits that are observed in this setting.
Acknowledgments
We would like to thank Editage (www.editage.cn) for English language editing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. doi:10.3322/caac.21590
2. Waks AG, Winer EP. Breast cancer treatment: a review. JAMA. 2019;321(3):288–300. doi:10.1001/jama.2018.19323
3. Hortobagyi GN, Stemmer SM, Burris HA, et al. Ribociclib as first-line therapy for HR-positive, advanced breast cancer. N Engl J Med. 2016;375(18):1738–1748. doi:10.1056/NEJMoa1609709
4. Baselga J, Campone M, Piccart M, et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N Engl J Med. 2012;366(6):520–529. doi:10.1056/NEJMoa1109653
5. Chlebowski RT. Changing concepts of hormone receptor-positive advanced breast cancer therapy. Clin Breast Cancer. 2013;13(3):159–166. doi:10.1016/j.clbc.2012.11.002
6. Rugo HS, Rumble RB, Macrae E, et al. Endocrine therapy for hormone receptor-positive metastatic breast cancer: American society of clinical oncology guideline. J Clin Oncol. 2016;34(25):3069–3103. doi:10.1200/JCO.2016.67.1487
7. Poggio F, Lambertini M, Blondeaux E, et al. Role of fulvestrant in the treatment of postmenopausal metastatic breast cancer patients. Expert Rev Clin Pharmacol. 2016;9(9):1153–1161. doi:10.1080/17512433.2016.1215243
8. Iorfida M, Mazza M, Munzone E. Fulvestrant in combination with CDK4/6 inhibitors for HER2- metastatic breast cancers: current perspectives. Breast Cancer. 2020;12:45–56.
9. Im SA, Lu YS, Bardia A, et al. Overall survival with ribociclib plus endocrine therapy in breast cancer. N Engl J Med. 2019;381(4):307–316. doi:10.1056/NEJMoa1903765
10. Slamon DJ, Neven P, Chia S, et al. Overall survival with ribociclib plus fulvestrant in advanced breast cancer. N Engl J Med. 2020;382(6):514–524. doi:10.1056/NEJMoa1911149
11. NCCN clinical practice guidelines in Oncology (NCCN guidelines) breast cancer. National Comprehensive Cancer Network. 2020. Available from: https://www.nccn.org/professionals/physician_gls/default.aspx#site.
12. Shah A, Bloomquist E, Tang S, et al. FDA approval: ribociclib for the treatment of postmenopausal women with hormone receptor-positive, HER2-negative advanced or metastatic breast cancer. Clin Cancer Res. 2018;24(13):2999–3004. doi:10.1158/1078-0432.CCR-17-2369
13. Slamon DJ, Neven P, Chia S, et al. Phase III Randomized Study of ribociclib and fulvestrant in hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: MONALEESA-3. J Clin Oncol. 2018;36(24):2465–2472. doi:10.1200/JCO.2018.78.9909
14. Elbasha EH, Chhatwal J. Theoretical foundations and practical applications of within-cycle correction methods. Med Decis Making. 2016;36(1):115–131. doi:10.1177/0272989X15585121
15. Zhang Y, Zeng X, Deng H, et al. Cost-effectiveness analysis of adding palbociclib as a second-line endocrine therapy for HR(+)/HER2(-) metastatic breast cancer from the US and Chinese perspectives. Clin Ther. 2019;41(6):1175–1185. doi:10.1016/j.clinthera.2019.04.033
16. Huntington SF, von Keudell G, Davidoff AJ, Gross CP, Prasad SA. Cost-effectiveness analysis of brentuximab vedotin with chemotherapy in newly diagnosed stage III and IV hodgkin lymphoma. J Clin Oncol. 2018;36(33):3307.
17. Wan X, Zhang Y, Tan C, Zeng X, Peng L. First-line nivolumab plus ipilimumab vs sunitinib for metastatic renal cell carcinoma: a cost-effectiveness analysis. JAMA Oncol. 2019;5(4):491–496. doi:10.1001/jamaoncol.2018.7086
18. Posada D, Buckley TR. Model selection and model averaging in phylogenetics: advantages of akaike information criterion and bayesian approaches over likelihood ratio tests. Syst Biol. 2004;53(5):793–808. doi:10.1080/10635150490522304
19. Kohn CG, Zeichner SB, Chen Q, Montero AJ, Goldstein DA, Flowers CR. Cost-effectiveness of immune checkpoint inhibition in BRAF wild-type advanced melanoma. J Clin Oncol. 2017;35(11):1194–1202. doi:10.1200/JCO.2016.69.6336
20. Diaby V, Adunlin G, Montero AJ. Survival modeling for the estimation of transition probabilities in model-based economic evaluations in the absence of individual patient data: a tutorial. Pharmacoeconomics. 2014;32(2):101–108. doi:10.1007/s40273-013-0123-9
21. Wan X, Luo X, Tan C, Zeng X, Zhang Y, Peng L. First-line atezolizumab in addition to bevacizumab plus chemotherapy for metastatic, nonsquamous non-small cell lung cancer: a United States-based cost-effectiveness analysis. Cancer. 2019;125(20):3526–3534. doi:10.1002/cncr.32368
22. Centers for medicare and medicaid services: medicare Part B drug average sale price. 2020. Available from: https://www.cms.gov/medicare/medicare-part-b-drug-average-sales-price/2020-asp-drug-pricing-files.
23. Drugs.com [online]. 2020. Available from: https://www.drugs.com/price-guide/faslodex.
24. Bajetta E, Procopio G, Celio L, et al. Safety and efficacy of two different doses of capecitabine in the treatment of advanced breast cancer in older women. J Clin Oncol. 2005;23(10):2155–2161. doi:10.1200/JCO.2005.02.167
25. Seidman AD. Gemcitabine as single-agent therapy in the management of advanced breast cancer. Oncology (Williston Park). 2001;15(2 Suppl 3):11–14.
26. Seidman AD, Tiersten A, Hudis C, et al. Phase II trial of paclitaxel by 3-hour infusion as initial and salvage chemotherapy for metastatic breast cancer. J Clin Oncol. 1995;13(10):2575–2581. doi:10.1200/JCO.1995.13.10.2575
27. Perez EA, Vogel CL, Irwin DH, Kirshner JJ, Patel R. Multicenter phase II trial of weekly paclitaxel in women with metastatic breast cancer. J Clin Oncol. 2001;19(22):4216–4223. doi:10.1200/JCO.2001.19.22.4216
28. Gradishar WJ, Krasnojon D, Cheporov S, et al. Significantly longer progression-free survival with nab-paclitaxel compared with docetaxel as first-line therapy for metastatic breast cancer. J Clin Oncol. 2009;27(22):3611–3619.
29. Isakoff SJ, Mayer EL, He L, et al. TBCRC009: a multicenter Phase II clinical trial of platinum monotherapy with biomarker assessment in metastatic triple-negative breast cancer. J Clin Oncol. 2015;33(17):1902–1909. doi:10.1200/JCO.2014.57.6660
30. Silver DP, Richardson AL, Eklund AC, et al. Efficacy of neoadjuvant cisplatin in triple-negative breast cancer. J Clin Oncol. 2010;28(7):1145–1153. doi:10.1200/JCO.2009.22.4725
31. Chan S, Friedrichs K, Noel D, et al. Prospective randomized trial of docetaxel versus doxorubicin in patients with metastatic breast cancer. J Clin Oncol. 1999;17(8):2341–2354. doi:10.1200/JCO.1999.17.8.2341
32. Gasparini G, Dal Fior S, Panizzoni GA, Favretto S, Pozza F. Weekly epirubicin versus doxorubicin as second line therapy in advanced breast cancer. A randomized clinical trial. Am J Clin Oncol. 1991;14(1):38–44. doi:10.1097/00000421-199102000-00009
33. O’Brien ME, Wigler N, Inbar M, et al. Reduced cardiotoxicity and comparable efficacy in a phase III trial of pegylated liposomal doxorubicin HCl (CAELYX/Doxil) versus conventional doxorubicin for first-line treatment of metastatic breast cancer. Ann Oncol. 2004;15(3):440–449. doi:10.1093/annonc/mdh097
34. Finn RS, Martin M, Rugo HS, et al. Palbociclib and letrozole in advanced breast cancer. N Engl J Med. 2016;375(20):1925–1936. doi:10.1056/NEJMoa1607303
35. Mehta RS, Barlow WE, Albain KS, et al. Combination anastrozole and fulvestrant in metastatic breast cancer. N Engl J Med. 2012;367(5):435–444. doi:10.1056/NEJMoa1201622
36. Miller K, Wang M, Gralow J, et al. Paclitaxel plus bevacizumab versus paclitaxel alone for metastatic breast cancer. N Engl J Med. 2007;357(26):2666–2676. doi:10.1056/NEJMoa072113
37. Wong W, Yim YM, Kim A, et al. Assessment of costs associated with adverse events in patients with cancer. PLoS One. 2018;13(4):e0196007. doi:10.1371/journal.pone.0196007
38. Rashid N, Koh HA, Baca HC, Lin KJ, Malecha SE, Masaquel A. Economic burden related to chemotherapy-related adverse events in patients with metastatic breast cancer in an integrated health care system. Breast Cancer. 2016;8:173–181.
39. Sorensen SV, Goh JW, Pan F, et al. Incidence-based cost-of-illness model for metastatic breast cancer in the United States. Int J Technol Assess Health Care. 2012;28(1):12–21. doi:10.1017/S026646231100064X
40. Lloyd A, Nafees B, Narewska J, Dewilde S, Watkins J. Health state utilities for metastatic breast cancer. Br J Cancer. 2006;95(6):683–690. doi:10.1038/sj.bjc.6603326
41. Mamiya H, Tahara RK, Tolaney SM, Choudhry NK, Najafzadeh M. Cost-effectiveness of palbociclib in hormone receptor-positive advanced breast cancer. Ann Oncol. 2017;28(8):1825–1831. doi:10.1093/annonc/mdx201
42. Husereau D, Drummond M, Petrou S, et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. BMC Med. 2013;11:80. doi:10.1186/1741-7015-11-80
43. Zhang B, Long EF. Cost-effectiveness analysis of palbociclib or ribociclib in the treatment of advanced hormone receptor-positive, HER2-negative breast cancer. Breast Cancer Res Treat. 2019;175(3):775–779. doi:10.1007/s10549-019-05190-3
44. Loke L, Lee SC, Pearce F, Ng K, Aziz MIA. Cost-effectiveness of ribociclib as initial treatment for premenopausal women with advanced breast cancer in Singapore. Cancer Rep. 2020;e1308.
45. Mistry R, Suri G, Young K, et al. Budget impact of including ribociclib in combination with letrozole on US payer formulary: first-line treatment of post-menopausal women with HR+/HER2- advanced or metastatic breast cancer. Curr Med Res Opin. 2018;34(12):2143–2150. doi:10.1080/03007995.2018.1503484
46. Buyukkaramikli NC, de Groot S, Riemsma R, et al. Ribociclib with an aromatase inhibitor for previously untreated, HR-positive, HER2-negative, locally advanced or metastatic breast cancer: an evidence review group perspective of a NICE single technology appraisal. Pharmacoeconomics. 2019;37(2):141–153. doi:10.1007/s40273-018-0708-4
47. Wan X, Zhang Y, Ma J, Tan C, Zeng X, Peng L. Ribociclib in hormone-receptor-positive advanced breast cancer: establishing a value-based cost in China. Breast. 2019;43:1–6. doi:10.1016/j.breast.2018.10.004
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.